-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
1/23
Israels Step Children
About the lack of pediatrics in the Unrecognized Villages in
the Negev and its Ramifications
A Position Paper by the Women Promote Health Group and
Physicians for Human
Rights
November 2008
Author: Heijer Abu Sharb
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
2/23
2
Brief
In the South of Israel there are forty five villages which
include about
83,000 residents, out of whom 60% are children. Most of the
villages are
unrecognized by the state thus, their right to health services
and necessary
health conditions is violated. Since 1999, eleven of the
villages were
recognized by the state, yet despite that recognition they do
not receive the
full services each resident is entitled to.
There are twelve clinics in the unrecognized villages and only
in eight
villages are there family health centers. There are no
pediatricians,
gynecologists and pharmacies in the clinics; in most cases the
staff does not
speak Arabic, reception hours are very limited etc.
According to data from the Soroka Medical Center, compared to
Jewish children,
more Bedouin children arrive at the emergency units; more
Bedouin children
need hospitalization in the pediatric ward and the emergency
units; and more
Bedouin children die due to their illness. Moreover, Bedouin
children who
arrive at the emergency department arrive at critical stages of
the illness,
due to a late diagnosis deriving from the lack of health
services,
infrastructure, roads, transportation and access routes for the
community.
Despite the high morbidity and mortality among the Bedouin
children in the
Negev, none of the clinics existing in the villages (all clinics
except for
one are run by Clalit), employ a pediatrician. On the other
hand, in
adjacent, rich Jewish communities such as Meitar, Omer and
Lehavim the
residents insured in Clalit, have pediatricians, gynecologists
and family physicians, many and more flexible reception hours and
accompanying services
that do not exist in the clinics in the unrecognized villages.
For instance,
in Omer there are 5.18 physician hours per 100 patients compared
to 1.86 in
Algrain. The Jewish residents have the option of being insured
in other health
funds (Maccabi, Meuhedet and Leumit), which operate in the
Jewish communities
and do not operate in the unrecognized villages.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
3/23
3
A survey conducted by the Women Promote Health group and
PHR-Israel among 70
residents of the villages show that due to the long distance of
the clinicsfrom the village center and due to the lack of basic
services such as
medications, professional medicine (especially pediatricians),
limited
reception hours and so on, many residents prefer to receive the
service in
townships or in private clinics. Thus, for instance:
Only 55% of the women visit the village clinic most of the time,
while 45%
dont visit the clinic at all or visit it sometimes.
48% of the women reported that after receiving treatment in the
village
clinic, they had to go to an additional clinic in order to
complete the
treatment; 77% of the women who reported visiting a different
clinic had been
forced to visit a private pediatrician, and 13% visited the
pediatricemergency unit.
32% of the women reported they visited the emergency unit with
their children
in the past year: 24% due to high fever, 16% due to an
unsuccessful treatment
by the clinic physician, and 12% due to dehydration.
50% of the women reported that they go to the clinic on foot,
with their
child, and that they do not have another way to get there. 51%
of the women
claimed that its a 5-15 minute walking distance, 35% indicated a
walking
distance of between 20-40 minutes and 14% indicated a 60-120
minute walking
distance.
As you can see, the establishment of the clinics in the
villages, most of
which were built only after a Supreme Court petition1, is only a
partial move
in the realization of the villages residents right to health. A
full
realization requires electricity and water connection and
additional necessary
health conditions. Moreover, the right to health is bound with
the right to
equality and therefore, the existence of clinics that offer a
low range of
services compared to the services available for residents in
clinics outside
the unrecognized villages in the Negev, violates the equal right
of the
residents of the villages to unified health services.
Furthermore, the core
principles of the National Health Insurance Law are not only
equality but also
the value of justice which means a bigger investment in resource
development
1High Court Petition 4540/00.
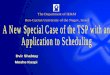
The Number of Reception Hours Physicians in Clalit Clinics
according to Settlement
38
0
81.5
031
0
109
55
214
36
83
36.5
0
50
100
150
200
250
MeitarBir Hadaj
OmerAlgrainLehavimUmmMatnan
Weekly reception hoursPediatrician
Weekly reception hours
All physicians
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
4/23
4
especially where it is most needed. Since the residents of the
unrecognized
villages suffer from higher morbidity and mortality, the state
should initiate
a differential investment when establishing health services
within the
villages.
With regards to pediatrics, in many places in the world the
family physician
is the main caregiver of the child and the pediatrician serves
as his advisor
(in England, for instance). This method has many advantages;
among others itis a comprehensive understanding of the familys
needs. However, the fact that
there is no pediatrician in the village clinics, where there are
numerous
children, with high morbidity and mortality rates and given the
harsh living
conditions, raises questions and calls for action.
PHR-Israel and the Women Promote Health group demand from the
state:
To act for the recognition of the unrecognized villages in the
Negev; to
connect them to all national infrastructures, especially water,
and to connect
the clinics to the electricity network in order to allow, among
other things,
refrigeration of medications;To act so that the scope, variety,
and quality of the services provided in the
villages' clinics are equal to available services in most
primary clinics in
other communities, and that pediatricians and gynecologists are
employed in
the existing clinics;
To differentially invest in developing the volume and variety of
health
services in the unrecognized villages in the Negev;
To act for the planning and implementation of programs designed
to reduce
morbidity and mortality rates among the residents of the
unrecognized villages
in the Negev in general, and their children in particular, so
that it will be
culturally fitting;
To make sure that the health services are adapted to the
cultural and labial
needs.
The "Women Promote Health" Group Background about the
Authors of the Position Paper
We are a group of Arab-Bedouin women, residents of the
unrecognized villages
in the Negev that formed in the framework of a course called
"Women Promote
Health" initiated by Physicians for Human Rights. We are
residents of tenunrecognized villages - Tel Arad, Qasar Alsir, Wadi
Alna'am, Al-Zarnug, Khashm
Zinna, Um Bateen, Wadi Ghwain-Tela Rashid and Albatel-
Karkur.
During the course, we were exposed to a lot of information
regarding health
and the right to health. When the course ended, we decided to
take action
while focusing on two issues: (1) Raising the awareness of women
to the right
to health, by means of workshops dealing with the subject and
(2) taking
advocacy steps demanding from The "Clalit" health fund and the
Ministry of
Health to employ pediatricians in the existing clinics.
This position paper presents our findings as for the second
cause: to make
sure that the existing clinics in the villages will provide
basic services pediatrics that are provided in our surrounding
communities.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
5/23
5
General Background about Underlying Determinants of Health
and Services in the Unrecognized Villages in the Negev
In the south of Israel there are forty five villages which
include about
83,000 residents, 60% out of whom are under 19 years old. Most
villages are
not recognized by the state, thus their right to health and
Underlying
determinants of Health, such as water, electricity, sewage,
garbage disposal,
adequate housing, paved roads, road signs etc, are violated. The
eleven
villages that were recognized by the state since 1999 still do
not receive the
full services every resident is entitled to.
The Lack of Underlying Determinants of Health
Naturally, children are more prone than adults to dehydration
and intestine
illnesses, due to the lack of accessibility to clean water,
adequate for
drinking. A "Diarrhea epidemic" erupts every August, during
which 16,000
Bedouin children are admitted to hospital, compared to 5,000
Jewish children;
that is to say that while the Bedouin children constitute only
15% of the
entire population of the Negev, they constitute 80% of the
entire children
population admitted to hospitals2.
Another danger lurking for the children in the summer time is
caused by the
living conditions in the tin shacks. These shacks double the
heat level and
many babies need medical care due to a rise in their body
temperature and
dehydration. In the winter, the condition worsens even more
since the extreme
cold in the house and the inability to provide safe heating
facilities (due to
the lack of electricity connection), causes the hospital
admissions (due tocold and burns) and even the death of
children.
3
The poor sanitary conditions, such as garbage accumulation, due
to the lack
of a disposal solution constitute a good base for mice which
have bitten
children more than once. Burning the garbage is not safe either.
It causes the
release of toxins that harm the children playing in the
surroundings.4
The Lack of Adequate Health Services
Due to the lack of necessary health conditions and the poor
health results,
the residents of the unrecognized villages in the Negev should
have highaccessibility to health services. Yet, the situation is
far from it. Today,
there are twelve clinics in the unrecognized villages and only
eight villages
have family care units. These clinics serve only 20% of the
residents of the
unrecognized villages. Moreover, the services provided in the
existing clinics
are lacking and are not accessible to the residents:
Physical accessibility: The lack of public transportation and
paved roads make
it hard to reach the clinics situated far from the village
center. It is
especially difficult for women, who are in charge of child care
and also
2O. Almi (May 2006). Physicians for Human Rights. Water
Discipline: Water, the Stateand the Unrecognized Villages in the
Negev.3Ibid.4Ibid.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
6/23
6
suffer social mobility limitations. This fact goes to show that
when locating
the clinics far away and in setting the reception hours (they do
not operate
in the afternoon and on Fridays), there is no proper adjustment
to the needs
of the population it is supposed to serve.
A Lack of Medications and Lab Services: Since the clinics are
not connected to
the electricity network and operate using generators, they are
only able toprovide medications that do not need refrigeration.
There are no pharmacists
in the clinics thus the nurse has two duties. Residents, who
need medications
that cannot be supplied by the clinics, are forced to reach the
clinics
located in townships5, the cost of which causes some not to take
their
medications.
Language: The medical staff in the clinics usually speaks only
Hebrew, a fact
that does not enable the mothers to communicate with the
doctors. They have
troubles explaining the problem as well as understanding the
orders given to
them by the medical staff.
Primary Mother-Child-Health care clinics: Even though there are
clinics in
twelve villages, only eight also have Primary
Mother-Child-Health care
clinics. These operate twice a week in the mornings, a fact that
causes a
heavy burden.
The Lack of Services to Un-Documented Children:
Thousands of Un-documented (status-less) children live in Israel
and
especially in the unrecognized villages in the Negev.6Since the
entitlement to
health services under the National Health Insurance law is
stipulated to
residency, a large number of children have no health insurance
and are not
entitled to medical care, except in a state of emergency. A
settlement
providing health services in return for payment, to
un-documented children,
was validated in February 2001 by the "Meuhedet" health fund.
The services
included in the basket are equal to those included in the
national health
basket provided to Israeli residents. Yet, one of the
limitations of the
settlement is that if one of the parents is Palestinian, the
child is not
entitled.7
This limitation practically prevents the only alternative
for
receiving medical care from most of the un-documented children
in the villages
(except for private medicine). Despite the limitation, the
children in the
villages that are entitled for the settlement suffer from
accessibility
problems, since there is no "Meuhedet" health fund in the
villages.
5 Between 1968 to the 1980's, the state established 7 townships:
Rahat, Tel-Sheva, Hura,Laqye, Segev-Shalom, Kuseife and Ar'ara. The
townships, as opposed to the villages,have been recognized by the
state, and are connected to the infrastructures and haveclinics.6In
a survey conducted by PHR-Israel and the "Women Promote Health"
group discussedlater in this paper - 5 out of 70 women reported
that their children have no healthinsurance since they have no
legal status.7Ran Cohen, coordinator immigrants and non residents
project, PHR-Israel. Thesettlement suffers from additional,
problematic limitations: the settlement is
voluntary and based on the parents responsibility to sign their
children and pay forthe service, and not on every child's right to
health, as opposed to Israeli childrenwho are entitled to health
services, without registration and payment; there is a sixmonth
waiting period for entitlement for children who were not born in
Israel; theinsurance does not cover health care for a condition
that existed prior to the entranceto Israel; the treatment is
expensive; etc.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
7/23
7
Children's Right to Health in the Unrecognized Villages in
the Negev: Situation Report
The children in the unrecognized villages in the Negev suffer
from a threefold
discrimination: being residents of the south they suffer from
higher morbidity
and mortality rates and lower availability of medical services
compared to the
rest of the country; being a part of the Arab minority in Israel
they suffer
from higher morbidity and mortality percentages and lower
availability of
medical services compared to the Jewish majority; being
Arab-Bedouin, the
residents of the unrecognized villages in the Negev suffer from
higher
morbidity and mortality percentages and lower availability of
medical services
compared even with the Arab minority.
Since the villages in the Negev are not recognized by the state,
they remain
invisible to the different authorities. Thus, for instance, they
are notregistered in the Central Bureau of Statistics, the Ministry
of Health and the
Soroka Medical center; therefore there is no available
information about their
medical condition. The little information we found about the
unrecognized
villages in the Negev, had been classified according to the
residents' tribal
origin and not according to the village in which they reside. As
a result, it
was difficult to receive exact data about the medical condition
of the village
children. For instance, when we wanted to check the percentage
of child
emergency admissions of children from the villages compared to
those from
townships and Jewish children, we faced a problem: The Soroka
Medical Center
had information about children according to their tribal origin
and notaccording to their village so that we were unable to ascribe
the children to a
specific village or township since members of one tribe can
reside both in a
township and in an unrecognized village.
Data collection constitutes a necessary basis for dealing with
inequality in
health. The lack of a data base specific for the population of
the
unrecognized villages does not allow dealing with the problem
and helps in its
perpetuation8.
Children's Health Condition in the Unrecognized Villages in the
NegevThe childhood years are critical. Poor health might influence
the child's
general functioning throughout his entire life. Not treating
health problems
might cause an untreatable health condition later on. The poor
housing, living
and hygienic conditions, the lack of infrastructures,
electricity, water,
sewage, roads, public transportation and health services, along
with the
socio-economic status and the demographic-social characteristics
of the Arab-
Bedouin population in the Negev, have a crucial effect on the
residents'
health conditions in general, and that of their children in
particular.
8Avni, s. (April, 2007). PHR-Israel. "The Right to Health among
Arab-Palestinians inIsrael: A Comparative Look." A Report for the
International Health Day.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
8/23
8
Injury, high morbidity, many emergency admissions and high
mortality among
Bedouin children, are extremely common phenomena9:
Infant Mortality:
The rate of infant mortality in the Arab-Bedouin population in
the Negev is
one of the highest in Israel: in 2005 the rate of infant
mortality was 4.72
out of 1,000 live births among the Jewish population compared to
15.45 out of1,000 live births among the Arab population.
10
In 2006, the rate of infant mortality in the general population
was 5.5 out of
1,000 live births. The rate within the Jewish population was 3.1
out of 1,000
live births and 13.7 out of 1,000 live births within the Arab
population in
the Negev. It should be mentioned that even if congenital
deficiencies are the
leading death factor among Arab children, it does not serve as
an explanation
for the gap.
Morbidity:
The lack of infrastructures running water, sewage and the lack
of
electricity leads to poor hygienic conditions which cause
contagion of
infective illnesses among children; A "diarrhea epidemic" erupts
every August,
during which 16,000 Bedouin children are admitted to hospital
every year,
compared to 5,000 Jewish children; that is to say that while the
Bedouin
children constitute only 15% of the entire population of the
Negev, they
constitute 80% of the entire children population admitted to
hospitals11; the
lack of adequate physical and environmental conditions lead to
domestic
accidents, road accidents, burns, poisoning, inhalation of
foreign bodies and
drowning; the environmental conditions expose the village
children to numerous
dangers such as snakes, scorpions, frostbites and sun burns; and
living close
to Ramat Hovav results in respiratory illnesses, oncological
illnesses and a
higher risk of general morbidity.
The poor economic state of the residents along with the loss of
the
traditional way of life, leads, among others, to malnutrition
among their
children a study showed that Bedouin children residing in the
unrecognized
villages have a 2.4 times higher chance of suffering from
malnutrition,
compared to those residing in townships (such as Rahat).12
In addition, the small number of Family Care Units in the
villages makes the
pregnancy supervision, necessary for the early diagnosis of
congenital
deficiencies13, growth supervision and proper development of
infants - hard.
9Weisblai, A. (November 20, 2006). "Situation Report Bedouin
Children in the Negev."Submitted to the 'committee on the Rights of
the child'.10National data on infant and child mortality until the
age of 5 in Israel December20, 2005, the Ministry of Health.11O.
Almi (May 2006). PHR-Israel. Water Discipline: Water, the State and
theUnrecognized Villages in the Negev.
12Ofer Meir, Ynet. "A New Study Reveals: Malnutrition among
First Graders in theSouth." 6.2.2005.13Sofer, S. (2006) in:
"Environmental (in) Justice Report: Health, Environment andSocial
Justice." Environmental Justice Committee.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
9/23
9
The rate of vaccine coverage among Arab-Bedouin in the Negev is
5% lower than
the rate in the Jewish sector.14
A larger number of Bedouin infants are hospitalized compared to
Jewish
children: in 2003 the rate of Bedouin children admitted was 32%
compared to
about 8% among the Jewish population. The high rate of
admissions among
Bedouin infants is attributed to the high rate of congenital
deficiencies,accidents and illnesses. Since 2000, we can see a
decrease in the admission
rates of infants among both populations, especially among the
Bedouin
population.15
According to Prof. Shaul Sofer16, based on data from the Soroka
Medical Center,
compared to Jewish children: more Bedouin children go to
emergency units; more
Bedouin children need to be admitted to pediatric wards; more
Bedouin children
need to be admitted to emergency units and a growing number die
due to their
illness. In addition, Bedouin children that reach the emergency
units arrive
at a critical stage of the illness, due to a delayed diagnosis
deriving fromthe lack of medical services, infrastructures, roads
and community access
routes.
9.1% 0f the Bedouin children in the Negev are children with
special needs
(suffering from physical, cognitive and different mental
disabilities)
compared to 7.7% out of the entire Israeli population. This rate
is higher
even in comparison with the parallel rates among the Arab and
Jewish
populations in Israel (8.3% and 7.6% respectively). 7.9% of the
Bedouin
children suffer from learning disabilities or behavioral and
emotional
problems.17
Health Services Availability for the Children of the
Unrecognized
Villages in the Negev
"Clalit" is the health fund operating all primary clinics
(except for one run
by "Leumit" in Algrain/said village) in the unrecognized
villages in the
Negev.
Only about 60% of the residents of the villages in which clinics
are located,
are registered in their clinics (Graph number 1)18.
Conversations of the "Women
Promote Health" group with residents, show that due to the long
distance of
the clinics from the village center and due to the lack of basic
services such
as medications, professional medicine (especially pediatrics),
limited
14The Health System in the Negev Description of the existing
conditions and needs
during the development of the area according to the national
plan. September 2005.15Weisblai, A. (November 20, 2006). "Situation
Report Bedouin Children in the Negev."Submitted to the 'committee
on the Rights of the child'.
16Sofer, S. (2006) in: "Environmental (in) Justice Report:
Health, Environment andSocial Justice." Environmental Justice
Committee.17Strosberg, N., Naon, D., Ziv, A. (July 2008). Shatil
and the Regional Council for theUnrecognized Villages in the Negev.
"Special-needs Children in the Bedouin Populationof the Negev:
Characteristics, Patterns of Service Use, and the Impact of Caring
forthe Children on the Mothers."18
The datum regarding the number of insured residents was
submitted by the RegionalCouncil for the Unrecognized Villages. It
was submitted following a freedom ofinformation appeal to the
supervisor from the "Clalit" health fund Mrs. Noa Denai.There are
more insured patients In the Al-Zarnoog clinic than residents.
According tothe Regional Council for the Unrecognized Villages, the
reason is that residents fromadjacent villages -Khashm Zanna and
Beer Al-Hamam, go to that clinic.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
10/23
10
reception hours etc., many residents prefer to receive the
treatment in the
townships. The residents told the women that those who are
registered to the
village clinics belong to the most weakened populations families
with many
children, living on income support benefit, families that do not
own a car,
widows, second wives and elderly people.
The Number of "Clalit" Patients in Villages with a "Clalit"
Clinic
0500
1,0001,5002,0002,5003,0003,5004,0004,5005,000
BirHadaj
UmmMa
tnan
QasarAlsi
r
UmBate
enDa
rijat
WadiGh
wain
Algrain
AbuT
alul
Al-Za
rnug
Number of residents
Number of clalit patients
In order to examine the medical services available to the
residents of the
unrecognized villages in the Negev, compared to the Jewish
residents living in
adjacent settlements in the Negev, we conducted a comparison
between three
unrecognized villages (Bir-Hadaj, Algrain and Umm-Matnan the
three villages
with the highest number of residents) and three Jewish adjacent
settlements
(Meitar, Omer and Lehavim)19:
The clinics in Meitar, Omer and Lehavim offer a wider range and
variety of
medical services. All of them have pediatricians and
gynecologists, an
expertise that is not available for the residents of the
unrecognized villages
in the Negev. The reception hours of the clinics situated in the
Jewish
settlements are spread out throughout the day, they are more
accessible and
offer services such as a pharmacy, dietitian and so on, which
are not
available in the village clinics.
19The data are taken from the "Clalit" health fund website.
Graph Number 1
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
11/23
11
See appendix for additional comparative data between the
clinics)(
These gaps are especially pungent considering the data regarding
the high
morbidity and mortality of the children in the unrecognized
villages, compared
to Jewish children and considering the data regarding the
social-economic
conditions of the residents of the unrecognized villages
compared to those in
adjacent settlements: Meitar, Lehavim and Omer head the
social-economic
stratification made by the Central Bureau of Statistics
(clusters 9,9 and 10
respectively) compared to the unrecognized villages in the Negev
which stand
at the bottom (they are actually not graded but the townships
such as Ar'ara
in the Negev, Segev Shalom, Laqye and Rahat, are graded at the
bottom of the
table cluster number 1).
The Accessibility of Health Services to the Children in the
Unrecognized Villages in the Negev
Seventy women, mothers to children, were interviewed by the
"Women Promote
Health" group, accompanied by PHR-Israel, in order to examine
the children's
accessibility of health services in the unrecognized villages in
the Negev.
The survey focused on the extent and manner of use of health
services in the
village clinics and on the limitations in receiving the service,
while
focusing on the medical needs of the children and the existing
solutions to
these needs.The interviews were conducted face to face, using a
structured questionnaire
in Arabic, in their homes or in the clinics (in four villages
Wadi Alna'am,
Um Bateen, Alsurra, and Al-Zarnug).
The ages of the interviewed women: 51% are 20-30 years old, 32%
are 30-40
years old, and 17% are over 40 years old.
Education level of the interviewed women: 22.8% havent studied
at all, 34.2%
haven't finished high school, and 38.5% finished high school.
The rest (3
women) acquired higher education.
Average Number of Children: 6. The answer to the question -
"Does any of your
children suffer from a chronic illness": 20% of the women
responded that they
38
0
81.5
0
31
0
109
55
214
36
83
36.5
0
50
100
150
200
250
MeitarBir Hadaj
OmerAlgrainLehavim
UmmMatnan
Weekly reception hours
pediatrician
Weekly reception hours
All physicians
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
12/23
12
have a child suffering from a chronic illness and needs monthly
supervision,
medications and treatment on a regular basis.
The Findings of the Interviews:20
Medical Services Usage:
In response to the question: "Were most of the visits to the
clinic aimed for
your children or for you or your husband?" 90% of the women
answered that most
of the times they visit the clinic due to their children's
needs.
In response to the question: "Who do you usually turn to when
your child is
ill21?" they gave the following answers:
55% of the women said that they visit the village clinic "most
of the
time"; the rest said that they "never" visit the clinic or
only
"sometimes".
20% of the women said that they visit a private physician "most
of the
time"; 55% "sometimes" visit a private physician.22
Few women visit the emergency unit "most of the time"; 53% visit
it"sometimes".
31% of the women visit a clinic in another village "most of the
time";
32% visit it "sometimes".
In response to the question "Have you ever visited the village
clinic and
later on had to visit another clinic in order to complete the
treatment of
your children?": 48% of the women said they had to visit another
clinic. Out
of them, 77% reported visiting a private physician, 13% reported
visiting the
emergency unit and the rest visited a clinic in another village
or the same
clinic again:
20The interviews were conducted in Arabic. The answers refer to
the percentage amongthe women who answered the specific
question.21
When answering this question we asked them to refer to 5
categories village clinic,private physician, emergency unit,
traditional care and a clinic in another village. Ineach of the
categories, they were able to tick "most of the time", "sometimes"
or"Never".22 Regarding the reasons for visiting a private
physician, read further in this sub-chapter.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
13/23
13
Graph Number 2
In response to the question "why did you need another visit?"
87.5% said that
the treatment at the clinic "did not help".
In response to the question "In the past year, have you visited
the emergency
unit with your children?" 32% said that they visited the
emergency unit with
their child in the past year.
In response to the question "In case you visited the emergency
unit, what was
the reason for visiting it?" the women said:
24% due to diarrhea20% due to a high fever
16% due to an unsuccessful treatment by the clinic physician
12% due to dehydration
The rest visited the emergency unit due to a fracture/shortness
of breath/
loss of consciousness/burn/swallowing of a foreign body.
051015202530
Diarrhea
The treatment didn't work
High fever
A fracture
Lack of oxygen
loss of consciousness
Swallowing of a foreign body
Dehydration
A burn
Graph Number 3
Accessibility to Medical Health:
In response to the question "How do you get to the clinic?" 50%
of the women
said that they reach the clinic with the child, on foot, and
that they have no
If you ever visited an additional health care provider who did
you visit?
010203040506070
8090
Private physicianClinic inother village
Same clinic
Emergency care
%
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
14/23
14
other way of reaching the clinic. The women described the
difficulty in
reaching the clinic, especially when the child is ill and they
are forced to
walk a long distance in adverse weather the terrible heat in the
summer and
the rain and harsh cold in winter. They emphasized that it is
especially hard
for pregnant women who are forced to carry their children. The
lack of a paved
road, suitable for walking and/or driving, adds to the poor
accessibility to
the clinic.
In response to the question "What is the walking distance from
your home to
the village clinic?" 51% of the women replied that it takes
between 5-15
minutes, 35% indicated that it takes between 20-40 minutes and
14% indicated
that it takes between 60-120 minutes.
Among the women that reach the clinic by car, 65% mentioned that
it takes
between 10-20 minutes and 35% mentioned a 25-30 minute ride. Due
to the lack
of public transportation in the villages, the women arrive with
their husband
or a relative. One might assume that a large proportion of the
women will notreach the village clinic unless their husband or a
relative drives them and
their children, due to the distance between their home and the
clinic.
Cultural Accessibility (Language):
In response to the question "Do you need help with the Hebrew
language?" 56%
of the women replied that they did. In response to the question
"If so, who
helps you translate?" 53% of the women replied they were helped
by their
husbands or relatives while 24% of the women were helped by the
medical staff
or by passers-by.
Turning to Private Medicine :
Turning to private pediatric medicine is a common, increasing
phenomenon among
the residents of the unrecognized villages in the Negev. The
major reason is
the lack of pediatricians and the limited reception hours in the
village
clinics. The private physicians receive patients at more
convenient hours when
the village clinics are closed in the afternoons, in the
evenings and on
Fridays, thus serving as an alternative solution for visiting
the "Moked"
service center when needed. In addition, the private physicians
offer their
service in Arabic, showing cultural understanding since they
belong to the
same culture. Turning to private medicine is not common only
among the
residents of the villages. Many insured patients turn to it also
when the
services are offered by the public health system. However,
pediatrics is a
trivial service provided in clinics throughout Israel, an
alternative that is
not provided to the residents of the unrecognized villages in
the existing
clinics. Therefore, turning to private medicine is almost an
inevitable
default and many pay for private medicine instead of receiving
the service in
the existing clinics.
Taken from an interview with A' a pediatrician owning a private
clinic:
I opened a private clinic since I could not accept the current
state of
affairs. People are looking for me at home; if I were to receive
patients in
the village clinic people would not come to my home. I did not
intend to open
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
15/23
15
a clinic but people know me and they know where I live. If a
woman comes to me
with her child who suffers from a high fever I cannot send her
home or for
treatment elsewhere when I know how difficult it is for her to
come at such
hours to the village clinic or to the emergency unit. The
emergency unit is
not the solution for her child's condition and it is a shame
that she go there
when it is not needed. In the beginning, people came to my home
and I could
not refuse to provide their children with the treatment; "this
one" knows meand "this one" I have treated in the past. Sometimes,
mothers expect me to
treat their children the same way I treated their neighbor's
son. In the end,
I was forced to open a private clinic. People come to me because
they know I
am a pediatrician and they want to receive the best treatment
for their
children. I feel bad when people pay double to the health fund
and to the
private physician. I thought that the minute I started charging
for the
treatment people would stop coming but that was not the case
they come and
pay".
H', from Assir:
My son had medical problems. When I approached the family
physician in the
village clinic, he gave him a medication and said: "it will
pass." The problem
was not solved, I came back many times and in the end, the child
was admitted
to the hospital, suffering from severe kidney problems. This was
caused due to
a negligent treatment by the clinic doctor. I do not visit the
clinic anymore,
and go straight to a private pediatrician."
In conclusion, the above mentioned findings show a lack of
accessibility of
the village clinic to their residents a lack in specialist
physicians, a
long distance from the village center, limited reception hours
and an
inability to communicate. Therefore, the women turn to
alternative solutions
private pediatricians, clinics in townships where pediatricians
receive
patients and even to the emergency unit.
Half of the women who visit the village clinic report that they
are anyway
forced to turn to another solution with the same problem. About
three quarter
of them, turn to a private physician, a time consuming and
expensive solution.
The main reason for turning to another solution is the feeling
that the family
physician did not solve the problem. Even though this problem
exists outside
the unrecognized villages in the Negev, the high percentage of
those looking
for other solutions, such as visiting the emergency units (a
third of the
women), might indicate problems in communication between the
physician and the
mother (language), a sense of disbelief caused by the fact that
the physician
is not a pediatrician, and a sense that no medical answer to the
patient's
needs is supplied.
This duplication causes not only a waste of time and resources
by the
individual but also a more costly service emergency units and an
economic
burden on the health system in general, due to lacking available
primary
medicine.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
16/23
16
The State's Duty to Realize the Right to Health23
The right to health was anchored in international conventions
signed by the
state of Israel and in local rules: The National Health
Insurance Law and The
Patients Rights Act. According to these, the state is obligated
to make sure
every person residing within its borders has access to medical
services and to
the Underlying Determinants of Health.
Non discrimination and equality constitute repetitive central
motives
throughout the International Covenant on Economic, Social and
Cultural Rights,
ratified by the State of Israel in 1991, as well as in the
general comment 14
of the monitoring committee, concerning article 12 of this
covenant which
deals with health. According to these, the state must ensure,
among others,
non discrimination in accessibility to health services and to
"necessary
conditions" for health.
One of the state's core obligations24
is to ensure that accessibility to health
services will be fulfilled in an in discriminatory fashion to
all, and
especially to vulnerable or marginalized groups. The covenant
outlines the
need to take measures to reduce infant mortality and promote the
healthy
development of infants and children, to prevent infectious
diseases and treat
them, to create health services infrastructure.
The UN Convention on the Rights of the Child (1989) acknowledged
"the right
of the child to the enjoyment of the highest attainable standard
of health"
and stresses that the state should pursue full implementation of
this right
and, in particular, shall take appropriate measures."25
The National Insurance Law came into force in 1995, and set the
rights of the
individual to health services and the state's obligation to fund
these
services. The law's major principles "Justice, Equality and
Mutual Help"
helped in reducing, to some extent, the inequality between
different residents
in Israel.
The Patients Rights Act came into force in 1996, and anchored
the patient's
rights toward the medical factor the physician and the medical
institute.
One of the articles of the law stresses that "a care giver or a
medical
institute shall not discriminate one patient from another based
on religion,
race, sex, nationality, state of origin, sexual tendency or
other."26
Yet, The National Insurance Law and The Patients Rights Act did
not offer a
sufficient response to reducing the inequality between different
residents in
general and between Jews and Arabs in particular. Although every
resident is
entitled, by law, to equal services, in fact there are gaps in
availability
and quality of the services provided in different settlements;
the residents
23This chapter was written by Shlomit Avni-Ouaknine, based on:
Avni, S. (April 2008).PHR-Israel. "The Right to Health among
Arab-Palestinians in Israel: A Comparative
Look."A Report for the International Health Day.24An obligation
the state must endure according to the International Covenant
onEconomic, Social and Cultural Rights, regardless of its
condition.25Convention on the Rights of the Child, 1989, article
24.26High Court Petition 4540/00.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
17/23
17
of the unrecognized villages in the Negev suffer from the
poorest health data
in Israel and poor availability and accessibility to health
services
clinics, family care units, specialist medicine, equipment,
pharmacy services
etc.
It is the state's obligation to reduce the gaps mentioned in
this position
paper health level, availability and accessibility of medical
services and"necessary conditions" for health derived from
international conventions and
local laws. The state's obligation to initiate an active action
to reducing
these gaps also has a medical logic (since it will improve the
health
condition of the Arab-Bedouins in the Negev) and an economic
logic (since an
ill population needs more medical services, more expensive and
complicated
services and "costs" working days, pensions etc.); it is its
human and moral
right.
Summary and Recommendations
The state of Israel, committed to the health of its entire
population does not
provide equal medical services to the residents of the
unrecognized villages
in the Negev in general and to their children in particular. The
existing
services in the few clinics established in the villages, lack
basic services
such as pediatrics and gynecology. This lack is especially
visible due to the
inequality in the range and variety of the services in the
unrecognized
villages compared to adjacent Jewish settlements.
The establishment of the clinics, most of which were built only
after a high
court petition27, is but a partial step towards the realization
of the
residents' right to health. A full realization requires
connecting the
villages to water and electricity and additional necessary
conditions for
health. Yet, this is not enough: the right to health is
connected with the
right to equality, therefore, clinics offering a poorer scope
and variety of
services compared to the services available for residents in
clinics outside
the unrecognized villages, violates the equal right of the
residents of the
unrecognized villages for unified health services. Moreover, The
National
Insurance Law emphasized not only equality but also the value of
justice whichmeans bigger investment in service development
especially where it is most
needed. Since the residents of the unrecognized villages suffer
higher
morbidity and mortality rates, the state must initiate
differential investment
in the building of health services especially among them.
With regards to pediatrics, in many places in the world, the
family physician
is the main caregiver of the child and the pediatrician serves
as his advisor
(in England, for instance). This method has many advantages: one
of which is a
comprehensive understanding of the familys needs. However, the
fact that
there is no pediatrician in the village clinics, where there are
numerous
27High Court Petition 4540/00.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
18/23
18
children, with high morbidity and mortality rates and given the
harsh living
conditions, raises questions and calls for action.
Recommendations for Policy Change28
1) The state must recognize the villages while including them in
the
process.
2) The state must connect the unrecognized villages to all
nationalinfrastructures, especially to the water network. The
clinics must be
connected to the electricity network in order to allow, among
other
things, the refrigeration of medications.
3) The state must act so that the scope, variety and quality of
services
provided in the village clinics are equal to those available in
most
primary clinics in other settlements. Therefore, the state must
provide
the existing clinics with pediatricians and gynecologists and
broaden
the existing services available in the family care units.
4) The state must initiate differential investments especially
in
developing the scope and variety of medical services in the
unrecognized
villages, due to the health data of the village residents.
5) The state must initiate and implement planning programs aimed
for
reducing the morbidity and mortality rates among the residents
of the
unrecognized villages in general and their children in
particular, in a
culturally adapted manner.
6) The medical services must be adapted to the residents'
cultural and
labial needs.
Author: Heijer Abu Sharb Translation from Hebrew: Noga Almi
Research: Heijer Abu Sharb, the "Women Promote Health"
group:Najah Abu-Nadi,
Maliha Al-Nasasarah, Nasra Al-Walidi and Amira Al-Hawashla
Author of the summary and the chapter: "The State's Duty to
Realize the Right
to Health": Shlomit Avni-Ouaknine
Questionnaire writing and analysis of results: Dr. Nadav
Davidovich, Gila
Zelikovich
Data collecting for the survey (interviews using
questionnaires): Amira Abu-
Kuydar, Hana Abu-Kuydar, Asma Abu-Kuydar, Amira Al-Hawashla,
Nasra Al-Walidi,
Sawsan Abu-Kaff, Sabrin Abu-Kaff, Zuhara Abu-Gharbi, Ismahan
Abu-Kuydar
Content editor: Shlomit Avni-Ouaknine
Lingual Editor: Hadas Ziv
This publication was produced with funding from the European
Commission through Oxfam GB. The contents of this document are
the sole
responsibility of Physicians for Human Rights-Israel and can
under no
circumstances be regarded as reflecting the position of the
European
Commission.
28Based on the recommendations submitted to the Goldberg
Committee: Abas, w.Regularization of the Bedouin settlement in the
Negev PHR-Israel's position.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
19/23
19
Appendix: Comparison of the Services Provided in Meitar,
Omer and Lehavim to the Services Provided in Bir Hadaj,
Algrain and Umm-Matnan29
A comparison of the services provided in the Meitar "Clalit"
clinic and the
Bir Hadaj "Clalit" clinic:
Bir Hadaj ClinicNumber of residents 5106 Number of "Clalit"
patients242960% of the residents are under 19
Meitar ClinicNumber of residents 6900 Number of "Clalit"
patients426336.1% of the residents are under 19
RemarksReceptiondays and
hours
Number ofreceptionHours per
Week
Number ofphysician
s
SpecialtyRemarksReceptiondays andHours
Number ofreceptionHours per
Week
Number ofphysician
s
Specialty
Number ofinsuredchildren301564
Number ofchildrenwithchronicillnesses108
000Pediatrics
Number ofinsuredchildren311538
Sun-Fri7:30-12:00,17:00-20:00
382Pediatrics
WednesdayThursday8:00-15:30
Sun-Thu8:30-16:00
552Familyphysician
Sun-Fri6:30-12:00,
17:00-20:00
677Familyphysician
0Gynecologist
Once aweek7:30-11:30
41Gynecologist
55Totalnumber ofhours
109 hoursTotalnumber ofhours
The clinic operates 5 daysa week between 8:00-15:30Lab
servicesTwice a week: Monday,Wednesday 8:30-9:30Family care unit:
twice a
week 8:30-15:30
Additional ServicesThe clinic operates 6 daysa week between
6:30-12:00and 16:30-20:00Lab services 5 days aweek:
7:00-9:30Dietitian twice a week
7:30-11:30 and 16:30-19:30Pharmacy 6 days a weekFamily care 5
times aweek 8:00-11:00, oneevening16:30-19:00
Additional Services
A Comparison of the two clinics reveals gaps in the scope and
the variety of medical
services:
1. The Meitar clinic has two pediatricians with a total of 38
weekly hours while
the Bir Hadaj clinic has no pediatrician at all, despite the
fact that there are
more children in Bir Hadaj according to the "Clalit" health
fund, 64.3% of the
patients are children between the ages of 0-18 (compared to
36.1% in Meitar
between the ages of 0-19. We assume that the percentage of the
children between
the ages of 0-18 insured in the "Clalit" health fund is not
different from their
percentage in the population).
2. The Meitar clinic has seven family physicians with a total of
67 weekly hours
1.57 weekly hours per 100 patients; the Bir Hadaj clinic has two
family
physicians with a total of 55 weekly hours 2.26 weekly hours per
100 patients.
3. Apart from family physicians and pediatricians, the Meitar
clinic has a
gynecologist 4 hours a week. The Bir Hadaj clinic does not have
any at all.
29The number of the residents was calculated on the basis of the
number of residents in2004 (according to data from the Regional
Council for the Unrecognized Villages) whilecalculating the Muslim
population growth in the south in 2004-2006 (according to datafrom
the Central Bureau of Statistics). The number of residents in the
Jewishsettlements is also taken from data from the Central Bureau
of Statistics, referring to
2006.30Calculated according to ratio of residents between the
ages of 0-19 in Meitar (CBS,2006): 36.1% out of 4263 "Clalit"
patients.31The number of patients in the "Clalit" health fund
between the ages of 0-18,according to data received on January 6,
2008, following a correspondence conductedwith Clalit by the group
and PHR-Israel.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
20/23
20
4. The total number of reception hours in the Meitar clinic 109
hours, which are
2.55 weekly hours per 100 patients compared to 2.26 per 100
patients in Bir
Hadaj. It should be noted once more that apart from the larger
number of
physicians' reception hours per capita, the Meitar clinic
provides specialized
physicians in three different fields while in Bir Hadaj the
family physician
receives all the patients, regardless of their medical
needs.
5. The clinic in Meitar is open 6 days a week while the Bir
Hadaj clinic is open 5
days a week.
6. The Meitar clinic gives services all day round both in the
morning and in the
afternoon while the Bir Hadaj clinic is open only until
16:00.
7. The Meitar clinic provides pharmacy and dietitian services,
which are not
provided in the Bir Hadaj clinic.
8. The lab services in Meitar operate 5 days a week for two and
a half hours daily,
while in Bir Hadaj they operate only twice a week for an hour
daily.
9. The family care unit in Meitar operates every morning and
once a week in the
afternoon, while in Bir Hadaj the same service operates only two
mornings a
week.
It should be mentioned that the Meitar clinic is more accessible
to its patients due to
proper infrastructures and public transportation while in Bir
Hadaj the roads to the
clinic are not paved and there is no public transportation.
In addition, it is important to mention that in Meitar the
residents have another
independent "Clalit" clinic (which according to the internet
website of the health fund
"receives patients from Meitar and the South Mount Hebron area
only") as well as a
"Meuhedet", a "Leumit" and a "Maccabi" clinic.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
21/23
21
A comparison of the services provided in the Omer "Clalit"
clinic and the
Algrain "Clalit" clinic:
Algrain ClinicNumber of residents 4267 Number of "Clalit"
patients193160% of the residents are under 19
Omer ClinicNumber of residents 6924 Number of "Clalit"
patients412928% of the residents are under 19
RemarksReceptiondays and
hours
Number ofreception
hours perweek
Number ofphysician
s
SpecialtyRemarksReceptiondays and
hours
Number ofreception
hours perweek
Number ofphysician
s
Specialty
Number ofinsuredchildren1311Number
ofchildrenwithchronicillnesses121
000Pediatrics
Number ofinsuredchildren321156
Sun-Fri6:30-12:00,17:00-19:30
81.54Pediatrics
Sun, mon,wed 8:00-16:00,Tue-8:00-14:00,thu-8:00-
13:00
361FamilyPhysician
Sun-Fri6:30-12:00,
17:00-20:00
129.56FamilyPhysician
000Gynecologist
Once aweek-16:30-19:30
31Gynecologist
36Totalnumber ofhours
214Totalnumber ofhours
The clinic operates 5 daysa week between 8:00-16:00Lab services
- twice aweek: Monday, Wednesday8:30-9:30Family care unit: twice
aweek 8:30-15:45
Additional ServicesThe clinic operates 6 daysa week between
6:30-12:00and 16:30-20:00Lab services 5 days aweek:
7:00-9:30Pharmacy 6 days a week 7:00-11:00 and 16:30-20:00The
clinic providesfetoprotein test on a daily
basis
Additional Services
A Comparison of the two clinics reveals gaps in the scope and
the variety of medical
services:
1. The Omer clinic employs 5 pediatricians and provides 81.5
weekly hours while in
Algrain there is no pediatrician at all, despite the fact that
there are more
children in Algrain according to the "Clalit" health fund 67.8%
of the
patients are children between the ages of 0-18 (compared to 28%
of the entire
Omer population who are between the ages of 0-19. We assume that
the percentage
of children between the ages of 0-18 is not different from its
percentage in the
general population).
2. The Omer clinic employs 6 family physicians and provides
129.5 weekly hours
3.13 weekly hours per 100 patients in Omer; the Algrain clinic
employs one
family physician providing a total of 36 hours 1.86 weekly hours
per 100
clinic patients.
3. Apart from the pediatricians and the family physicians, the
Omer clinic provides
a 3-hour weekly service of a gynecologist while the Algrain
clinic has no
gynecologist.
4. The total reception hours in the Omer clinic are 214, which
are 5.18 hours per
100 patients, compared to 1.86 per 100 patients in Algrain. It
should be noted
once more that apart from the larger number of physicians'
reception hours per
capita, the Omer clinic provides specialized physicians in three
different
fields while in Algrain the family physician receives all the
patients,
regardless of their medical needs.
32Calculated according to the ratio of residents between the
ages of 0-19 in Omer (CBS,2006): 28% out of 4129 "clalit"
patients.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
22/23
22
5. The Omer clinic operates 6 days a week while the Algrain
clinic operates 5 days
a week.
6. The Omer clinic gives services all day round both in the
morning and in the
afternoon while the Algrain clinic is open only until 16:00.
7. The Omer clinic provides pharmacy services, which is not
provided in the Algrain
clinic.
8. The lab services in Omer operate 5 days a week for two and a
half hours daily,
while in Algrain they operate only twice a week for an hour
daily.
9. The Omer clinic provides fetoprotein test 5 days a week, a
service not provided
at all at the Algrain clinic.
It should be mentioned that the Omer clinic is more accessible
to its patients due to
proper infrastructures and public transportation while in
Algrain the roads to the
clinic are not paved and there is no public transportation.
In addition, it is important to mention that there is also a
"Meuhedet", a "Leumit" and
a "Maccabi" clinic.
A comparison of the services provided in the Lehavim "Clalit"
clinic and the
Umm-Matnan "Clalit" clinic:
Umm-Matnan ClinicNumber of Residents 4467 Number of "Clalit"
Patients151960% of the residents are under 19
Lehavim ClinicNumber of residents 5600 Number of "Clalit"
patients351736.5% of the residents are under 19
RemarksReceptiondays and
hours
Number ofreceptionhours per
week
Number ofphysician
s
SpecialtyRemarksReceptiondays andhours
Number ofreceptionhours per
week
Number ofphysician
s
Specialty
Number ofinsuredchildren979Number
ofchildrenwithchronicillnesses65
000Pediatrics
Number ofinsuredchildren1283
Sun-Fri7:00-12:00,17:00-20:00
314Pediatrics
Sun-thu8:00-15:30,
36.51FamilyPhysician
Sun-Fri7:00-12:00,
17:00-20:00
494FamilyPhysician
000Gynecologist
Once aweek-17:00-20:00
31Gynecologist
36.5Totalnumber ofhours
83Totalnumber ofhours
The clinic operates 5 daysa week between 8:00-15:30
Lab services - twice aweek: Monday, Wednesday8:00-10:00Family
care unit: twice aweek tue, thu 9:00-15:30
Additional ServicesThe clinic operates 6 daysa week between
6:30-12:00
and 16:30-20:00Lab services 5 days aweek: 7:00-9:30Dietitian 3
days a week 7:00-12:00 Pharmacy 6days a week 8:00-12:00and
17:00-20:00Family care unit 3 days aweek, mon-tue8:30-12:00, thu
16:00-19:30
Additional Services
A Comparison of the two clinics reveals gaps in the scope and
the variety of medical
services:
1. The Lehavim clinic employs 4 pediatricians who provide 31
weekly hours while in
Umm-Matnan there is no pediatrician at all, despite the fact
that there are 979
"Clalit" patients between the ages of 0-18.
-
8/8/2019 Physicians for Human Rights-Israel: Israels Step
Children Position Paper about the lack of pediatrics in the
Unrec
23/23
2. The Lehavim clinic employs 4 family physicians who provide 49
weekly hours 1.3
weekly hours per 100 patients; the Umm-Matnan clinic employs one
family
physician providing a total of 36.5 hours 2.4 weekly hours per
100 patients.
3. Apart from the pediatricians and the family physicians, the
Lehavim clinic
provides a 3-hour weekly service of a gynecologist while in
Umm-Matnan there is
no gynecologist at all.
4. The total reception hours in the Lehavim clinic is 83 hours,
which constitute
2.35 weekly hours per 100 patients, compared to 2.4 per 100
patients in Umm-
Matnan. It should be noted once more that apart from the larger
number of
physicians' reception hours per capita, the Lehavim clinic
provides specialized
physicians in three different fields while in Umm-Matnan the
family physician
receives all the patients, regardless of their medical
needs.
5. The Lehavim clinic operates 6 days a week while the
Umm-Matnan clinic operates 5
days a week.
6. The Lehavim clinic gives services all day round both in the
morning and in the
afternoon while the Umm-Matnan clinic is open only until
15:30.
7. The Lehavim clinic provides pharmacy and dietitian services,
which are not
provided in the Umm-Matnan clinic.
8. The lab services in Lehavim operate 5 days a week for two and
a half hours
daily, while in Umm-Matnan they operate only twice a week for
two daily hours.
9. The Lehavim clinic provides family care unit services
operating every day while
in Umm-Matnan the services are provided only twice a week.
The accessibility to the Lehavim clinic is also easier than that
in Umm-Matnan due to
proper infrastructures in Lehavim.
It should be mentioned that there are additional clinics serving
the Lehavim community:
"Meuhedet", "Leumit" and "Maccabi".