Embed Size (px)
Citation preview
Physiology of the
central nervous system
Motor division of the CNS
Reflex
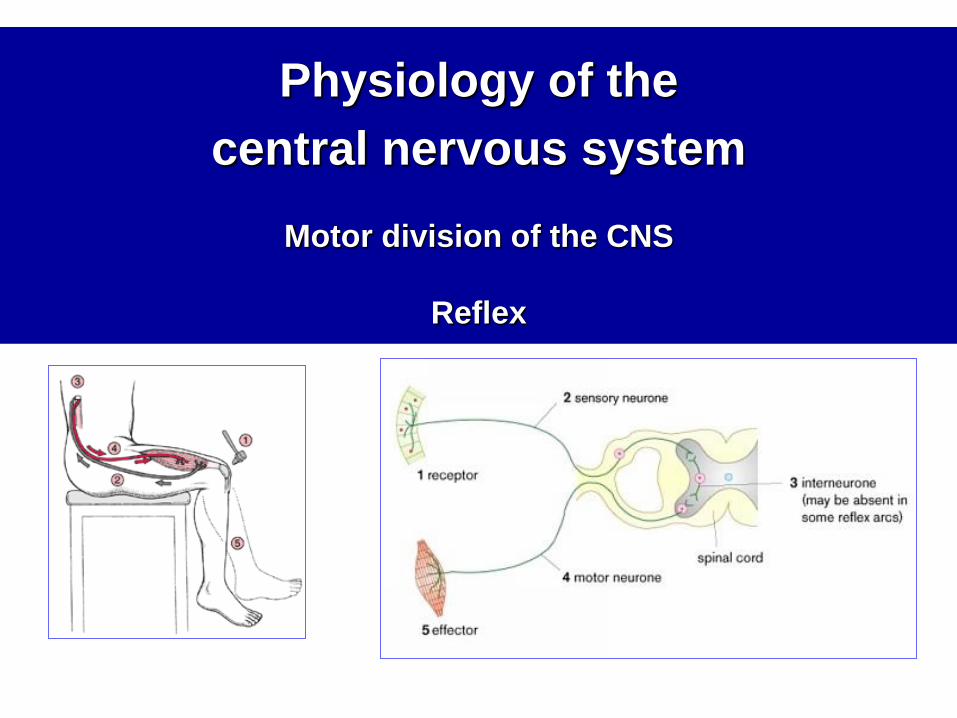
General function of the nervous system (NS)
Nervous system
-communication network of neurons that allows
the organism to interact with the environment
(external, internal)
• main function: regulation of body functions
• purpose: adaptation to changes - maintenance
of homeostasis and survival
http://www.alz.org/braintour/images/neuron_forest.jpg
1. Peripheral NS
2. Central nervous system
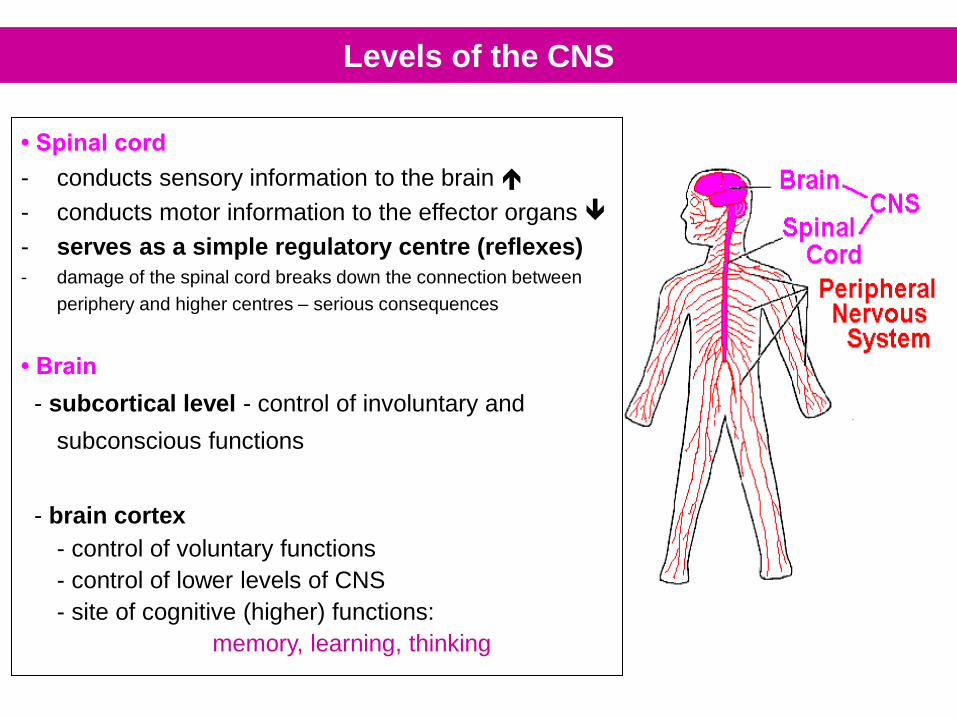
• Spinal cord
- conducts sensory information to the brain
- conducts motor information to the effector organs
- serves as a simple regulatory centre (reflexes)
- damage of the spinal cord breaks down the connection between
periphery and higher centres – serious consequences
• Brain
- subcortical level - control of involuntary and
subconscious functions
- brain cortex
- control of voluntary functions
- control of lower levels of CNS
- site of cognitive (higher) functions:
memory, learning, thinking
Levels of the CNS
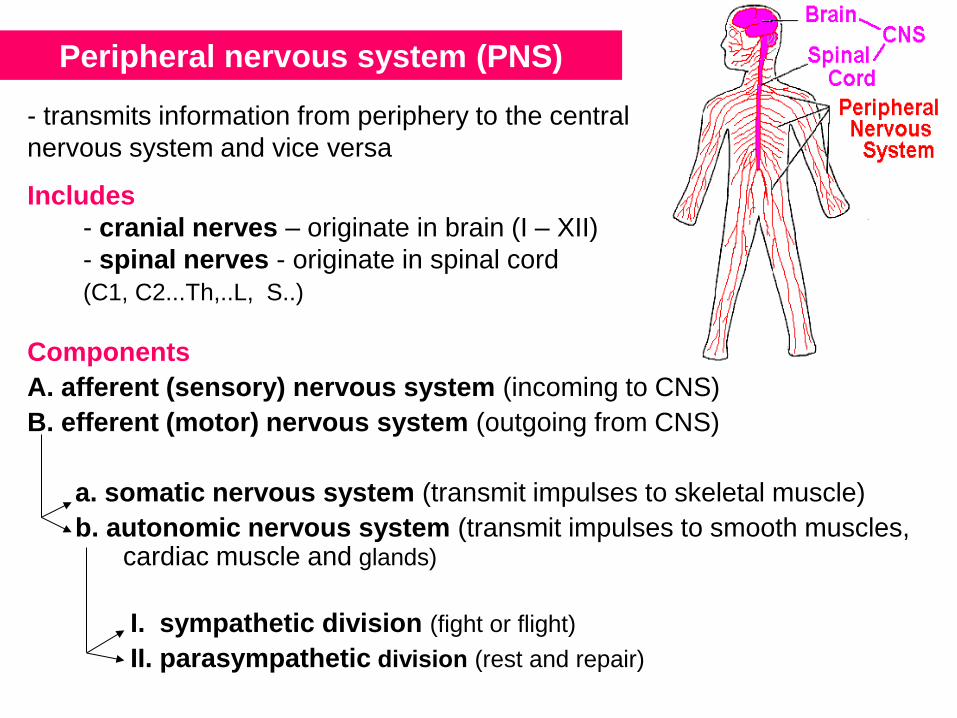
Peripheral nervous system (PNS)
- transmits information from periphery to the central
nervous system and vice versa Includes
- cranial nerves – originate in brain (I – XII)
- spinal nerves - originate in spinal cord
(C1, C2...Th,..L, S..)
Components
A. afferent (sensory) nervous system (incoming to CNS)
B. efferent (motor) nervous system (outgoing from CNS)
a. somatic nervous system (transmit impulses to skeletal muscle)
b. autonomic nervous system (transmit impulses to smooth muscles, cardiac muscle and glands)
I. sympathetic division (fight or flight)
II. parasympathetic division (rest and repair)
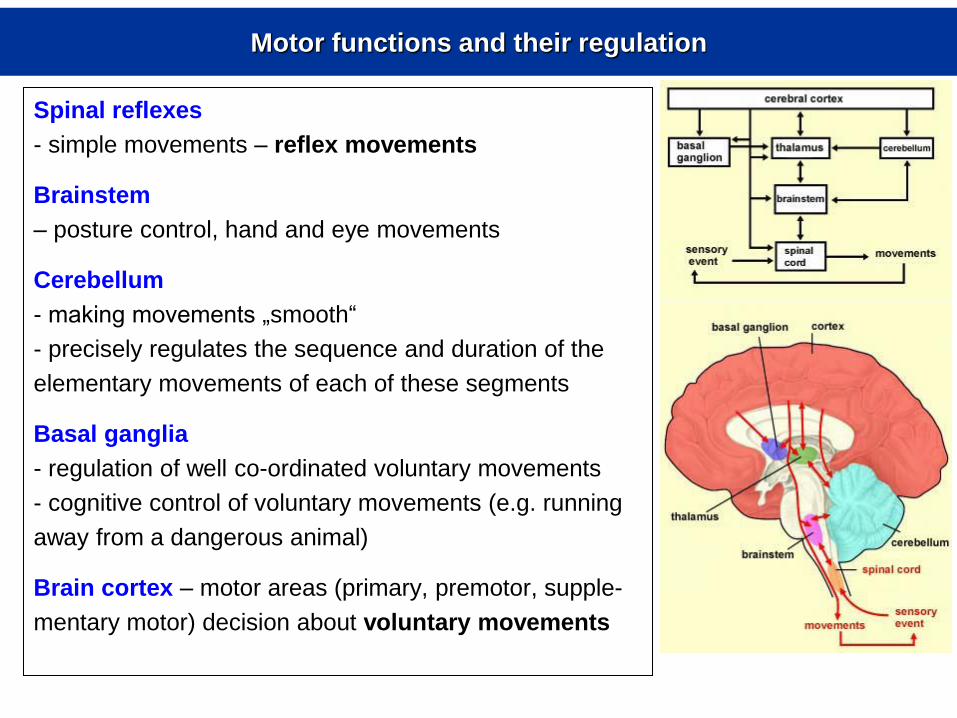
Motor functions and their regulation
Spinal reflexes
- simple movements – reflex movements
Brainstem
– posture control, hand and eye movements
Cerebellum
- making movements „smooth“
- precisely regulates the sequence and duration of the
elementary movements of each of these segments
Basal ganglia
- regulation of well co-ordinated voluntary movements
- cognitive control of voluntary movements (e.g. running
away from a dangerous animal)
Brain cortex – motor areas (primary, premotor, supple-
mentary motor) decision about voluntary movements
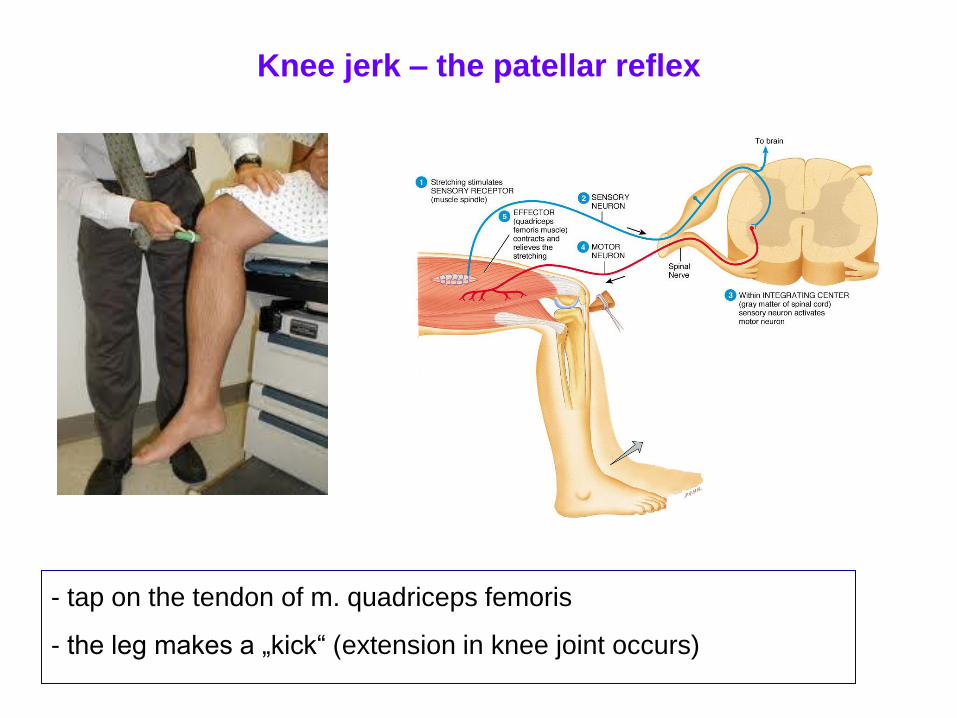
Knee jerk – the patellar reflex
- tap on the tendon of m. quadriceps femoris
- the leg makes a „kick“ (extension in knee joint occurs)
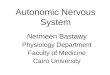
Reflex
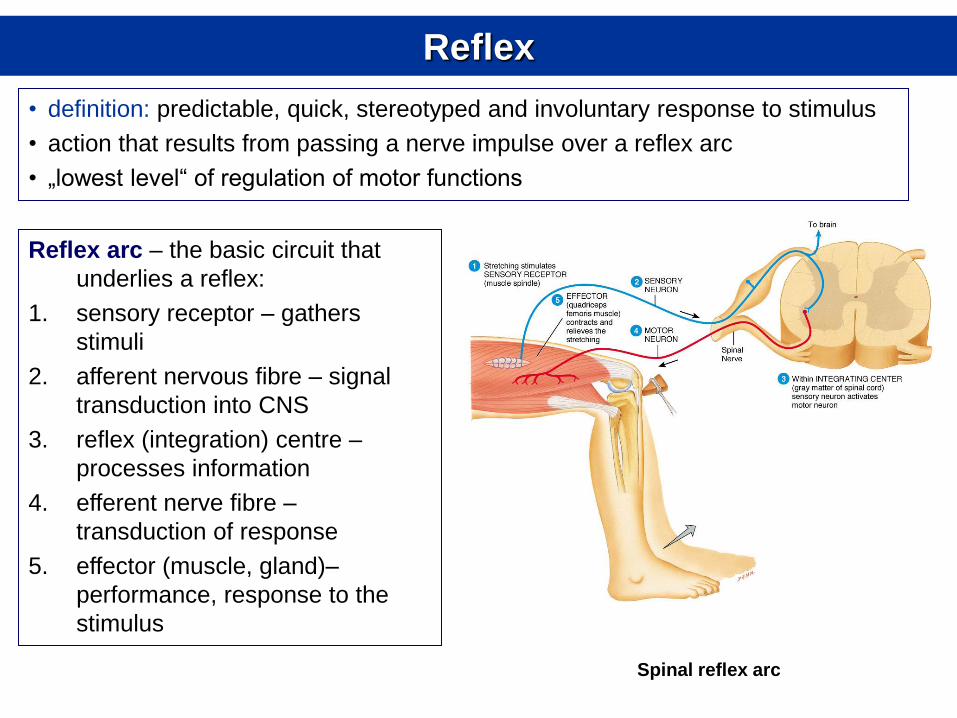
• definition: predictable, quick, stereotyped and involuntary response to stimulus
• action that results from passing a nerve impulse over a reflex arc
• „lowest level“ of regulation of motor functions
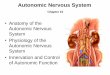
Reflex arc – the basic circuit that
underlies a reflex:
1. sensory receptor – gathers
stimuli
2. afferent nervous fibre – signal
transduction into CNS
3. reflex (integration) centre –
processes information
4. efferent nerve fibre –
transduction of response
5. effector (muscle, gland)–
performance, response to the
stimulus
Spinal reflex arc
Classification of reflexes – with respect to:
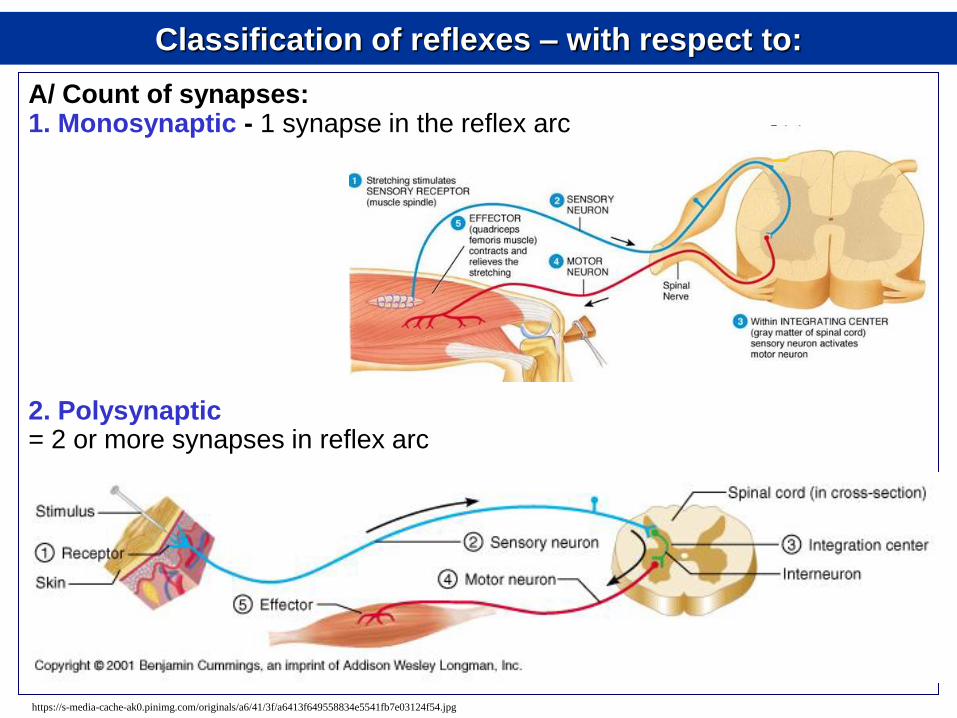
A/ Count of synapses: 1. Monosynaptic - 1 synapse in the reflex arc 2. Polysynaptic = 2 or more synapses in reflex arc
https://s-media-cache-ak0.pinimg.com/originals/a6/41/3f/a6413f649558834e5541fb7e03124f54.jpg
Classification of reflexes – with respect to:
B/ Type of sensory receptor
Exteroceptive – receptor in the reflex arc is an exteroceptor (gathers stimuli
from external environment)
Proprioceptive – receptor in the reflex arc is an proprioceptor (gathers stimuli
about position of the body)
Interoceptive – receptor in the reflex arc is an proprioceptor (gather stimuli
from internal environment)
C/ Integration (reflex) centre Cranial – centre in nuclei of the cranial nerves Spinal – centre in the spinal cord Extracentral – integration centre in autonomic ganglia
D/ Effector Somatic – effector: skeletal muscle Autonomic (visceral) – effector: cardiac muscle, smooth muscle, gland E/ Origin Inborn – related to locomotion, defence, food intake, sexual behaviour Acquired – develop during life
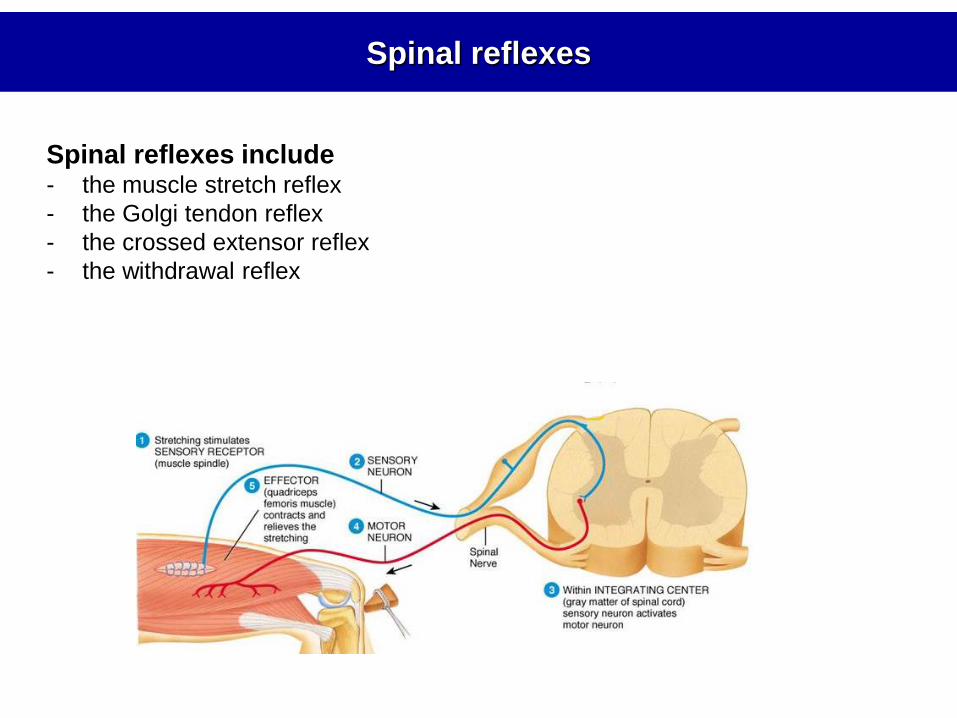
Spinal reflexes
Spinal reflexes include - the muscle stretch reflex
- the Golgi tendon reflex
- the crossed extensor reflex
- the withdrawal reflex
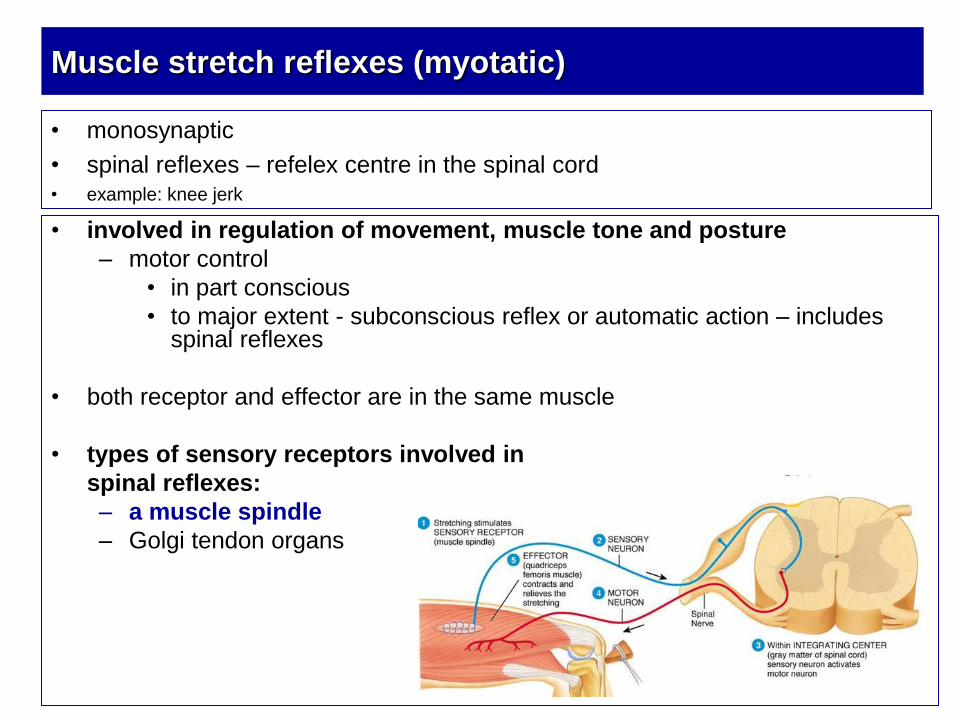
• involved in regulation of movement, muscle tone and posture
– motor control
• in part conscious
• to major extent - subconscious reflex or automatic action – includes spinal reflexes
• both receptor and effector are in the same muscle
• types of sensory receptors involved in
spinal reflexes:
– a muscle spindle
– Golgi tendon organs
Muscle stretch reflexes (myotatic)
• monosynaptic
• spinal reflexes – refelex centre in the spinal cord • example: knee jerk
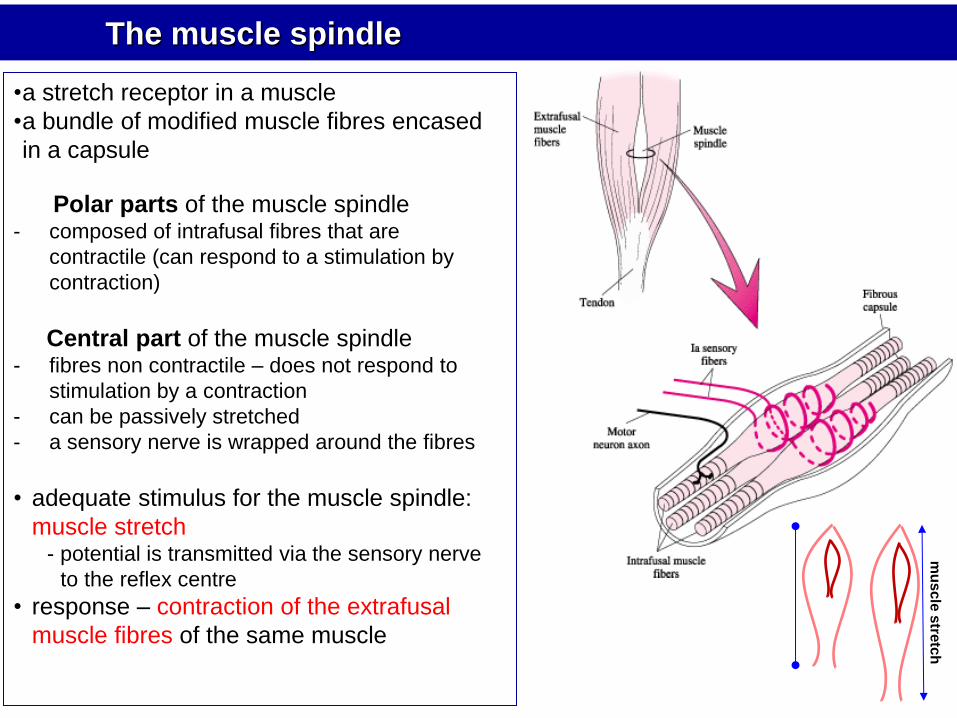
The muscle spindle
•a stretch receptor in a muscle
•a bundle of modified muscle fibres encased
in a capsule
Polar parts of the muscle spindle - composed of intrafusal fibres that are
contractile (can respond to a stimulation by
contraction)
Central part of the muscle spindle - fibres non contractile – does not respond to
stimulation by a contraction
- can be passively stretched
- a sensory nerve is wrapped around the fibres
• adequate stimulus for the muscle spindle:
muscle stretch - potential is transmitted via the sensory nerve
to the reflex centre
• response – contraction of the extrafusal
muscle fibres of the same muscle
c c
mu
scle
stre
tch
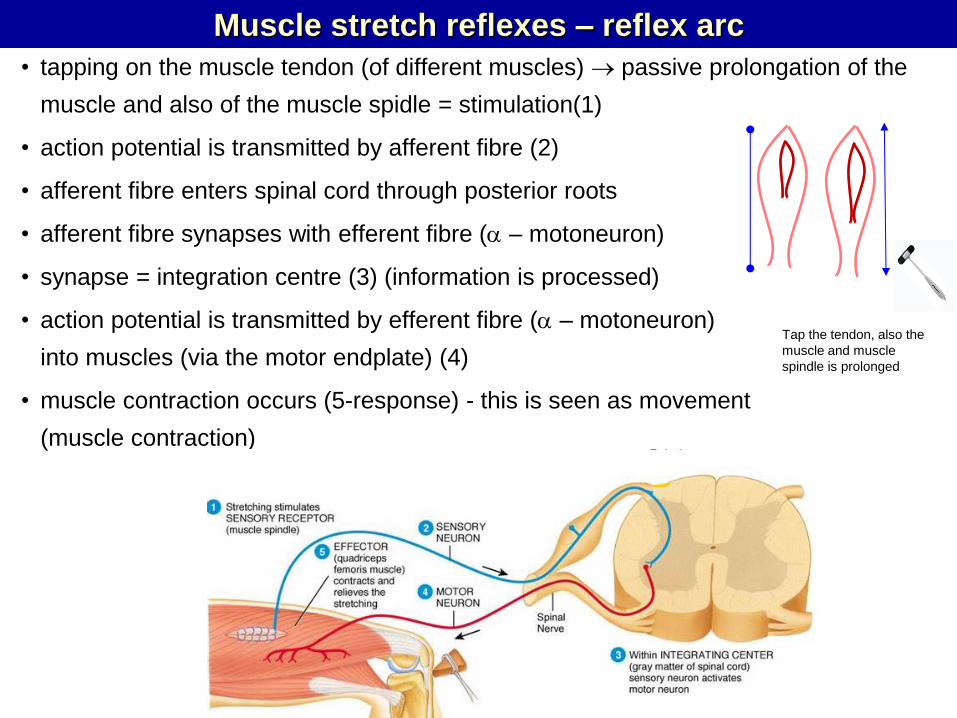
• tapping on the muscle tendon (of different muscles) passive prolongation of the
muscle and also of the muscle spidle = stimulation(1)
• action potential is transmitted by afferent fibre (2)
• afferent fibre enters spinal cord through posterior roots
• afferent fibre synapses with efferent fibre (a – motoneuron)
• synapse = integration centre (3) (information is processed)
• action potential is transmitted by efferent fibre (a – motoneuron)
into muscles (via the motor endplate) (4)
• muscle contraction occurs (5-response) - this is seen as movement
(muscle contraction)
Muscle stretch reflexes – reflex arc
c c
Tap the tendon, also the
muscle and muscle
spindle is prolonged
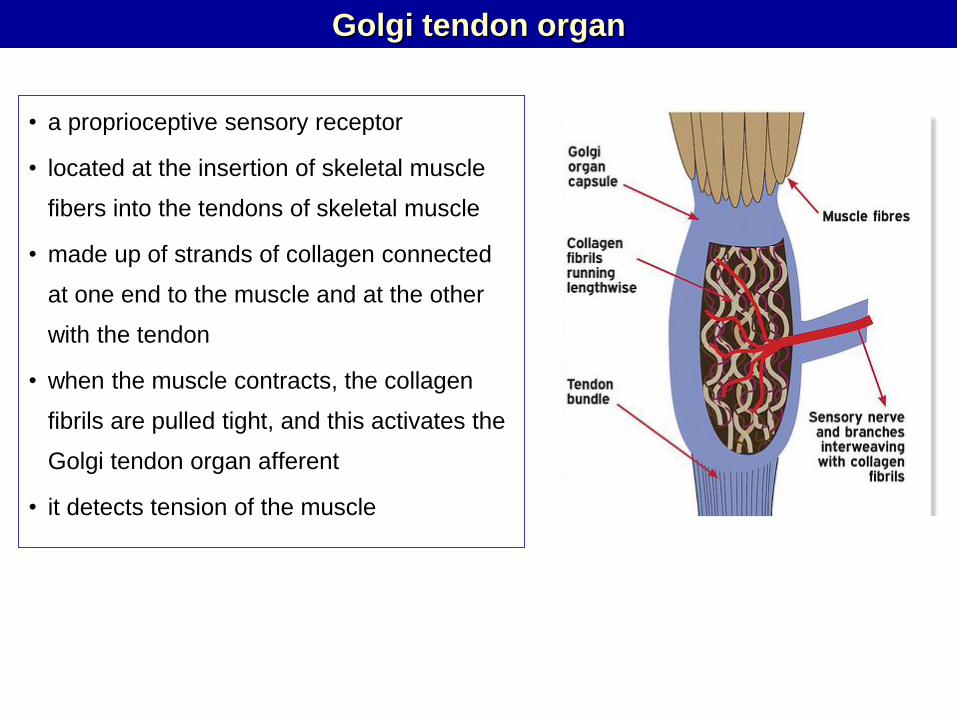
• a proprioceptive sensory receptor
• located at the insertion of skeletal muscle
fibers into the tendons of skeletal muscle
• made up of strands of collagen connected
at one end to the muscle and at the other
with the tendon
• when the muscle contracts, the collagen
fibrils are pulled tight, and this activates the
Golgi tendon organ afferent
• it detects tension of the muscle
Golgi tendon organ
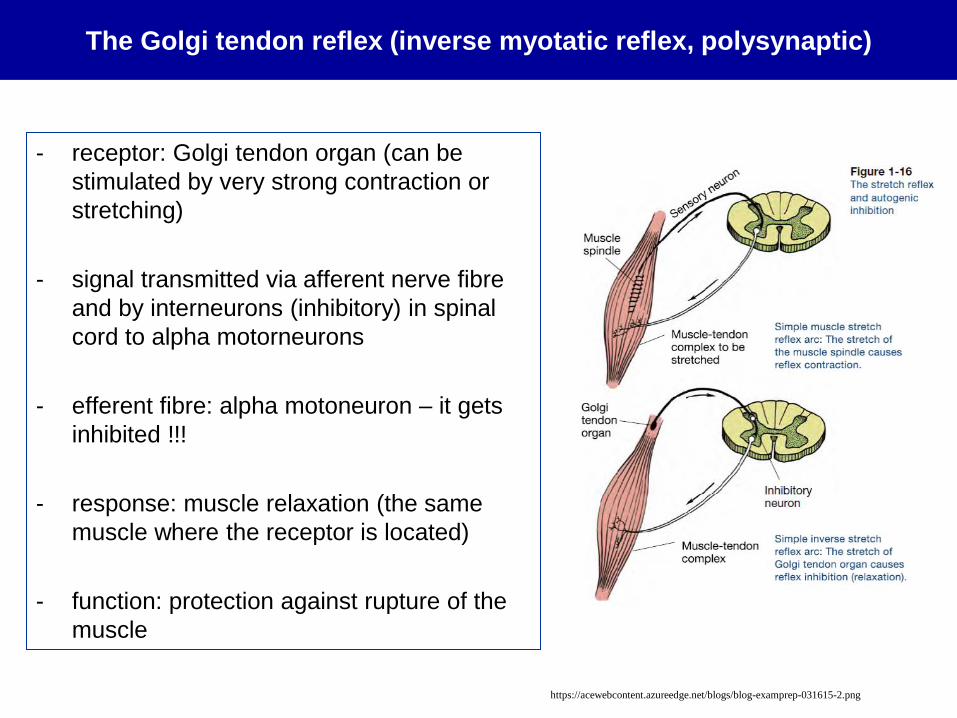
- receptor: Golgi tendon organ (can be
stimulated by very strong contraction or
stretching)
- signal transmitted via afferent nerve fibre
and by interneurons (inhibitory) in spinal
cord to alpha motorneurons
- efferent fibre: alpha motoneuron – it gets
inhibited !!!
- response: muscle relaxation (the same
muscle where the receptor is located)
- function: protection against rupture of the
muscle
The Golgi tendon reflex (inverse myotatic reflex, polysynaptic)
https://acewebcontent.azureedge.net/blogs/blog-examprep-031615-2.png
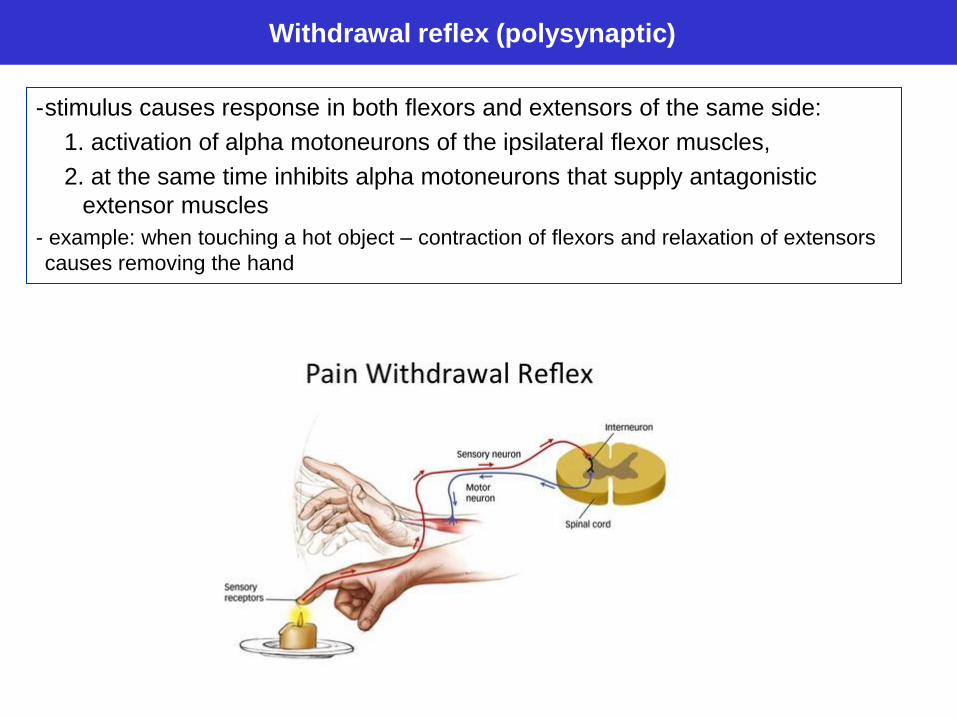
-stimulus causes response in both flexors and extensors of the same side:
1. activation of alpha motoneurons of the ipsilateral flexor muscles,
2. at the same time inhibits alpha motoneurons that supply antagonistic
extensor muscles
- example: when touching a hot object – contraction of flexors and relaxation of extensors
causes removing the hand
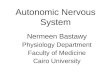
Withdrawal reflex (polysynaptic)
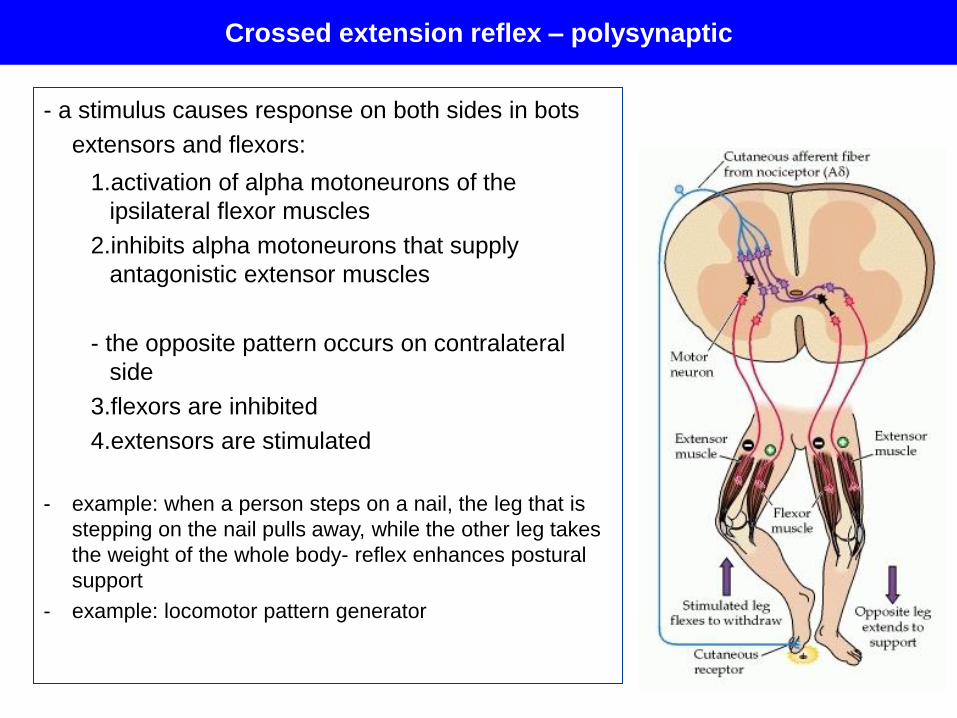
- a stimulus causes response on both sides in bots
extensors and flexors:
1.activation of alpha motoneurons of the
ipsilateral flexor muscles
2.inhibits alpha motoneurons that supply
antagonistic extensor muscles
- the opposite pattern occurs on contralateral
side
3.flexors are inhibited
4.extensors are stimulated
- example: when a person steps on a nail, the leg that is
stepping on the nail pulls away, while the other leg takes
the weight of the whole body- reflex enhances postural
support
- example: locomotor pattern generator
Crossed extension reflex – polysynaptic
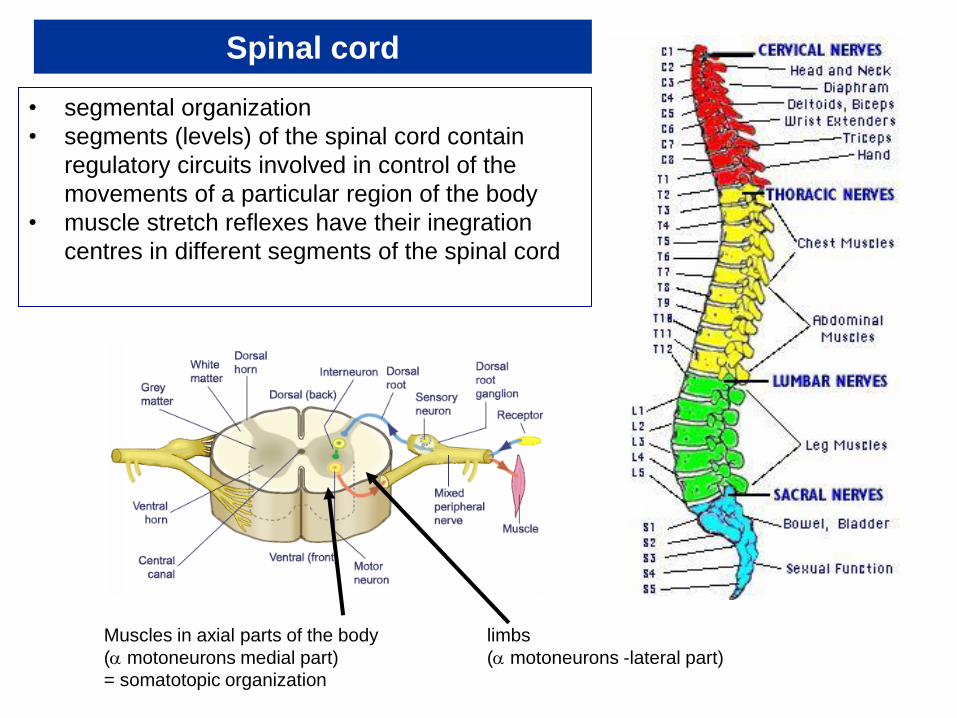
Spinal cord
• segmental organization
• segments (levels) of the spinal cord contain
regulatory circuits involved in control of the
movements of a particular region of the body
• muscle stretch reflexes have their inegration
centres in different segments of the spinal cord
Muscles in axial parts of the body limbs
(a motoneurons medial part) (a motoneurons -lateral part)
= somatotopic organization
Examination of reflexes in a human
• basic examination in neurology
• indicates the function of reflex arc (and all its components)
• reflex - stereotypic reaction = predicted response
• normoreflexia – normal reflex response on a stimulus
• abnormal response indicates disorder in a part of reflex arc
Types of abnormal results:
• hyperreflexia (or clonus) – hyperactive reflex
• hyporeflexia – diminished reflex
• areflexia – absence of response
• abnormal reflex – the response on the stimulation is abnormal
Principle
• sensory receptors are stimulated
• the reflex response on stimulation is observed and evaluated
Procedure
• the patient is in sitting or lying position (depends on the reflex)
• sensory receptors are stimulated by a reflex hammer, cotton,
light, needle (depends on the reflex that we want to examine)
• examine following reflexes (see next slides)
Task: Examination of reflexes in a human
Reflex examination video
https://www.youtube.com/watch?v=eqOpNQH09pA
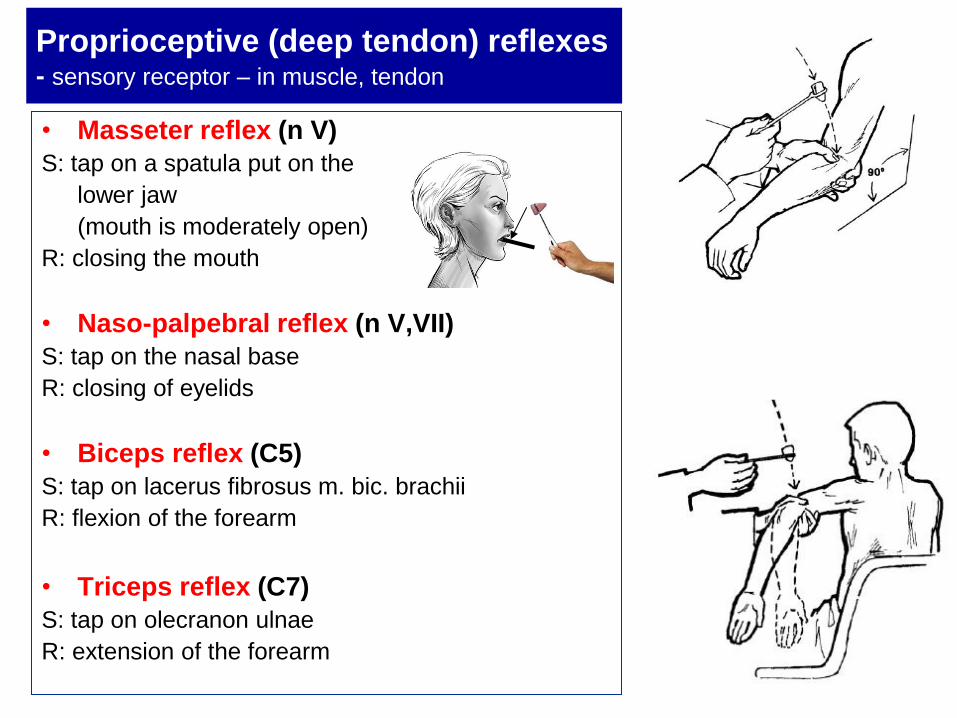
Proprioceptive (deep tendon) reflexes - sensory receptor – in muscle, tendon
• Masseter reflex (n V)
S: tap on a spatula put on the
lower jaw
(mouth is moderately open)
R: closing the mouth
• Naso-palpebral reflex (n V,VII)
S: tap on the nasal base
R: closing of eyelids
• Biceps reflex (C5)
S: tap on lacerus fibrosus m. bic. brachii
R: flexion of the forearm
• Triceps reflex (C7)
S: tap on olecranon ulnae
R: extension of the forearm
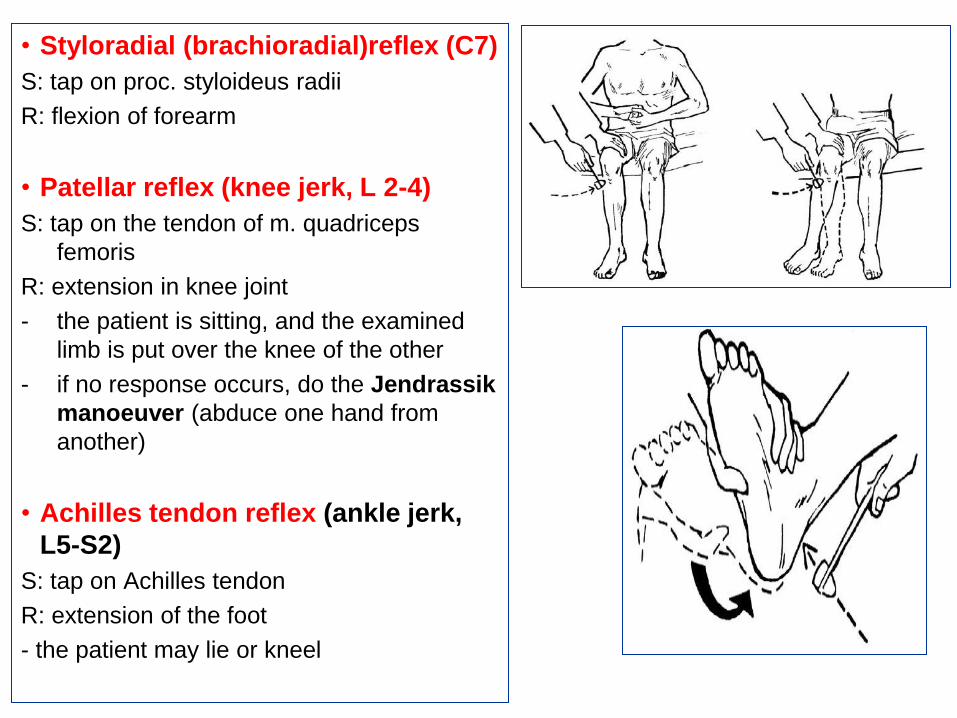
• Styloradial (brachioradial)reflex (C7)
S: tap on proc. styloideus radii
R: flexion of forearm
• Patellar reflex (knee jerk, L 2-4)
S: tap on the tendon of m. quadriceps
femoris
R: extension in knee joint
- the patient is sitting, and the examined
limb is put over the knee of the other
- if no response occurs, do the Jendrassik
manoeuver (abduce one hand from
another)
• Achilles tendon reflex (ankle jerk,
L5-S2)
S: tap on Achilles tendon
R: extension of the foot
- the patient may lie or kneel
Achilles tendon reflex measurement
Principle:
- thyroid hormones (thyroxin, triiodthyronine) influence the activity of
the central nervous system
- examination of Achilles tendon reflex is an indirect indicator of thyroid
activity (Ankle jerk)
- reflex time (stimulation – response) depends directly on the level of
thyroid hormones
- normal reflex response – euthyrosis
- weak response – hypothyrosis
- excessive response – hyperthyrosis
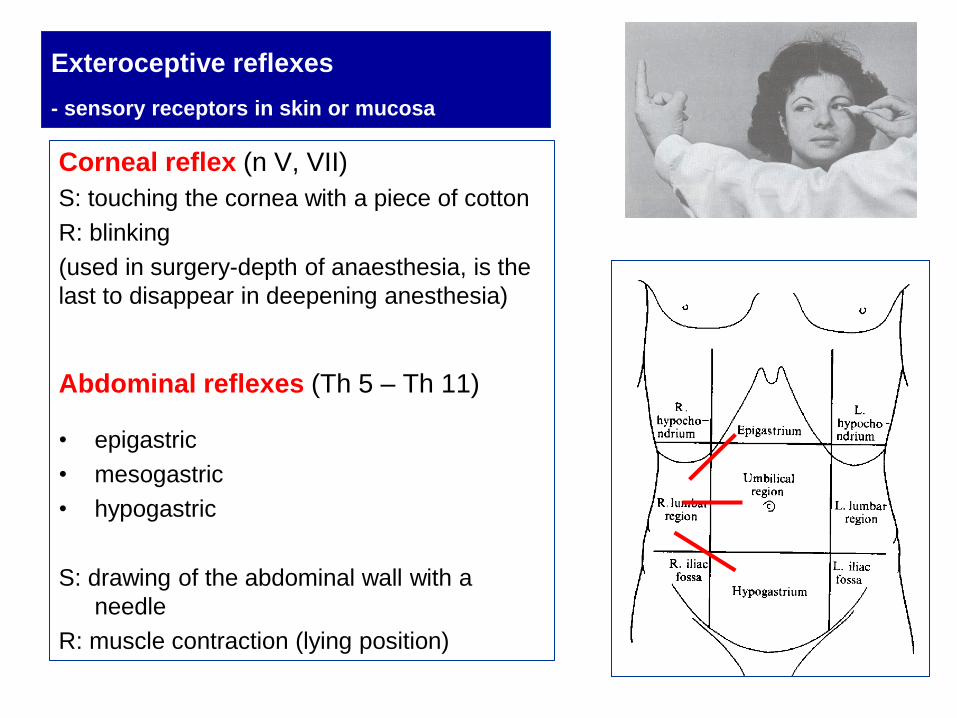
Exteroceptive reflexes
- sensory receptors in skin or mucosa
Corneal reflex (n V, VII)
S: touching the cornea with a piece of cotton
R: blinking
(used in surgery-depth of anaesthesia, is the
last to disappear in deepening anesthesia)
Abdominal reflexes (Th 5 – Th 11)
• epigastric
• mesogastric
• hypogastric
S: drawing of the abdominal wall with a
needle
R: muscle contraction (lying position)

Plantar reflex (L5-S2)
S: stimulation of external side of planta pedis with a needle (from heel to little
finger and other fingers)
R: plantar flexion or the toe (or all fingers)
- if pyramidal pathway is impaired the response in plantar reflex is abnormal
(this is called Babinski phenomenon)
R: extension of the toe
- normal in babies up to 6-8 months, later a sign of disorder
- indicates abnormalities in pyramidal tract
Autonomic (vegetative) reflexes - response – transmitted by autonomic fibres
• Pupilary light reflex
S: illumination of an eye (use battery)
R: miosis – diameter of the pupil becomes narrow
- consensual reaction – if one eye is illuminated,
miosis occur bilaterally
• Oculocardial reflex
S: moderate pressure on the eyeball
R: decrease in pulse frequency (by 5-10 beats per minute)
• Orthostatic reflex
S: sudden change position from lying to sitting
R: increase in pulse frequency
• Solar reflex
S: pressure against solar plexus
R: drop in pulse frequency
– all reflexes- measure heart rate only 15´´, then multiply by 4 (rate per min)
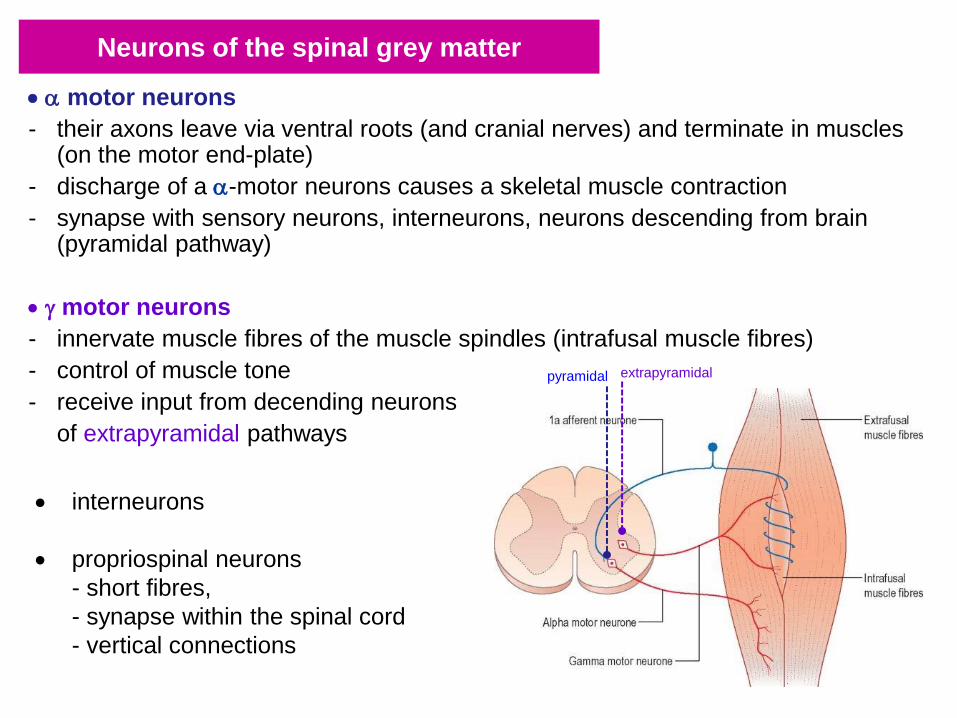
Neurons of the spinal grey matter
a motor neurons
- their axons leave via ventral roots (and cranial nerves) and terminate in muscles (on the motor end-plate)
- discharge of a a-motor neurons causes a skeletal muscle contraction
- synapse with sensory neurons, interneurons, neurons descending from brain (pyramidal pathway)
g motor neurons
- innervate muscle fibres of the muscle spindles (intrafusal muscle fibres)
- control of muscle tone
- receive input from decending neurons
of extrapyramidal pathways
interneurons
propriospinal neurons
- short fibres,
- synapse within the spinal cord
- vertical connections
extrapyramidal pyramidal
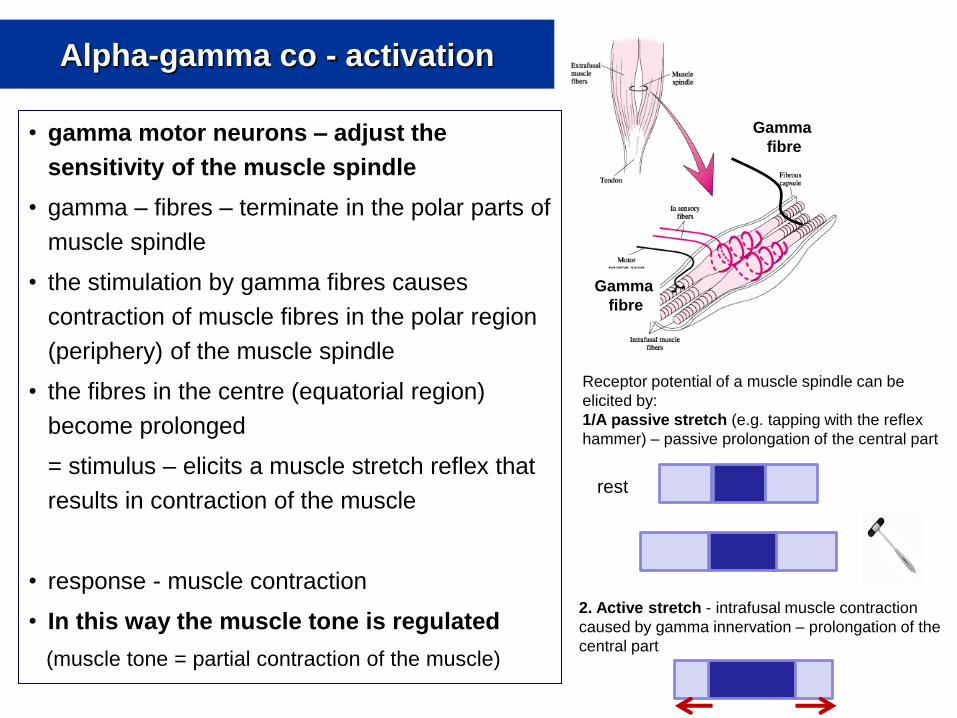
Alpha-gamma co - activation
• gamma motor neurons – adjust the
sensitivity of the muscle spindle
• gamma – fibres – terminate in the polar parts of
muscle spindle
• the stimulation by gamma fibres causes
contraction of muscle fibres in the polar region
(periphery) of the muscle spindle
• the fibres in the centre (equatorial region)
become prolonged
= stimulus – elicits a muscle stretch reflex that
results in contraction of the muscle
• response - muscle contraction
• In this way the muscle tone is regulated
(muscle tone = partial contraction of the muscle)
Gamma
fibre
rest
Receptor potential of a muscle spindle can be
elicited by:
1/A passive stretch (e.g. tapping with the reflex
hammer) – passive prolongation of the central part
2. Active stretch - intrafusal muscle contraction
caused by gamma innervation – prolongation of the
central part
Gamma
fibre
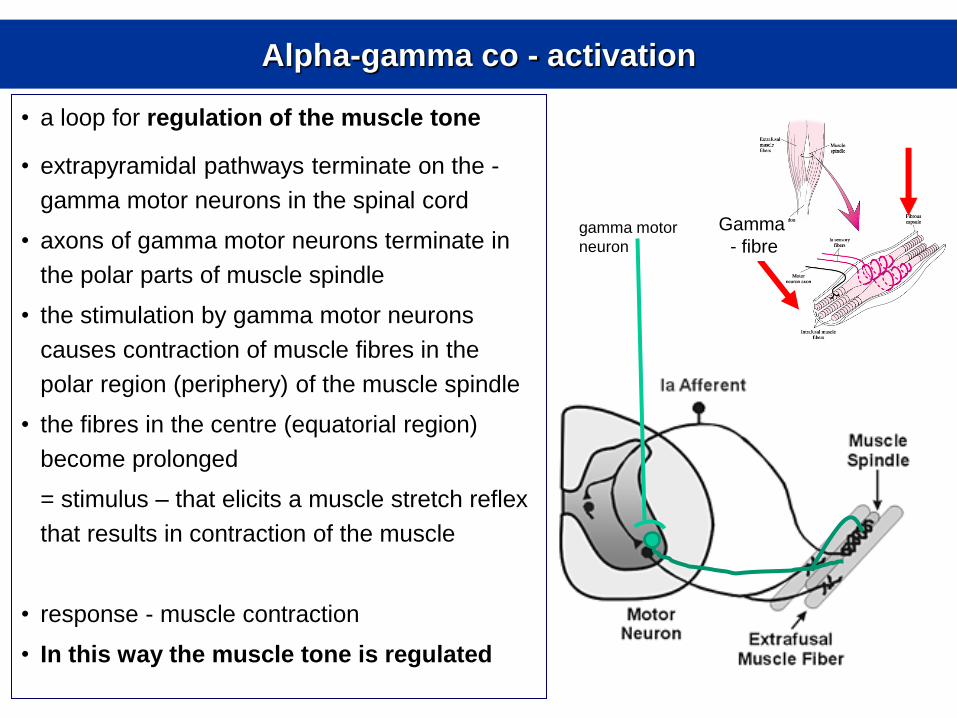
Alpha-gamma co - activation
• a loop for regulation of the muscle tone
• extrapyramidal pathways terminate on the -
gamma motor neurons in the spinal cord
• axons of gamma motor neurons terminate in
the polar parts of muscle spindle
• the stimulation by gamma motor neurons
causes contraction of muscle fibres in the
polar region (periphery) of the muscle spindle
• the fibres in the centre (equatorial region)
become prolonged
= stimulus – that elicits a muscle stretch reflex
that results in contraction of the muscle
• response - muscle contraction
• In this way the muscle tone is regulated
Gamma
- fibre gamma motor
neuron
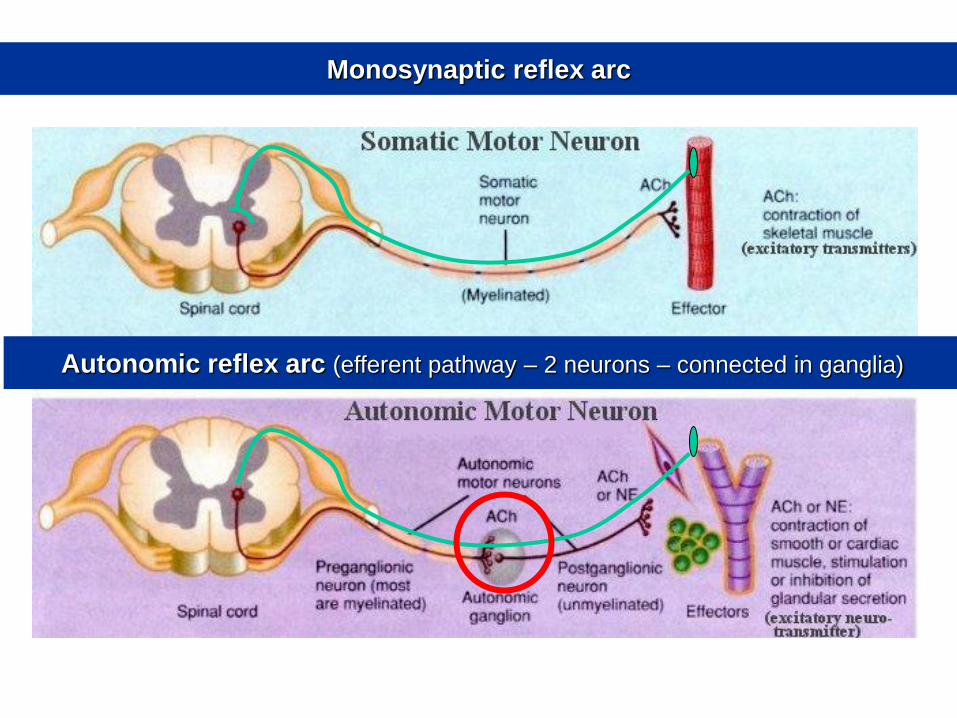
Monosynaptic reflex arc
Autonomic reflex arc (efferent pathway – 2 neurons – connected in ganglia)
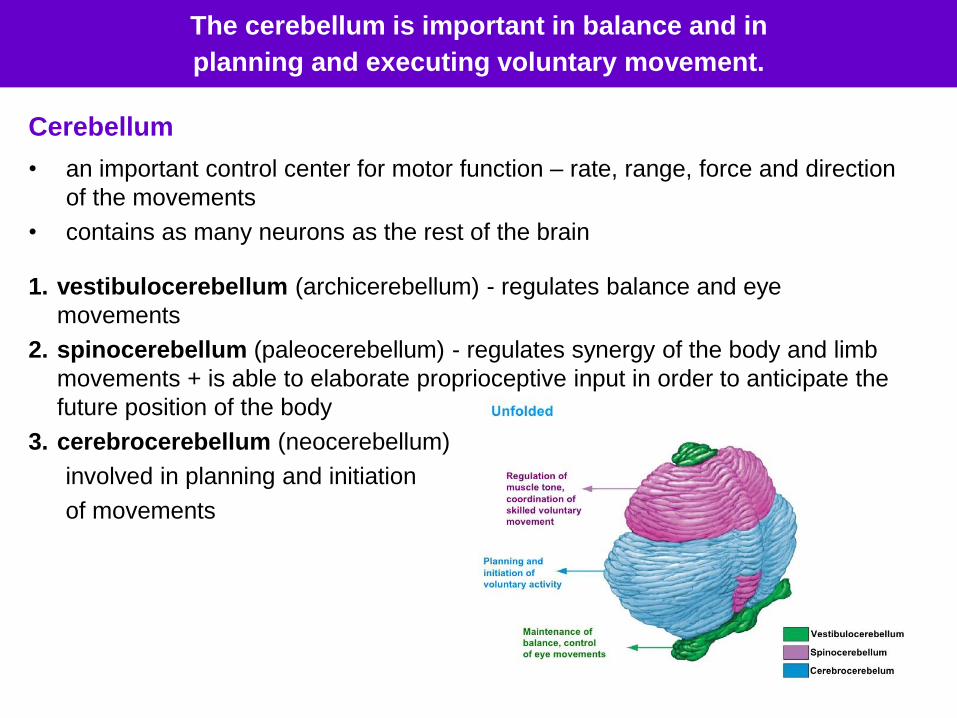
The cerebellum is important in balance and in
planning and executing voluntary movement.
Cerebellum
• an important control center for motor function – rate, range, force and direction
of the movements
• contains as many neurons as the rest of the brain
1. vestibulocerebellum (archicerebellum) - regulates balance and eye
movements
2. spinocerebellum (paleocerebellum) - regulates synergy of the body and limb
movements + is able to elaborate proprioceptive input in order to anticipate the
future position of the body
3. cerebrocerebellum (neocerebellum)
involved in planning and initiation
of movements
Examination of the cerebellum
Scanning speech
• Scanning speech refers to slow, slurred, monotonous, and irregular
speech that is associated with dysarthria due to oral motor ataxia.
Causes enunciation of individual syllables.
• Test: Ask the patient to say: “the British parliament”. In case of
scanning speech it becomes “the Brit-tish Par-la-ment.”
Nystagmus
• Ocular findings are generally less prominent, but ipsilateral gaze-
evoked nystagmus are is seen with fast phase toward side of cerebellar
lesion.
• Test: Ask the patient to follow your finger and observe presence of
nystagmus.
http://stanfordmedicine25.stanford.edu/the25/cerebellar.html
Dysmetria (Finger to nose & finger to finger test)
• Limb ataxia is usually seen clinically as difficulty with coordinated tasks.
• Test: Ask patient to fully extend arm then touch nose or ask them to touch their
nose then fully extend to touch your finger. You increase the difficulty of this
test by adding resistance to the patient's movements or move your finger to
different locations. Abnormality of this is called dysmetria.
Rebound phenomenon
• If the patient pulls on your hand and when you slip your hand out of their
grasp, normally the antagonist muscles will contract and stop their arm from
moving in the desired direction.
• In cerebellar disease this response is completely absent causing to limb to
continue moving in the desired direction.
• Test: Have the patient pull on your hand and when they do, slip your hand out
of their grasp. Observe the presence of rebound phenomenon.
(Be careful that you protect the patient from the unarrested movement causing
them to strike themselves.)
Rapid alternating movements
• Common finding in cerebellar disease is dysdiadochokinesia
(incoordination when performing rapid alternating movements).
• Test: Ask patient to place one hand over the next and have them flip one
hand back and forth (pronate and supinate) as fast as possible
(alternatively you can ask the patient to quickly tap their foot on the floor as
fast as possible).
Hypotonia
• Low muscle tone may be present in cerebellar diesases.
• Test: Perform the examination of the patellar reflex (knee jerk). “Pendular”
knee jerk, leg keeps swinging after knee jerk more than 4 times (4 or less
is normal).
Gait
• Test: Ask the patient to walk straight forward
• In cerebellar disorders – the gait is commonly wide based and
staggering. They may fall to the side of the lesion.
Romberg’s test
• Whilst Rombergs test does not directly test for cerebellar ataxia, it
helps to differentiate cerebellar ataxia from sensory ataxia. In cerebellar
ataxia the patient is likely to be unsteady on their feet even with the
eyes open.
• Test: Perform Romberg’s test by asking the patient to stand unaided
with their eyes closed and heels together.
• If the patient sways (titubation) or loses balance then this test is
positive. Stand near the patient in case they fall.
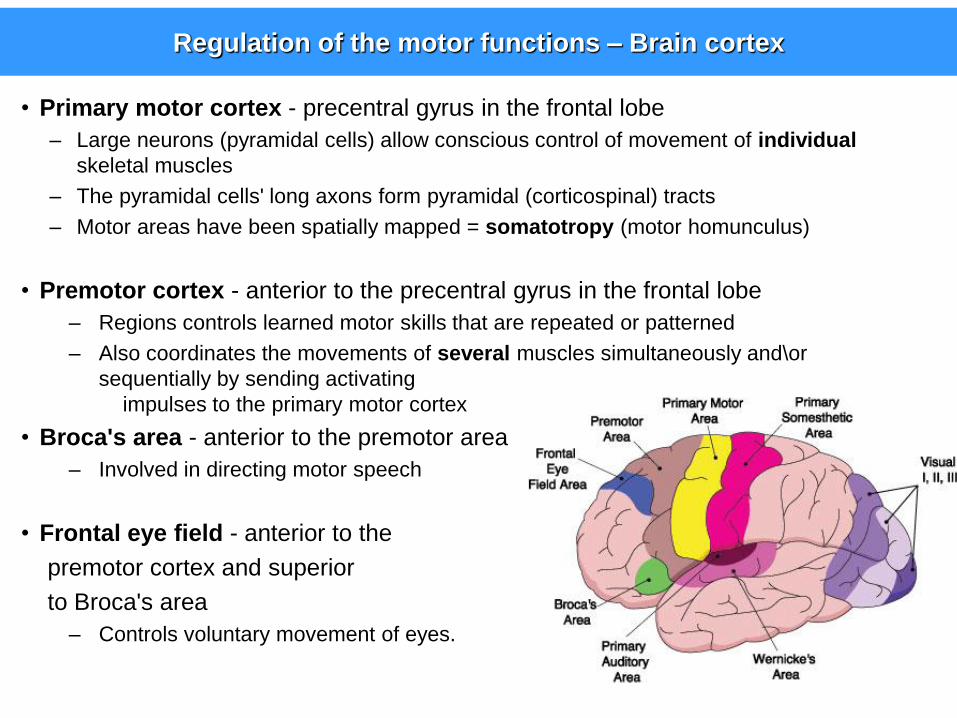
Regulation of the motor functions – Brain cortex
• Primary motor cortex - precentral gyrus in the frontal lobe
– Large neurons (pyramidal cells) allow conscious control of movement of individual
skeletal muscles
– The pyramidal cells' long axons form pyramidal (corticospinal) tracts
– Motor areas have been spatially mapped = somatotropy (motor homunculus)
• Premotor cortex - anterior to the precentral gyrus in the frontal lobe
– Regions controls learned motor skills that are repeated or patterned
– Also coordinates the movements of several muscles simultaneously and\or
sequentially by sending activating
impulses to the primary motor cortex
• Broca's area - anterior to the premotor area
– Involved in directing motor speech
• Frontal eye field - anterior to the
premotor cortex and superior
to Broca's area
– Controls voluntary movement of eyes.
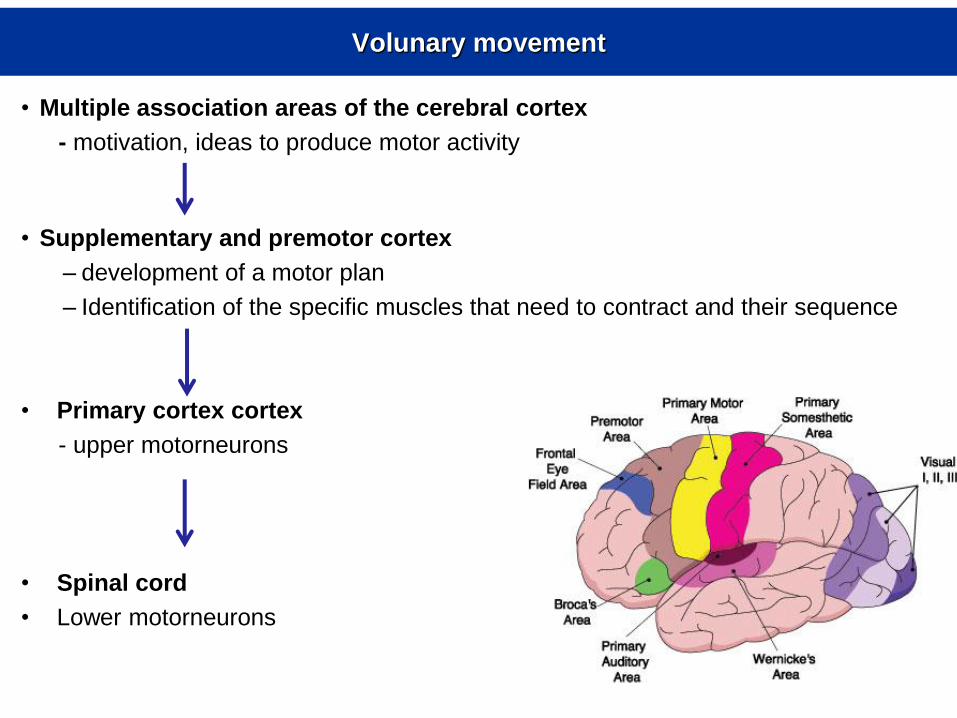
Volunary movement
• Multiple association areas of the cerebral cortex
- motivation, ideas to produce motor activity
• Supplementary and premotor cortex
– development of a motor plan
– Identification of the specific muscles that need to contract and their sequence
• Primary cortex cortex
- upper motorneurons
• Spinal cord
• Lower motorneurons
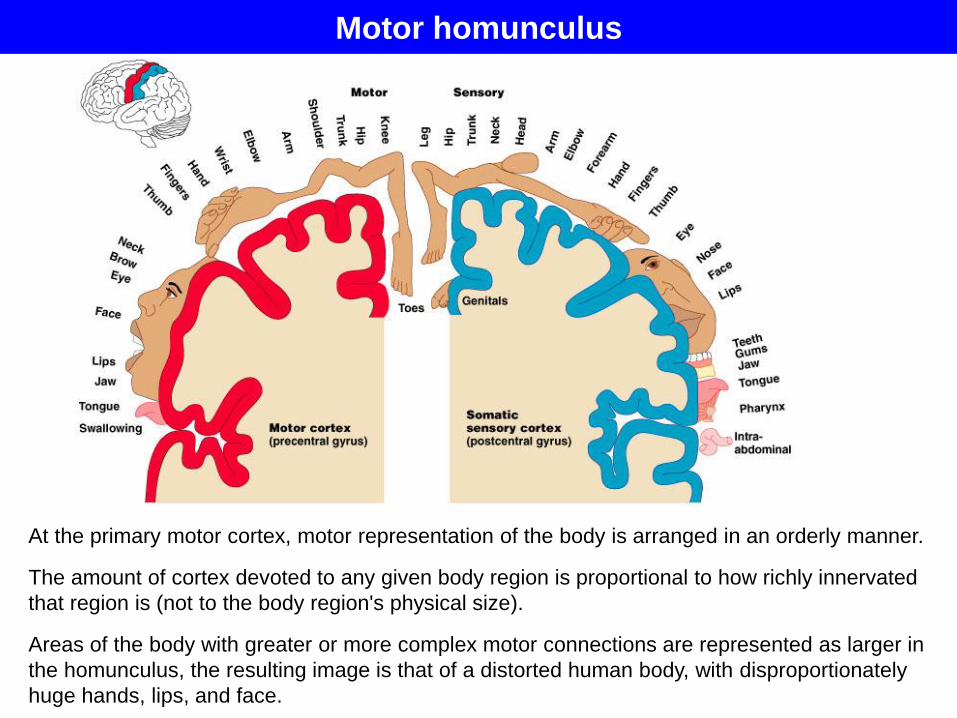
Motor homunculus
At the primary motor cortex, motor representation of the body is arranged in an orderly manner.
The amount of cortex devoted to any given body region is proportional to how richly innervated
that region is (not to the body region's physical size).
Areas of the body with greater or more complex motor connections are represented as larger in
the homunculus, the resulting image is that of a distorted human body, with disproportionately
huge hands, lips, and face.
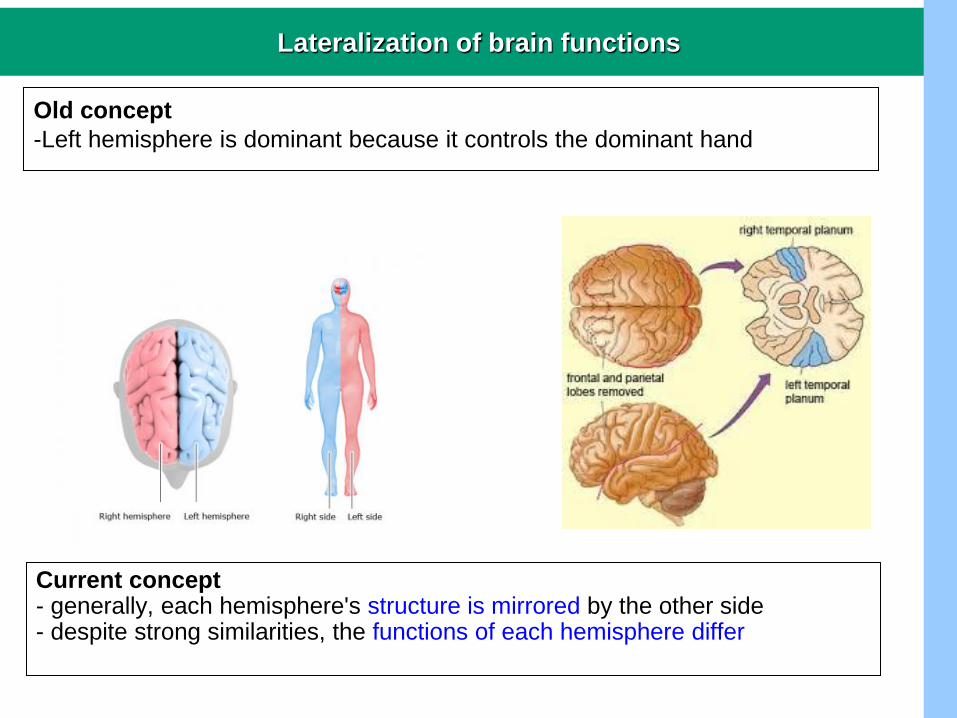
Lateralization of brain functions
Old concept
-Left hemisphere is dominant because it controls the dominant hand
Current concept - generally, each hemisphere's structure is mirrored by the other side - despite strong similarities, the functions of each hemisphere differ
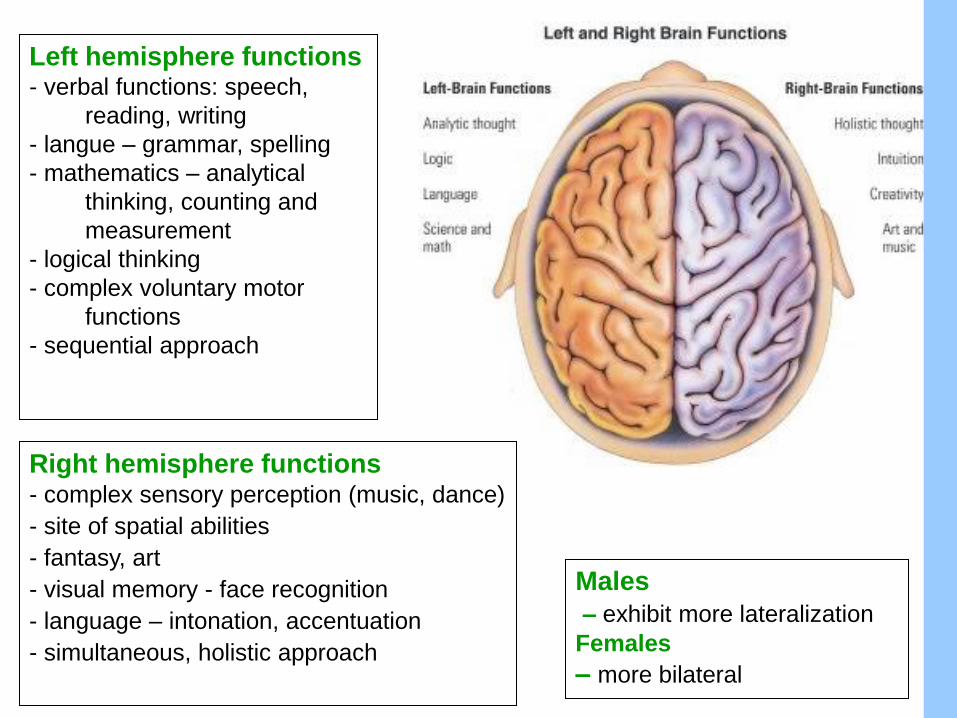
Left hemisphere functions - verbal functions: speech,
reading, writing
- langue – grammar, spelling
- mathematics – analytical
thinking, counting and
measurement
- logical thinking
- complex voluntary motor
functions
- sequential approach
Right hemisphere functions - complex sensory perception (music, dance)
- site of spatial abilities
- fantasy, art
- visual memory - face recognition
- language – intonation, accentuation
- simultaneous, holistic approach
Males
– exhibit more lateralization
Females
– more bilateral
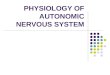
Task: Assessment of motor handedness
• handedness - the preference of one hand over the other
• usually one hand is considered dominant
• most people are right-handed (90% of population)
• some individuals exhibit the ability to use both hands equally (ambidexterity)
• preference for one hand is most likely the effect of brain lateralization
• handedness has a genetic basis, it is also influenced by socio-cultural pressures
http://www.well.ox.ac.uk/_asset/image/nov-10-handedness-and-language.jpeg/fit/460/768
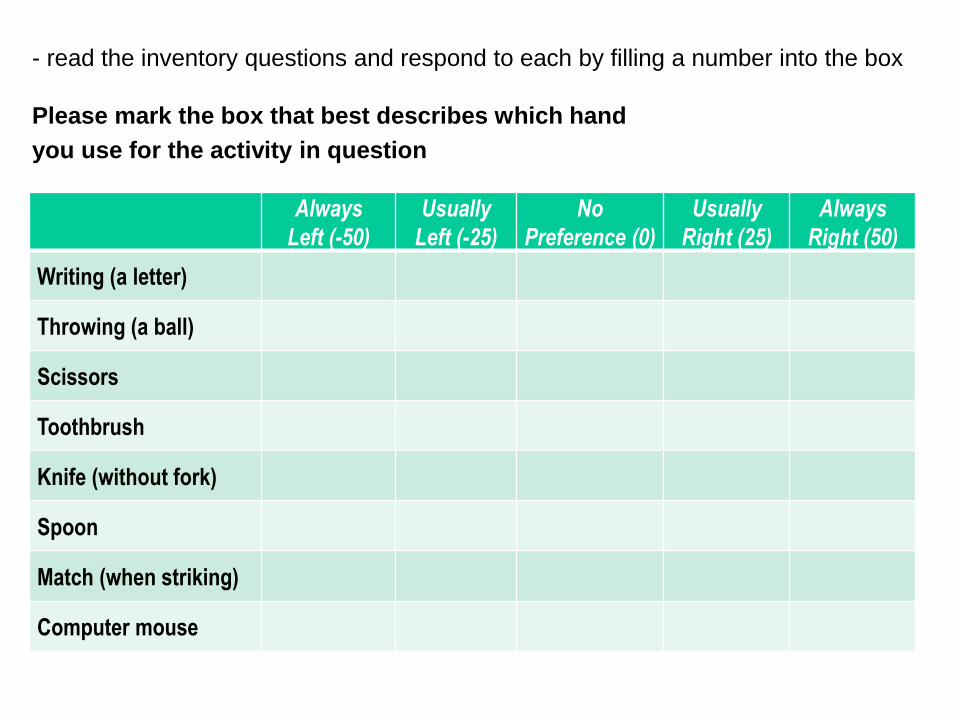
- read the inventory questions and respond to each by filling a number into the box
Please mark the box that best describes which hand
you use for the activity in question
Always
Left (-50)
Usually
Left (-25)
No
Preference (0)
Usually
Right (25)
Always
Right (50)
Writing (a letter)
Throwing (a ball)
Scissors
Toothbrush
Knife (without fork)
Spoon
Match (when striking)
Computer mouse
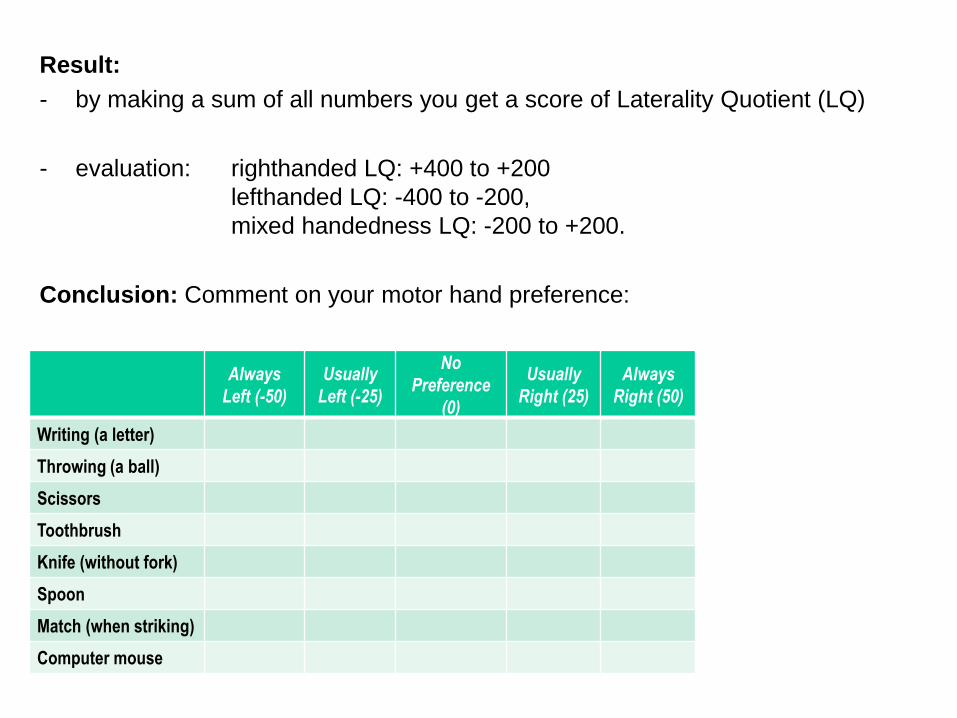
Result:
- by making a sum of all numbers you get a score of Laterality Quotient (LQ)
- evaluation: righthanded LQ: +400 to +200
lefthanded LQ: -400 to -200,
mixed handedness LQ: -200 to +200.
Conclusion: Comment on your motor hand preference:
Always
Left (-50)
Usually
Left (-25)
No
Preference
(0)
Usually
Right (25)
Always
Right (50)
Writing (a letter)
Throwing (a ball)
Scissors
Toothbrush
Knife (without fork)
Spoon
Match (when striking)
Computer mouse