Embed Size (px)
Citation preview
Physical Activity to Improve CV Health in Women: a Pragmatic Trial
Women’s Health Initiative Strong & Healthy The WHISH Trial
CCC-lead PI: Marcia Stefanick, Ph.DBehavioral Science Director: Abby King, Ph.D.
Stanford University School of Medicine
DCC Multiple-PI: Andrea LaCroix, Ph.D.(lead) Charles Kooperberg, Ph.D., FHCRC
(Fred Hutchinson Cancer Research Center)
Clustered R01s ≥ $500K/yrPAR-13-128 (Investigator Initiated Multi-Site Clinical Trials - Collaborative RO1).
WHISH Trial
Primary Hypothesis An intervention designed to improve levels of aerobic physical activity based on national (DHHS*)
recommendations for older U.S. adults, combined with muscle strengthening, balance and flexibility exercises, and reduced sedentary behavior, will reduce major CV events (CV death, MI, stroke) in older (WHI) women, compared to “usual activity” controls over ~4 years of follow-up
Physical Activity Guidelines Advisory Committee(2008). Report of the Physical Activity Guidelines Advisory Committee, 2008. Washington, DC: U.S. Department of Health and Human Services. http://www.health.gov/paguidelines/guidelines/chapter5.aspx
*
WHISH Trial
Primary Aim Conduct a pragmatic trial in approximately 52,500 women enrolled in the WHI Extension Study, for whom CV outcomes are available, randomized to a centralized, tailored physical activity intervention or “usual activity” (observational control comparison).
Primary Safety Aim Evaluate whether an intervention based on DHHS-recommended levels of physical activity for older American adults increases the risk of total clinical fracture, hip fracture, falls, or non-CVD mortality over ~4 years
WHISH Trial
Secondary Aim Evaluate whether this tailored, PA intervention reduces risk of selected PA-linked secondary outcomes, potentially ameliorable through regular physical activity, of importance to maintaining independence in older women
Secondary Hypotheses Women randomized to the WHISH PA intervention (compared to observational control) will have: Lower rates of venous thromboembolic events (VTE)
and peripheral artery disease (PAD); Less loss of physical function including higher rates of
ongoing mobility (and independence)
Secondary Safety AimEvaluate whether increased PA increases CABG or PCI
WHISH Trial
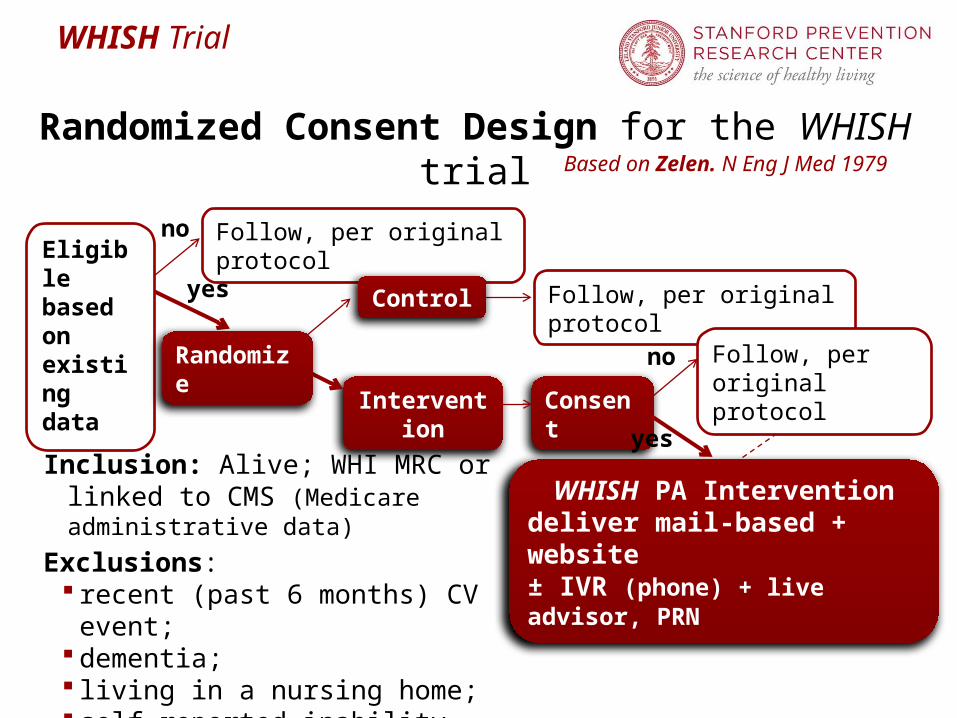
Eligible based on existing data
Intervention
Consent
WHISH PA Interventiondeliver mail-based + website ± IVR (phone) + live advisor, PRN
Follow, per original protocolno
yes
no
yes
Based on Zelen. N Eng J Med 1979
Randomized Consent Design for the WHISH trial
Randomize
Follow, per original protocol
Follow, per original protocol
Inclusion: Alive; WHI MRC or linked to CMS (Medicare administrative data)
Exclusions: recent (past 6 months) CV event; dementia; living in a nursing home; self-reported inability to walk
Control
WHISH Trial
Assumptions in randomized consent design Existing data are adequate for primary eligibility
determination Original consent and protocol covers
Re-approach for additional studies All outcome ascertainment procedures
Control arm represents “standard of care” Randomization is ethical Power calculations account for
Lack of adherence/cross-over Dilution of effect from non-consenters
Fraction consenting to intervention expected to be high Primary analysis based on ITT principle, includes:
non-consenters those found to be ineligible after randomization
WHISH Trial
Pragmatic Trial considerationsRandomized Consent Design* in well-characterized cohort
(WHI infrastructure creates tremendous efficiencies**)Scientific Advantages:
Increases external validity (no/limited Hawthorne effect in control arm)
Provides estimates of effectiveness, rather than efficacyPractical advantages
Avoids resentful demoralization in control groupSimplifies recruitment/consent and reduces associated costs
Intervention based on National Recommendations (DHHS) and Publicly Available Resources (NIA Go4Life®) to be delivered by widely used Technology (interactive voice response, IVR + telephone) – pilot tested in small WHI sample; will offer two levels of consenting
Outcomes collected in WHI: ~20,000 in Medical Records Cohort (MRC) + additional 32,500 linked to CMS records; NDI searches
*Adamson et al, Contemporary Clin Trials 2006;27:305-319.
**
WHISH Trial
WHISH Intervention – in brief Goals per DHHS (2008) PA Guidelines for older adults
Consent mailings to women assigned to Intervention will include basic recommendations/goals and Go4Life® pamphlet (exercises)
Go4Life® Written Materials, DVD, Websitepublicly available evidence-based exercise and physical activity
materials developed by the National Institute on Aging “Full Consent” reinforced and individualized by means of an
algorithm-driven telephone- delivered interactive voice response (IVR) system managed centrally at Stanford, with “light (human) touch” (telephone and mailed materials), as neededWeekly for 6 weeks, Bi-monthly for 6 weeks, then Monthly
“Mailings Only” consent option (2-4x/yr) – may become “Full” Special materials for women who use walkers, canes, wheelchairs,
and to deal with injuries & rehabilitation
National (& Regional) Community Facilities/Resources, e.g. Senior Centers, Ys (Silver Sneakers), Special Programs
WHISH Trial
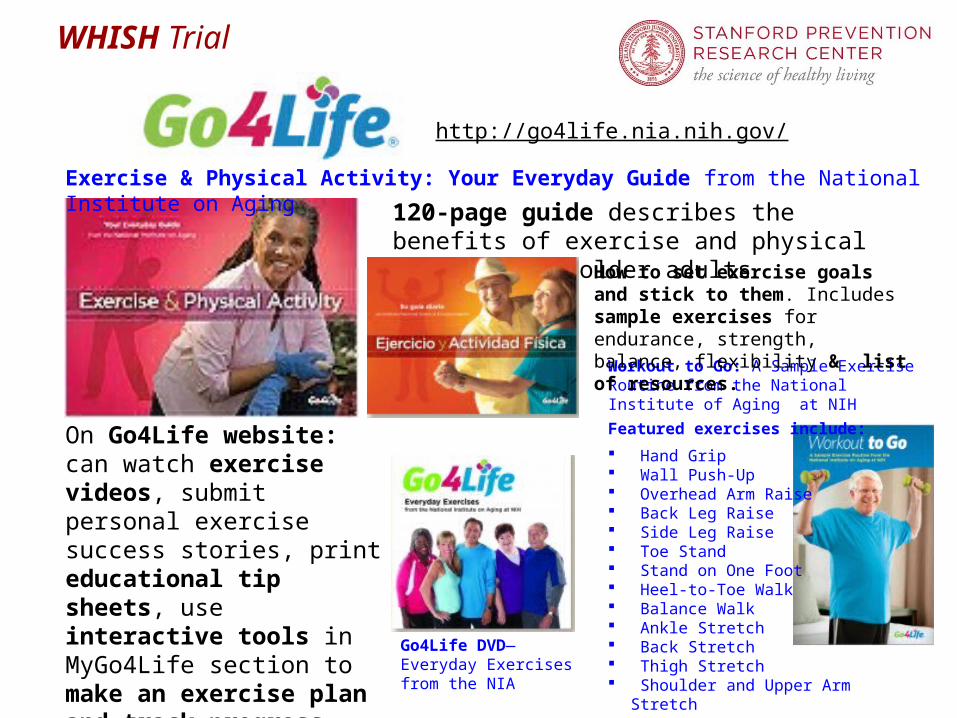
http://go4life.nia.nih.gov/
On Go4Life website: can watch exercise videos, submit personal exercise success stories, print educational tip sheets, use interactive tools in MyGo4Life section to make an exercise plan and track progress over time.
Exercise & Physical Activity: Your Everyday Guide from the National Institute on Aging
120-page guide describes the benefits of exercise and physical activity for older adults
Workout to Go: A Sample Exercise Routine from the National Institute of Aging at NIH
Featured exercises include:
Hand Grip Wall Push-Up Overhead Arm Raise Back Leg Raise Side Leg Raise Toe Stand Stand on One Foot Heel-to-Toe Walk Balance Walk Ankle Stretch Back Stretch Thigh Stretch Shoulder and Upper Arm Stretch
Go4Life DVD—Everyday Exercises from the NIA
How to set exercise goals and stick to them. Includes sample exercises for endurance, strength, balance, flexibility & list of resources.
WHISH Trial
Background: The use of interactive voice response (IVR)
technology for healthcare applications and for medical and psychological research is growing.
Health-related IVR examples include:Follow up of patients after hospital dischargePeer support to patients with chronic heart failureIncrease of medication adherenceWeight loss promotion in pre-diabetic patientsPhysical activity in older adults (CHAT, King et al, 2007)
Physical activity in WHI participants – WHISH pilot
WHISH Trial
218 Community-dwelling Under-activeAdults ages ≥ 55 yrs, randomized to:
Community Health Advice by Telephone:CHAT Project
Telephone Advice by (IVR)
COMPUTER
Attention-Control
arm
Telephone Advice by
HUMAN
Assessments at 0, 6, 12, & 18 mos.
King, Friedman, Marcus, et al., Health Educ Res, 2002
WHISH Trial
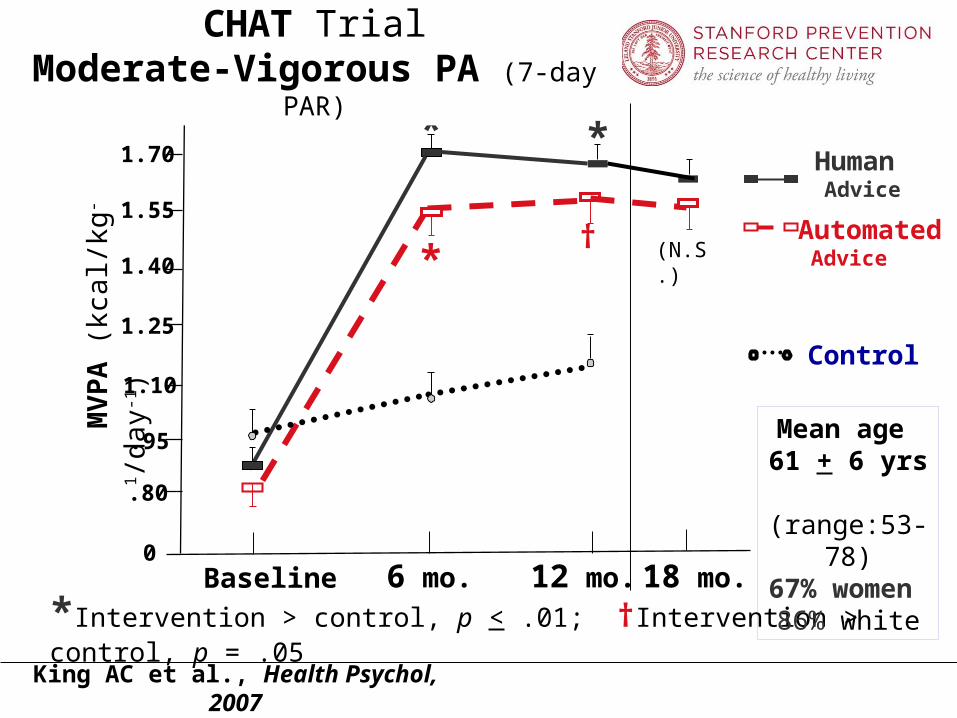
MV
PA
(kc
al/k
g-1/d
ay-1)
Baseline 6 mo. 12 mo.
*Intervention > control, p < .01; †Intervention > control, p = .05
0
.80
.95
1.10
1.25
1.40
1.55
1.70
1.85
*
Control
Automated Advice
Human Advice
†
CHAT TrialModerate-Vigorous PA (7-day PAR)
*
*
King AC et al., Health Psychol, 2007
18 mo.
(N.S.)
Mean age 61 + 6 yrs
(range:53-78)67% women
86% white
WHISH Trial
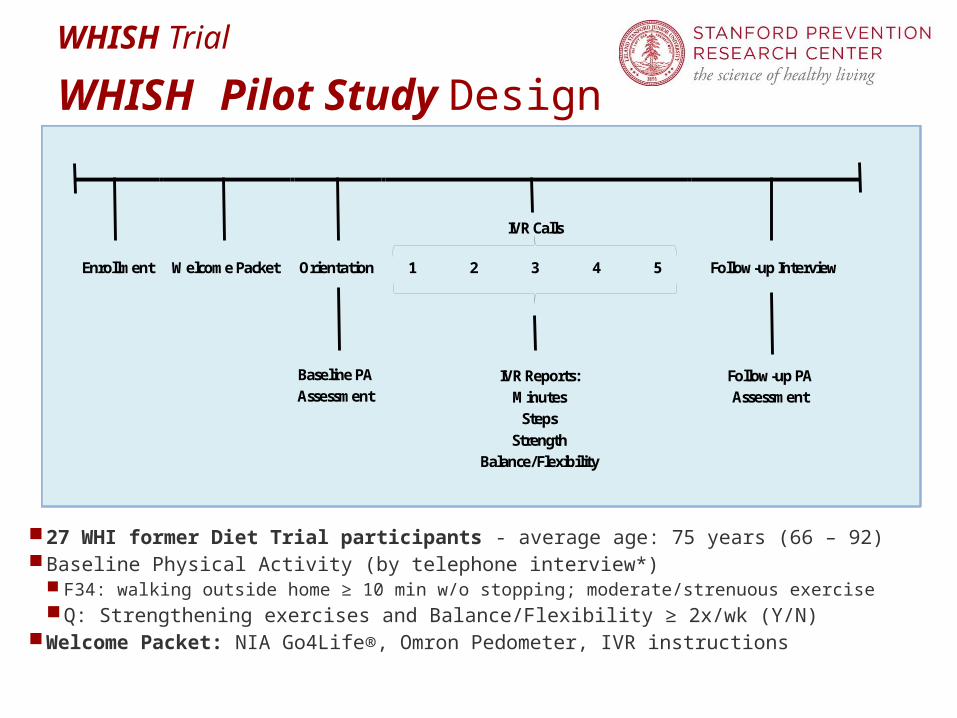
WHISH Pilot Study Design
Baseline PA Assessment
IVR Reports: Minutes
Steps Strength
Balance/Flexibility
Follow-up PA Assessment
IVR Calls
Enrollment Welcome Packet Orientation 1 2 3 4 5 Follow-up Interview
27 WHI former Diet Trial participants - average age: 75 years (66 – 92)Baseline Physical Activity (by telephone interview*)
F34: walking outside home ≥ 10 min w/o stopping; moderate/strenuous exerciseQ: Strengthening exercises and Balance/Flexibility ≥ 2x/wk (Y/N)
Welcome Packet: NIA Go4Life®, Omron Pedometer, IVR instructions
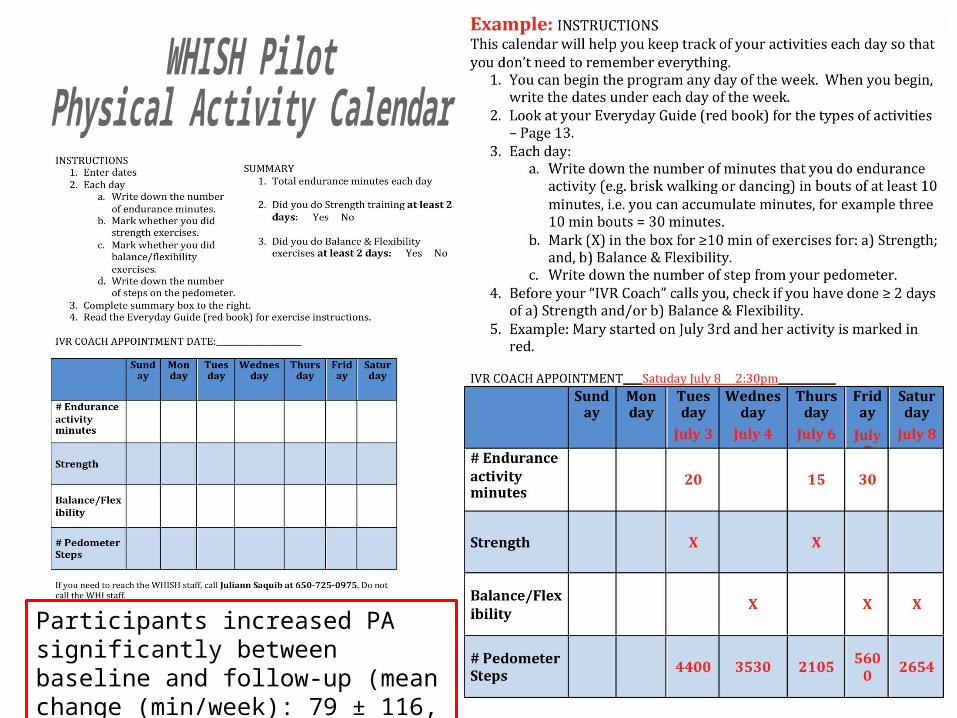
Participants increased PA significantly between baseline and follow-up (mean change (min/week): 79 ± 116, p<.001).
WHISH Trial
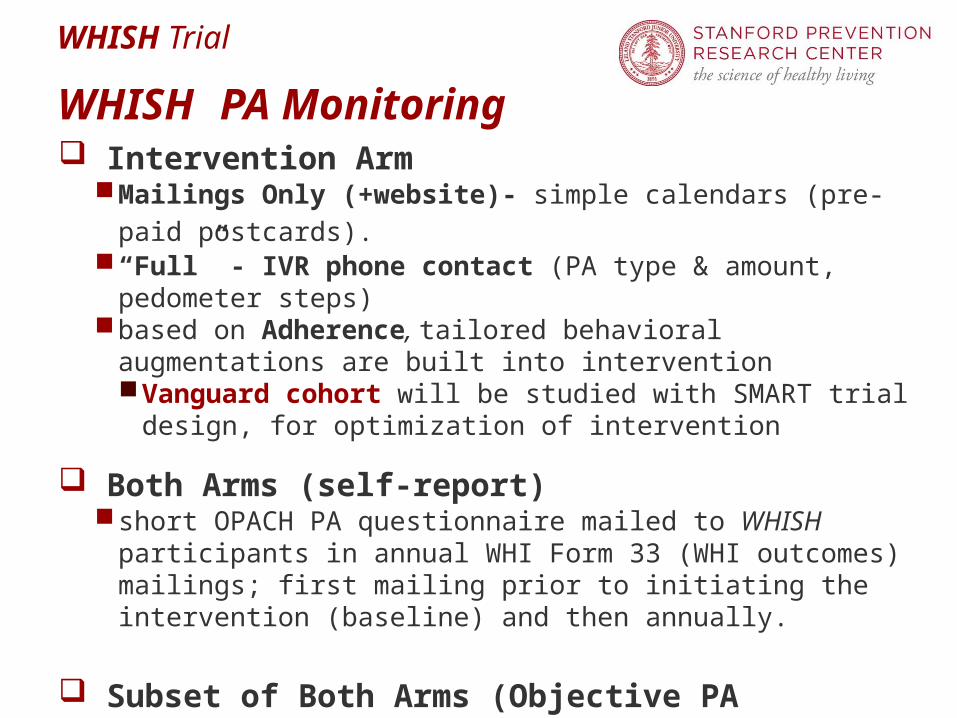
WHISH PA Monitoring Intervention Arm
Mailings Only (+website)- simple calendars (pre-paid postcards). “Full” - IVR phone contact (PA type & amount, pedometer steps)based on Adherence, tailored behavioral augmentations are built
into interventionVanguard cohort will be studied with SMART trial design, for
optimization of intervention
Both Arms (self-report) short OPACH PA questionnaire mailed to WHISH participants in
annual WHI Form 33 (WHI outcomes) mailings; first mailing prior to initiating the intervention (baseline) and then annually.
Subset of Both Arms (Objective PA Monitoring) ~1000 from each arm, randomly selected among OPACH/WHISH
participants for 7-day accelerometry (B, 6-, 18- and 24-months)
WHISH Trial
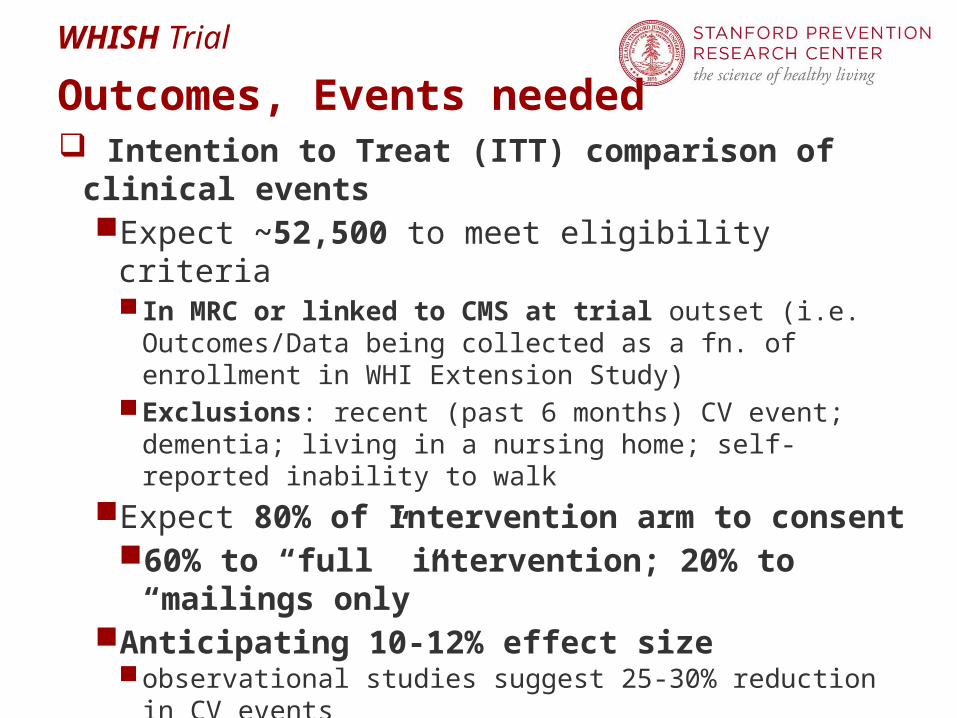
Outcomes, Events needed Intention to Treat (ITT) comparison of clinical events
Expect ~52,500 to meet eligibility criteria In MRC or linked to CMS at trial outset (i.e. Outcomes/Data
being collected as a fn. of enrollment in WHI Extension Study)Exclusions: recent (past 6 months) CV event; dementia; living in
a nursing home; self-reported inability to walk
Expect 80% of Intervention arm to consent 60% to “full” intervention; 20% to “mailings only”
Anticipating 10-12% effect size observational studies suggest 25-30% reduction in CV events
WHI: currently observed annualized rates: 0.90%/yr, suggests a ~ 4 year follow-up is needed
WHISH Trial
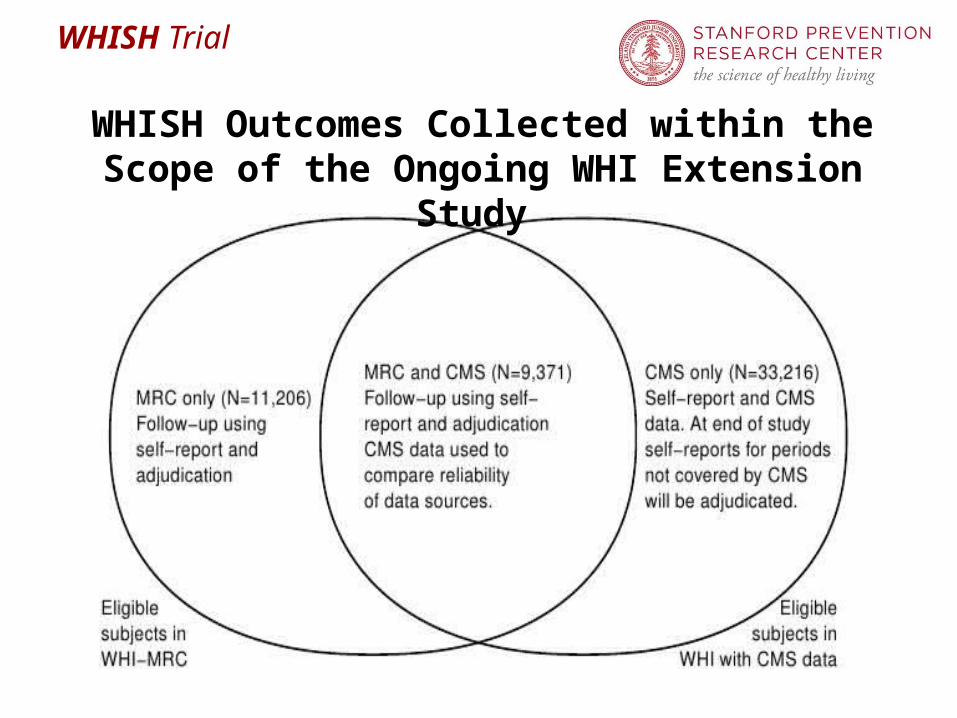
WHISH Outcomes Collected within the Scope of the Ongoing WHI Extension Study
WHISH Trial
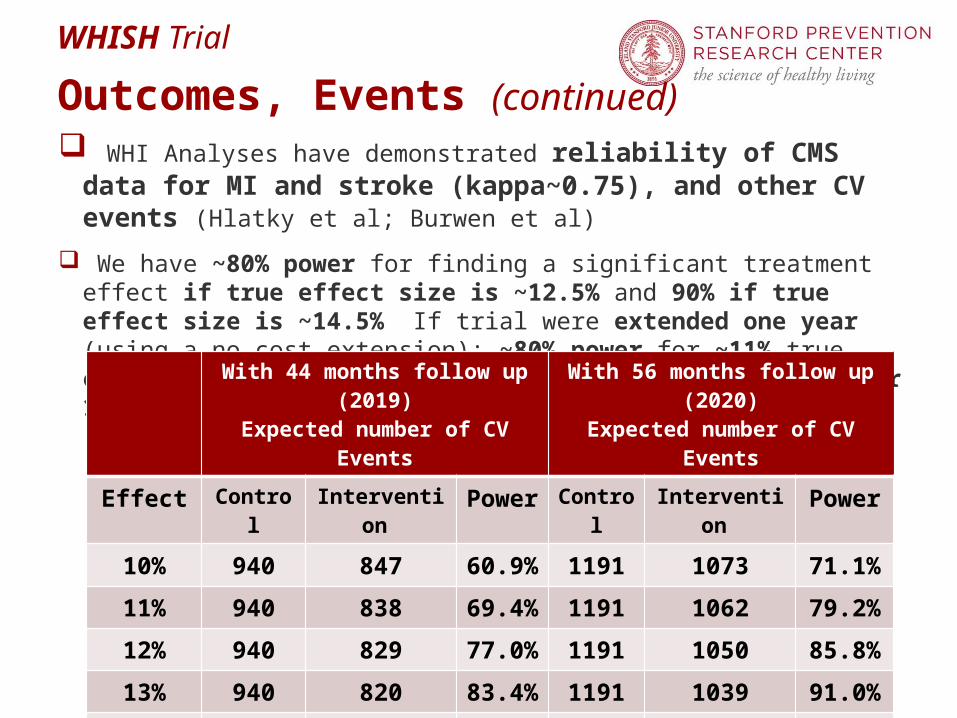
Outcomes, Events (continued) WHI Analyses have demonstrated reliability of CMS data for MI and
stroke (kappa~0.75), and other CV events (Hlatky et al; Burwen et al)
We have ~80% power for finding a significant treatment effect if true effect size is ~12.5% and 90% if true effect size is ~14.5% If trial were extended one year (using a no cost extension): ~80% power for ~11% true effect size, and 90% if the effect size is a little under 13%.
With 44 months follow up (2019)
Expected number of CV Events
With 56 months follow up (2020)
Expected number of CV Events
Effect Control
Intervention
Power
Control
Intervention
Power
10% 940 847 60.9%
1191 1073 71.1%
11% 940 838 69.4%
1191 1062 79.2%
12% 940 829 77.0%
1191 1050 85.8%
13% 940 820 83.4%
1191 1039 91.0%
14% 940 810 88.6%
1191 1027 94.5%
15% 940 801 92.5%
1191 1015 96.9%
WHISH Trial
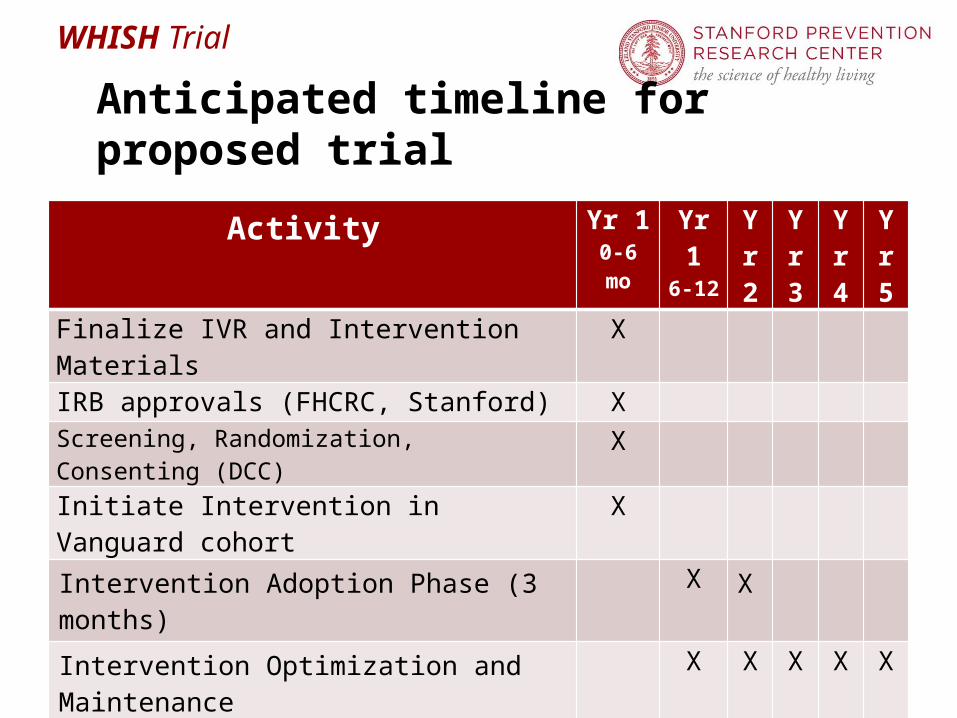
Anticipated timeline for proposed trial
Activity Yr 10-6 mo
Yr 16-12
Yr 2
Yr 3
Yr 4
Yr 5
Finalize IVR and Intervention Materials X
IRB approvals (FHCRC, Stanford) X Screening, Randomization, Consenting (DCC) X
Initiate Intervention in Vanguard cohort X
Intervention Adoption Phase (3 months) X X
Intervention Optimization and Maintenance X X X X X
Study closeout X
Analyses/publication of final manuscripts X