Embed Size (px)
Citation preview
BERNARD F. PETfINGILL, JR., Ph.D.
Physicians' estimates ofdisability vs patients'reports of pain
Dr. Pettingill is assistant professor of medicine in the section of rheumatology andrehabilitation at Louisiana State University Medical Center. Reprint requests to himthere, /542 Tulane A venue, New Orleans, LA 70//2.
ABSTRACT: The author analyzed data from a survey of 119chronic rheumatoid arthritis patients il1 an attempt to correlate afunctional index scored by physicians and the levels of pain reported by the patients. A close correlation was found between thetwo ratings, except for patients who reported very severe pain.This suggests that in most cases a physician can, by interpretingthe patient's reported level of pain in light of the medical historyand physical examination, accurately assess the patient's level offunctional activity.
Disability and pain have alwaysbeen somewhat subjective and difficult to measure. In particular, itremains uncertain whether there isany correlation between the physician's clinical estimates of a patient's degree of pain and disabilityand what the patient is actuallyexperiencing. With the wide availability of medical and rehabilitative treatment, and with the dependence of insurance payers on physician's assessments, it becomes important to measure whether anysuch correlation exists.
Today, disability is usually inter-
preted in one of two ways: (1) interms of ability to be gainfully employed; or (2) as a comparison between the condition of the disabledperson and that of a healthy personof the same age. Problems aboundin both interpretations.
First, in terms of work capacity, aperson unfit for employment in onejob may be fit for another if thework conditions (e.g., environment,type of work, hours) are altered byconsent between the disabledworker and the employer. The entire definition of "work" changes inlight of these concessions.
Second, a person's disabilitycannot be judged by only one set ofstandards. The level of disability isin many ways controlled by theindividual's ability to adapt tochanging conditions. In short, aperson is well if he or she can carryon usual daily activities; a person isdisabled to the extent that he or shedepends on help from others.
Several studies in Great Britain 1.2
have been aimed at the identification of the disabled population thatdeserves public medical and socialsupport. Recent research in theUnited States has largely focusedon measuring levels of disability ofpatients who are suffering fromvarious diseases. 3
PatientsIn an attempt to clarify the relationship between the identificationof disability by a physician and theindividual's perception of his or herdisability, we undertook a study ofrheumatoid arthritis patients. Arthritis is a major cause of disabilityin the population of developedcountries. It has been described asthe disease that kills the fewest but
DECEMBER 1979 • VOL 20 • NO 12 827

Disability vs pain
cripples the most. More than 5'12million people, or about 10% of thepopulation of England, consult aphysician annually with arthriticcomplaints.4
Our study was based on 119 patients between 20 and 66 years ofage who were admitted to one offour hospitals for the nonsurgicaltreatment of rheumatoid arthritis
The level ofdisability is inmany ways controlled by theindividual's ability to adaptto changing conditions.
in and around Manchester, England. The four different types offacilities are described in a separatepaper,' which also analyzes thecomparative costs and effects of themedical management of these samepatients.
Methods
Four hospital-based consultantphysicians who specialize in thetreatment of arthritis and rheumatism agreed to participate in thestudy. Each consultant was locatedat a separate treatment center. Following the completion of a shortquestionnaire by the physician, patients were admitted to one of thefour facilities for the correctivetreatment of rheumatoid arthritis.The consultant rheumatologist incharge determined the level of disability of his own patients.
Physician assessment
The Steinbrocker FunctionalIndexh was used to assess each patient medically. It has four ratingsof function: incapacitated (4); limited (3); adequate (2); and complete (I). A low score of I indicatesthat the patient is not incapaci-
828
tated; a score of 4 represents complete disability.
Patient assessment
A standard verbal descriptivescale,? pioneered by Keele in 1948and replicated in numerous studies,was modified for use to assess apatient's level of pain. Originally,the scale contained five categoriesor states of pain: (I) none; (2)slight; (3) moderate; (4) severe; and(5) agonizing. For this study, onlyfour categories were used; the category "none" was eliminated andthe category "agonizing" was replaced by "very severe." Reducingthe verbal index categories to fourmade it possible to correlate themdirectly with the categories on theSteinbrocker Index. Since there arepersistent research problems in trying to quantify pain, we simplyasked each patient to assess his painsubjectively and assign it a score ofI to 4.8
Results
Results of Chi-square tests showedthat patients in all facilities weredemographically equivalent andthere were no intergroup differences in number of patients,mean age, sex, social class, age atonset of disease, or duration of disease. Other variables inspected(such as number of joints involvedand joint causing most difficulty)did not bias the results of this study.
The only statistically significantdemographic variable among thepatient groups was the equalnumber of men and women amongthe small patient population at oneof the four treatment facilities. Inthe other three facilities, there werethree times as many women asmen. Most patients (63%) were between 40 and 59 years of age; andon the whole, patients had the dis-
ease an average of 9.5 years. Morethan 50% were middle class, withan equal proportion of lower- andupper-class patients among thefour facilities.
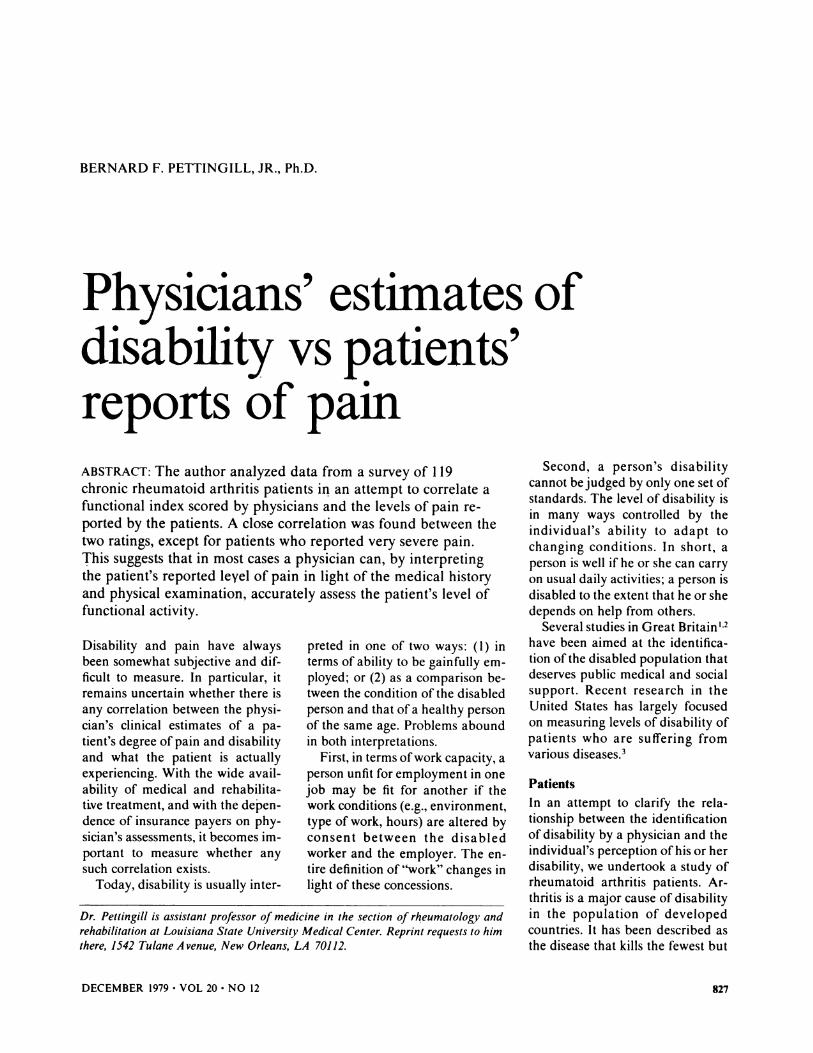
Pain-scale scores
As noted above, each patient, uponadmission to the study, rated himself or herself on a four-point verbal descriptiv.e pain scale. The results are shown in Figure I. Some12 patients rated their pain asslight; 46 patients complaine9 ofmoderate pain; 39 others statedtheir pain was severe; and 22 complained of very severe pain.
Physician's Steinbrocker Index
Figure 2 illustrates the ratings fromthe consultants' Steinbrocker Indexof 119 study patients. This indexwas scored independently of thepatient's verbal index after theconsqltant rheumatologist conducted a complete history andphysical examinatlon on each patient. Fifteen patients were ratedslight; 63 patients were considered
The only significantdiscrepancy was for thosepatients who recorded verysevere pain.
moderately disabled; 35, severelydisabled; and only six, incapacitated or very severely disabled.
Statistical significance
The Chi-square test (with Yate'scorrection) was used to determinethe probability associated with thehypothesis that the ratings from theSteinbrocker Index were not significantly different from those of thepatients themselves. Each categoryof the Steinbrocker ratings was
PSYCHOSOMATICS
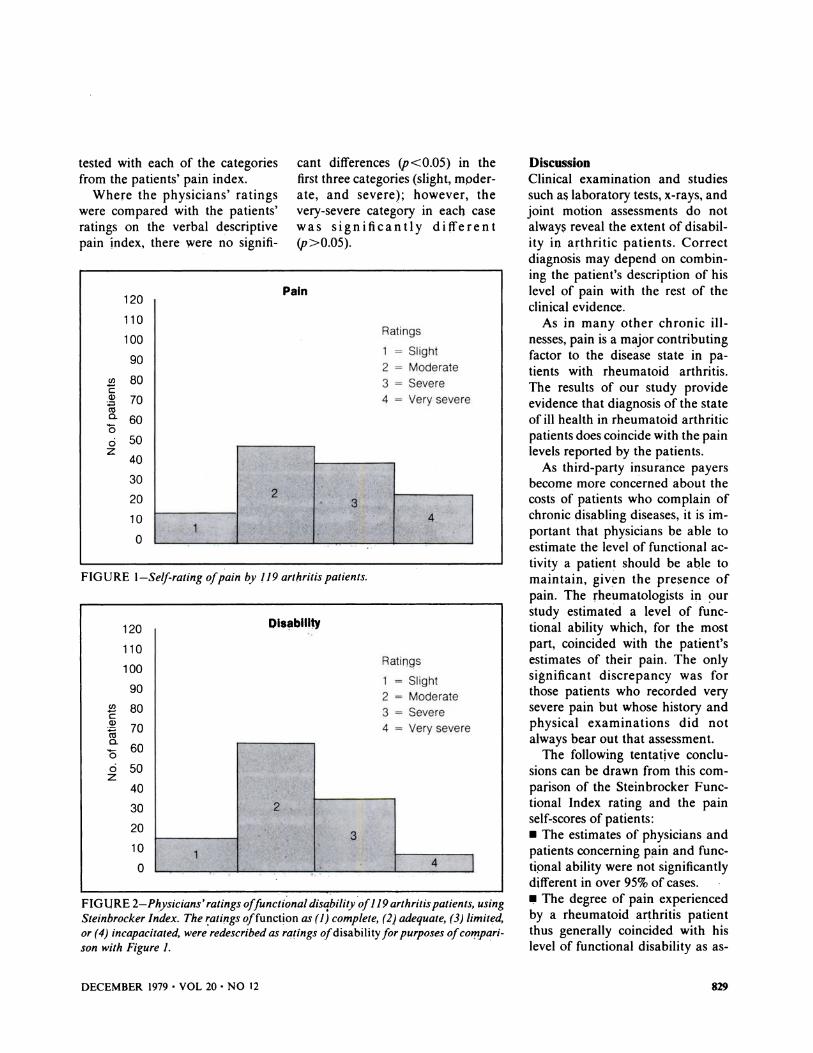
FIGURE I-Selfrating ofpain by 119 arthritis patients.
FIGURE 2-Physicians' ratings offunctional disability of119 arthritis patients, usingSteinbrocker In'dex. The ~ati!lgs offunction as (I; complete, (2) adequate, (3) limited,or (4) incapacitated, were redescribed as ratings ofdisability for purposes ofco",parj.son with Figure 1.
Oisablllw
tested with each of the categoriesfrom the patients' pain index.
Where the physicians' ratingswere compared with the patients'ratings on the verbal descriptivepain Index, there were no signifi-
DiscussionClinical examination and studiessuch as laboratory tests, x-rays, andjoint motion assessments do notalways reveal the extent of disability in arthritic patients. Correctdiagnosis may depend on combining the patient's description of hislevel of pain with the rest of theclinical evidence.
As in many other chronic illnesses, pain is a m<ljor contributingfactor to the disease state in patients with rheumatoid arthritis.The results of our study provideevidence that diagnosis of the stateof ill health in rheumatoid arthriticpatients does coincide with the painlevels reported by the patients.
As third-party insurance payersbecome more concerned about thecosts of patients who complain ofchronic disabling diseases, it is important that physicians be able toestimate the level of functional activity a patient should be aQle tomaintain, given the presence ofpain. The rheumatologists in ~:>ur
study estimated a level of functional ability which, for the mostpart, coincided with the patient'sestimates of their pain. The onlysignificant discrepancy was forthose patients who recorded verysevere pain but whose history andphysical examinations did notalways bear out that assessment.
The following tentative conclusions can be drawn from this comparison of the Steinbrocker Functional Index rating and the painself-scores of patients:• The estimates of physicians andpatients concerning p",in and functipnal ability were not significantlydifferent in over 95% of cases.III!I The degree of pain experiencedby a rheumatoid arthritis patientthus generally coincided with hislevel of functional disability as as-
cant differences (p<O.05) in thefirst three categories (slight, moderate, and severe); however, thevery-severe category in each casewas significantly different(p>O.05).
Pain
Ratings
1 = Slight
2 = Moderate3 = Severe4 = Very severe
2
3I'
14 I
Ratings
1 = Slight
2 = Moderate
3 = Severe
4 = Very severe
2 . 34
1
120
110
100
90
~ 80Q)
~ 70a.o 60ci 50z
40
30
20
10
o
120
110
100
90
en 80~~ 70(\)
a. 60oci 50z
40
30
20
10
o
DECEMBER 1979 • VOL 20 • NO 12 829

Disability vs pain
sessed by a physician. (Note similarity, Figures I and 2.)• Those patients who complainedof very severe pain were not, in theopinion of their physicians, experiencing very severe disability.
The findings of this study implythat the degree of functional activity. or capacity correlates directlywith pain as perceived by the individual patient and so, in most cases,rheumatologists can accurately estimate a patient's functional capacity on the basis of the patient's ownestimate of the severity of hispain. 0
REFERENCES1. Harris AI: Handicapped and Impaired in Great
Britain, pt I. london, Her Majesty's StationeryOffice, 1971.
2. sainsbury S: Measuring Disability. OccasionalPapers on Social Administration No. 54. london, G Bell and Sons, Publishers, 1973.
3. Bush JW, Chen NM, Patrick Dl: Health statusindex in cost effectiveness analysis of PKU.program, in Berg R (ed): Health Status Indexes. Hospital Research and EducationalTrust. Chicago, 1973.
4. Statistical Appendix (1952). Digest of data onthe rheumatic diseases. Ann Rheumatic Dis33(1):103, Jan 1974.
5. Pettingill BF: A Feasibility Study of the Cost-Effectiveness Analysis 01 the Treatment 01 Rheumatoid Arthritis, thesis. University of Manchester, Department of Economics and Social Administration, 1977
6. Steinbrocker 0, Traeger CH, Butterman RC:Therapeutic criteria in rheumatoid arthritis.JAMA 140:659-662, 1949.
7. Huskisson EC: Measurement ot pain. Lancet2:1127-1131, Nov 9,1974.
B. ZbOrowski M: Culture components in responseto pain. J Social Issues 8:6-19, 1952.
830
Academy
of Psychosomatic Medicine
Best Journal PaperAwards 1978-79
Each year the Academy of Psychosomatic Medicine presentsan award for the best paper published in Psychosomatics. Thisyear's winner was chosen from papers published from JUly 1978through June 1979. The award committee is appointed by theEditor in Chief of the Journal and the President of the Academy.The winner and runners-up are:
Winner:DiHerential diagnosis of somatopsychic disordersRichard C.W. Hall, William P. Gruzenski, and Michael K.PopkinJune 1979
Second Place:Ventricular premature beats, stress, and sudden deathRegis A. DeSilva and Bernard lownNovember 1978
Third Place:The liaison psychiatrist: Social role and statusPaul C. MohlJanuary 1979
Honorable Mention:Emotional stress as a factor in ventricular arrhythmiasPatrick T. Donlon, Arnold Meadow, and Ezra AmsterdamApri/1979
Blepharospasm: Organic or functional?Jesse O. Cavenar, Jr., Ingrid J. Brantley, and Ernest BraaschOctober 1978
PSYCHOSOMATICS





























