Embed Size (px)
Citation preview
Original article
Physical examination and laboratory tests in the management of patientswith rheumatoid arthritis: development of recommendations for clinical
practice based on published evidence and expert opinion
Thao Pham a, Laure Gossec b, Bruno Fautrel c, Bernard Combe d, René-Marc Flipo e,Philippe Goupille f, Xavier Le Loët g, Xavier Mariette h, Xavier Puéchal i, Daniel Wendling j,
Thierry Schaeverbeke k, Jean Sibilia l, Jacques Sany d, Maxime Dougados b,*a Service de rhumatologie, CHU de la Conception, Marseille, France
b Service de rhumatologie, hôpital Cochin, Paris, Francec Service de rhumatologie, groupe hospitalier Pitié-Salpêtrière, Paris, France
d Service d’immuno-rhumatologie, CHU Lapeyronie, Montpellier, Francee Service de rhumatologie, CHRU Roger-Salengro, Lille, France
f Service de rhumatologie, CHU, Tours, Franceg Service de rhumatologie, CHU de Rouen, Bois-Guillaume, France
h Service de rhumatologie, hôpital de Bicêtre, Le Kremlin-Bicêtre, Francei Service de rhumatologie, centre hospitalier, Le-Mans, France
j Service de rhumatologie, CHU Jean-Minjoz, Besançon, Francek Service de rhumatologie, CHU Pellegrin, Bordeaux, France
l Service de rhumatologie, CHU Hautepierre, Strasbourg, France
Received 22 July 2004; accepted 29 October 2004
Available online 21 January 2005
Abstract
Objectives. – To develop recommendations for the physical and laboratory-test follow-up of patients with rheumatoid arthritis (RA) seenin everyday practice, using evidence from the literature, supplemented with expert opinion when needed.
Methods. – A scientific committee selected 7–10 questions using the Delphi consensus procedure. Evidence-based responses to eachquestion were sought in the literature and were then used by a panel to develop recommendations. To fill in gaps in knowledge from theliterature, the panelists relied on their personal opinion.
Results. – The seven questions dealt with the physical and laboratory-test follow-up of RA and the factors predicting disease severity. Theliterature review identified 799 articles whose title and abstract suggested relevance to the study. Elimination of articles that provided no dataon the study topic left 128 original articles. The panel developed seven recommendations, one for each question, which were accepted byconsensus.
Conclusion. – Recommendations about the physical and laboratory-test follow-up of patients with RA seen in everyday practice weredeveloped. Because they constitute an objective foundation built by consensus among experts, should improve the uniformity and quality ofcare provided to RA patients in everyday practice.© 2005 Elsevier SAS. All rights reserved.
Keywords: Rheumatoid arthritis; Clinical follow-up; Laboratory-test monitoring; Patient; Everyday clinical practice
* Corresponding author. Service de rhumatologie B, hôpital Cochin, 27, rue du Faubourg Saint-Jacques, 75014 Paris, France. Tel.: +33 1 58 41 25 62; fax:+33 1 43 54 92 56.
E-mail address: [email protected] (M. Dougados).
Joint Bone Spine 72 (2005) 222–228
http://france.elsevier.com/direct/BONSOI/
1297-319X/$ - see front matter © 2005 Elsevier SAS. All rights reserved.doi:10.1016/j.jbspin.2004.10.010
1. Introduction
Recent improvements in the prognosis of rheumatoidarthritis (RA) can be ascribed not only to therapeutic advances,but also to better standardization of the management of thedisease [1]. Uniformity of the tools used to evaluate diseaseactivity is among the factors that contributes to standardizedcare [2–6]. Nevertheless, no gold standard is available forevaluating disease activity in patients with RA, and a plethoraof tools is used to evaluate treatment responses in clinicaltrials and everyday practice [6–9]. Although well validatedand widely used in clinical research, these tools are not alwayssuited to everyday rheumatological practice. Epidemiologi-cal studies identify pathophysiology-related risk factors at thelevel of a population but, again, their methodology is ill-suited to everyday practice.
The objective of this study was to have rheumatologistsdevelop evidence-based recommendations designed to stan-dardize the management of RA patients in everyday rheuma-tological practice. We elected to focus on three areas: thephysical and laboratory-test follow-up of RA patients, theevaluation of structural damage [10], and patient education[11]. The present article reports the results pertaining to thefirst of these three areas.
2. Methods
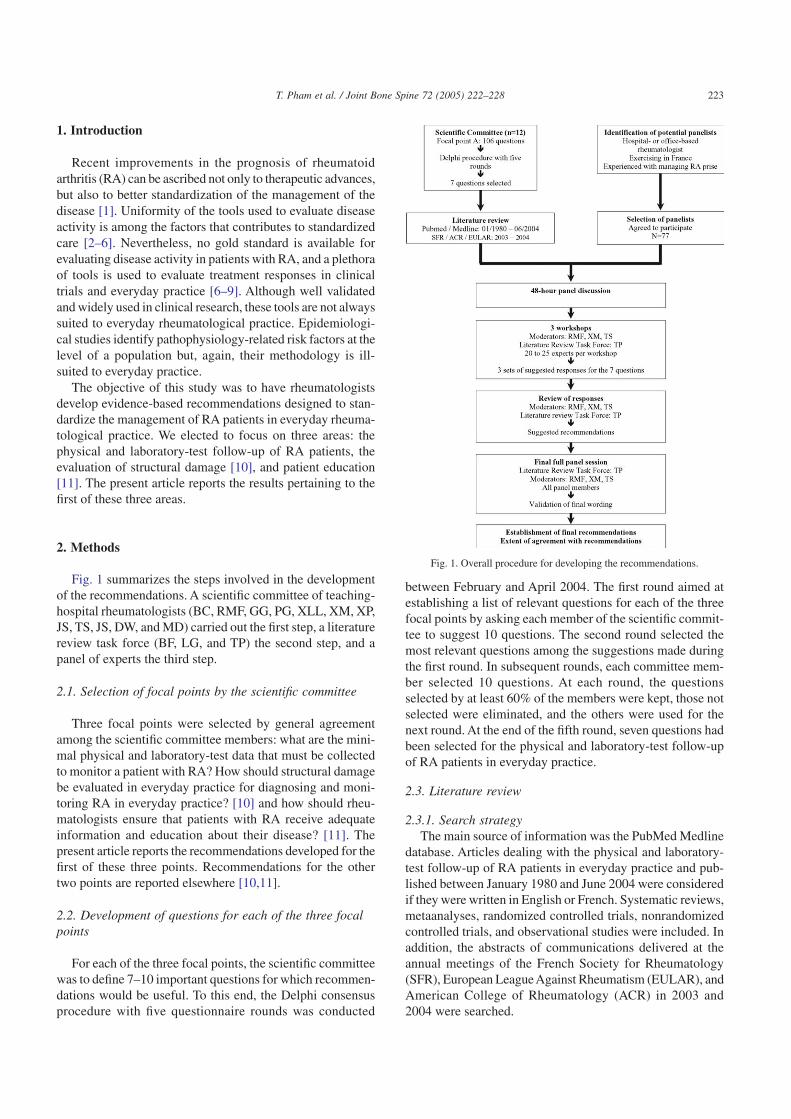
Fig. 1 summarizes the steps involved in the developmentof the recommendations. A scientific committee of teaching-hospital rheumatologists (BC, RMF, GG, PG, XLL, XM, XP,JS, TS, JS, DW, and MD) carried out the first step, a literaturereview task force (BF, LG, and TP) the second step, and apanel of experts the third step.
2.1. Selection of focal points by the scientific committee
Three focal points were selected by general agreementamong the scientific committee members: what are the mini-mal physical and laboratory-test data that must be collectedto monitor a patient with RA? How should structural damagebe evaluated in everyday practice for diagnosing and moni-toring RA in everyday practice? [10] and how should rheu-matologists ensure that patients with RA receive adequateinformation and education about their disease? [11]. Thepresent article reports the recommendations developed for thefirst of these three points. Recommendations for the othertwo points are reported elsewhere [10,11].
2.2. Development of questions for each of the three focalpoints
For each of the three focal points, the scientific committeewas to define 7–10 important questions for which recommen-dations would be useful. To this end, the Delphi consensusprocedure with five questionnaire rounds was conducted
between February and April 2004. The first round aimed atestablishing a list of relevant questions for each of the threefocal points by asking each member of the scientific commit-tee to suggest 10 questions. The second round selected themost relevant questions among the suggestions made duringthe first round. In subsequent rounds, each committee mem-ber selected 10 questions. At each round, the questionsselected by at least 60% of the members were kept, those notselected were eliminated, and the others were used for thenext round. At the end of the fifth round, seven questions hadbeen selected for the physical and laboratory-test follow-upof RA patients in everyday practice.
2.3. Literature review
2.3.1. Search strategyThe main source of information was the PubMed Medline
database. Articles dealing with the physical and laboratory-test follow-up of RA patients in everyday practice and pub-lished between January 1980 and June 2004 were consideredif they were written in English or French. Systematic reviews,metaanalyses, randomized controlled trials, nonrandomizedcontrolled trials, and observational studies were included. Inaddition, the abstracts of communications delivered at theannual meetings of the French Society for Rheumatology(SFR), European LeagueAgainst Rheumatism (EULAR), andAmerican College of Rheumatology (ACR) in 2003 and2004 were searched.
Fig. 1. Overall procedure for developing the recommendations.
223T. Pham et al. / Joint Bone Spine 72 (2005) 222–228

2.3.2. Article selectionKeywords from the following groups were combined to
retrieve publications: arthritis or rheumatoid arthritis; out-comes, clinical outcomes, biological outcomes, or pain;assessment, or evaluation, or activity score; severity, or pro-gression, or predictive factors; Health Assessment Question-naire (HAQ); anti-TNF, or TNF blockers, or adalimumab, orinfliximab, or etanercept; daily practice, or clinical practice,or practice guidelines. The articles thus retrieved were sub-jected to a stepwise selection process based on their title,abstract, and full text, in that order. Articles that dealt onlywith the efficacy of a treatment without providing data on thephysical and/or laboratory-test parameters used to monitorRA patients were eliminated.
2.3.3. Level of the evidence and strengthof the recommendations
A score was assigned to each selected study based on itsdesign, i.e., on the likelihood of bias. The score was used todefine the level of evidence from the study (Table 1) [12].The answers to the questions developed by the scientific com-mittee were based on the highest possible level of evidence.For example, when a response was available from a level Istudy, studies with designs lower down in the hierarchy werenot reviewed. The level of evidence was then used to deter-mine the strength of the recommendations (Grades A throughD, Table 2) [12]. Other factors that influenced the strengthgrade were the treatment effect, potential adverse effects, easeof administration, cost, and applicability of study conclu-sions. Grades were determined a posteriori by the literaturereview task force.
2.3.4. Presentation of the literature review datato the scientific committee members
This occurred in June 2004 in Berlin, Germany. For eachfocal point, the moderators, who were members of the scien-tific committee, defined the modalities for the panel confer-ences.
2.4. Panel conferences
2.4.1. Selection of panelistsPanelists had to be French rheumatologists with extensive
experience in the management of RA. Of the 575 expertsinvited, 77 attended the Berlin meeting in June 2004; amongthem, 53.2% worked full-time in hospitals, 11.7% full-timein office practice, and 35.1% part-time in office-practice andpart-time in hospitals. Estimates by these 77 rheumatologistsof the number of RA patients they managed each month wereas follows: <five in 1.5% of cases, 5–9 in 12.3% of cases,10–19 in 26.2% of cases, 20–29 in 23.1% of cases, 30–39 in12.3% of cases, and >40 in 24.6% of cases.
2.4.2. Development of evidence-based recommendations bythe panel
The results of the literature review were reported to thepanel by the task force member in charge of each focal point(TP for physical and laboratory-test follow-up). This was doneduring three workshops, each attended by 20–25 panelists. Theworkshops were moderated by scientific committee members(RMF, XM, and TS for physical and laboratory-test follow-up). The evidence from the literature was presented for eachof the seven questions, and for each article the level of evi-dence was given. The order of the questions was different inthe three workshops. At the end of each workshop, the panel-ists were asked to suggest answers to the questions, as a pre-liminary to the development of evidence-based recommenda-tions. Gaps in knowledge available from the literature werefilled in by the panelists’ expert opinion. Suggested answerswere used by the three moderators and the relevant literature-review task force member to write a recommendation; whendisagreements about a question were noted across work-shops, several alternative answers were developed. The finalrecommendations were chosen during a meeting of all panel-ists, scientific committee members, and task force members.The extent of agreement among the experts was evaluatedusing the five-category Likert scale (strongly disagree, dis-agree, neither agree nor disagree, agree, and strongly agree).
3. Results
3.1. Literature review
The literature review identified 78,191 articles on RA, ofwhich 9476 provided data on the physical and/or laboratory-test follow-up of patients with RA. Selection on the title thenthe abstract left 799 articles. Articles that provided no infor-mation on physical and/or laboratory-test follow-up wereeliminated. This left 128 original articles, of which none wererandomized controlled trials or metaanalyses of physical orlaboratory-test criteria for monitoring RA patients in every-day practice. The articles reported either studies on tools formeasuring clinical and biological disease activity, random-ized controlled trials of drugs or treatment strategies, or pro-
Table 1Classification of levels of evidence according to study design [12]
Level Evidence based on1 a A metaanalyses of randomized controlled trials1 b At least one randomized controlled trial2 a At least one controlled trial without randomization2 b At least one other type of quasi-experimental study3 Nonexperimental descriptive studies4 Expert opinion, clinical experience of respected authorities
Table 2Strength of recommendations [12]
StrengthA Directly based on category 1 evidenceB Directly based on category 2 evidence or extrapolated recommen-
dation from category 1 evidenceC Directly based on category 3 evidence or extrapolated recommen-
dation from category 1 or 2 evidenceD Directly based on category 4 evidence or extrapolated recommen-
dation from category 1, 2, or 3 evidence
224 T. Pham et al. / Joint Bone Spine 72 (2005) 222–228
spective observational studies, most notably on factors pre-dicting severe disease. Quality scores (level of evidence)varied widely across studies.
3.2. The recommendations
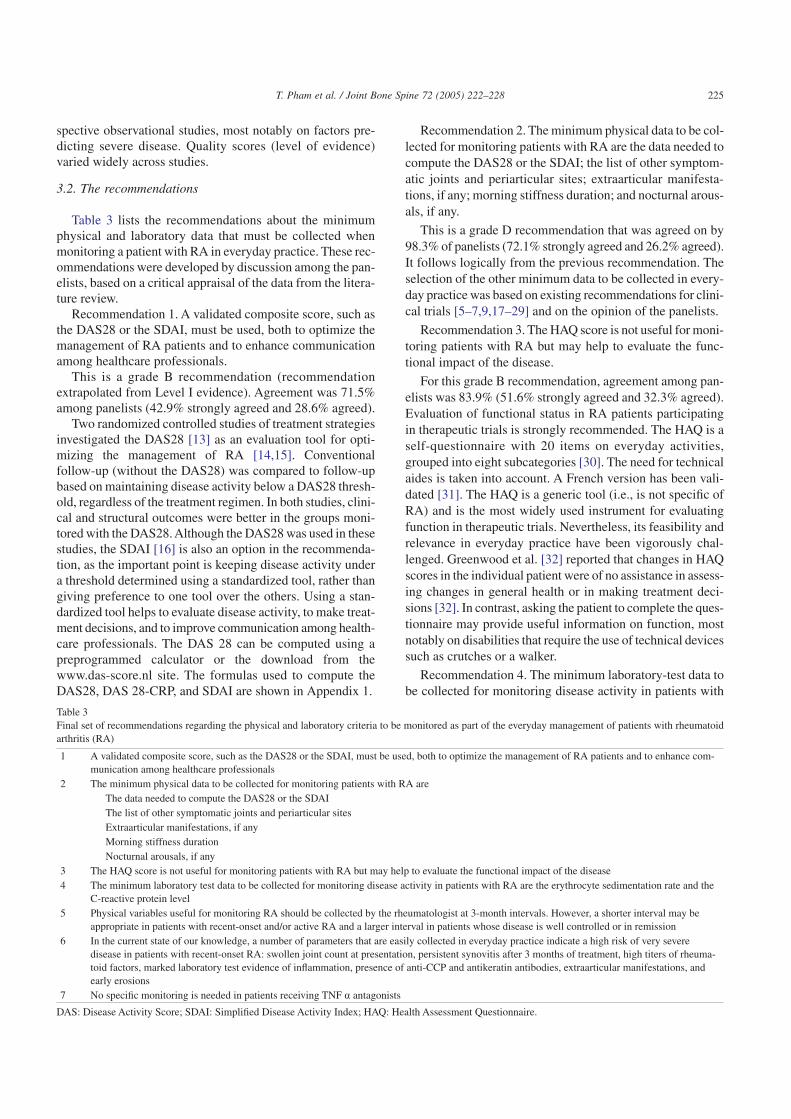
Table 3 lists the recommendations about the minimumphysical and laboratory data that must be collected whenmonitoring a patient with RA in everyday practice. These rec-ommendations were developed by discussion among the pan-elists, based on a critical appraisal of the data from the litera-ture review.
Recommendation 1. A validated composite score, such asthe DAS28 or the SDAI, must be used, both to optimize themanagement of RA patients and to enhance communicationamong healthcare professionals.
This is a grade B recommendation (recommendationextrapolated from Level I evidence). Agreement was 71.5%among panelists (42.9% strongly agreed and 28.6% agreed).
Two randomized controlled studies of treatment strategiesinvestigated the DAS28 [13] as an evaluation tool for opti-mizing the management of RA [14,15]. Conventionalfollow-up (without the DAS28) was compared to follow-upbased on maintaining disease activity below a DAS28 thresh-old, regardless of the treatment regimen. In both studies, clini-cal and structural outcomes were better in the groups moni-tored with the DAS28.Although the DAS28 was used in thesestudies, the SDAI [16] is also an option in the recommenda-tion, as the important point is keeping disease activity undera threshold determined using a standardized tool, rather thangiving preference to one tool over the others. Using a stan-dardized tool helps to evaluate disease activity, to make treat-ment decisions, and to improve communication among health-care professionals. The DAS 28 can be computed using apreprogrammed calculator or the download from thewww.das-score.nl site. The formulas used to compute theDAS28, DAS 28-CRP, and SDAI are shown in Appendix 1.
Recommendation 2. The minimum physical data to be col-lected for monitoring patients with RA are the data needed tocompute the DAS28 or the SDAI; the list of other symptom-atic joints and periarticular sites; extraarticular manifesta-tions, if any; morning stiffness duration; and nocturnal arous-als, if any.
This is a grade D recommendation that was agreed on by98.3% of panelists (72.1% strongly agreed and 26.2% agreed).It follows logically from the previous recommendation. Theselection of the other minimum data to be collected in every-day practice was based on existing recommendations for clini-cal trials [5–7,9,17–29] and on the opinion of the panelists.
Recommendation 3. The HAQ score is not useful for moni-toring patients with RA but may help to evaluate the func-tional impact of the disease.
For this grade B recommendation, agreement among pan-elists was 83.9% (51.6% strongly agreed and 32.3% agreed).Evaluation of functional status in RA patients participatingin therapeutic trials is strongly recommended. The HAQ is aself-questionnaire with 20 items on everyday activities,grouped into eight subcategories [30]. The need for technicalaides is taken into account. A French version has been vali-dated [31]. The HAQ is a generic tool (i.e., is not specific ofRA) and is the most widely used instrument for evaluatingfunction in therapeutic trials. Nevertheless, its feasibility andrelevance in everyday practice have been vigorously chal-lenged. Greenwood et al. [32] reported that changes in HAQscores in the individual patient were of no assistance in assess-ing changes in general health or in making treatment deci-sions [32]. In contrast, asking the patient to complete the ques-tionnaire may provide useful information on function, mostnotably on disabilities that require the use of technical devicessuch as crutches or a walker.
Recommendation 4. The minimum laboratory-test data tobe collected for monitoring disease activity in patients with
Table 3Final set of recommendations regarding the physical and laboratory criteria to be monitored as part of the everyday management of patients with rheumatoidarthritis (RA)
1 A validated composite score, such as the DAS28 or the SDAI, must be used, both to optimize the management of RA patients and to enhance com-munication among healthcare professionals
2 The minimum physical data to be collected for monitoring patients with RA areThe data needed to compute the DAS28 or the SDAIThe list of other symptomatic joints and periarticular sitesExtraarticular manifestations, if anyMorning stiffness durationNocturnal arousals, if any
3 The HAQ score is not useful for monitoring patients with RA but may help to evaluate the functional impact of the disease4 The minimum laboratory test data to be collected for monitoring disease activity in patients with RA are the erythrocyte sedimentation rate and the
C-reactive protein level5 Physical variables useful for monitoring RA should be collected by the rheumatologist at 3-month intervals. However, a shorter interval may be
appropriate in patients with recent-onset and/or active RA and a larger interval in patients whose disease is well controlled or in remission6 In the current state of our knowledge, a number of parameters that are easily collected in everyday practice indicate a high risk of very severe
disease in patients with recent-onset RA: swollen joint count at presentation, persistent synovitis after 3 months of treatment, high titers of rheuma-toid factors, marked laboratory test evidence of inflammation, presence of anti-CCP and antikeratin antibodies, extraarticular manifestations, andearly erosions
7 No specific monitoring is needed in patients receiving TNF a antagonists
DAS: Disease Activity Score; SDAI: Simplified Disease Activity Index; HAQ: Health Assessment Questionnaire.
225T. Pham et al. / Joint Bone Spine 72 (2005) 222–228

RA are the erythrocyte sedimentation rate and the C-reactiveprotein level.
This is a grade D recommendation accepted by 84.4% ofpanelists (54.7% strongly agreed and 29.7% agreed). Its fol-lows logically from recommendation 1, as it is based on useof a validated composite index for monitoring disease activ-ity [13,16], on current recommendations for clinical trials[5,17,33], and on the opinion of the panelists. Use of proteinC levels is recommended when the erythrocyte sedimenta-tion rate is difficult to interpret, for instance, in patients withmonoclonal or polyclonal gammopathy.
Recommendation 5. Physical variables useful for monitor-ing RA should be collected by the rheumatologist at 3-monthintervals. However, a shorter interval may be appropriate inpatients with recent-onset and/or active RA and a larger inter-val in patients whose disease is well controlled or in remis-sion.
This is a grade B recommendation. Agreement was 98.4%(82.0% strongly agreed and 16.4% agreed). Two randomizedcontrolled studies of treatment strategies compared differentintervals for physical examinations and laboratory-tests[14,34]. In one of these studies, intensive follow-up withmonthly evaluations and a DAS28 target of less than 2.4 wascompared to conventional follow-up with 3-monthly evalua-tions and no target, in patients with recent-onset RA (meandisease duration, 20 months) [14]. After 18 months, symp-tomatic and structural control was better in the intensivefollow-up group than in the conventional strategy group. Inthe other study, patients with established RA (mean diseaseduration, 10 years) were randomly allocated to conventionalfollow-up with evaluations every 3–4 months or to direct-access follow-up, in which rheumatologist visits occurred bypatient request [34,35]. After 6 years, no significant differ-ences were found between the two groups for clinical or bio-logical disease activity, pain, function, or structural damage.Therefore, the panelists recommended a visit every 3 months.Nevertheless, this follow-up schedule should be adjusted asneeded: shorter intervals are warranted in patients with recent-onset and/or active RA, as well as to evaluate the effective-ness and safety of new treatment regimens, whereas patientswhose disease is well controlled or in remission can be evalu-ated at longer intervals.
Recommendation 6. In the current state of our knowledge,a number of parameters that are easily collected in everydaypractice indicate a high risk of very severe disease in patientswith recent-onset RA: swollen joint count at presentation, per-sistent synovitis after 3 months of treatment, high titers ofrheumatoid factors, marked laboratory-test evidence ofinflammation, presence of anti-CCP and antikeratin antibod-ies, extraarticular manifestations, and early erosions.
For this grade C recommendation, agreement among pan-elists was 88.0% (53.5% strongly agreed, 34.5% agreed, 1.7%neither agreed nor disagreed, 6.9% disagreed, and 3.5%strongly disagreed). The complexity of this recommendationstems from the lack of a definition of disease severity for RA:thus, severity can be assessed in terms of function, structural
damage, or mortality. Numerous observational studies havesought to identify factors that predict severe disease, and theirresults are somewhat conflicting [36–50]. The parameterslisted in the recommendation were selected primarily on thebasis of their suitability to everyday practice.
Recommendation 7. No specific monitoring is needed inpatients receiving TNF a antagonists.
This is a grade D recommendation. Agreement was 88.0%among panelists (53.5% strongly agreed, 34.5% agreed, 1.7%neither agreed nor disagreed, 6.9% disagreed, and 3.5%strongly disagreed). This recommendation was establishedonly for patients receiving a TNF a antagonist as single-drugtherapy. For none of the available TNF a antagonists does theSummary of Product Characteristics recommend specificmonitoring. In therapeutic trials and the postmarketing expe-rience recorded by the Food and Drug Administration [51], afew cases of agranulocytosis, pancytopenia, and liver failurehave occurred. However, these manifestations are so uncom-mon, and the hematologic side effects so sudden, that no rou-tine monitoring tests have been recommended by the FDA orEuropean Medicines Agency (EMEA). Nevertheless, a highindex of suspicion should be maintained and regular bloodcell counts and liver function tests may be useful in somepatients. Laboratory-tests used to monitor patients on TNF aantagonist therapy should be selected mainly according to theclinical picture, disease activity, and concomitant treatments.
4. Discussion
The objective of this study was to find answers to unre-solved questions relevant to the everyday management ofpatients with RA [10,11]. The recent introduction of newdrugs and therefore of new treatment strategies has radicallychanged the management of RA [52]. Clearly, this new situ-ation requires new recommendations to help French rheuma-tologists in their everyday practice.
The recommendations described here are mainly evidence-based. However, because large gaps in knowledge still exist,some recommendations are partly based on expert opinion[53]. An extensive search of the literature published beforeJune 2004 was conducted by a task force under the responsi-bility of a scientific committee, and for each article the levelof evidence and relevance to our topic were evaluated. Thedata thus compiled were used to drive discussions among77 panel members over a 2-day period. All the panelists wererheumatologists recognized as having extensive experiencewith managing RA. Their opinion was particularly valuablewhen the published data failed to provide answers to the ques-tions asked. However, the panel was not multidisciplinary,and there was no external review of selected articles or draftrecommendations. All the panelists gave their opinion. At theend of the panel discussion, the scientific committee evalu-ated the strength of each recommendation, based not only onthe level of the published evidence, but also—and this is anoriginal feature of our work—on the extent of agreementamong panelists.
226 T. Pham et al. / Joint Bone Spine 72 (2005) 222–228

Several factors may explain why most of the recommen-dations are grade D. First, the questions were selected by thescientific committee members, all of whom were rheumatol-ogy professors, who probably focused on problems they feltwere not only important, but also difficult to solve despitetheir extensive knowledge of the literature. Therefore, it isnot surprising that higher-grade recommendations were notachieved. Furthermore, follow-up is well standardized in clini-cal research trials but is far less so in everyday practice. Jointdiseases are no exception to this rule.
Therefore, for this type of recommendations, we believethat expert opinion is valuable. Nevertheless, a grading sys-tem is highly desirable. With the conventional approach, thereis only one grade for expert opinion. This prompted us toevaluate the extent of agreement among experts for each rec-ommendation, using the five-category Likert scale, which wascompleted anonymously. Although agreement was usuallyvery high, it should be borne in mind that the Likert scale
was completed by the experts who developed the recommen-dations. Studies are needed to determine the level of agree-ment among experts who are well experienced in the man-agement of RA but did not participate in developing therecommendations. Subsequent steps will include disseminat-ing the recommendations and encouraging their application,evaluating their impact, and finally updating them regularly,with the ultimate goal of improving the management of RA.
Acknowledgments
This study was supported by Abbott France.We are grateful to Catherine Mazzacco, Hubert Drougard,
and Gérard Goldfarb from Laboratoires Abbott France fortheir support and to the 77 experts who gave of their knowl-edge and experience to participate in developing these rec-ommendations (names listed in [11]).
Appendix 1. Computation of composite indices [13,16]
DAS 28=0.56 �TJC + 0.28 �SJC + 0.70 ln� ESR � + 0.014 � EVA �
DAS 28-CRP=0.56�TJC + 0.28�SJC + 0.36 ln � CRP � mg/l � + 1 � + 0.014 � VAS � + 0.96
SDAI = TJC + SJC + VAS patient + VAS physician + CRP � mg/dl �
TJC: tender joint count (28); SJC: swollen joint count (28); VAS: visual analog scale for overall health (0–100); ESR:erythrocyte sedimentation rate; CRP: C-reactive protein (in mg/l for the DAS 28-CRP and in mg/dl for the SDAI).
References
[1] Davis RM, Wagner EG, Groves T. Advances in managing chronicdisease. Research, performance measurement, and quality improve-ment are key. BMJ 2000;320:525–6.
[2] Boers M, Tugwell P, Felson DT, et al. World Health Organization andInternational League of Associations for Rheumatology core end-points for symptom modifying antirheumatic drugs in rheumatoidarthritis clinical trials. J Rheumatol Suppl 1994;41:86–9.
[3] Boers M, Felson DT. Clinical measures in rheumatoid arthritis: whichare most useful in assessing patients? J Rheumatol 1994;21:1773–4.
[4] Tugwell P, Boers M. Developing consensus on preliminary core effi-cacy endpoints for rheumatoid arthritis clinical trials. OMERACTCommittee. J Rheumatol 1993;20:555–6.
[5] Tugwell P, Boers M. OMERACT conference on outcome measures inrheumatoid arthritis clinical trials: introduction. J Rheumatol 1993;20:528–30.
[6] Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M,Fried B, et al. The American College of Rheumatology preliminarycore set of disease activity measures for rheumatoid arthritis clinicaltrials. The Committee on Outcome Measures in Rheumatoid ArthritisClinical Trials. Arthritis Rheum 1993;36:729–40.
[7] Pincus T, Sokka T. Quantitative measures for assessing rheumatoidarthritis in clinical trials and clinical care. Best Pract Res Clin Rheu-matol 2003;17:753–81.
[8] Van Riel PL, Van Gestel AM, Van de Putte LB. Development andvalidation of response criteria in rheumatoid arthritis: steps towards aninternational consensus on prognostic markers. Br J Rheumatol 1996;35(Suppl 2):4–7.
[9] Van der Heijde DM, Van ’t Hof M, Van Riel PL, Van de Putte LB.Development of a disease activity score based on judgment in clinicalpractice by rheumatologists. J Rheumatol 1993;20:579–81.
[10] Gossec L, Fautrel B, Pham T, Combe B, Flipo R, Goupille P, et al.Structural evaluation in the management of patients with rheumatoidarthritis: development of recommendations for clinical practice basedon published evidence and expert opinion. Joint Bone Spine 2005 (thisissue).
[11] Fautrel B, Pham T, Gossec L, Combe B, Flipo R, Goupille P, et al.Role and modalities of information and education in the managementof patients with rheumatoid arthritis: development of recommenda-tions for clinical practice based on published evidence and expertopinion. Joint Bone Spine 2005 (in press).
[12] Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guidelines:developing guidelines. BMJ 1999;318:593–6.
[13] Prevoo ML, Van ’t Hof MA, Kuper HH, Van Leeuwen MA,Van de Putte LB, Van Riel PL. Modified disease activity scores thatinclude twenty-eight-joint counts. Development and validation in aprospective longitudinal study of patients with rheumatoid arthritis.Arthritis Rheum 1995;38:44–8.
[14] Porter RD, Grigor C, Stirling A, Capel HA. A randomized controlledtrial of strategy of tight control of disease activity in rheumatoidarthritis-outcome over 18 months. Arthritis Rheum 2003;48:S232.
[15] Fransen J, Speyer I, Moens H, Van Riel P. The effectiveness ofsystematic monitoring of RA disease activity in daily practice(TRAC): a multicentre cluster-RCT. Ann Rheum Dis 2004;63:84.
[16] Smolen JS, Breedveld FC, Schiff MH, Kalden JR, Emery P, Eberl G,et al. A simplified disease activity index for rheumatoid arthritis foruse in clinical practice. Rheumatology (Oxford) 2003;42:244–57.
[17] Van Riel PL, Van de Putte LB. Clinical assessment and clinical trialsin rheumatoid arthritis. Curr Opin Rheumatol 1994;6:132–9.
[18] Van der Heijde DM, Van ’t Hof MA, Van Riel PL, Theunisse LA,Lubberts EW, Van Leeuwen MA, et al. Judging disease activity inclinical practice in rheumatoid arthritis: first step in the developmentof a disease activity score. Ann Rheum Dis 1990;49:916–20.
227T. Pham et al. / Joint Bone Spine 72 (2005) 222–228
[19] Boers M, Van Riel PL, Felson DT, Tugwell P. Assessing the activity ofrheumatoid arthritis. Baillieres Clin Rheumatol 1995;9:305–17.
[20] Van Gestel AM, Anderson JJ, Van Riel PL, Boers M, Haagsma CJ,Rich B, et al. ACR and EULAR improvement criteria have compa-rable validity in rheumatoid arthritis trials. American College ofRheumatology European League of Associations for Rheumatology. JRheumatol 1999;26:705–11.
[21] Mason JH, Meenan RF, Anderson JJ. Do self-reported arthritis symp-tom (RADAR) and health status (AIMS2) data provide duplicative orcomplementary information? Arthritis Care Res 1992;5:163–72.
[22] Fransen J, Langenegger T, Michel BA, Stucki G. Feasibility andvalidity of the RADAI, a self-administered rheumatoid arthritis dis-ease activity index. Rheumatology (Oxford) 2000;39:321–7.
[23] Fuchs HA, Brooks RH, Callahan LF, Pincus T. A simplified twenty-eight-joint quantitative articular index in rheumatoid arthritis. Arthri-tis Rheum 1989;32:531–7.
[24] Ritchie DA, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieve-son P, et al. Evaluation of a simple articular index for joint tendernessin rheumatoid arthritis. Clinical studies with an articular index for theassessment of joint tenderness in patients with rheumatoid arthritis.Ann Rheum Dis 1969;28:196.
[25] Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieve-son P, et al. Clinical studies with an articular index for the assessmentof joint tenderness in patients with rheumatoid arthritis. QJM 1968;37:393–406.
[26] Egger MJ, Huth DA, Ward JR, Reading JC, Williams HJ. Reducedjoint count indices in the evaluation of rheumatoid arthritis. ArthritisRheum 1985;28:613–9.
[27] Pincus T, Brooks RH, Callahan LF. A proposed 30–45 minute 4 pagestandard protocol to evaluate rheumatoid arthritis (SPERA) thatincludes measures of inflammatory activity, joint damage, and long-term outcomes. J Rheumatol 1999;26:473–80.
[28] Fuchs HA, Callahan LF, Kaye JJ, Brooks RH, Nance EP, Pincus T.Radiographic and joint count findings of the hand in rheumatoidarthritis. Related and unrelated findings. Arthritis Rheum 1988;31:44–51.
[29] Birrell FN, Hassell AB, Jones PW, Dawes PT. Why not use OSRA? Acomparison of Overall Status in Rheumatoid Arthritis (RA) with ACRcore set and other indices of disease activity in RA. J Rheumatol1998;25:1709–15.
[30] Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patientoutcome in arthritis. Arthritis Rheum 1980;23:137–45.
[31] Guillemin F, Braincon S, Pourel J. Measurement of the functionalcapacity in rheumatoid polyarthritis: a French adaptation of the HealthAssessment Questionnaire (HAQ). Rev Rhum Mal Osteoartic 1991;58:459–65.
[32] Greenwood MC, Doyle DV, Ensor M. Does the Stanford HealthAssessment Questionnaire have potential as a monitoring tool forsubjects with rheumatoid arthritis? Ann Rheum Dis 2001;60:344–8.
[33] Felson DT, Anderson JJ, Boers M, Bombardier C, Furst D, Gold-smith C, et al. American College of Rheumatology. Preliminary defi-nition of improvement in rheumatoid arthritis. Arthritis Rheum 1995;38:727–35.
[34] Kirwan J, Hewlett S, Mitchell K, Hehir M, Pollock J, Blair P, et al.RCT of patient-initiated review versus regular physician-initiatedfollow-up in rheumatoid arthritis, extended to 6 years. Ann RheumDis 2004;63:75.
[35] Kirwan JR, Mitchell K, Hewlett S, Hehir M, Pollock J, Memel D, et al.Clinical and psychological outcome from a randomized controlledtrial of patient-initiated direct-access hospital follow-up for rheuma-toid arthritis extended to 4 years. Rheumatology (Oxford) 2003;42:422–6.
[36] Combe B, Cantagrel A, Goupille P, Bozonnat MC, Sibilia J, Eliaou JF,et al. Predictive factors of 5-year health assessment questionnairedisability in early rheumatoid arthritis. J Rheumatol 2003;30:2344–9.
[37] Bukhari M, Lunt M, Harrison BJ, Scott DG, Symmons DP, Silman AJ.Rheumatoid factor is the major predictor of increasing severity ofradiographic erosions in rheumatoid arthritis: results from the NorfolkArthritis Register Study, a large inception cohort. Arthritis Rheum2002;46:906–12.
[38] Goronzy JJ, Matteson EL, Fulbright JW, Warrington KJ, Chang-Miller A, Hunder GG, et al. Prognostic markers of radiographicprogression in early rheumatoid arthritis. Arthritis Rheum 2004;50:43–54.
[39] Meyer O, Labarre C, Dougados M, Goupille P, CantagrelA, DuboisA,et al. Anticitrullinated protein/peptide antibody assays in early rheu-matoid arthritis for predicting five year radiographic damage. AnnRheum Dis 2003;62:120–6.
[40] Vencovsky J, Machacek S, Sedova L, Kafkova J, Gatterova J, Pesa-kova V, et al. Autoantibodies can be prognostic markers of an erosivedisease in early rheumatoid arthritis. Ann Rheum Dis 2003;62:427–30.
[41] Van Gaalen FA, Van Aken J, Huizinga TW, Schreuder GM, Breed-veld FC, Zanelli E, et al. Association between HLA class II genes andautoantibodies to cyclic citrullinated peptides (CCPs) influences theseverity of rheumatoid arthritis. Arthritis Rheum 2004;50:2113–21.
[42] Drossaers-Bakker KW, Zwinderman AH, Vlieland TP, Van Zeben D,Vos K, Breedveld FC, et al. Long-term outcome in rheumatoidarthritis: a simple algorithm of baseline parameters can predict radio-graphic damage, disability, and disease course at 12-year followup.Arthritis Rheum 2002;47:383–90.
[43] Wiles NJ, Dunn G, Barrett EM, Harrison BJ, Silman AJ, Sym-mons DP. One-year followup variables predict disability 5 years afterpresentation with inflammatory polyarthritis with greater accuracythan at baseline. J Rheumatol 2000;27:2360–6.
[44] Van Jaarsveld CH, Ter Borg EJ, Jacobs JW, Schellekens GA, Gmelig-Meyling FH, Van Booma-Frankfort C, et al. The prognostic value ofthe antiperinuclear factor, anti-citrullinated peptide antibodies andrheumatoid factor in early rheumatoid arthritis. Clin Exp Rheumatol1999;17:689–97.
[45] Dixey J, Solymossy C, Young A. Is it possible to predict radiologicaldamage in early rheumatoid arthritis (RA)? A report on the occur-rence, progression, and prognostic factors of radiological erosionsover the first 3 years in 866 patients from the Early RA Study (ERAS).J Rheumatol Suppl 2004;69:48–54.
[46] Valenzuela-Castano A, Garcia-Lopez A, Perez-Vilches D, Rodriguez-Perez R, Gonzalez-Escribano MF, Nunez-Roldan A. The predictivevalue of the HLA shared epitope for severity of radiological jointdamage in patients with rheumatoid arthritis. A 10 year observationalprospective study. J Rheumatol 2000;27:571–4.
[47] Moreno I, Valenzuela A, Garcia A,Yelamos J, Sanchez B, Hernanz W.Association of the shared epitope with radiological severity of rheu-matoid arthritis. J Rheumatol 1996;23:6–9.
[48] Mattey DL, Hassell AB, Dawes PT, Cheung NT, Poulton KV, Thom-son W, et al. Independent association of rheumatoid factor and theHLA-DRB1 shared epitope with radiographic outcome in rheumatoidarthritis. Arthritis Rheum 2001;44:1529–33.
[49] Kaltenhauser S, Wagner U, Schuster E, Wassmuth R, Arnold S,Seidel W, et al. Immunogenetic markers and seropositivity predictradiological progression in early rheumatoid arthritis independent ofdisease activity. J Rheumatol 2001;28:735–44.
[50] Wolfe F, Michaud K, Gefeller O, Choi HK. Predicting mortality inpatients with rheumatoid arthritis. Arthritis Rheum 2003;48:1530–42.
[51] Safety update TNFa blocking agents. Available from: http://www.fda.gov/ohrms/dockets/ac/03/transcripts/3930T1.htm.
[52] Raissouni N, Gossec L, Ayral X, Dougados M. New concepts in thediagnosis and treatment of recent-onset polyarthritis. Joint BoneSpine 2005 (this issue).
[53] Dougados M, Netteridge N, Burmester G, Euller-Ziegler L,Guillemin F, Hirvonen J, et al. EULAR standardized operating proce-dures for the elaboration, evaluation, dissemination and implementa-tion of recommendations endorsed by the EULAR standing commit-tees. Ann Rheum Dis 2004;62:1172–6.
228 T. Pham et al. / Joint Bone Spine 72 (2005) 222–228










