Embed Size (px)
Citation preview
Physician assessment and revalidation in the UK
Regional Health Regulation Conference - Dubai23 October 2014
Niall DicksonChief Executive and Registrar, GMCChair, IAMRA
A safety critical industry?
• Institute of Medicine in the US estimates that Healthcare is 10 years behind other safety critical industries (2000)
• Errors difficult to detect• Poor history of reporting serious
incidents• High levels of litigation –
individuals and institutions defensive
• Poor history of reporting incompetent colleagues
• Blame culture • Management focus on volume• High levels of trust among
consumers• Major asymmetry in knowledge
and understanding
Early moves to tackle safety
• To Err is Human (1999) • An Organisation with a Memory (2000)• The Bristol Inquiry (2001)• Iatrogenic Injury (2001)
To Err is Human Institute of Medicine 1999 An Organisation with a Memory Department of Health 2000 The Bristol Inquiry HMSO 2001 Iatrogenic Injury Commonwealth Government of Australia 2001
Revalidation – what is it & what does it mean?
UK Revalidation - is the process by which doctors are required to show on a regular basis that they are up to date and fit to practise.
aka: relicensure, recertification
In the past, UK professional regulation was only interested in a doctor’s competence at the point of registration, or when concerns/complaints were raised.
UK Revalidation is part of a wider employer-led system of improved clinical governance and oversight, that is designed to give ongoing assurance that every doctor is competent and fit to practise.
The system is intended to drive safety around both individual doctors and systems
Sir Cyril Chantler, Julia Fullerton Batten, National Portrait Gallery, 2006Lancet 2001vol 353 (1999), p 1181
Revalidation – why do we need it?
’Medicine used to be simple ineffective and relatively safe. It is now complex, effective and potentially dangerous’
The capacity to do good is greater
The capacity to do harm is also greater
Trust is the foundation of medical practice – it needs to be reinforced
The medical register can move from being an historical record of educational achievement to a contemporary affirmation of competence
Every other safety industry checks its people
Every major business throughout the world uses appraisal and systems of performance management

How does Revalidation drive improvement? Revalidation has three clear aims
Bring all doctors into a governed system – including lone
practitioners, basic trained doctors, peripatetic locums
Help to identify problems earlier
Encourage self reflection
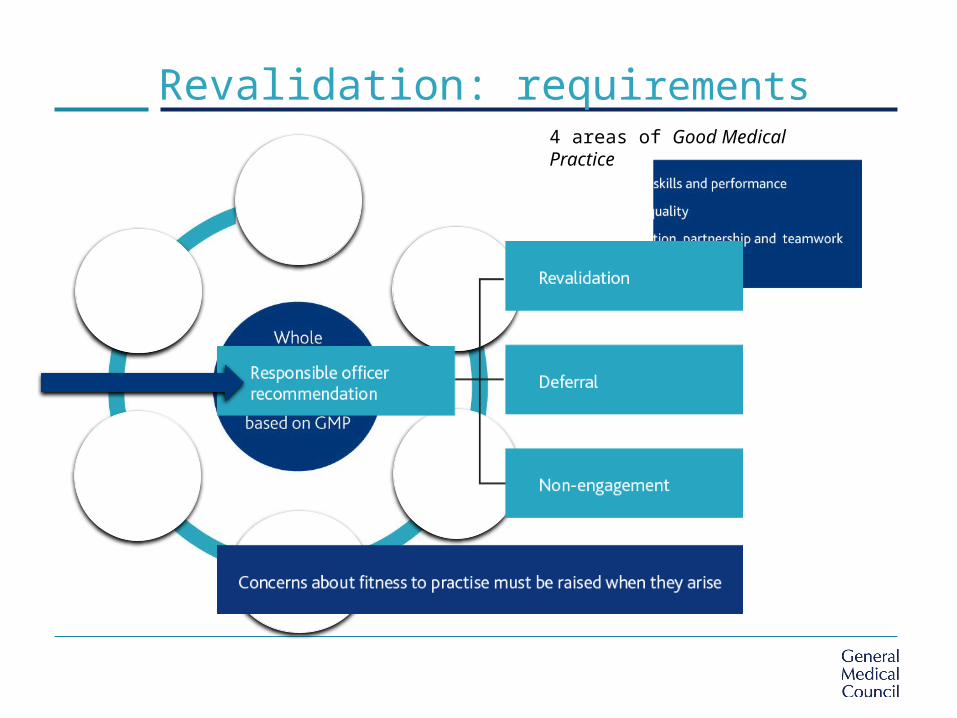
Revalidation: requirements4 areas of Good Medical Practice
Rolling out the Revalidation process

Where are we now? The numbers
Doctors subject to revalidation in the UK: 229,555
GMC figures, as at 10 October 2014
all UK doctors
recommendations
recommendations received by the GMC: 85,509
number of doctors revalidated: 67,911
number of deferrals: 14,984
number of doctors not engaging with their Responsible Officers: 79
revalidated doctors
deferred doctors
non-engaged doctorsWe have removed 664 licenses from
doctors who have failed to engage with the process at any stage

Revalidation – early days
“Big improvement in quality with the advent of
revalidation” -Responsible officer
“These are early days. As we develop better systems and
introduce new practices and embed them, we are getting
better at this. Inevitably doctors complain, at times, that
this is just about ticking boxes. My approach has been to
make appraisal a part of quality improvement” – Responsible
officer
The Early Benefits and Impact of Medical Revalidation, Revalidation Support Team Report, March 2014

Engaged doctors leads to greater patient safety
Appraisal rates are going up.
Doctors are starting to recognise the value of Revalidation as an affirmation of competence and fitness to practise
Nath, V, Searle, B, Kaur, M, The Kings Fund, Medical revalidation From compliance to commitment, March 2014
2011 - 63.3%
2012 - 72.7%
2013 - 76.1%
2014 - 83.8%
20.5% increase since March 2011
NHS England, October 2014, excludes doctors in training
‘Revalidation has started to create a level playing field for doctors within organisations, a change that was particularly relevant for those groups who have traditionally felt marginalised.’
Kings Fund report: Revalidation - The early experiences and views of responsible officers from London, Author: Vijaya Nath, October 2013
Revalidation: early reports
Evidence also shows there is: An increased focus on the quality
of appraisers and the appraisal process
Indicative signs that concerns about a doctors practice are being identified at an earlier stage
Strong support for the system among ROs and appraisers
A change in the views among doctors
The Early Benefits and Impact of Medical Revalidation, Revalidation Support Team Report, March 2014
Revalidation – early impact
The GMC has suspended approval of
revalidation recommendations in two
organisations after concerns about
the robustness of the process
50% increase in doctors giving up
their licence to practice since 2012 -
doctors choosing not to be part of the
system
855 deferred due to local processes
686 deferred because they are under
GMC investigation or in our processes
GMC figures, as at 10 October 2014
How will we know it is working?
Peninsula Medical School undertaking a major research
project to evaluate Revalidation.
http://www.gmc-uk.org/Evaluating_the_strategic_impact_of_medical_revalidation.pdf_55293756.pdf
Does revalidation help identify potential concerns earlier?
How are GMC guidelines on appraisal being applied in practice and how might they be improved?
What level of involvement do patients want in the Revalidation process?
Has the process of collecting the supporting information and the appraisal process increased doctors’ levels of reflection?
The future of Quality Improvement
Revalidation can:
lead to better support for doctors to engage in PDP
foster belief in doctor’s own development
give greater transparency and assurance for patients
deliver safer and better care
be a driver for quality improvement
Moving towards Revalidation must be seen as part of the
wider quality movement within healthcare in the UK
Not just a tick box exercise for doctors
Data collection and critical analysis for ongoing improvement

Most systems based on CPD rather than assessment of competence.
UK – GMC model for doctors is new and will be evaluated and revised. NMC currently consulting on process for nurses.
US – ‘Relicensure’ being considered by FSMB. Speciality specific models (ABIM) already in place.
AUS – 1st phase unsuccessful. Commitment to revisit - change 3-6 years away.
UAE – Abu Dhabi and Dubai are looking to develop their own model.
IAMRA – will be producing reports, exploring different models worldwide and encouraging exchanges of information
Other models of revalidation