Embed Size (px)
Citation preview

The Journal of Clinical InvestigationVol. 46, No. 10, 1967
Physiologic Studies of the Pulmonary Capillary Bed afterBarium Sulfate Embolization *
WALTER J. DALY AND JOHN A. WALDHAUSEN(From the Departments of Medicine and Surgery and the Heart Research Center, Indiana
University School of Medicine, Indianapolis, Indiana)
Abstract. 22 anesthetized dogs were given a barium sulfate suspension in-travenously in a dose sufficient to double mean pulmonary artery pressure.10 sec breath-holding carbon monoxide diffusing capacity (DLCO10) was mea-sured before and after this standard embolization in each dog. No post-em-bolic decrease in DLcoio was observed. In the study of this apparent paradox,it was found that the potential for further increase in DLC010 during exerciseremained after embolization. During rest prolongation of breath holding to60 sec decreased CO absorption significantly more in the embolized than in thenonembolized dogs. While DLCO10 was not affected by standard barium em-bolization, oxygen diffusing capacity was clearly decreased. The bronchialcollateral circulation did not participate in preventing a DLCOio decrease afterembolization since surgical interruption of the bronchial circulation did notalter the response to barium. Microscopic examination of lung sections takenafter standard embolization showed plugging of precapillary vessels in the4050-S range. These studies suggest that acute precapillary embolic obstruc-tion of vessels of this size interferes remarkably little with CO absorption overshort periods of time, probably because of continued CO absorption in por-tions of the capillary net distal to the sites of impaction. The remarkableanastomotic nature of this capillary network with multiple sources of accesspossibly provides the anatomic basis for this observation. This study dem-onstrates a clear dissociation between acute changes in pulmonary vascularresistance and DLco10-both during rest and exercise.
Introduction
Carbon monoxide absorption during a briefbreath-holding period as described by Krogh andmodified by Ogilvie, Forster, Blakemore, andMorton (1) has been used as a measure of thediffusing capacity of the lung (Dr.co) and by in-
* Received for publication 18 April 1967 and in re-vised form 5 July 1967.Reported in part at the 1966 meeting of the American
Society for Clinical Investigation, Atlantic City, N. J.This study was supported in part by research grants
H-6228, H-9243, and H-4080 from the National HeartInstitute, U. S. Public Health Service and in part by theIndiana Heart Association.Address requests for reprints to Dr. Walter J. Daly,
Department of Medicine, Indiana University MedicalCenter, 1100 W. Michigan Street, Indianapolis, Ind.46207.
ference as an index of the functional behavior ofthe pulmonary capillary bed in normal and abnor-mal situations (2, 3). The available evidencesuggests that naturally occurring diseases whichcause obliteration or obstruction of the pulmonarymicrocirculation decrease diffusing capacity (4-8),whereas acute vascular obstruction may occur withlittle or no change in Dr.co (9, 10). This studywas designed to evaluate the effects of acutelyproduced precapillary microobstruction on changesin the pulmonary capillary bed as reflected inchanges in DLcO.
Methods
22 dogs with weights ranging between 16 and 26 kgwere anesthetized intramuscularly with 2-3 mg of mor-phine per kg followed 30-45 min later by 14-18 mg of
1617

WALTER J. DALY AND JOHN A. WALDHAUSEN
pentobarbital per kg given intravenously. The animalswere ventilated with a cuffed endotracheal tube and aconstant volume respirator. End tidal C02 concentrationwas recorded continuously with an infrared C02 analyzer.Respiratory volume and frequency were regulated tomaintain end tidal C02 concentration between 5 and 5.5%o.Catheters were placed in the main pulmonary artery, pul-monary "capillary wedge" position and the central aortausing fluoroscopic control. In each case pressures wereaccepted as "wedged" only if they were obtained withthe catheter in a typically peripheral position relativelyfree of cardiac motion, if the pressure contour was com-patible, and if either arterialized blood could be as-pirated from the catheter or no blood at all was obtain-able. A small polyethylene tube was inserted into aforeleg vein for easy injection of a barium sulfate sus-pension into the peripheral venous circulation.
In each phase of the study 10 sec breath-holding carbonmonoxide diffusing capacity, DLcoio, oxygen consumption,blood oxygen capacity, and intravascular pressures weremeasured. DLcoo was determined by a modified breath-holding technique previously reported from this labora-tory for use in dogs (11). With this system, the diffus-ing mixture, containing 1% neon and 0.5% carbon mon-oxide in air, is inspired from a bag-in-box apparatus, heldand expired by regulating the pressure in an airtightplethysmographic box in which the dog rests on its back.The standard deviation of 10-15 such measurements infive dogs, each used on 4-5 different days, averaged 1.1ml/(min X mm Hg). In each case duplicate DLco,o mea-surements and other measurements appropriate to thephase of the study were made before and just after in-travenous administration of sufficient 30% suspension ofbarium sulfate to produce a doubling of the observedmean pulmonary artery pressure. This degree of em-bolization was used as a "standard embolus" load through-out the study. The actual quantity of barium requiredwas highly variable. 1 ml quantities of the suspension
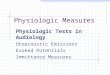
FIG. 1. PHOTOMICROGRAPH OF A SECTION OF LUNG OB-
TAINED FROM A DOG SUBJECTED TO A STANDARD BARIUM EM-
BOLUS STUDY. Two barium filled vessels are included inthe central portion of the field. X 250.
were given at 2-min intervals until the desired doublingof pressure was observed. Intravascular pressures wereintegrated electronically and recorded photographically.Oxygen consumption was determined before and afterbarium embolization from a 3 or 4 min collection of ex-pired gas. The gas volumes were measured in a Tissotspirometer and the expired oxygen concentrations weredetermined with a paramagnetic oxygen analyzer. Bloodoxygen capacity was measured spectrophotometrically(12).Barium sulfate particle size was determined with a
series of standard sieves and microfilters. By weight,0.02%o of samples of barium passed through a standard13.5-15 A filter, 15% through a 37 A filter, and 82%through 105 u filter. Sections of lung were examinedmicroscopically to estimate the site of vascular obstruc-tion. Barium emboli were seen chiefly in arterioles orprecapillaries in the 40-50 A range. No emboli largerthan 75 0 and none smaller than 20 0 were identified(Fig. 1).The project was divided into several phases:(a) In the initial phase of the study, DLco1o, oxygen
consumption, and intravascular pressures were measuredbefore and after the standard barium embolization.
(b) Similar observations were made in three dogs pre-viously prepared by bilateral "hilar stripping" to removethe branchial collateral circulation. In each case theanimal had a staged operation in which one main stembronchus was divided and reanastomosed. The hilarstructures were stripped away, including the pulmonaryarterial and venous adventitia. 3 days later the oppositelung was similarly prepared and 2 days later the animalswere subjected to the barium study. After the experi-ment was terminated, the completeness of the bronchialartery interruption was tested by injection of a greenradiopaque barium gelatin mixture into the dorsal aortaunder a pressure of 200 mm Hg. The lungs were ex-cised and observed for filling of the bronchial collateralcirculation with the green barium mass both grossly andradiographically. In no case was any evidence of residualbronchial circulation detected. This technique had previ-ously been used in this laboratory and shown regularly tooutline the canine bronchial circulation.
(c) In seven dogs at rest the effect of prolongedbreath holding during carbon monoxide absorption wastested. The rate of CO absorption during the standard10 sec breath hold was compared with CO absorption dur-ing a 60 sec breath-holding period both before and sub-sequent to the standard embolization. During the pro-longed breath-holding period the dogs were carefullyobserved for respiratory effort. The combination of deepinspiration and anesthesia was sufficient to suppress therespiratory drive for this length of time.
(d) In five dogs the effect of standard barium embo-lization on DLCo1o was compared with its effect onDLO2. Oxygen diffusing capacity was determined by amodification of the method described by Bartels and co-workers (13). In each instance the animal breathed 40%ooxygen for 15 min and 10% oxygen for 15 min. Theexpirate was collected over the last 5 min of each period.
1618

PHYSIOLOGIC STUDIES OF THE PULMONARY CAPILLARY BED AFTER MICROEMBOLI 1619
TABLE I
Effects of standard barium sulfate embolization
DLCO1o Pulmonary artery 02 capacity
mean pressureDog Before After Before After Before After
ml/(min X mg Hg) mm Hg mi/100 ml7-21 11.1 14.6 12 426-23 14.3 15.8 19 326-16 8.1 8.4 18 307-23 8.3 10.4 11 297-22 8.8 11.8 11 387-20 17.4 18.3 18 377-2 10.9 13.6 15 438-23 8.1 11.6 14 318-24 7.2 10.2 12 308-25 10.4 12.8 17 3810-18 9.6 11.5 16 43 19.73 24.7210-15 11.8 11.0 14 39 15.34 17.159-13 11.2 13.1 14 269-15 10.3 11.6 12 30 16.76 21.759-16 11.3 10.2 8 24 19.40 20.8010-19 19.6 19.4 16 46 18.40 22.4010-20 11.5 15.3 16 57 14.00 20.30
Mean 11.2 12.9 14 36 17.27 21.19SD 3.3 3.0 3 8 2.31 2.51P 0.001 0.001 0.01
In this phase of the study the concentration of oxygenand carbon dioxide inspired and the concentrations of theexpired samples were determined by the Micro-Scho-lander technique. Duplicate analyses of C02 were re-quired to check within 0.03 ml/100 ml and oxygen within0.04 ml/100 ml. Blood oxygen content and capacity weredetermined spectrophotometrically (12). In our labora-tory, this method is sufficiently accurate to duplicatevalues within 0.06 + 0.06 volumes/100 ml. Blood pH,Pco2 and Po, were determined with appropriate electrodes.Actual mixed venous blood samples were obtained fromthe pulmonary artery catheter. The alveolar Po2 wascalculated from the usual alveolar air equation, assum-ing ideal alveolar PcO2 = arterial Pco2. The quantity ofveno-arterial shunting was estimated during 40% 02breathing, assuming equilibrium of alveolar and end-capillary Po2. The diffusion component of the alveolar-arterial Po2 difference was determined during 10%o oxygenbreathing, assuming no change in veno-arterial shunting.Mean alveolar-capillary Po2 gradient was estimatedwith the Bohr integration expressed in Thews' nomogram(14). With this method oxygen diffusing capacity wasdetermined and compared with DLco,O both before andafter standard embolization.
(e) Muscular exercise was induced in eight dogs witha modified Kao stimulator (C. B. Branch, Grand Prairie,Tex.) as previously described from this laboratory(11). Exercise sufficient to produce a fourfold increasein oxygen consumption was induced. DLco,, was deter-mined at rest and during the 4th to 6th min of such ex-ercise both before and after standard barium embolization.At the end of each experiment the animal was sac-
rificed after having been anaesthetized intravenously withpentobarbital.
Paired comparison t tests were done in all cases withthe control observation from each animal used for com-parison with its experimental observation.
Results
(a) After barium sulfate embolization in aquantity sufficient to double pulmonary arterypressure, DLCO10 increased from 11.2 ± 3.3 to12.9 ± 2.9 ml/(min X mm Hg) (P = 0.001). Ac-tually the mean pulmonary artery pressure in-creased from 14 to 36 mm Hg. Blood oxygencapacity increased from 17.27 + 2.31 to 21.19 +2.51 ml/100 ml blood (P = 0.01) (Table I).Such increases in blood oxygen capacity occur indogs subjected to a variety of stresses and can berelated to contraction of the splenic reservoir(15). The magnitude of the increase in DLo10observed under these circumstances is appropriatefor the observed increase in hemoglobin capacityavailable for carbon monoxide absorption. (Thiswas established from the relationship, 1/DL =1/DM + 1/VcO, standard values for Vc and DMpreviously established for dogs in this laboratoryand appropriate corrections for 0 based on theobserved change in oxygen capacity.)

WALTER J. DALY AND JOHN A. WALDHAUSEN
FAcoOlog -
FACO
0.5
0.
10 SEC 60 SEC
FIG. 2. DISAPPEARANCE OF CARBON MONOXIDE DURING
BREATH HOLDING BEFORE AND AFTER STANDARD BARIUM
SULFATE EMBOLIZATION. Loge (FAcos/FAcoT) = the na-
tural log of the ratio of initial alveolar CO concentrationto final CO concentration. Solid bars indicate mean valuesof resting seven dogs before embolization and hatched barsindicate mean value of seven dogs after embolization.Brackets indicate standard error of the mean.
(b) In the three dogs that had bronchial arterystripping, DLCOoio averaged 11.5 ml/(min x mmHg) before and 11.4 ml/(min x mm Hg) afterstandard embolization.
(c) Fig. 2 compares the loge ratios of initialCO concentration over final CO concentration,loge (FACOO/FACO T), before and after emboli dur-ing 10- and 60-sec breath holds. Before emboli-zation prolonging breath holding from 10 to 60 sec
increased loge (FACOo/FACOT) from 0.618 0.017to 2.14 + 0.080. After embolization, while the
pulmonary artery pressure was increased from13.7 2.9 to 37.9 11.9 mm Hg, increasing thebreath-holding period from 10 to 60 sec increasedloge (FACOO/FACOT) from 0.685 + 0.015 to 1.59+ 0.080. The difference between the loge ratiosat 60 sec was significant at the P = 0.005 level.
(d) In each of the five dogs in which the effectof standard embolization on DLO2 was comparedwith its effect on DLCO10, oxygen diffusing capac-
ity was profoundly decreased by such emboliza-tion whereas DLCOSO remained unaffected. TableII shows the effects of standard barium emboliza-tion on DLO2, DLCO10, cardiac output, pulmonaryartery pressure, pulmonary wedge pressure, andcalculated pulmonary vascular resistance. Em-bolization decreased DLO, from 13.4 + 4.1 ml02/(min X mm Hg) to 6.2 + 3.4 ml 0,/(min X
mm Hg) (P = 0.01), whereas DLCOio, cardiacoutput, and wedge pressure were not appreciablychanged. Pulmonary artery pressure increasedfrom 15 + 2 to 42 + 4 mm Hg and calculatedpulmonary vascular resistance from 3.2 1.8 to15.7 + 7.8 (mm Hg X min) /liter.
(e) During muscular exercise sufficient to in-crease the average oxygen consumption from 111+ 25 to 610 183 ml/min, DLCo10 increased from10.9 3.5 to 22.5 + 10.8 ml/(min X mm Hg),while pulmonary artery pressure increased from16 3 to 31 12 mm Hg. After standard em-
bolization, with a resting pulmonary artery mean
pressure of 35 + 5 mm Hg, similar exerciseincreased pulmonary artery pressure to 50 16ml/min and increased DLCoio from 13.2 + 3.2 to20.4 6.6 ml/(min X mm Hg) (Table III).
BLE II
Comparison of effects of microemboli on DLO2 and DLcojo
Mean PA Mean wedge Pulmonary vascularDLO2 DLCOIO Cardiac output pressure pressure resistance
Dog Before After Before After Before After Before After Before After Before After
ml/(min X mm Hg) ml/(min X mm Hg) liters/mix mm Hg mm Hg (mm Hg X min)liter
3-21 12.9 4.8 8.7 8.8 3.25 2.26 12 37 7 8 1.5 12.83-7 9.9 7.8 12.2 12.1 3.16 3.23 15 48 5 5 2.5 13.32-28 13.5 4.9 10.3 10.8 1.55 1.88 15 42 6 5 5.8 19.94-4 20.4 11.1 15.6 17.2 4.40 5.26 17 41 9 10 1.8 5.93-28 10.5 2.2 10.0 13.2 2.52 1.25 16 40 5 7 4.3 26.4
Mean 13.4 6.2 11.4 12.4 2.98 2.78 15 42 6 7 3.2 15.7SD 4.2 3.4 2.7 3.1 1.05 1.56 2 4 2 2 1.8 7.8P 0.01 NS NS 0.001 NS 0.025
NS, not significant.
1620

PHYSIOLOGIC STUDIES OF THE PULMONARY CAPILLARY BED AFTER MICROEMBOLI 1621
TABLE III
Effects of microembolization on DLcO1, responses to exercise
DLCO1O 02 consumption Mean PA pressure Mean wedge pressure
Dog R EX BaR BaEx R Ex BaR BaEx R Ex BaR BaEx R Ex BaRBaEx
ml/ (min X mm Hg) ml/min mm Hg mm Hg7-21 11.1 24.4 14.6 22.0 91 642 107 582 12 28 42 58 5 6 4 36-23 14.3 17.6 15.8 24.8 123 328 100 317 19 27 32 55 3 4 5 66-16 8.1 15.2 8.4 16.5 18 22 30 40 4 3 5 47-20 17.4 43.7 18.3 33.6 132 818 185 838 18 40 37 58 6 5 5 47-2 10.9 32.9 13.6 18.7 79 860 135 528 15 54 43 82 5 4 4 58-23 8.1 13.4 11.6 13.6 150 532 160 540 14 17 31 35 3 4 3 68-24 7.2 13.1 10.2 13.9 93 554 90 278 12 34 30 38 4 - 4 78-25 10.4 19.8 12.8 20.0 108 535 132 458 17 25 38 33 6 6 4 4
Mean 10.9 22.5 13.2 20.4 111 610 130 506 16 31 35 50 4 4 4 5SD 3.5 10.8 3.2 6.6 25 183 34 186 3 12 5 17 1 1 1 1P NS NS 0.001 NS
R, rest; Ex, exercise; BaR, rest after barium sulfate; BaEx, exercise after barium sulfate; NS, not significant.
The two resting DLco10 averages and two exerciseDLco10 averages were not statistically different norwas the exercise DLCO10 increment before andafter barium statistically different. Pulmonarycapillary wedge pressures were not affected byexercise either before or after embolization.
Discussion
A variety of studies have examined the clinicalusefulness of DL0O measurements. In generalthose conditions characterized by obstruction andobliteration of the pulmonary capillary bed havebeen associated with decreases in DLCo10 (4-8).An attempt was made to simulate these conditionsacutely by producing precapillary pulmonary vas-cular obstruction sufficient to induce meaningfulincreases in pulmonary vascular resistance. Bar-ium sulfate suspension was used in this study andhas been used by other investigators (16, 17).Knisely, Wallace, Mahaley, and Satterwhite ob-served the lung directly during embolization witha variety of particle sizes and materials, includingbarium sulfate. They observed that most arti-ficial embolic materials were heavily coated withthrombotic material by the time they lodged inthe pulmonary vessels so that their original sizecould not be the sole determinant of the size ofthe vessel embolized (16). They also observedthat arteriolar and precapillary emboli did notalways impede flow or empty vessels distal to theobstruction because of extensive collateral circu-lation through the capillary network. Pump has
observed that obstruction at or distal to arteriolesof the third division (his estimate, 119 t diameter)would have little effect on the distal vascular bedbecause of the continuity and numerous anasto-moses between different regions of the capillarynet (18). Knisely and coworkers' observationsalso demonstrated that fine particles such as bar-ium sulfate can pass completely through the lung.Whether a portion of the administered bariumsulfate passes through the lung is not critical tothe present study, since the dose of embolic mate-rial used was determined solely by the pressureeffect observed in each individual animal. Micro-scopic examination of the sections of lung obtainedafter this standard embolization showed no evi-dence of capillary obstruction and rare obstructionof vessels larger than 60 /, but did show extensiveplugging at the 40-50 /z level. Barium plugs thatdid not completely fill the lumen of the affectedvessel were not identified.The results of the present study clearly demon-
strate a dissociation between acute increases inpulmonary vascular resistance induced by micro-embolization and DLCOio. This dissociation isconsistent with the observations of Williams andSobol who used 60-u glass beads and found noappreciable change in steady-state D..co whenpulmonary artery pressure was increased by mi-croembolization (10). Two alternative explana-tions are available for the somewhat paradoxicalpreservation of a reasonably normal DLCO10.Either the unaffected capillary bed enlarged andbecame more active in CO absorption, or the

WALTER J. DALY AND JOHN A. WALDHAUSEN
-capillary bed distal to the emboli remained activein CO absorption, or both. Mechanisms are avail-able to initiate expansion of the unembolized capil-lary bed. As during normal exercise, the in-creased pulmonary artery pressure after embolimight open portions of the bed not available toCO during rest, thus preventing a DLCo decreaseas the pulmonary vascular resistance is increasedby barium embolization. Preservation of the capa-bility to increase DLCOio further during muscularexercise suggests that the unchanged postembolicDLCO0, is not solely a utilization of the extensivepulmonary capillary reserve but that the capacityfor still further expansion of the capillary bedremains after this degree of embolization. Yet,increases in pulmonary vascular resistance of thedegree observed suggest obstruction of substan-tially more than 50% of the pulmonary vascularbed (19, 20). Nevertheless, evidence other thancontinued DLCO increases during exercise is re-quired to establish whether CO absorption takesplace in the capillary net distal to sites of ob-struction.
It seems well established that breath-holdingcarbon monoxide absorption over short periods oftime is independent of blood flow if pulmonaryvascular pressures do not change (21). Conse-quently one may postulate continued CO absorp-tion during a 10 sec breath hold in portions of thepulmonary capillary net that remain filled withblood after barium embolization. Both Kniselyand coworkers (16) and Staub (22), using differ-ent techniques, have observed the continued pres-ence of red cells in pulmonary capillaries afterflow has stopped, and Staub has pointed out thepossibility of continued CO absorption by thosestagnant red cells, causing paradoxically highDLCO and gross dissociation of DLo0 and pulmo-nary capillary flow. If this were indeed the reasonfor the absence of decreases in DLCO,0 after micro-embolization, one would expect the rapid build-upof carbon monoxide back pressure resisting dif-fusion in areas of stagnant or sluggish flow distalto microemboli. During more prolonged breathholds, therefore, CO absorption should decreasemore rapidly after emboli. Piiper has examinedthe theoretical and practical implications of un-even distribution of diffusing capacity and itseffects on carbon monoxide absorption duringbreath-holding periods of variable length and has
concluded that the decrease in apparent DLCo asthe duration of breath holding is increased is amanifestation of uneven distribution of diffusingcapacity. The development of focal increases incapillary Pco is a part of such unevenness (23).In this study, when the breath-holding period wasprolonged from 10 to 60 sec, CO absorption diddecrease appreciably more after embolization thanbefore embolization. This observation favors thethesis that after emboli the apparent paradox ofan unaffected DL0O10 may indeed depend upon COabsorption in areas of relatively no flow.
Since extremely low partial pressures of COare present in the alveoli and the hemoglobin COcapacity is relatively so great, CO absorption islimited by blood flow only at the lowest flow ratesor after more prolonged exposure with develop-ment of significant capillary Pco. Oxygen ab-sorption on the other hand at ambient Po2 is, ofcourse, flow dependent. In this study it wasshown that embolization with barium, althoughleaving DLCo10 and total blood flow unaffected,did decrease DLO2 profoundly. This again is quitecompatible with the concept that carbon monoxidewas continuing to be absorbed in areas of the pul-monary capillary bed which were filled but verypoorly perfused while DLO, became a much moresensitive index of gross unevenness of flow dis-tribution. In the absence of a decrease in totalblood flow, the decrease in DLO2 after emboliprobably depends upon the development of re-gional variations in capillary transit time withincomplete equilibration of alveolar end capillaryPo2. This mechanism has been examined in detailby Staub (24). If on the other hand DLCO10were maintained at a relatively normal level afteremboli by utilization of the usually inactive por-tions of the capillary bed, i.e. by opening new areasof the net, capillary transit times and DLO2 shouldhave been relatively unaffected after embolization.This study did not examine exercise DLO2 after em-boli, but prediction based on this thesis requireseven further decrease in DLO2 during exercise.The bronchial circulation did not contribute to
the postembolic normal DLC010 level since the phe-nomenon was not affected after interruption of thebronchial arteries. It is known that bronchialcollateral flow normally increases when pulmonaryartery flow decreases and may participate in gasexchange (25). However, this was not requisite
1622

PHYSIOLOGIC STUDIES OF THE PULMONARY CAPILLARY BED AFTER MICROEMBOLI 1623
for the maintenance of the normal DLco0o afterstandard embolization.
Although the normal increase in breath holdingDLCO during muscular exercise is not totally ex-
plained, the available evidence suggests: (a) thatit is dependent either upon dilation of previouslyfunctioning capillaries or recruitment of ones pre-
viously empty of hemoglobin; (b) that this en-
largement of the effective pulmonary capillary bedis dependent upon the effects of increased pressure
within the pulmonary capillary bed. The resultsof the present study indicate that precapillary ob-struction to flow may increase vascular resistancebut that the collateral access to the capillary net-work may be adequate to permit a normal DLco.After standard barium emboli, the exercise incre-ment in vascular pressure remains effective inmaking available a larger capillary bed for COabsorption, a much greater absolute pressure beingrequired however.An anatomic basis for the physiologic observa-
tions observed in this study has been demonstratedby numerous investigators who have described theextensive collateral communication within the pul-monary capillary network (16, 18, 22, 26). Thisnetwork is so liberally supplied with collateralsources that arteriolar obstruction at one site mayvery possibly leave the distal pulmonary capillarybed unaffected.
This study then demonstrates: (a) that changesin DLCoo may be dissociated from acute changesin pulmonary vascular resistance induced by a
standardized barium sulfate embolus; (b) that thecontinued CO absorption is not dependent upon
bronchial collateral flow but probably occurs incapillaries distal to the site of obstruction unevenlyperfused but filled through collateral channels. In-creased participation of portions of the capillarynetwork not normally involved in CO absorptionat rest cannot be excluded but does not seem tobe the sole basis for the continued ability to absorbCO at a normal rate over short periods of time.During further increases in pulmonary arterypressure induced by exercise, these collateral chan-nels are sufficient to induce normal increases inexercise DLCO10. In all probability the mainte-nance of the normal DLCOio observed in this studydepends upon the remarkable pulmonary capillaryanastomosing network with access to this networkfrom a variety of sources.
The acute precapillary obstruction produced inthese dogs is different from the naturally occurringdiseases associated with obstruction and oblitera-tion of the microvascular bed because in thesedogs destruction of the distal capillary bed doesnot occur. It is doubtful that an exact humancounterpart for this phenomenon will be discov-ered except rarely in situations where micro-embolization may be encountered.
In their review of 31 patients with "alveolar-capillary block" Marks, Cugell, Cadigan, andGaensler report comparison of DLCOio and DLO2in 14 patients (4). These 14 patients can beclearly divided into two groups, those with com-parable and low DLO2 and DLCOio values and thosewith reasonably normal DLco10 yet low DLO2.Those patients with least reduction of DLCo0i hadthe greatest discrepancy between DLCO10 and DLO2.Those patients were also classed as least severe andin general had evidence of the disease for a shortertime. This consideration of their data in the lightof the present study suggests that this group of pa-tients may indeed represent a clinical setting inwhich there are areas of the capillary bed accessi-ble to CO but with sufficient disparity of capillarytransit times to impair DLO2.
References
1. Ogilvie, C. M., R. E. Forster, W. S. Blakemore, andJ. W. Morton. 1957. A standardized breathholding technique for the clinical measurement ofthe diffusing capacity of the lung for carbonmonoxide. J. Clin. Invest. 36: 1.
2. Daly, W. J., S. T. Giammona, J. C. Ross, and H.Feigenbaum. 1964. Effects of pulmonary vascularcongestion on postural changes in the perfusionand filling of the pulmonary vascular bed. J. Clin.Invest. 43: 68.
3. Steiner, S. H., R. Frayser, and J. C. Ross. 1965.Alterations in pulmonary diffusing capacity andpulmonary capillary blood volume with negativepressure breathing. J. Clin. Invest. 44: 1623.
4. Marks, A., D. W. Cugell, J. B. Cadigan, and E. A.Gaensler. 1957. Clinical determination of thediffusing capacity of the lungs. Comparison ofmethods in normal subj ects and patients with"alveolar-capillary block" syndrome. Am. J. Med.22: 51.
5. Burrows, B., J. E. Kasik, A. H. Niden, and W. R.Barclay. 1961. Clinical usefulness of the single-breath pulmonary diffusing capacity test. Am.Rev. Respirat. Diseases. 84: 789.

WALTER J. DALY AND JOHN A. WALDHAUSEN
6. Burgess, J. H., and J. M. Bishop. 1963. Pulmonarydiffusing capacity and its subdivisions in polycy-themia vera. J. Clin. Invest. 42: 997.
7. Auchincloss, J. H., Jr., and R. Gilbert. 1964. Single-breath diffusing capacity as an aid in evaluationand prognosis of cardiopulmonary disease. Am.Rev. Respirat. Diseases. 90: 28.
8. Sackner, M. A., N. Akgun, P. Kimbel, and D. H.Lewis. 1964. The pathophysiology of sclero-derma involving the heart and respiratory system.Ann. Internal Med. 60: 611.
9. Colp, C. R., and M. H. Williams, Jr. 1962. Pul-monary function following pulmonary embolization.Am. Rev. Respirat. Diseases. 85: 799.
10. Williams, M. H., Jr., and B. J. Sobol. 1963. Effectsof a systemic A-V fistula and of pulmonary em-bolization on diffusing capacity. J. Appl. Physiol.18: 553.
11. Brashear, R. E., J. C. Ross, and W. J. Daly. 1966.Pulmonary diffusion and capillary blood volumein dogs at rest and with exercise. J. Appl. Physiol.21: 516.
12. Hickam, J. B., and R. Frayser. 1949. Spectropho-tometric determination of blood oxygen. J. Biol.Chem. 1M0: 457.
13. Bartels, H., R. Beer, E. Fleischer, H. J. Hoffheinz,J. Krall, G. Rodewald, J. Wenner, and I. Witt.1955. Bestimmung von Kurzschlussdurchblutungund Diffusionskapazitit der Lung bei Gesundenund Lungenkranken. Pfluegers Arch. Ges. Physiol.261: 99.
14. Thews, G. 1959. Ein Nomogramm zur einfachenBestimmung des 02-Diffusionfaktors (02-Diffu-sionskapazitit) der Lunge. Pflugers Arch. Ges.Physiol. 268: 281.
15. Cruickshank, E. W. H. 1926. Of the output ofhaemoglobin and blood by the spleen. J. Physiol.(London). 61: 455.
16. Knisely, W. H., J. M. Wallace, M. S. Mahaley, Jr.,and W. M. Satterwhite, Jr. 1957. Evidence, in-
cluding in vivo observations, suggesting mechani-cal blockage rather than reflex vasospasm as thecause of death in pulmonary embolization. Am.Heart J. 54: 483.
17. Halmagyi, D. F. J., and H. J. H. Colebatch. 1961.Cardiorespiratory effects of experimental lungembolism. J. Clin. Invest. 40: 1785.
18. Pump, K. K. 1966. The circulation in the periph-eral parts of the human lung. Diseases Chest. 49:119.
19. Cournand, A., R. L. Riley, A. Himmelstein, and R.Austrian. 1950. Pulmonary circulation and alveo-lar ventilation-perfusion relationships after pneu-monectomy. J. Thoracic. Cardiovascular Surg. 19:80.
20. Lategola, M. T. 1958. Pressure-flow relationshipsin the dog lung during acute, subtotal pulmonaryvascular occlusion. Am. J. Physiol. 192: 613.
21. Lawson, W. H., Jr., H. N. Duke, R. W. Hyde, andR. E. Forster. 1964. Relationship of pulmonaryarterial and venous pressure to diffusing capacity.J. Appl. Physiol. 19: 381.
22. Staub, N. C. 1963. The interdependence of pul-monary structure and function. Anesthesiology. 24:831.
23. Piiper, J., and R. S. Sikand. 1966. Determination ofDeo by the single breath method in inhomogeneouslungs: theory. Respirat. Physiol. 1: 75.
24. Staub, N. C. 1963. Alveolar-arterial oxygen tensiongradient due to diffusion. J. Appl. Physiol. 18:673.
25. Mandelbaum, I., and S. T. Giammona. 1964. Bron-chial circulation during cardiopulmonary bypass.Ann. Surg. 164: 985.
26. Irwin, J. W., W. S. Burrage, C. E. Aimar, and R. W.Chesnut, Jr. 1954. Microscopical observationsof the pulmonary arterioles, capillaries, and venulesof living guinea pigs and rabbits. Anat. Record.119: 391.
1624

![Index [ftp.feq.ufu.br]ftp.feq.ufu.br/Luis_Claudio/Segurança/Safety/Double/fire_handbook... · Backdraft Explosion 174 Barium 216 Barium Carbonate 300 Barium Chlorate 300 Barium Nitrate](https://img.pdfslide.us/doc/110x75/5ea2585052451660ed3ed304/index-ftpfequfubrftpfequfubrluisclaudioseguranasafetydoublefirehandbook.jpg)




![Capillary thermostatting in capillary electrophoresis · Capillary thermostatting in capillary electrophoresis ... 75 µm BF 3 Injection: ... 25-µm id BF 5 capillary. Voltage [kV]](https://img.pdfslide.us/doc/110x75/5c176ff509d3f27a578bf33a/capillary-thermostatting-in-capillary-electrophoresis-capillary-thermostatting.jpg)