Embed Size (px)
Citation preview

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2015
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1058
Physical Functioning, BodyComposition and Exercisein Elderly Community-livingIndividuals with Stroke
BIRGIT VAHLBERG
ISSN 1651-6206ISBN 978-91-554-9120-8urn:nbn:se:uu:diva-236899

Dissertation presented at Uppsala University to be publicly examined in Gunne-salen, Ingång10, Akademiska sjukhuset, Uppsala, Friday, 23 January 2015 at 09:00 for the degree ofDoctor of Philosophy (Faculty of Medicine). The examination will be conducted in English.Faculty examiner: RPT, Ass professor Erik Rosendahl (Umeå University).
AbstractVahlberg, B. 2015. Physical Functioning, Body Composition and Exercise in ElderlyCommunity-living Individuals with Stroke. Digital Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine 1058. 81 pp. Uppsala: Acta UniversitatisUpsaliensis. ISBN 978-91-554-9120-8.
A comprehensive view of physical function, body composition and exercise post-stroke that isbased on clinical examination is lacking. The effects of a progressive resistance and balance(PRB) exercise program have not been fully evaluated in community-living individuals afterstroke.
The overall aim of this thesis was to explore and describe physical function, physical activity,body composition, nutritional status and psychological factors. Another aim was to evaluateboth the short-term and long-term effects of a PRB exercise program.
Physical function, physical activity, body composition, nutritional status and psychologicalfactors were assessed in community-living individuals (65-85 years) approximately 1 year afterstroke. Paper I-II (n=195, n=134) had a cross-sectional design and the main outcome wasmobility and physical activity. In paper III-IV, (n=67, n=43) individuals were randomly assignedto either a PRB exercise program group or a control group. The main outcomes were balance,mobility, fat-free mass (FFM) and fat-mass (FM).
In paper I, mobility was reduced and physical activity level was low compared to age-matchedhealthy controls. Factors explaining the variance in mobility were age, physical activity, fall-related self-efficacy and EQ-5D. In paper II, >20% had a BMI ≥30 kg/m2 and had an alteredbody composition that was mainly characterised by a high fat-mass index (FMI). Neither fat-freenor FM were associated with mobility in this cohort. The factors associated with low mobilitywere low physical activity Odds ratio (OR) (CI 95%) 8.2 (2.8-24.2), risk for malnutrition, OR5.8 (1.6-21.1), and each 10-year period, OR 2.8 (1.24-6.24). Individuals participating in thePRB exercise program (paper III, n=67) revealed significantly higher balance, walking capacityand comfortable walking speed compared to the control group at 3 months. The faster walkingspeed persisted at 6 and 15 months. In paper IV (n=43), at 3 months, the PRB exercise grouphad a significant reduction in FM percentage and a decrease in IGF-1 compared with the controlgroup. Further, changes in FMI were associated with improved walking capacity.
Many individuals perceived partly modifiable disabilities 1 year after stroke. Exercising ingroups for 3 months improved physical function and decreased fat-mass percentage and IGF-1.
Birgit Vahlberg, Department of Neuroscience, Box 593, Uppsala University, SE-75124Uppsala, Sweden.
© Birgit Vahlberg 2015
ISSN 1651-6206ISBN 978-91-554-9120-8urn:nbn:se:uu:diva-236899 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-236899)

To my surprise

Opponent: Erik Rosendahl RPT, Associate Professor Department of Community Medicine and Rehabilitation Umeå University, Sweden Evaluation comitee: MD, Adjunct Professor Andreas Teren´t Department of Medical Sciences, Cardiovascular epidemiology Uppsala University, Sweden Adjunct Professor MD, Jörgen Borg Department of Clinical Sciences Karolinska Institutet, Sweden Professor RPT, Lena von Koch Department of Clinical Sciences, Occupational Therapy Karolinska Institutet, Sweden Supervisors: RPT, Associate Professor Karin Hellström Department of Neuroscience, Physiotherapy Uppsala University, Sweden MD, Professor Tommy Cederholm Department of Public Health and Caring Sciences, Clinical Nutrition and Metabolism Uppsala University, Sweden RPT, Senior lecturer Lena Zetterberg Department of Neuroscience, Physiotherapy Uppsala University, Sweden

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Vahlberg B, Cederholm T, Lindmark B, Zetterberg L, Hellström K. Factors related to performance-based mobility and self-reported physical activity in individuals one to three years after stroke: a cross-sectional cohort study. J Stroke Cerebral Diseases. 2013; 22(8): e426-34
II Vahlberg B, Hellström K, Lindmark B, Zetterberg L, Ceder-
holm T. Body Composition, Nutritional Status, and Physical Function in Community-Living Individuals 1-2 Years after Suffering a Stroke. Submitted.
III Vahlberg B, Cederholm T, Lindmark B, Zetterberg L, Hellström K. Effects of Progressive Resistance and Balance
training in Chronic Stroke: A Randomized Controlled Tri-al. Submitted.
IV Vahlberg B, Lindmark B, Zetterberg L, Hellström K, Ceder-
holm T. Body composition after progressive resistance and balance training in older adults after stroke. Submitted.


Contents
Preface .......................................................................................................... 13
INTRODUCTION ........................................................................................ 15 Stroke ....................................................................................................... 15 Risk factors for stroke .............................................................................. 16
Hypertension and hypercholesterolemia .............................................. 16 Physical inactivity ................................................................................ 17 Nutritional risk and prevention ............................................................ 17
Post-stroke conditions .............................................................................. 18 Physical function and physical activity ............................................... 19 Body composition ................................................................................ 20 Nutritional changes .............................................................................. 21 Psychological factors ........................................................................... 22
Exercise and recommendations among individuals with stroke ............... 23 Progressive resistance training after cardiovascular disease including stroke ........................................................................................................ 24
Rationale .............................................................................................. 25
AIMS ............................................................................................................ 27
METHODS ................................................................................................... 28 Design ...................................................................................................... 28 Recruitment and participants .................................................................... 28 Procedure in the paper I-II (Cross-sectional design) ................................ 31 Procedure in paper III and IV (Randomised controlled trial) ................... 32 Assessments (paper I-IV) ......................................................................... 33
Demography and morbidity ................................................................. 33 Body structure and function: ............................................................... 34 Body function and activity ................................................................... 35 Activity ................................................................................................ 35 Participation ......................................................................................... 36 Personal factors .................................................................................... 37
Exercise intervention (Paper III-IV) ......................................................... 37 Statistics ................................................................................................... 39 Descriptive statistics ................................................................................. 40 Statistics: Paper I-II ................................................................................. 40 Statistics: Paper III-IV .............................................................................. 41

RESULTS ..................................................................................................... 43 Associations with mobility and physical activity in elderly community-living individuals (paper I-II). .................................................................. 43 The short-term and long-term effects of a progressive resistance and balance exercise program in elderly community-living individuals after stroke (paper III-IV). ................................................................................ 47
DISCUSSION ............................................................................................... 53 Summary of results ................................................................................... 53 Associations to physical function and physical activity ........................... 53 Body composition, nutritional status and cardiometabolic risk-markers . 57 Effects of a 3-month progressive resistance and balance exercise program .................................................................................................... 58 Methodological considerations................................................................. 60
Individuals included............................................................................. 60 Data collection ..................................................................................... 61
Main conclusions ...................................................................................... 63 Clinical implications ................................................................................ 64
Svensk sammanfattning ................................................................................ 65 Delarbete I: ............................................................................................... 65 Delarbete II: .............................................................................................. 66 Delarbete III ............................................................................................. 67 Delarbete IV ............................................................................................. 67
Acknowledgements ....................................................................................... 69
REFERENCES ............................................................................................. 72

Abbreviations
ACoSM American College of Sports Medicine AHA American Heart Association Apo A1 Apolipoprotein A1 Apo B Apolipoprotein B BIA Bioimpedance analysis BMI Body Mass Index CI Cerebral infarction CCI Charlson Comorbidity Index CCT Circuit Class Training CG Control group CRS Cardiovascular disease risk score CVD Cardiovascular disease EQ-5D EuroQol-5D EQ-5D-VAS EuroQol-5D Visual Analog Scale FES(-S) Falls Efficacy Scale-Swedish version FFM Fat free mass FFMI Fat free mass index FM Fat mass FMI Fat mass index FM% Fat mass percentage FoF Fear of falling GDS-20 Geriatric Depression Scale HDL High-density lipoprotein HRQoL Health Related Quality of Life IG Intervention group IGF-1 Insulin-like Growth factor-1 ICH Intracerebral hemorrhage ICF International Classification of Functioning
Disability and Health LDL Low density lipoprotein M-MAS UAS-99 Modified Motor Assessment Scale Uppsala University Hospital-99 PASE Physical Activity Scale for the Elderly PRB Progressive Resistance and Balance RS Riksstroke SPMSQ Short Portable Mental Status Questionnaire

SPPB Short Physical Performance Battery
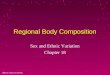
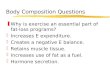
The International Classification of Functioning, Disability and Health (ICF) can be divided in to two different parts: functioning, where functioning mir-rors the positive aspects between a person and the surroundings, and disabil-ity, where disability (an umbrella term for impairments, activity limitations and participant restrictions) describes the negative aspects, i.e., loss of func-tion (1). Further, the ICF comprises the following components: 1) body func-tions, anatomic structures and their related impairment; 2) activities and activity limitations; and 3) participation and participating restrictions as well as environmental and personal factors (Figure 1). The ICF can be used in different ways for rehabilitation and research and in mapping function and disability. The aim of ICF is to provide a unified and standardised language and framework to describe health and related states (1). In the present thesis, ICF is used to visualise the targeted areas.
Figure 1. The International Classification of Functioning, Disability and Health (ICF)
Health condition
(disorder or disease)
Health condition
(disorder or disease)
Health condition
(disorder or disease)
Body functions
and structuresActivities Participation
Environmental factors Personal factors

13
Preface
The experiences I have working as a physiotherapist with post-stroke indi-viduals at the Geriatric Clinic at The Uppsala University Hospital are the basis for this thesis. These clinical experiences made me wonder how the patients continued with rehabilitation and their ordinary lives henceforth. Over the years, I also had the opportunity to spend some summers working in a 4-week stroke program at Sätra Brunn, an old health spa located near Uppsala. This program included both individual treatments as well as group sessions. Rehabilitation was carried out in a beautiful environment with nu-merous social possibilities. I realised that participation in these stroke pro-grams, several years after the stroke, enabled the individuals to improve their functional and psychological status. Meeting other individuals who had suf-fered strokes previously seemed crucial for their well-being.
The long-term effects of a stroke may differ between individuals, despite a similar location and stroke magnitude, as the effects are influenced by per-sonal and environmental factors. This is crucial for planning an individual-ised rehabilitation. I realised that I wanted to find out in more detail how the individuals with stroke perceived their lives from a long-term perspective and what type of disabilities and functional losses were most common. This provided the basis for the two first cross-sectional studies in this thesis. I also wanted to evaluate group-exercising with respect to the individual’s functioning, muscular prerequisites, nutritional status and cardiometabolic risk factors; the latter were new areas for me.
This thesis is dedicated to all the individuals with stroke that shared their experiences with me and thereby made it possible to compare my former clinical knowledge with new scientific knowledge.
I wish to thank all the participating individuals for making this thesis pos-sible and my wish is that this research can add some missing pieces and con-tribute to a better everyday life for individuals post-stroke.

14

15
INTRODUCTION
Stroke In Sweden, approximately 30,000 people have a stroke each year, and ap-proximately 23,000 of those people suffer from their first stroke according to Riksstroke (the Swedish stroke register, RS) (2). The mean age for stroke in Sweden is 74 years for men and 79 years for women (3). Approximately 80% are more than 65 years old at the time of the stroke. The definition of stroke according to the World Health Organization (WHO) is “rapidly de-veloping clinical symptoms and/or focal signs, and at times global loss of cerebral function, with symptoms lasting more than 24 hours or leading to death, with no apparent cause other than of vascular origin” (4). Stroke is one manifestation of cardiovascular disease (CVD) and can be divided into different types: cerebral infarction or ischemic stroke, intracerebral haemor-rhage and subarachnoid haemorrhage (3). Stroke and transient ischemic at-tack (TIA) have similar pathophysiological backgrounds and TIA is a strong predictor of stroke, especially in the first 90 days after the TIA (2). The inci-dences of TIA are 8000 – 12000 cases annually in Sweden according to RS. Further, the total cost for stroke in Sweden is calculated to be 18.3 billion Swedish kronor per year according to RS (2).
In the RS individualised data within health-care production concerning hospital care, rehabilitation and secondary prevention are registered. All hospitals admitting patients with acute stroke are included in the register, which covers > 80% of all stroke events in Sweden (2). At 3 and 12 months follow-ups, additional data are gathered by a postal questionnaire sent to the individual and then are further registered in RS. In this thesis, some data are collected from RS at the time of the stroke and after 1 year. In 2013, ap-proximately 41% of the individuals with stroke displayed unmet needs of rehabilitation after 1 year, according to RS 1-year follow-up (5). Based on earlier reports, that was the origin of the present thesis. Among the older individuals (> 75 years), self-perceived unmet rehabilitation needs are even higher. In the Uppsala University Hospital, only cases of acute stroke are reported to the RS register.
Long-term survival after stroke continues to improve, and because the elderly population is growing, this results in an increased number of indi-viduals in Sweden who previously have had a stroke (5). Stroke is more common in men > 65 years old and in women ≥ 85 years (6). The preva-

16
lence of stroke is approximately 30% higher in men, but women have a higher rate of cardio-embolic stroke and experience a worse outcome be-cause of the typical greater age at stroke onset. Women also tend to suffer from post-stroke depression and low quality of life more frequently com-pared to men (7).
If the strong decline in stroke mortality seen in the past decades contin-ues, this may not result in a change in the absolute number of stroke deaths, because of the aging population (8). The morbidity burden after stroke is likely to become more important than the mortality burden because of better survival rates. Preventive strategies and rehabilitation methods must be im-proved to reduce stroke-related disability, enhance physical fitness and pre-vent future cardiovascular events (8, 9).
Risk factors for stroke The population-based Framingham Heart Study has played an important role since 1949 in establishing the now widely accepted knowledge regarding cardiovascular diseases (CVD) (10). The study is still ongoing and has re-cently enrolled a third generation of participants. The Framingham Heart Study has been able to identify important risk factors for CVD and, in fact, coined the term “risk factors” (10). Stroke is a heterogenic disease, and there can be differences in risk factors between the types of stroke and gender (7). Lifestyle related diseases, including cardiometabolic diseases (i.e., CVD, obesity, metabolic syndrome and type II diabetes), can, to a high degree, be prevented by a healthy lifestyle. Hypertension, abdominal obesity, smoking, diabetes, alcohol, physical inactivity, depression and an unhealthy diet are examples of modifiable risk factors that are important both for prevention of the primary event and for recovery after a stroke (11).
Hypertension and hypercholesterolemia Hypertension is the greatest risk factor for stroke and is also the most modi-fiable factor (12, 13). Hypertension can be defined as a systolic blood pres-sure (BP) ≥ 140 mm Hg or a diastolic BP ≥ 90 mm Hg. Lifestyle modifica-tions, as a component of antihypertensive therapy, are associated with a re-duction in blood pressure and include dietary modifications and regular physical activity (13).
Hypercholesterolemia is another risk-factor for atherosclerotic CVD and mortality, especially a high concentration of low-density lipoprotein (LDL) (13). A low concentration of high density lipoprotein (HDL) is also a risk factor for atherosclerosis. The HDL is primarily affected by regular physical activity, whereas high LDL can be modified through nutritional changes and lipid-lowering medications, e.g., statins. If necessary, lipid-lowering medica-

17
tion should be prescribed following a stroke according to current guidelines (13). However, statins also have some side effects that are primarily associ-ated with muscle symptoms (e.g., myopathy) (14). Individuals with stroke have an increased prevalence of hypertension, diabetes and hypercholes-terolemia (metabolic syndrome) (13). Additionally, individuals with diabetes also have an increased risk for death following stroke as well as an increased risk for having another stroke or a myocardial infarction (15).
Lipid disorders can also be measured with the ratio between apolipoprote-in B (apoB) and apolipoprotein A1 (apo-A-1) (16, 17). Apolipoproteins are found to predict cardiac risk in individuals above the age of 70(18).
Physical inactivity Physical activity is defined as any bodily movement produced by skeletal muscles resulting in energy expenditure (19). Reasons for a sedentary life-style can include an increased dependence on cars because work and home are separate units, an increased number of automatic procedures, increased television and computer usage and a feeling of insecurity about moving around in society (20). Physical inactivity and a sedentary lifestyle together increase the likelihood for inflammatory processes and hence increase the risk for CVDs (21). A high level of physical activity has a beneficial effect on most stroke risk factors. Moreover, it has been proven that individuals with high levels of physical activity have a 67% lower prevalence of meta-bolic syndrome compared to individuals reporting a sedentary lifestyle (22). There is a lack of evidence on the effect from non-pharmacological studies, i.e., well-designed exercise studies, on cardiovascular risk-markers and body composition after stroke (9). Knowledge about the effects of sedentary be-haviour and ways to optimise physical activity after stroke are important issues in physiotherapy.
Nutritional risk and prevention Hankey (23) concluded that the two main threats to global health and risk of stroke are over-consumption of salt and calories. Salt reduction can lower blood pressure and reduce stroke mortality, whereas obesity and over-nutrition can lead to diabetes mellitus, hypertension and hypercholes-terolemia. A diet rich in fruits, vegetables, dietary fibre and fish in conjunc-tion with a limited intake of saturated fat, trans-fatty acids and cholesterol helps to protect against stroke (13, 24). The INTERSTROKE study high-lighted that increased consumption of fish and fruit reduces the risk for stroke (11). Over-nutrition can increase the risk for stroke; the development of obesity, hypertension, hypercholesterolemia and diabetes as a result of a high caloric intake might be the cause of this increased stroke risk (23). There is a profile of cardiometabolic and inflammatory markers that be-

18
comes apparent when one´s Body Mass Index (BMI) increases from a nor-mal weight to obesity. Individuals with a BMI of ≥ 30 kg/m2 have a doubled risk of ischemic and haemorrhagic stroke compared to individuals with a BMI of < 23 kg/m2 (24). Among both men and women, obesity is most common in the elderly. Interestingly, and in contrast, recent studies have reported lower mortality, improved functional outcomes and a lower risk for re-admission from recurrent stroke in obese patients compared with lean patients (25, 26).
Many individuals with stroke are undernourished at hospital admission, and their nutritional status is known to deteriorate further during their hospi-tal stay (24). Both under-weight and overweight/obesity are important states to consider in individuals after stroke. Nutritional status can affect C-reactive protein (CRP), plasma albumin and serum insulin-like growth factor-I (IGF-I). Furthermore, it is suggested that inflammatory markers, such as CRP, are a triggering factor for stroke, because increased concentrations have been associated with metabolic syndrome and FM (27). CRP-levels are influenced by weight changes, i.e., increased body fat is positively related to CRP, while increased intake of dietary fibre is related to lower CRP (28). Albumin is a marker of malnutrition and deficiency in caloric and protein intake and is an indicator of mortality and morbidity (24). Albumin levels have been proven to be neuro-protective because there is an association between high serum albumin and protein supplementation and better functional outcomes, as well as lower mortality rates in sub-acute stroke patients (29). Except for nutritional intake, the IGF-1 level can vary with different ages, gender, oes-trogen status, exercise status, stress levels and BMI (30). Higher levels of physical activity, optimal protein intake and younger age predisposes for higher IGF-1 levels. In addition, both normal high and low levels of IGF-1 are associated with insulin sensitivity (31).
Post-stroke conditions Stroke causes disabilities of various degrees; the localisation of the stroke and the severity of the brain injury determine the impact of stroke. A typical sign of stroke and TIA is sudden weakness/numbness of the face, arm or leg occurring mostly on one side of the body. Motor function can be lost; the major part of motor recovery occurs within the first 6 months (32). Confu-sion and difficulties in speaking or understanding, walking and balance diffi-culties are also common symptoms. Other consequences that are not imme-diately apparent could be of a cognitive and perceptual (e.g., sensory and visual impairments) nature. In the latest report and 1-year follow-up from RS (2013), it was found that 88% were independent in daily activities at the time of the stroke (5). After 1 year this was 75%, which can depend on another stroke or fall incidences. Another cause for the loss of independence might

19
be that rehabilitation stops after approximately 3 months. Moreover, most individuals < 75 years are independent in moving inside and outside their homes, but this is in contrast to being > 75 years. In women > 75 years, about half need help in walking and transferring (5).
Long-term changes in physical function, psychological factors, nutrition and body composition after stroke can include affected mobility (33), motor impairments (34), inactivity (35, 36), reduced health-related quality of life (37), depression (38), low fall-related self-efficacy (39), falls and fear of falling related to balance disturbances (40), problems with walking in the community (40), altered body composition with less muscle mass, or in-creased fat mass and malnutrition (24, 41, 42). Further, white matter changes or leukoaraiosis are also issues in the elderly, as well as in stroke subjects, and result in cognitive decline, balance disturbances and increased depres-sion (43).
Physical function and physical activity In this thesis, physical function is an umbrella term for measurements that include mobility, walking, motor function and balance. Different definitions of mobility can be obtained from different perspectives (44). Mobility is not stabilised after post-stroke inpatient rehabilitation and it is reported that 12-43% of post-stroke individuals show further deterioration of mobility during the next one to three years (45-47). Gait speed, balance and lower extremity function, as measured by the Short Physical Performance Battery (SPPB), provides a good estimate of the future risk for hospitalisation, health deterio-ration and mortality in initially nondisabled, older adults (48). However, the value of using the SPPB in assessment of functional progression after stroke needs to be further explored (49).
Self-selected gait-speed below 1 m/s can identify older persons at risk for health-related outcomes (50, 51), and a gait-speed of more than 1.2 m/s is needed to cross a street safely (52). This is in line with a meta-analysis pro-posing that a faster gait-speed, i.e., > 1.0 m/s in older people, suggests a better life-expectancy while a slower gait-speed, < 0.6 m/s, is indicative of poor physical function and health (53). Small or substantially meaningful changes for the Six Minute Walk test (6MWT) are 20 or 25 to 50 meters, respectively, compared to 0.05 m/s to 0.1 m/s for the walking speed in com-parable groups (54, 55). The above knowledge can be used in clinical as-sessments of gait and in designing preventive interventions.
Individuals who have impaired balance at least six months after stroke are at risk for falls and are shown to have low activity and participation scores (56). This highlights the importance of focusing on factors such as falls and balance self-efficacy during rehabilitation. Another study on post-stroke individuals confirms this finding because fallers are more likely to report a reduced fall-related self-efficacy compared with non-fallers (40). Within 12

20
months post-stroke, there is a two-fold increase in hip and femur fractures caused by falling (57). Increased risk for falls is also connected to sarcopenia and associated disabilities (27, 58).
Community-living individuals without stroke have a higher level of physical activity compared to individuals of the same age with stroke, meas-ured by the Physical Activity Sale for the Elderly (PASE) (35). The mean PASE score was 161 in the healthy control group and 119 in the stroke group. Interestingly, but not unexpectedly, motor function was not crucial for the level of physical activity. A low level of physical activity after stroke can depend on the consequences from the stroke as well as a sedentary life-style before, due to the effects of age and comorbid diseases (21). Cardiores-piratory fitness in stroke victims is found to be approximately 50% of the expected value in an age- and gender matched reference group (59). Activity limitations, such as in walking and chair-rising, are associated with low car-diorespiratory fitness level as well as low muscle strength (59, 60). It is im-portant to assess how physical function can interact with physical activity to identify possible actions to support and assess the level of physical activity after stroke.
Body composition Skeletal muscle can be considered the main organ for disabilities after stroke, but it receives little attention despite structural, functional and meta-bolic changes. Beginning at age 50, there is a normal loss of muscle mass ranging from 1 to 2% per year that also affects muscle strength and muscle quality (41, 42, 51, 61, 62). Muscle strength in the legs is associated with physical function, such as being able to climb stairs, walk at different speeds and maintain mobility, which are all common difficulties after a stroke (63). Stroke can further be linked to skeletal muscle changes as a result of abnor-malities, denervation, remodelling and spasticity causing atrophy, especially in more severe cases (64). A stroke-induced sarcopenia in hemiplegic stroke was recently introduced that partly differs from age-dependent sarcopenia (64).
Impaired glucose metabolism is found in more than 80% of stroke survi-vors (65). Changes in muscle and fat mass in aging and after stroke, together with inactivity, can lead to impaired glucose metabolism and progression to diabetes, which increases the risk for another stroke or myocardial infarc-tion. There is evidence that post-stroke individuals have significantly less muscle mass in the paretic limbs compared to their non-paretic side (41). Muscle mass loss after 1 year is also different in those who regain walking capacity 2 months after stroke compared to non-walking individuals, which is not surprising because weight-loading is important in preventing or slow-ing muscle loss (66). Considering the role muscles play in glucose metabo-

21
lism and in slowing bone mineral loss, changes in muscle mass may be even more important.
For this thesis, sarcopenia was defined as a “fat free mass index (FFMI, kg/m²) below the 25th percentile of a reference population together with usual gait speed < 1.0 m/s” according to the International Working Group on Sarcopenia (51, 67). Currently, no definition of sarcopenia is fully ac-cepted, and sarcopenia is not included in the classifications of diseases. Sar-copenia can predict loss of mobility and independence and may be a conse-quence of physical inactivity, age, nutritional deficits and hormonal changes (62). Unfortunately, limited data are available on muscle pathology after stroke and the state is not considered in current guidelines. There are also few studies that describe body composition, i.e., muscle mass and FM and sarcopenia after stroke, as well as few studies that measure changes in body composition over time or that reports effects from intervention studies after stroke (41).
An increasing prevalence of obesity in older individuals causes an in-creased burden on health care systems in developed countries as a result of sarcopenic obesity, i.e., obesity and sarcopenia occurring together (27, 68). Sarcopenic obesity in this thesis was defined as a FFMI below the 25th per-centile and a fat mass index (FMI) above the 50th percentile of a reference population, as earlier described (69). Baumgartner showed that individuals older than 60 years with sarcopenic obesity have a much higher risk for re-duced balance, gait and falls in the previous year, but not much is known about sarcopenic obesity in individuals post-stroke (41, 42, 70). Obese, eld-erly individuals have a higher muscle mass but poor muscle quality com-pared to the non-obese and frail elderly due to the anabolic effect induced by their body weight (71). This may contribute to the obesity paradox, recently reported after stroke (26). Lower mortality, improved functional outcomes and a lower risk for re-admission has recently been reported in obese indi-viduals with stroke, in contrast to previous findings (25). It can be assumed that low physical activity level and reduced cardio-respiratory fitness may be greater health threats than obesity itself (72).
Nutritional changes Malnutrition, i.e., weight loss after stroke, is common (24, 73). Different neurological deficits may occur as a result of decreased function, and motor functions that allow for the necessary arm-movements for eating, chewing and swallowing can be lost due to hemiparesis. Perceptual deficits, visual-field defects and oral or motor apraxia are conditions that can also affect nutritional status. A number of stroke patients are malnourished upon hospi-tal admission and continue to deteriorate further after being hospitalised (24).

22
Jönsson et al. (73) also showed an increased prevalence of overweight in individuals approximately one year after stroke, rising from 52% immedi-ately after the stroke to 61%, 1 year after the stroke. A reduction of five to ten percent of one’s bodyweight can improve lipid profiles and insulin sensi-tivity in overweight and obese individuals (74).
Inflammatory activity, as measured by CRP, is often elevated in individu-als with stroke and upon discharge from the hospital, and also associated to further vascular events and deaths together with aging (75, 76). Further, CRP levels can be used to stratify post-stroke individuals into high risk and low risk groups, with CRP levels ≥ 1.5 g/L having a poorer diagnosis. Albumin levels have been found to associate mortality with cardiovascular disease, cancer and other causes (77). Furthermore, low levels of albumin in ischemic stroke are reported to be significantly associated with a higher score (> 3 on the modified Rankin scale) and poor outcome, together with high recurrence of stroke and death in different stroke subtypes (24, 78). In conclusion, rela-tively high serum albumin levels in acute stroke have a positive effect on functional outcome. After ischemic stroke, the IGF-1 levels are revealed to be both neuroprotective, regenerative and correlated with better functional outcomes (79). Low levels of IGF-1 have been observed after stroke and might reflect malnutrition and low levels of physical activity (80).
Psychological factors Post-stroke individuals have a broad range of symptoms, but few studies have comprehensively assessed these physical and psychological factors (81). Major psychological consequences after stroke include decreased cog-nitive function (82), depression (38), low health-related quality of life (HRQoL) (37), decreased fall-related self-efficacy (83) and fear of falling (FoF) (40). After a stroke, individuals may have impaired cognitive func-tions, such as problems with memory, language, calculation and executive functions, indicating problems in daily living (82).
Depression has a great impact on life satisfaction 1 year after stroke; ac-tive rehabilitation can affect life satisfaction and thus lead to decreased de-pression (38). Anti-depression treatment is another option in more severe cases. It is important to detect and manage depression several years after stroke to improve life satisfaction and reduce the risk for another stroke (11). However, it is unclear what type, intensity and duration of exercise might improve depression as well as HRQoL; additional controlled studies are therefore warranted (84).
In Sweden, health-related quality of life (HRQoL) using EQ-5D is known to vary between socio-economic groups and diseases (85). Moreover, the frequency of moderate and severe problems increases with age. Individuals with both myocardial infarction and stroke have lower HRQoL compared with patients with other diagnoses and those with stroke revealed the lowest

23
HRQoL, which was even lower when combined with myocardial infarction (37).
Self-efficacy can be defined as the degree of confidence a person per-ceives that is connected to their ability to perform specific behaviours (83). Individuals with high self-efficacy tend to cope better with challenging tasks, put forth more effort, and persist longer with particular tasks in the face of aversive stimuli. Fall-related self-efficacy is a psychological issue that might influence functional decline and limit individual functions beyond that of physical function. The activities in daily life over 10 months after a stroke can be predicted by fall-related self-efficacy (39). Low fall-related self-efficacy is also significantly associated with impaired physical function in individuals after stroke (40). Impaired vision, low cognition or a wrong idea about one’s own physical abilities in any direction are characteristics that may influence fall-related self-efficacy (40). Knowledge pertaining to how self-efficacy influences behaviour is important in the planning of effective interventions and in identifying individuals with low self-efficacy.
Physical function and previous falls are associated with fear of falling in individuals with stroke (40, 86). A FoF can be defined as an ongoing con-cern about falling that might restrict the performance of daily activities (87). An increased risk for falling, hip fractures and FoF are common after stroke and the reported incidences vary between 40% to 70% (88).
Exercise and recommendations among individuals with stroke Exercise and training are used synonymously in this thesis and are classified as a subcategory of physical activity; the definition of exercise is a physical activity that is planned, structured and repetitive for the purpose of condi-tioning any part of the body (19). Furthermore, physical fitness is defined as a set of physiological attributes including cardiorespiratory fitness, muscle strength, body composition and flexibility and relates to the ability to per-form physical activities for an extended period (19). Due to physical inactiv-ity or immobilisation, physical fitness can deteriorate 12-14% in 10 days but aging also reduces fitness level. The American College of Sports Medicine (ACoSM) and the American Heart Association (AHA) guidelines on secon-dary prevention after stroke recommend that those capable of participating in physical activity and with stroke or TIA receive at least 30 minutes of mod-erate-intensity exercise, 1-3 times a week (13). Moderate intensity can be defined as vigorous activity sufficient to break a sweat or noticeably elevate the heart rate. Supervision from a healthcare professional is needed for indi-viduals with disabilities. An expert in physical therapy or in cardiac rehabili-tation can provide supervision, or at a minimum, an exercise regimen (13).

24
Progressive resistance training after cardiovascular disease including stroke Muscle strength and power are closely related to muscle function and are essential for standing up from a sitting position or when walking (89). A small decline in muscle function has a greater impact on weaker individuals with disabilities and can consequently lead to difficulties in daily activities. Progressive resistance training (PRT) is carried out to improve muscle strength and endurance or muscle power output by making repeated muscle contractions resisted by body weight, elastic devices, free weights or special-ised machines in a progressive manner (84). Currently, there is insufficient data to report effects on physical fitness, mobility (i.e., walking speed and walking capacity) and further physical function after participating in PRT after stroke, according to a recent systematic review (84). There is also a lack of well-designed randomised controlled trials reporting on the effects of PRT on psychological factors such as health-related quality of life and mood/depression after stroke (84).
The training dose is important and includes duration (minutes of ses-sions), frequency (days/weeks) and intensity (amount of effort) (90). The recommendation for PRT to be effective is that it should be performed 2-3 times/week, with 8-10 different exercises that target all major muscle groups (90, 91). Duration in different exercise interventions are usually 8-12 weeks in older adults (92). The ACoSM also recommends 1-2 minutes of resting between lower intensity exercises.
Percentage of maximum load, i.e., a repetition maximum (RM), can be used to describe the intensity of a strength exercise (93). The definition of 1- RM is the maximum weight that can be lifted one time. Another way to de-scribe the intensity of strength training is by the maximum amount of weight being lifted. Furthermore, for individuals with CVD, the resistance should be reduced with an increasing number of repetitions (reps) (90). Using weight loads permitting > 15 reps enhances endurance and is considered to be per-formed with low intensity. Using weight loads with 8-15 reps is performed with a moderate intensity and improves muscular strength and endurance (90).
Effects of training can also be influenced by whether the training is task-specific and whether progression is being made (94, 95). Progression in this thesis refers to gradually adjusting the load for the exercise improvement of the individual (91, 96). The ACoSM recommends that balance training should include dynamic movements affecting the centre of gravity, progres-

25
sively more challenging postures that reduce the base of support, stressing postural muscles and reducing sensory input (97).
According to the AHA, the early stages of PRT should allow for muscu-loskeletal adaptation and good techniques at a moderate level to follow the recommendations on repetition range (90). This is of particular importance for individuals with cardiovascular disease such as stroke, because many are sedentary and have comorbidities. Absolute contraindications are e.g., un-stable coronary heart disease, uncontrolled hypertension (> 180/110 mm Hg) and uncontrolled arrhythmias (90).
Aerobic training and regular cardiac rehabilitation together with lifestyle counselling have shown some effects on cardiovascular risk-markers in chronic stroke patients (9, 98). Circuit Class Training (CCT) is when indi-viduals use workstations to practice intensively in groups with a focus on repetition of functional exercises and continual progression (99). Gym train-ing, performed as CCT for 12 weeks, has shown some positive effects on gait speed and walking capacity after stroke compared to the typical physio-therapy (99). Changes in gait speed in that study persisted at follow-up after 24 weeks. Further, CCT favours group dynamics while including peer sup-port and social interaction and are considered to be effective in individuals with mild to moderate disability after stroke (100). Social interaction is known to provide psychological benefits such as improved mood and higher self-efficacy (101).
Rationale Suffering a stroke can turn life up-side-down and might lead to lifelong dis-abilities and fears. Thus, to meet the perceived unmet rehabilitation needs 1 year after stroke there was a need to explore physical function and physical activity, nutritional status, body-composition and psychological factors in older individuals with chronic stroke. Further, obtaining a comprehensive objective view of their everyday life situation post-stroke was essential. The intended meaning was to further develop and evaluate exercising to reduce the effect of the stroke and in many cases, a sedentary lifestyle. This knowl-edge may be used in the future planning of rehabilitation.

26

27
AIMS
The overall aim of this thesis was to explore and describe physical function, physical activity, body composition, nutritional status (including cardiome-tabolic risk markers) and psychological factors in elderly community-living individuals, approximately 1 year after stroke. Furthermore, another aim was to evaluate the short-term and long-term effects of a progressive resistance and balance exercise program. The specific aims in this thesis were: 1. To explore and describe mobility and physical activity and investigate the association with psychological determinants and demographic characteristics (Paper I). 2. To explore and describe body composition, physical function and lifestyle factors, such as physical activity and nutritional status, and their impact on mobility. In addition, in the same cohort, another aim was to evaluate in-flammatory, nutritional and cardiometabolic biomarkers (Paper II). 3. To evaluate the effects of a 3 month progressive resistance and balance exercise program on short-term and long-term physical and psychological functioning and physical activity level (Paper III). 4. To: (1) investigate the effect of a progressive resistance and balance exer-cise program on body composition, cardiometabolic risk markers and indica-tors of growth and nutrition; (2) evaluate possible associations between changes in physical function and body composition (Paper IV).

28
METHODS
Design The thesis comprises paper I-II with a cross-sectional design and papers III-IV as a randomised controlled trial (Table 1). Written informed consent was provided by all subjects. The studies have been approved by the Regional Ethical Review Board, Uppsala (Dnr 200:067/2). The intervention trial was registered at ClinicalTrial.gov (Unique identifier: NCT1161329).
Recruitment and participants All of the papers were based on the same sample presented in paper I. All eligible subjects in the geographic area of Uppsala County were identified, treated previously and registered to RS at the Uppsala University Hospital. After the stroke, rehabilitation and after-care were delivered in different settings throughout Uppsala County. Recruitment was carried out between October 2009 and April 2011.
In paper I, community-dwelling individuals between 65 and 85 years of age with a first or recurrent stroke 1-3 years before inclusion were included. Excluded were individuals with severe cognitive dysfunction, dementia or other communication problems (revealed from medical records or during examination). In total, 279 individuals were found to be eligible for paper I, and a total of 195 individuals, i.e., 70%, provided their full consent for par-ticipating. Three individuals were further excluded at the time of examina-tion, due to difficulties understanding questions and instructions. If the indi-vidual declined to fully participate, they were asked whether they wanted to participate by answering the EQ-5D by telephone (102). From the 279 eligi-ble individuals, 81 of the 82 individuals who did not want to participate fully were willing to answer questions on the EQ-5D and the EQ-5D-Visual Ana-log Scale (VAS) (102).
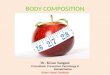
In Paper II, data from 134 of the individuals presented in paper I is in-cluded. Individuals not being able to perform BIA for any reason were fur-ther excluded (Figure 2).

29
Figure 2. Flow-chart of the phases in the papers I-II
For the randomised controlled trial (RCT), paper III comprised data from 67 of the 195 individuals found eligible in study I (76% male, mean age: 73 years). A median of 13 months had passed since the stroke. Individuals were included if they had the ability to walk a minimum of 10 m and had at least one of the following: lack of outdoor walking for at least 5 days per week (derived from the Physical Activity Scale for the Elderly) (103), a low fall-related self-efficacy (Falls Efficacy Scale-Swedish version < 115 points) (39), balance difficulties (Berg Balance Scale ≤ 52 points) (104), or repeated falls within the last year. Individuals with cognitive deficits (Short Portable Mental Status Questionnaire < 7 points)(105), or a systolic blood pressure >180 mmHg were excluded. Those matching the inclusion criteria who were willing to participate were randomised to an intervention group (n=34) or a control group (n=33). Of the 67 individuals included at baseline, 24% (n=8) and 6% (n=2) were lost to follow-up at 3 months in the intervention group (IG) and control group (CG), respectively. The attrition rate increased to 29% at 15 months in the intervention group (Figure 3).
279 individuals were asked to participate
195 individuals were included Did not undergo BIA due to (n=61):
Reduced balance (n=27).
Examined outside the hospital (n=15).
Pacemaker (n=10).
Technical error (n=9).
BIA assessment
(n=134)
En
rollm
ent
All
ocat
ion
Paper I
Paper II
81 declined full participation (answered EQ-5D)

30
Figure 3. Flow diagram of the phases of the randomised controlled trial (paper III).
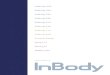
In paper IV, 43 of the 67 individuals in paper III were evaluated. Individuals with pacemakers and those lacking BIA were further excluded. Eligible in-dividuals participated in the same PRB exercise program as described in paper III (IG, n=20) or a control group (CG, n=23). Data from 24 individuals were excluded because of the following reasons: reduced static balance and standing capacity (n=17), pacemaker (n=4) and technical error (n=3) (Figure 4).
Assessed for eligibility (n=198) Declined participation (n=8)
Ineligible (n=122)
Eligible, but could not be reached for inclusion (n=2) Randomized (n=67)
Allocated to Intervention group (n=34)
Declined participation (n=2)
Declined participation (n=6)
Medical condition (n=2)
Declined participation (n=1)
Analyzed after 6 months (n=25) Analyzed after 6 months (n=30)
Drop-out because of acute disease (n=1)
Declined participation (n=1)
Analyzed after 15 months (n=24) Analyzed after 15 months (n=29)
Allocated to Control group (n=33)
Analyzed after 3 months (n=26) Analyzed after 3 months (n=31)
Declined participation (n=1)

31
Figure 4. Flow diagram of the phases of the randomised controlled trial (paper IV).
Procedure in the paper I-II (Cross-sectional design) In paper I and II, potential participants received written information by mail about the study. The participants were also contacted by phone, and if they provided oral consent, a meeting at the hospital was scheduled. Self-reported questionnaires including physical activity level (PASE) the prior week (103, 106), psychological factors such as depression (GDS-20) (107), fall-related self-efficacy (FES(S) (108) and HRQoL (102), were sent to the eligible indi-viduals ahead of the clinical assessment meeting. These self-reported ques-tionnaires were rechecked at the time of the assessment. At the hospital, after signing the written consent for participation, non-fasting venous blood sam-ples were obtained. The samples were stored frozen (at -70°C) in a biobank until forthcoming analysis.
Approximately 7% were examined in their own home or at other smaller hospitals in the region around Uppsala. Performance-based data were collected at one time in the hospital by one person (BV): motor func-tion (M-MAS UAS-99) (109); mobility (SPPB) (110); balance (BBS) (104) and the 10-m walking test (111, 112) at a self-selected pace were recorded. Age and comorbidity were collected via patient records and questionnaires. Level of cognition (SPMSQ) (113) and self-reported data such as FoF and number of falls within the last year were also obtained at the time of the assessment. The cognition test was performed as a face-to-face interview.
Assessed for eligibility
(n=195)
Analyzed in the
IG
(n=20)
Analyzed in the
CG
(n=23)
Randomized (n=43)
Did not undergo BIA (n=22) because of
• Reduced static balance and standing capacity (n=17)
• Pacemaker (n=4) • Technical error (n=3)
Baseline testing (n=67)
Allocation

32
In addition, data were recorded at the clinical examination for further use in paper II and paper IV: body composition (BIA), nutritional status (MNA-SF) (106) and current prescribed drugs. Data were also obtained from RS register at the time of the stroke, including risk factors such as diabetes mel-litus, atrial fibrillation, hypertension, smoking, and previous stroke or TIA. At the 1 year follow-up, the participants’ need for social support and infor-mation on whether they were living alone were gathered from the RS regis-ter.
Procedure in paper III and IV (Randomised controlled trial) All individuals were informed about the study and had provided written in-formed consent before entering the study. Sixty-seven individuals from study I were randomised to an intervention group (IG, n=34; progressive resistance and balance (PRB) exercise program twice weekly for 3 months) or a control group (CG, n=33) in paper III. An experienced physiotherapist, blinded to group allocation, performed all the assessments at study start, and after 3, 6 and 15 months, respectively.
In Paper III, the Primary outcomes were: Balance (Berg Balance Scale) (104) and mobility (Short Physical Performance Battery) (114) at 3 months. The Secondary outcomes were: walking capacity (The 6-MWT) (115), 10-m comfortable walking speed (111), physical activity levels (The PASE) (103), health-related quality of life (EuroQol-5D (EQ-5D) (102), depression (The Geriatric Depression Scale (GDS-20) (107), and fall-related self-efficacy (the Swedish version of the Falls Efficacy Scale FES(S) (39). Approximately 1 year after stroke, 43 of the 67 selected individuals pre-sented in paper III (n=67) were further analysed in paper IV. They were part of the same intervention group as previously described in paper III (IG, n=20; progressive resistance and balance exercise program twice weekly for 3 months) or a control group (CG, n=23). Primary outcomes were: FFMI, kg/m2, FMI, kg/m2 and how potential changes in body composition related to improved physical function includ-ing walking capacity, balance and mobility. Secondary outcomes were: car-diometabolic risk markers and bio-chemical indicators of growth and nutri-tion.

33
Assessments (paper I-IV) An overview of the different measurements in the papers is given in table 1.
Table 1. Assessments used in paper I-IV
Design Cross-sectional RCT Assessments Paper I
n=195 Paper II n=134
Paper III n=67
Paper IV n=43
Body structure and function Body composition, BIA x x Body Mass Index, BMI x x Depression, GDS-20 x x Cognition, SPMSQ x x x x Inflammatory, nutritional and cardiometabolic biomarkers
x
x
Body function and activity Motor function, M-MAS x x x Nutritional status, MNA-SF x x Activity Bergs Balance Scale, BBS x x x Mobility, SPPB x x x x 10 MWT x x x 6-MWT x x Participation HRQoL, EQ-5D x x Physical activity scale for the elderly, PASE
x
x
x
x
Personal factors Fear of falling, FOF x Fall-related self-efficacy, FES(S)
x x
Falls, yes/no x Abbreviations: RCT. Randomized Controlled Trial; 6MWT, the 6-Minute Walk Test; 10mWT, the 10 meter walk test.
Demography and morbidity Demographic data, including age, gender and comorbidity, were collected via patient records and questionnaires. The Charlson Comorbidity Index (CCI) was used to classify comorbid conditions (116). Leukoaraiosis was identified by roughly screening brain imaging answers at the time of the stroke. Blood pressure was measured manually with the subject in the supine position after resting for 10 minutes. Values were recorded once to the near-est even figure.
The following assessments are ordered according to the International Classification of Functioning, Disability and Health (ICF) (1).

34
Body structure and function: Body composition measurements Body composition as measured by BIA was performed with Tanita total innerscan BC-545, Tanita Inc., Tokyo, Japan, with age, gender, weight, height and exercise specificity. Measurements were performed while the individual was standing and while weighing the individual barefoot with light indoor clothing. BIA actually determines resistance to the flow of an electric current through body tissues for estimation of total body water and calculation of FFM in absolute kg and FM as a percentage of total mass.
Definition of FFM depletion: FM (kg) was calculated using FM% multi-plied with body weight divided with 100. The FMI, (kg/m2) was calculated as the FM (kg) divided by the height (m) squared. The FFMI was calculated as FMI subtracted from BMI, i.e., skeletal muscle, bone and organ weight was considered (117).
Definition of FMI: Fat mass was measured in kg and was normalised to the subject´s height (m) squared into an FMI.
Definition of obesity: Obesity was defined by a FM% and FMI above the 90th percentile of a reference population (67). Reference values for FM% are 20-30% for women and 12-20% for men (118). Further, BMI values ≥ 30 kg/m² also indicated obesity.
Body Mass Index BMI (kg/m²) was calculated from the individual’s weight (kilogram) and height in meters square, kg/m², in accordance with the World Health Organi-zation (WHO) standards (119). Values < 18.5 kg/m² were considered under-weight, values between 18.5-24.9 kg/m² were considered normal, values from 25 to 29.9 kg/m² were considered overweight and values ≥ 30 kg/m² indicated obesity.
The Geriatric Depression Scale Depression symptoms were assessed using the Geriatric Depression Scale (GDS-20) (107). The original version has been tested for reliability and va-lidity in subjects who have experienced a stroke (120, 121). The GDS has 20 items (0-20 points) and includes insomnia, anxiety, panic, pain, and hypo-chondria (107). Greater than or equal to 6 points was used as the cut-off for possible depression.
Short Portable Mental Status Questionnaire The Short Portable Mental Status Questionnaire was used to evaluate cogni-tion (113). It consists of 10 questions, such as, “Who is the present prime minister?” Ten correct answers give a maximum score of 10. The scale has been tested for reliability and validity when administered by telephone (105).

35
Inflammatory, nutritional and cardiometabolic biomarkers Non-fasting venous blood samples were drawn, and the samples were frozen at - 70°C. The biochemical variables were as follows: apoB/apoA1-ratio, total cholesterol, Low Density Lipoprotein (LDL), High Density Lipoprotein (HDL), plasma albumin, serum IGF-1 and CRP. The biochemical analyses were performed and analysed in agreement with the Department of Clinical Chemistry at the Uppsala University Hospital, Sweden. Apolipoprotein A1 and B, total cholesterol, LDL, HDL, albumin and CRP were analysed on an Abbott Architect ci8200 Analyzer (Abbott Laboratories, Abbott Park, IL, USA) using reagents obtained from Abbott. IGF-1 was analysed on a Sie-mens Immulite 2000 XPi with reagents obtained from Siemens (Siemens AG, Erlangen, Germany).
Body function and activity Modified Motor Assessment Scale UAS-99 The Modified Motor Assessment Scale UAS-99 (M-MAS UAS-99) was used to assess motor impairments (109), which includes eight areas of motor function, e.g., transfers, arm and hand function, and one item related to sit-ting balance. The maximum score is 55, indicating a good overall perform-ance (109). The original M-MAS has been used in stroke-affected individu-als and has well-established reliability and sensitivity (122).
Nutritional status A Mini Nutritional Assessment scale-Short Form (MNA-SF) (123) was used to identify nutritional status. The MNA-SF consists of six questions and anthropometric measures that cover the past three months and address food intake and weight loss, mobility, acute diseases or psychological stress and neuropsychological problems (123). The scale is scored from 0 to 14. Nor-mal nutritional status without risk for malnutrition is indicated by a score of 12 or more. Risk for malnutrition is indicated by a score of 7 to 11; current malnutrition is indicated by a score of less than 7 points (123). Malnutrition was also estimated according to BMI < 22 kg/m², which implies a risk for malnutrition in individuals’ ≥ 65 years old and in individuals who have ex-perienced a stroke. MNA-SF is found to be reliable and valid among an older population (106, 124).
Activity The Berg Balance Scale Functional balance was assessed using the Berg Balance Scale (104). It con-sists of 14 balance items, mainly in standing positions, and is scored from 0 to 56 points. Each item is scored 0 to 4 points. A higher score indicates bet-

36
ter balance. A cut-off of 45 points has been used to predict which individuals are not likely to fall (112). The scale is valid and reliable and is frequently used in individuals with stroke (104, 125).
Short Physical Performance Battery Mobility was assessed by the SPPB (110), which includes an assessment of balance, gait speed, and chair rising. The performance is scored from 0 to 4, providing a sum score of 12 points, where a higher score reflects better mo-bility. The SPPB is valid and reliable in older persons (54, 114, 126). By converting the 10 mWT (m/s) into 5 subgroups based on the walking speed, we were able to give 0 to 4 points for walking speed on the SPPB. 0 points (p) = not able to walk, 1p = ≤ 0.43 m/s, 2 p = 0.44-0.60 m/s, 3 p = 0.61-0.77 m/s, 4p = ≥ 0.78 m/s. Classification of limitations based on Short Physical Performance Score: 0-3 severe limitations; 4-6 moderate limitations; 7-9 mild limitations; 10-12 minimal limitations (127).
10-meter walking test (10mWT) The 10-mWT (self-selected pace) (111, 112) was used to measure gait-speed. The time taken to walk was measured with a stop watch while the observer stood behind the participant. Definition of slow walking speed: a cut-off of > 1.0 m/s was used for normal walking speed. The test has accept-able psychometric properties in individuals who experienced a stroke (111).
The Six-Minute Walk Test (6-MWT) This test was developed to assess cardiopulmonary function and was used in this thesis to evaluate walking capacity (128). The maximal distance at a usual pace over a 30 m course during 6 minutes was recorded (129). The test was standardised according to the American Thoracic Society and feed-back was given each minute (129). Heart rate and perceived exertion were recorded before starting and after the test. The test is used in individuals with cardiopulmonary problems and stroke (84, 130) but reliability and validity has not been established for stroke patients.
Participation Health-related quality of life EuroQol-5D (EQ-5D) was used to assess health related quality of life, either by assessing 5 items (mobility, self-care, usual activities, pain/discomfort and anxiety/depression), each with three levels, or by using EQ-VAS as a rating scale from 0 to 100 (102). A weighted index value between 0 and 1 was calculated, where 1 indicated the highest quality of life. Any value from the index scale below 0 was calculated as a score of 0. EQ-5D is valid and reliable in individuals who have experienced a stroke (131, 132).

37
Physical Activity Scale for the Elderly The PASE assesses level of physical activity in elderly individuals (103). The calculation of the PASE score was performed by taking the average number of hours spent on an activity per day in the prior week multiplied by an activity coefficient. The item categories are walking outside the home, light sports, moderate sports, strenuous sports, muscle strength, light house-work, heavy housework, home repairs, lawn work or yard care, outdoor gar-dening, caring for another person and work for pay or as a volunteer. The PASE score may range from 0 to more than 400. The original scale has an acceptable reliability and has been used in subjects that have experienced a stroke. In addition, the scale is valid in elderly persons with disabilities and stroke (103, 133-135).
Personal factors Fear of falling One single-item question was used to assess fear of falling: “Are you afraid of falling?” Answers of “yes” or “no” were used to dichotomise the items. The question was constructed for this study.
The Swedish version of the Falls Efficacy Scale Fall-related self-efficacy was assessed using the Swedish version of the Falls Efficacy Scale FES(S). This questionnaire consists of 13 activities, including both personal and instrumental activities of daily living (108). The confi-dence when performing the different activities was rated using a visual ana-log scale ranging from 0 (not confident at all) to 10 (completely confident). FES(S) has a maximum score of 130 and has an acceptable test-retest reli-ability and validity for assessing subjects who have experienced a stroke (108, 136).
Falls One single-item question was used to assess falls: “Have you fallen in the last year?” Answers of “yes” or “no” were used to dichotomise the items. The question was constructed for this study.
Exercise intervention (Paper III-IV) Individuals assigned to the exercise intervention, i.e., the progressive resis-tance and balance (PRB) exercise program, received a graded circuit class training program twice a week for 3 months. The training consisted of dif-

38
ferent work stations with functional exercises involving the major muscle groups, particularly the lower extremity function (Table 2) (137).
Table 2. Descriptions of the progressive resistance and balance exercise program and the group discussion.
Warming up: Stationary cycling or walking Progressive resistance and balance exercises:
Squat in a parallel or walking stance A1 Body weight transfer in a parallel or walking stance A2, A3 Standing up from sitting in parallel or walking stance A4, A5 Side and forward lunge A6, A7 Step-up A8 Walking forward in tandem gait B1 Walking in various directions B2 Walking with turns B3, B8 Walking over obstacles B4 Step onto and over boxes B5 Walking on a soft surface Questions concerning physical activity: “What is a physical activity to you?” “What are the barriers and facilitators for you to be physically active?” “What reasons do you perceive for increasing your physical activity level in your daily life?” “How ready are you to make changes to your physical activity level in the near future?” “What pro and cons do you perceive with being physically active?” “How much time do you spend sitting each day?” “What are your future plans to be physically active?”
B6
A: static (fixed base of support) and dynamic (changing base of support) balance exercises in combination with strength exercises B: dynamic balance exercises while walking
The intervention included three stages: 1) warming up (10 minutes; station-ary cycling or walking), 2) circuit training (approximately 45 minutes) and 3) motivational session consisting of discussions related to physical activity (20 minutes). A short rest of 5-10 minutes was also provided after the first seven exercises. The exercises were retrieved from the high intensity func-tional exercise program (HIFE) (137).
The exercises applied in the RCT were performed at a low to moderate in-tensity and were intended to improve strength and muscular endurance. At least 10 repetitions were performed for each exercise in accordance with statements from the ACoSM/AHA (90, 138). Any medical reason for drop out was recorded together with exercise fidelity (e.g., attendance and weight progression). The Borg scale of perceived exertion was used to regulate the intensity throughout the study (139). During training, all individuals wore a belt around their waist that could be loaded with individual weights ranging from 1–12 kg. The program consisted of 14 exercises. The first 7 exercises

39
in the circuit training were combined balance and lower-limb strength exer-cises. The next 7 were balance exercises performed while walking. The indi-viduals worked in intervals at their own highest possible intensity for 2 min-utes, followed by 1 minute to rest and change to the next exercise. The exer-cise progression included increasing the weights according to the perceived exertion or adjusting the exercise performance to increase the balance de-mands (137).
One physiotherapist and one assistant conducted the PRB exercise pro-gram, and the number of participants ranged from 2 to 7. An individually tailored home-exercise was added to support the in-house PRB exercise pro-gram. During the group discussion, physical activity behaviour and risk fac-tor modifications were discussed for 20 minutes. One or two questions were discussed at each session from an individualised perspective. Follow-ups of the home-exercises were also included.
Serious adverse advents were defined as any fall or other adverse advents, such as heart problems, occurring during training. Level of exercise and physical activity were only recorded during the assessments at 3, 6 and 15 months.
Individuals allocated to the control group were not encouraged to make any changes in their daily lives; however, they were not restricted from be-ing physically active.
Statistics Analyses used in paper I-IV are presented in table 3. All statistical analyses were performed by BV with some supervision from Uppsala Clinical Re-search Center.
Table 3. Statistical analyses used in paper I-IV
Cross-sectional Randomized con-trolled trial
Methods Paper I
Paper II
Paper III
Paper IV
Descriptive analysis Median and interquartile range X X X X Numbers and frequencies X X X X Mean and standard deviations X X X X Distribution of data Shapiro-Wilk W test X X X X Histogram X X X X Differences between groups: Chi-squared test X X X X Fishers exact test X X X X

40
Student´s two sample t-test X X Mann-Whitney U-test X X Wilcoxons sign-rank test X X Paired sample t-test X Area under the receiver operating characteristics curve
X
X
Cohen´s d test X Associations between variables: Pearson´s correlations coefficient Spearman´s rank correlation
X X
X X
X X
X X
Linear regression X Binary logistic regression X
Descriptive statistics Descriptive statistics were used for demographic data in all studies. Continu-ous variables were presented as the mean and standard deviation (SD). Given ordinal data, the median and the inter-quartile range (IQR) were pre-sented. For nominal data, absolute or relative numbers (%) or both were described.
Statistics: Paper I-II The statistical analyses included both descriptive univariate and multivariate models. Two separate multiple linear regression models were used to explore factors associated with mobility (SPPB) or physical activity (PASE).
Before explanatory variables were included in the multivariate regression models, unadjusted (i.e., univariate) analyses were conducted. The correla-tion between the dependent variables SPPB and PASE, together with poten-tial independent variables, were analysed using the Spearman´s rank correla-tion. Further, all significant independent variables were included in the mul-tivariate analysis. Both mobility and physical activity scores were treated as quantitative and continuous variables in the analyses. Ordinal explanatory variables were dichotomised due to median values or a known cut-off. The SPPB was used as the independent variable when the PASE was the depend-ent variable and vice versa. All regression analyses were controlled for age, sex and comorbidity. The variance inflation factors (VIF) were calculated and found acceptable. The residuals were normally distributed and no stan-dardised residuals >3 were found. A variance explained by an adjusted R square 0-0.25 was considered little to poor, 0.25-0.50 fair, 0.50-0.75 moder-ate and ≥ 0.75 very good to excellent (140). When data were missing for one item (chair-stand, SPPB, n=24), it was replaced with information from a

41
similar subscale (sit to stand, M-MAS). A total of 195 individuals were in-cluded and the amount of missing data did not exceed 3% in any scale, but totalled 9% all together. Imputation by group mean or median values was performed in cases of missing values.
In paper II, the data were categorised into two different age classes: 65-74 years and 75-85 years. The results are reported separately for men and women. The amount of missing data in the present study was low, and the imputation technique originated from paper I. The correlation between the SPPB and potential independent variables were analysed using the Spear-man´s rank correlation. Logistic regression models were used to predict bi-nary outcomes in the presence of several explanatory variables after testing for multi-collinearity. Odds ratios and 95 % CIs for low versus high mobil-ity, with SPPB as a dependent variable, were calculated to determine inde-pendent covariates. Univariate binary logistic analysis was used to analyse the associations with mobility (SPPB). Body composition was not signifi-cantly associated with the SPPB and was therefore excluded from further analyses. Nutritional status (MNA-SF), physical activity (PASE), age and gender were used as independent variables. Identified independent variables with a P-value <0.05 were further included in the multiple logistic regression models. All estimates were adjusted for age (65-74 and 75-85 years) and gender.
To estimate the prevalence of sarcopenia and sarcopenic obesity, different percentiles of a gender- and age-matched reference population were used to define the conditions (67). For details, see paper II.
Statistics: Paper III-IV The RCT presented in paper III was designed to have 80% power to detect a 2-point difference on the Berg Balance Scale between the exercise and con-trol group with a standard deviation of 8 points and with the statistical sig-nificance level set at 0.05 (two-tailed) for all analyses. This calculation was based on effects from a pilot study performed prior to the PRB exercise group. However, this exercise study was completed with fewer participants than had been calculated for as a result of statistically significant improve-ment on the BBS (primary outcome) and slow recruitment.
The intention-to-treat principle was applied in the analyses using all available data according to the individuals´ original group assignment. A multiple imputation was performed for missing values according to the hot deck method (141). This technique sorts available respondents in certain subsets; in this study, gender and comorbidity. Values selected randomly from matching subjects were used to replace missing data. If no matching subject was detected, data were randomly selected from the entire dataset. In addition, a complete case analysis was also performed.

42
An attendance rate was calculated for each participant as the number of attended exercise sessions divided by the total sessions. Because the distribu-tion of data was unknown and included some outliers, the Mann-Whitney U-test was used for all between-group analyses at 3, 6 and 15 months. The me-dian differences in changes were calculated as Hodges-Lehmann estimates. The difference between the individuals´ pre- and post-treatment data was used to calculate the effect size by using the area under the receiver operat-ing characteristics curve (AUC). The null hypothesis was that the true area = 0.5 indicated no differences in effect between the groups. A complete case analysis was also applied and was performed in a similar manner as the in-tention to treat analysis.
Paper IV was considered to be exploratory. All statistical analyses are based on complete case analysis. An attendance rate was calculated for each participant as the number of attended exercise sessions divided by the total sessions. The results are reported separately for men and women. Cardiovas-cular disease risk scores (CRS) was calculated using a prediction algorithm based on age, resting blood pressure, smoking status at the time of stroke, diabetic status, total cholesterol and HDL (142). Smoking status and diabetes were considered unchanged at 3 months. Student´s two-sample t-test was used to compare changes between the exercise and control groups during the intervention period, given normal-distributed and continuous data. Given ordinal or not normally distributed data, the Mann- Whitney U-test was used for between-group analysis at 3 months. Within-group effects for continuous variables were analysed by paired sample t-test, comparing outcome meas-ures at baseline and after 3 months, respectively. Given not normally distrib-uted or ordinal data, the Wilcoxons sign-rank test was used to analyse within group changes from baseline to 3 months. The association between changes in FFMI or FMI and changes in the 6MWT at 3 months was evaluated either using Spearman´s rank correlation or Pearson´s correlation coefficient.
All statistical analyses were performed with SPSS 19.0 (IBM, Armonk, NY, USA) and were considered statistically significant if P > 0.05.

43
RESULTS
Associations with mobility and physical activity in elderly community-living individuals (paper I-II). In paper I, 195 individuals were included. Eighty-one individuals declined full participation but answered questions on the EQ-5D (56% women). The mean age at study start was 74±5 years. A median of 13 months had passed since stroke onset. The proportion of men was 71%. The distribution of 1 or more comorbidities according to the Charlson Comorbidity Index was 41%. Mobility was reduced with a SPPB score of less than 10 points in 50% of the individuals, walking speed was slower (1.10 ± 0.86 m/s), and level of physical activity was lower (mean PASE 97 ± 66 points) in older individuals following stroke compared to age-matched healthy controls (35). The me-dian value of motor function according to M-MAS UAS-99 was 55 points and 59% reached the highest possible score, indicating ceiling-effects and high motor function. Possible depression and FoF were reported in more than one-third of individuals post-stroke. The proportion of more than one fall in the most recent year was reported to be 46%. The EQ-5D was slightly reduced compared to an age- and gender matched reference population (143). Furthermore, the EQ-5D scores were 0.63 and 0.73 in the not fully participating and the full participants, respectively (P= 0.006). Additionally, corresponding EQ-5D VAS mean scores were 0.54 and 0.71, respectively (P= <0.001).
Factors explaining the variance in mobility were age, physical activity, fall-related self-efficacy and health-related quality of life, which described 42% of the variance in mobility (SPPB) for older individuals after stroke (Table 4).

44
Tab
le 4
: Mul
tipl
e re
gres
sion
ana
lyse
s w
ith
perf
orm
ance
-bas
ed m
obil
ity
(SP
PB
) as
the
depe
nden
t out
com
e va
riab
le a
nd a
ge, s
ex, c
omor
bidi
ty,
fall
-rel
ated
sel
f-ef
fica
cy, c
ogni
tive
impa
irm
ent,
phys
ical
act
ivit
y, d
epre
ssio
n, H
RQ
oL, f
ear
of f
alli
ng a
nd f
alls
as
the
inde
pend
ent v
aria
bles
in
indi
vidu
als
1-3
year
s af
ter
stro
ke (
n=19
5).
U
niv
aria
te a
nal
ysis
M
ult
ivar
iate
an
alys
is
B
eta
P 95
%C
I B
eta
P 95
%C
I A
ge, y
-.
26
<.0
01
-.2
to -
.7
-.19
.0
01
-.17
to -
.045
F
emal
e se
x -.
06
.38
-1.3
to .5
CC
I -.
11
-.12
-.
8 to
.1
F
alls
-rel
ated
sel
f-ef
fica
cy,
FE
S(S
), <
124
poin
ts
-.
51
<
.001
-3.6
to -
2.2
-.
24
.0
01
-2
.2 to
-.5
5 C
ogn
itiv
e im
pai
rmen
t,
SP
MS
Q, 1
0 po
ints
-.26
<.0
01
-2
.4 to
-.7
Ph
ysic
al a
ctiv
ity,
P
AS
E ≥
0 p
oint
s
.52
<
.001
.02
to .0
3
.29
<
.001
.007
to .0
18
Dep
ress
ion
, G
DS
, ≥ 6
poi
nts
-.
26
<
.001
-2.4
to -
.7
HR
QoL
, EQ
-5D
, 0-1
.4
8 <
.001
4.
0 to
6.8
.1
8 .0
2 .3
5 to
3.5
6 F
ear
of f
alli
ng, y
es
-.23
.0
01
-2.2
to -
.6
F
alls
, yes
-.
21
.003
-2
.0 to
-.4
Tot
al a
dju
sted
R2 =
0.42
A
bbre
viat
ions
: C
CI,
Cha
rlso
n C
omor
bidi
ty I
ndex
; C
I, c
onfi
denc
e in
terv
al;
Eur
o-Q
oL,
EQ
-5D
; F
ES
(S),
Fal
l-re
late
d S
elf-
effi
cacy
Sca
le (
Sw
edis
h ve
rsio
n),
Swed
ish
vers
ion
of th
e G
eria
tric
Dep
ress
ion
Scal
e; H
RQ
oL, h
ealth
-rel
ated
qua
lity
of li
fe; P
ASE
, Phy
sica
l Act
ivity
Sca
le f
or th
e E
lder
ly;
SP
MS
Q, S
hort
Por
t-ab
le M
enta
l Sta
tus
Que
stio
nnai
re; S
PP
B, S
hort
Phy
sica
l Per
form
ance
Bat
tery
. P
< 0
.05.

45
Tab
le 5
. Mul
tipl
e re
gres
sion
ana
lyse
s w
ith
self
-rep
orte
d ph
ysic
al a
ctiv
ity
(PA
SE
) as
the
depe
nden
t out
com
e va
riab
le a
nd a
ge, s
ex, c
omor
bidi
-ty
, m
obil
ity,
fal
l-re
late
d se
lf-e
ffic
acy,
cog
niti
ve im
pair
men
t, de
pres
sion
, HR
QoL
and
fea
r of
fal
ling
as
the
inde
pend
ent v
aria
bles
in in
divi
du-
als
1-3
year
s af
ter
stro
ke (
n=19
5).
U
niv
aria
te a
nal
ysis
M
ult
ivar
iate
an
alys
is
B
eta
P
95%
CI
Bet
a
P 9
5% C
I A
ge, y
-.
11
.13
-3.2
to 0
.4
Fem
ale
sex
-.05
.4
9 -2
7.6
to 1
3.3
CC
I -.
13
.17
-17.
8 to
3.2
Mob
ilit
y, S
PPB
, ≤
9 po
ints
.5
<
.001
-81.
8 to
-49
.5
-.
33
<
.001
-.50
to -
.32
Fal
ls-r
elat
ed s
elf-
effi
cacy
, F
ES
(S),
<12
4 po
ints
-.43
<.0
01
-7
3.5
to -
40.0
-.18
.031
-.42
to -
.16
Cog
nit
ive
imp
airm
ent,
S
PM
SQ
, 10
poin
ts
-.
20
.0
05
3.
6 to
20.
5
Dep
ress
ion
, GD
S,
≥ 6
poi
nts
-.
28
<
.001
-56.
1 to
-19
.3
HR
QoL
, EQ
-5D
, In
dex
0-1
-.43
<.0
01
78
.9 to
144
.4
.1
9
.014
.44
to .1
8 F
ear
of f
alli
ng, y
es
-.4
.051
-3
8.0
to .9
3
Tot
al a
dju
sted
R2 =
0.31
A
bbre
viat
ions
: C
CI,
Cha
rlso
n C
omor
bidi
ty I
ndex
; C
I, c
onfi
denc
e in
terv
al;
Eur
o-Q
oL,
EQ
-5D
; F
ES
(S),
Fal
l-re
late
d S
elf-
effi
cacy
Sca
le (
Sw
edis
h ve
rsio
n);
Swed
ish
vers
ion
of th
e G
eria
tric
Dep
ress
ion
Scal
e; H
RQ
oL, h
ealth
-rel
ated
qua
lity
of li
fe; P
ASE
, Phy
sica
l Act
ivity
Sca
le f
or th
e E
lder
ly;
SP
MS
Q, S
hort
Por
t-ab
le M
enta
l Sta
tus
Que
stio
nnai
re; S
PP
B, S
hort
Phy
sica
l Per
form
ance
Bat
tery
. P <
0.0
5.

46
One additional multiple regression analyses model was further performed; mobility, HRQoL and fall-related self-efficacy were related to physical ac-tivity (PASE) and described 31% of the variance (Table 5). Both analyses were controlled for sex, age and comorbidity.
Paper II was complemented by measurements of body composition, BMI, cardiometabolic risk markers and nutritional status; 134 individuals of the 195 individuals in paper I were analysed. The mean age was 74 ± 4 years and the proportion of men was 69%. The BMI values indicated that 71% of the individuals studied were overweight or obese (BMI > 30 kg/m2 in 22%). Total percent fat mass (FM%) was > 20 in 86% of the men, whereas 90 % of the women had an FM% above 30% of the reference population. Fourteen percent were considered at-risk for malnutrition according to MNA-SF. Walking speed was slow (1.08 ± 0.25 m/s), and the level of physical activity was low (mean PASE 108 ± 65 points) in the study population. Further, mo-bility was affected (median SPPB of 10 points) and SPPB cores ≤ 9 in 40% indicated increased risk for disability. Sarcopenia, i.e., reduced FFMI and a gait speed < 1 m/s, was noticed in 3% while 7% displayed sarcopenic obe-sity defined as increased FMI together with reduced FFMI. Further, a sig-nificant association between chair-stand, one item in the SPPB, and physical activity (r= -0.35, P>0.001), nutritional status (r= -0.21, P=0.015) and FMI (r= 0.21, P= 0.017) were revealed.
Neither FFMI nor FMI was associated with mobility, as measured by the SPPB, in this cohort. The logistic regression analysis revealed that the fac-tors associated with low mobility was low physical activity, Odds Ratio; OR (CI 95%) 8.2 (2.8-24.2), risk for malnutrition, OR 5.8 (1.6-21.1) and each 10-year period, OR 2.8 (1.2-6.2) (Figure 3).

47
Figure 5. The odds ratio of low mobility (SPPB) based on the Physical Activity Scale for the Elderly (PASE; medium vs. high and low vs. high) and the Mini Nutri-tional Assessment-Short Form (MNA-SF). Analyses were adjusted for gender and age (per 10-year increment).
Furthermore, 10% percent of the individuals had plasma cholesterol concen-trations ≥ 6 mmol/l and LDL values ≥ 3.5 mmol/l. Women had significantly higher total cholesterol and HDL levels compared to men.
The short-term and long-term effects of a progressive resistance and balance exercise program in elderly community-living individuals after stroke (paper III-IV). Of 67 individuals randomly assigned to the PRB exercise program (interven-tion group, IG, n=34) in paper III, 57 individuals completed the whole inter-vention period (85%). At 3 months, in the short-term, the attrition rate was 24% in the PRB exercise group, increasing to 29% at 15 months. Thirty-

48
three individuals were included in the control group (CG) and the attrition was 6%. The proportion of males was 76% (mean age: 74±5 years). Accord-ing to the GDS, approximately 42% scored > 6 points at baseline, indicat-ing possible depression. Sixteen percent of the participants scored < 45 points on the BBS and 63% scored < 10 points on the SPPB at baseline measurements. Motor function was considered to be high at baseline. Age and gender did not differ between PRB exercise completers and drop-outs, but differences were noted in the BBS and motor function M-MAS UAS-99, with the drop-outs having significantly less scores. Attendance rate in the exercise group was 91% (median). In addition, no adverse events were noted during exercise.
The Intention-to treat analysis revealed that the PRB exercise group was associated with significantly higher scores in terms of balance (2.5 vs. 0 points, ES; 0.72 (SE 0.062); P=0.001), walking capacity (30 vs. 0 m, ES; 0.64 (SE) 0.07); P=0.05) and comfortable walking speed (0.04 vs.-0.05 m/s, ES; 0.68 (SE 0.067); P=0.012) compared to the control group at 3 months (Table 6). There were no other significant differences between the groups for any other outcomes at any time point. The complete case analysis confirmed this result (data not shown).
In paper IV, 20 individuals were analysed from the PRB exercise group described in paper III and 23 individuals from the control group, due to available BIA measurements. The mean age was 73±5 years (73% men). In both groups (at study start), BMI indicated that the individuals were over-weight or obese and had an average supine blood pressure values above rec-ommended levels, e.g., 58%. No significant between or within-group changes in BMI or blood pressure were seen after 3 months of exercising. Cardiovascular disease risk score revealed a 10 year increased risk of a fu-ture cardiovascular disease event > 20% at baseline, with no between-group changes present at 3 months.
At 3 months, a complete case analyses revealed a significant reduction in the PRB exercise group in terms of FM% (-1.5 vs. 0.13%; effect size, ES, 0.62, standard error (SE), 0.80; P=0.0.39) and a decrease in serum IGF-1 (-12 vs. 4 μg/l, ES; 0.62, P=0.026) compared with the control group, whereas levels of CRP and albumin were stable (Table 7).
A significant within-group reduction in the FM% (-1.50, ES; 0.56, P=0.023) and fat mass (FM, kg) (-1.47, ES; 0.57 P=0.021) of the IG, but not in the CG (-0.19 kg, ns), were also revealed. Changes in FMI were associated with improved walking capacity (6MWT, 25 vs. -10 m) at 3 months, in favour of the IG (r=0.47, P= 0.04).

49
Tab
le 6
. Phy
sica
l Fun
ctio
n, P
hysi
cal A
ctiv
ity a
nd P
sych
olog
ical
Fac
tors
aft
er 1
2 w
eeks
of
PR
B e
xerc
ise
or C
ontr
ol G
roup
rev
eale
d by
the
Inte
ntio
n-T
o-T
reat
ana
lysi
s
PR
B e
xerc
ise
(n=
34)
Con
trol
Gro
up
(n
=33
)
Out
com
e m
easu
re
A
sses
smen
t B
asel
ine
leve
l an
d
Ab
solu
te C
han
ge
Med
ian(
IQR
)
Bas
elin
e le
vel a
nd
A
bso
lute
Ch
ange
M
edia
n(IQ
R)
Med
ian
Dif
fere
nce
in C
han
ge (
95%
CI)
E
ffec
t si
ze
(ES
) P
-Val
ue
BB
S
(0-5
6 po
ints
) B
asel
ine
3 m
o 6
mo
15 m
o
49(6
) 2.
5(5)
1(
4)
1(3)
51(7
) 0(
2)
0(3)
0(
3)
-2
.5(-
4 to
-1)
-1
(-3
to 1
) -2
(-4
to 0
)
0.
72
0.
001
0.24
0.
06
SPP
B
(0-1
2 po
ints
) B
asel
ine
3 m
o 6
mo
15 m
o
9(4)
1(
2)
0(2)
1(
3)
9(3)
0(
1)
0(1)
0(
2)
-1
(-1
to 0
) 0(
-1 to
1)
0(-2
to 0
)
0.09
0.
68
0.3
6-M
WT
, met
ers
Bas
elin
e 3
mo
6 m
o 15
mo
365(
198)
30
(72)
25
(97)
-7
(71)
345(
198)
0(
40)
25(7
0)
0(47
)
-2
5(-5
0 to
0)
-10(
-45
to 2
0)
5(-2
0 to
30)
0.
64
0.
05
0.46
0.
77
10m
WT
,(m
/s)
B
asel
ine
3 m
o 6
mo
15 m
o
1.0(
0.59
) 0.
04(0
.24)
0.
09(0
.22)
0.
9(0.
24)
1.11
(0.5
2)
-0.0
5(0.
21)
-0.0
07(0
.24)
-0
.07(
0.26
)
-0
.11(
-0.1
9 to
-0.
03)
-0.1
5(-0
.24
to -
0.06
) -0
.11(
-0.2
1 to
0.0
07)
0.
68
0.
012
0.00
1 0.
034
PA
SE
(≥0
poi
nts)
B
asel
ine
3 m
o 6
mo
15 m
o
79(8
0)
10(7
7)
-3(5
9)
1(60
)
59(9
5)
2(71
) 10
(64)
-2
(60)
-0
.5(-
26 to
26)
-2
1(-3
to 4
9)
4(-1
8 to
34)
0.96
0.
074
0.74
E
Q 5
D,
(0-
1)
Bas
elin
e 3
mo
6 m
o 15
mo
0.72
5(0.
23)
0(0.
22)
0(0.
33)
0(0.
30)
0.72
5(0.
23)
0(0.
16)
0(0.
17)
0(0.
22)
0(
-0.1
2 to
0.0
5)
0.04
7(0
to 0
.16)
0.
016(
-0.0
9 to
0.1
2)
0.63
0.
17
0.56

50
GD
S-2
0 (0
-20
poin
ts)
Bas
elin
e 3
mo
6 m
o 15
mo
3(9)
-1
(5)
-1(4
) -1
(5)
6(7)
0(
2)
-1(3
) -1
(2)
0(
-2 to
1)
0(-1
to 2
) 0(
-2 to
1)
0.
89
0.61
0.
69
FE
S(S
) (0
-130
poi
nts)
B
asel
ine
3 m
o 6
mo
15 m
o
0(26
) 0(
26)
-2(2
4)
0(31
)
0(20
) 0(
20)
0(26
) 0(
27)
0(
-10
to 7
) 2(
-8 to
11)
-2
(-17
to 6
)
0.83
0.
60
0.56
A
ll v
aria
bles
are
obt
aine
d fr
om n
on-p
aram
etri
c an
alys
es. M
edia
n di
ffer
ence
in c
hang
e is
cal
cula
ted
as H
odge
s L
ehm
ans
Est
imat
e.
Abb
revi
atio
ns: B
BS
, Ber
g B
alan
ce S
cale
; FE
S(S
); F
all-
Rel
ated
Sel
f-E
ffic
acy
Sca
le, G
DS
-20,
Ger
iatr
ic D
epre
ssio
n S
cale
; IQ
R, I
nter
quar
tile
ran
ge; P
AS
E,
Phy
sica
l Act
ivit
y S
cale
for
the
Eld
erly
; PR
B, P
rogr
essi
ve R
esis
tanc
e an
d B
alan
ce; S
PP
B; S
hort
Phy
sica
l Per
form
ance
Tes
t; 6
-MW
T, 6
-Min
ute
Wal
k T
est;
10
mW
T, 1
0-m
eter
Wal
k T
est.
P<
0.05
.

51
Tab
le 7
. With
in-g
roup
and
Bet
wee
n-gr
oup
diff
eren
ces
of b
ody
com
posi
tion
and
phys
ical
fun
ctio
n at
the
star
t of
inte
rven
tion
and
afte
r 3
mon
ths.
In
terv
enti
on g
rou
p (
n=
20)
Mal
e (n
=16
), F
emal
e (n
=4)
C
ontr
ol G
rou
p (
n=
23)
Mal
e (n
=15
), F
emal
e (n
=8)
D
iffe
ren
ce B
etw
een
In
terv
enti
on-C
ontr
ol
3 m
onth
s
Ass
essm
ent
occa
sion
B
ase-
lin
e 3-
mo
foll
ow-u
p
Ab
solu
te
Ch
ange
P
-va
lue
Bas
e-li
ne
3-m
o fo
l-lo
w-u
p
Ab
solu
te
Ch
ange
P
-va
lue
Mea
n/M
edia
n
dif
fere
nce
in
chan
ge
(95%
CI)
P-
valu
e
FF
M, k
g, m
edia
n (I
QR
)
0.70
All
indi
vidu
als
-0.7
(7.
8)
0.14
-1
.1 (
4.6)
0.
18
0.50
(-2
.0 to
4.2
)
Mal
e 61
.30
(11.
1)
59.8
2 (7
.6)
-0.8
0 (9
.1)
56
.20
(15.
7)
56.5
(8.
9)
-0.9
5 (3
.0)
Fem
ale
43.1
0 (1
4.2)
42
.57
(3.7
) 0.
75 (
6.6)
47.1
5 (3
.8)
43.2
(7.
0)
-2.6
0 (7
.2)
FF
MI,
kg/
m²,
med
ian
(IQ
R)
All
indi
vidu
als
0.26
(1.
2)
0.53
0.
02 (
1.3)
0.
93
-0.1
6 (-
0.9
to 0
.4)
0.53
Mal
e 19
.95
(2.6
) 20
.09
(2.3
) 0.
13 (
1.4)
20.5
0 (3
.2)
20.7
5 (2
.0)
-0.1
6 (1
.0)
Fem
ale
16.8
3 (1
.4)
17.1
1 (1
.1)
0.44
(0.
7)
17
.8 (
3.3)
17
.51
(1.8
) 0.
06 (
1.9)
FM
, kg,
mea
n (S
D)
All
indi
vidu
als
-1.4
7 (2
.6)
0.02
1
-0
.019
(2.
2)
0.97
1.
45 (
-0.5
to 2
.9)
0.05
7
Mal
e 23
.96
(6.4
) 22
.30
(7.4
) -1
.66
(2.8
)
25.2
3 (
(7.1
) 24
.95
(6.2
) 0.
31 (
2.2)
Fem
ale
30.3
0 (5
.7)
27.4
7 (7
.0)
-0.6
9 (2
.0)
33
.80
(12.
9)
33.2
1 (1
3.0)
-0
.59
(2.2
)
FM
%, m
ean
(SD
)
All
indi
vidu
als
-1.5
0 (2
.7)
0.02
3
0.
13 (
2.6)
0.
80
1.63
(0.
01 to
3.3
) 0.
048
Mal
e 27
.01
(4.9
) 25
.51
(5.9
) -1
.51
(2.9
)
28.5
2 (3
4.8)
28
.22
(3.7
) 0.
41 (
2.3)
Fem
ale
39.6
8 (
3.3)
37
.57
(5.2
) -1
.45
(2.3
)
40.7
8 (8
.7)
40.4
1 (9
.0)
-0.3
8 (3
.0)

52
FM
I, k
g/m
², m
ean
(IQ
R)
All
indi
vidu
als
-0.4
0 (0
.9)
0.05
3
-0
.20
(1.1
) 0.
38
0.20
(-0
.4 to
0.8
) 0.
51
Mal
e 7.
55 (
2.1)
7.
11 (
2.4)
-0
.44
(0.9
)
8.20
(2.
2)
8.07
(1.
9)
-0.1
8 (1
.2)
Fem
ale
11.0
7 (1
.9)
10.5
8 (4
.9)
-0.2
7 (0
.8)
12
.94
(8.4
) 12
.70
(5.2
) -0
.24
(0.9
)
BM
I, k
g/m
², m
ean
(SD
)
All
indi
vidu
als
-0.2
3 (1
.3)
0.42
29
.07
(4.6
)
-0.2
3 (1
.2)
0.36
0.
007
(-0.
8 to
0.8
) 1.
0
Mal
e 27
.4 (
6.0)
27
.1 (
3.3)
-0
.34
(1.4
)
28.3
(3.
1)
28.2
(5.
7)
-0.2
1 (1
.4)
Fem
ale
28.4
(2.
5)
27.9
(2.
9)
0.24
(0.
6)
30
.6 (
6.7)
30
.3 (
6.6)
-0
.27
(0.6
)
PA
SE
(≥0
poi
nts)
m
edia
n (S
D)
100
(72)
11
0 (8
5)
16 (
74)
0.51
90
(86
) 95
(79
) 2
(108
) 0.
78
0.5(
-34.
0 to
36.
0)
1.0
BB
S (
0-56
poi
nts)
, m
edia
n (I
QR
) 51
.5 (
7)
53.5
(5)
1
(3)
0.01
3 52
.5 (
6)
52.0
(4)
1
(1)
0.34
-1
(-2
to 0
) 0.
2 6-
MW
T (
met
ers)
, m
edia
n (S
D)
390
(109
) 42
0 (1
81)
25 (
65)
0.06
7 39
5 (1
41)
385
(170
) -1
0 (4
5)
0.29
-2
5 (-
55.0
to 0
.0)
0.03
9 S
PP
B (
0-12
poi
nts)
, m
edia
n (I
QR
) 9
(5)
11(4
) 0
(3)
0.25
9
(3)
10 (
2)
0 (1
) 0.
12
0 (-
1 to
1)
0.9
Ch
air
rise
(se
c),
med
ian
(IQ
R)
14.0
(6.
1)
13.5
(6.4
) 0.
5 (4
.7)
0.78
17
.0 (
8.1)
15
.0 (
5.2)
0.
05 (
2.6)
0.
64
-0.3
(-1
.9 to
1.9
) 0.
7 D
ata
are
pres
ente
d as
the
mea
ns (
SD)
or m
edia
ns (
IQR
) an
d 95
% C
Is b
ased
on
the
com
plet
e-ca
se a
naly
sis.
The
Hod
ges-
Leh
man
n te
st w
as u
sed
to e
stim
ate
the
med
ian.
P-v
alue
s w
ere
obta
ined
usi
ng n
on-p
aram
etri
c an
alys
es f
or o
rdin
al a
nd n
ot n
orm
al d
istr
ibut
ed d
ata.
The
sig
nifi
canc
e le
vel w
as s
et a
t P<
0.05
. A
bbre
viat
ions
: B
BS
, B
ergs
Bal
ance
Sca
le;
BM
I, B
ody
Mas
s In
dex;
CIs
, co
nfid
ence
int
erva
ls;
FF
MI,
fat
-fre
e m
ass
inde
x; F
MI,
fat
-mas
s in
dex;
FM
, fa
t m
ass;
FM
%, f
at m
ass
perc
ent;
PAS
E, P
hysi
cal A
ctiv
ity S
cale
for
the
Eld
erly
; 6-M
WT
, Six
-Min
ute
Wal
king
Tes
t; S
PP
B, S
hort
Phy
sica
l Per
form
ance
Tes
t

53
DISCUSSION
Summary of results Elderly individuals approximately 1 year after stroke had many apparent reversible disabilities such as low mobility and walking capacity, possible depression, and slow gait-speed even if their motor function was considered high. Further, the level of physical activity was considered low. Another important finding of this thesis was that older individuals who have experi-enced a stroke had a body composition that consists of an increased amount of fat with overweight and obesity, which can lead to further complications. However, only a few individuals revealed low muscle mass. High values of certain cardiometabolic risk factors, e.g., elevated total cholesterol, LDL-cholesterol and hypertension, were depicted despite medication. Many of these disabilities and risk factors can be changed by increasing the level of physical activity and having more healthy eating habits. Participation in a 3 month progressive resistance and balance exercise program improved bal-ance ability, walking capacity and gait speed, but in the long-term these im-provements were mainly lost. Further, we showed a significant decrease in IGF-1 in favour of the exercise group at 3 months, which might reflect im-proved insulin sensitivity. We were also able to detect a slight increase in muscle mass after exercising together with a similar decrease in FM, while BMI showed an overall reduction except for in the women in the exercise group. Changes in walking capacity were positively associated to changes in fat mass percentage.
Given this result, the negative effects of stroke for community-living eld-erly individuals may be due to modifiable causes, and can be further ad-dressed. A progressive resistance and balance exercise program improves short-term physical function but further efforts are needed for the change to persist over time. Insulin sensitivity and fat mass percentage might as well be lowered by resistance exercising.
Associations to physical function and physical activity Age, physical activity, fall-related self-efficacy and health-related quality of life were related to mobility, explaining 42% of the variance in SPPB. This is comparable to a study also reporting on mobility 1 year after stroke (45).

54
Notably, in that prospective cohort study mobility was measured by the Riv-ermead Mobility Index (RMI), which is a different scale compared to the SPPB. The RMI covers different activities from turning over in bed to run-ning. That regression model explained 48% of the variance in RMI, which was predicted by functional status, sitting balance, time between stroke onset and baseline measurements and age (45). However, different regression models are difficult to compare due to differences in measures used and methodological shortcomings.
The high proportion of fallers described in paper I, approximately 50%, might be an indication of bodily decline and might therefore explain some of the inactivity found in this cohort, further contributing to progress in the reduction of muscle mass and strength and a decline in mobility. This hy-pothesis might be true because the fall-related self-efficacy also explained part of the variance in both mobility and physical activity. Self-efficacy while performing daily tasks have previously been found to be closely re-lated to motor function, balance, ambulation and activities in daily living, especially in elderly individuals after stroke (108). Individuals with low self-perceived fall-related self-efficacy showed less improvement, indicating that to minimise dependence in daily life it may be important to consider en-hancement in fall-related self-efficacy when planning rehabilitation interven-tions for individuals after stroke. In our study cohort, the median score of BBS in paper I was 53 points. In healthy older individuals living at home (70 to 79 years), the average score on the BBS varies between 52-55 points for women and 52-56 points for men, respectively (112). The BBS, with a well described cut-off of 45 points, is relatively good in predicting which indi-viduals are not likely to fall (112). By applying this cut-off of 45 points, we showed that among the participants in paper I, 88% scored > 45 points on the BBS (112). Despite this, up to 30% of the individuals with scores > 45 points perceived a FoF. This might be one possible reason for sedentary behaviour, i.e., non-exercise seated or lying behaviour, and low levels of physical activity.
Additionally, HRQoL was significantly associated with both mobility and level of physical activity. This result complements previous results from a review showing that disability and post-stroke depression are consistent de-terminants of HRQoL (144). Among individuals in paper I, more than one-third revealed possible depression, which, except for HRQoL, also affects functional recovery, cognitive function and health-care use. Additionally, mostly women declined participation in study I, which was not surprising, because women usually reveal lower values on the EQ5D and therefore might be less motivated to participate in research (143). This might have affected mobility as well in this study. With more women participating, the mobility could have been even worse, because women are also likely to show a greater reduction in mobility while aging (145). It can be speculated that this might have been the main cause for the minor difference in HRQoL

55
reported in this study when compared to a population survey in Stockholm (143).
Earlier studies on mobility 1 to 3 years after stroke revealed the presence of several ongoing disabilities, many of which were confirmed by this study (45-47). Further, the multivariate model with SPPB as the dependent vari-able revealed an association with age, which is in line with previous findings (117). The risk for low mobility increased exponentially from reported low physical activity to medium physical activity compared to those with the highest reported level of physical activity as seen in figure 2 (paper II). In paper I, half of the participating individuals exhibited low mobility with a median SPPB score of 10 (IQR: 4). Because low mobility, i.e., the SPPB, is predictive of disability and hospitalisation, it seems reasonable to highlight those elderly individuals with stroke and mobility < 10 points on the SPPB who should be a cause for concern and therefore addressed in clinical prac-tice (146, 147).
Moreover, we were able to show that being at risk for under-nutrition (MNA-SF < 12 points) was associated with an increased risk for low mobil-ity (OR 5.80, CI 1.26-21.1). Previous studies have reported that individuals with a high percentage of body fat and a high BMI (> 30 kg/m2) also had a higher likelihood of functional limitations and diminished mobility capacity in old age (27, 148). Low muscle strength and obesity combined increases the risk for mobility limitations and a decline in walking speed (149). In contrast, results considering the association between mobility disability and FFM or sarcopenic obesity in older individuals are contradictory (27, 149, 150). Except for a significant association between chair-stand (one individ-ual item from the SPPB) and FMI, we were not able to detect any association between any of the body composition measurements and physical function in paper II. Studies investigating sarcopenic obesity in individuals after stroke are not found, but are needed.
Among the independent factors, 31% of the variance in physical activity was explained by the SPPB, EQ-5D and fall-related self-efficacy as meas-ured by FES(S), indicating an association between mobility and level of physical activity in both regression models. Low physical activity is a gen-eral health problem, especially in individuals at-risk for stroke and following a stroke (34, 36, 151). Further, individuals living in the community post-stroke are less physically active, despite good motor function, compared to individuals without stroke of the same age (35). A longitudinal study inves-tigating sedentary behaviour in the first year after stroke reported that despite functional ability, individuals were highly sedentary and remained so over the first year after stroke (152). Developing interventions to reduce sedentary behaviour are, therefore, warranted.
A slow walking speed, one item in the SPPB, could be a prerequisite for the low level of physical activity found in paper I and II. Swedish data (RS) show that on a national level at 1 year, most individuals < 75 years can move

56
both within and outside independently (5). In contrast, women in specific that were > 75 years need more help when moving around. The mean walk-ing speed in the individuals in paper I was found to be 1.10 (0.86) m/s with a significantly lower gait speed for women, which is in line with previous findings (53). Walking speed is associated with survival and well-being and reflects health and functional status among older individuals; individuals with a walking speed < 1.0 m/s should be a cause for concern (53). An in-crease of the walking speed of 0.1 m/s has shown to increase the chance of 10 year survival, especially among those > 75 years. A slow gait speed might also reflect reduced muscle mass, primarily in the lower extremities, which is likely to occur while aging (62). Furthermore, walking affects organ sys-tems such as the heart, lungs, circulatory and central nervous systems. A slow walking speed may be a result of damaged systems and a high energy cost of walking (53).
Many more factors are known to influence level of physical activity, e.g., depression, fatigue, available facilities for older individuals and the built environment including transit possibilities (153-155). Altogether, a primary goal should be to support physical activity soon after a stroke. Walking speed being part of the SPPB and age and sex can be valuable tools to be used by the clinician as good indicators of health and survival.
Physical activity was associated with HRQoL as measured by EQ-5D. In our study group, we found a slightly higher deterioration in EQ-5D when compared to individuals in a population-based survey from Stockholm county, Sweden (143). The reduction of HRQoL in individuals with stroke and myocardial infarction is greater when compared to other patient catego-ries and might have contributed as well to the low level of physical activity (37). Individuals with a history of either stroke or myocardial infarction or both report significantly higher proportions of problems compared to indi-viduals without these diseases. In general, higher risk factor levels decrease the HRQoL. Thus, as reported in paper II, risk factors such as diabetes, hy-perlipidaemia, hypertension and smoking are likely to have negative influ-ences on HRQoL (37). Another reason for the difference in HRQoL might be that non-participants in cohort studies are more likely to have social prob-lems as well as higher morbidity compared to participants, which might ex-plain the HRQoL in the present study (156). In paper I, approximately 38% revealed possible depression on the GDS-20 indicating mental problems, which are known to have the greatest impact for individuals’ overall HRQoL (index) (37, 85).

57
Body composition, nutritional status and cardiometabolic risk-markers Unpublished data presented in paper II reveals that 14% were at risk for malnutrition and that more than 20% had a BMI > 30 kg/m2, indicating obe-sity. Further, we found that 87% of the individuals had a FM% above the reference value used, i.e., > 20% in men and > 30% in women, respectively (118). This, together with a high frequency of overweight, might be the re-sult of a sedentary life style as reported in paper I and other studies and is most likely in concordance with a high energy intake (35, 151). The reported prevalence of protein and energy malnutrition in stroke survival varies from 6 to 62% due to different assessment tools, the timing of the assessment and differences in patient characteristics (157). We are the first to assess and define sarcopenic obesity in individuals with chronic stroke; in paper II, we reported a prevalence of 8% in a relatively high functioning population. In a cross-sectional study with 3136 Spanish individuals older than 65 years, the prevalence of sarcopenic obesity ranged from approximately 14 -18%, de-fined by using muscle mass and FM cut-off (68). Using a different definition based on BMI and hand-grip strength, epidemiological studies give a preva-lence of 4-9% in older individuals (mean age: 75 years) (158). Changes in body composition could be highly variable in individuals after stroke and could be influenced by several factors such as physical activity, nutritional status, hormonal and inflammatory factors (42). Individuals post-stroke with persistent walking ability have reported an increase of FM only in the paretic leg (66). It might be speculated that individuals with more disabilities and a more pronounced motor impairment display a higher prevalence of sarco-penic obesity as well as sarcopenia after stroke.
In paper I-II, motor function was high; 59-67% reported the highest pos-sible score on the M-MAS UAS-99, and all were community-living indi-viduals. Moreover, based on the definition of sarcopenia in this study, we found that 3% had low muscle mass in paper II. In an older population, the prevalence of sarcopenia was 1-29% based on the definitions being used (62). The prevalence of low muscle mass in paper II could be a consequence of the many individuals in our study cohort that had high BMI and high FFM together with mobility limitation, because high BMI may induce under-estimation of sarcopenia. Recent data including obese subjects reports that higher amounts of muscle mass are linked with less metabolic alterations such as lower inflammatory profiles and better insulin sensitivity (159).
Further, we report IGF-1 and inflammatory values (CRP) within given reference values despite a low level of physical activity and 14% being at risk for malnutrition. Some studies have reported that high serum IGF-1 after stroke is positively correlated to hemiparesis and functional recovery (79). One recent study failed to confirm this relation but found that the IGF-1 level during the acute stroke phase was influenced by the stroke lesion size

58
and that the IGF-1 levels found in stroke individuals were low and might be explained by a low level of physical activity and malnutrition (80).
In addition, further analysis of cardiometabolic risk-markers in paper II revealed that 10% had unfavourable cholesterol levels with plasma choles-terol ≥ 6 mmol/L together with LDL values ≥ 3.5 mmol/L; these cholesterol levels might be linked to nutritional intake. Approximately two-thirds were prescribed statins, targeting the LDL cholesterol level, but we were unable to report any further association between prescribed statins and unfavourable high cholesterol levels. One recently published study with observations from the RS-register reported that more patients were on statins at discharge from the hospital in 2010, approximately 61%, compared to earlier years (160). This can be compared to the 70% in paper II that were on statin treatment. The reason for unfavourable cholesterol levels might be low compliance to the prescribed medication. Furthermore, in paper II we showed that women had significantly higher total cholesterol and HDL cholesterol levels in com-parison to the males. Both the women and the men had relatively high HDL cholesterol levels despite the reported low level of physical activity.
In our stroke cohort, many individuals were overweight or obese. It can be concluded that individuals after stroke reveal a special need for intensi-fied focus on increasing the level of physical activity, nutrition care man-agement and rehabilitation. Because individuals after stroke can be either underweight or overweight-obese, an individually tailored long-term treat-ment plan might be effective, preferably performed in the early rehabilitation phase (24 hours until 3 months) after stroke (24, 73, 157).
Effects of a 3-month progressive resistance and balance exercise program In paper III, we found significantly improved balance (BBS, 2.5 vs. 0 points) at 3 months after participating in the PRB exercise program relative to the exercise group. There are several potential explanations to the improved balance ability reported in paper III that may be interrelated. By exposing themselves to challenging balance exercises, with some supervision during the organised training, the individual´s self-perceived FoF might have de-creased. Thus, some individuals might have exposed themselves to more demanding activities in daily life due to the gradually improved balance. Our result is in contrast to a previous randomised controlled trial reporting on post-stroke individuals after participation in the high intensity functional exercise (HIFE) program (161). In that study, improved performance of eve-ryday life activities and improved falls efficacy were reported but improved balance was not reported. However, older people living in residential care who participated in the HIFE program revealed positive long-term effects on

59
balance, gait and lower-limb strength (162). The interpretation of the result in paper III-IV is that older individuals with balance disturbances due to stroke need a safe and supervised training situation to improve their balance.
The differences in the 6-MWT and 10mWT (paper III) were 30 m and 0.09 m/s, respectively, after the intervention. Considering the calculated effect size (ES: 0,64-0.68) and the minimum clinically important differences for the 6-MWT and walking speed which have been estimated as 20–25 m and 0.05 m/s, respectively, this finding might be considered a small to mod-erate effect (55, 163). One reason for impaired walking performance can be called critical power, meaning that one chose the speed to endure almost indefinitely below the ventilatory threshold (164). The 6-MWT reflects the ability and capacity to perform daily activities and is a test of sub-maximal aerobic capacity, approximately corresponding to the first ventilatory thresh-old. Subjects walking at a self-selected speed do not exceed critical power (164).
The characteristics of the present study population described in paper III and IV are, in many cases, similar to the factors that might reduce the 6-MWT (115). In our study cohort, we found a body composition consisting of increased FM and also, to a minor degree, reduced FFM in conjunction with high BMI, which are factors known to negatively affect the distance walked in 6 minutes (115). Further, participating stroke individuals were elderly and many showed comorbidity in addition to their stroke: diabetes type II, previ-ous myocardial infarction or, in some cases, reduced pulmonary function. All these factors are likely to reduce the distance walked in 6 minutes and, as such, affect the results of an intervention study. It can be speculated that improved balance in favour of the exercise group could be the main reason for achieving a longer distance walked in 6 minutes. In contrast, 76% of the individuals were men in the PRB exercise group (paper III) and had an over-all preserved cognitive function, which is also indicative of a longer walking distance. All individuals were exercising in their own highest possible inten-sity, despite weight loading and number of repetitions, which is comparable to low and moderate intensity with more than 10 repetitions per exercise. This might have improved their aerobic capacity as well, reflecting the in-creased walking distance in this group of individuals with low physical ac-tivity.
A total of 43 individuals, 12 women and 31 men, were able to perform the BIA before and after the intervention period and were included in paper IV. To our knowledge, we are the first to report on changes in body composition after exercising in individuals 1 year after stroke. In our study we found a slight non-significant improvement in FFMI and a reduction in FM% in fa-vour of the PRB exercise group, with an overall reduced BMI. Weight loss and a reduction of BMI are in parallel with a decrease in both muscle and fat mass. Our results indicate that we have managed to counteract the loss of muscle mass related to weight loss, because the FFMI was increased after 3

60
months of progressive resistance and balance group-training. Moreover, the FM% significantly decreased after exercising in comparison with the control group, which is favourable because a high amount of fat may be associated with muscle weakness and reduced insulin sensitivity (148). Age-related body composition changes affected muscle quality (strength/muscle mass), together with obesity, in older inactive individuals after stroke, can conse-quently lead to the state known as sarcopenic obesity, which was also af-fected from the PRB exercise program with a slight reduction (27, 68).
Moreover, we showed a significant reduction in IGF-1 at 3 months after the PRB exercise program in relation to the control group. This is somewhat surprising because resistance training usually stimulates IGF-1 production, which is important for muscle anabolism (62). One may speculate that this could reflect a higher insulin sensitivity, because the participating individu-als were obese and older (31).
Ectopic fat deposition can change muscle composition and further decline muscle strength and function, which might be one reason for the negatively affected physical functioning in our study (148). Excessive fat deposition within the visceral area, liver, heart and muscles is clearly associated with negative health consequences but may not be similarly related to physical function. Our previous reported improvement in walking capacity (6-MWT) was not related to an increase in muscle mass in this study population. How-ever, muscle function might be improved regardless of similar changes in mass. Factors, such as myofibrillar proteins, inflammation, nutrition and endocrine status, are important for muscle function, i.e., strength and power (62). At 3 months, our exploratory trial revealed a significant association between improvements in 6-MWT and changes in FMI in the exercise group. This effect might be caused by an altered body composition due to the progressive resistance and balance program and a simultaneous weight reduction, especially among males.
Methodological considerations Individuals included All the individuals included in the thesis were living at home at the time of entering the study and therefore individuals with more severe stroke were not captured. This was also the focus of the present study. However, ap-proximately 85-90% were living at home 3 months after stroke, according to RS 1 year follow-up in 2013 (5). All individuals who were enrolled in the present study had had a mild to moderate stroke. From these perspectives, the population in this thesis might be considered representative of the com-munity-living stroke population in Sweden. The mean age of the individuals in the different papers were close to the age where women and man have

61
their first stroke, which further strengthens the external validity and the gen-eralisability to the whole stroke population. In addition, we excluded indi-viduals with severe aphasia and cognitive impairments, because their prob-lems made it hard to follow the study design and manage the self-report of some measurements.
The recruitment to the exercise study described in paper III-IV progressed slowly, and because significant findings on the primary outcome were noted, the intervention was closed before a sufficient sample was obtained. The risk for type II errors was thereby increased. Based on a pilot-study prior to study start, it was estimated that 128 individuals would be enough to detect differ-ences between the PRB exercise program and the control group. However, the study was finalised with 67 individuals included at baseline. The attrition rate was 24% after 3 months and increased to 29% at 15 months follow-up in the PRB exercise group. This might introduce bias. Still, the intention-to-treat analysis was compared to the complete case analyses and revealed about the same results (paper III). Cut-offs for common acceptable attrition-rates in exercise studies are lacking (165).
It was evident that environmental factors, such as the lack of transport possibilities, sometimes influenced the participation in the PRB exercise group. This could be one reason not to participate in exercising, especially for those living outside the centre of Uppsala. Therefore, it seems important and reasonable for healthcare services to pay attention to those individuals and provide them with advice regarding how to be more physically active and which activities and facilities they can participate in. Prescribed physical activity might be helpful to introduce older individuals suffering from stroke to different exercise modalities and possible activities to perform, to increase their daily activity.
Data collection The process of identifying eligible individuals for inclusion may be biased because some individuals could not be reached as a result of different rea-sons. In addition, some factors might have affected external validity and a generalisation to all individuals with stroke. An uneven distribution between genders (male, 71%) was present throughout the papers. Furthermore, those who did not want to fully participate (n=81) answered questions from EQ-5D and reported a lower HRQoL compared to those who were enrolled in the study. This can be compared to a Swedish study reporting a significantly lower health-index for women, especially in the high age-groups and, as such, mirroring the low EQ-5D seen in non-participants (143). In total, ap-proximately 21% of the men declined participation and 44% of the women declined. The study group was, however, not comparable in EQ-5D with a Swedish age-matched normal population, revealing a mean of 0.73 for all individuals compared to 0.80 for the individuals in Stockholm county (143).

62
Many of the participating individuals had possible depression, which is in line with other studies and reports (5, 38).
In paper I, all data were collected using standardised measurements with acceptable psychometric properties and were collected at one time-point. That strengthens the internal validity. Measurements were made by one sin-gle person. The self-reported questionnaires were filled out before the indi-vidual came to the hospital for examination, but was then re-checked to minimise missing values. Despite this procedure, there were some data miss-ing, but not > 3% for any scale. Imputation by mean or median values in paper I-II when data were missing could slightly have affected the mean of the whole study population. However, the study population was relatively large in relation to the missing values.
A limitation with self-reporting questionnaires when measuring physical activity is the risk for overestimation due to difficulties in obtaining the ex-act frequency, intensity and duration. Despite this, such questionnaires are inexpensive and suitable for larger trials. PASE is a questionnaire measuring physical activity in older individuals and has previously been used in the stroke population (34-36). Using self-reporting in a stroke population can be difficult because the respondents could have undetected mental impairment. However, the PASE scores have shown significant correlation to a portable accelerometer in those over 70 years old (r= 0.64, P < 0.05) (166). This adds support to the validity of the PASE, measuring level of physical activity in older individuals (166). In addition, to prevent missing data, the rechecking of answers was also essential to minimise misunderstandings. Objective measurements, such as using accelerometer data for registration of physical activity, might have added more accurate data, but may also be uncertain due to reduced compliance with using the device.
In paper II and IV, measurements of BIA only included individuals who were able to stand, which excluded individuals with reduced static balance. Individuals being examined outside the hospital were further excluded from the BIA assessment as well. This restricts the possibility to generalising the results from the present study to more severe damaged individuals with stroke. There might be a validity problem as well involved in the BIA as-sessment used in this thesis and therefore there are some concerns about the definition criteria for sarcopenia being used (89). Computed tomography (CT scan) and magnetic resonance imaging (MRI) are the gold standard in research for measuring body composition (89) but dual energy X-ray absorp-tiometry (DXA) and BIA is also used for research purposes. Further, addi-tional examinations included into the study design, i.e., hand grip strength, might have strengthened the results (89). This method is frequently used and the reason for not including grip strength as a measurement was that the SPPB, including chair-stand, could be considered a functional measurement for muscle strength and performance in the lower extremities (51, 110).

63
The study population in paper III originated from the first 195 individuals examined in paper I. This paper includes most of the recommendations for a clinical trial with methodological quality, e.g., randomised allocation, con-trol group, intention-to-treat analysis and concealed allocation. The drop-out rate in paper III was 24% after 3 months and increased further to 29 % after 15 months, which introduced some bias to the results. To minimise this problem, a multiple imputation technique was used, to preserve the alloca-tion to the different groups. The assessor was blinded to the group allocation, but some unmasking might have occurred during follow-up, since the partic-ipants had no restrictions in revealing which group they participated in. This increased the risk of bias.
An independent experienced physiotherapist not involved in the randomi-sation procedure or the PRB exercise group performed all assessments at baseline, 3, 6 and 15 months, increasing the internal validity.
Main conclusions • Individuals 1-3 years after stroke, without major cognitive decline and
severe aphasia, perceived many disabilities that could be modifiable. Low mobility and low physical activity, high possible depression, re-duced walking capacity and a slow walking speed were highly present. Frequent falls and a fear of falling were common among participants as well. Fall-related self-efficacy and mobility may promote the level of physical activity.
• Many individuals were overweight or obese with an unfavourable high fat mass and high cholesterol and LDL levels. Factors associated with risk for low mobility were low and medium physical activity, risk for malnutrition, and age per 10 years.
• A progressive resistance and balance program for 3 months can be effec-tive in the short-term to improve physical function, i.e., balance, walking capacity and gait speed. In the long-term, at follow-up after 6 and 15 months, the increase in walking speed persisted.
• A progressive resistance and balance program slightly altered body compositional changes 1 year after stroke. There was a significant asso-ciation between changes in walking capacity and changes in fat mass in-dex after exercising. Exercising might improve insulin sensitivity as well, according to the decreased IGF-1 level.

64
Clinical implications • If the level of physical activity is low, implying an increased risk
for future cardiovascular incidents and low mobility, treatments for enhanced physical activity and reduced sedentary time should be addressed quickly after stroke onset.
• The majority of the post-stroke individuals were overweight or obese with a body composition characterised by increased fat mass, meaning that treatments for healthy eating should be incor-porated into stroke-rehabilitation.
• A 3 months progressive resistance and balance training program performed as a circuit class with individualised intensity and pro-gression are effective in improving physical function directly after exercising. Therefore, to maintain improved functions in the long-term, additional strategies targeting behaviour changes might be effective.
• Assessments of body composition should be considered after
stroke.

65
Svensk sammanfattning
Stroke är vanligt i högre åldrar och mer än åttio procent av de som insjuknar är över sextiofem år. Många av de riskfaktorer som orsakar stroke och även hjärtinfarkt är beroende av livsstil och går därmed att förändra. Högt blod-tryck, bukfetma, rökning, diabetes, alkohol, fysisk inaktivitet, depression och ohälsosam kosthållning är bland de vanligaste riskfaktorerna för stroke.
Allt fler patienter vårdas vid stroke enheter i akut skedet men avsevärt fär-re personer får fortsatt inneliggande rehabilitering efter den initiala fasen. Istället skrivs fler personer ut direkt till hemmet, med eller utan hem rehabi-litering. Detta kan vara en orsak till att hemhjälpsbehovet också ökat. Detta är särskilt förekommande bland äldre individer. Sekundär preventionen har förbättrats med allt flera personer som erhåller adekvat medicinering. Trots detta upplever ungefär 30% av individerna att de behöver mer rehabilitering 1 år efter stroke, enligt Riksstrokes sammanställning från år 2013. Detta behov har även funnits i tidigare rapporter från Riksstroke.
Det övergripande syftet med denna avhandling var att beskriva fysisk funktion, fysisk aktivitet, kroppssammansättning, nutritions status (inklusive kardiometabola riskmarkörer) samt psykologiska faktorer hos hemmaboende individer 1 år efter stroke. Ytterligare ett syfte var att utvärdera kortsiktiga och långsiktiga effekter av ett 3 månaders progressivt styrke- och balansträ-nings program.
Delarbete I: Det första delarbetet kartlägger nivå på fysisk funktion, fysisk aktivitet samt psykologiska faktorer hos 195 hemmaboende individer, 1 till 3 år efter stro-ke. Vi ville även studera vilka faktorer som kunde förklara mobilitet och fysisk aktivitet. Personer med kognitiv nedsättning eller påtagliga språkliga svårigheter exkluderades. Inkluderade personer fick svara på enkäter med frågor rörande fysisk aktivitet, hälso-relaterad livskvalitet, fall-relaterad self-efficacy och depression. De tillfrågades också om eventuella fall incidenter det senaste året och om de upplevde fallrädsla. Individerna undersöktes vid ett tillfälle vad gällde balansförmåga, mobilitet (en kombination av gånghas-tighet, balans och uppresning från stol), gånghastighet och motorisk funk-tion. Resultatet visade att personerna hade låg mobilitet, vilket bedöms kun-na öka risken för framtida sjukhusinläggning och funktionsnedsättning. Vi-

66
dare hade individerna en låg gånghastighet och en låg fysisk aktivitetsnivå i jämförelse med äldre utan stroke. Trettioåtta procent hade möjlig depression och 46% hade fallit mer än en gång senaste året. Kvinnorna uppvisade en signifikant högre fallrädsla i jämförelse med männen och totalt sett angav 37% att de var rädda att falla.
Resultatet visade att ålder, fysisk aktivitet, fall-relaterad self-efficacy och hälsorelaterad livskvalitet förklarade variationen i mobilitet. Det starkaste sambandet till mobilitet sågs för fysisk aktivitet. Kön, samsjuklighet, kogni-tion, depression, fall och fallrädsla spelade mindre roll. Vidare kunde varia-tionen i fysisk aktivitet förklaras av mobilitet, fall-relaterad self-efficacy och hälsorelaterad livskvalitet. Det starkaste sambandet till fysisk aktivitet sågs för mobilitet. Ålder, kön, samsjuklighet, kognition, depression och fallrädsla spelade mindre roll. Slutsatsen från arbetet var att individerna hade många besvär och funktionsnedsättningar som kunde behandlas samt att fall-relaterad self-efficacy och mobilitet var viktiga faktorer för att främja fysisk aktivitet i denna patientgrupp.
Delarbete II: I vårt andra arbete studerades kroppssammansättning, nutritions status (in-klusive kardiometabola riskmarkörer) och fysisk funktion/fysisk aktivitet hos 134 av de 195 individerna som inkluderades i delarbete I. Exklusionskriteri-erna var detsamma som i delarbete I, men individer med pacemaker och de som inte kunde utföra mätning av kroppsammansättning (bioelektrisk impe-dans analys, BIA, (Tanita®) av andra skäl exkluderades. Alla personer i studien besvarade frågeformulär angående sin fysiska aktivitetsnivå och sitt nutritions status. Mobilitet och självvald gånghastighet undersöktes liksom kroppssammansättning. Varje individs BMI beräknades utifrån vikt och längd. Resultatet visade att > 20% hade ett BMI över 30 kg/m2, vilket klassi-ficeras som fetma. Fjorton procent bedömdes ha risk för under-nutrition och 3% uppvisade sarkopeni (låg muskelmassa i kombination med en gånghas-tighet < 1m/s) medan 8% hade en kombination av låg muskelmassa och hög andel fettmassa, dvs sarkopen obesity. Av de inkluderade personerna hade 10% kolesterol nivåer över 6 mmol/l samtidigt med LDL-kolesterol värden över 3.5 mmol/L, vilket bedömdes innebära en förhöjd kardiovaskulär risk. Kvinnorna hade signifikant högre total kolesterol och HDL-kolesterol i jäm-förelse med männen.
Vi analyserade även sambandet mellan låg mobilitet och faktorer som ål-der, kön, fysisk aktivitet och nutritionsstatus. I denna grupp var de starkaste sambanden, uttryckt som Odds kvoter (95 % konfidensintervall), låg fysisk aktivitet, OR 8.2 (2.8-24.2), risk för under-nutrition, OR 5.8 (1.6-21.1) och hög ålder OR, 2.78 (1.24-6.24). Slutsatsen blev att fetma och sarkopen obe-sity var tämligen vanligt förekommande i denna grupp av individer efter

67
stroke. Interventioner riktade mot förbättrad nutrition och ökad fysisk aktivi-tet behövs hos individer efter stroke.
Delarbete III I det tredje delarbetet har effekterna av ett progressivt styrke- och balans (PRB) träningsprogram på fysisk funktion, fysisk aktivitet och psykologiska faktorer undersökts. Uppföljningar ägde rum efter 3, 6 och 15 månader. Stu-dien har genomförts som en randomiserad kontrollerad studie med totalt 67 försökspersoner (76 % män, medelålder 73 år). Primära utfallsmått var ba-lans (Berg Balans Skala, 0-56 poäng) och mobilitet (Short Physical Perfor-mance Battery, 0-12 poäng) vid 3 månader. Sekundära utfallsmått var gång-kapacitet, 10 meters gång hastighet, fysisk aktivitetsnivå, hälsorelaterad livs-kvalitet, depression och fall-relaterad self-efficacy. Trettiofyra försöksperso-ner randomiserades till en träningsgrupp, som utförde ett funktionellt träningsprogram 2 gånger per vecka under 3 månader, med fokus på ökad benstyrka och balans i stående och gående. Alla personer bar ett viktbälte under träningen där vikterna gradvis justerades, utifrån varje individs förut-sättning. Individerna fick också en individuellt anpassad hemövning att utfö-ra mellan träningstillfällena. Kontrollgruppen bestod av 33 försökspersoner som inte erhöll några specifika behandlingsåtgärder. Efter 3 månader uppvi-sade individerna i träningsgruppen en signifikant förbättring av balans (Berg balans test), gångkapacitet (6-minuters gångtest) samt den självvalda gång-hastigheten (10-meters gångtest) jämfört med kontroll gruppen. Effekten på gånghastigheten kvarstod vid 6 och 15 månaders uppföljning.
Slutsatsen av detta delarbete var att ett progressivt styrke- och balansträ-nings program förbättrade balans, gång kapacitet och gånghastighet kortsik-tigt i en kronisk fas efter stroke. Sammanfattningsvis, behövs ytterligare åtgärder för att förbättringarna skall kvarstå över tid.
Delarbete IV I det här delarbetet låg fokus på effekter av tre månaders gruppträning med avseende på förändring av kroppssammansättning (muskelmassa och fett-massa) och nutritionsstatus i relation till förändringar i fysisk funktion. Stu-dien är genomförd som en explorativ/utforskande randomiserad kontrollerad studie. Vi analyserade 43 (73% män, medelålder 73 år) av de 67 försöksper-sonerna som deltog i den randomiserade kontrollerade studien som beskrivs i delarbete III. Primärt ville vi nu studera effekten av ett progressivt styrke- och balansträningsprogram på kroppssammansättning, kardiometabola risk-markörer och nutritionsindikatorer. Fettfri massa (främst muskelmassa) och fettmassa bestämdes med bioelektrisk impedans-analys (Tanita®). Fysisk

68
funktion bestämdes som gångkapacitet, balans och mobilitet. Tjugo individer deltog aktivt i PRB-träningsprogrammet, medan kontrollgruppen bestod av 23 individer som inte erhöll några särskilda behandlingsåtgärder. Mätningar utfördes före och direkt efter interventionen.
Vi kunde visa att fettmassan (procent) minskade signifikant efter tre må-naders PRB träning jämfört med kontrollgruppen. Den fettfria massan, dvs. bl.a. muskelmassa, ökade något i träningsgruppen, men förändringen var inte statistiskt signifikant. BMI hade totalt sett minskat något i båda grupperna. Serum insulin-like growth factor-I (IGF-1) var signifikant lägre efter tre månaders träning i jämförelse med kontrollgruppen. Detta kan möjligen vara ett tecken på ökad insulinkänslighet. Varken blodtryck eller kardiovaskulära riskpoäng hade förändrats vid tre-månadersmätningen. Vidare såg vi att minskningen av fettmasseindex (kg/m2) uppvisade ett signifikant samband med ökning i gångkapacitet, mätt med 6-minuters gångtest efter tre månader. Det fanns inga statistiska samband mellan förändringar i muskelmassa och förändringar i fysisk funktion efter tre månaders träning.
Sammanfattningsvis sågs en minskning av fettmassan vilket kan vara för-delaktigt ur kardiovaskulär risk synpunkt. Minskningen i fettmassa var också förenat med bättre gångkapacitet. Muskelmassan ökade något eller kvarstod oförändrad trots en generell minskning av BMI. Serum IGF-1 minskade något i träningsgruppen vilket möjligen kan vara ett uttryck för ökad insulin känslighet. Effekt av progressiv styrketräning på kroppssammansättning och nutritionsfaktorer är viktigt att studera vidare.

69
Acknowledgements
The data collection within this thesis was carried out at the Geriatric Clinic at Uppsala University Hospital in Sweden and the work was carried out at the Department for Neuroscience, Physiotherapy at Uppsala University. I wish to express my gratitude to all those individuals who have helped me and supported me throughout the thesis process:
Karin Hellström, my supervisor, for your excellent supervision, flexibility, and encouragement through the years. I am grateful for the opportunity to our working collaboration and that you have been easy to reach throughout the whole process of writing this thesis. You are the one that made me inter-ested in the scientific world.
Tommy Cederholm, my co-supervisor, for your excellent supervision and for your ability to create a friendly atmosphere. You have always spared some room in your busy schedule for me. Thank you also for the stimulating scientific discussions we have had, it has been a great pleasure to share your knowledge and competence.
Lena Zetterberg, my co-supervisor, for your support in being structured when writing manuscripts. I appreciate your interest in details and I want to thank you for your help and the discussions we have had.
Birgitta Lindmark, my co-author, for your valuable scientific knowledge in the stroke research area. I also want to thank you for the opportunity to write this thesis, I have enjoyed most of the moments.
Susanna Tuvemo Johnson, my present PhD colleague and my former de-partment head at the Geriatric Clinic, for your support in development work and other more personal issues. Without you and your interest and engage-ment in research projects this process could not have been possible. Thanks also for aiding in the data collection and for inspiring and stimulating discus-sions through the years.
Agneta Nitka, Elisabet Degerman, Susann Friman Vestlund, Evalotta Lind-berg and other participating physiotherapists for your excellent competence

70
in stroke rehabilitation and for your involvement in the progressive resis-tance exercise program.
Mona-Lisa Wernroth, Uppsala Clinical Research (UCR) center, for valuable statistical advice and supervision.
Andreas Fugmann and Örjan Nordmark for sharing your medical knowledge in geriatric rehabilitation and acute stroke care. I have highly appreciated your help with answering my questions.
Siv Tengblad and Marianne Belin for the collection and management of blood samples.
The present PhD-students at the Institution for Neuroscience, Physiotherapy at Uppsala University: Ann Essner, Carina Hagman, Christina Emilson, He-nrik Johansson, Regina Bendrik, Sören Spörndly Nees, Ylva Åkerblom and Åsa Revenäs. We have shared some common experiences throughout these years. I also want to thank you for the discussions and for the fun we have shared. You will sooner than you know reach the end of the thesis process.
The former PhD-students at the Institution for Neuroscience, Physiotherapy at Uppsala University: Annika Bring, Charlotte Urell, Helena Igelström, Mikael Andersson and Sara Holm. Thank you for all the fun we have had together and for inspiring discussions over the years we shared.
My physiotherapy colleagues at the Geriatric Clinic at Uppsala University Hospital for your interest in my progress in the research area. Your effort to improve geriatric rehabilitation is admirable.
My physiotherapy and research colleagues at the Uppsala University for our coffee table discussions and for your interest in my progress in the research area. Your effort to improve your pedagogic skills and the learning process is admirable.
The research colleagues and the present PhD-students (including Viola Adamsson) at the Department of Public Health and Caring Science, Clinical Nutrition and Metabolism: Thank you for being able to join some of your meeting and for taking part of your excellent research. Thank you for the all the fun moments I have been able to share with you.
All participating individuals with stroke: without you this work would not have been possible.

71
Thanks to my friends from my early years in Boden and Luleå; Elisabeth Lindberg, Lisa Löfgren, Marianne Mattsson, Maria Pettersson and not at least Maria Wrangel for being supportive and encouraging in the process of the thesis production.
My relatives and other friends.....

72
REFERENCES
1. WHO - International Classification of Functioning, Disability and Health: ICF. Geneva. WHO.World Health Organisation; 2008. 2. RIKSstroke. RIKSstroke, the Swedish Stroke Register.[cited November 2014]; availble from: http://www.riksstroke.org. 3. Socialstyrelsen. The National Board of Health and Welfare. Stroke care. Supplementary material to the National Guidelines 2009 (swedish). [cited November 2014]; Available from http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/17790/Stroke-Vetenskapligt-underlag 2009. 4. Hatano S. Experience from a multicentre stroke register: a preliminary report. Bull World Health Organ. 1976;54(5):541-53. 5. RIKSstroke. Riks-Stroke the Swedish stroke register ett år efter stroke: rapport från Riksstroke, 1-årsuppföljning 2013. Umeå: 2013. 6. Appelros P, Stegmayr B, Terént A. Sex differences in stroke epidemiology: a systematic review. Stroke. 2009;40(4):1082-90. 7. Appelros P, Stegmayr B, Terént A. A review on sex differences in stroke treatment and outcome. Acta Neurol Scand. 2010;121(6):359-69. 8. Kunst AE, Amiri M, Janssen F. The decline in stroke mortality: exploration of future trends in 7 Western European countries. Stroke. 2011;42(8):2126-30. 9. Mackay-Lyons M, Thornton M, Ruggles T, Che M. Non-pharmacological interventions for preventing secondary vascular events after stroke or transient ischemic attack. Cochrane Database Syst Rev. 2013;3:CD008656. 10. Wolf PA. Contributions of the Framingham Heart Study to Stroke and Dementia Epidemiologic Research at 60 Years. Arch Neurol. 2012;69(5):567-71. 11. O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112-23. 12. Fagard RH, Cornelissen VA. Effect of exercise on blood pressure control in hypertensive patients. Eur J Cardiovasc Prev Rehabil. 2007;14(1):12-7. 13. Furie KL, Kasner SE, Adams RJ, Albers GW, Bush RL, Fagan SC, et al. Guidelines for the prevention of stroke in patients with

73
stroke or transient ischemic attack: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2011;42(1):227-76. 14. Abd TT, Jacobson TA. Statin-induced myopathy: a review and update. Expert Opin Drug Saf. 2011;10(3):373-87. 15. Olsson T, Viitanen M, Asplund K, Eriksson S, Hägg E. Prognosis after stroke in diabetic patients. A controlled prospective study. Diabetologia. 1990;33(4):244-9. 16. Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, Steiner E. High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. Lancet. 2001;358(9298):2026-33. 17. Walldius G, Jungner I. Is there a better marker of cardiovascular risk than LDL cholesterol? Apolipoproteins B and A-I--new risk factors and targets for therapy. Nutr Metab Cardiovasc Dis. 2007;17(8):565-71. 18. Walldius G, Jungner I. The apoB/apoA-I ratio: a strong, new risk factor for cardiovascular disease and a target for lipid-lowering therapy--a review of the evidence. J Intern Med. 2006;259(5):493-519. 19. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126-31. 20. Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ, et al. Breaks in sedentary time: beneficial associations with metabolic risk. Diabetes Care. 2008;31(4):661-6. 21. Boysen G, Krarup LH. Benefits of physical activity for stroke survivors. Expert Rev Neurother. 2009;9(2):147-9. 22. Kallings LV, Sierra Johnson J, Fisher RM, Faire U, Ståhle A, Hemmingsson E, et al. Beneficial effects of individualized physical activity on prescription on body composition and cardiometabolic risk factors: results from a randomized controlled trial. Eur J Cardiovasc Prev Rehabil. 2009;16(1):80-4. 23. Hankey GJ. Nutrition and the risk of stroke. Lancet Neurol. 2012;11(1):66-81. 24. Gariballa SE. Nutritional factors in stroke. Br J Nutr. 2000;84(1):5-17. 25. Andersen KK, Olsen TS. The obesity paradox in stroke: Lower mortality and lower risk of readmission for recurrent stroke in obese stroke patients. Int J Stroke. 2013.[Epub ahead of print]. 26. Doehner W, Schenkel J, Anker SD, Springer J, Audebert HJ. Overweight and obesity are associated with improved survival, functional outcome, and stroke recurrence after acute stroke or transient ischaemic attack: observations from the TEMPiS trial. Eur Heart J. 2013;34(4):268-77. 27. Zamboni M, Mazzali G, Fantin F, Rossi A, Di Francesco V. Sarcopenic obesity: a new category of obesity in the elderly. Nutr Metab Cardiovasc Dis. 2008;18(5):388-95.

74
28. Johansson-Persson A, Ulmius M, Cloetens L, Karhu T, Herzig KH, Onning G. A high intake of dietary fiber influences C-reactive protein and fibrinogen, but not glucose and lipid metabolism, in mildly hypercholesterolemic subjects. Eur J Nutr. 2014;53(1):39-48. 29. Idicula TT, Waje-Andreassen U, Brogger J, Naess H, Thomassen L. Serum albumin in ischemic stroke patients: the higher the better. The Bergen Stroke Study. Cerebrovasc Dis. 2009;28(1):13-7. 30. Scarth JP. Modulation of the growth hormone-insulin-like growth factor (GH-IGF) axis by pharmaceutical, nutraceutical and environmental xenobiotics: an emerging role for xenobiotic-metabolizing enzymes and the transcription factors regulating their expression. A review. Xenobiotica. 2006;36(2-3):119-218. 31. Friedrich N, Thuesen B, Jørgensen T, Juul A, Spielhagen C, Wallaschofksi H, et al. The association between IGF-I and insulin resistance: a general population study in Danish adults. Diabetes Care. 2012;35(4):768-73. 32. Hankey GJ, Spiesser J, Hakimi Z, Bego G, Carita P, Gabriel S. Rate, degree, and predictors of recovery from disability following ischemic stroke. Neurology. 2007;68(19):1583-7. 33. Craig LE, Wu O, Bernhardt J, Langhorne P. Predictors of poststroke mobility: systematic review. Int J Stroke. 2011;6(4):321-7. 34. Danielsson A, Willén C, Sunnerhagen KS. Physical activity, ambulation, and motor impairment late after stroke. Stroke Res Treat. 2012;2012:818513. 35. Danielsson A, Meirelles C, Willen C, Sunnerhagen KS. Physical Activity in Community-Dwelling Stroke Survivors and a Healthy Population Is Not Explained by Motor Function Only. PM R. 2014;6(2):139-45. 36. Krarup LH, Truelsen T, Gluud C, Andersen G, Zeng X, Kõrv J, et al. Prestroke physical activity is associated with severity and long-term outcome from first-ever stroke. Neurology. 2008;71(17):1313-8. 37. Bach JP, Riedel O, Pieper L, Klotsche J, Dodel R, Wittchen HU. Health-related quality of life in patients with a history of myocardial infarction and stroke. Cerebrovasc Dis. 2011;31(1):68-76. 38. Appelros P, Viitanen M. Prevalence and predictors of depression at one year in a Swedish population-based cohort with first-ever stroke. J Stroke Cerebrovasc Dis. 2004;13(2):52-7. 39. Hellström K, Lindmark B, Wahlberg B, Fugl-Meyer AR. Self-efficacy in relation to impairments and activities of daily living disability in elderly patients with stroke: a prospective investigation. J Rehabil Med. 2003;35(5):202-7. 40. Andersson AG, Kamwendo K, Appelros P. Fear of falling in stroke patients: relationship with previous falls and functional characteristics. Int J Rehabil Res. 2008;31(3):261-4. 41. English C, McLennan H, Thoirs K, Coates A, Bernhardt J. Loss of skeletal muscle mass after stroke: a systematic review. Int J Stroke. 2010;5(5):395-402.

75
42. English C, Thoirs K, Coates A, Ryan A, Bernhardt J. Changes in fat mass in stroke survivors: a systematic review. Int J Stroke. 2012;7(6):491-8. 43. Group LS. 2001–2011: a decade of the LADIS (Leukoaraiosis And DISability) Study: what have we learned about white matter changes and small-vessel disease? Cerebrovasc Dis. 2011;32(6):577-88. 44. Bussmann JB, Stam HJ. Techniques for measurement and assessment of mobility in rehabilitation: a theoretical approach. Clin Rehabil. 1998;12(6):455-64. 45. van de Port IG, Kwakkel G, Schepers VP, Lindeman E. Predicting mobility outcome one year after stroke: a prospective cohort study. J Rehabil Med. 2006;38(4):218-23. 46. van de Port IG, Kwakkel G, van Wijk I, Lindeman E. Susceptibility to deterioration of mobility long-term after stroke: a prospective cohort study. Stroke. 2006;37(1):167-71. 47. van Wijk I, Algra A, van de Port IG, Bevaart B, Lindeman E. Change in mobility activity in the second year after stroke in a rehabilitation population: who is at risk for decline? Arch Phys Med Rehabil. 2006;87(1):45-50. 48. Studenski S, Perera S, Wallace D, Chandler JM, Duncan PW, Rooney E, et al. Physical performance measures in the clinical setting. J Am Geriatr Soc. 2003;51(3):314-22. 49. Stookey AD, Katzel LI, Steinbrenner G, Shaughnessy M, Ivey FM. The short physical performance battery as a predictor of functional capacity after stroke. J Stroke Cerebrovasc Dis. 2014;23(1):130-5. 50. Cesari M, Kritchevsky SB, Penninx BW, Nicklas BJ, Simonsick EM, Newman AB, et al. Prognostic value of usual gait speed in well-functioning older people--results from the Health, Aging and Body Composition Study. J Am Geriatr Soc. 2005;53(10):1675-80. 51. Fielding RA, Vellas B, Evans WJ, Bhasin S, Morley JE, Newman AB, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopenia. J Am Med Dir Assoc. 2011;12(4):249-56. 52. Langlois JA, Keyl PM, Guralnik JM, Foley DJ, Marottoli RA, Wallace RB. Characteristics of older pedestrians who have difficulty crossing the street. Am J Public Health. 1997;87(3):393-7. 53. Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, et al. Gait speed and survival in older adults. JAMA. 2011;305(1):50-8. 54. Perera S, Mody S, Woodman R, Studenski S. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743-9. 55. Gremeaux V, Troisgros O, Benaïm S, Hannequin A, Laurent Y, Casillas JM, et al. Determining the minimal clinically important difference for the six-minute walk test and the 200-meter fast-walk test during cardiac rehabilitation program in coronary artery disease patients after acute coronary syndrome. Arch Phys Med Rehabil. 2011;92(4):611-9.

76
56. Schmid AA, Van Puymbroeck M, Altenburger PA, Dierks TA, Miller KK, Damush TM, et al. Balance and balance self-efficacy are associated with activity and participation after stroke: a cross-sectional study in people with chronic stroke. Arch Phys Med Rehabil. 2012;93(6):1101-7. 57. Pouwels S, Lalmohamed A, Leufkens B, de Boer A, Cooper C, van Staa T, et al. Risk of hip/femur fracture after stroke: a population-based case-control study. Stroke. 2009;40(10):3281-5. 58. Cederholm TE, Bauer JM, Boirie Y, Schneider SM, Sieber CC, Rolland Y. Toward a definition of sarcopenia. Clin Geriatr Med. 2011;27(3):341-53. 59. Brazzelli M, Saunders DH, Greig CA, Mead GE. Physical fitness training for stroke patients. Cochrane Database Syst Rev. 2011;9(11):CD003316. 60. Flansbjer UB, Lexell J, Brogårdh C. Long-term benefits of progressive resistance training in chronic stroke: a 4-year follow-up. J Rehabil Med. 2012;44(3):218-21. 61. Hughes VA, Frontera WR, Roubenoff R, Evans WJ, Singh MA. Longitudinal changes in body composition in older men and women: role of body weight change and physical activity. Am J Clin Nutr. 2002;76(2):473-81. 62. Cruz-Jentoft AJ, Landi F, Schneider SM, Zúñiga C, Arai H, Boirie Y, et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. 2014;43(6):748-59. 63. Bean JF, Olveczky DD, Kiely DK, LaRose SI, Jette AM. Performance-based versus patient-reported physical function: what are the underlying predictors? Phys Ther. 2011;91(12):1804-11. 64. Scherbakov N, von Haehling S, Anker SD, Dirnagl U, Doehner W. Stroke induced Sarcopenia: muscle wasting and disability after stroke. Int J Cardiol. 2013;170(2):89-94. 65. Ivey FM, Ryan AS, Hafer-Macko CE, Garrity BM, Sorkin JD, Goldberg AP, et al. High prevalence of abnormal glucose metabolism and poor sensitivity of fasting plasma glucose in the chronic phase of stroke. Cerebrovasc Dis. 2006;22(5-6):368-71. 66. Jørgensen L, Jacobsen BK. Changes in muscle mass, fat mass, and bone mineral content in the legs after stroke: a 1 year prospective study. Bone. 2001;28(6):655-9. 67. Schutz Y, Kyle UU, Pichard C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18-98 y. Int J Obes Relat Metab Disord. 2002;26(7):953-60. 68. Gomez-Cabello A, Pedrero-Chamizo R, Olivares PR, Luzardo L, Juez-Bengoechea A, Mata E, et al. Prevalence of overweight and obesity in non-institutionalized people aged 65 or over from Spain: the elderly EXERNET multi-centre study. Obes Rev. 2011;12(8):583-92. 69. Engvall IL, Elkan AC, Tengstrand B, Cederholm T, Brismar K, Hafstrom I. Cachexia in rheumatoid arthritis is associated with

77
inflammatory activity, physical disability, and low bioavailable insulin-like growth factor. Scand J Rheumatol. 2008;37(5):321-8. 70. Baumgartner RN, Wayne SJ, Waters DL, Janssen I, Gallagher D, Morley JE. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res. 2004;12(12):1995-2004. 71. Biolo G, Cederholm T, Muscaritoli M. Muscle contractile and metabolic dysfunction is a common feature of sarcopenia of aging and chronic diseases: From sarcopenic obesity to cachexia. Clin Nutr. 2014;33(5):737-48. 72. Blair SN. Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med. 2009;43(1):1-2. 73. Jönsson AC, Lindgren I, Norrving B, Lindgren A. Weight loss after stroke: a population-based study from the Lund Stroke Register. Stroke. 2008;39(3):918-23. 74. Aronne LJ, Isoldi KK. Overweight and obesity: key components of cardiometabolic risk. Clin Cornerstone. 2007;8(3):29-37. 75. Di Napoli M, Papa F, Bocola V. C-reactive protein in ischemic stroke: an independent prognostic factor. Stroke. 2001;32(4):917-24. 76. Kuwashiro T, Sugimori H, Ago T, Kuroda J, Kamouchi M, Kitazono T, et al. Predictive role of C reactive protein in stroke recurrence after cardioembolic stroke: the Fukuoka Stroke Registry. BMJ Open. 2013;3(11):e003678. 77. Phillips A, Shaper AG, Whincup PH. Association between serum albumin and mortality from cardiovascular disease, cancer, and other causes. Lancet. 1989;2(8677):1434-6. 78. Babu MS, Kaul S, Dadheech S, Rajeshwar K, Jyothy A, Munshi A. Serum albumin levels in ischemic stroke and its subtypes: correlation with clinical outcome. Nutrition. 2013;29(6):872-5. 79. Åberg D, Jood K, Blomstrand C, Jern C, Nilsson M, Isgaard J, et al. Serum IGF-I levels correlate to improvement of functional outcome after ischemic stroke. J Clin Endocrinol Metab. 2011;96(7):1055-64. 80. Okazaki H, Beppu H, Mizutani K, Okamoto S, Sonoda S. Changes in serum growth factors in stroke rehabilitation patients and their relation to hemiparesis improvement. J Stroke Cerebrovasc Dis. 2014;23(6):1703-8. 81. Green TL, King KM. Functional and psychosocial outcomes 1 year after mild stroke. J Stroke Cerebrovasc Dis. 2010;19(1):10-6. 82. Liman TG, Heuschmann PU, Endres M, Floel A, Schwab S, Kolominsky-Rabas PL. Changes in Cognitive Function over 3 Years after First-Ever Stroke and Predictors of Cognitive Impairment and Long-Term Cognitive Stability: The Erlangen Stroke Project. Dement Geriatr Cogn Disord. 2011;31(4):291-9. 83. Jones F, Riazi A. Self-efficacy and self-management after stroke: a systematic review. Disabil Rehabil. 2011;33(10):797-810.

78
84. Saunders DH, Sanderson M, Brazzelli M, Greig CA, Mead GE. Physical fitness training for stroke patients. Cochrane Database Syst Rev. 2013;10:CD003316. 85. Burström K, Sun S, Gerdtham UG, Henriksson M, Johannesson M, Levin L, et al. Swedish experience-based value sets for EQ-5D health states. Qual Life Res. 2014;23(2):431-42. 86. Murphy SL, Williams CS, Gill TM. Characteristics associated with fear of falling and activity restriction in community-living older persons. J Am Geriatr Soc. 2002;50(3):516-20. 87. Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. J Gerontol. 1990;45(6):P239-43. 88. Weerdesteyn V, de Niet M, van Duijnhoven HJ, Geurts AC. Falls in individuals with stroke. J Rehabil Res Dev. 2008;45(8):1195-213. 89. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412-23. 90. Williams MA, Haskell WL, Ades PA, Amsterdam EA, Bittner V, Franklin BA, et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2007;116(5):572-84. 91. Lee MJ, Kilbreath SL, Singh MF, Zeman B, Davis GM. Effect of progressive resistance training on muscle performance after chronic stroke. Med Sci Sports Exerc. 2010;42(1):23-34. 92. Liu CJ, Latham NK. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst Rev. 2009(3):CD002759. 93. Todd JS, Shurley JP, Todd TC. Thomas L. DeLorme and the science of progressive resistance exercise. J Strength Cond Res. 2012;26(11):2913-23. 94. Sherrington C, Lord SR, Herbert RD. A randomized controlled trial of weight-bearing versus non-weight-bearing exercise for improving physical ability after usual care for hip fracture. Arch Phys Med Rehabil. 2004;85(5):710-6. 95. de Vreede PL, Samson MM, van Meeteren NL, Duursma SA, Verhaar HJ. Functional-task exercise versus resistance strength exercise to improve daily function in older women: a randomized, controlled trial. J Am Geriatr Soc. 2005;53(1):2-10. 96. Medicine ACoS. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687-708. 97. Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, et al. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc. 2009;41(7):1510-30.

79
98. Kirk H, Kersten P, Crawford P, Keens A, Ashburn A, Conway J. The cardiac model of rehabilitation for reducing cardiovascular risk factors post transient ischaemic attack and stroke: a randomized controlled trial. Clin Rehabil. 2014;28(4):339-49. 99. van de Port IG, Wevers LE, Lindeman E, Kwakkel G. Effects of circuit training as alternative to usual physiotherapy after stroke: randomised controlled trial. BMJ. 2012;344:e2672. 100. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet. 2011;377(9778):1693-702. 101. Wevers L, van de Port I, Vermue M, Mead G, Kwakkel G. Effects of task-oriented circuit class training on walking competency after stroke: a systematic review. Stroke. 2009;40(7):2450-9. 102. EuroQol--a new facility for the measurement of health-related quality of life. The EuroQol Group. Health Policy. 1990;16(3):199-208. 103. Washburn RA, Smith KW, Jette AM, Janney CA. The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153-62. 104. Berg K, Wood-Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med. 1995;27(1):27-36. 105. Roccaforte WH BW, Bayer BL, Wengel SP. Reliability and validity of short portable mentale status questionnaire administered by telephone. J Geriatr Psychiatry Neurol. 1994;7(1):33-8. 106. Guigoz Y. The Mini Nutritional Assessment (MNA) review of the literature--What does it tell us? J Nutr Health Aging. 2006;10(6):466-85; discussion 85-7. 107. Gottfries GG, Noltorp S, Nørgaard N. Experience with a Swedish version of the Geriatric Depression Scale in primary care centres. Int J Geriatr Psychiatry. 1997;12(10):1029-34. 108. Hellström K NL, Fugl-Meyer A.X. Relation of confidence in task performance with balance and motor function after stroke. Physiotherapy Theory and Practise. 2001;17:55-65. 109. Carr J SR. Modifierad motor assessment scale. Phys Ther. 1988;68(7):1117. 110. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):85-94. 111. Tyson S, Connell L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions: a systematic review. Clin Rehabil. 2009;23(11):1018-33. 112. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys Ther. 2002;82(2):128-37.

80
113. Pfeiffer. A short portable mentale ststus questionnaire for the assessment of organic brain deficit in elderly patients. J am geriatr soc. 1975;23(10):433-41. 114. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556-61. 115. Enright P. The six-minute walk test. Respir Care. 2003;48(8):783-5. 116. Goldstein LB, Samsa GP, Matchar DB, Horner RD. Charlson Index comorbidity adjustment for ischemic stroke outcome studies. Stroke. 2004;35(8):1941-5. 117. Janssen I, Heymsfield S, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002;50(5):889-96. 118. Abernathy RP, Black DR. Healthy body weights: an alternative perspective. Am J Clin Nutr. 1996;63(3 Suppl):448-51. 119. World Health Organization. Physical status: the use and interpretation of anthropometry. Geneva, Switzerland: WHO; 1995; 1995. 120. Sivrioglu EY, Sivrioglu K, Ertan T, Ertan FS, Cankurtaran E, Aki O, et al. Reliability and validity of the Geriatric Depression Scale in detection of poststroke minor depression. J Clin Exp Neuropsychol. 2009;31(8):999-1006. 121. Agrell B, Dehlin O. Comparison of six depression rating scales in geriatric stroke patients. Stroke. 1989;20(9):1190-4. 122. Carr JH, Shepherd RB, Nordholm L, Lynne D. Investigation of a new motor assessment scale for stroke patients. Phys Ther. 1985;65(2):175-80. 123. Bauer JM, Kaiser MJ, Anthony P, Guigoz Y, Sieber CC. The Mini Nutritional Assessment--its history, today's practice, and future perspectives. Nutr Clin Pract. 2008;23(4):388-96. 124. Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging. 2009;13(9):782-8. 125. Berg K W-DS, Willaims JL et al. Measuring balance in the elderly: validation of an instrument. Can J Public Health. 1992;83:7-11. 126. Ostir GV, Volpato S, Fried LP, Chaves P, Guralnik JM, Study WsHaA. Reliability and sensitivity to change assessed for a summary measure of lower body function: results from the Women's Health and Aging Study. J Clin Epidemiol. 2002;55(9):916-21. 127. Puthoff ML. Outcome measures in cardiopulmonary physical therapy: short physical performance battery. Cardiopulm Phys Ther J. 2008;19(1):17-22. 128. Guyatt GH, Sullivan MJ, Thompson PJ, Fallen EL, Pugsley SO, Taylor DW, et al. The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J. 1985;132(8):919-23.

81
129. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-7. 130. Dean CM, Richards CL, Malouin F. Walking speed over 10 metres overestimates locomotor capacity after stroke. Clin Rehabil. 2001;15(4):415-21. 131. Dorman PJ, Waddell F, Slattery J, Dennis M, Sandercock P. Is the EuroQol a valid measure of health-related quality of life after stroke? Stroke. 1997;28(10):1876-82. 132. Dorman P, Slattery J, Farrell B, Dennis M, Sandercock P. Qualitative comparison of the reliability of health status assessments with the EuroQol and SF-36 questionnaires after stroke. United Kingdom Collaborators in the International Stroke Trial. Stroke. 1998;29(1):63-8. 133. Lindahl M HL, Petersen A, Truelsen T, Boysen G. Self-reported physical activity after ischemic stroke correlates with physical capacity. Advances in physiotherapy. 2008;10:188-94. 134. Martin KA, Rejeski WJ, Miller ME, James MK, Ettinger WH, Messier SP. Validation of the PASE in older adults with knee pain and physical disability. Med Sci Sports Exerc. 1999;31(5):627-33. 135. Dinger MK, Oman RF, Taylor EL, Vesely SK, Able J. Stability and convergent validity of the Physical Activity Scale for the Elderly (PASE). J Sports Med Phys Fitness. 2004;44(2):186-92. 136. Hellström K, Lindmark B. Fear of falling in patients with stroke: a reliability study. Clin Rehabil. 1999;13(6):509-17. 137. Rosendahl E, Gustafson Y, Nordin E, Lundin-Olsson L, Nyberg L. A randomized controlled trial of fall prevention by a high-intensity functional exercise program for older people living in residential care facilities. Aging Clin Exp Res. 2008;20(1):67-75. 138. Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1435-45. 139. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982;14(5):377-81. 140. Colton T. Statistics in Medicine.: Little Brown and Company, Boston 1974. 141. Andridge RR, Little RJ. A Review of Hot Deck Imputation for Survey Non-response. Int Stat Rev. 2010;78(1):40-64. 142. D'Agostino RB, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-53. 143. Burström K, Johannesson M, Rehnberg C. Deteriorating health status in Stockholm 1998-2002: results from repeated population surveys using the EQ-5D. Qual Life Res. 2007;16(9):1547-53. 144. Carod-Artal FJ, Egido JA. Quality of life after stroke: the importance of a good recovery. Cerebrovasc Dis. 2009;27 Suppl 1:204-14.

82
145. Nakano MM, Otonari TS, Takara KS, Carmo CM, Tanaka C. Physical performance, balance, mobility, and muscle strength decline at different rates in elderly people. J Phys Ther Sci. 2014;26(4):583-6. 146. Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. 2000;55(4):M221-31. 147. Deshpande N, Metter EJ, Lauretani F, Bandinelli S, Guralnik J, Ferrucci L. Activity restriction induced by fear of falling and objective and subjective measures of physical function: a prospective cohort study. J Am Geriatr Soc. 2008;56(4):615-20. 148. Kuk JL, Saunders TJ, Davidson LE, Ross R. Age-related changes in total and regional fat distribution. Ageing Res Rev. 2009;8(4):339-48. 149. Stenholm S, Alley D, Bandinelli S, Griswold ME, Koskinen S, Rantanen T, et al. The effect of obesity combined with low muscle strength on decline in mobility in older persons: results from the InCHIANTI study. Int J Obes (Lond). 2009;33(6):635-44. 150. Rolland Y, Lauwers-Cances V, Cristini C, Abellan van Kan G, Janssen I, Morley JE, et al. Difficulties with physical function associated with obesity, sarcopenia, and sarcopenic-obesity in community-dwelling elderly women: the EPIDOS (EPIDemiologie de l'OSteoporose) Study. Am J Clin Nutr. 2009;89(6):1895-900. 151. Krarup LH, Truelsen T, Pedersen A, Lerke H, Lindahl M, Hansen L, et al. Level of physical activity in the week preceding an ischemic stroke. Cerebrovasc Dis. 2007;24(2-3):296-300. 152. Tieges Z, Mead G, Allerhand M, Duncan F, van Wijck F, Fitzsimons C, et al. Sedentary behaviour in the first year after stroke: a longitudinal cohort study with objective measures. Arch Phys Med Rehabil. 2014.[Epub ahead of print]. 153. Trost SG, Blair SN, Khan KM. Physical inactivity remains the greatest public health problem of the 21st century: evidence, improved methods and solutions using the '7 investments that work' as a framework. Br J Sports Med. 2014;48(3):169-70. 154. Alzahrani MA, Dean CM, Ada L, Dorsch S, Canning CG. Mood and Balance are Associated with Free-Living Physical Activity of People after Stroke Residing in the community. Stroke Res Treat. 2012;2012:470648. 155. Young CA, Mills RJ, Gibbons C, Thornton EW. Poststroke fatigue: the patient perspective. Top Stroke Rehabil. 2013;20(6):478-84. 156. Rosengren A, Wilhelmsen L, Berglund G, Elmfeldt D. Non-participants in a general population study of men, with special reference to social and alcoholic problems. Acta Med Scand. 1987;221(3):243-51. 157. Foley NC, Salter KL, Robertson J, Teasell RW, Woodbury MG. Which reported estimate of the prevalence of malnutrition after stroke is valid? Stroke. 2009;40(3):e66-74.

83
158. Stenholm S, Harris T, Rantanen T, Visser M, Kritchevsky S, Ferrucci L. Sarcopenic obesity: definition, cause and consequences. Curr Opin Clin Nutr Metab Care. 2008;11(6):693-700. 159. Fornari R, Francomano D, Greco EA, Marocco C, Lubrano C, Wannenes F, et al. Lean mass in obese adult subjects correlates with higher levels of vitamin D, insulin sensitivity and lower inflammation. J Endocrinol Invest. 2014.[Epub ahead of print]. 160. Appelros P, Jonsson F, Åsberg S, Asplund K, Glader EL, Åsberg KH, et al. Trends in stroke treatment and outcome between 1995 and 2010: observations from Riks-Stroke, the Swedish stroke register. Cerebrovasc Dis. 2014;37(1):22-9. 161. Holmgren E LB, Gosman-Hedström G, Nyberg L, Wester P. What is the Benefit of a High Intensive Exercise program after stroke - A Randomized Controlled Study. Adv in Physiother. 2010;12:115-24. 162. Rosendahl E, Lindelöf N, Littbrand H, Yifter-Lindgren E, Lundin-Olsson L, Håglin L, et al. High-intensity functional exercise program and protein-enriched energy supplement for older persons dependent in activities of daily living: a randomised controlled trial. Aust J Physiother. 2006;52(2):105-13. 163. Casanova C, Celli BR, Barria P, Casas A, Cote C, de Torres JP, et al. The 6-min walk distance in healthy subjects: reference standards from seven countries. Eur Respir J. 2011;37(1):150-6. 164. Martin PE, Rothstein DE, Larish DD. Effects of age and physical activity status on the speed-aerobic demand relationship of walking. J Appl Physiol (1985). 1992;73(1):200-6. 165. Fewtrell MS, Kennedy K, Singhal A, Martin RM, Ness A, Hadders-Algra M, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dis Child. 2008;93(6):458-61. 166. Washburn RA, Ficker JL. Physical Activity Scale for the Elderly (PASE): the relationship with activity measured by a portable accelerometer. J Sports Med Phys Fitness. 1999;39(4):336-40.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1058
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-236899
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2015