Embed Size (px)
Citation preview
PHYSIOLOGY LECTURE PRESENTATIONS BY - DR SHAHAB PhD, MD
Respiratory System
Physiology
ByDr. SHAHAB
SHAIKHLecture : Clinical Examination of RS•••••••••••••••••••••••••••••
•••••
PhD MD
Physiology lecture presentations by - DR SHAHAB PhD, MD
The Doctor
Physiology lecture presentations by - DR SHAHAB PhD, MD
Respiratory System Physiology
Clinical Examination of RS
Inspection Palpation Percussion Auscultation
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection
• Comfortable at rest . . . . ?• Breathless . . . .?• Cyanosis . . . . .?• Chest wall appearance:• Chest wall movement:• Breathing:• Neck region:
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection• Chest wall appearance:
– a. Shape• Normally Ellipsoid• Barrel Chest - Hyperexpansion (A-P diameter
increased) eg. COPD
– b. Symmetry– c. Scars / Lesions– d. Deformity:
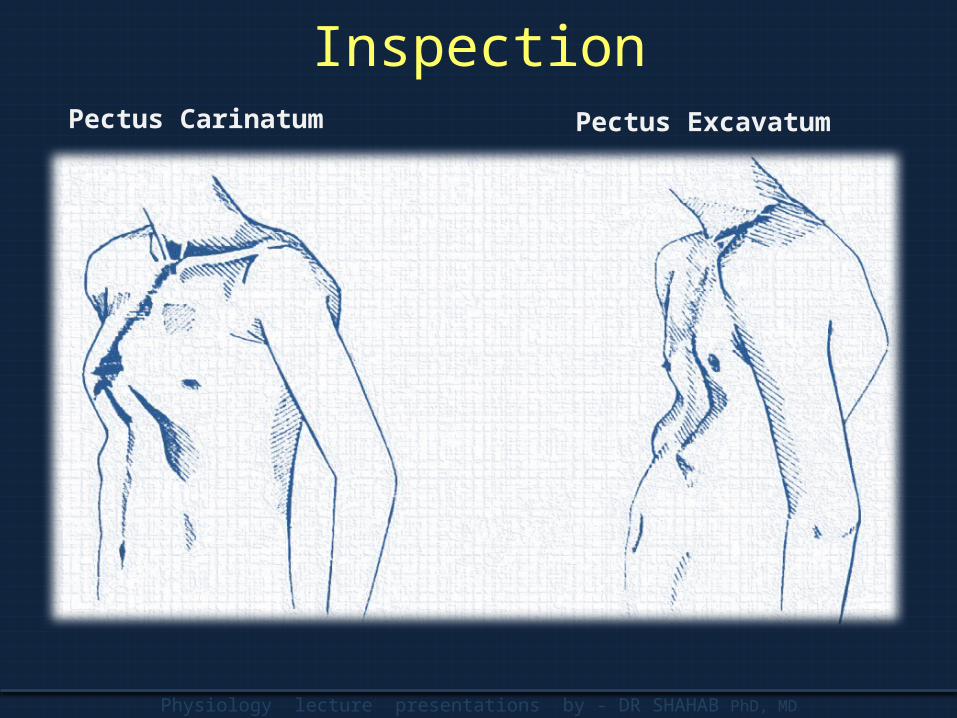
• Pectus carinatum –sternum bulges forwards (‘pigeon chest deformity’)
• Pectus excavatum –sternum caves inwards (Funnel chest deformity)
Physiology lecture presentations by - DR SHAHAB PhD, MD
InspectionPectus Carinatum Pectus Excavatum
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection
• Chest wall movement:– a. Expansion– b. Symmetry of movement– c. Paradoxical movement:
• Phrenic nerve paralysis • Flail chest
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection
• Breathing:– Respiratory rate:– Tachypnoea is a respiratory rate > 16/min and is
caused by increased ventilatory drive as in fever, asthma and COPD, or reduced ventilatory capacity as in pneumonia, pulmonary oedema and interstitial lung disease.
– A slow respiratory rate can occur in association with opioid toxicity, hypothyroidism, raised intracranial pressure, hypothalamic lesions, and hypercapnia.
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection
• Breathing:– Respiratory depth– Respiratory Rhythm– Type of respiration:
• Normal• Kussamul: Hyperventilation with deep, sighing
respirations (Küssmaul respiration) is a response to the reduced arterial pH in metabolic acidosis. This can occur in acute renal failure, lactic acidosis, diabetic ketoacidosis and in salicylate and methanol poisoning. The patients appear to have 'air hunger'.
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection• Breathing:
• Cheyne stroke: Cheyne-Stokes breathing, or periodic respiration, is characterized by a period of increasing rate and depth of breathing followed by diminishing respiratory effort and rate, usually ending in a period of apnoea or hypopnoea. The cycle then repeats. It is seen most frequently in stroke involving the brain stem, and in severe cardiac failure. However, it may be normal during sleep in the elderly.
– Use of accessory muscles: These include the sternocleidomastoids, platysma and pectoral muscles. Use of accessory muscles is characteristic of patients with COPD who have hyperinflated lungs.
Physiology lecture presentations by - DR SHAHAB PhD, MD
Inspection
• Neck region:– Position of Trachea
• Causes of tracheal deviation– Towards the side of the lung lesion
» Upper lobe or lung collapse » Upper lobe fibrosis » Pneumonectomy
– Away from the side of the lung lesion» Tension pneumothorax » Massive pleural effusion
– Supraclavicular fossae– Visible pulsation, JVP– Lymph nodes
Physiology lecture presentations by - DR SHAHAB PhD, MD
Palpation
• Tenderness• Temperature• Position of Trachea:• Chest Expansion:• Tactile Vocal Fremitus:• Apex beat localization:
Physiology lecture presentations by - DR SHAHAB PhD, MD
PalpationPosition of Trachea: Use one or two fingers in supra sternal notch !
Physiology lecture presentations by - DR SHAHAB PhD, MD
Palpation
• Chest Expansion:– Both sides of the thorax should expand equally
during tidal and maximal inspiration.– Reduced expansion on one side indicates
abnormality on that side, e.g. pleural effusion, lung or lobar collapse, pneumothorax and unilateral fibrosis.
– Bilateral reduction in chest wall movement is common in advanced COPD and diffuse pulmonary fibrosis
Physiology lecture presentations by - DR SHAHAB PhD, MD
Palpation• Tactile Vocal Fremitus:
– Tactile vocal fremitus is the transmission of voice sounds from central airways to the chest wall. It is increased by solid lung, provided the airways supplying that part of the lung are patent.
– It is important to decide whether areas found to be dull to percussion show increased tactile vocal fremitus (suggesting consolidation or fibrosis) or reduced tactile vocal fremitus (suggesting fluid or collapse)
– During assessment of tactile vocal fremitus, it is conventional to ask the patient to say 'ninety -nine'. In other languages, other numbers or phrases are used. (The intention is to produce a nasal 'oi' sound).
Physiology lecture presentations by - DR SHAHAB PhD, MD
Palpation• Apex beat localization:
– Deviation of the cardiac apex beat indicates shift of the lower mediastinum.
– Displacement of the cardiac impulse without deviation of the trachea is usually due to left ventricular enlargement but can also occur in scoliosis, kyphoscoliosis, or severe pectus excavatum.
– The cardiac apex beat may be difficult to localize in obesity, pericardial effusion, poor left ventricular function or patients with lung hyperinflation as in COPD.
Physiology lecture presentations by - DR SHAHAB PhD, MD
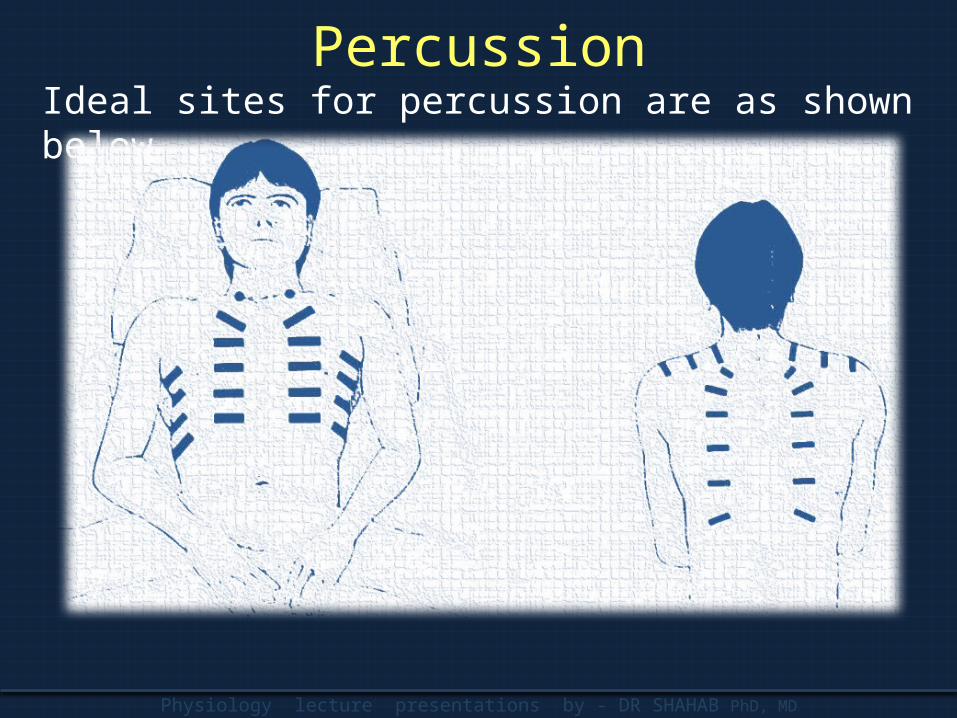
PercussionIdeal sites for percussion are as shown below
Physiology lecture presentations by - DR SHAHAB PhD, MD
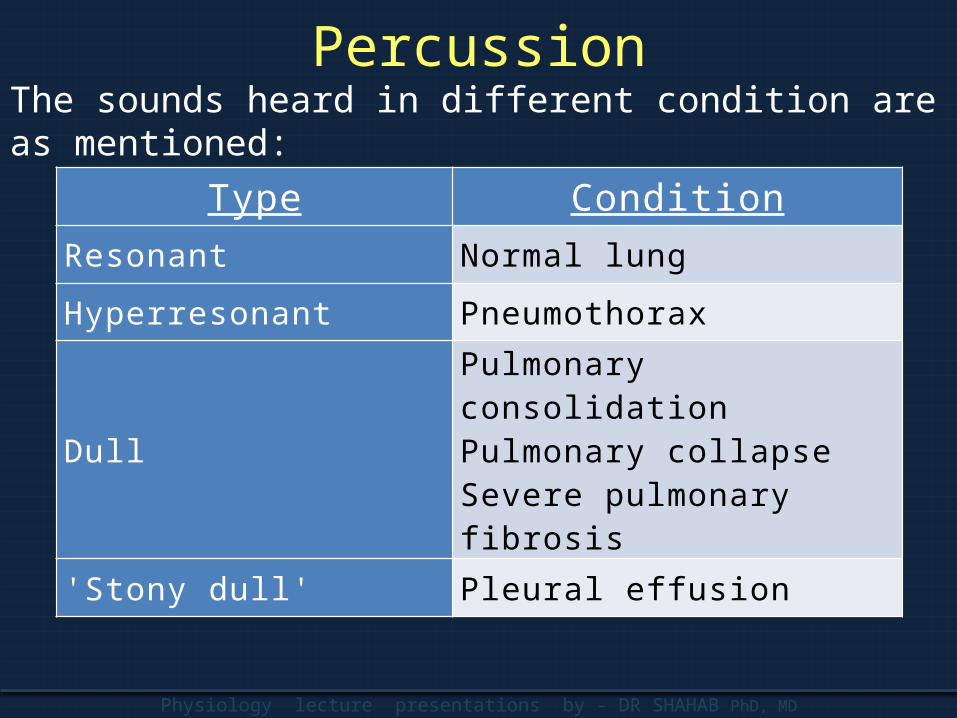
PercussionThe sounds heard in different condition are as mentioned:
Type ConditionResonant Normal lung
Hyperresonant Pneumothorax
DullPulmonary consolidationPulmonary collapseSevere pulmonary fibrosis
'Stony dull' Pleural eff usion
Physiology lecture presentations by - DR SHAHAB PhD, MD
Auscultation• The stethoscope was invented by a French
physician, Laennec, in 1819.• Auscultate both sides alternately, comparing
findings over a large number of equivalent positions to ensure that localized abnormalities are not missed.
Physiology lecture presentations by - DR SHAHAB PhD, MD
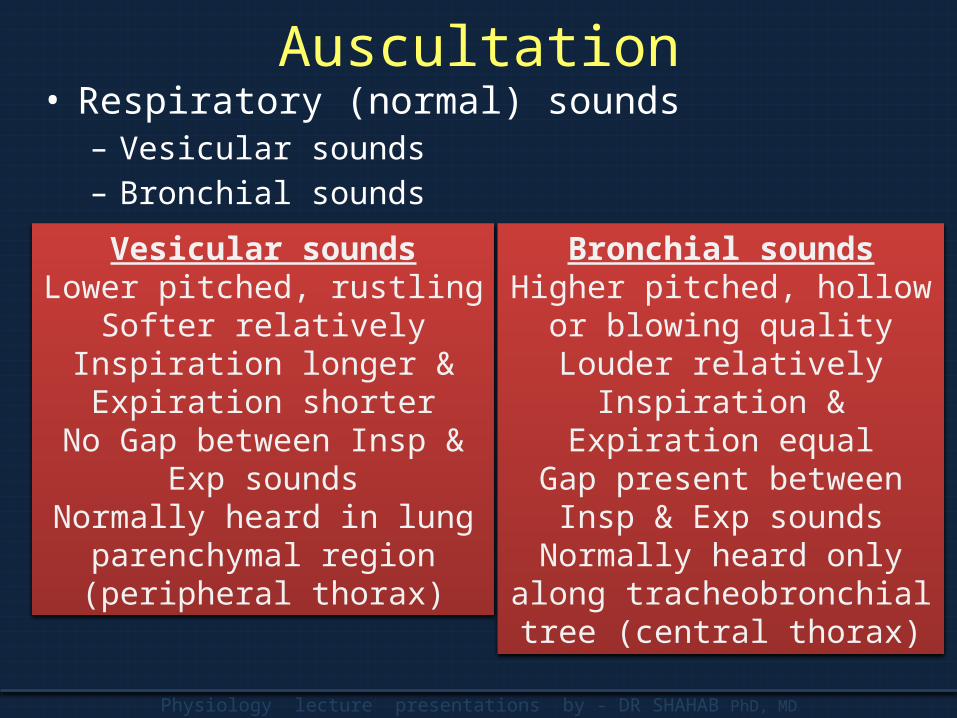
Auscultation• Respiratory (normal) sounds
– Vesicular sounds– Bronchial sounds
Vesicular soundsLower pitched, rustling
Softer relativelyInspiration longer & Expiration
shorterNo Gap between Insp & Exp
soundsNormally heard in lung
parenchymal region (peripheral thorax)
Bronchial soundsHigher pitched, hollow or
blowing qualityLouder relatively
Inspiration & Expiration equalGap present between Insp &
Exp soundsNormally heard only along
tracheobronchial tree (central thorax)
Physiology lecture presentations by - DR SHAHAB PhD, MD
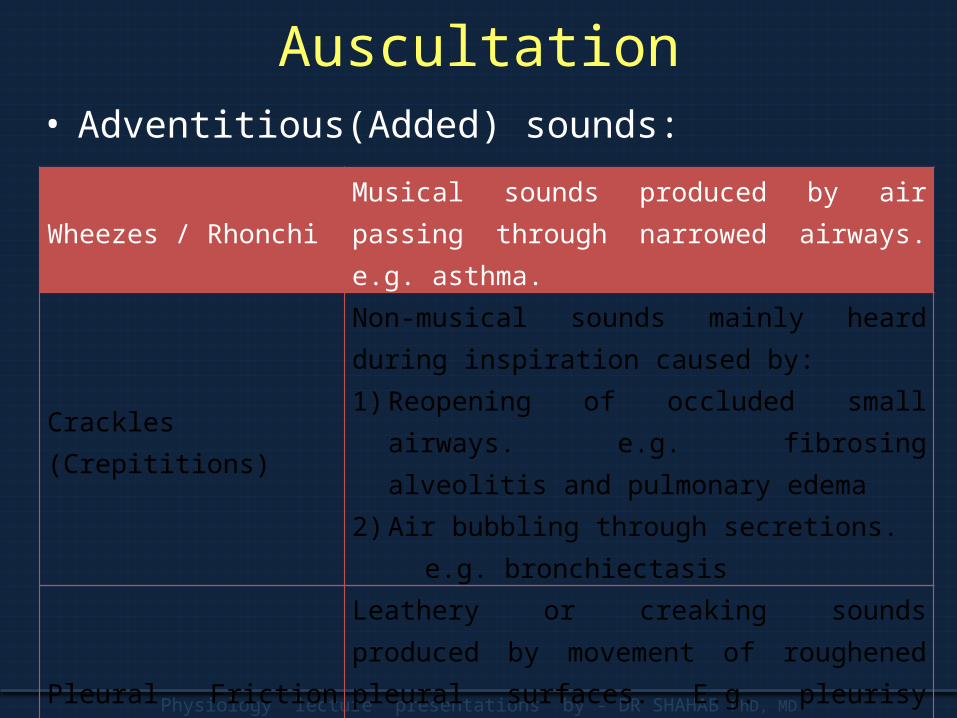
Auscultation• Adventitious(Added) sounds:
Wheezes / Rhonchi Musical sounds produced by air passing through narrowed airways. e.g. asthma.
Crackles (Crepititions)
Non-musical sounds mainly heard during inspiration caused by: 1) Reopening of occluded small airways. e.g.
fibrosing alveolitis and pulmonary edema2) Air bubbling through secretions.
e.g. bronchiectasis
Pleural Friction rub
Leathery or creaking sounds produced by movement of roughened pleural surfaces. E.g. pleurisy caused by pneumonia, pulmonary infarction. Usually associated with pleural pain.
Physiology lecture presentations by - DR SHAHAB PhD, MD
Auscultation• vocal resonance :
– assess vocal resonance by asking the patient to say 'one, one, one'. In the normal lung a whispered note will not be heard but over consolidated lung, as in pneumonia, the sound is transmitted producing 'whispering pectoriloquy'.
Physiology lecture presentations by - DR SHAHAB PhD, MD
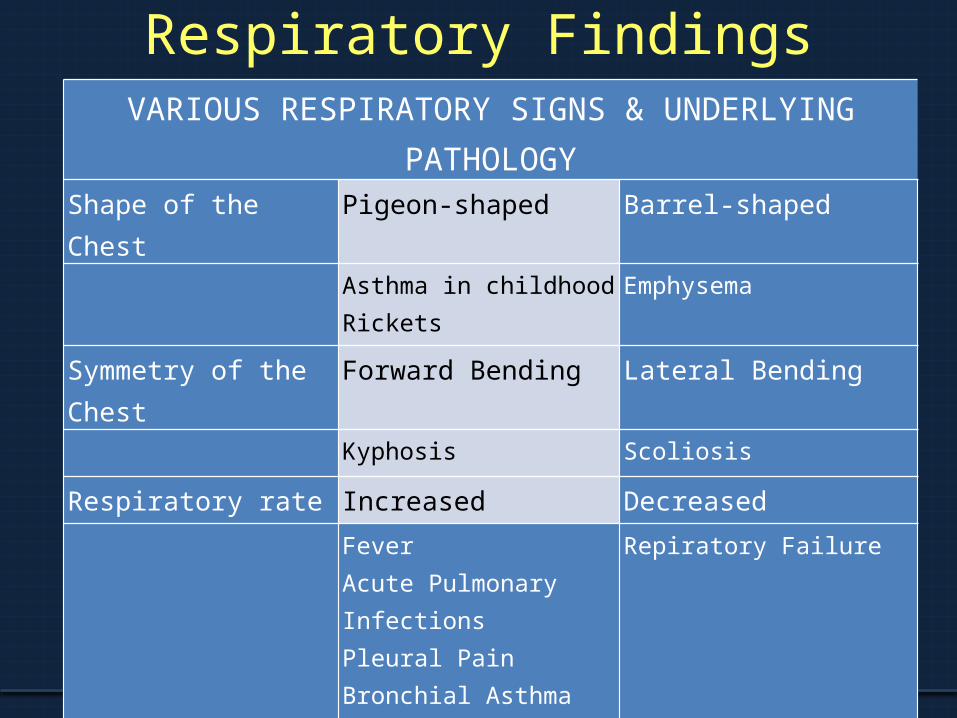
Respiratory FindingsVARIOUS RESPIRATORY SIGNS & UNDERLYING PATHOLOGY
Shape of the Chest Pigeon-shaped Barrel-shaped
Asthma in childhoodRickets
Emphysema
Symmetry of the Chest Forward Bending Lateral Bending
Kyphosis Scoliosis
Respiratory rate Increased Decreased
FeverAcute Pulmonary InfectionsPleural PainBronchial AsthmaPulmonary Edema
Repiratory Failure
Physiology lecture presentations by - DR SHAHAB PhD, MD
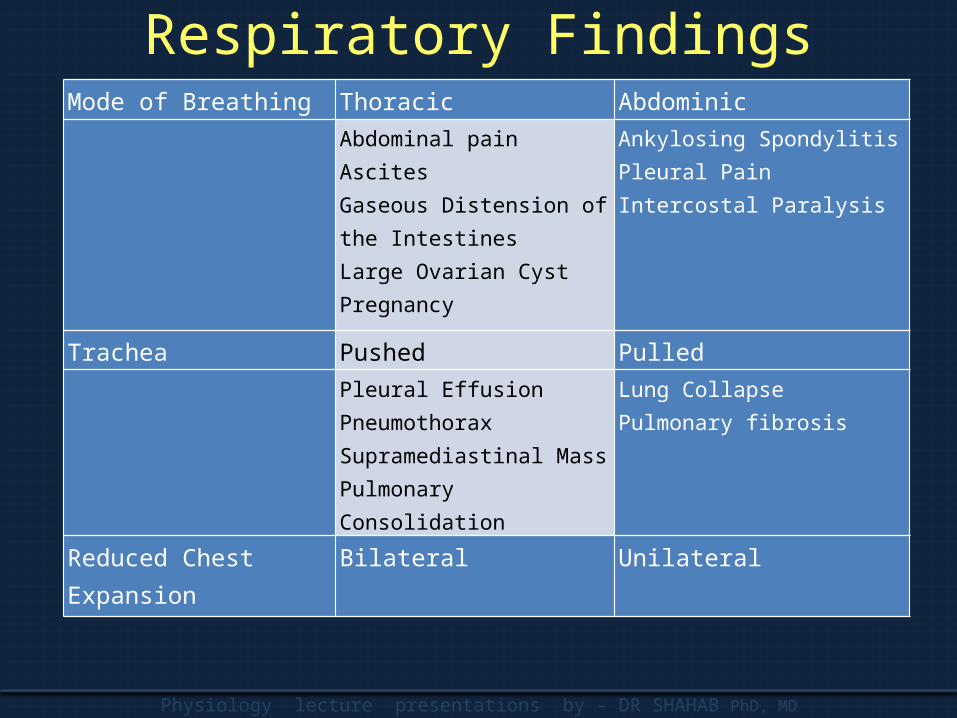
Respiratory FindingsMode of Breathing Thoracic Abdominic
Abdominal painAscitesGaseous Distension of the IntestinesLarge Ovarian CystPregnancy
Ankylosing SpondylitisPleural PainIntercostal Paralysis
Trachea Pushed Pulled
Pleural EffusionPneumothoraxSupramediastinal MassPulmonary Consolidation
Lung CollapsePulmonary fibrosis
Reduced Chest Expansion Bilateral Unilateral
Physiology lecture presentations by - DR SHAHAB PhD, MD
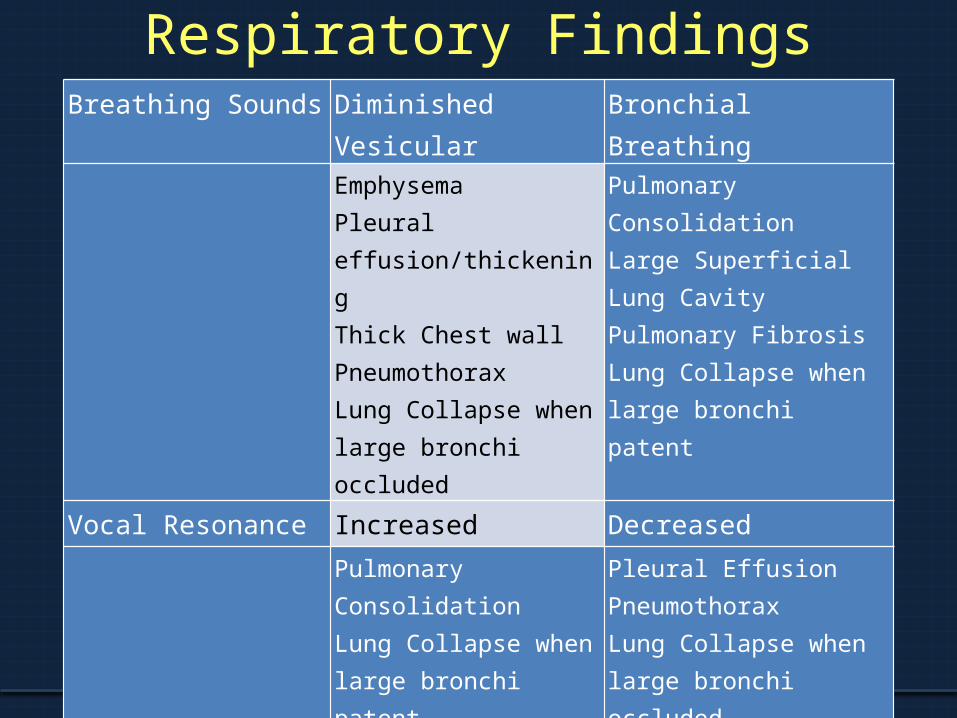
Respiratory FindingsBreathing Sounds Diminished Vesicular Bronchial Breathing
EmphysemaPleural effusion/thickeningThick Chest wallPneumothoraxLung Collapse when large bronchi occluded
Pulmonary ConsolidationLarge Superficial Lung CavityPulmonary FibrosisLung Collapse when large bronchi patent
Vocal Resonance Increased Decreased
Pulmonary ConsolidationLung Collapse when large bronchi patent
Pleural EffusionPneumothoraxLung Collapse when large bronchi occluded
PHYSIOLOGY LECTURE PRESENTATIONS BY - DR SHAHAB PhD, MD
Thank You