Embed Size (px)
Citation preview

R E V I E W A R T I C L E
Physiologic strategies to prevent fainting responses during orafter whole blood donation_3202 1..12
Wouter Wieling, Christopher R. France, Nynke van Dijk, Hany Kamel, Roland D. Thijs,
and Peter Tomasulo
Vasovagal syncope (VVS) is a consistent, but infre-quent (0.1%-0.3%) complication of volunteer, wholeblood donation. Given the large number of blood dona-tions, a significant number of donors is involved.Syncope occasionally leads to injury. Recent rigorousdata collection and analysis have led to the associationof a small number of donor and donation factors withthe risk of syncope. An analysis of the time course ofsyncope reactions among approximately 500,000 wholeblood donors suggests that there are three distinctperiods of risk for vasovagal reactions before, during,and after phlebotomy. This review examines the physi-ologic mechanisms that contribute to these periods ofincreased risk including the direct effects of removal ofapproximately 500 mL of whole blood, the psychologicalstress of instrumentation and giving blood (i.e., fear ofneedles, pain, and the sight of blood), and the orthos-tatic effects superimposed on a hypovolemic state afterthe donation. Specifically, we describe interventions thathave been useful in controlling VVS in patients withfainting syndromes and we examine the potential ofthese interventions in the blood donation context, basedon the physiologic principles involved. Finally, wepropose an intervention (dietary replacement of salt lostwith blood donation) that has not been applied in trans-fusion medicine previously but which has the potentialto reduce risk.
While whole blood donation is very safe,some donors experience vasovagal reac-tions during or after donation. The fre-quency of vasovagal syncope (VVS) is low,
0.1%-0.3%,1-3 but given the large number of blood dona-tions (27 million in Europe and the United States annu-ally4 [W. de Kort, Sanquin Blood Supply Foundation, TheNetherlands, personal communication, 2011]), a signifi-cant number of donors are involved, as many as 27,000 to81,000. In addition to the possible injuries experienced byreacting donors, these reactions if severe are highly dis-ruptive and lead to fewer donations from reactingdonors5-7 and probably from their immediate circle ofcontacts. Prevention of vasovagal reactions in blooddonors is thereby an important issue.
The mechanisms underlying VVS in blood donors arethought to include the direct effects of removal of about500 mL of whole blood, the psychological stress of instru-mentation and giving blood (i.e., fear of needles, pain, andthe sight of blood), and the orthostatic effects superim-posed on a hypovolemic state after the donation. Recentstudies have shed some light on the timing of vasovagal
ABBREVIATIONS: BDRI = Blood Donation Reactions Inventory;
VVS = vasovagal syncope.
From the Department of Medicine and the Department of
General Practice/Family Medicine, Academic Medical Centre,
University of Amsterdam, The Netherlands; the Department of
Psychology, Ohio University, Athens, Ohio; Blood Systems, Inc.,
Scottsdale, Arizona; the Dutch Epilepsy Clinics Foundation
(SEIN), Heemstede, The Netherlands; and the Department of
Neurology, Leiden University Medical Centre, Leiden, The
Netherlands.
Address reprint requests to: Wouter Wieling, Department of
Medicine, Suite FV4-221, Academic Medical Centre, University
of Amsterdam, Meibergdreef 9, 1105 Amsterdam, The
Netherlands; e-mail: [email protected].
Received for publication February 28, 2011; revision
received April 13, 2011, and accepted April 13, 2011.
doi: 10.1111/j.1537-2995.2011.03202.x
TRANSFUSION **;**:**-**.
Volume **, ** ** TRANSFUSION 1

reactions in donors and physical characteristics of donorsthat predict vasovagal reactions,1,5,8-10 and prospectivestudies on potential interventions to further reduce therisk of syncope and injury are being performed.11-13
Lower-body muscle tensing, plasma volume expan-sion, and water drinking have been applied as physiologicstrategies to prevent syncope in patients with orthostaticintolerance,14 but it is not well known how these strategiesshould be applied or combined before, during, and afterwhole blood donation. The aim of this review is todescribe the application of these three physiologic strate-gies in the light of the recently published time course ofvasovagal reactions in the setting of whole blood dona-tion.1,15 The focus will be on the physiology of the preven-tion of full VVS with complete whole blood donation.
TIME COURSE OF VASOVAGALREACTIONS DURING BLOOD DONATIONS
We will use the term VVS for blood donation-associatedtransient loss of consciousness. VVS is associated witharterial hypotension and/or bradycardia. Clinically, theseepisodes are preceded by various symptoms includinglightheadedness, dizziness, yawning, nausea, sweating,pallor, unclear thinking, and visual disturbances.16
However, in the absence of simultaneous hemodynamicmeasurements, isolated symptoms of lightheadedness orpallor during blood donation are not a proof of animpending syncope but may also result from anxiety.Since blood pressure measurements are lacking in theregular blood donation setting, these symptoms withoutloss of consciousness (often labeled as “presyncope” or“mild adverse events”) will not be discussed in our review.
VVS before venipunctureBetween arriving at the donation site and the venipunc-ture, the fainting rate is extremely low (0.004%).1,18 Factorsassociated with VVS before venipuncture are donor’syoung age and inexperience, that is, first-time status.1
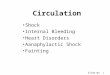
VVS during donation (venipuncture to stand up)A complete blood donation typically takes 7 to 9 minutesduring which the donor is in a recumbent or semirecum-bent position.15 During the first 4 minutes after introduc-tion of the needle the fainting rate continues to be verylow (Fig. 1).15 Thus, immediate VVS due to the psychologi-cal stress of introduction of the needle alone is a very rareevent in blood donors.
0.000
0.020
0.040
0.060
0.080
0.100
0.120
0.140
0.160
0.180
0.200
0.220
0.240
0.260
0.280
0.300
0.320
-10 -7 -5 -3 -1 1 3 5 7 9
11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 48 51 53 57 60 63 68 70 73 76 79 81 83 88 91 93 99 102
106
114
123
134
160
265
Rat
e/1
00
0
Time (min) in relation to needle removal (t = 0)
Overall Vasovagal Syncope Rate in Allogeneic WB Intended Donations, 2007
Male
Female
Donor recumbent Donor ambulating or uprightDonor recumbent
227,345 Donations 341 VVS
327,168 Donations1,130 VVS
Fig. 1. Time course of VVS among whole blood donors. The overall VVS rate in men and women attempting to give whole blood
expressed as a rate per time period from 10 minutes before the end of phlebotomy until 265 minutes after the end of phlebotomy.
The authors of this study assumed that most donors stood up approximately 4 minutes after needle withdrawal and that the
5-minute peak in loss of consciousness reactions was related to this change in position. Collection staff support this assumption
based on experience. WB = whole blood.
WIELING ET AL.
2 TRANSFUSION Volume **, ** **

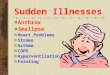
The very low fainting rate in the first few minutesincreases toward the end of the donation with a sharppeak around the period of removal of the needle (Fig. 1).Approximately 10% of the total number of VVS associatedwith complete blood donations occurs during the 1minute around the removal of the needle (Fig. 2).15
After removal of the needle, donors to Blood Systems,Inc. (Scottsdale, AZ; from which organization the dataprovided in Figs. 1, 2, and 3 come) are requested to sit withtheir feet hanging over the side of the donation chair orbed before standing up. This transition step to the uprightposition is not required by the Food and Drug Administra-tion (FDA) and it is unlikely that there is uniformity in thisprocedure in the United States. Subjects remain in thesitting position for approximately 1 to 3 minutes. TheBlood Systems, Inc. standard operating procedure doesnot require the documentation of the time the donorassumes the upright posture so the time must be esti-mated and one must assume that it varies from donor todonor. The number of VVS episodes before the donorstands up amounts to approximately 40% of the totalnumber of VVS episodes during and after complete whole
blood donation (Fig. 3). In this period, VVS is associatedwith donor’s small blood volume and inexperience.1
The amount of blood removed during a whole blooddonation (540 mL)1,15 is about the same as the amountof blood pooled downward rapidly during standing upfrom a supine position (300-800 mL).18 Previous studieshave consistently documented that intravascular instru-mentation during orthostatic stress results in a verypronounced increase in VVS responses in subjects withouta clinical history or tendency for VVS.19,20 In the classicalstudy by Stevens19 performed in healthy young adultUnited States Air Force pilots and navigators the increasewas fivefold with approximately 50% of the subjects expe-riencing VVS. In the study by de Jong-de Vos van Steen-wijk20 in healthy 6- to 16-year-old subjects a fainting rateof 10% during standing increased to 40% after introduc-tion of a venous line. Thus the effect of progressive volumedepletion induced by removal of 540 mL of blood duringdonation in combination with the psychological stress ofthe instrumentation (i.e., fear of needles, pain, and thesight of blood)21-24 is a likely explanation for the peak faint-ing rate around the time of removal of the needle. Unex-
-10 -9 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Incomplete 1 0 1 0 2 0 6 2 19 104 5 2 3 1 7 1 0 1 1 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Complete 1 1 0 3 3 2 11 15 14 150 56 63 67 54 89 66 68 51 86 54 47 50 34 23 20 28 21 18 17 21 14 11 10 8 9 5 4 8 2 8
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
150
160
Freq
uen
cy
Time (min) in relation to needle removal (t = 0)
Donor recumbent Donor ambulating or upright
Frequency of VVS Reactions Among Allogeneic WB Intended Collections, 2007
Incomplete vs. Complete Donations
Donations VVS ReactionsIncomplete 17,606 160Complete 536,907 1,311
Fig. 2. Time course of VVS among donors intending to give whole blood. The actual number of VVS reactions per 1-minute time
period from 10 minutes before the end of phlebotomy until 30 minutes after the end of phlebotomy among men and women
intending to give whole blood. The figure includes incomplete (<450 mL) and complete donations. Donations are terminated before
the desired volume is collected because of slow blood flow, pain at venipuncture site, vasovagal reactions, and other causes.
WB = whole blood.
FAINT PREVENTION DURING BLOOD DONATION
Volume **, ** ** TRANSFUSION 3

pected pain22 induced by removal of the needle may alsobe involved.
VVS on site after standing upCentral blood volume is decreased after a donation of540 mL of whole blood. This implies that cardiac fillingpressures will be subnormal and that the capacity to bufferorthostatic reductions in central blood volume islimited.25-28 Accordingly there is an increased tendency fororthostatic intolerance after whole blood donation. Ortho-static intolerance may manifest itself in the following ways.First, the initial transient (first 20-30 sec) decrease in bloodpressure that is always present upon active standing afterprolonged supine rest (Fig. 4) may be exaggerated resultingin pronounced lightheadedness or even syncope.29
Second, during prolonged standing, postural tachycardiaand genuine VVS may occur due to the large decrease incentral blood volume (Fig. 4).25,30,31
Initial orthostatic hypotension may explain the sharppeak increases in syncope around 1 minute after standingup. The occurrence of the second peak in Fig. 1, approxi-mately 4 minutes after arising occurs during sitting orstanding in the refreshment area, can be explained by VVS.In the first 6 minutes after arising approximately 30% of allVVS reactions occur and the total on-site VVS amounts toapproximately 90% of all VVS.1,15 Factors associated withVVS in this period are donor’s young age and small esti-mated blood volume.1
Off-site VVSApproximately 10% of VVS in the data set occurred afterthe donor left the donation site.1 The last VVS in thestudies mentioned above occurred less than 5 hours afterneedle removal. It should be realized that the prevalenceof off-site syncope may be underestimated, because fromdeparture, there is no active follow-up of the donors: theoff-site VVS rate is dependent on reactions voluntarilyreported by donors. Off-site reactions are more commonin females and in donors who have given a higher percent-age of their estimated blood volume.1 These reactions areimportant since they are more often associated with inju-ries than on-site reactions.1,8,17
STRATEGIES TO PREVENTFAINTING REACTIONS
Physical counterpressure maneuvers: evidencefor effectiveness to combat orthostatic andemotional VVSIn the past decade, patients with a tendency for vasovagalfaints have successfully implemented physical counter-pressure maneuvers like leg crossing and tensing of legand abdominal muscles to combat orthostatic intoler-ance.14 The mechanism underlying the effectiveness ofthese maneuvers is a static contraction of the skeletalmuscles in the legs, buttocks, pelvic region, and abdomi-
0
10
20
30
40
50
60
70
80
90
100
-10 -9 -7 -6 -5 -4 -3 -2 -1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Per
cen
tag
e
Time (min) in relation to needle removal (t = 0)
Cumulative
Male - Incomplete
Female - Incomplete
Male - Complete
Female - Complete
VVS Onset Time Distribution in Complete and Incomplete WB Donations, 2007
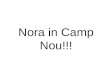
Fig. 3. Time course of VVS reactions among male and female donors giving complete and partial units of whole blood expressed as
a percentage of the total reactions by sex that occurred in each time period. The figure includes incomplete (<450 mL) and com-
plete donations. Donations are terminated before the desired volume is collected because of slow blood flow, pain at venipuncture
site, vasovagal reactions, and other causes. Cumulative plots are presented. WB = whole blood.
WIELING ET AL.
4 TRANSFUSION Volume **, ** **

nal wall resulting in emptying of large capacitance veinsand thereby in an increase in central blood volume,cardiac filling pressures, stroke volume, and cardiacoutput.32-34 Different investigators have used slightly dif-ferent maneuvers (leg crossing, leg and abdominal muscletensing, leg crossing combined with lower body muscletensing, buttock clenching).33,35-37 Interventions that areeffective have in common that they involve tensing of legand abdominal muscles. In the following we will use theterm lower-body muscle tensing. Arm tensing has alsobeen applied35 but this maneuver only is effective becauseit is typically accompanied by strong leg and abdominalmuscle tension. Arm tensing alone does not translocate alarge amount of blood centrally, because the venousvolume in the arms is small.
The effectiveness of lower body muscle tensing incombating orthostatic vasovagal fainting has been dem-onstrated in physiologic studies32-34 and clinical trials.38
Physical counterpressure maneuvers are effective almostinstantaneously. The minimal delay (2-3 sec) between theonset of muscle tensing and the start of the increase inblood pressure (Fig. 5) is accounted for by the transfertime of the blood between the right and the left ventricle(approx. 4-5 heart beats).33,39
Physical counterpressure maneuvers have also beenused successfully by psychologists to decondition bloodinjection injury phobias (emotional faints),23,40 but thephysiologic effects involved have hardly been studied. Anexample of the impressive effects of leg crossing com-bined with lower-body muscle tensing in the semisitting
Fig. 4. Vasovagal fainting in 22-year-old male subject. Note the pronounced initial blood pressure decrease and marked increase in
heart rate after 6 minutes of standing. After 11 to 12 minutes standing blood pressure (BP) and heart rate (HR) start to decrease to
very low values ending in a faint; the period when the heart rate drops to values below 50 beats/min represents a period of asystole of
7 seconds. The arrow indicates the moment of the faint. On lying down, heart rate and blood pressure recover quickly. The picto-
grams indicate lying supine, free standing, and complaints of lightheadedness.
Fig. 5. Original tracing in a male subject aged 34 years during
a vasovagal episode while tilted head up. The dotted line indi-
cates the start of the physical counterpressure maneuver
(combination of leg crossing and lower-body muscle tensing).
A reflex increase in heart rate (HR) is observed almost imme-
diately. The increase in blood pressure (BP) is delayed due to
the transfer time of blood from the right to the left ventricle.
The pictogram indicates leg crossing combined with lower-
body muscle tensing.
FAINT PREVENTION DURING BLOOD DONATION
Volume **, ** ** TRANSFUSION 5

position on arterial blood pressure in a medical studentduring a session of deconditioning of a blood injectioninjury phobia is given in Fig. 6.41 Note again that the effectsof muscle tensing are almost instantaneous. Physicalcounterpressure maneuvers are thereby of prime impor-tance as a strategy to prevent, abort, and/or enhancerecovery of vasovagal fainting in blood donors.
Physical counterpressure maneuver in the contextof whole blood donationsDitto and colleagues36 published the first study that exam-ined physical counterpressure maneuvers in the contextof whole blood donations. In a small pilot study, theseinvestigators randomized relatively inexperienced blooddonors to either standard donation or donation aftervideo instruction in muscle tensing. The 2-minute videotaught donors to repeatedly tense the muscles of theirarms, legs, and abdomen at 5-second intervals whilemaintaining a normal breathing pattern. Results indicatedthat predonation video instruction was associated withan attenuation of donor reports of reactions on theBlood Donation Reactions Inventory (BDRI, a subjectivemeasure of prefaint symptoms). These findings werelater confirmed and extended in studies using largernumbers of donors and a placebo-controlled comparisongroup.12,42-44 The results of muscle tensing studies in blooddonation context are given in Table 1. Although an attenu-ation of donor reports of reactions on the BDRI supportthe notion that muscle tensing reduces subjective reportsof presyncopal reactions, additional studies in largesamples of donors are required to determine level of effec-tiveness in preventing full VVS in the blood donationsetting.
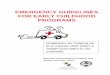
Two recent studies have addressed directly the hemo-dynamic effects of muscle tensing during whole blooddonation. Ditto and coworkers37 reported higher levels ofheart rate, cardiac output, and blood pressure duringwhole-body applied tension. In another study, Kowalskyand coworkers45 demonstrated that donors who engagedin repeated lower-body muscle tensing during donationshow significantly higher levels of cerebral oxygenationcompared to those who engaged in a minimal foot move-ment designed as a distraction control condition. As canbe seen in Fig. 7, those who engaged in muscle tensingmaintained cerebral oxygenation levels above predona-tion baseline levels despite their loss of blood volume.
Advice to apply physical counterpressure maneuversduring and after donation should be as simple and spe-cific as possible to keep donors interested. Taking the timecourse of vasovagal reactions during blood donation(Fig. 1) and the instantaneous effect of physical counter-pressure maneuvers on blood pressure (Figs. 5 and 6) intoaccount, we propose the use of lower-body muscle tensingin the following way.
SupineTo promote arm blood flow during the period the blood istaken, the donors are instructed to periodically squeezea small rubber ball with the donating arm. Rhythmicsqueezing a small ball will not have an important effect asfar as translocation of a large amount of venous bloodfrom the arm centrally (see before). However, squeezing aball may have a reflex influence on preventing VVS by
Fig. 6. Effects of lower body tension in a medical student with
blood phobia during a deconditioning session. (A) The threat
of the needle induces bradycardia and a decrease in pressure
with sensations of lightheadedness. (B) During a 1-minute
period leg crossing and lower-body tensing is applied three
times for 5 to 10 seconds inducing increases of systolic blood
pressure (BP) of approximately 25 mmHg. The pictograms
indicate threat of the needle, sensations of lightheadedness,
and leg crossing combined with lower-body muscle tensing in
sitting position.
WIELING ET AL.
6 TRANSFUSION Volume **, ** **

increasing heart rate, cardiac contractility, and sympa-thetic outflow (exercise pressor response).46,47 In additionto arm squeezing, we suggest instructing donors to applylower-body muscle tensing whenever they experiencelightheadedness. Increasing intrathoracic pressure bystraining (Valsalva maneuver) during lower-body muscletensing should be avoided, because it impedes venousreturn to the heart and thereby reduces the effectivenessof the maneuver.14 The optimal duration and frequency ofmuscle contractions and relaxation remain to be estab-lished. For the time being, in response to perceived light-headedness, we advise lower-body muscle tensing with orwithout the legs crossed with a duration of 5 to 10 secondsfor contractions and a frequency of three times per minute(Fig. 6) during the first part of the phlebotomy.
All donors should be advised to apply lower-bodytensing when the bag is nearly full and especially aroundthe time the tubing is clamped and the needle is removed,because this period is accompanied by a sharp increase invasovagal responses (Fig. 1). The collection staff may wishto signal the need to perform the increased muscle tensingas the bag fills, by asking the donor to switch the ball fromthe venipuncture arm to the contralateral arm and toperform lower-body muscle tensing. During the perioddirectly after removal of the needle, with the donors sittingup with their feet hanging over the side of the donationchair or bed, leg crossing and lower-body tensing isadvised especially in case of symptoms.
UprightAll donors should be advised to apply lower-body muscletensing on arising after donation. They should also beinstructed regarding the usefulness of leg crossing withmuscle tensing as a preventive measure if they stand whilethey are in the refreshment area and for the first hour afterdonation. In case of symptoms of an impending vasovagalfaint, they should be advised to tense their lower-bodymuscles maximally. Further, they should be instructedthat if this intervention is ineffective, they should imme-diately squat, kneel down, or lay flat on their backs. Squat-ting (to sit in a crouching position with the knees bent andthe buttocks on or near the heels) is an emergencymeasure that is about as effective as lying down to increasecardiac filling and reduce the risk of loss of conscious-ness.14 On arising from the squatting position lower-bodymuscle tension should again be applied to prevent a tran-sient arterial blood pressure decrease.48 While there arecurrently no data on the use of muscle tension after dona-tion, the physiologic data supporting the utility of theseinterventions in patients with fainting disorders and thedata from blood donors during donation justify a study toassess its effectiveness.
TABLE 1. A summary of findings from randomized controlled trials that have examined the effect of muscletensing on BDRI scores
Study Sample Comparison Was BDRI reduced?
Ditto et al.42 n = 605 Placebo vs. standard donationMuscle tensing vs. placebo Yes, in womenMuscle tensing vs. standard donation Yes, in women
Ditto et al.36 n = 178 Muscle tensing vs. standard donation Yes, in those with <3 prior donationsDitto and
France43n = 467 Placebo vs. standard donation
Muscle tensing vs. placebo YesMuscle tensing vs. standard donation Yes
Ditto et al.44 n = 1209 Placebo vs. standard donationUpper-body tension (arms only) vs. standard donationLower-body tension (legs/abdomen) vs. standard donation YesFull-body tension vs. standard donation YesUpper-body tension (arms only) plus distraction vs. standard donation Yes
France et al.12 n = 414 Placebo vs. standard donationWater vs. placebo Yes, in womenWater plus leg lift vs. standard Yes, in women
Fig. 7. Mean (�SEM) change in cerebral oxygenation during
whole blood donation for donors engaging in lower body
applied muscle tension (�) or a distraction control involving
gentle foot flexion (�). Because blood donation draw times
vary across individuals, cerebral oxygenation data were aver-
aged into three equal periods for all participants (i.e., first,
second, and third interval of their donation).
FAINT PREVENTION DURING BLOOD DONATION
Volume **, ** ** TRANSFUSION 7

Dietary salt supplement: evidence foreffectiveness to combat orthostatic intoleranceThe sodium content of dietary salt (NaCl) determines thevolume of the extracellular fluid, including the plasmavolume and thereby the blood volume.49-51 An increase indietary salt will increase the plasma and blood volume.Adequacy of the blood volume, and in particular theamount of blood available for the cardiac ventricles(central blood volume), is a crucial factor in circulatoryadjustment to an upright posture.28 Accordingly, benefi-cial effects of an increase in dietary sodium intake on themagnitude of the plasma volume and orthostatic toler-ance are reported in patients with symptomatic orthos-tatic hypotension due to autonomic failure,52 in otherwisehealthy subjects with orthostatic intolerance,53 in dehy-drated athletes,54,55 and in deconditioned astronautsreturning to earth.56
El-Sayed and Hainsworth53 have documented thatchronic plasma volume expansion induced by an increasein dietary salt impressively increases the time to faintduring a combined tilt-body suction experiment. Specifi-cally, the time to faint increased from approximately 20minutes on a standard salt diet to 30 minutes on a high-salt diet. Astronauts are relatively hypovolemic from theirzero-gravity exposure and many experience significantorthostatic hypotension soon after return to earth. As acountermeasure an acute isotonic fluid-loading proce-dure is performed on landing day. The standard procedureconsists of the consumption of 1.0-g salt tablets (i.e.,tablets with 17 mmol NaCl) per 125 mL of water with atotal volume of 15 mL/kg body weight in 2 hours.56 For anastronaut with a body weight of 70 kg, the fluid loadingamounts to the consumption of 70 ¥ 15 = 1050 mL ofwater with 8.4 g of NaCl (143 mmol), that is, roughly theequivalent of 1 L of isotonic saline (0.9% NaCl). The 1 Lof NaCl fluid loading will be distributed over the totalextracellular fluid space (approx. 20% of the body weight).With a body weight of 70 kg the extracellular fluid volumeexpansion by consumption of 1 L of isotonic saline willamount to 1000/1400 = 70 mL per liter of extracellularfluid. The plasma volume is part of the extracellular fluidvolume. With an estimated plasma volume of approxi-mately 3 L in an astronaut of 70 kg, 1 L of isotonic salinewill increase the plasma volume by approximately200 mL.
Dietary salt supplement in blood donorsA donation of 540 mL of whole blood implies a loss ofapproximately 320 mL of plasma water and approximately2.9 g of NaCl (i.e., almost 1.2 g of sodium). FDA food labelslist grams (or milligrams) of sodium because there areusually other sodium-containing salts in food products(e.g., sodium citrate). In the following discussion about
dietary salt supplement, we therefore will use sodiumcontent.
A daily intake of fewer than 2.3 g of sodium is recom-mended, but most US citizens have a higher intake(approx. 3-4 g).57 The amount of extra salt needed (1.2 gNa2+) is within the fluctuations in intake that occur withnormal diets occasionally in daily life.
To prevent VVS the 320 mL of plasma loss due to thedonation of blood needs to be corrected as quickly as pos-sible by oral intake of 1.2 g of sodium and extra water,ideally before or otherwise shortly after phlebotomy. Thechallenge is to devise a trial of a salt replacement strategythat is simple and effective. The time course of salt excre-tion after an oral load is a key factor in this strategy. Acuteincreases in sodium intake are excreted slowly by thebody, with roughly 50% retained within 24 hours.50,58 A cupof soup (250 g) has a salt content of about 0.8 g Na2+. Thus,if on the evening before donation 3 cups of soup areconsumed (2.4 g Na2+), more than 1.2 g of Na2+ can beexpected to be retained on the next day (i.e., enough toreplace the donation-related loss). However, such a largeextra intake of soup and/or sodium the day before dona-tion is not feasible from the blood center and blood donorperspective. An extra sodium intake of approximately 1 g(with 0.5 g retained) may be a more realistic goal, and thusextra sodium intake on the day of donation is needed. Ifsodium intake is increased on the morning of a blooddonation by drinking endurance sport drinks and eatingsalted snacks like pretzels or soup, almost all of the saltcan be expected to be retained during the period thehomeostatic mechanisms are trying to restore the effec-tive circulating volume.50 Plasma water also must berestored and thus sufficient fluid intake is mandatory. Abottle of endurance sports drink (approx. 250 mL) con-tains 0.2 g Na2+ and some glucose that will promote intes-tinal Na2+ uptake. It is an isotonic solution that is rapidlyabsorbed. With two bottles of endurance sports drink (onebottle before and one after donation) the loss of plasmawater (320 mL) will be restored and in addition approxi-mately 0.4 g Na2+ will be added leaving a Na2+ deficit ofabout 0.8 g. A 1-oz bag of pretzels contains approximately0.34 g of Na.2+ Thus with two bottles of a sport drink and2 oz of pretzels (or alternatively 2 cups of soup) thesodium deficit of 1.2 g can be corrected on the day ofdonation. It is important to note that, to date, apart froman older study17 no studies have documented the benefi-cial effects of salt replacement on the tendency for VVSduring and after whole blood donation.
One may argue that not only the plasma water, butalso the volume of the red blood cell mass (with a wholeblood donation of 540 mL approx. 220 mL) must besupplemented after donation by additional NaCl andwater to restore the effective circulating volume. Thus, thecalculated 1.2 g of NaCl supplement is a conservativeestimate.
WIELING ET AL.
8 TRANSFUSION Volume **, ** **

Pressor response to water drinking: evidence forincrease in blood pressure and effectiveness tocombat orthostatic intolerance in patients withautonomic failure and normal subjects withtendency for VVSIf one drinks 500 mL of water it will be distributed over thetotal body water (approx. 60% of body weight) and therebywill barely increase the plasma volume. Water drinkingwill result in a water diuresis due to its effect on plasmaosmolality. In supine healthy subjects the water diuresisstarts within 30 minutes after the intake of the water load(half-life of antidiuretic hormone is approx. 30 min) and israpid. Most of a water load will be excreted in hours.50,59,60
Despite the negligible effects on plasma volume, rapidingestion of 500 mL of water has been shown to be effectivein combating orthostatic intolerance in patients withprimary autonomic failure.60,61 The maximal effect occursafter 30 to 40 minutes. It amounts to an increase of 30 to40 mmHg in systolic blood pressure and the effect lasts forapproximately 1 hour. The blood pressure increase iscaused by an increase in sympathetic nerve outflow, butthe afferent signal for this sympathetic activation isunknown. Stretch of the stomach wall by the water loadand induction of hypoosmolality in the portal venoussystem have been postulated. At present the latter mecha-nism seems to be the best explanation for the underlyingmechanism in patients with autonomic failure.60
Water drinking barely increases blood pressure inhealthy young subjects, but preliminary data suggest thata water load of 500 mL can be applied to improve orthos-tatic tolerance in healthy subjects.62-64 Lu and coworkers63
and Claydon and coworkers62 have reported that drinking500 mL of water 15 minutes before a tilt-body suctionorthostatic stress test increases the standing time byapproximately 5 minutes. Impressive as it is, this 5-minuteincrease in standing time is a transient effect. The bestavailable evidence about the duration of a water load onsympathetic outflow comes from a study that recordedmuscle sympathetic nerve activity after water load of500 mL.65 The muscle sympathetic nerve activity increaselasted for 1 hour. In contrast, plasma volume expansionwith Na and water has a very prolonged effect (>1 day).
Water drinking in blood donorsTo date, three studies have specifically examined theeffects of predonation water loading on the experience ofvasovagal reactions to blood donation. The first study toexamine predonation water loading in the context ofblood donation was conducted as a small, randomizedcontrolled trial of college men and women who weredonating for the first time.66 Donors were randomlyassigned to drink either 0 or 500 mL of bottled waterapproximately 30 minutes before donation. Ratings ofvasovagal reactions were obtained immediately after
donation using the BDRI, and group comparisonsrevealed that water loading significantly reduced reac-tions relative to the no-water control group. This findingwas later confirmed in a study of nearly 9000 high schooldonors who ingested either no water or 473 mL of waterapproximately 0 to 30+ minutes before donation.67 Basedon phlebotomist reports, those who received water had asignificantly lower reaction rate compared to those whodid not (9.9 and 12.5%, respectively). Further analysesindicated that the benefit of water loading was most con-sistent among first-time donors and more likely to beevident when ingestion occurred closer to the time ofactual donation. Most recently, Ando and colleagues68
reported that individuals with pulse rate increases of 15 ormore beats per minute upon standing before donationwere at elevated risk for vasovagal reactions to blooddonation. Further, they noted that reactions among thesehigh-risk donors (large postural increase indicates poororthostatic tolerance) were significantly attenuated afteringestion of 300 mL of water 15 minutes before donation.These observations by Ando and colleagues do not comeunexpectedly; postural tachycardia is a marker of orthos-tatic circulatory intolerance. For instance, it is verycommon after prolonged bed rest and after space flight.Water drinking has been shown to diminish posturaltachycardia.69 In sum, although acute water ingestionappears to have a salutary effect on donation reactions,additional research is needed to address such issues asindividual differences in response, ideal dose and timingof ingestion relative to blood draw, and the potentialbenefit of salt loading before or during the donationprocess. None of these studies examined the effect on vas-ovagal reactions that occurred after the donor left thedonation site.
Salt and water versus water aloneThere are no controlled trials available comparing therelative effectiveness of isotonic plasma volume expan-sion with a 1.2-g sodium supplementation plus extrawater versus the consumption of 500 mL of water alone.The physiologic data as outlined above strongly argue forthe isotonic salt approach, since the effects are pro-longed for hours. The delayed reactions with injuries aremost troublesome and they appear to be plasma volumedependent. Water drinking alone will not correct hypov-olemia. On the other hand, the transient beneficial effectof water intake under hypovolemic conditions may beapplied to diminish a tendency to faint during theactual period of blood donation. Further studies areclearly needed to document which approach is mosteffective. Advice should be as simple as possible and asimilar fluid load before and after donation would beideal. In addition the advice given should be acceptableto donors.
FAINT PREVENTION DURING BLOOD DONATION
Volume **, ** ** TRANSFUSION 9

SYNTHESIS
Our review has provided a physiologic explanation forblood donor VVS at various times before, during, and afterdonation. In addition, we have analyzed some interven-tions that have been shown to reduce the rate of VVS and,where appropriate, provided a physiologic rationale for thesuccess of these interventions. Finally, we have proposedthat a new intervention, salt supplementation, should berigorously assessed on the basis of the understanding ofthe important role dietary salt plays in controlling intravas-cular volume and the evidence of its efficacy in patientswith orthostatic hypotension due to autonomic failure,patients with a tendency for vasovagal faints, dehydratedathletes, and deconditioned astronauts returning to earth.While we recognize that there are no data on salt replace-ment in blood donors, our proposal assumes that mainte-nance of blood volume or rapid restoration of bloodvolume after donation will help all donors and shouldreduce the rate of reactions and injuries regardless of age,sex, blood volume, and donation experience. It is known,however, that some reactions are more likely to be associ-ated with injury than others. The higher risk reactions arethose which occur when the donor is upright and when thedonor is off site.1,8 In addition it is known that youngdonors, inexperienced donors, and donors with low esti-mated blood volume have a higher VVS rate than moreexperienced, mature, and larger donors.5,10 Female sex andlow estimated blood volume are factors strongly associatedwith off-site and late VVS reactions.8 Therefore, rapid res-toration of blood volume may be particularly valuable forthese donors. A trial of salt supplementation should beinitiated with a monitoring system that permits assess-ment of the impact on those donors most likely to react andmost likely to be injured after a reaction.
While VVS reactions with loss of consciousness arethose most likely to be associated with injury, ideally inter-ventions selected to reduce fainting would also have thepotential to reduce the more common, milder reactionsthat can reduce donor satisfaction and likelihood ofreturn.6,70 It is known that there are no significant differ-ences between the predictors of mild reactions and moresevere reactions5,8,10 and a recently completed preliminarytrial13 of three interventions (control of maximum per-centage of blood volume to be donated, water drinking,and muscle tensing) showed that the beneficial impact ofthe interventions is similar on multiple reaction types.Thus, it seems reasonable to assume that a reduction in allreaction types could be achieved with an intervention pri-marily based on an understanding of VVS.
CONFLICT OF INTEREST
The author(s) certify that they have no affiliation with or finan-
cial involvement in any organization or entity with a direct
financial interest in the subject matter or materials discussed in
this manuscript.
REFERENCES
1. Bravo M, Kamel H, Custer B, Tomasulo P. Factors associ-
ated with fainting—before, during and after blood dona-
tion. Vox Sang 2011 May 3. doi: 10.1111/j.1423-0410.2011.
01494.x.
2. Eder AF, Dy BA, Kennedy JM, Notari Iv EP, Strupp A, Wissel
ME, Reddy R, Gibble J, Haimowitz MD, Newman BH,
Chambers LA, Hillyer CD, Benjamin RJ. The American Red
Cross donor hemovigilance program: complications of
blood donation reported in 2006. Transfusion 2008;48:
1809-19.
3. Trouern-Trend JJ, Cable RG, Badon SJ, Newman BH, Pop-
ovsky MA. A case-controlled multicenter study of vasovagal
reactions in blood donors: influence of sex, age, donation
status, weight, blood pressure, and pulse. Transfusion
1999;39:316-20.
4. Whitaker BI, Green J, King M, Leibeg L, Mathew S,
Schlumpf K, Schreiber G. The 2007 nationwide blood col-
lection and utilization survey report. Washington (DC):
Department of Health and Human Services; 2008.
5. Eder AF, Hillyer CD, Dy BA, Notari EP, Benjamin RJ.
Adverse reactions to allogeneic whole blood donation by
16- and 17-year-olds. JAMA 2008;299:2279-86.
6. France CR, Rader A, Carlson B. Donors who react may not
come back: analysis of repeat donation as a function of
phlebotomist ratings of vasovagal reactions. Transfus
Apher Sci 2005;33:99-106.
7. Newman BH, Newman DT, Ahmad R, Roth AJ. The effect of
whole-blood donor adverse events on blood donor return
rates. Transfusion 2006;46:1374-9.
8. Kamel H, Tomasulo P, Bravo M, Wiltbank T, Cusick R,
James RC, Custer B. Delayed adverse reactions to blood
donation. Transfusion 2010;50:556-65.
9. Rios JA, Fang J, Tu Y, Wright DJ, Spencer B, Hillyer CD,
Hillyer KL, Eder AF, Benjamin RJ. The potential impact of
selective donor deferrals based on estimated blood volume
on vasovagal reactions and donor deferral rates. Transfu-
sion 2010;50:1265-75.
10. Wiltbank TB, Giordano GF, Kamel H, Tomasulo P, Custer
B. Faint and prefaint reactions in whole-blood donors: an
analysis of predonation measurements and their predictive
value. Transfusion 2008;48:1799-808.
11. Eder AF, Dy BA, Kennedy JM, Demaris P, Procaccio A, Ben-
jamin RJ. Improved safety for young blood donors with
new selection criteria for total blood volume. Transfusion
2010;50 Suppl 2S:3A.
12. France CR, Ditto B, Wissel ME, France JL, Dickert T, Rader
A, Sinclair K, McGlone S, Trost Z, Matson E. Predonation
hydration and applied muscle tension combine to reduce
presyncopal reactions to blood donation. Transfusion
2010;50:1257-64.
WIELING ET AL.
10 TRANSFUSION Volume **, ** **

13. Tomasulo P, Kamel H, Bravo M, James RC, Custer B. Inter-
ventions to reduce the vasovagal reaction rate in young
whole blood donors. Transfusion 2011; 51. doi: 10.1111/
j.1537-2995.2011.03074.x.
14. Wieling W, Colman N, Krediet CT, Freeman R. Nonphar-
macological treatment of reflex syncope. Clin Auton Res
2004;14 Suppl 1:62-70.
15. Tomasulo P, Bravo M, Kamel H. Time course of vasovagal
syncope with whole blood donation. ISBT Sci Ser 2010;5:
52-8.
16. Wieling W, Thijs RD, van Dijk N, Wilde AA, Benditt DG,
van Dijk JG. Symptoms and signs of syncope: a review of
the link between physiology and clinical clues. Brain 2009;
132:2630-42.
17. Poles FC, Boycott M. Syncope in blood donors. Lancet
1942;2:531-5.
18. Smit AA, Halliwill JR, Low PA, Wieling W. Pathophysiologi-
cal basis of orthostatic hypotension in autonomic failure.
J Physiol 1999;519(Pt 1):1-10.
19. Stevens PM. Cardiovascular dynamics during orthostasis
and the influence of intravascular instrumentation. Am J
Cardiol 1966;17:211-8.
20. de Jong-de Vos van Steenwijk CC, Wieling W, Johannes
JM, Harms MP, Kuis W, Wesseling KH. Incidence and
hemodynamic characteristics of near-fainting in healthy
6- to 16-year old subjects. J Am Coll Cardiol 1995;25:1615-
21.
21. Cotton TF, Lewis T. Observations upon fainting attacks
due to inhibitory cardiac impulses. Heart 1918-1920;7:23-8.
22. Engel CL, Romano J. Studies of syncope; biologic interpre-
tation of vasodepressor syncope. Psychosom Med 1947;9:
288-94.
23. van Dijk N, Velzeboer SC, Destree-Vonk A, Linzer M,
Wieling W. Psychological treatment of malignant vasovagal
syncope due to bloodphobia. PACE 2001;24:122-4.
24. van Lieshout JJ, Wieling W, Karemaker JM, Eckberg DL.
The vasovagal response. Clin Sci (Lond) 1991;81:575-86.
25. Fu Q, Witkowski S, Okazaki K, Levine BD. Effects of gender
and hypovolemia on sympathetic neural responses to
orthostatic stress. Am J Physiol Regul Integr Comp Physiol
2005;289:R109-16.
26. Levine BD. Regulation of central blood volume and cardiac
filling in endurance athletes: the Frank-Starling mecha-
nism as a determinant of orthostatic tolerance. Med Sci
Sports Exerc 1993;25:727-32.
27. Ludwig DA, Convertino VA. Predicting orthostatic
intolerance: physics or physiology? Aviat Space Environ
Med 1994;65:404-11.
28. Wieling W, van Lieshout JJ. Maintenance of postural nor-
motension. In: Low PA, Benarroch EE, editors. Clinical
autonomic disorders. Philadelphia (PA): Wolters Kluwer
Health/Lippincott Williams & Wilkins; 2008. p. 57-67.
29. Wieling W, Krediet CT, van Dijk N, Linzer M, Tschakovsky
ME. Initial orthostatic hypotension: review of a forgotten
condition. Clin Sci (Lond) 2007;112:157-65.
30. Fu Q, Levine BD. Why do young women (donors) faint?
Transfusion 2010;50:522-5.
31. ten Harkel AD, Baisch F, Karemaker JM. Increased orthos-
tatic blood pressure variability after prolonged head-down
tilt. Acta Physiol Scand Suppl 1992;604:89-99.
32. Krediet CT, de Bruin IG, Ganzeboom KS, Linzer M, van
Lieshout JJ, Wieling W. Leg crossing, muscle tensing,
squatting, and the crash position are effective against vas-
ovagal reactions solely through increases in cardiac output.
J Appl Physiol 2005;99:1697-703.
33. Krediet CT, van Dijk N, Linzer M, van Lieshout JJ, Wieling
W. Management of vasovagal syncope: controlling or
aborting faints by leg crossing and muscle tensing. Circula-
tion 2002;106:1684-9.
34. van Dijk N, de Bruin IG, Gisolf J, Bruin-Bon HA, Linzer M,
van Lieshout JJ, Wieling W. Hemodynamic effects of leg
crossing and skeletal muscle tensing during free standing
in patients with vasovagal syncope. J Appl Physiol 2005;98:
584-90.
35. Brignole M, Croci F, Menozzi C, Solano A, Donateo P,
Oddone D, Puggioni E, Lolli G. Isometric arm counter-
pressure maneuvers to abort impending vasovagal
syncope. J Am Coll Cardiol 2002;40:2053-9.
36. Ditto B, Wilkins JA, France CR, Lavoie P, Adler PS. On-site
training in applied muscle tension to reduce vasovagal
reactions to blood donation. J Behav Med 2003;26:53-65.
37. Ditto B, Byrne N, Holly C. Physiological correlates of
applied tension may contribute to reduced fainting during
medical procedures. Ann Behav Med 2009;37:306-14.
38. van Dijk N, Quartieri F, Blanc JJ, Garcia-Civera R, Brignole
M, Moya A, Wieling W. Effectiveness of physical counter-
pressure maneuvers in preventing vasovagal syncope: the
Physical Counterpressure Manoeuvres Trial (PC-Trial).
J Am Coll Cardiol 2006;48:1652-7.
39. Wieling W, Harms MP, ten Harkel AD, van Lieshout JJ,
Sprangers RL. Circulatory response evoked by a 3 s bout of
dynamic leg exercise in humans. J Physiol 1996;494(Pt
2):601-11.
40. Ost LG, Fellenius J, Sterner U. Applied tension, exposure in
vivo, and tension-only in the treatment of blood phobia.
Behav Res Ther 1991;29:561-74.
41. Busweiler LA, de Jong JP, Beunderman R, van Dijk N,
Wieling W. Preventing fainting due to needles or blood.
Ned Tijdschr Geneeskd 2010;154:A1847.
42. Ditto B, France CR, Lavoie P, Roussos M, Adler PS. Reduc-
ing reactions to blood donation with applied muscle
tension: a randomized controlled trial. Transfusion 2003;
43:1269-75.
43. Ditto B, France CR. The effects of applied tension on
symptoms in French-speaking blood donors: a random-
ized trial. Health Psychol 2006;25:433-7.
44. Ditto B, France CR, Albert M, Byrne N. Dismantling applied
tension: mechanisms of a treatment to reduce blood
donation-related symptoms. Transfusion 2007;47:2217-22.
45. Kowalsky JM, France JL, Wissel ME, France CR. Effect of
FAINT PREVENTION DURING BLOOD DONATION
Volume **, ** ** TRANSFUSION 11

applied muscle tension on cerebral oxygenation during
blood donation. Transfusion 2011. doi: 10.1111/j.1537-
2995.2011.03075.x.
46. Hollander AP, Bouman LN. Cardiac acceleration in man
elicited by a muscle-heart reflex. J Appl Physiol 1975;38:
272-8.
47. Rowell LB. Human cardiovascular control. New York:
Oxford University Press; 1993.
48. Krediet CT, Go-Schön IK, Kim YS, Linzer M, van Lieshout
JJ, Wieling W. Management of initial orthostatic
hypotension: lower body muscle tensing attenuates the
transient arterial blood pressure decrease upon standing
from squatting. Clin Sci (Lond) 2007;113:401-7.
49. Boron WF, Boulpaep EL. Medical physiology. 2nd ed.
Philadelphia (PA): Saunders; 2008.
50. Rose BD, Post TW. Clinical physiology of acid-base and
electrolyte disorders. 5th ed. New York: McGraw-Hill
Professional; 2001.
51. Wieling W, van Lieshout JJ, Hainsworth R. Extracellular
fluid volume expansion in patients with posturally related
syncope. Clin Auton Res 2002;12:242-9.
52. ten Harkel AD, van Lieshout JJ, Wieling W. Treatment of
orthostatic hypotension with sleeping in the head-up tilt
position, alone and in combination with fludrocortisone.
J Intern Med 1992;232:139-45.
53. El-Sayed H, Hainsworth R. Salt supplement increases
plasma volume and orthostatic tolerance in patients with
unexplained syncope. Heart 1996;75:134-40.
54. Merson SJ, Maughan RJ, Shirreffs SM. Rehydration with
drinks differing in sodium concentration and recovery
from moderate exercise-induced hypohydration in man.
Eur J Appl Physiol 2008;103:585-94.
55. Von Duvillard SP, Braun WA, Markofski M, Beneke R, Lei-
thauser R. Fluids and hydration in prolonged endurance
performance. Nutrition 2004;20:651-6.
56. Waters WW, Platts SH, Mitchell BM, Whitson PA, Meck JV.
Plasma volume restoration with salt tablets and water after
bed rest prevents orthostatic hypotension and changes in
supine hemodynamic and endocrine variables. Am J
Physiol Heart Circ Physiol 2005;288:H839-H847.
57. Bibbins-Domingo K, Chertow GM, Coxson PG, Moran A,
Lightwood JM, Pletcher MJ, Goldman L. Projected effect of
dietary salt reductions on future cardiovascular disease. N
Engl J Med 2010;362:590-9.
58. Walser M. Phenomenological analysis of renal regulation
of sodium and potassium balance. Kidney Int 1985;27:837-
41.
59. Blomhert G, Gerbrandy J, Borst JG, Molhuysen JA, de Vries
LA. Diuretic effect of isotonic saline solution compared
with that of water; influence of diurnal rhythm. Lancet
1951;2:1011-5.
60. May M, Jordan J. The osmopressor response to water
drinking. Am J Physiol Regul Integr Comp Physiol 2011;
300:R40-R46.
61. Jordan J, Shannon JR, Black BK, Ali Y, Farley M, Costa F,
Diedrich A, Robertson RM, Biaggioni I, Robertson D. The
pressor response to water drinking in humans : a sympa-
thetic reflex? Circulation 2000;101:504-9.
62. Claydon VE, Schroeder C, Norcliffe LJ, Jordan J,
Hainsworth R. Water drinking improves orthostatic toler-
ance in patients with posturally related syncope. Clin Sci
(Lond) 2006;110:343-52.
63. Lu CC, Diedrich A, Tung CS, Paranjape SY, Harris PA, Byrne
DW, Jordan J, Robertson D. Water ingestion as prophylaxis
against syncope. Circulation 2003;108:2660-5.
64. Pitt MS, Marshall P, Diesch JP, Hainsworth R. Cardiac
output by Portapres. Clin Sci (Lond) 2004;106:407-12.
65. Scott EM, Greenwood JP, Gilbey SG, Stoker JB, Mary DA.
Water ingestion increases sympathetic vasoconstrictor dis-
charge in normal human subjects. Clin Sci (Lond) 2001;
100:335-42.
66. Hanson SA, France CR. Predonation water ingestion
attenuates negative reactions to blood donation. Transfu-
sion 2004;44:924-8.
67. Newman B, Tommolino E, Andreozzi C, Joychan S, Pocedic
J, Heringhausen J. The effect of a 473-mL (16-oz) water
drink on vasovagal donor reaction rates in high-school stu-
dents. Transfusion 2007;47:1524-33.
68. Ando SI, Kawamura N, Matsumoto M, Dan E, Takeshita A,
Murakami K, Kashiwagi S, Kiyokawa H. Simple standing
test predicts and water ingestion prevents vasovagal reac-
tion in the high-risk blood donors. Transfusion 2009;49:
1630-6.
69. Shannon JR, Diedrich A, Biaggioni I, Tank J, Robertson RM,
Robertson D, Jordan J. Water drinking as a treatment for
orthostatic syndromes. Am J Med 2002;112:355-60.
70. Rader AW, France CR, Carlson B. Donor retention as a
function of donor reactions to whole-blood and
automated double red cell collections. Transfusion
2007;47:995-1001.
WIELING ET AL.
12 TRANSFUSION Volume **, ** **