Embed Size (px)
Citation preview

1
Physical Therapy Management After Minimally Invasive Hip Replacement in
the Acute Care Setting: A Case Study
Jennifer Manz, SPT, Suzanne Ryer, PT, MPT
2
Background and Purpose. Hip osteoarthritis is the most prevalent cause of
debilitating pain within the general population. When this condition becomes
severe enough where it is not responding to conservative treatment, surgical
management may be required. Minimally invasive hip replacements have been on
the rise due to muscle sparing, allowing for fast recovery. Therefore, the purpose of
this case report is to describe physical therapy management and outcomes of
patients after two unique minimally invasive hip procedures.
Case Description. A 61-year old woman underwent a right direct anterior hip
replacement, and a 77-year old woman underwent a left supercapsular hip
replacement. Both patients required surgical intervention due to deteriorating
joints caused by osteoarthritis. They were to receive physical therapy treatment in
the acute care environment in order to address related impairments from surgery,
which would help them regain functional independence for safe and appropriate
discharges home.
Outcomes. Hip range of motion, hip strength, balance, walking distance, gait speed,
and functional independence disability measures were generally better for the
patient who underwent the direct anterior hip replacement. However, both patients
were able to regain functional independence during bed mobility, transfers,
ambulation, and stair negotiation for safe discharges home within two to three days
after surgery without complications.

3
Discussion. Both patients who underwent minimally invasive hip replacements to
preserve gluteal musculature demonstrated positive outcomes in the acute care
environment. In conjunction with physical therapy management, both
demonstrated minimal postoperative pain, speedy return to functional activities,
limited length of stay in the hospital, and high patient satisfaction with outcomes
after minimally invasive hip replacement surgery.
4
Background and Purpose
Osteoarthritis (OA) is the most common musculoskeletal disease, which results in
progressive degeneration of a joint and loss of articular cartilage. It is estimated by
the World Health Organization that 10% of the world population over the age of
sixty has clinical symptoms associated with OA. 1 Hip OA has been identified as the
most prevalent cause of debilitating pain within the general population, resulting in
decreased mobility, quality of life, and ability to perform activities of daily living
(ADLs). When this condition becomes so severe that it does not respond to
conservative treatment, surgical management may be required.2
New methods for total hip arthroplasty (THA) known as minimally invasive
surgeries (MIS) have been on the rise in recent years. Currently, there is consensus
on multiple benefits of this technique over standard approaches including better
pain management, use of rapid recovery protocols, and low complication rates.3
Howell et al. determined the use of MIS allows for high patient satisfaction,
decreased bleeding, faster recovery of function, and decreased length of hospital
stay.4 Goosen et al. found a statistically significant advantage of MIS to standard
approaches regarding Harris Hip Scores with better scores with pain, walking
distance, stairs, gait, and range of motion at both six weeks and one year after
surgery.5
Two types of MIS are a direct anterior approach and a supercapsular approach. The
direct anterior approach is a specialized technique that provides stability of the
5
femur through a single incision, promoting minimal posterior soft tissue dissection.
This technique prevents dislocation and allows rapid muscle recovery through
preserving abductor musculature.6 While literature is limited in describing physical
therapy outcomes after the direct anterior approach, an article by Mayr et al. found
quick return to normal gait function. By twelve weeks, patients had improved
cadence, walking speed, single limb support, stride length, and total hip motion in
the sagittal and frontal planes as compared to patients with an anterolateral
approach.7 Taunton et al. found that muscular and functional recovery of patients
after a direct anterior approach was significantly superior compared to an
anterolateral or posterior approach. Patients with the direct anterior approach had
decreased perioperative pain, early postoperative function including walking time
and less reliance of an assistive device, and high patient satisfaction.8 Another MIS
includes the supercapsular approach, which has a capsular incision providing
“micro-superior” access to joint space. This technique promotes external rotator
sparing to prevent posterior dislocation. While this approach has had
approximately seven years of clinical success, there is no current literature looking
at patient outcomes. It has been noted that there are low complication and
dislocation rates with accelerated recovery, however authors have not yet looked
into therapy outcomes postoperatively.9
While literature has looked at outcomes of patients who have had a MIS a few weeks
to a year postoperatively, there currently is no research that describes outcomes of
patients in the acute environment. There is also limited evidence comparing
6
immediate outcomes of patients after a direct anterior approach versus a
supercapsular approach for hip replacement. It is important to look at outcomes in
an acute environment after hip surgery to determine a typical postoperative
functional status of patients in order to choose the best discharge disposition.
Therefore, the purpose of this case report is to describe physical therapy
management and outcomes of two patients, one after a direct anterior hip
replacement, and the other after a supercapsular hip replacement.
Case Description
Patient 1-History and Systems Review
The patient was a 61-year old female who underwent a right direct anterior THA. A
thorough chart review revealed a past medical history of resolved depressive
disorder, resolved adjustment disorder, and a resolved colon malignant neoplasm.
She was a non-smoker with normal BMI and lived an active lifestyle prior to her
worsening pain. The postoperative note reported no complications, range of motion
(ROM) within functional limits, and symmetrical leg length. She reported she was
able to function at an independent level with all ADLs and maintain fulltime
employment before the THA. She had constant 8/10 pain with any movement,
however functioned through the pain. She verbalized her wish to return home at
discharge with her husband, where she would have to negotiate a flight of stairs to
the basement to perform laundry.
Clinical Impression
7
The patient was a 61-year old functioning at an independent level prior to THA with
a healthy lifestyle. With the ability to perform all activities on her own prior to
surgery, it appeared that she would be able to fully participate in physical therapy
sessions with an excellent outcome provided no other medical complications. It
appeared she would not have any difficulties with the healing process provided her
limited medical history. Given her willingness to get out of bed and perform
functional activities on her day of surgery, it was determined that she would have a
good rehab potential and a discharge home was expected.
Patient 2-History and Systems Review
The patient was a retired 77-year old patient who underwent a left supercapsular
THA. A thorough chart review revealed a past medical history of hypertension and
postoperative nausea. The patient was a non-smoker with normal BMI who was
active prior to surgery. The postoperative note reported no complications, ROM
within functional limits, and symmetrical leg length. She was agreeable to
participate with PT, however complained of nausea and fatigue. The patient
reported she was able to perform all ADLs independently prior to surgery, with the
exception of being modified independent with stairs, ambulation in the house and
community, lower extremity dressing, and household chores due to pain. Her MD
put her at 50% weight-bearing in January 2012 due to her quickly deteriorating
joint. She verbalized her goal was to return home with her husband at discharge.
Her home environment would require negotiating four stairs with bilateral railings
into the house.
8
Clinical Impression
The patient had good functional mobility prior to surgery and was a non-smoker
with a relatively uncomplicated past medical history, however may be slightly
limited by postoperative nausea. The patient’s age would also suggest a possible
slower progression throughout physical therapy treatment. However, with the
support of her husband, her overall rehab potential was good and a discharge home
was expected.
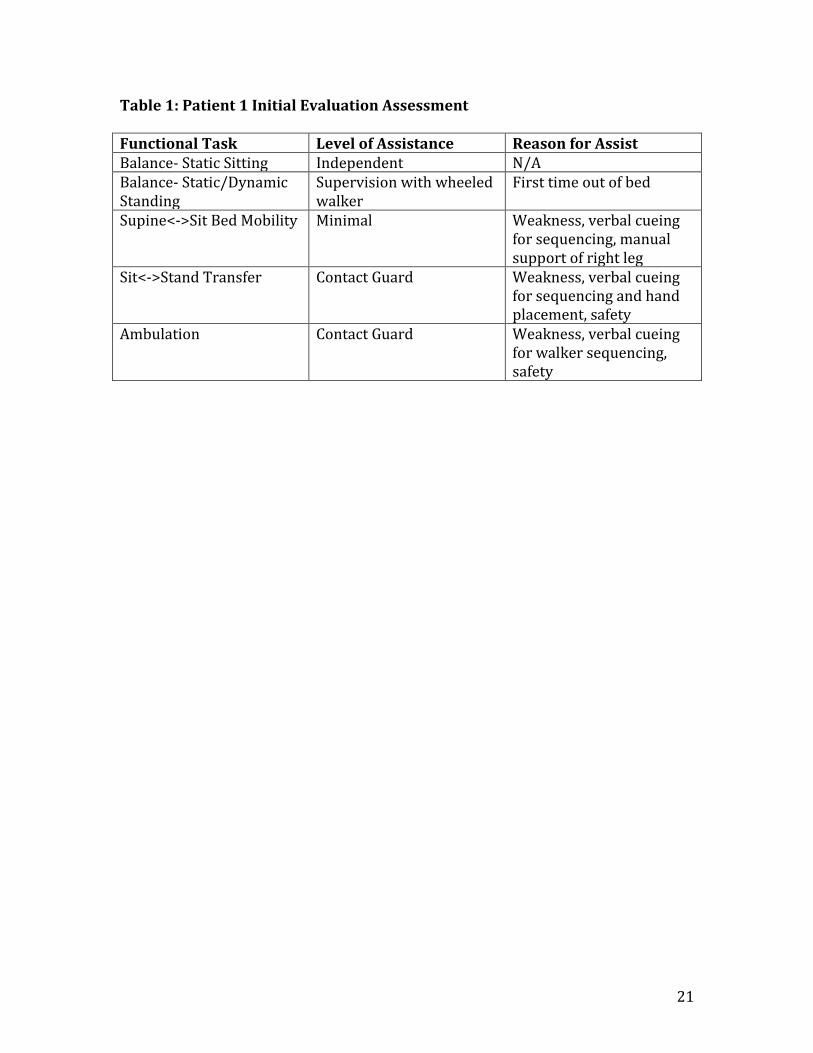
Initial Examination
Patient 1
The patient reported pain at rest at 1/10 on the validated Numerical Rating Scale
(0=no pain, 10=worst imaginable pain) as a dull ache10. Upon observation, the
patient had typical post-surgical edema in the right hip. The patient was educated
on her WB as tolerated status and safe zone precautions after her surgery including
no hip flexion past 120°, avoiding extreme end-ranges, and no combinations of
movements.
The patient was observed to have bilateral upper extremity and left lower extremity
ROM within functional limits. It has been determined that visual measurements are
in good agreement with goniometric measurements for hip ROM.11 A strength
screen was performed on the left lower extremity per Reese12, which has been
determined to be a valid and reliable method to assess strength13. The right lower
extremity was not formally assessed on the day of surgery, however ROM and
9
strength were limited based on visual assessment. Upon gait assessment, the patient
utilized a step to pattern with decreased stance time on her right leg while
ambulating ten feet with a wheeled walker. Currently, there is not a systematic
approach to determine the reliability of gait analysis14. A complete assessment of
level of assistance with functional tasks is noted in Table 1. Due to lethargy and
weakness, evaluation was completed at this time. Pain with activity was unchanged
compared to rest.
Patient 2
The patient reported pain at rest at 0/10 on the Numerical Rating Scale (0=no pain,
10=worst imaginable pain). Upon observation, the patient had typical post-surgical
edema in the left hip. The patient was educated on her weight bearing as tolerated
status and safe zone precautions after her surgery including no hip flexion past
120°, avoiding extreme end-ranges, and no combinations of movements.
The patient demonstrated bilateral upper extremity and right lower extremity
strength and ROM within functional limitations. The left lower extremity was not
formally assessed on the day of surgery, however ROM and strength were limited
upon visual assessment due to patient fear of damaging the new hip. Upon gait
assessment, the patient utilized a step to pattern with decreased stance time on her
left leg while ambulating twelve feet with a wheeled walker. A complete assessment
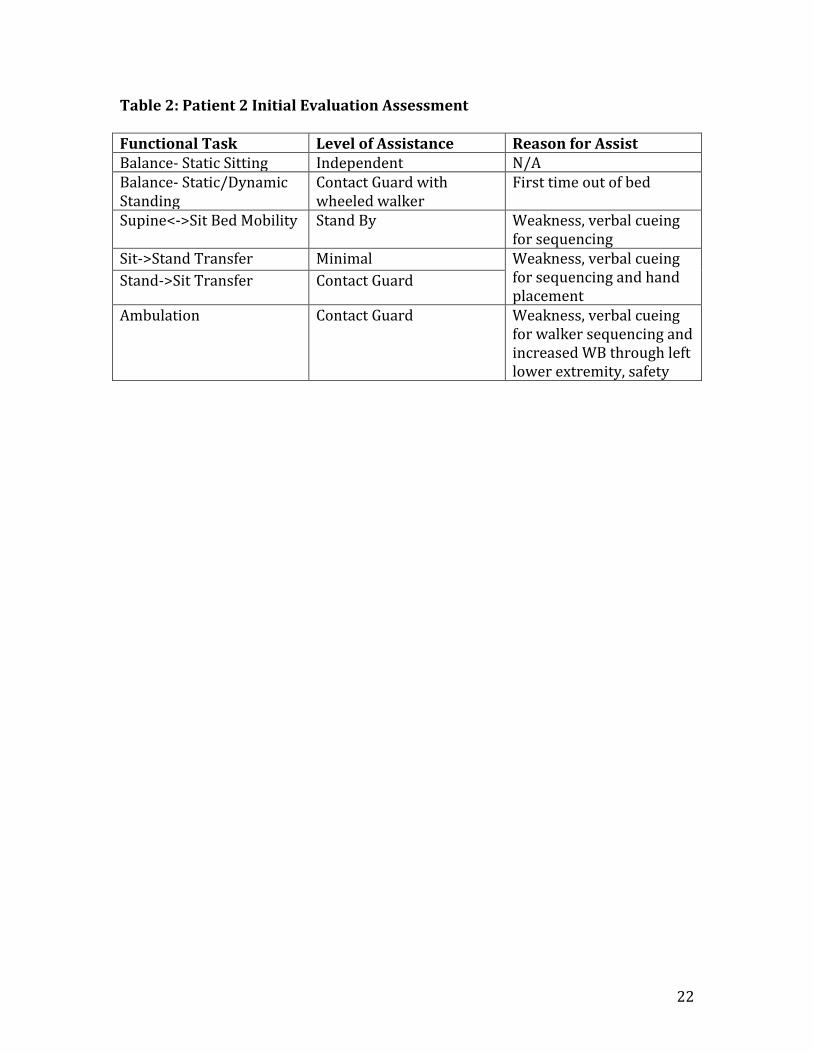
of level of assistance with functional tasks is noted in Table 2. The patient
10
completed five standing marches, which completed the evaluation. Pain with
activity was unchanged from rest.
Clinical Impression
Both patients presented with swelling, decreased ROM and strength, balance
deficits, decreased activity tolerance, endurance, and safety awareness, which
limited bed mobility, transfers, ambulation, stairs, and car transfers. The following
goals were created: Modified independence with home exercise program, bed
mobility, transfers, ambulating 150 feet with wheeled walker, and negotiation of
stairs with least restrictive assistive device, as well as the ability to demonstrate
understanding of a proper car transfer technique. The plan of care included seeing
the patients two times per day for 3-4 days and included functional training,
strengthening, ROM, endurance training, patient/family training, equipment
evaluation, bed mobility, gait training, continued evaluation, stair retraining,
neuromuscular re-education and safety education.
Intervention
Both patients who underwent MIS were involved in a physical therapy treatment
program consisting of functional training, neuromuscular re-education, and a
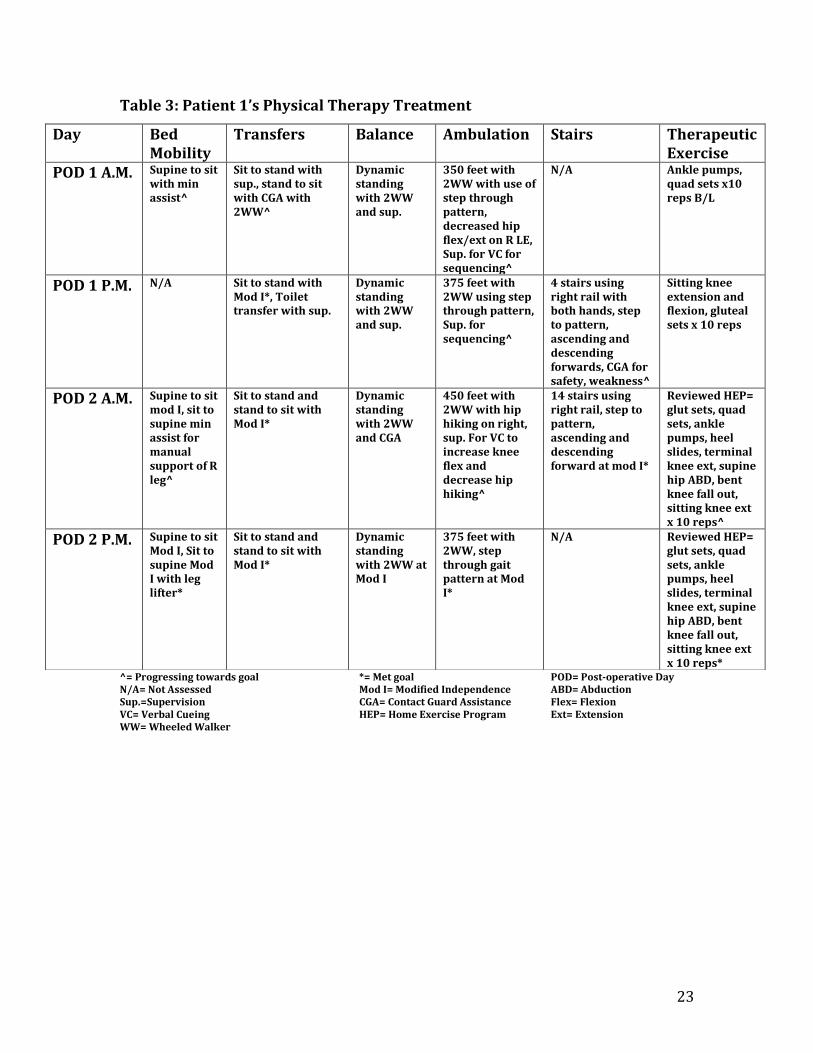
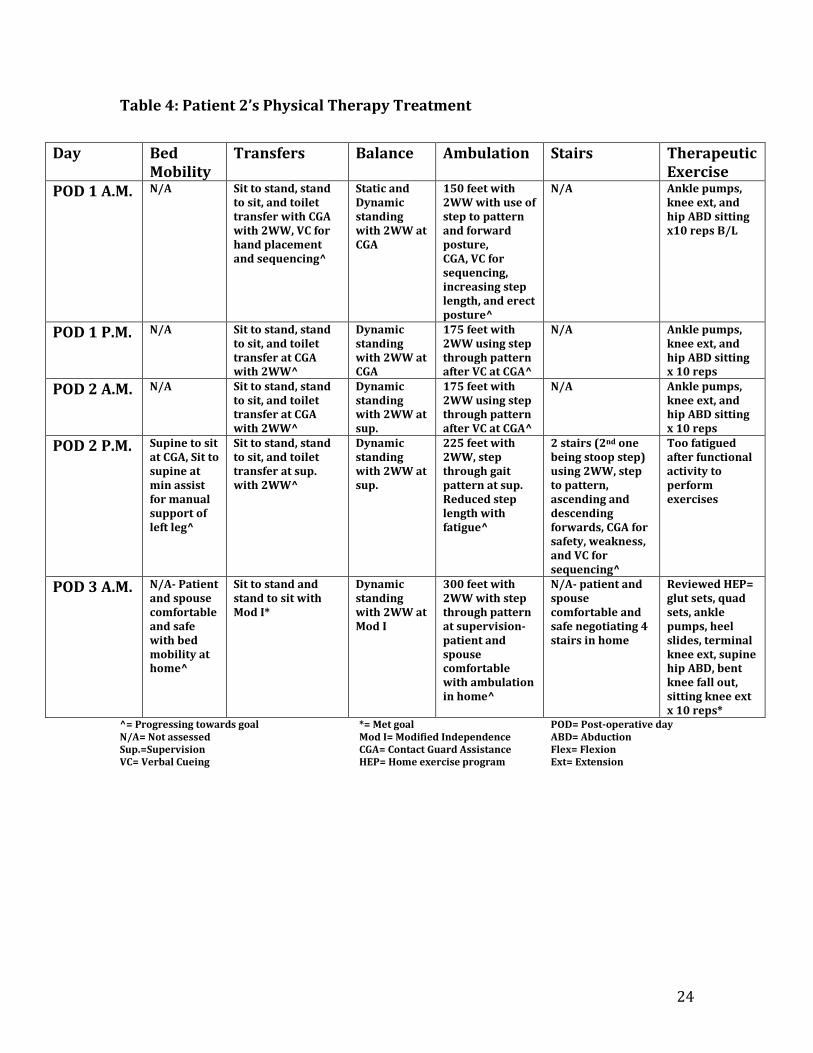
therapeutic exercise program. A detailed outline of daily physical therapy
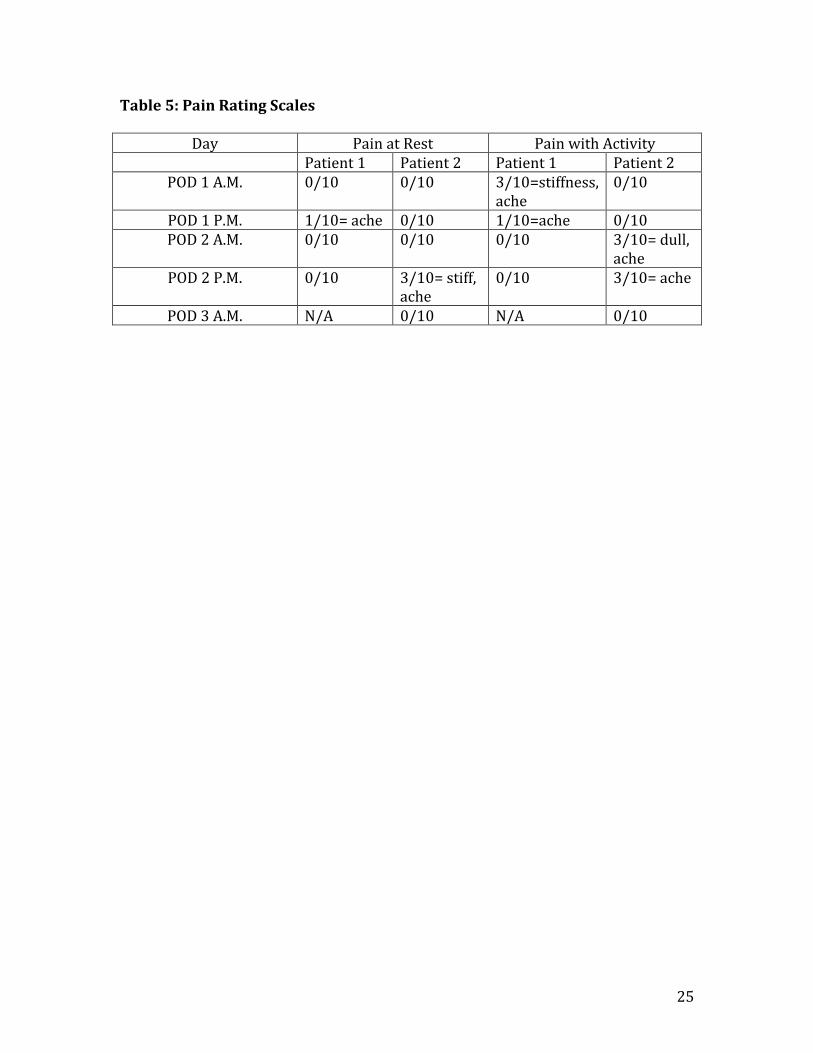
treatments for both patients is shown in Tables 3 and 4. Pain levels at rest and
during treatment sessions are outlined in Table 5.
11
Functional Training
Functional training was incorporated to prepare and determine their safety and
readiness for home. Bed mobility, transfers, ambulation, and stair negotiation were
included in both of the patients’ plan of care prior to safe discharge. It has been
determined that progressive functional training is a safe and effective treatment
method that should be incorporated to increase strength and functional
performance during the rehabilitation process of patients after hip surgery.15 With
an improvement in functional performance, a patient may have increased readiness
to return home with confidence due to an improved quality of life.
Neuromuscular Re-education
Neuromuscular re-education was utilized to address static and dynamic balance
during sitting and standing. Balance is an important aspect after hip surgery
because balance deficits are known to be a predictor of severe walking disability.14
In order to improve balance, other tasks were included during ambulation such as
head movements and engaging in dual task performances such as walking and
talking at the same time.
Therapeutic Exercise
ROM and strength exercises are significant in acute care after THA to maintain
flexibility, relieve stiffness, and improve muscular strength for functional tasks.
When strength falls below a particular threshold, functional performance can
progressively deteriorate. Bed rest further compromises strength after orthopedic
12
surgery, so it is imperative to prevent a decrease in muscle performance.
Progressive resistance training can produce a significant increase in functional
performance including walking speed.14 With the exercises noted in Tables 3 and 4,
hip and knee musculature were activated to prevent atrophy and maintain muscle
performance for functional tasks including transfers, ambulation, and stair
negotiation.
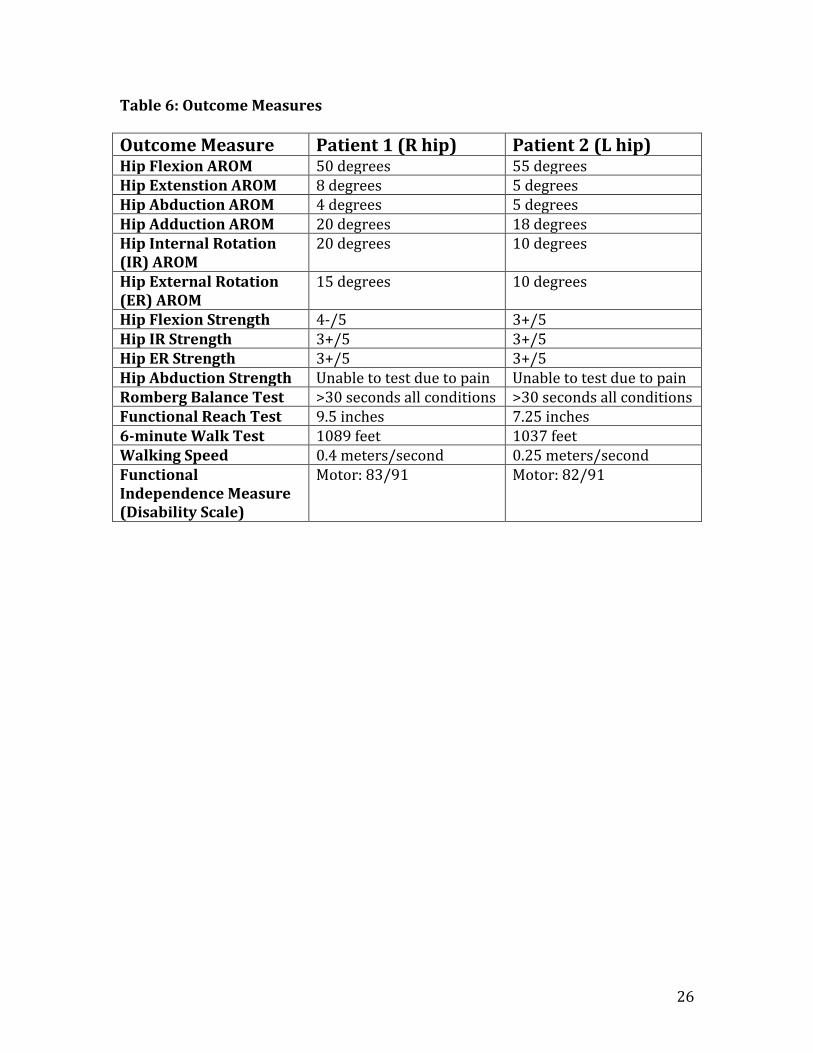
Outcomes
Outcome measures included pain, ROM, strength, Romberg and Functional Reach for
balance, gait speed, walking distance, and the Functional Independence Measure
(FIM) disability scale. Both patients made adequate functional gains to be
discharged home. Patient 1 was discharged in the afternoon on postoperative day
(POD) 2, whereas Patient 2 was discharged in the morning of POD 3. The discharge
time was determined by patient readiness and surgeon approval. Pain levels at the
final session were 0/10 for both patients. All other outcome measures are noted in
Table 6. On the day of discharge, Patient 1 reported it was unbelievable how well
she was able to move pain-free after surgery. She described that prior to surgery,
she was unable to move at all without constant 8/10 pain. Patient 2 reported
similar improvements in function including the fact that she felt unlike she had in
years without postoperative pain.
Measurements of hip ROM were done with a one degree incremented goniometer
per Norkin and White.15 Intratester reliability for hip ROM according to Ellison et al
13
is 0.96-0.99 for internal and external rotation, and varies significantly for other
measurements.15 The active ROM measurements for both patients were fairly
comparable, however Patient 1 displayed higher measurements for hip extension,
adduction, internal rotation, and external rotation, while Patient 2 had better
measurements with hip flexion and abduction. Strength measurements taken per
Reese were fairly similar in both patients with the exception of Patient 1 having
slightly higher hip flexion strength.
The Romberg Test is used to measure static balance. The test-retest validity for
those greater than 55 years-old is 0.76 with eyes closed and 0.90 with eyes open.16
Both patients were able to complete all four tasks for greater than thirty seconds,
showing no increased risk for falls. The other balance test used to determine safety
and readiness for home was the Functional Reach. It has been determined that it is
a useful clinical measure for detecting balance impairment and change in balance
performance over time.17 Both patients were able to forward reach greater than six
inches, showing no increased risk for falls.
Functional walking capacity was measured through the 6-minute walk test
described by the American Thoracic Society18. There is no optimal reference range
that describes the necessary distance for independent and functional ambulation
after THA. As shown in Table 6, Patient 1 was able to ambulate fifty feet further
than Patient 2. It is important to note that both patients ambulated with wheeled
walkers. Walking speed is a reliable, valid, sensitive, and specific measure that is
14
utilized to determine functional status, appropriate discharge disposition, and fall
risk. Following Fritz and Lusardi’s walking speed times related to function, Patient
1 ranked as a limited community ambulator needing intervention to reduce fall risk
with a likely discharge home. Patient 2 ranked between a limited community
ambulator and household ambulator needing intervention to reduce fall risk with a
likely discharge home.19
Lastly, the FIM was used as a disability scale based on the International
Classification of Impairment, Disabilities, and Handicaps. This scale measures the
amount of assistance that is required for an individual to carry out ADLs. There is
excellent test-retest reliability (ICC=0.90) for the motor aspect of the FIM in elderly
adults.20 Both patients were ranked at an Independent or Modified Independent
level of assistance for self-care tasks, sphincter control, transfers, and locomotion.
Discussion
The purpose of this case report was to describe functional outcomes of patients
after unique minimally invasive hip replacements prior to discharge from the acute
care environment. The outcomes observed in Patient 1 after the direct anterior
approach are consistent with the minimal literature that is currently available on
MIS. Similar to the outcomes described by Taunton et al., Patient 1 had minimal
postoperative pain, high patient satisfaction, and a speedy postoperative return to
function.8 She was able to perform all functional activity within one day of surgery
and her pain was controlled from 0-3/10, allowing her to fully participate in
15
physical therapy treatment. By POD 2, she met all goals required for a safe return
home including bed mobility, transfers, ambulation, stair negotiation, and
demonstration of a car transfer. She had a normal gait pattern using the wheeled
walker including equal stride length, appropriate walking speed, equal percent of
single leg support, and normal cadence prior to discharge, which is similar to the
findings suggested by Mayr et al. The outcomes of this case study differed from
Mayr’s findings as Patient 1 had decreased total hip motion in the sagittal and
coronal planes. It is hypothesized that this may be due to stiffness in the right hip
prior to ambulation or minor apprehension during ambulation due to fear of
increasing pain levels with full WB similar to preoperative ambulation.
Outcomes found with Patient 2 after the supercapsular approach are similar to the
outcomes described in current literature about MIS. Positive outcomes found with
this patient included high patient satisfaction, limited bleeding, limited length of
stay in the hospital, and fast functional recovery, similar to findings by Howell et al.4
Patient 2 ambulated a functional household distance of 150 feet POD 1. She
completed negotiation of two stairs with a wheeled walker with limited assistance
for safety on POD 2. Although Patient 2 was still progressing towards her goals for
ambulation and stair negotiation on POD 3, she and her husband felt safe and
comfortable with these functional tasks to return home.
When comparing outcome measures observed upon discharge of both patients,
Patient 1 generally had higher scores than Patient 2, even if minimal. There may be
16
several reasons for her apparent higher functional level. First, Patient 2 reported
anxiousness during functional tasks due to fear of damaging her newly replaced hip.
This may have led to reduced weight bearing and stance time on her surgical leg,
which would decrease step length and limit her walking distance and gait speed.
Another factor that may have played a role were the different age demographics.
Patient 2 was sixteen years older than Patient 1, suggesting she had more age
related changes affecting recovery. Some of these factors include decreased bone
mass, less flexible joints due to fluid or cartilage loss, increased fat deposits in
muscle, decreased muscle contractibility, vertebral column mineral loss causing
postural changes, reduced muscle mass, and slowed movement due to unsteady gait
caused by early fatigue. The final hypothesis as to why there may have been
different functional outcomes between patients is within their medical history.
Patient 2 had hypertension, postoperative nausea, as well as a history of falls. She
stated she wanted to take her time during all functional activities with therapy to
reduce the likelihood of becoming nauseous. With a history of falls, she reported
she recently had slowed down her ambulation speed to be more cautious. With
both of these factors in mind, it may have played a role in the 6-minute walk test and
gait speed outcome measures.
Although this description of patient outcomes after MIS was appropriate provided
the patients’ demographics, functional level prior to surgery, and postoperative
functional level, some limitations can be identified. First, some optimal examination
outcome measures were unable to be performed. The first of these include passive

17
ROM due to the surgeon’s protocol of avoiding end-range motions. This would have
been useful to determine if the impaired ROM was due to joint restriction or muscle
weakness. Hip abductor strength was not formally tested due to both patients
reporting pain with the necessary positioning. While visual observation of
trendelenburg sign can suggest gluteus medius weakness, formal muscle testing is
more valid and reliable. The use of a more valid and reliable balance measure such
as the Functional Gait Assessment, Dynamic Gait Index, or Berg Balance Scale was
unable to be used because both patients used a wheeled walker, which may not give
an appropriate functional level on these scales. Patients are required to use a
wheeled walker for a minimum of six weeks after surgery to ensure proper healing
and gait pattern per surgeon protocol. Ideally, an AlphaFIM would have been used
as a disability index for patients in the acute care environment. Unfortunately, it has
limited availability due to being an internet-based product that requires financial
resources. Another limitation includes the different demographics of both patients.
It is difficult to compare functional outcomes with such a difference in age and past
medical history that affects the recovery and healing processes after an orthopedic
surgery. The final limitation is that the FIM was not assessed prior to surgery, and
these pre- and postoperative functional measures could have allowed for more
accurate assessment of improvement in ADLs after surgery.
Future research related to physical therapy outcomes in the acute care environment
after hip MIS is critical to determine the optimal surgical approach and physical
therapy management for fast and functional recovery of patient. In order for this to

18
occur, it would be necessary to look at a higher sample size to compare multiple
patients with similar demographics to promote internal consistency. Having
patients fill out a disability scale prior to surgery would allow for a more
appropriate comparison of preoperative and postoperative functional levels. It
would also be necessary to incorporate patients with standard hip protocols within
a study to compare with patients with MIS, allowing for a functional comparison of
outcomes of patients with less preservation of soft tissue to those who had limited
to no muscle dissection. In order to determine best functional outcomes, long-term
investigations would be ideal to follow the patients after their stay in the hospital
with a 3-month and 6-month follow-up that could look for any post-surgical
complications after the acute care environment.
19
References 1. Pereira D, Peleteiro B, Araujo J, Branco J, Santos RA, Ramos E. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarth Cartilage. 2011;19(11):1270-1285. 2. Dagenais S, Garbedian S, Wai E. Systematic Review of the Prevalence of Radiographic Primary Hip Osteoarthritis. Clin Orthop Relat Res. 2009;467(3):623-637. 3. Malik A, Dorr LD. The science of minimally invasive total hip arthroplasty. Clin Orthop Related Res. 2007; 463: 74-84. 4. Howell JR, Garbuz DS, Duncan CP. Minimally invasive hip replacement: rationale, applied anatomy, and instrumentation. Orthop Clin North Am. 2004;35(2):107-118. 5. Goosen JH, Kollen BJ, Castelein RM, Kuipers BM, Verheyen CC. Minimally Invasive versus Classic Procedures in Total Hip Arthroplasty: A Double-blind Randomized Controlled Trial. Clin Orthop Relat Res. 2011;469(1):200-208. 6. Masonis J, Thompson C, Odum S. Safe and accurate: Learning the direct anterior total hip arthroplasty. Orthopedics. 2008;31(12):129-134. 7. Mayr E, Nogler M, Benedetti MG, et al., A prospective randomized assessment of earlier functional recovery in THA patients treated by minimally invasive direct anterior approach: A gait analysis study. Clin Biomech. 2009;24(10):812–8. 8. Taunton MJ. Direct Anterior Approach for Total Hip Arthroplasty. US Musculoskeletal Review. 2011;6(1):42-45. 9. Chow J, Penenberg B, Murphy S. Modified micro-superior percutaneously-assisted total hip: early experiences & case reports. Curr Rev Musculoskelet Med. 2011;4(3):146-150. 10. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152:2399-2404. 11. Norkin C, White D. Measurement of Joint Motion: A Guide to Goniometry (4th edition). F.A. David Company: Philadelphia;2009. 12. Reese, N. Muscle and Sensory Testing: Second Edition. Elsevier Saunders: St. Louis; 2005: 253-329. 13. Wadsworth, C., Krishnan, R., Sear, M., Harrold, J., Nielsen, D. Intrarater Reliability of Manual Muscle Testing and Hand-held Dynametric Muscle Testing. Phys Ther. September 1987;67(9):1342-1347. 14. Toro B, Nester C, Farren P. A review of observational gait assessment in clinical practice. Physiotherapy Theory & Practice. September 2003;19(3):137-149. 15. Hauer K, Specht N, Schuler M, Bartsch P, Oster P. Intensive physical training in geriatric patients after sever falls and hip surgery. Age Ageing. 2002;31:49-57. 16. Steffen T, Seney M. Test-Retest Reliability and Minimal Detectable Change on Balance and Ambulation Tests, the 36-Item Short-Form Health Survey, and the Unified Parkinson Disease Rating Scale in People with Parkinsonism. Phys Ther. 2008;88(6):733-746. 17. Duncan PW, Weiner DK, Chandler J, Studenski S. Functional Reach: A new Clinical Measure of Balance. J Gerontol. 1990;45(6):192-197. 18. American Thoracic Society. ATS Statement: Guidelines for the Six-Minute Walk Test. Am J Respir Crit Care Med. 2002;166:111-117.

20
19. Fritz S, Lusardi M. White Paper: “Walking Speed: the Sixth Vital Sign”. J Geriatr Phys Ther. 2009;32(2):2-5. 20. Pollak N, Rheault W. Reliability and validity of the FIM for persons aged 80 years and above from a multilevel continuing care retirement community. Arch Phys Med Rehabil. 1996;77:1056-1061.
21
Table 1: Patient 1 Initial Evaluation Assessment Functional Task Level of Assistance Reason for Assist Balance- Static Sitting Independent N/A Balance- Static/Dynamic Standing
Supervision with wheeled walker
First time out of bed
Supine<->Sit Bed Mobility Minimal Weakness, verbal cueing for sequencing, manual support of right leg
Sit<->Stand Transfer Contact Guard Weakness, verbal cueing for sequencing and hand placement, safety
Ambulation Contact Guard Weakness, verbal cueing for walker sequencing, safety
22
Table 2: Patient 2 Initial Evaluation Assessment Functional Task Level of Assistance Reason for Assist Balance- Static Sitting Independent N/A Balance- Static/Dynamic Standing
Contact Guard with wheeled walker
First time out of bed
Supine<->Sit Bed Mobility Stand By Weakness, verbal cueing for sequencing
Sit->Stand Transfer Minimal Weakness, verbal cueing for sequencing and hand placement
Stand->Sit Transfer Contact Guard
Ambulation Contact Guard Weakness, verbal cueing for walker sequencing and increased WB through left lower extremity, safety
23
Table 3: Patient 1’s Physical Therapy Treatment
^= Progressing towards goal *= Met goal POD= Post-operative Day N/A= Not Assessed Mod I= Modified Independence ABD= Abduction Sup.=Supervision CGA= Contact Guard Assistance Flex= Flexion VC= Verbal Cueing HEP= Home Exercise Program Ext= Extension WW= Wheeled Walker
Day Bed Mobility
Transfers Balance Ambulation Stairs Therapeutic Exercise
POD 1 A.M. Supine to sit with min assist^
Sit to stand with sup., stand to sit with CGA with 2WW^
Dynamic standing with 2WW and sup.
350 feet with 2WW with use of step through pattern, decreased hip flex/ext on R LE, Sup. for VC for sequencing^
N/A Ankle pumps, quad sets x10 reps B/L
POD 1 P.M. N/A Sit to stand with Mod I*, Toilet transfer with sup.
Dynamic standing with 2WW and sup.
375 feet with 2WW using step through pattern, Sup. for sequencing^
4 stairs using right rail with both hands, step to pattern, ascending and descending forwards, CGA for safety, weakness^
Sitting knee extension and flexion, gluteal sets x 10 reps
POD 2 A.M. Supine to sit mod I, sit to supine min assist for manual support of R leg^
Sit to stand and stand to sit with Mod I*
Dynamic standing with 2WW and CGA
450 feet with 2WW with hip hiking on right, sup. For VC to increase knee flex and decrease hip hiking^
14 stairs using right rail, step to pattern, ascending and descending forward at mod I*
Reviewed HEP= glut sets, quad sets, ankle pumps, heel slides, terminal knee ext, supine hip ABD, bent knee fall out, sitting knee ext x 10 reps^
POD 2 P.M. Supine to sit Mod I, Sit to supine Mod I with leg lifter*
Sit to stand and stand to sit with Mod I*
Dynamic standing with 2WW at Mod I
375 feet with 2WW, step through gait pattern at Mod I*
N/A Reviewed HEP= glut sets, quad sets, ankle pumps, heel slides, terminal knee ext, supine hip ABD, bent knee fall out, sitting knee ext x 10 reps*
24
Table 4: Patient 2’s Physical Therapy Treatment
^= Progressing towards goal *= Met goal POD= Post-operative day N/A= Not assessed Mod I= Modified Independence ABD= Abduction Sup.=Supervision CGA= Contact Guard Assistance Flex= Flexion VC= Verbal Cueing HEP= Home exercise program Ext= Extension
Day Bed Mobility
Transfers Balance Ambulation Stairs Therapeutic Exercise
POD 1 A.M. N/A Sit to stand, stand to sit, and toilet transfer with CGA with 2WW, VC for hand placement and sequencing^
Static and Dynamic standing with 2WW at CGA
150 feet with 2WW with use of step to pattern and forward posture, CGA, VC for sequencing, increasing step length, and erect posture^
N/A Ankle pumps, knee ext, and hip ABD sitting x10 reps B/L
POD 1 P.M. N/A Sit to stand, stand to sit, and toilet transfer at CGA with 2WW^
Dynamic standing with 2WW at CGA
175 feet with 2WW using step through pattern after VC at CGA^
N/A Ankle pumps, knee ext, and hip ABD sitting x 10 reps
POD 2 A.M. N/A Sit to stand, stand to sit, and toilet transfer at CGA with 2WW^
Dynamic standing with 2WW at sup.
175 feet with 2WW using step through pattern after VC at CGA^
N/A Ankle pumps, knee ext, and hip ABD sitting x 10 reps
POD 2 P.M. Supine to sit at CGA, Sit to supine at min assist for manual support of left leg^
Sit to stand, stand to sit, and toilet transfer at sup. with 2WW^
Dynamic standing with 2WW at sup.
225 feet with 2WW, step through gait pattern at sup. Reduced step length with fatigue^
2 stairs (2nd one being stoop step) using 2WW, step to pattern, ascending and descending forwards, CGA for safety, weakness, and VC for sequencing^
Too fatigued after functional activity to perform exercises
POD 3 A.M. N/A- Patient and spouse comfortable and safe with bed mobility at home^
Sit to stand and stand to sit with Mod I*
Dynamic standing with 2WW at Mod I
300 feet with 2WW with step through pattern at supervision- patient and spouse comfortable with ambulation in home^
N/A- patient and spouse comfortable and safe negotiating 4 stairs in home
Reviewed HEP= glut sets, quad sets, ankle pumps, heel slides, terminal knee ext, supine hip ABD, bent knee fall out, sitting knee ext x 10 reps*
25
Table 5: Pain Rating Scales
Day Pain at Rest Pain with Activity Patient 1 Patient 2 Patient 1 Patient 2
POD 1 A.M. 0/10 0/10 3/10=stiffness, ache
0/10
POD 1 P.M. 1/10= ache 0/10 1/10=ache 0/10 POD 2 A.M. 0/10 0/10 0/10 3/10= dull,
ache POD 2 P.M. 0/10 3/10= stiff,
ache 0/10 3/10= ache
POD 3 A.M. N/A 0/10 N/A 0/10
26
Table 6: Outcome Measures
Outcome Measure Patient 1 (R hip) Patient 2 (L hip) Hip Flexion AROM 50 degrees 55 degrees Hip Extenstion AROM 8 degrees 5 degrees Hip Abduction AROM 4 degrees 5 degrees Hip Adduction AROM 20 degrees 18 degrees Hip Internal Rotation (IR) AROM
20 degrees 10 degrees
Hip External Rotation (ER) AROM
15 degrees 10 degrees
Hip Flexion Strength 4-/5 3+/5 Hip IR Strength 3+/5 3+/5 Hip ER Strength 3+/5 3+/5 Hip Abduction Strength Unable to test due to pain Unable to test due to pain Romberg Balance Test >30 seconds all conditions >30 seconds all conditions Functional Reach Test 9.5 inches 7.25 inches 6-minute Walk Test 1089 feet 1037 feet Walking Speed 0.4 meters/second 0.25 meters/second Functional Independence Measure (Disability Scale)
Motor: 83/91 Motor: 82/91













![“Table-less” and “Assistant-less” Direct Anterior ... · of direct anterior approach (DAA) hip arthroplasty using a standard operating table [1,2,3,4]. With more surgeons](https://img.pdfslide.us/doc/110x75/5f0a13767e708231d429e6d7/aoetable-lessa-and-aoeassistant-lessa-direct-anterior-of-direct-anterior.jpg)















