Upload
others
View
7
Download
0
Embed Size (px)
Citation preview
Physiomimetic Models of AdenomyosisJuan S. Gnecco, PhD1,2 Alex T. Brown, PhD1,2 Ellen L. Kan, BS1,2 Lauren Baugh, PhD1,2
Clara Ives, BS1,2 Megan Loring, MD1,3 Linda G. Griffith, PhD1,2
1Center for Gynepathology Research, Massachusetts Institute ofTechnology, Cambridge, Massachusetts
2Department of Biological Engineering, Massachusetts Institute ofTechnology, Cambridge, Massachusetts
3Endometriosis and Adenomyosis Care Collaborative, Center forMinimally Invasive Gynecologic Surgery, Newton Wellesley Hospital,Newton, Massachusetts
Semin Reprod Med 2020;38:179–196
Address for correspondence Linda G. Griffith, PhD, MassachusettsInstitute of Technology, Room 16-429, 77 Massachusetts Avenue,Cambridge, MA 02139 (e-mail: [email protected]).
Deconstructing Adenomyosis:What to Model?
In constructing any in vitro disease model, the first question is“whattomodel.”Thisquestionisoftenrelativelyeasilyansweredfordiseases with germ line genetic mutations and clearly definedclinical phenotypes directly linked to themolecularmutation, suchascysticfibrosis. Insuchcases,highthroughputphenotypicscreens
in cell lines, based on correcting a known molecular defect, havebeen remarkably effective in identifying blockbuster clinical thera-pies.1Adenomyosis isarguablyat theoppositeendof thespectrum.
First, the clinical landscape is convoluted: adenomyosis isover 10 times more prevalent than most single-gene defectdiseases; symptoms overlap and are comorbid with myriadother diseases and conditions; there is no consensus on thedefinition of “disease” nor a clearly defined set of metrics to
Keywords
► adenomyosis► organoids► models of
adenomyosis► tissue engineering► microfluidic device
Abstract Adenomyosis remains an enigmatic disease in the clinical and research communities.The high prevalence, diversity of morphological and symptomatic presentations, arrayof potential etiological explanations, and variable response to existing interventionssuggest that different subgroups of patients with distinguishable mechanistic driversof disease may exist. These factors, combined with the weak links to geneticpredisposition, make the entire spectrum of the human condition challenging tomodel in animals. Here, after an overview of current approaches, a vision for applyingphysiomimetic modeling to adenomyosis is presented. Physiomimetics combines asystem’s biology analysis of patient populations to generate hypotheses aboutmechanistic bases for stratification with in vitro patient avatars to test these hypothe-ses. A substantial foundation for three-dimensional (3D) tissue engineering of adeno-myosis lesions exists in several disparate areas: epithelial organoid technology;synthetic biomaterials matrices for epithelial–stromal coculture; smooth muscle 3Dtissue engineering; and microvascular tissue engineering. These approaches canpotentially be combined with microfluidic platform technologies to model the lesionmicroenvironment and can potentially be coupled to other microorgan systems toexamine systemic effects. In vitro patient-derived models are constructed to answerspecific questions leading to target identification and validation in a manner thatinforms preclinical research and ultimately clinical trial design.
Issue Theme Adenomyosis andEndometriosis; Guest Editors,Linda C. Giudice, MD, PhD, MSc,Lisa M. Halvorson, MD, ElizabethA. Stewart, MD, and LukRombauts, PhD, FRANZCOG, MD
DOI https://doi.org/10.1055/s-0040-1719084.ISSN 1526-8004.
Copyright © 2020 by Thieme MedicalPublishers, Inc., 333 Seventh Avenue,New York, NY 10001, USA.Tel: +1(212) 760-0888.
THIEME
179
Published online: 2020-11-09
mailto:[email protected]://doi.org/10.1055/s-0040-1719084https://doi.org/10.1055/s-0040-1719084
diagnose it and assess response to therapy; anddiagnostic biastoward older multiparous patients clouds true incidence.2–5
Patientswith pain, heavymenstrual bleeding, and/or infertili-ty may have adenomyosis—or something else entirely—as anunderlying cause.6 About 40% of patients with symptoms, butno indication of adenomyosis onmagnetic resonance imaging(MRI) or ultrasound, are found to have adenomyosis lesionsuponhistopathological assessment.7Symptom-targeting ther-apies for adenomyosis, like those for endometriosis,8 workremarkablywell in some patients, but are not at all effective ortolerated in others.Moreover, there is neither reliablemannerto predict who will respond nor alternative therapies (otherthan developing copingmechanisms around eternal suffering)for those who do not.9,10 As such, adenomyosis is not onedisease, and it is unlikely there is one model that captures allsalient features for all patients.
Second, the etiologies—given the prevalence and vastdiversity in patient presentations, there is likely more thanone—are obscure: adenomyosis appears to arise from acomplex web of gene–environment interactions that maystart in utero; it might be triggered perinatally via seeding ofthe myometrium by cells that escape the endometrium; itmight arise later in life due to uterinemechanical injury; or itmight arise due to invasion of the myometrium by endome-trium injured by an inflammatory insult.2,4,11–13 This diver-sity of possible etiologies, along with the diversity of clinicalpresentations, underscores a shortcoming in how the diseaseresearch has traditionally been approached: adenomyosis is“a” disease. Yet, every patient is different.While there are notlikelymillions of individual diseases, there are likelymultipledifferent constellations of molecular networks—immunenetworks, invasion networks, and metabolic networks—that go awry to instigate symptomatic and phenotypicappearance of ectopic endometrium in the myometrium,giving rise to groups of patients who could potentially bestratified molecularly as has been proposed for endometri-osis.8,9,14–17 Animal models—where strain variation, geneticperturbations, and targeted interventions to modulate spe-cific pathways can be deployed to probe potential contribu-tions to the adenomyotic etiology—offer insights into whereto look for such mechanistic stratification in humans.
This last point brings us to the third big challenge withmodeling adenomyosis—the relative lack of deep clinical andpathological phenotyping to guide patient stratification intotractable and mechanistically targetable subgroups.5 Suchclinical phenotyping and disease staging/classification isintertwined with therapeutic development through impactson reimbursements for treatment18 and evaluation of effica-cy of various forms of treatment for clusters of patients withwell-defined characteristics, as is done most thoroughly forcancer.19,20 In this way, adenomyosis is the sister, though notprecisely the twin, of endometriosis, which is inadequatelystaged based on lesion number, size, and location.8 Likeendometriosis, adenomyosis is currently only definitivelydiagnosed via surgical intervention (usually, a hysterectomy)and histopathological characterization. However, adeno-myosis, as one of several pathologies that contribute toabnormal uterine bleeding (AUB), is included in the PALM-
COEIN system for classifying such disorders, as first de-scribed in 20116 and updated in 2018.21 PALM-COEINserves as a crucial tool for patient–clinician–researchercommunication; hence, it is a step toward personalizedmedicine for the patients suffering from AUB as a symptomof adenomyosis.
The state of personalizedmedicine for adenomyosis is stilldistant from as compared with cancer and other diseases. Inthis era of molecular stratification, oncologists routinelytailor treatments to a combination of physical features inaddition to molecular biosignatures linked to disease mech-anism and prognosis, sometimes using patient-derived orga-noids or tissue models to test drug sensitivity.22 Mechanisticmarkers also inform the development of preclinical in vitromodels, providing scientists an essential connection to thetranslational medicine. Such approaches are nascent only forendometriosis and even more primitive for adenomyosis, inpart because somatic mutations, which are highly informa-tive in cancer, are at best weakly associated with ectopicendometrial diseases. Hence, classifications based on proteinor metabolic network states (or possibly epigenetics), com-plemented with clinical phenotypic data incorporating pa-tient symptoms and life-long prognosis,17,23,24 are thereforean appealing route to classification; such approaches willlikely yield constellations of “molecular signatures” of dis-ease state, rather than one single indicator of “diseased, ornot.”14 An exemplary model for how other noncancer im-mune-mediated disease communities have spurred suchphenotyping is the Juvenile Diabetes Research Foundation-sponsored Network for Pancreatic Organ Donors with Dia-betes (nPOD) program.25 Application of programs like thesewould significantly improve our understanding of adenomy-otic disease.
Finally, a fourth challenge is which stage(s) of disease tomodel. Modeling the features of disease as they present indiagnosed patients, who often have advanced varieties ofdisease progression, is arguably essential for identifyingmolecular targets and developing new therapies to treatthese patients, and even more so for judicious prescriptionof existing therapies. Modeling proposed etiologies mayyield preventive measures, or early treatment options, pre-suming a diagnostic for nascent stage disease, can be defined.The features of such models—and the throughputs requiredfor getting useful information out of them—are somewhatbut not entirely overlapping. Patients with advanced diseasemay also have nascent progressing disease, for example.Precise definition of the clinical phenotype, along withmechanistic hypotheses about the features of disease beingstudied, as they relate to the clinic, is an essential first step indesigning, and then in implementing, in vitro models ofadenomyosis.
A Roadmap of Phenomena to Model
How do we define what to model? Adenomyosis studiesgenerally lack the kind of deep clinical phenotyping that linksmolecular and cellular pathological findings to patient symp-toms, comorbidities, andtreatment responses.However, several
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.180
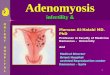
commonly observed pathological phenotypes can be modelednow using in vitro models, with a longer-term goal of morespecialized patient avatars focusing on specific subgroups. Theoverall vision for the role of in vitro models is illustratedin ►Fig. 1. Briefly, we envision that there are a relatively smallnumber of subsets of patients who are phenomenologicallysimilar, but distinct enough from each other that differenttherapeutic approaches are needed. Tissues and body fluidsharvested from patients are used on the one hand for “omics”analysis—which can include genomics, proteomics, metabolo-mics—of molecular/cellular networks that enable stratificationof patients into groups with data-informed machine learningmethods,14 based at least in part on mechanistic hypothesesthat may distinguish the groups. Mechanistic stratificationoffers a path to target identification and experimental hypothe-sis testing. On the other hand, tissue banks created from thepatients are used to create patient avatars that can be used totest hypotheses about mechanistic stratification and targets,
with thegoal of informing translational researchandemployingpersonalized therapies (►Fig. 1). In vitro models can thuspotentially inform directions in clinical phenotyping, in aniterative fashion.
Conceptualizing Models of Adenomyosis“Physiomimetics” is the process of conceptualizing a complexphysiological process to defineessential features, thenbuildingin vitro models that capture the most relevant aspects ofphysiology in ways that can ultimately yield clinically action-able outcomes. Physiomimetic models encompass a range ofexperimental complexities, from relatively standard culture ofindividual cell types up through complex three-dimensional(3D) microfluidic models, driven by biological questions. Westart here by conceptualizing established adenomyosis lesionphenotypes and the dynamic behaviors implicated in theirpathophysiology, as the etiology of nascent adenomyoticlesions is still obscure, and there is great need to treat
Fig. 1 Physiomimetic approach for developing targeted therapies for adenomyosis. Hypotheses regarding different mechanisms of diseasethat may be operative in patient subgroups are tested with tissue and fluid samples from a large patient population containing the subgroups (1);analysis of tissue and fluid samples to refine hypotheses about mechanism (2a and 3) are performed in tandem with development of cell banksand construction of patient avatars (2b). Mechanistic hypothesis about patient subgroups and interventions can then be tested in patientavatars representing the subgroups to define stratified clinical trials, or inform more judicious use of existing therapies.
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 181
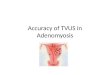
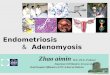
established adenomyotic lesions. Furthermore, the mecha-nisms contributing to disease progression may be operativeto some extent in disease onset. We focus on diffuse adeno-myosis lesions, as cystic adenomyosis lesions can in someinstances be treated surgically.26 Conceptually, here we defineadenomyotic lesion as the ectopic presence of lesion-initiatingcells—endometrial epithelial glands and stroma—surroundedby the lesionmicroenvironment comprisingmyometrialmusclecells, nerves, vasculature, and immune cells with associatedextracellular matrix (ECM; ►Fig. 2).
Dynamic behaviors of lesion-initiating cells that are im-plicated in pathologies include (1) invasion into surroundingmicroenvironment, potentially seeding new, distant lesions;(2) proliferation, which may drive lesion growth, invasion, orfeed into a hormone-driven cycle of cell death and prolifera-tion; and (3) production of inflammatory cytokines, chemo-kines, proteases, and other modulators of signaling andremodeling of the local microenvironment27,28 (►Fig. 2).The dynamic responses of the microenvironment associated
with pathologies include (1) smooth muscle hyperplasia oflocal myometrial cells (or recruitment of fibroblasts ormesenchymal stem cells that acquire that phenotype29);(2) influx and activation of immune cells; (3) recruitmentof vasculature and modulation of vascular permeability,possibly with local bleeding and clotting; (4) enhancementof sensory innervation and regression of sympathetic inner-vation; and (5) stiffening of the local microenvironment, viamatrix deposition and cellular changes. Cells within lesionsrespond to local cues, includingmechanical stimulation frommyometrial contractions, and to systemic cues, notably sexsteroids, but are also modulated by nutrition, systemicinflammation, stress hormones, and other factors. Theseresponses play out in an orchestrated fashion, as each celltype expresses a unique repertoire of receptors for the cues,including estrogen and progesterone receptors.30–32Many ofthe same phenomena are the subject of substantial investi-gation in carcinomas, but the spotlight on dynamic changesspurred by cyclic variation in sex steroids is omnipresent in
Fig. 2 Conceptualization of an adenomyosis lesion, showing the biological components and pathological processes to consider in building an invitro model.
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.182
adenomyosis. After a review of the known features of themyometrium and its changes in adenomyosis, we thenconsider how each of these dynamic phenomena can bemodeled in vitro.
The Uterus in AdenomyosisThe presence of adenomyosis in the myometrium induceschanges throughout the uterus inways that suggest interest-ing hypotheses that can be tested using well-designed invitro models. The myometrium is composed of the innermyometrium (or junctional zone, JZ), characterized as havinga relatively greater cell density with relatively less ECM, andthe outer myometrium, which is more ECM-rich and has alower cell density.33 On a cellular level, the myometriumcomprises layers of smooth muscle cells (SMCs) arrangedinto fibular bundles approximately 0.3mm in diameter,interwoven with blood vessels and connective, lymphatic,and nerve tissue.33,34 These layers of SMC bundlesare oriented in different directions around the uterus toenable complex contractile patterns that drive fluid flow inthe nonpregnant uterus.33 In adenomyosis, these contractilefunctions can become dysregulated.35,36 Like the endome-trium, the inner myometrium/JZ exhibits molecular andcellular changes in response to cyclic hormones throughthe menstrual cycle—such as tissue thickening and modula-tion of estrogen and progesterone receptor expression—butthe outer myometrium appears less sensitive to menstrualcycle hormonal changes at both the gross anatomical leveland themolecular level.37–39How these differences translateinto the propensity for adenomyosis lesions to drive symp-toms is unknown, but it is a potential facet that could bemodeled in vitro. The healthy human myometrium is typi-cally well delineated from the endometrium, but this cleardelineation is blurred in adenomyosis, suggesting invasion ofcells from the endometrium into the myometrium, attribut-ed by one theory to microtraumas at the endometrial–myometrial interface during uterine peristalsis.11,38,40–43
Changes in ECM architecture and composition, as well assmooth muscle hyperplasia of the region immediatelysurrounding lesions, characteristically affect multiple celltypes and may involve chemical and mechanical cues.Patients with adenomyosis have been shown to have in-creased levels of matrix metalloproteinases (MMP)-2 and-9, suggesting abnormal matrix remodeling may be presentin these patients.44 Inflammation may be driven by repeat-ed local bleeding in the lesion,45 which may further en-hance contractile phenotypes that in turn drive fibrogenicprocesses.46
Endometrial cells in adenomyotic tissue exhibit many aber-rant behaviors, including apparent resistance to progesterone,epithelial–mesenchymal transitions, decreased apoptosis re-gardless of menstrual phase, and other processes.11 Althoughadenomyosis-targeting therapeutic approaches are intendedto suppress aberrant proliferation of endometrial-derived tis-sues by targeting proestrogenic pathways or inducing proges-terone action,11 these approaches fail in some patients, afinding consistent with dysregulation of specific hormonereceptors ESR1, ESR2, and PGR isoforms A and B in adenomyo-
sis.47,48 The downstream consequences of estrogenic signalingand acquired progesterone resistance that may contribute tothe etiologyofdiseaseare still notwell understood, and invitromodels offer an opportunity to parse the individualmechanisms.
Adenomyosis is associated with both pain and heavy men-strual bleeding. Several studies have reported an increasedsensory nerve fiber density in both ectopic lesions and eutopicendometrium inwomenwith endometriosis, along with reduc-tion in sympathetic nerves, suggesting a possible diagnosticcriterion.49–52 Nerve fibers are increased in the fibrotic endo-metriosis nodules in the rectovaginal space and greater nervefiber infiltration of lesions is found in patients with greaterpain.53–55 Increased nerve fiber density is also associated withan increase inmacrophages,56with some evidence of estrogenmodulation of the crosstalk.57 Similar analysis of nerve fiberandmacrophagedensity inadenomyosis is relatively scarce, butone study examined nerve fiber density in the endometriumand myometrium of women with adenomyosis and fibroids,and found no difference.58
The immune environment in the uterus is dynamic, withdramatic increases in the number of macrophages, uterinenatural killer (NK) cells, and other immune componentsduring the secretory phase. The extent to which theincreased number of immune cells arises from in situ prolif-eration of tissue-resident cells or from recruitment of circu-lating monocytes is still unclear.59–61 Furthermore, whetherCD45þ intraepithelial lymphocytes (IELs) that are character-istically observed in the epithelial layer in adenomyosislesions62 derive from locally recruited cells (and are there-fore part of the microenvironment) or derive from IELspresent in the epithelial layer of the eutopic endometrium(and are therefore lesion-initiating cells) is unknown. Thecrosstalk betweennerves andmacrophages or other immunecells may contribute to pain and/or bleeding. An intriguingclinical finding, albeit from a small study, examined macro-phage density in the uteri of 54 patients undergoing hyster-ectomy for adenomyosis due to pain as the primarysymptom, with a comparison group of 20 women undergo-ing hysterectomy for adenomyosis with heavy menstrualbleeding as the primary symptom,63 where adenomyosiswas tentatively diagnosed by both transvaginal ultrasoundand MRI prior to surgery. Greater leukocyte infiltration wasseen in both the myometrium and endometrium of patientswith pain, and groups ofmacrophageswere seen near lesionsand interspersed in the muscle in the patients with pain; inboth groups, there were macrophages around blood vessels,as macrophages are known to regulate vessel permeability.64
Although the detailed interactions between the vasculatureand adenomyotic lesions are not fully appreciated in theestablishment and progression of adenomyosis, increasedmicrovessel density has been observed in adenomyosis,65,66
and a recent meta-analysis of studies examining vascularmorphology and marker expression in the myometrium andendometrium suggests increased angiogenesis in the endo-metrium of women with adenomyosis.67 Early studies thatexplored immune responses in adenomyosis showed thatthe disruption of the JZ at the endometrial–myometrial
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 183
interface may result from the abnormal aggregation ofmacrophages in the myometrium, similar to the increasednumber of macrophages previously observed in endometri-osis patients.68 Finally, intriguing data on sex hormoneresponsiveness of mast cells, which are among the mostcommon immune cell types in the myometrium and impli-cated in the pain associated with interstitial cystitis, maycontribute to adenomyosis symptoms.69 These observationssuggest that recapitulating immune–epithelial–neuronalinteractions in vitro using patient-specific cells may yieldinsights between symptomology and molecular and cellularbehaviors characteristic of distinct patient populations.
Interestingly, the eutopic endometrium of patients withadenomyosis confer dysregulated angiogenesis, innerva-tion, immune cell presence, and gene and protein expres-sion that suggest greater invasive and survival potential atectopic sites and contribution to symptoms.70–74 Globalchanges in the myometrium outside the peri-lesion envi-ronment, including smooth muscle hypertrophy, increasedstiffness, and immune cell infiltration,38,75 raise questionsabout whether these global changes precede, or are theresult of, lesion establishment—a hypothesis that couldpotentially be tested in vitro.
Designing, Building, and Interpreting InVitro Models
The growing evidence that animal models do not captureessential features of humandiseases involving chronic inflam-mation, sex steroid signaling, or other complex, molecularphenomena is driving development of sophisticated in vitromodels that capture complex tissue architecture, and evendynamic perfusion of microvascular networks, using humanpatient-derived cells. While these approaches are just nowemerging, especially driven by applications in cancer, cardio-vascular, and liver diseases, they offer promise for modelingadenomyosis. In this section, we review basic approaches totissue engineering of the uterine environment, includingdiscussion of cell sourcing and 3D model design. Then, in thenext section,we turn tomodeling specific phenotypic facets ofadenomyosis including invasion, vascular and systemic inter-actions, mechanics, and innervation, drawing from impactfulwork in disparate tissue systems.
Basic Approaches in Tissue Engineering of theEndometrium and MyometriumThe functions of the uterus arise from the integrated actionsof epithelia, stromal fibroblasts, myometrial smooth muscle,immune cells, and endothelial cells, which are each directlyand indirectly responsive to variations in sex hormones.Thus, many responses of various cell types to hormonechanges are indirect and governed by dynamic communica-tions with other cells. The endometrial epithelial response toprogesterone, for example, is governed by signaling proteinsproduced by the progesterone-responsive stromal fibro-blasts, which in turn respond to endothelial-derived signalsto enhance the decidualization process.31,76 While parsingresponses of individual cell types to hormonal and other
perturbations in vitro is an essential first step to understand-ing the integrated responses, building models that capturethe dynamic interlinked hormone responsiveness in vitro isultimately essential for illuminating complex phenomenalike adenomyosis.
Cell Sources: Explants, Cell Lines, Primary CellsFor decades, explant cultures of the endometrium andmyome-triumwere the only external window into the functions of thehuman uterus in vitro36,77–81 and, until recent advances inprimary cell culture, they remained preferred models for anal-ysis of complex primary tissue functions.31,81,82 Endometrialexplants in the absence of ECM quickly deteriorate,83 but canundergooutgrowthandremodelingwhenembedded inafibrinmatrix.84 For the endometrium—the presumed instigator ofadenomyosis lesions—definition of protocols for isolating andculturing epithelial cells and stromal fibroblasts from endome-trial biopsies85 enabledmechanistic studies on patient-derivedsamples, allowing diverse healthy and diseased donors to becombined in different ways to parse contributions of each celltype to health and disease. Primary cells remain the goldstandard for mechanistic disease studies, but permanent epi-thelial86,87andstromal88–90cell lines thatexhibitmany(butnotall) tissue-specific hormone-responsive features, and somedisease states, have been routinely used for protocol develop-ment, pilot studies, and investigations of general features ofendometrial cell behavior. The carcinoma-derived Ishikawacell line is most commonly used for “normal” epithelia,91–93
the h-TERT-immortalized endometriosis-derived “12Z” line isused for invasive endometrial epithelia,15,87,94 and the h-TERT-immortalized stromal cell line “tHESC”89,91 is used for endo-metrial stromal cells. (Caution: cell line contamination wasreported for the endometrial epithelial cell line “HES”86; hence,routineSNPprofilingofcell lines is recommended for these, as itis with all cell lines, to validate provenance.) While cell linesoffer convenience and relatively good reproducibility, includingfrom laboratory to laboratory (subject to the typical cell linedrift), they have some shortcomings for reproducing primarycell behaviors,91 including greatly skewed cytokine andgrowthfactor production profiles.95 Pilot studies with cell lines can,however, offer insights that can be investigated further inmoredifficult-to-culture primary cells.15
The majority of studies on primary endometrial cells focuson stromal cells, as they can readily be expanded in standardculture and frozen to create tissue banks, allowing repeatedstudies from the same donor within limits of passage num-ber.96,97 For years, however, investigators were limited by thelack of robust protocols for expansion and cryopreservation ofendometrial epithelial cells, with few laboratories reportingsuccess.98 The landscape changed dramatically in 2017 withpublication of the first two studies describing robust expan-sion and cryopreservation of human endometrial epithelialcells as organoids (►Fig. 3a), with retention of hormoneresponsiveness, cellular architecture, polarity, heterogeneity,and other functions,99,100 using modifications of protocolsfirst described by Clevers and coworkers for expansion ofhuman intestinal epithelia.101 In the Clevers approach, epithe-lial cells are either dispersed as individual cells or fragments
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.184
and cultured inMatrigel, a basementmembrane-rich isolate ofa tumor cell line propagated in mice.101 While Matrigel hadlong been used as an ECM for 3D culture of endometrialglands99,102 and many other types of epithelial cells, enablingremarkable retention of tissue phenotype, Clevers defined acocktail of growth factors andothermediumsupplements thatspur dramatic proliferation of the stem cell compartment,allowing the cells in an initial biopsy to expand orders ofmagnitude in culture and withstand cryopreservation, whilepreserving their ability to differentiate into proper tissuephenotypes upon a change inmedium composition to removestem cell cues.101 This organoid approach has also beenapplied to derive continuously propagated organoid culturesfrom ectopic endometrium and endometrial tumors.103
An additional advance essential to building and character-izingphysiologically relevant3Dmodels is the identificationofboth mesenchymal and epithelial stem and progenitor cellcompartments within the human endometrium.96,104–106
Intriguingly, recent data suggest that stem or at least progeni-tor cells are present in the endometrial functional layer andluminal regions of the endometrium, as evidenced by in situhybridization for expression of the epithelial stem cell markerLGR5.107 The tools to identify putative stem and progenitorcells arevaluable inassessing thephenotypic statesofcells thatare used to initiate models, and to assess their phenotypesunder long-term culture conditions, especially to test hypoth-eses regarding possible contributions of these stem cells toectopic adenomyosis lesions.108 Related to efforts to identify
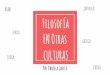
Fig. 3 Development of 3D in vitro models using synthetic hydrogels and endometrial epithelial organoids technologies. (a) Endometrialepithelial organoids (EEOs) promote the culture, expansion, and propagation of epithelial cells using 3D hydrogel systems. EEOs retain epithelialstructure, heterogeneity, and function of the native tissue glands. (b) Bio-labile, synthetic extracellular matrices (ECMs) can be designed toestablish EEOs cultures and cocultures that include additional cell populations, such as endometrial stromal cells (ESCs). (c) Polyethylene glycol(PEG)-derived hydrogels are fully defined, modular, and can be tuned by modifying their molecular and biophysical properties to mimic keyfeatures of the adenomyotic and endometriotic phenotype.
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 185
and characterize functions of stem and progenitor cells inpostnatal endometrium are efforts to create uterine tissue denovo from induced pluripotent stem cells (iPSCs), which couldpotentially advance patient-specific disease modeling as theyhave for other diseases. Encouragingly, a protocol for creationof human stromal cells with responses to progesterone char-acteristic of endometrial stromal cells undergoing deciduali-zation in vitro has been developed,109 providing a foundationfor future efforts to reproduce other uterine tissues.
Tomodel the pathogenesis of adenomyosis, it is importantto consider its ectopic environment in addition to the lesion-initiating cells. The myometrium comprises several celltypes, but themajor focus in in vitromodels is onmyometrialSMCs, which have different properties in the inner (JZ) andouter myometrium and express different receptor and sig-naling repertoires.33,37,110 Protocols for deriving and cultur-ing primary SMCs developed for many other tissues(vascular, intestinal, etc.) facilitated development of robustprotocols for isolation and culture of myometrial SMCs,which are commonly obtained from hysterectomy or caesar-ean section specimens. Cell origin (geographic location,pregnant or nonpregnant uterus) is an important consider-ation in defining primary cell source for myometrium. Per-manent myometrial cell lines are also widely used forcircumscribed studies such as screening drug actions.111–113
Finally, all studies with patient-derived cells must carefullyconsider the donor profiles in design and interpretation ofexperiments. Age and parity may influence donor cell pheno-type. Unlike endometriosis lesions, which can be collectedfrom even very young patients, almost all myometrial tissue,along with adenomyosis lesion tissue, is derived from hyster-ectomy specimens. Although protocols for resecting and biop-sying adenomyotic tissue have been described,7,26,114 theseprocedures are not widely practiced. Thus, significant barriersexist in creating tissue banks from young patients who sufferfrom adenomyosis.
General Approaches to 3D Tissue Engineering ofEndometrium and Myometrium Using Natural andSynthetic ECMsAn enduring challenge at present is to define suitable con-ditions to sustain long-term cocultures of multiple endome-trial cell types that each has their own ECMandgrowth factorrequirements. Matrigel comprises a mix of proteins andproteoglycans typical of the epithelial basement membrane,which filters proteins from the stromal compartment thatrequires a type I collagen and fibronectin-rich ECM with avery different composition of proteoglycans and associatedmatrix-bound growth factors.115 The first 3D primary cellendometrial coculture model, tailored for studying blasto-cyst implantation, addressed this by embedding stromalfibroblasts in a collagen gel, mimicking features of thestromal matrix, which was coated by a thin layer of Matrigelonto which the epithelial cells were seeded, resulting in aconfluent well-differentiated epithelia monolayer compris-ing ciliated and secretory (glandular) epithelia.116 Versionsof this model using cell lines, with stromal cells in collagentopped with Matrigel, were adapted to mimic the upregula-
tion of MMPs and accompanying matrix degradation follow-ing progesterone withdrawal as a trigger ofmenstruation28,117 as well as some features of themenstrualresponse to hormones, and other shorter-term aspects ofstromal epithelial communication.91,118 In a simpler version,in which stromal cells were embedded in Matrigel withepithelial cells on top, epithelial cells underwent 3D mor-phogenesis and proliferated, but stromal cells were relativelynonproliferative within the gel,119 suggesting the need forcell-type–tailored ECM. An alternate approach, adapted froma successful clinical matrix for healing full-thickness (der-mal–epidermal) wounds in skin, is to seed stromal cells in aporous collagen matrix fabricated by freezing and lyophiliz-ing a type I collagen solution, and overlaying the matrix withepithelial cells, which produce their own basementmembrane.120
These models employing natural ECMs have shortcomings,in part because there are no “one-size-fits-all” ECMs for bothepithelia and stroma (andpotentially other cell types), and alsobecause natural proteins are impure (Matrigel has myriadgrowth factors); are substantially variable from lot-to-lot; arerelatively rapidly degradedbycells; and are subject tovariationin structural and mechanical properties depending on howquickly or slowly the gels are polymerized.115,121 Variation isfurther exacerbated as some investigators use atelocollagen,which yields very different outcomes than whole collagen.122
These shortcomings have prompted a sustained effort in thebiomaterials community to create synthetic alternatives toMatrigel and collagen.123,124 A popular approach exploits therelative inertness of poly(ethylene glycol) (PEG), which iscommercially available in multi-arm star/branched configura-tions activated with cell-compatible reactive groups, to createmodular cell-encapsulating hydrogels crosslinked with shortmatrix metalloprotease (MMP)-sensitive peptides and incor-porating synthetic integrin-binding motifs.121,123–126 Othertypesof syntheticgel ECMsbasedentirelyonsyntheticproteinsor semisynthetic gels based on modified hyaluronic acid arealso widely used.124,127 The local and bulk mechanical modu-lus, permeability, degradation properties, and biochemicalrecognition motifs—all of which have been correlated to cellresponses115,121,125—can be tuned independently tomatch theneeds of individual cells and tissues.
Recently, a locally responsive, “one-size-fits-all” PEG-basedmodular synthetic ECM was developed specifically for cocul-ture of human endometrial epithelial and stromal cells, incor-porating synthetic integrin-binding peptides for both celltypes, and synthetic peptides that capture and sequester thedifferent ECM proteins produced by epithelial and stromalcells.92,95,121 A version of this synthetic ECM also supportsexpansion of human endometrial organoids121 and formationof networks by humanmicrovascular endothelial cells,125 thusproviding a foundation for engineering complex 3D cocultures(►Fig. 3b). Thismatrixcanbedissolvedbyamicrobial enzymeto release cells and local cell–cell signaling molecules foranalysis.92,121 A relatively unsolved problem, however, isformulation of culture media compositions that support mul-tiple different cell types. Solution of this problemmay requirefiner specification and validation of “physiological” cell
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.186
phenotypes, particularly for stromal cells which are oftengrown in serum-containing media optimized for maximalcell proliferation rates, rather than specific tissue functions.
Tissue engineering of the myometrium has benefitted ex-tensively from the intense activity in using 3D models toilluminate arterial smoothmuscle pathophysiology and regen-eratebloodvessels,where the roles ofbasementmembrane, 3Darchitecture, celldensity, andbiomechanical stimulationoncelland tissue phenotype have been analyzed.128 Understandingand modulating contractions in the pregnant uterus, to inter-vene therapeutically in preterm birth, has been the majorapplication focus of in vitro 3D myometrial explant and tis-sue-engineered models.36,111–113,129–132 Tissue-engineeredmodels employingmyometrial SMCs embedded in 3D collagengels, adapted from successful models for vascular applications,offer advantages over explants by enabling a reproducible cellsource from a tissue bank to be employed in multiple experi-ments,131 and providing control over which cell types arepresent, to parse contributions of various immune cell pop-ulations, for example. An innovation involving an ECM-freemagnetic cell aggregation112 has been adapted to the myome-trial contraction assays, but approaches involving syntheticECMs are still only nascent for other SMC applications.133
To summarize this section, the essential cell-based founda-tion for creating complex, 3Dmodels ofmyometrial–endome-trial interactions has been established through a combinationof advances in basic methods of cell culture, combined withtechnologies for controlling the ECMmicroenvironment withsynthetic biomaterials (►Fig. 3c). These tools can be furthercombined with microfluidic devices to model pathologicphenotypes in a physiomimetic sense.
Modeling the Dynamic Processes of theAdenomyotic Microenvironment
The fundamental tools for building 3D tissue models are theconstituent cells, scaffolds, matrices, platforms, and solublecues that facilitate reconstruction or morphogenesis ofphysiologically relevant mimics of tissues. These fundamen-tal tools are then deployed in specialized ways to modelspecific dynamic processes and phenotypes. Here, wedescribe the processes illustrated in ►Fig. 2, and drawfrom applications in other disease research areas to illustratehow fundamental tissue engineering tools are often com-bined with other devices to further control elements of theculture microenvironment, such as mechanical stimulation,innervation, or fluid flow.
Invasion and SurvivalWhether adenomyosis initially arises from a true invasion ofthe myometrium from the endometrium or through trans-port of endometrial cells into the myometrium by othermeans is debated, but once present, the displaced endome-trial cells form lesions that grow and invade the surroundingtissue as the lesion enlarges. Cancer, wound healing, immuneresponse to infection, and myriad other pathophysiologicalbehaviors—including endometriosis and adenomyosis—havemotivated a vast array of mechanistic experimental studies
and biophysical models of cell migration and inva-sion.15,122,134–136 Although various authors often inter-change the terms migration and invasion, here we willrefer to migration as a phenomenon of movement along atwo-dimensional (2D) surface (e.g., endothelial cells movingacross a denuded region of a vessel) or a quasi-2D surface(highly porous 3D matrix such as a large-pore transwellmembrane), where no ECM degradation is required formovement. In contrast, we define invasion as a 3D processwhere breakdown ofmatrix or cell–cell junctions is required.
Migrating and invading cells inherently integrate an array ofindividual molecular processes to generate biophysical forcesresulting incellmovement,whichmayberandomor influencedby chemotactic (chemical-based), durotactic (matrix stiffness-based), or haptotactic (adhesion-based) gradients.134,136 Thisintegration can result in nonintuitive outcomes, necessitatingcareful attention to quantitative experimental parameters andmetrics. For example, experimentally, cell migration speedsexhibit maxima for intermediate values of ECM-coating densi-ties, across many different cell types and ECM coatings, aspredicted by a biophysical model describing the balancebetween cell-matrix adhesion forces and cell-generated con-tractile forces.134 Growth factors, which modulate both cell-matrix adhesion and cell contractile force generation, canappear to increase or decrease cell speed for a given ECM-coating density, depending onwhich side of the biphasic curveis operative for the chosen condition.137 3D invasion assaysinherently integrate more complex processes. The diversity intypes of 3D movement, together with cell-mediated matrixdegradation, results in different biophysical phenomena gover-nance compared with that of 2D migration assays.122,138
Although therearenumerousstudies focusingonmigrationand invasion of cells derived from eutopic or ectopic tissue inpatientswith endometriosis,15,139 studies on adenomyosis aremore limited and focused on stromal cells.136,140,141 Consid-eration of how the individual molecular components in theextracellular environment (e.g., adhesion molecules, growthfactors, porosity and stiffness of the matrix, matrix remodel-ing) and intracellular environment (e.g., integrin–cytoskeletallinks, actin–myosin contractile forces, signaling pathwaysgoverning protein–protein associations) are integrated bio-physically provides insight into why literature reports com-paring adenomyotic and healthy cell migration and invasionare conflicting.136 When eutopic endometrial stromal cellsfrom adenomyosis patients and controls were compared in anassay format involvingmigration/invasionof cells across a thinporous membrane coated with Matrigel for 24 hours, nodifferences between the two groups were observed.140 How-ever, when eutopic endometrial stromal cells from patientswith adenomyosis were compared with controls in an assaythat involved invasion for 10days into a1 cm-thick slab of typeI collagengel, adenomyotic cells invaded further than controls;invasion of both control and adenomyotic cells was furtherenhanced when myometrial cells from control donors wereincluded in the gel, and even further enhanced again if thedonormyometrial cells were from an adenomyosis patient.141
Furthermore, this same assay format revealed that estradioland tamoxifen drive additional increases in the invasiondepth
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 187
of cells in each condition, while progesterone blunts theeffects.142 The 24-hour Matrigel invasion assay may not havecaptured differences between control and diseased popula-tions, due to a combination of the relatively short assay time,use of an epithelial basement membrane-type matrix (Matri-gel) rather than a stromal-like matrix (collagen I), and thepotential for themany growth factors in Matrigel to stimulatechemokinesis (randommotility) in a way that drove maximalinvasion and obscured the differences. Still, whether theseendometrial cells would invade a true smooth muscle struc-ture, and if so,whether the factors regulating such invasionarethe same as those regulating migration in ECM, is an interest-ing question for future models to address.
The enduringchallenge, asnotedat theoutsetof this article,is whether new targets for therapeutics are revealed, and if so,whether drugs that treat them (as well as existing drugs) canbe circumscribed to certain groups of patients who might beidentified by accessible clinical tests. Answering these relatedquestions, especially in a manner that captures the multiplephenotypes leading to symptomatic pain and bleeding inadenomyosis, isstill at anearly stageofphysiomimeticanalysisfor any type of therapeutic. With respect to identifying newtargets, a study employing a high-throughput 3D invasionassay for the 12Z endometriotic cell line in collagen gels thatexamined invasion as a function of growth factor/cytokinestimulation, intracellular kinase signaling pathway response,and proteolytic shedding of cell surface receptors and growthfactors15might be considered relevant for adenomyosis, as the12Z line likely shares features with adenomyotic epithelia. Asnotedearlier, experimentswith cell linesoffer insights that canbe followed up with primary cells. In the study, a Bayesiananalysis linking the recursive protease-growth factor-kinasesignaling loops revealed potential vulnerabilities in the net-work involving, among others, JUN kinase (JNK), and thisprediction was experimentally verified with inhibitors.15 In-terestingly, a JNK inhibitor was also identified as a driver ofinflammation in a separatestudyofperitonealfluid inpatientswith surgically verified endometriosis, where a subset ofpatients exhibited a constellation of signature cytokines.14
Two preclinical studies indicated effectiveness of a JNK inhibi-tor against endometriosis,143,144 yet a clinical study in a non-stratified patient population (NCT01630252, NCT01631981)failed tomeet endpoints. (None of the patients in either studywere evaluated for possible adenomyosis, which is oftencomorbid with endometriosis and may contribute to symp-toms andwhichmay also respond to therapies for endometri-osis.) Further exploration of this hypothesis with the types ofmodels now being developed that include multicellular com-partments and robust metrics may provide insights into howto design a clinical trial to treat subsets of patientswith certaincharacteristics.
Adenomyosis invasion phenocopies features of carcino-ma invasion into smooth muscle. Although the overwhelm-ing majority of in vitro invasion studies have investigatedinvasion into ECM-rich tissues, the conceptual frameworkfor building 3D invasion models in muscle has been mappedout over the past decade by observations in clinical speci-mens and intravital microscopy of carcinoma invasion in
muscle in mouse models.135 Epithelial invasion into muscleis associated with changes in multiple facets of cell cyto-skeletal and mechanosensing behaviors, driving a prefer-ence for stiff environments.135 Cells can invade into muscleas individual cells, or as chains, clusters, or collectivestrands, following the collagenous matrix between bundlesor migrating along individual SMCs.135 Features of collec-tive cell invasion have been observed in deep infiltratingendometriosis lesions in the rectocervical space,55 suggest-ing the possible invasion from adenomyotic lesions ema-nating from the cervical region of the uterus. The role of theregular smooth muscle contractions in the invasion processis still speculative, as there are consequences for mechanicaldamage, as well as promoting mitosis.135 Hence, the devel-opment of models that experimentally recapitulate thesemultiple features is the goal of adenomyosis physiomimeticmodeling.
Vascularization and Immune InteractionsWith a vision toward building an adenomyosis lesion modelthat incorporates large-scale features of the lesion microenvi-ronment, including a vascular bed, creation of amicrovascularnetworkbecomes essential for survival andhomeostasis of theengineered tissue. First, the microvascular system in theuterus, as in other organs, is essential for providing oxygenand nutrients. The dimensions of 3D in vitro models areinherently limited by diffusion of oxygen and nutrients toapproximately 0.2mm formetabolically active tissue like liverand muscle, and slightly larger for relatively acellular connec-tive tissues such as dermis.115 Second, the microvascularbarrier also regulates trafficking of immune cells (andpossiblycirculating stem cells) and plays essential roles in tissuehomeostasis through paracrine signaling to tissues, servingas the nidus for commencing decidualization of the endome-trium.145Vascular function ismodulated by systemic and locallevels of sex hormones and inflammatory cues.146,147 In vitro,cultures of endometrial stromal and epithelial cells in thepresence of estrogen regulate angiogenesis,148 and signalsfrom flow-activated endothelial cells enhance hormone re-sponse in endometrial stromal cells.145
Encouragingly, a fusion of tissue engineering and micro-fluidic cell culture technologies has spurred development ofdevices and protocols that could be applied to modelingadenomyosis lesions. Microfluidic devices with planar cul-tures that probe endothelial–stromal–immune interactionshave already been applied to study the role of environmentalchemicals on facets of endometriosis phenotypes.149 Micro-fluidic and mesofluidic devices incorporating 3D tissue struc-tures that can be perfused continuously with culture media,imaged, and sampled in situ are endemic tools in the emergingfield of “microphysiological systems (MPSs)”—in vitro repre-sentations of complex physiological phenomena involvingmultiple cell types and dynamic behaviors in 3D. A crucialfirst step was to define protocols for the creation of stable,perfusable microvascular networks in a collagen or fibrin gelsituated between two channels perfused with cell culturemedia (►Fig. 4a).150–152 Stable microvessels from endothelialcells andfibroblasts seeded in the centralgel region (►Fig. 4b),
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.188
enabling phenomena involving trafficking of immune(►Fig. 4c) and tumor cells across the endothelial barrier tobe observed in detail (►Fig. 4d).153 These foundationalapproaches have now been widely adapted to support appli-cations as diverse as in vitro tumor and islet microvasculari-zation and formation of functional blood–brainbarriers.154–157 These studies establish principles for how amicrovascularized endometrial–stromal lesion could bemod-eled; indeed, the authors are currently leveraging them tobuild multicellular microvascularized models of endometri-osis lesions, employing primary patient-derived endometrialepithelial, stromal, and immune cells for analysis of howmicrovascular permeability and immune cell recruitmentare regulated as a function of circulating sex steroids. Amodelof vascularized muscle developed for analyzing fibrosis andmuscle damage158 could potentially be adapted for creating amodel of vascularized adenomyosis in the host tissue. Onesignificant technical challenge relevant for modeling repro-ductive tissues is that the material most commonly used forfabricating microfluidic devices, polydimethylsiloxane(PDMS), absorbs lipophilic compounds like estrogen and pro-gesterone, making it almost impossible to control their con-centrations and thus tissue exposure.159 Among fabricationmaterials, PDMS is uniquely permeable to oxygen—a limitingnutrient inmost cultures; hence, significant design changes toprovide oxygenation are required in transitioning to moresuitable materials, but these shifts are gradually occurring ascommercial chips based on thermoplastics are coming intouse.160
Biomechanical StimulationIt isnowwell recognized that themechanical complianceof theECMmicroenvironment—“stiffness” or “softness”—dramatical-ly influences the phenotypes of epithelial cells, stem cells, and
other cell types.161 Matrices that are relatively stiff comparedwith the normal mechanical properties that a cell experiencescan drive transition of fibroblasts to myofibroblasts and epi-thelial cells to a tumor-like phenotype.161 Similarly, tumor cellsaccustomed to a stiff environment may exhibit poor survivaland growth when placed into a more normal mechanicalenvironment—a factor that may contribute to the difficulty ingrowing cells from endometriosis and adenomyosis lesions.These adaptations occur through a compendiumofmechanicalsignaling pathways that are integrated in part by the intracel-lular translocation of transcriptional regulators YAP and TAZ tothe nucleus, allowing differences in mechanical signaling be-tween two different tissue environments in vivo to be inferredfrom immunohistochemistry.162 An elegant in vivo–in vitromechanical signaling study involving the myometrium firstdemonstrated links between the mechanical properties ofuterine leiomyomas (fibroids) relative to surrounding myome-trium and the corresponding relative amounts of nuclear YAP/TAZ (via immunohistochemistry), and then showed that isolat-ed myometrial SMCs or fibroid cells cultured in 2D on a set ofsynthetic hydrogel substrates with systematically varied me-chanical stiffness recapitulated the trends in nuclear YAP/TAZseen for each cell type in vivo, along with enhanced ECMdeposition by fibroid cells as seen in vivo.162 This in vivo–invitro correspondence suggests that the in vitromodelmay be auseful proxy for analyzing potential therapeutic interventionsinto mechanical signaling pathways. Other behaviors, such asinvasion/survival, may require a 3D environment to capturethese invivobehaviors. Toward thisgoal,wehave observed thatnormal human endometrial epithelial cells, which exhibit aprototypical spherical organoid morphology when cultured insoft synthetic hydrogels,121 adopt a lesion-like morphologywith invasive protrusions and epithelial-mesenchymal transi-tion (EMT)-like cellular morphology when cultured in stiff
Fig. 4 Microfluidic model of immune and tumor cell trafficking between the microvasculature and tissues. (a) A microfluidic devicecomprising a central tissue-containing channel, flanked by two channels for flow of culture medium, is inoculated with a mixture of fibrincontaining endothelial and stromal cells. Over the initial few days, cells undergo morphogenesis to form perfusable microvascular networkswhich are stable for weeks in culture as shown in (b) for a day 23 culture (actin stain). (c) Immune cells (green) can be perfused through themicrovasculature (red) to model peripheral cell recruitment. (d) The dynamic cell-level phenomena in the devices can be imagined by confocal ortwo-photon microscopy to observe phenomena such as neutrophil–tumor cell interactions in the extravasation of tumor cells through thevascular wall into tissue. (Images from Zhang et al,110 permission is in progress.)
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 189
synthetic hydrogels (Gnecco et al, unpublished data Aug, 15,2020; ►Fig. 3c). These type of reductionist models may helpparse the relative contributions of inflammatory cues, hor-mones,andothermicroenvironment factors reported inadeno-myosis lesions. However, the myometrium is not just a staticmicroenvironment. The nonpregnant myometrium undergoesconstant contractions tomove fluid, inways that are disruptedin adenomyosis.35,36 The propensity of endometrial cells toform endometriosis lesions in smooth muscle of the intestinaltract and adenomyosis lesions in the myometrium, and tosimilarly be associated with hyperplastic smooth muscle (ormyofibroblasts) in other ectopic contexts such as the bladder,ureter, rectocervical space, and relatively absent from themesentery and omentum, suggests an interesting tropism formicroenvironments that may offer mechanical stimulation.
Although the ability of drugs and hormones to altercontractile phenotype of myometrial cells has been usedas a screen in explant and 3D culture assays,81,113,129 and tocompare general contractile abilities of normal andadenomyotic myometrium,36 extension to more complexquestions of etiology and interaction with endometriumunder dynamic conditions is only nascent. Dynamic me-chanical stimulation of human uterine cells in 2D hasshown that endometrial stromal cells can acquire a con-tractile phenotype163 and that human myometrial cellsexhibit dramatic shifts in the phosphoproteome understretch.164 A study designed to illuminate the possibleeffects of myometrial contractions on endometrial pheno-type used a novel microfluidic reactor to coculture anendometrial cell line on a layer of myometrial cells, in amanner that exposed the coculture to dynamic peristalsisthat generated shear flow in the fluid impinging on theendometrial epithelial cell layer.165 This proof-of-principlestudy performed with cell lines showed morphologicalchanges in the epithelial barrier in response to the mechan-ical forces,165 and provides a foundation for next-generationexperiments with primary cells and a more complex tissuearchitecture, building on the well-developed observationsabout tissue engineering of vascular smooth muscle underpulsatile mechanical stimulation.166
InnervationIn addition to the well-known animal dorsal root gangliasources of neurons, the efficient derivation of geneticallydiverse peripheral sensory neurons from human cells hasprovided novel avenues for investigating and culturing hu-man nerve fibers in vitro167,168 and for building models forneuromotor action and pain.167 While models of the endo-metrium have not yet been explored, microfluidic models ofenteric nerve–epithelial interactions in the intestine areexemplary of the approaches.169 Similarly, a microfluidicmodel of neuronal activation of vascularized skeletal musclecontraction, which allows quantitative analysis of axonalgrowth, muscle maturations, and contraction, provides atemplate for design of a similar device for the myome-trium.170 Ultimately, these tools might be combined to buildmodels of innervated, vascularized adenomyosis lesions,
using patient-specific samples to understand the manifesta-tion of debilitating menorrhea.
Systemic and Organ–Organ interactionsFinally, adenomyosis and other chronic inflammatory diseasesboth exert and respond to systemic effects, potentially includ-ing those emanating from the gut microbiome. A growingnumber of microfluidic and mesofluidic models are beingdeveloped to connect MPSs representing multiple differentorgan systems (e.g., gut, liver, heart, brain) in a continuouslycommunicating fluidic network for extended (weeks) cultureperiods, using fabricationmaterials that avoid the problems ofPDMS.171–173 A new pumping technology driven by integrat-ingmicrofluidic pumps that are safe for immune cells onto theplatform has been applied to examine the interplay betweentissue-resident cells in the gut and liver and circulating im-mune cells in response to short-chain fatty acid metabolitesproduced in the colon, revealing paradoxical responses.173
Such technologies might be used in the future to examinechronic cell trafficking between the vasculature and lesions ina single-MPSmodel of adenomyosis as a function of hormonecycles, or, more ambitiously, the interplay between the bonemarrow–adenomyosis lesion axis with respect to circulatingcells and factors, given the interplay between bone marrow–derived cells and wound healing/lesion phenomena.174
Data-Driven Analysis and PredictiveModeling of Human Responses
A premise of the physiomimetics approach (►Fig. 1) is thatpatients can first be stratified on the basis of a combination ofclinical phenotypes andmolecular network analysis, to gener-ate hypotheses formechanistically distinguishable subgroups.In vitro tissue-engineeredmodels of these subgroups can thenbe constructed using well-characterized patient-derivedspecimens and perturbed. Finally, multi-omic measurementscombinedwith phenotypicmetrics can be interpreted to driveidentification and validation of therapies for patient sub-groups, thusprovidinga foundation for stratified clinical trials.Molecular stratification of endometrium-derived diseases isstill in early stages. A meta-analysis of genome-wide associa-tion studies for endometriosis showed stronger reproducibili-ty across eight of nine disease-associated loci for patientswithStage III/IV disease comparedwith Stage I,175 suggesting theremay be clues to processes that amplify lesion characteristics.However, the loci implicate genes widely expressed through-out thebody; thus, one could reasonably construct hypothesesaround gut permeability influencing systemic immune func-tion, for example, as apossible contributingmechanism.Whilesystems-level physiomimetic modeling of complex systemicimmunereactions involving gutpermeabilityareemerging,173
these are not the most likely place to begin to parse adeno-myosis. Similarly, transcriptomic changes in endometrial bi-opsies are more pronounced in severe versus mildendometriosis,176 suggesting several possible pathways forintervention. However, without othermeasurements of lesiontissue context and associated symptom characteristics, these
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.190
datasets provide incomplete directions on designing physio-mimetic models to test mechanisms.
These types of analyses might be paired, though, withphenotypic assays representing dynamic lesion properties.For example, the fine-grained in vitro analysis of pancreatictumor organoid invasion characteristics, used for parsingmechanistic relationships between pancreatic cancer muta-tion subtypes and survival,177 might provide phenotypic dis-crimination among patient subgroups, which could in turnlead to additionalmolecular phenotypingbasedonhypothesesregarding mechanisms governing the phenotypes. Even theassay used for the pancreatic tumors, however, revealedparadoxical relationships with survival177—suggesting an as-say incorporating more complex tumor–stroma interactionscould bemore revealing. A piece of a physiomimetic puzzle forendometriosis, involving a bioinformatics prediction that JNKwould govern cytokine release from peritoneal macrophages,whichwas thenconfirmed invitrowithpatient samples,14mayalso have implications for adenomyosis, as macrophages arealso involved. A physiomimetic model incorporating patientmacrophages along with lesions may reveal disease-relatedphenotypic characteristics that could bemodulatedwith a JNKinhibitor. At a systems level, the effects of potential newtherapeutics can also be assessed using multi-MPS systemsincluding liver and the immune system, incorporating featuresof liver metabolism and other metabolic and systemic trans-formations, using multi-omics to parse complex systemresponses.172,173 These technologies are developing quicklyandmay greatly enhance physiomimeticmodeling of gynecol-ogy diseases in general once resources to clinically phenotypepatients and build corresponding tissue banks are identified.
Conclusions and Future Directions
The enormous spectrum of symptoms, histological/morpho-logical appearances, and associated comorbidities that occurin patients with adenomyosis suggest that there may bedistinct subsets of patients who could be targeted withpersonalized therapies—if the rules for defining these patientpopulations and approaches for developing the targetedtherapies are established and implemented in an integratedfashion. The complexity of adenomyosis requires a physio-mimetic approach: parsing the phenomena that may con-tribute using computational modeling approaches and thenbuilding a physiological model that provides informationthat translates back into the clinic. The fundamental in vitrotissue engineering approaches necessary to create physio-mimetic models have largely been established: methods toconceptually and computationally characterize the diseaseto generate hypotheses about patient stratificationapproaches; methods to create tissue banks of relevant celltypes derived from carefully phenotyped patients; 3D syn-thetic matrices to engineer microenvironments in a repro-ducible way; microfluidic platforms to control vascular andnerve interactions with 3D tissues; and analytical outputsusing functional and molecular assays. The future of model-ing adenomyosis lesion complexity arguably depends onhow well these tools become democratized, whether large
enough patient populations can be pooled to define thebedside-to-bench-to-bedside paradigm of physiomimeticmodeling, and whether standardized methods can be de-fined and implemented for access to patient myometrial/adenomyotic tissue in younger patients who undergo fertili-ty-sparing procedures. We are optimistic that the roadmapdescribed here will spur multidisciplinary teams to hastendevelopment and implementation of better treatments forpatients.
FundingNational Institutes of Health http://dx.doi.org/10.13039/100000002 EB029132 National Science Foundationhttp://dx.doi.org/10.13039/100000001
Conflict of InterestNone declared.
AcknowledgmentsWe thank Hilary Critchley, Stacey Missmer, and DougLauffenburger for critical reading of the manuscript.This work was supported by the John and Karine BeggFoundation, the Manton Foundation, the National ScienceFoundation, and NIH U01 EB029132.
References1 Lopes-Pacheco M. CFTR modulators: the changing face of cystic
fibrosis in the era of precision medicine. Front Pharmacol 2020;10:1662
2 Benagiano G, HabibaM, Brosens I. The pathophysiology of uterineadenomyosis: an update. Fertil Steril 2012;98(03):572–579
3 Chapron C, Tosti C, Marcellin L, et al. Relationship betweenthe magnetic resonance imaging appearance of adenomyosisand endometriosis phenotypes. Hum Reprod 2017;32(07):1393–1401
4 García-Solares J, Donnez J, Donnez O, Dolmans MM. Pathogene-sis of uterine adenomyosis: invagination or metaplasia? FertilSteril 2018;109(03):371–379
5 Habiba M, Gordts S, Bazot M, Brosens I, Benagiano G. Exploringthe challenges for a new classification of adenomyosis. ReprodBiomed Online 2020;40(04):569–581
6 Munro MG, Critchley HO, Broder MS, Fraser ISFIGO WorkingGroup on Menstrual Disorders. FIGO classification system(PALM-COEIN) for causes of abnormal uterine bleeding in non-gravid women of reproductive age. Int J Gynaecol Obstet 2011;113(01):3–13
7 Tellum T, Qvigstad E, Skovholt EK, Lieng M. In vivo adenomyosistissue sampling using a transvaginal ultrasound-guided corebiopsy technique for research purposes: safety, feasibility, andeffectiveness. J Minim Invasive Gynecol 2019;26(07):1357–1362
8 ZondervanKT, Becker CM, Koga K,Missmer SA, Taylor RN, ViganòP. Endometriosis. Nat Rev Dis Primers 2018;4(01):9
9 Koninckx PR, Ussia A, Adamyan L,Wattiez A, GomelV,Martin DC.Heterogeneity of endometriosis lesions requires individualisa-tion of diagnosis and treatment and a different approach toresearch and evidence based medicine. Facts Views Vis ObGyn2019;11(01):57–61
10 OsugaY, Fujimoto-OkabeH,HaginoA.Evaluationof theefficacyandsafetyofdienogest in thetreatmentofpainful symptoms inpatientswith adenomyosis: a randomized, double-blind, multicenter, pla-cebo-controlled study. Fertil Steril 2017;108(04):673–678
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 191
11 Vannuccini S, Tosti C, Carmona F, et al. Pathogenesis of adeno-myosis: an update on molecular mechanisms. Reprod BiomedOnline 2017;35(05):592–601
12 Inoue S, Hirota Y, Ueno T, et al. Uterine adenomyosis is anoligoclonal disorder associated with KRAS mutations. Nat Com-mun 2019;10(01):5785
13 Shaked S, Jaffa AJ, Grisaru D, Elad D. Uterine peristalsis-inducedstresses within the uterine wall may sprout adenomyosis. Bio-mech Model Mechanobiol 2015;14(03):437–444
14 Beste MT, Pfäffle-Doyle N, Prentice EA, et al. Molecular networkanalysis of endometriosis reveals a role for c-Jun-regulatedmacrophage activation. Sci Transl Med 2014;6(222):222ra16
15 Miller MA, Meyer AS, Beste MT, et al. ADAM-10 and -17 regulateendometriotic cell migration via concerted ligand and receptorshedding feedback on kinase signaling. Proc Natl Acad Sci U S A2013;110(22):E2074–E2083
16 Shafrir AL, Missmer SA. Towards subtypes - deep endometriosisoestrogen receptor-α expression. Nat Rev Endocrinol 2020;16(10):541–542
17 Zondervan KT, Rahmioglu N, Morris AP, et al. Beyond endome-triosis genome-wide association study: from genomics to phe-nomics to the patient. Semin Reprod Med 2016;34(04):242–254
18 Conklin JE, Lieberman JV, Barnes CA, Louis DZ. Disease staging:implications for hospital reimbursement and management.Health Care Financ Rev 1984;1984:13–22
19 Gonnella JS, Hornbrook MC, Louis DZ. Staging of disease. A case-mix measurement. JAMA 1984;251(05):637–644
20 Gonella J, Louis DZ, Guozum MVE, Callahan CA, Barnes CA.Disease staging. In: Gonella J, ed. Disease Staging. MI: AnnArbor; 2001:927
21 Munro MG, Critchley HOD, Fraser ISFIGO Menstrual DisordersCommittee. The twoFIGOsystems for normal andabnormaluterinebleeding symptoms and classification ofcauses ofabnormal uterinebleeding in the reproductive years: 2018 revisions. Int J GynaecolObstet 2018;143(03):393–408
22 Driehuis E, van Hoeck A, Moore K, et al. Pancreatic cancerorganoids recapitulate disease and allow personalized drugscreening. Proc Natl Acad Sci U S A 2019;116(52):26580–26590
23 Vitonis AF, Vincent K, Rahmioglu NWERF EPHect WorkingGroup, et al; World Endometriosis Research Foundation Endo-metriosis Phenome and Biobanking Harmonization Project: II.Clinical and covariate phenotype data collection in endometri-osis research. Fertil Steril 2014;102(05):1223–1232
24 Rahmioglu N, Fassbender A, Vitonis AFWERF EPHect WorkingGroup, et al; World Endometriosis Research Foundation Endo-metriosis Phenome and Biobanking Harmonization Project: III.Fluid biospecimen collection, processing, and storage in endo-metriosis research. Fertil Steril 2014;102(05):1233–1243
25 Pugliese A, Yang M, Kusmarteva I, et al. The Juvenile DiabetesResearch Foundation Network for Pancreatic Organ Donors withDiabetes (nPOD) program: goals, operational model and emerg-ing findings. Pediatr Diabetes 2014;15(01):1–9
26 Gordts S, Campo R, Brosens I. Hysteroscopic diagnosis andexcision of myometrial cystic adenomyosis. Gynecol Surg2014;11(04):273–278
27 Critchley HO, Jones RL, Lea RG, et al. Role of inflammatorymediators in human endometrium during progesterone with-drawal and early pregnancy. J Clin Endocrinol Metab 1999;84(01):240–248
28 Critchley HOD, Maybin JA, Armstrong GM, Williams ARW.Physiology of the endometrium and regulation of menstruation.Physiol Rev 2020;100(03):1149–1179
29 Vigano P, Candiani M, Monno A, Giacomini E, Vercellini P,Somigliana E. Time to redefine endometriosis including itspro-fibrotic nature. Hum Reprod 2018;33(03):347–352
30 Thiruchelvam U, Dransfield I, Saunders PT, Critchley HO. Theimportance of themacrophagewithin the human endometrium.J Leukoc Biol 2013;93(02):217–225
31 Osteen KG, Rodgers WH, Gaire M, Hargrove JT, Gorstein F,Matrisian LM. Stromal-epithelial interaction mediates steroi-dal regulation of metalloproteinase expression in humanendometrium. Proc Natl Acad Sci U S A 1994;91(21):10129–10133
32 Henderson TA, Saunders PT, Moffett-King A, Groome NP, Critch-ley HO. Steroid receptor expression in uterine natural killer cells.J Clin Endocrinol Metab 2003;88(01):440–449
33 Myers KM, Elad D. Biomechanics of the human uterus. WileyInterdiscip Rev Syst Biol Med 2017;9(05):
34 Aguilar HN, Mitchell BF. Physiological pathways and molecularmechanisms regulating uterine contractility. Hum Reprod Up-date 2010;16(06):725–744
35 Mehasseb MK, Bell SC, Pringle JH, Habiba MA. Uterine adeno-myosis is associated with ultrastructural features of alteredcontractility in the inner myometrium. Fertil Steril 2010;93(07):2130–2136
36 Guo SW, Mao X, Ma Q, Liu X. Dysmenorrhea and its severity areassociated with increased uterine contractility and overexpres-sion of oxytocin receptor (OTR) in women with symptomaticadenomyosis. Fertil Steril 2013;99(01):231–240
37 Brosens JJ, Barker FG, de Souza NM. Myometrial zonal differen-tiation and uterine junctional zone hyperplasia in the non-pregnant uterus. Hum Reprod Update 1998;4(05):496–502
38 Benagiano G, Brosens I, Habiba M. Structural and molecularfeatures of the endomyometrium in endometriosis and adeno-myosis. Hum Reprod Update 2014;20(03):386–402
39 Strauss JF, Lessey BA, eds. The structure, function, and evaluationof the female reproductive tract. . In: Yen & Jaffe’s ReproductiveEndocrinology, Elsevier, NY. 2009:191–233
40 Leyendecker G, Wildt L. A new concept of endometriosis andadenomyosis: tissue injury and repair (TIAR). HormMol Biol ClinInvestig 2011;5(02):125–142
41 IbrahimMG, Chiantera V, Frangini S, et al. Ultramicro-trauma inthe endometrial-myometrial junctional zone and pale cellmigration in adenomyosis. Fertil Steril 2015;104(06):1475–83.e1, 3
42 Zhang Q, Duan J, Liu X, Guo SW. Platelets drive smooth musclemetaplasia and fibrogenesis in endometriosis through epitheli-al-mesenchymal transition and fibroblast-to-myofibroblasttransdifferentiation. Mol Cell Endocrinol 2016;428:1–16
43 Kobayashi H, Kishi Y, Matsubara S. Mechanisms underlyingadenomyosis-related fibrogenesis. Gynecol Obstet Invest 2020;85(01):1–12
44 Li T, Li YG, Pu DM. Matrix metalloproteinase-2 and -9 expressioncorrelated with angiogenesis in human adenomyosis. GynecolObstet Invest 2006;62(04):229–235
45 Guo SW. Fibrogenesis resulting from cyclic bleeding: the HolyGrail of the natural historyof ectopic endometrium. HumReprod2018;33(03):353–356
46 Li H, Yu Y, Shi Y, et al. HoxA13 stimulates myometrial cells tosecrete IL-1β and enhance the expression of contraction-associ-ated proteins. Endocrinology 2016;157(05):2129–2139
47 Mehasseb MK, Panchal R, Taylor AH, Brown L, Bell SC, Habiba M.Estrogen and progesterone receptor isoform distributionthrough the menstrual cycle in uteri with and without adeno-myosis. Fertil Steril 2011;95(07):2228–2235, 2235.e1
48 Jichan Nie, Xishi Liu, Guo SW. Promoter hypermethylation ofprogesterone receptor isoform B (PR-B) in adenomyosis and itsrectification by a histone deacetylase inhibitor and a demethyl-ation agent. Reprod Sci 2010;17(11):995–1005
49 Scheerer C, Frangini S, Chiantera V, Mechsner S. Reduced sym-pathetic innervation in endometriosis is associated to Sema-phorin 3C and 3F expression. Mol Neurobiol 2017;54(07):5131–5141
50 Wang G, Tokushige N, Fraser IS. Nervefibers andmenstrual cyclein peritoneal endometriosis. Fertil Steril 2011;95(08):2772–2774
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al.192
51 Al-Jefout M, Dezarnaulds G, Cooper M, et al. Diagnosis ofendometriosis by detection of nerve fibres in an endometrialbiopsy: a double blind study. Hum Reprod 2009;24(12):3019–3024
52 Browne AS, Yu J, Huang RP, Francisco AM, Sidell N, Taylor RN.Proteomic identification of neurotrophins in the eutopic endo-metrium of women with endometriosis. Fertil Steril 2012;98(03):713–719
53 Anaf V, Simon P, El Nakadi I, et al. Relationship between endo-metriotic foci and nerves in rectovaginal endometriotic nodules.Hum Reprod 2000;15(08):1744–1750
54 Mechsner S, Kaiser A, Kopf A, Gericke C, Ebert A, Bartley J. A pilotstudy to evaluate the clinical relevance of endometriosis-associ-ated nervefibers in peritoneal endometriotic lesions. Fertil Steril2009;92(06):1856–1861
55 García-Solares J, Dolmans MM, Squifflet JL, Donnez J, Donnez O.Invasion of human deep nodular endometriotic lesions is asso-ciated with collective cell migration and nerve development.Fertil Steril 2018;110(07):1318–1327
56 Tran LV, Tokushige N, Berbic M, Markham R, Fraser IS. Macro-phages and nerve fibres in peritoneal endometriosis. HumReprod 2009;24(04):835–841
57 Greaves E, Temp J, Esnal-Zufiurre A, Mechsner S, Horne AW,Saunders PT. Estradiol is a critical mediator of macrophage-nerve cross talk in peritoneal endometriosis. Am J Pathol 2015;185(08):2286–2297
58 Zhang X, Lu B, Huang X, Xu H, Zhou C, Lin J. Innervation ofendometrium and myometrium in women with painful adeno-myosis and uterine fibroids. Fertil Steril 2010;94(02):730–737
59 Vacca P, Vitale C, Montaldo E, et al. CD34þ hematopoieticprecursors are present in human decidua and differentiateinto natural killer cells upon interaction with stromal cells.Proc Natl Acad Sci U S A 2011;108(06):2402–2407
60 Armstrong GM, Maybin JA, Murray AA, et al. Endometrialapoptosis and neutrophil infiltration during menstruationexhibits spatial and temporal dynamics that are recapitulatedin a mouse model. Sci Rep 2017;7(01):17416
61 Russell P, Anderson L, Lieberman D, et al. The distribution ofimmune cells and macrophages in the endometrium of womenwith recurrent reproductive failure I: Techniques. J ReprodImmunol 2011;91(1-2):90–102
62 Bulmer JN, Jones RK, Searle RF. Intraepithelial leukocytes inendometriosis and adenomyosis: comparison of eutopic andectopic endometrium with normal endometrium. Hum Reprod1998;13(1O):2910–2915
63 OrazovMR, Radzinsky VE, Nosenko EN, KhamoshinaMB, DukhinAO, Lebedeva MG. Immune-inflammatory predictors of thepelvic pain syndrome associated with adenomyosis. GynecolEndocrinol 2017;33(Suppl 1):44–46
64 He H, Mack JJ, Güç E, et al. Perivascular macrophages limitpermeability. Arterioscler Thromb Vasc Biol 2016;36(11):2203–2212
65 Schindl M, Birner P, Obermair A, Kiesel L, Wenzl R. Increasedmicrovessel density in adenomyosis uteri. Fertil Steril 2001;75(01):131–135
66 Liu X, ShenM, Qi Q, ZhangH, Guo SW. Corroborating evidence forplatelet-induced epithelial-mesenchymal transition and fibro-blast-to-myofibroblast transdifferentiation in the developmentof adenomyosis. Hum Reprod 2016;31(04):734–749
67 Harmsen MJ, Wong CFC, Mijatovic V, et al. Role of angiogenesis inadenomyosis-associated abnormal uterine bleeding and subfertil-ity: a systematic review.HumReprodUpdate2019;25(05):647–671
68 Ota H, Igarashi S, Hatazawa J, Tanaka T. Is adenomyosis animmune disease? Hum Reprod Update 1998;4(04):360–367
69 De Leo B, Esnal-Zufiaurre A, Collins F, Critchley HOD, SaundersPTK. Immunoprofiling of human uterine mast cells identifiesthree phenotypes and expression of ERβ and glucocorticoidreceptor. F1000 Res 2017;6:667
70 Benagiano G, Brosens I. The endometrium in adenomyosis.Womens Health (Lond) 2012;8(03):301–312
71 Tremellen KP, Russell P. The distribution of immune cells andmacrophages in the endometrium of women with recurrentreproductive failure. II: adenomyosis andmacrophages. J ReprodImmunol 2012;93(01):58–63
72 Ota H, Tanaka T. Stromal vascularization in the endometriumduring adenomyosis. Microsc Res Tech 2003;60(04):445–449
73 Ota H, Igarashi S, Hatazawa J, Tanaka T. Immunohistochemicalassessment of superoxide dismutase expression in the endome-trium in endometriosis and adenomyosis. Fertil Steril 1999;72(01):129–134
74 Herndon CN, Aghajanova L, Balayan S, et al. Global transcriptomeabnormalities of the eutopic endometrium from women withadenomyosis. Reprod Sci 2016;23(10):1289–1303
75 Acar S, Millar E, Mitkova M, Mitkov V. Value of ultrasound shearwave elastography in the diagnosis of adenomyosis. Ultrasound2016;24(04):205–213
76 Al-Sabbagh M, Lam EW, Brosens JJ. Mechanisms of endometrialprogesterone resistance. Mol Cell Endocrinol 2012;358(02):208–215
77 Hellweg G, Shaka JA. Endometrial granulocytes; tissue culturestudies of endometrium and decidua with special attention tothe endometrial granulocytes. Obstet Gynecol 1959;13(05):519–529
78 Kawaguchi K, Fujii S, Konishi I, Okamura H, Mori T. Ultrastruc-tural study of cultured smooth muscle cells from uterine leio-myoma and myometrium under the influence of sex steroids.Gynecol Oncol 1985;21(01):32–41
79 Gellersen B, Bonhoff A, Hunt N, Bohnet HG. Decidual-typeprolactin expression by the humanmyometrium. Endocrinology1991;129(01):158–168
80 Heidari Kani MH, Chan E-C, Young RC, Butler T, Smith R, Paul JW.3D cell culturing and possibilities for myometrial tissue engi-neering. Ann Biomed Eng 2017;45(07):1746–1757
81 Arrowsmith S, Keov P, Muttenthaler M, Gruber CW. Contractilitymeasurements of human uterine smooth muscle to aid drugdevelopment. J Vis Exp 2018;(131):56639
82 Gaide Chevronnay HP, Lemoine P, Courtoy PJ, Marbaix E, HenrietP. Ovarian steroids, mitogen-activated protein kinases, and/oraspartic proteinases cooperate to control endometrial remodel-ing by regulating gene expression in the stroma and glands.Endocrinology 2010;151(09):4515–4526
83 Schäfer WR, Fischer L, Roth K, et al. Critical evaluation of humanendometrial explants as an ex vivo model system: a molecularapproach. Mol Hum Reprod 2011;17(04):255–265
84 Fasciani A, Bocci G, Xu J, et al. Three-dimensional in vitro cultureof endometrial explants mimics the early stages of endometri-osis. Fertil Steril 2003;80(05):1137–1143
85 Osteen KG, Hill GA, Hargrove JT, Gorstein F. Development of amethod to isolate and culture highly purified populations ofstromal and epithelial cells from human endometrial biopsyspecimens. Fertil Steril 1989;52(06):965–972
86 Korch C, SpillmanMA, Jackson TA, et al. DNA profiling analysis ofendometrial and ovarian cell lines reveals misidentification,redundancy and contamination. Gynecol Oncol 2012;127(01):241–248
87 Banu SK, Lee J, Starzinski-Powitz A, Arosh JA. Gene expressionprofiles and functional characterization of human immortalizedendometriotic epithelial and stromal cells. Fertil Steril 2008;90(04):972–987
88 Samalecos A, Reimann K,Wittmann S, et al. Characterization of anovel telomerase-immortalized human endometrial stromal cellline, St-T1b. Reprod Biol Endocrinol 2009;7:76
89 Krikun G, Mor G, Alvero A, et al. A novel immortalized humanendometrial stromal cell line with normal progestational re-sponse. Endocrinology 2004;145(05):2291–2296
Seminars in Reproductive Medicine Vol. 38 No. 2-3/2020
Physiomimetic Models of Adenomyosis Gnecco et al. 193
90 Wu J, Taylor RN, Sidell N. Retinoic acid regulates gap junctionintercellular communication in human endometrial stromalcells through modulation of the phosphorylation status ofconnexin 43. J Cell Physiol 2013;228(04):903–910
91 Schutte SC, James CO, Sidell N, Taylor RN. Tissue-engineeredendometrial model for the study of cell-cell interactions. ReprodSci 2015;22(03):308–315
92 Valdez J, Cook CD, Ahrens CC, et al. On-demand dissolution ofmodular, synthetic extracellular matrix reveals local epithelial-stromal communication networks. Biomaterials 2017;130:90–103
93 Arnold JT, Lessey BA, Seppälä M, Kaufman DG. Effect of normalendometrial stroma on growth and differentiation in Ishikawaendometrial adenocarcinoma cells. Cancer Res 2002;62(01):79–88
94 Zeitvogel A, Baumann R, Starzinski-Powitz A. Identification of aninvasive, N-cadherin-expressing epithelial cell type in endome-triosis using a newcell culturemodel. Am J Pathol 2001;159(05):1839–1852
95 Cook CD, Hill AS, Guo M, et al. Local remodeling of syntheticextracellular matrix microenvironments by co-cultured endo-metrial epithelial and stromal cells enables long-term dynamicphysiological function. Integr Biol 2017;9(04):271–289
96 Barragan F, Irwin JC, Balayan S, et al. Human endometrial fibro-blasts derived from mesenchymal progenitors inherit progester-one resistance and acquire an inflammatory phenotype in theendometrial niche in endometriosis. Biol Reprod 2016;94(05):118
97 von Wolff M, Stieger S, Lumpp K, Bücking J, Strowitzki T, ThalerCJ. Endometrial interleukin-6 in vitro is not regulated directly byfemale steroid hormones, but by pro-inflammatory cytokinesand hypoxia. Mol Hum Reprod 2002;8(12):1096–1102
98 Chen JC, Hoffman JR, Arora R, et al. Cryopreservation and recoveryof human endometrial epithelial cells with high viability, purity,and functional fidelity. Fertil Steril 2016;105(02):501–10.e1
99 Turco MY, Gardner L, Hughes J, et al. Long-term, hormone-responsive organoid cultures of human endometrium in achemically defined medium. Nat Cell Biol 2017;19(05):568–577
100 BorettoM, Cox B, NobenM, et al. Development of organoids frommouse and human endometrium showing endometrial epithe-lium physiology and long-term expandability. Development2017;144(10):1775–1786
101 Sato T, Vries RG, Snippert HJ, et al. Single Lgr5 stem cells buildcrypt-villus structures in vitro without a mesenchymal niche.Nature 2009;459(7244):262–265
102 Valentijn AJ, Saretzki G, Tempest N, Critchley HO, Hapangama DK.Human endometrial epithelial telomerase is important for epithe-lial proliferation and glandular formation with potential implica-tions in endometriosis. Hum Reprod 2015;30(12):2816–2828
103 Boretto M, Maenhoudt N, Luo X, et al. Patient-derived organoidsfrom endometrial disease capture clinical heterogeneity and areamenable to drug screening. Nat Cell Biol 2019;21(08):1041–1051
104 Hapangama DK, Drury J, Da Silva L, et al. Abnormally locatedSSEA1þ/SOX9þ endometrial epithelial cells with a basalis-likephenotype in the eutopic functionalis layer may play a role inthe pathogenesis of endometriosis. Hum Reprod 2019;34(01):56–68
105 Gargett CE, Schwab KE, Zillwood RM, Nguyen HP, Wu D. Isolationand culture of epithelial progenitors and mesenchymal stem cellsfrom human endometrium. Biol Reprod 2009;80(06):1136–1145
106 Tempest N, Maclean A, Hapangama DK. Endometrial stem cellmarkers: current concepts and unresolved questions. Int J MolSci 2018;19(10):E3240
107 Tempest N, Baker AM, Wright NA, Hapangama DK. Does humanendometrial LGR5 gene expression suggest the existence ofanother hormonally regulated epithelial stem cell niche? HumReprod 2018;33(06):1052–1062
108 Valentijn AJ, Palial K, Al-Lamee H, et al. SSEA-1 isolates humanendometrial basal glandular epithelial cells: phenotypic andfunctional characterization and implications in the pathogenesisof endometriosis. Hum Reprod 2013;28(10):2695–2708
109 Miyazaki K, Dyson MT, Coon V JS, et al. Generation of progester-one-responsive endometrial stromal fibroblasts from humaninduced pluripotent stem cells: role of the WNT/CTNNB1 path-way. Stem Cell Reports 2018;11(05):1136–1155
110 Zhang Y, Zhou L, Li TC, Duan H, Yu P, Wang HY. Ultrastructuralfeatures of endometrial-myometrial interface and its alterationin adenomyosis. Int J Clin Exp Pathol 2014;7(04):1469–1477
111 Hutchinson JL, Rajagopal SP, Yuan M, Norman JE. Lipopolysac-charide promotes contraction of uterine myocytes via activationof Rho/ROCK signaling pathways. FASEB J 2014;28(01):94–105
112 Souza GR, Tseng H, Gage JA, et al. Magnetically bioprinted humanmyometrial 3D cell rings as amodel for uterine contractility. Int JMol Sci 2017;18(04):E683
113 Vaes RDW, van den Berk L, Boonen B, van Dijk DPJ, Olde DaminkSWM, Rensen SS. A novel human cell culture model to studyvisceral smooth muscle phenotypic modulation in health anddisease. Am J Physiol Cell Physiol 2018;31