Embed Size (px)
Citation preview

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2014
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1008
Physical Activity and Alzheimer's Disease
Measurements, Observations and Subjective Experiences
YLVA CEDERVALL
ISSN 1651-6206ISBN 978-91-554-8967-0urn:nbn:se:uu:diva-223687

Dissertation presented at Uppsala University to be publicly examined in Gunnesalen,Akademiska sjukhuset ing 10, Uppsala, Friday, 13 June 2014 at 13:00 for the degree ofDoctor of Philosophy (Faculty of Medicine). The examination will be conducted in Swedish.Faculty examiner: Professor Per-Olof Sandman (Karolinska institutet, Institutionen förNeurobiologi, Vårdvetenskap och Samhälle: Umeå Universitet, Institutionen för omvårdnad).
AbstractCedervall, Y. 2014. Physical Activity and Alzheimer's Disease. Measurements, Observationsand Subjective Experiences. Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1008. 82 pp. Uppsala: Acta Universitatis Upsaliensis.ISBN 978-91-554-8967-0.
Gait disturbances such as slow walking speed and step-to-step variability have been reportedamong people with mild Alzheimer’s disease (AD) and as risk factors for functional decline,dependency, and falls. Additionally, AD-related emotional reactions and decreased initiativecan lead to physical inactivity. The aims of this thesis, therefore, were to explore how the abilityto be physically active is affected in the early years of AD, and how people with mild AD andtheir cohabitants reason about physical activity as part of their everyday life.
To meet the aims, an approach inspired by mixed methods research was used, coveringmeasurements, observations and subjective experiences. Data were collected from differentsources in parallel. Participants with mild AD were recruited at the Memory Clinic, UppsalaUniversity Hospital. In Study I, a case study with two couples in which one member hadAD, in-depth interviews and participating interviews were performed. Physical activity such aswalking was viewed as a meaningful routine improving well-being. Participants were positiveabout making adjustments to enable physical activity. In Study II, the 25 participants withAD showed a significant lower walking capacity (10 m comfortable walk test, 6-minute walktest, Timed-up-and-Go test) at baseline compared to controls. The decline continued duringthe subsequent two years. The influence of a cognitive task on walking was distinct, despitethis, participants maintained a health-promoting level of physical activity during the two-yearstudy-period. In Study III, gait testing in the motor laboratory of 21 participants with ADshowed a marked impact on gait parameters (e.g. slowed speed, decreased step length) by acognitive task. Additionally, specific dual-task gait disturbances were frequent. In Study IV,in-depth interviews with 14 participants with AD indicated that physical activity was viewedas a meaningful activity, used as a means to maintain well-being and selfhood, and contributedto continuity in life.
In conclusion, walking capacity deteriorates and declines in the early stages of AD. A simplecognitive task can have a substantially negative impact on walking already in mild AD. Incontrast, people with AD can also gain “self-promoting benefits” from physical activity beyondthe common health-promoting benefits.
Keywords: Caregiver, continuity theory, dementia, dual-task, gait analysis, in-depth interview,mixed methods research, participant observation, physical capacity, qualitative, selfhood,walking
Ylva Cedervall, Department of Public Health and Caring Sciences, Geriatrics, Box 609,Uppsala University, SE-75125 Uppsala, Sweden.
© Ylva Cedervall 2014
ISSN 1651-6206ISBN 978-91-554-8967-0urn:nbn:se:uu:diva-223687 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-223687)

Att röra sig är en nödvändig ingrediens i tillvaron
En deltagare


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals (I-IV).
I Cedervall Y, Åberg AC. Physical activity and implications on well-being in mild Alzheimer’s disease: A qualitative case study on two men with dementia and their spouses. Physiother Theory Pract, 2010;26:226-39.
II Cedervall Y, Kilander L, Åberg AC. Declining walking capaci-
ty, but maintained aerobic activity in early Alzheimer’s disease. Am J Alzheimers Dis Other Demen, 2012;27:180-7.
III Cedervall Y, Halvorsen K, Åberg AC. A longitudinal study of
gait function and characteristics of gait disturbances in individ-uals with Alzheimer’s disease. Gait and Posture 2014;39:1022-27.
IV Cedervall Y, Torres S, Åberg AC. Maintained well-being and selfhood through physical activity: the meanings that people with Alzheimer’s disease attach to being active. Submitted
Reprints were made with the kind permission from the publishers.


Contents
Preface ............................................................................................................ 9
Abbreviations and definitions ....................................................................... 11
Introduction ................................................................................................... 15 Alzheimer’s disease ............................................................................. 15 Physical activity ................................................................................... 16
Aims .............................................................................................................. 22
Methods ........................................................................................................ 23 Theoretical perspectives ...................................................................... 25 Ethical considerations .......................................................................... 27 Participants .......................................................................................... 28 Data collection and analysis ................................................................ 32
Results ........................................................................................................... 38 Study I - A qualitative case study ........................................................ 38 Study II – Clinical measurements and observations ............................ 39 Study III – Laboratory-based gait measures and observations ............ 40 Study IV - Subjective experiences of physical activity in individuals with AD ............................................................................................... 44
Methodological considerations ..................................................................... 46 Sampling .............................................................................................. 46 Data collection ..................................................................................... 47 Analyses ............................................................................................... 50 Trustworthiness ................................................................................... 51 Mixed methods .................................................................................... 52
General discussion ........................................................................................ 53 Physical activity capacity and performance ......................................... 53 Activity-promoting factors .................................................................. 56 Selfhood maintenance through physical activity ................................. 59
Main conclusions .......................................................................................... 62

Clinical reflections ........................................................................................ 63 Can we use performance-based tests? ................................................. 63 Physical activity as a means to self-promotion .................................... 64
Sammanfattning på svenska (Summary in Swedish) .................................... 66
Acknowledgements ....................................................................................... 69
References ..................................................................................................... 72
Appendix ....................................................................................................... 82

9
Preface
This thesis has its origin in my experiences as a physiotherapist at the Memory Clinic at the Uppsala University Hospital. Many of the patients and relatives I met asked me for advice about physical activity because they had the intention to face the symptoms and consequences of the cognitive im-pairments with, to some extent, physical activity and exercises. I asked my-self; why do they strive to continue being physically active? Does physical activity have a certain meaning for them that I do not fully understand?
At that time, research had just started to draw attention to the fact that in-dividuals with mild Alzheimer’s disease, in addition to cognitive impair-ments, show gait impairments and have a lower physical activity level than cognitively healthy individuals (Camicioli et al., 1997; Pettersson et al., 2002). These findings were new and particularly interesting from a physio-therapist’s point of view. Would it be possible to prevent gait impairments that occurred early in the course of Alzheimer’s disease by physiotherapy interventions? I realized that I needed to learn more about the individuals’ personal experiences of physical activity, and the challenges they had to deal with in their daily life to remain physically active. What could I, as a physio-therapist, do to support them? These very first thoughts provided the basis for the qualitative case study and later on for the longitudinal project from which this thesis has emerged. My driving force was a wish to examine if physical activity can reinforce well-being and health for people living with Alzheimer’s disease. I do hope that this piece of research will improve the understanding of their prerequisites and challenges, and contribute to a better everyday life for those living with Alzheimer’s disease.


11
Abbreviations and definitions
AD FAST ICF MCI
Alzheimer’s disease Functional Assessment Staging International Classification of Functioning Disabilityand Health Mild Cognitive Impairments
MMSE Mini-Mental State Examination TUG Timed Up-and-Go test WHO World Health Organization
The concepts used in this thesis are based on the terminology outlined in the International Classification of Functioning Disability and Health (ICF) (WHO, 2008). The definitions displayed below are based on the ICF if not otherwise stated.
The overall aim of the ICF is “to provide a unified and standard language and framework for the description of health and health-related states” (WHO, 2008). It also provides a general thought model to organize thoughts and important information about the individuals’ physical, psychological, and social functioning in the environment (Pless et al., 2011).
According to the ICF, functioning and disability include components of body function and body structure, activity and participating, as well as envi-ronmental and personal factors (Figure 1). A individual’s functioning stands for the positive aspects of the interaction between a person (with specific health conditions) and environmental and personal factors. Disability de-scribes the negative aspects (loss of functioning).

12
Figure 1. Interactions between the components of ICF
Definitions of concepts Activity
The execution of a task or an action, for example walking.
Aerobic activity
Type of physical activity in which large muscles move in a rhythmic manner for a sustained period of time. Maintain/improves cardiorespiratory fitness (Nelson et al., 2007; WHO, 2010).
Attention functions
The cognitive function of being able to focus during a required period of time, also includes the ability divide attention between two tasks. Part of “Specific mental functions” in ICF.
Capacity
The highest level of functioning that a person can reach in a domain in the Activities and Participating list in the ICF at a given moment. Capacity is meas-ured in a uniform or standard environment.
Cognitive functions
The ability to process thoughts (e.g. memory, lan-guage, calculation, executive function) (APA, 2000; McKhann et al., 2011). Part of “Specific mental
Activities
Health condition(disorder or disease)
ParticipationBody Functionsand Structures
Personal Factors
EnvironmentalFactors

13
functions” in ICF. Disability
An umbrella term for impairments, activity limita-tions and participation restrictions.
Dual-task cost
The percentage time difference between only walk-ing and walking when simultaneously performing a concurrent cognitive task (i.e. naming animals).
Dual-tasking
Performance of two tasks simultaneously. In this thesis, walking was considered the primary task and the cognitive tasks (i.e. naming animals) were the secondary tasks.
Environmental factors
Constitute the physical, social, and attitudinal envi-ronments in which people live.
Executive functions
The cognitive function of decision making, abstract thinking, mental flexibility, planning and carrying out plans (i.e. higher-level cognitive functions), Part of “Specific mental functions” in ICF.
Exercise
A subcategory of physical activity that is planned, structured, repetitive and has the purpose to maintain or improve physical fitness (Caspersen et al., 1985; WHO, 2010).
Functioning
An umbrella term for body function and body struc-tures, activities and participation.
Gait
Any method of locomotion characterized by periods of loading and unloading the lower limbs (Kirtley, 2009). Here used to describe gait patterns and com-ponents that make up gait in the motor laboratory setting (Study III).
Mental functions
A body function domain in ICF, which includes the functions of the brain, both global mental functions (e.g. consciousness) and specific mental functions (i.e. cognitive functions).
Mild Cognitive Impairment
A decline in memory and/or other cognitive func-tion, which is notable for the patient and evident on testing, but not severe enough to interfere with ac-tivities in daily life (Winblad et al., 2004).
Participating Involvement in a life situation. Performance
Activities performed in a person’s ordinary envi-ronment.
Personhood
Defined by Kitwood (1997) as “The standard or status that is bestowed upon a human being, by oth-ers, in the context of relationship and social being”. The concept of Personhood is the base of person-

14
centred research and care in the area of dementia (O'Connor et al., 2007; SBU, 2008a). According to Harré (1998) the concept “person” describes the physical existence of a human being.
Physical activity
Any bodily movement produced by skeletal muscles that result in energy expenditure (Caspersen et al., 1985; WHO, 2010). Here mainly used when refer-ring to gait/walking and health promoting physical activity, in which a certain intensity and duration is central (i.e. health-enhancing physical activity, lei-sure time physical activity, recreational time physi-cal activity, habitual physical activity, aerobic ac-tivity).
Selfhood
According to Harré (1998), selfhood is not an entity, rather a “site”, which is viewed to comprise three aspects of self (the self of personal identity, the self of physical and mental attributes, and the self of social roles).
Single-tasking
In this thesis, used to describe a walking task per-formed without a simultaneously cognitive task.
Walking
Gait when one foot is always on the ground, put into context and purposeful action .
Walking capacity
Performance during clinical measurements of walk-ing.
Well-being
A general term encompassing the total universe of human life, including physical, mental and social aspects.

15
Introduction
In recent years research has demonstrated that individuals in the early stages of Alzheimer’s Disease (AD), in addition to cognitive impairments, have gait disturbances such as greater step-to-step variability (Eggermont et al., 2010; Wittwer et al., 2008), which increases the risk of future falls and de-pendence (Gleason et al., 2009; Hausdorff, 2005). A suggested explanation for the gait disturbances is that walking in real life requires well-functioning executive and attention functions (Sheridan et al., 2007; Shumway-Cook et al., 2012). These cognitive functions are often affected in AD (Hausdorff et al., 2005; Snijders et al., 2007; Yogev-Seligmann et al., 2008). In addition, decreased initiation of activities, and emotional reactions, for example social withdrawal and anxiety, are common (Cook et al., 2008). This can compli-cate participation in organized exercises, as well as the maintenance of a health-promoting level of physical activity (SoS, 2012).
A low physical activity level has been reported among people with mild AD (Burns et al., 2008; Pettersson et al., 2002), which may affect body func-tion, as well as mood, behaviour, cognitive function, and dependency (Blankevoort et al., 2010; Heyn et al., 2004). It is, however, unclear which factors individuals with AD perceive as barriers towards physical activity, and what meaning physical activity plays in everyday life for them and for their cohabitants (Lautenschlager et al., 2010).
It is therefore essential to explore these aspects of physical activity among people in the early stages of AD. By using clinical and laboratory measure-ments and observations of walking under different circumstances it may be possible to identify relevant early changes in walking ability. Moreover, complementing such data with the subjective experiences of individuals with AD and their cohabitants, adds an important understanding of which factors that limits, and facilitates people with AD to maintain physical activity.
Alzheimer’s disease Alzheimer’s disease is a progressive neurodegenerative disease and accounts for about 60% of dementia cases. The prevalence of AD is expected to rise because of the growing number of older people in the population. The main risk factors for AD are old age and genetic factors. The general age of onset is 65 or older, but the neurodegenerative process starts many years before the

16
individual is able to notice any cognitive impairment (Basun et al., 2013; SBU, 2008b).
The dementia syndrome is defined as a decline of cognitive function from a previously higher level, severe enough to interfere with activities of daily living, and persisting for more than six months. Worsening of memory is a core symptom along with decline of at least one more cognitive function, such as thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. (APA, 2000; McKhann et al., 2011). In addition, executive and attention functions are commonly affected. There is, however, a wide individual variation in symptoms and progression, and survival time from diagnosis varies from 2 to 20 years (Basun et al., 2013; SBU, 2008b).
During the initial years following the onset of AD, symptoms are com-monly mild. This stage of the disease is therefore often referred to as mild AD. At this early stage, individuals have trouble with instrumental activities of daily living such as paying bills and handling medication. The need for assistance in everyday life increases gradually when the disease progresses. At the moderate stage of AD, memory loss has worsened and the person requires help to cope with personal care. At the severe stage, the person gradually loses their gait ability, communication, and needs help with all personal care including feeding (Basun et al., 2013; SBU, 2008b).
Physical activity
Physical activity as health promotion Regularly performed physical activity is an important factor to promote health in the population (FYSS, 2008). The American College of Sports Medicine, the American Heart Association (Nelson et al., 2007), and the World Health Organization (WHO) (2010) have published specific public health recommendations in relation to physical activity. The recommenda-tions in focus comprise physical activity recommendations for adults older than 65 years and recommendations for people aged 50-64, with clinically significant chronic conditions or functional limitations that affect movement abilities. These health recommendations include aerobic-, muscle strength-, flexibility- and balance activities, but here we will focus on the aerobic ac-tivity recommendations.
In order to improve health, a minimum of 30 minutes aerobic activity of moderate intensity in bouts of at least 10 minutes are recommended to occur five days a week. This is in addition to the light intensity routine activities performed in daily life. Moderate intensity aerobic activities raise the heart-beat to 55-70% of maximum heart rate and leaves the person feeling warm and slightly out of breath. Among older individuals, the intensity level should be relative to a person’s aerobic fitness (Nelson et al., 2007).

17
In health promotion a range of concepts related to physical activity is used (see Abbreviations and definitions). They all describe activities that are not essential for daily living, but produce health benefits for individuals when performed at a moderate intensity (e.g. walking, bicycling, swimming and gardening) (FYSS, 2008; Nelson et al., 2007).
Walking is the most common habitual physical activity among the Swe-dish population. Factors which contribute to higher physical activity levels are a high education level and a distance of less than one kilometre from the housing to green spaces (FHI, 2010). Recreational physical activities in natu-ral surroundings are appreciated among the Swedish population and it has been proposed that the reason for the positive experiences of being in nature (e.g. when going for a walk in the woods) is that it provides relaxation (Daun et al., 1996), restorative experiences (Kaplan, 1995; Korpela et al., 2001), and improves well-being (Bowler et al., 2010).
Additionally, aerobic activity on a health promoting level has been high-lighted in recent years as a non-pharmacological treatment that can have a positive effect on the brain structure and function in older adults (Tseng et al., 2011). This was shown for example by Colcombe et al. (2006) who con-ducted a randomized clinical trial in which sedentary elderly people partici-pated in an aerobic training group for a one-hour period, three times a week, while the control group was engaged in stretching. After six months of aero-bic exercise, the participants had improved cardiorespiratory fitness, and the brain volume had increased, mainly in the prefrontal and the temporal corti-ces. In line with these results Erickson et al. (2011) reported that after six months of aerobic exercise on a moderate level hippocampal size increased, and spatial memory improved. These results suggest a biological base for the role of aerobic fitness in enhancing brain health and cognitive function in elderly people. Thus, these results imply that aerobic exercise is a promising non-pharmacological treatment in preventing age-related cognitive decline. Similarly, physical activity may be beneficial for brain health in individuals with mild cognitive impairment (MCI) (Ten Brinke et al., 2014) and demen-tia (Bherer et al., 2013; Intlekofer et al., 2012), and for enhancing emotional function in older people (Erickson et al., 2013). However, it is unclear what types of exercises, and the intensity and duration that are most effective in improving cognitive and emotional functions in elderly individuals (Lauten-schlager et al., 2010).
Physical activity and Alzheimer’s disease People with AD are covered by the same public health recommendations as the rest of the population and it is plausible that individuals with AD achieve health benefits from physical activity (SoS, 2010). Previously, improvements in ability to perform daily activities (Forbes et al., 2013), physical functioning (Blankevoort et al., 2010; Heyn et al., 2004), possibly also

18
cognitive function (Forbes et al., 2013) and a reduction in the number of falls have been reported among people with AD (Pitkala et al., 2013). Additional-ly, a higher level of physical activity has been reported to be associated with prolonged survival in AD (Scarmeas et al., 2011).
However, individuals with AD may have difficulties to remain physically active even in the early stages of the disease (Burns et al., 2008; Pettersson et al., 2002). There are several factors related to the dementia diagnosis which may affect the performance of physical activities, for example a de-creased ability to take initiative (Cook et al., 2008), deteriorated attention-, executive- and perceptual functions (including visuospatial perception), and ability to find the way (Basun et al., 2013). Similarly, feelings of anxiety and unease can lead to social withdrawal and increase the risk of inactivity (Beard et al., 2009; Husband, 2000; Phinney, 1998). Each one of these fac-tors mentioned may individually lead to a decline in physical functioning and independence.
Gait disturbances and dual-tasking in Alzheimer’s disease Until the 1990s, AD was perceived as a disease that mainly affected cogni-tive functions, and spared motor functions to its later stages. However, it was known then, that individuals with AD had an increased risk of falls and frac-tures, but the causes were unclear (Buchner et al., 1987). In 1995, Alexander et al. showed that individuals with AD differed from healthy individuals by walking slower and crossing obstacles in their path with less safety. Moreo-ver, Nakamura et al. (1996) reported that gait disturbances increased with the severity of dementia and that a decrease of step length appeared to be a pre-dictor for falls. It was hypothesized that an impaired ability to perform two tasks simultaneously (i.e. dual-tasking) could explain why people with AD fell under certain circumstances. Therefore, Camicioli et al. (1997) conduct-ed a study in which they combined a cognitive task (i.e. naming names) with walking five metres back and forth (the “Talking-While-Walking” test). They found that people with AD slowed more than cognitively intact people during the dual-task walk. This study was followed by others that confirmed these early findings, e.g. Pettersson et al. (2005, 2007).
A corner stone in understanding the relation between cognition and gait was the findings reported by Lundin et al. in 1997. They found that an ina-bility to hold an informal conversation when walking (“Stops-walking-while-talking”) was a predictor for future falls among elderly people. These findings underscored that cognitive function and ability to walk is interrelat-ed and indicated that impaired cognitive function can increase the risk of falls (Gleason et al. 2009).
Today, it is established that people with mild AD have an impaired walk-ing capacity, such as slower gait speed, shorter step length and increased step-to-step variability compared to cognitively healthy individuals (e.g.

19
Wittwer et al., 2008). Walking capacity continues to deteriorate as the de-mentia progresses and a significant decline has been reported during a period of only one year (Tangen et al., 2012; Wittwer et al., 2010). In addition, the described gait disturbances are accentuated during dual-task conditions among individuals with mild AD (Allali et al., 2008; Ijmker et al., 2011; Maquet et al., 2010; Muir et al., 2011), but longitudinal studies investigating dual-task ability in the early stages of AD have not been found in the litera-ture.
Executive and attention functions have been found to play a central role in the ability to walk safely and stably in everyday life (Allali et al., 2008; Hausdorff et al., 2005; Sheridan et al., 2007; Yogev-Seligmann et al., 2008). In agreement with this a lower executive function performance on the pen-and-paper test was reported to be associated with slow usual gait speed in people with MCI (McGough et al., 2011). When walking in real life, there is a constant need to adapt to environmental factors such as curbs, uneven sur-faces, and rapidly evolving situations (e.g. cars, busses, and other people). These environmental factors altogether put high demands on the ability to make quick decisions, carry out plans, and divide and shift attention etc. As executive and attention functions are often affected in the early stages of AD, impairments of these functions have been suggested to explain reported instability and the increased fall risk among people with AD. In addition, recent research indicates that people with AD have problems to merge de-tails into a meaningful whole. They may therefore receive a slightly frag-mentary picture of their environment (Mårdh, 2013). There are, however, conflicting findings as to whether an impaired dual-task ability when walk-ing, is associated with falling or not among older people (Beauchet et al., 2009).
Research over recent years has therefore been focused on investigating dual-task ability when walking. Different methods have been used to meas-ure the impact of a concurrent cognitive task on walking. As mentioned be-fore, Camicioli et al. (1997) combined walking back and forth with a quite simple cognitive task (naming names). In laboratory settings, walking straight has often been used in combination with a more complex cognitive task such as counting backwards (Allali et al., 2008). Accordingly, the com-bination of a more complex motor task, such as the Timed Up-and-Go-Test, with a cognitive task has also been suggested (Horak et al., 2009).
The Timed Up-and-Go test (TUG) (Podsiadlo et al., 1991) is a well-established test for measuring basic mobility. Time is recorded when an in-dividual completes the following sequence: starts from a seated position, stands up, walks three metres, turns around, walks back, and sits down. The mobility sequence is often performed at a comfortable (usual) walking speed. The TUG test combined with either a manual task (carrying a cup of water) or a cognitive task (subtractions), were equal in predicting older peo-

20
ple who were prone to fall (Shumway-Cook et al., 2000), but the manual task has been more frequently used in the clinical setting. Appealing factors about using the TUG test for assessing dual-tasking are that it is well known, easy to administer and requires little time, and is reliable for individuals with AD (Ries et al., 2009). Additionally, as the mobility component is complex the cognitive task may not have to be too challenging for a person with cog-nitive impairments to expose dual-task impairments.
Physical activity in daily living with AD The cohabitants of community-dwelling people at a mild stage of AD are often responsible for a large portion of informal care (Gruffydd et al., 2006; SoS, 2010; WHO, 2012). This often includes support and prompting of ha-bitual physical activities such as walks (Cook et al., 2008; Jansson et al., 2001; McCurry et al., 2011). One would presume that assistance of this kind would increase the caregiver burden. However, there are indications that informal caregivers view regular physical activity for their partner with AD as a meaningful and important activity (Jansson et al., 2001; Pitkala et al., 2010). Informal caregivers whose partners participated in a six-month exer-cise programme reduced their caregiver burden in comparison to a control group (Canonici et al., 2012). In the same way, caregivers of a partner with AD participating in a four-month home-based exercise programme reported less stress, despite the fact that the caregivers supervised the daily exercises (Vreugdenhil et al., 2012). Thus, involvement in structured physical activi-ties may be beneficial not only for the person with AD, but also for the in-formal caregiver (Yu et al., 2013).
Subjective experiences of physical activity from the perspective of indi-viduals with AD and cohabitants have rarely been evaluated in research. In an interview study, Malthouse et al. (2013) found that community-dwelling individuals with AD appreciated exercises, but preferred to perform activi-ties in their home environments, indicating that individual tailored physical exercises might be preferable for this group. In that study, caregivers acted as facilitators of activities, but also as gatekeepers to protect the partner from activities that might be experienced as too stressful. In other studies, prefer-ences for outdoor activities (e.g. walks and gardening), have been empha-sized, not only for individuals’ needs, but also for interactions between peo-ple with dementia and their informal caregivers (Gibson, 2007). Being phys-ically active outdoors was reported to be appreciated for confirming the abil-ity to maintain desired activities (Olsson et al., 2013), enjoyment, exercise, fresh air and emotional well-being (Duggan et al., 2008). Interactions with neighbours were another positive factor that participants in both these stud-ies mentioned in association with being outdoors.

21
Currently, there is insufficient knowledge about the impact of AD on the ability to remain physically active in everyday life and we also do not fully know the views of physical activity of those concerned.

22
Aims
This thesis has for its focus physical activity among individuals in the early stages of Alzheimer’s disease. The overall aims were to explore how the ability to be physically active is affected in the early stages of AD, and how people with mild AD and their cohabitants reason about physical activity as part of everyday life.
Specific aims of the Studies I, II, III and IV were to:
I. Improve the understanding of experiences regarding ability to be
physically active from the perspective of individuals with mild AD and their cohabitants.
II. Investigate and describe changes in walking capacity and physical activity levels during a period of two years among individuals who initially had mild AD.
III. Investigate and describe longitudinal changes in gait parameters
under single- and dual-task conditions, during a period of two years among individuals who initially had mild AD.
IV. Further the understanding of how people with mild AD reason about
physical activity, focusing on their ability to be active, and the meaning they attach to physical activity.

23
Methods
This thesis has an exploratory approach, inspired by mixed methods re-search. The first study conducted (Study I), was a qualitative case study in-cluding two couples (Figure 2). In each couple, one party had mild AD. The findings from this first study constituted the basis for planning and conduct-ing a longitudinal project in which measurements, observation data, and data on subjective experiences were collected from individuals with mild AD, and from their cohabitants.
This thesis, comprises the case study (Study I), two longitudinal studies presenting results from measuring and observing aspects of physical activity (Studies II and III), and findings from the baseline interviews with the partic-ipants with mild AD (Study IV) (Figure 2). In the following sections the theoretical perspectives used will be presented.

Fig
ure
2. A
flo
w c
hart
of
data
col
lect
ion
in S
tudi
es I
, II,
III
, and
IV
.
A
D=
part
icip
ants
with
Alz
heim
er’s
dis
ease
, HC
=he
alth
y co
ntro
ls, C
oh=
coha
bita
nts
III
Gai
ta
nal
ysis
AD
, n=2
1
IIC
linic
al
me
asu
res
AD
, n=2
5
II
Clin
ical
m
eas
ure
sH
C, n
=25
III
Gai
ta
nal
ysis
AD
, n=
21
IIC
linic
al
me
asu
res
AD
, n=2
2
III
Gai
tan
alys
isA
D, n
=21
IIC
lin
ical
m
eas
ure
sA
D, n
=22
IVIn
terv
iew
sA
Dn
=14
IC
ase
st
ud
yA
D, n
=2C
oh
, n=2
1-y
ear
fo
llow
-up
Bas
elin
e2
-ye
ar f
ollo
w-u
p

25
Theoretical perspectives
The theoretical base for mixed methods research In order to meet the overall aims focusing on measurements, observations and the participants’ subjective experiences of physical activity in the early stages of AD, an approach inspired by mixed methods research was used in the present work (Johnson et al., 2004). Mixed methods research has been emphasized in recent years as it enables the conduct of research that pro-vides a holistic and multifaceted interpretation of the subject addressed in a research project (Bryman, 2004; Creswell, 2009). Mixed methods research is viewed as both a method (“a doing tool”) and a methodology (“a thinking tool”) and is not committed to any one system of philosophy (Andrew et al., 2009). Epistemologically, mixed methods research has its roots in pragma-tism and, as such it is not bound to traditional viewpoints that research should be performed in the paradigms of either empirical-holistic research traditions or natural sciences (positivism) (Bryman, 2004; Creswell, 2007; Johnson et al., 2004), instead, researchers in mixed methods research believe that epistemological and ontological issues are of minor importance for the research findings and interpretations. They emphasise the research questions and use available methods and procedures to understand the problem under study (Creswell, 2009). In line with this thinking is the viewpoint among some philosophers of sciences that the differences between the two para-digms should not be exaggerated, because traits from one of the paradigms are often used in the other and vice versa (Bryman, 2004; Föllesdal, 1994).
In this thesis, the decision to use an approach inspired by mixed methods research was based on the complexity of the research questions addressed in the project (Andrew et al., 2009; Creswell, 2009; Polit et al., 2008). Thus, to meet the aims of this work, which covered measurements, observations, and subjective experiences of aspects of physical activity, data from different sources were collected separately, but in parallel. The findings and results from Studies I, II, III, and IV are separately reported in the Results section, but interpreted and discussed in an integral manner in the General discussion section (Andrew et al., 2009; Creswell, 2009).
In research, the concept understanding is fundamental, but it has fairly different meanings in the empirical-holistic compared with the positivistic paradigms. Therefore, some clarification is necessary. Within the empirical-holistic paradigm, the concept understand is defined as an insight into the meaning of something (Grön et al., 1988; Trost et al., 2011). The researcher tries to understand the problem from an inner perspective, i.e. from the per-spective of those being studied. Understand in this context comprises a sci-entific interpretation and analysis that is more theoretical than only under-standing something in everyday life. Thus, the concept understand used in

26
the empirical-holistic paradigm is close to the concepts of empathy and meaning.
Understand in the natural sciences, on the other hand, has a slightly dif-ferent meaning. The researcher in the natural science paradigm aims to study the world “objectively”, from an outer perspective. In this context, the con-cept understand is often used to explain an event. Thus, an event is ex-plained (understood) if it is proven to be a consequence of a certain cause (Persson et al., 2012). By explaining a result, the potential cause is de-scribed.
When advocating mixed methods research in a project such as the present one, the results from one of the methods can contribute to understanding the research problem and provide plausible explanations to the findings from the other method (and vice versa) (Bryman, 2004). Additionally, a theoretical framework used to guide the analysis of text data (e.g. from interviews) can help to understand and interpret findings on a more abstract level and may, therefore, contribute to a potential explanation of the findings. Here we have used the Continuity theory (Atchley, 1989; 1999) and Harré’s framework of Selfhood (1998) to interpret the results. These theories will be introduced in the following section.
Selfhood and continuity in dementia Harré’s theoretical framework of Selfhood (1998) has its origin in social constructionism and has been used in several studies involving people with dementia to illuminate manifestations of selfhood (Hedman et al., 2013; Kelly, 2010; Olsson et al., 2013; Sabat, 2002; Sabat et al., 1999). According to this framework, individuals interact with others to construct meaning in life. Selfhood is constructed and reconstructed in an on-going process and, therefore, has implications for how people cope with illness (Caddell et al., 2010).
In this framework, the selfhood is regarded as comprising three aspects of self. To have a sense of self is to be able to express these three aspects of self with its own characteristics. The first form is the self of personal identity, which in speech can be manifested by the use of “I”, “me”, “mine”, “ours” etc. and constitutes the subjective experience of being a person. From this point, individuals can relate to themselves and to others. This form of self has been shown to persist even in the moderate-severe stages of dementia (Caddell et al., 2010). The second form is the self of individuals’ physical and mental attributes and their beliefs about these characteristics (e.g. traits, skills). In contrast to the first form of self, the attributes attached to a person, for example, an ability to do certain activities, and beliefs in those abilities, undergo changes during the course of dementia (Hedman et al., 2013; Olsson et al., 2013). The third form of selfhood is the self of social roles (i.e. social persona) that we construct in varying situations during our lifetimes. It com-prises the different ways people display themselves to others and the way in

27
which others perceive a person. This aspect of selfhood is severely threat-ened when a person is diagnosed with dementia, primarily because of the reactions and behaviour of others (Clare, 2003; Harré, 1998).
Dementia can hence pose a threat to individuals’ different aspects of self-hood (Steeman et al., 2006). People in the early stages of AD have described attempts to balance a wish to maintain a prior (healthy) self, with a need to construct a new (adapted) self because of the impact of dementia (Pearce et al., 2002). The first strategy older adults use when trying to adapt to chang-ing circumstances in life, is often to strive to achieve continuity. According to the Continuity theory developed by Achtley, people adapt by preserving a sense of continuity in internal and external structures (Atchley, 1989; 1999). Continuity of both ideas and lifestyle is hence of key importance. According to this theory, older adults strive to establish an external life situation that supports continuity of their internal ideas of their self and life, despite changes in health and social circumstances. Thus, they can experience conti-nuity and change of selfhood simultaneously (Caddell et al., 2011; Hedman et al., 2013; Åberg et al., 2005).
The framework of Selfhood and the Continuity theory are closely related, as the selfhood of a person provides continuity with the former life at the same time as it is under constantly revision through interactions with others. In the present work, Harré’s framework of Selfhood, was mainly used in the analysis and interpretation of interview findings in Study IV, but also for conducting a comprehensive interpretation of results from all four studies in this thesis in the General discussion and the Clinical reflections sections. The Continuity theory was used to illuminate interview and observation findings as a complement to the framework of Selfhood, and both were adopted for the comprehensive interpretation displayed in the General discussion and the Clinical reflections sections.
Ethical considerations The Regional Ethical Review Board in Uppsala approved the studies in this thesis.
There are ethical issues in research involving people with dementia which have to be considered. One main issue is that an individual with cognitive impairments may have difficulties to give his/her consent to participate based on the given information. Therefore, a range of precautions were taken to ensure that participating would not be experienced as harmful. These will be described in the following paragraph.
In Study I, the physicians at the Memory Clinic at the Uppsala University Hospital identified two potential couples according to the inclusion criteria. Both couples accepted to participate and gave their oral informed consent. During the inclusion process in Studies II and III, a consecutive inclusion was made from patients with AD at the Memory Clinic. Potential partici-

28
pants were identified by a review of the records. The physicians gave their clearance before patients were contacted. At the first phone contact, the po-tential participant and the spouse were briefly informed about the longitudi-nal project. If they accepted, written information was sent to them. A week after the phone contact, they were approached again, additional information was given and a time for inclusion assessment was booked if they accepted. Both participants and spouses were questioned and gave their informed oral and written consent that the person with AD would participate in the study. This was made in order to ensure that participating in the longitudinal study would not increase the caregiver burden or expose the participants to harm.
A purposive selection of participants in Studies II and III was made for inclusion to the interview study (Study IV). Potential participants were con-tacted by phone or in person, and a similar procedure as described above was performed. The participants chose whether the interview would take place in their homes or at the Uppsala University Hospital. All interviews were per-formed in privacy, without the partner being present.
During all test procedures and interviewing, efforts were made to make sure that the participants felt comfortable and relaxed. Before each yearly follow-up, the participants and the spouses were contacted by phone. They were reminded that participation was voluntary and that they could terminate it (if they wished to) without explaining why. If they accepted to continue, a visit time was booked.
Participants All participants with AD were recruited at the Memory Clinic at the Uppsala University Hospital. The AD diagnosis fulfilled the current research criteria of probable AD according to DSM-IV-TR (APA, 2000), and NINCDS-ADRDA (McKhann et al., 1984). The inclusion criteria for the participants with AD were: Mini-Mental State Examination (MMSE) score of 20-30 (Folstein et al., 1975), Functional Assessment Staging (FAST) stage 3 or 4 (indicate “early dementia” and “mild dementia”, respectively) (Reisberg, 1988), age 80 years or younger, and community dwelling with a cohabitant. All participants were capable to walk without a walking aid (Åberg et al., 2003), and had no other illnesses, injuries or pain that substantially affected mobility. An overview of the participants’ characteristics is displayed in Table 1, and an overview over the Studies I, II, III, and IV is displayed in Table 2.

Tab
le 1
. Ove
rvie
w o
f th
e St
udie
s I,
II,
III
, and
IV
.
S
tud
y I
Stu
dy
II
Stu
dy
III
Stu
dy
IV
Mai
n f
ocu
s
Sub
ject
ive
expe
rien
ces
of
peop
le w
ith
AD
and
coh
abit
ants
Cro
ss s
ecti
onal
dif
fere
nces
, and
lo
ngit
udin
al c
hang
es o
f w
alki
ng
capa
city
and
phy
sica
l act
ivit
y le
vels
Lon
gitu
dina
l cha
nges
in g
ait f
unc-
tion
dur
ing
sing
le a
nd d
ual-
task
ing
Sub
ject
ive
expe
rien
ces
of p
eopl
e w
ith
AD
Ap
pro
ach
Q
uali
tati
ve c
ase
stud
y an
d
cros
s se
ctio
nal
Qua
ntit
ativ
e, c
ross
sec
tion
al, a
nd
long
itud
inal
Q
uant
itat
ive
and
long
itud
inal
Q
uali
tati
ve a
nd c
ross
sec
tion
al
Par
tici
pan
ts
Tw
o m
en w
ith
AD
, age
74
and
63
and
thei
r tw
o fe
mal
e sp
ouse
s
25 p
eopl
e w
ith
AD
, age
73
(55-
79),
14
mal
e/11
fem
ale*
25
hea
lthy
con
trol
s, a
ge 7
0 (5
6-79
),
14 m
ale/
11 f
emal
e
21 p
eopl
e w
ith
AD
, age
72
(55-
78),
10
mal
e/11
fem
ale
14 p
eopl
e w
ith
AD
: age
72
(59-
79),
6
mal
e/8
fem
ale
MM
SE
sco
re
Md
(ra
nge
)
AD
: 21
p an
d 22
p
AD
: 25
(21-
30)
p H
ealt
hy c
ontr
ols:
30
(28-
30)
p
AD
: 25
(21-
30)
p A
D: 2
3.5
(21-
30)
p
Dat
a
coll
ecti
on
m
eth
ods
Indi
vidu
al in
-dep
th in
terv
iew
s P
arti
cipa
nt o
bser
vati
ons
Mea
sure
men
ts o
f w
alki
ng c
apac
ity,
ph
ysic
al a
ctiv
ity
leve
l, co
gnit
ive
func
tion
O
bser
vati
ons
of d
ual-
task
wal
king
pe
rfor
man
ce
Rep
orts
of
fall
s
Lab
orat
ory
base
d ga
it a
naly
sis
by a
m
otio
n ca
ptur
e sy
stem
M
easu
rem
ents
of
cogn
itiv
e fu
nc-
tion
Indi
vidu
al in
-dep
th in
terv
iew
s
Dat
a
anal
ysis
m
eth
ods
The
mat
ic a
naly
sis
Des
crip
tive
sta
tist
ics
Non
-par
amet
ric
stat
isti
cs
Bet
wee
n an
d w
ithi
n su
bjec
ts
com
pari
son
Des
crip
tive
sta
tist
ics
Par
amet
ric
stat
isti
cs
Non
-par
amet
ric
stat
isti
cs (
doub
le
supp
ort,
corr
elat
ions
) W
ithi
n su
bjec
ts c
ompa
riso
n V
isua
l exa
min
atio
ns o
f m
otio
n ca
ptur
e fi
les
Qua
lita
tive
con
tent
ana
lysi
s
AD
= A
lzhe
imer
’s D
isea
se,
MM
SE
=M
ini-
Men
tal S
tate
Exa
min
atio
n, *
Dro
p ou
ts in
the
2-ye
ar f
ollo
w-u
p: n
=3

Tab
le 2
. Per
form
ance
bas
ed te
st o
f w
alki
ng c
apac
ity a
nd c
ogni
tive
func
tion.
Mea
sure
men
t R
epor
ted
in S
tud
y D
escr
ipti
on
10 m
com
fort
able
wal
king
te
st (
m/s
)
II, I
V
The
par
ticip
ant s
tart
s fr
om a
sta
ndin
g po
siti
on a
nd w
alks
10
m a
t com
fort
able
wal
king
spe
ed. T
imin
g st
arts
whe
n on
e fo
ot m
oves
in o
rder
to ta
ke a
ste
p, a
nd s
tops
whe
n th
e fi
nish
ing
line
is to
uche
d or
cr
osse
d by
the
lead
ing
foot
.
6-m
inut
e w
alki
ng te
st (
m)
II
The
par
ticip
ant i
s in
stru
cted
to w
alk
back
and
for
th a
long
a 3
0 m
hal
lway
as
far
as p
ossi
ble
duri
ng 6
m
inut
es. I
nfor
mat
ion
is g
iven
whe
n ha
lf-t
ime
has
elap
sed,
whe
n on
e m
inut
e is
left
, and
whe
n si
x m
inut
es h
ave
elap
sed.
Enc
oura
gem
ent i
s gi
ven
once
, aft
er o
ne m
inut
e of
wal
king
.
Tim
ed U
p-an
d-G
o te
st (
s)
II, I
V
The
par
ticip
ant s
its
on a
cha
ir w
ith a
rm r
ests
, and
is in
stru
cted
to w
alk
at h
er/h
is c
omfo
rtab
le s
peed
for
3
met
res,
pas
ses
a ta
pe m
arke
r on
the
floo
r, tu
rns
arou
nd, w
alks
bac
k an
d si
ts d
own.
Tim
ing
star
ts w
hen
the
subj
ect’
s ba
ck le
aves
the
back
of
the
chai
r an
d st
ops
whe
n th
e bo
ttom
touc
hes
the
seat
.
Tim
ed U
p-an
d-G
o du
al-
task
test
(s)
II, I
V
The
par
tici
pant
per
form
s th
e T
UG
test
(se
e ab
ove)
and
sim
ulta
neou
sly
perf
orm
s a
cogn
itiv
e ta
sk a
t a
self
-sel
ecte
d pa
ce (
i.e. r
ecite
d na
mes
or
anim
als)
. Her
e on
ly th
e na
min
g an
imal
task
wil
l be
pres
ente
d.
The
y ar
e in
stru
cted
to p
rior
itiz
e th
e w
alki
ng ta
sk.
Min
i-M
enta
l Sta
te
Exa
min
atio
n (s
core
)
I, I
I, I
II, I
V
A c
ompo
site
scr
eeni
ng te
st o
f co
gnit
ive
func
tion
. Max
imum
sco
re: 3
0 p.
A s
core
of
20-2
5 p
indi
cate
m
ild
dem
enti
a, 1
0-19
p m
oder
ate
dem
enti
a, a
nd b
elow
10
p se
vere
dem
enti
a.
C
lock
Dra
win
g te
st (
scor
e)
II
, III
Ass
esse
s vi
suos
patia
l fun
ctio
n, s
eman
tic m
emor
y, a
nd p
lann
ing.
The
par
tici
pant
set
num
bers
and
han
ds
show
ing
“ten
min
utes
to tw
o” o
n a
cloc
k fa
ce.
Ver
bal F
luen
cy te
st
(num
ber)
II
, III
Ass
esse
s se
man
tic
mem
ory
and
lang
uage
. The
par
tici
pant
nam
es a
s m
any
anim
al w
ords
as
poss
ible
du
ring
60
s.
Tra
il M
akin
g T
est A
(s)
II, I
II
A
sses
ses
exec
utiv
e fu
ncti
on; v
isua
l att
enti
on, e
xecu
tive
and
psy
chom
otor
spe
ed. O
n a
pape
r w
ith
25
num
bere
d ci
rcle
s, th
e pa
rtic
ipan
t dra
ws
a li
ne f
rom
1 to
25
as f
ast a
s po
ssib
le.

31
Participating couples in Study I Two community-dwelling men with mild AD were recruited to participate in a qualitative case study along with their spouses. In addition to the criteria mentioned above, the men and their spouses were considered to have rele-vant contributions to make regarding the questions addressed in the study, and regarded as capable of holding a conversation for at least half an hour. Based on these criteria the physicians at the Memory Clinic suggested two couples. They were subsequently invited and both agreed to participate.
Participants in Studies II – IV The participants in Studies II, III, and IV were based on a sample of 25 indi-viduals with AD (Table 1). They were recruited consecutively during 20 months from the Memory Clinic at the Uppsala University Hospital. Of the 48 individuals with AD who fulfilled the inclusion criteria according to the medical records, 19 declined participation because of lack of time, long trav-elling distance to the hospital, or other reasons not mentioned. The remain-ing 29 eligible individuals underwent a brief examination, and it was found that three of them no longer fulfilled the inclusion criteria, and another one withdrew consent to participate. Thus, 25 individuals with AD were included to participate in the longitudinal project (Studies II and III).
At baseline, the 25 participants with AD were compared with 25 cogni-tively healthy age and group-matched controls to reflect the baseline status of the participants with AD. Nineteen of the healthy controls were recruited from a register of cognitively healthy people 65 years of age or older. They had previously consented to participate in clinical research at the Memory Clinic. The six cognitively healthy controls, younger than 65 years of age, were recruited from the staff at a Geriatric Clinic. The healthy controls scored 28-30 points on the MMSE (Folstein et al., 1975), and 1 or 2 on the FAST (indicate “normal adult” and “normal older adult”, respectively) (Reisberg, 1988).
Twenty-two of the 25 participants with AD completed the two-year peri-od including clinical measurements of walking capacity and physical activity levels (Study II), and 21 of the 25 participants with AD completed the two-year study period including gait analysis in the motor laboratory (Study III). Twenty one of the 22 participants were still community-dwelling at the two-year follow-up. Reasons for discontinuation were severe illness other than AD (n=2), cohabitant’s occupation (n=1) or severity of dementia (n=1).
A purposive sample (Bryman, 2002) of 14 people with AD was selected from participants included in Studies II and III, to participate in individual in-depth interviews. These 14 individuals were selected with the intention to achieve a wide variation with regards to age, gender, physical activity level, dependency in activities, residence, and education level.

32
Data collection and analysis
Study I – A qualitative case study Data on the four participants’ experiences and perceptions related to differ-ent aspects of physical activity were collected by individual in-depth inter-views. An interview guide with open-ended questions was used. The areas of questioning dealt with how the participants felt that the AD had influenced the men’s ability to be physically active and the participants’ thoughts about the importance of physical activity. Two interviews and two participant ob-servations were made with each man with AD. Their spouses were inter-viewed once each. Each interview lasted for 45-60 minutes. The interviews were carried out in privacy without the spouse being present. Data collection for each couple lasted for about a month. The interviews were tape recorded and then transcribed verbatim. The participant observations were carried out in their home environment during physical activities they normally did sev-eral times a week. Suitable times were chosen in agreement with the partici-pants and the observations lasted 45-120 minutes. During the participant observations, the men’s ability to perform physical activities in everyday life was observed. Field notes were taken during the observations, and immedi-ately afterwards summarized into a written text.
The written text material from in-depth interviews and participant obser-vations was analysed according to the thematic analysis guidelines described by Braun and Clarke (2006). However, in the following, the terms of the identified patterns will follow the terminology outlined by Graneheim & Lundman (2004, 2008), which was the analysis method applied in Study IV. Thereby, comparisons and relations between the findings in Studies I and IV can be carried out more easily. Thus, the analysis concept category is com-posed of codes with a similar content and refers to analysis patterns of text data on a descriptive and low abstraction level (manifest content). A catego-ry answers the question “What?”. Accordingly, the concept theme reflects the connection thread in two or more categories and links the underlying meaning together on an interpretive level, i.e. an analysis of the latent con-tent. A theme answers the question “How?”
The analysis involved repeated reading of the text material and coding of important features into potential categories. This stage was followed by a preliminary identification of categories and sub-categories based on analysis and interpretation of the entire data set. The main supervisor (AC Åberg) and Y Cedervall held repeated peer debriefings to explore various aspects of the preliminary findings, and to refine the interpretations and definition of cate-gories. The analysis and interpretations were performed both on a descriptive and on a more comprehensive level. Finally, categories and sub-categories relevant to the aim of the study were confirmed, named, and then considered

33
in relation to theoretical perspectives and findings from other studies. Multi-ple triangulations (i.e. method-, time-, space-, and person-triangulation) (Polit et al., 2008), were used to enable a thick description and provided a basis for establishing trustworthiness
Study II – Clinical measurements and observations The data was collected on three occasions; at baseline, and after one and two years (Figure 2). The participants with AD and the healthy controls complet-ed five walking capacity tests (Table 2): the 10 m comfortable walk test (Watson, 2002), the 6-minute walk test (Bean et al., 2002; Steffen et al., 2002), and three different types of the TUG test (Podsiadlo et al., 1991; Shumway-Cook et al., 2000). The TUG tests were performed in the follow-ing order: one TUG single-task and two types of TUG dual-task (naming names and naming animals). We will here present results only from the TUG dual-tasks naming animals because this dual-task type had the greatest im-pact on walking capacity. The participants’ need for verbal cueing during TUG-testing was recorded as present or not present. Verbal cueing was rec-orded as present if the participant needed instructions to turn around, to sit down, or if he/she asked questions about how to perform the test during test-ing. No verbal cueing was given to encourage the participants to walk faster, to continue to walk if they hesitated, or if they made occasional stops during walking. The 10 m walk test was chosen to assess general physical function, the 6-minute walk test to assess endurance and walking capacity, and the TUG tests to assess basic mobility and capacity to divide attention when walking. These are reliable measures for use on individuals with AD (Ries et al., 2009; Suttanon et al., 2011).
In addition, measurements of aerobic activity level (Ainsworth et al., 1993, 2000; Nelson et al., 2007) were applied in the AD- and in the control group. Physical activity level was assessed by diary registrations of aerobic activities (Bryman, 2004; Nelson et al., 2007; WHO, 2010). In the AD group, the cohabitants performed or supervised the registrations. The record-ed activities were then classified according to the coding scheme proposed by Ainsworth et al. (1993, 2000) as a basis, related to public health recom-mendations, and then quantified by calculating estimated minutes of aerobic activity/week (moderate intensity or higher) and number of days/week with 30 minutes of aerobic activity (moderate intensity or higher).
Falls the previous year were registered. A fall was defined as an event which results in a person coming to rest inadvertently on the ground or floor or other lower level (Lamb et al., 2005). In the AD group, cohabitants re-ported participants’ falls.
The AD group completed four cognitive tests (Table 2): the MMSE (Folstein et al., 1975), the Clock Drawing test (Freedman et al., 1994), the Verbal Fluency test (Solomon et al., 1998), and the Trail-Making Test A (Lezak, 1995). The control group completed the MMSE.

34
Statistical analysis Non-parametric statistics were applied because of the small sample size and data on ordinal levels. Cross-sectional differences at baseline between the AD group and the control group were calculated by the Mann-Whitney U-test (continuous variables), and Fisher’s test (categorical variables). Longi-tudinal differences in the AD-group in walking capacity, aerobic activity level and cognitive function were calculated using Friedman’s test. The Wil-coxon signed-rank test was used for post hoc pair wise analyses on differ-ences during the follow-up period. Correlations between walking capacity and cognitive function were assessed by Spearman’s rank correlation coeffi-cient. All tests were two-tailed. The level of significance was set at p<0.05, except for post hoc pair wise comparisons, where significance was p<0.025 to adjust for multiple comparisons. The percentage time differences (dual-task cost) between mean time of TUG single- and dual-task were calculated.
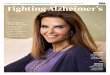
Study III – Gait parameter measurements and gait observations The data collection was conducted on three occasions, at baseline, and one and two years (Figure 2). A Qualisys® motion capture system, which is a three-dimensional optical gait analysis system, was used. The standard marker set-up at the motor laboratory of the Uppsala University Hospital included 18 reflecting markers applied on defined anatomical landmarks (Figure 3). The marker set up was developed at the Lundberg Motion Analy-sis Laboratory at Sahlgrenska University Hospital, Sweden. A six camera Pro Reflex® system recorded the position of the markers at a sampling fre-quency of 240 Hz and low-pass-filtered with a cut off frequency of 6 Hz. At each gait occasion, the following gait parameters were computed: gait speed (m/s), step width (m), step length (m), step height (m), and double support (seconds spent with both feet on the ground). The participant walked bare-foot a distance of approximately 7 metres. Data on gait parameters were collected from the middle part (approximately 3 metres). All gait parameters were examined at the participant’s comfortable gait speed during three dif-ferent conditions in the following order: five single-task trials, three dual-task trials naming names, and three dual-task trials naming animals. Here only the dual-task test, naming animals will be presented because this dual-task type had the greatest impact on gait.
A brief explanation of the test procedure and instructions on how to walk during the tests were initially given to the participants in a narrative way. Thereafter, standardize instructions were given before each of the trials. If necessary, repeated instructions were given. The participants were instructed to prioritize the motor task during the dual-task trials (i.e. continue walking even if they did not come up with any words).

35
.
Figure 3. The marker set-up during gait testing in the motor laboratory (the person is not a participant in the study, and he has given us his permission to use the photo).
Data processing The data was processed using the software Visual 3D (C-Motion Inc., Ger-mantown, DM, USA) and gait parameters were computed according to the developed Qualisys® motion capture system. The first single-task trial was considered a practice round and therefore excluded from the statistical anal-ysis. Thus, the statistical results presented here are based on mean values of 3-4 steps in the middle part of each trial of four single-task trials and three dual-task trials naming animals. The visual examinations are based on all available motion capture files for each participant.
Statistical analysis All parameters were normally distributed except double support. Therefore, parametric statistics were applied for calculating longitudinal differences in gait speed, step width, step length and step height (repeated measures ANO-VA). Non-parametric statistics were applied for longitudinal differences in double support (Friedman’s test). For cross-sectional analysis of differences between single- and dual-task gait parameters, the paired samples t-test was used for normally distributed gait parameters, and the Wilcoxon signed-rank test for double-support. The Spearman’s rank correlation coefficient was
The marker placement Shoulder Thoracic vertebrae 12 Sacrum Anterior superior iliac spine Superior part of the patella Knee joint line Tuberosity of the tibia Lateral malleoulus Toe Heel

36
used to assess correlations between gait parameters and cognitive function. All tests were two-tailed. The levels of significance were set to p<0.05 for cross-sectional and longitudinal differences. The cross-sectional dual-task cost percent was calculated between single-task gait parameters and dual-task gait parameters (see Abbreviations and definitions). The Bonferroni method was used to correct for multiple comparisons of normally distributed gait parameters, and the Wilcoxon signed-rank test for post hoc tests of dou-ble support time (p<0.025 to adjust for multiple comparisons). To minimal-ize the risk of type 1-error, the significance for correlations was set at p<0.01.
Systematic visual examination A systematic visual examination of all motion capture files was performed, with the intention of comparing gait patterns at single- and dual-tasking. The visual examination comprised scrutinizing all the motion capture files (i.e. each gait trail) several times from different angles and at different gait speeds. A preliminary classification of the characteristics of the different dual-task gait disturbances was performed. Thereafter, the different types of gait disturbances were compared with each other, and the preliminary classi-fication was refined. During the analysis process, repeated peer debriefings were held between the main supervisor (AC Åberg) and Y Cedervall. Final-ly, a classification of dual-task gait disturbances was determined.
Study IV – Subjective experiences of people with AD Data collection consisted of two individual in-depth interviews within a month with each of the 14 participants. The interviews were performed in private. The informants decided if the interviews would take place in their homes or at the Uppsala University hospital. An interview guide with open-ended questions was used as a basis. The guide covered questions regarding the participants’ experiences about how the ability to be physically active had been influenced by the dementia and their thoughts related to physical activity. A free narration was encouraged and the initial questions were fol-lowed by probing questions. At the second interview in the set, focus was on obtaining clarifications and deepening the understanding of the experiences and thoughts expressed in the first interview, and to touch areas that were not commented upon or only briefly mentioned during the first interview. Each interview lasted 30-60 minutes. The interviews were tape recorded and thereafter transcribed into written text. A qualitative content analysis was used to analyse and interpret the manifest and latent content (Graneheim et al., 2004; Lundman et al., 2008).
The qualitative content analysis started with repeated readings of all the transcribed text data. Preliminary thoughts and analysis ideas were noted and used as a starting point for the analysis and interpretation. Meaning units (one or two sentences) related to the aim were identified and coded (short

37
description of the content). Codes with a similar content were grouped into preliminary descriptive sub-categories. They were checked and compared against the text of origin in an on-going process and finally grouped into four descriptive categories. Thereafter, an analysis of the latent content was con-ducted. During this phase of the analysis process, the data was interpreted at a higher abstraction level to identify underlying connecting thoughts in two or more categories. Preliminary interpretations were checked and compared with the text of origin several times and finally three sub themes and one overarching theme were identified, which constituted a plausible interpreta-tion of the role physical activity plays for individuals with AD. In order to establish trustworthiness, repeated peer debriefing sessions were conducted during the analysis process. The co-authors (S Torres and AC Åberg) acted as peers to Y. Cedervall, who was the primary coder.

38
Results
In the following, the main results from Studies I, II, III, and IV will be pre-sented. They all reflect different perspectives on how the ability to be physi-cally active is affected in the early stages of AD. To explore the diverse as-pects and further understanding, three main strategies were used, namely, exploring by measurements (Studies II and III), observation (Studies I, II and III), and sharing the participants’ subjective experiences (Studies I and IV). In Studies I and IV descriptive statistics on the participants’ cognitive func-tion were reported, and in Study IV the text data were complemented by data on walking capacity, gait function, and aerobic activity levels (see Table 1 and 2 for an overview).
Study I - A qualitative case study Three central categories that described the participants’ experiences related to physical activity and their perceptions of the importance of physical activ-ity were identified: 1) Physical activity as health reinforcement; 2) Barriers to physical activity;3) Adaptation strategies (Figure 4).
Figure 4. Three categories describing experiences related to the ability to be physi-cally active and the perceived importance of such activity.
Physical activity as health
reinforcement
Adaptation strategies
Barriers to physical activity

39
Physical activity such as walking was described as an important routine in everyday life for the two men with AD. Important driving forces for them were enjoyment of nature and body movement, and positive attitudes to-wards physical activity in general. The spouses said that their husbands ben-efited from taking walks, in particular by gaining increased well-being but they also expressed opinions on the importance of being physically active in general. Despite the positive experiences and perceptions regarding physical activity, all four participants mentioned several barriers to it, caused by the dementia. However, the men with AD did not appear to dwell on these barri-ers to the same extent as their spouses.
One main barrier was tiredness, which restricted the activity level of both men during the day. Along with tiredness, difficulties in finding the way seemed to be a significant barrier. The picture, however, was contradictory. On the one hand, both spouses talked about the difficulties their husbands had in finding the way, and on the other hand, both men took outdoor walks on their own almost daily. None of the men showed any difficulties to find the way on their routine walks during the participant observations. The spouses and one of the men additionally spoke about “peculiar behaviour” among the men that was considered incomprehensible. This “peculiar behav-iour” referred difficulties in adjusting the body to the environment (e.g. walking straight into objects, standing in the way). Impaired walking ability was mentioned by one of the two couples as a barrier and included a deterio-ration of balance and endurance, but this was only partly confirmed during the observations.
The spouses expressed their opinion that their men benefited from out-door walks and that the walks contributed in making their day meaningful. Therefore, the spouses made considerable practical and mental adjustments in everyday life to enable their husbands to stay physically active. Practical adaptation strategies consisted of, for example, security routines to overcome risks for the men getting lost, and mental strategies to take things one day at a time and not to worry in advance.
Study II – Clinical measurements and observations
Cross-sectional results At baseline, the AD group had a significantly lower walking capacity and cognitive function than the healthy control group (e.g. Md. walking speed 1.11 vs. 1.32 m/s, MMSE 25 p vs. 30 p, p<0.001), but comparable levels of aerobic activity (Md. 335 vs. 340 minutes/week, p=0.564). In both groups, 20 out of 24 (missing data n=1) (83%) reached the public health recommen-dations of aerobic activity. The TUG dual-task cost was 89% in the AD group and 11% in the control group. However, there were no significant correlations between walking capacity tests and cognitive function tests at

40
baseline in the AD-group. Eight participants with AD needed verbal cueing to complete the TUG test but only one in the control group. For the TUG dual-task, 12 participants in the AD group needed verbal cueing but none in the control group. In the AD group, three participants had experienced one fall during the last year. In the control group, 10 participants had fallen once or twice during the same period.
Longitudinal results Twenty-two of the 25 participants with AD completed the two-year study period and their results were included in the longitudinal calculations (Table 3). During the two-year follow-up period, walking capacity declined in the AD group when assessed by the 10 m walk test, 6-minute walk test, and TUG single-task. Additionally, cognitive function declined significantly, but aerobic activity levels did not change significantly. Thirteen out of 21 need-ed verbal cueing during the TUG single-task test (without a cognitive task). No significant difference was observed in the TUG dual-task, but five partic-ipants with AD were not able to perform the test despite verbal cueing re-garding performance (i.e. “turn around”, “sit down”). The difficulties were due to cognitive impairments. Of the 17 participants completing the TUG dual-task on all three occasions, 10 individuals required verbal cueing to complete the task. In comparison, moderately significant correlations were detected only between the TUG dual-task and the MMSE (rs=-0.567, p=0.014) and the clock drawing test (rs=-0.579, p=0.019), but not between any other of the walking capacity and cognitive tests.
The rate of falls in the AD group did not change significantly during the follow-up period.
Study III – Laboratory-based gait measures and observations There was a significant decline in gait speed and step length during single- and dual-tasking (Table 3). Dual-task cost was marked at baseline, but ap-peared to remain on a stable level during the study period. However, the cross-sectional differences between single- and dual-tasks gait parameters were significant for all comparisons, except the one-year follow-up values for step width (see Figure 5 for gait speed).

41
m/s
Figure 5. The cross-sectional differences between gait speed single-task and dual-task (m/s). The differences are significant for comparisons between single-task and dual-task on all three occasions.
Systematic visual examination of the motion capture files revealed three different characteristics of gait disturbances that only occurred during dual-tasking (see Appendix): 1) Temporal disturbance, 2) Spatial disturbance, and 3) Instability in single stance. Temporal disturbance consisted of occa-sional stops in single or double stance, Spatial disturbance comprised varia-ble step length, step width or deviating direction, and Instability in single stance correction of the stance foot position in single stance. Twelve partici-pants showed at least one specific type of gait disturbance at baseline, but the number did not increase during the study period (n=10, n=10). However, there was a tendency of an increase in showed gait disturbances during the study period (16/15/18). It is to be noted that the prevalence of a specific type of gait disturbance was not consistent, but occurred irregularly. The most common types of gait disturbances were occasional stops in double stance, variable step width/deviation direction, and variable step length.
1.14 1.11.01
0.74 0.76
0.64
0
0.2
0.4
0.6
0.8
1
1.2
Baseline 1-yearfollow-up
2-yearfollow-up
Gait Speed
Dual-task gait speed

Tab
le 3
. Lon
gitu
dina
l dif
fere
nces
in p
artic
ipan
ts w
ith A
lzhe
imer
’s d
isea
se c
once
rnin
g w
alki
ng c
apac
ity, a
erob
ic a
ctiv
ity le
vels
, and
gai
t pa
ram
eter
s (S
tudy
II
and
III)
.
n
Bas
elin
e M
d (r
ange
) O
ne-y
ear
foll
ow-u
p M
d (r
ange
) T
wo-
year
fol
low
-up
Md
(ran
ge)
p-va
lue
Min
i-M
enta
l Sta
te E
xam
inat
ion
scor
e (0
-30)
, Md
(ran
ge)
21
25 (
21-3
0)
22 (
16-2
9)
20 (
9-28
) <
0.00
1a, b
Wal
king
cap
acit
y
10
m c
omfo
rtab
le w
alk
test
(m
/s)
22
1.11
(0.
83-2
.0)
1.11
(0.
5-1.
43)
1.08
(0.
48-1
.43)
0
.022
c
6-
min
ute
wal
k te
st (
m)
22
494
(344
-712
) 44
5 (1
74-7
03)
430
(160
-616
) <
0.00
1a, b
T
UG
si
ngle
-tas
k (s
) 21
11
(8-
14)
12 (
9-30
) 12
.5 (
9-27
) 0
.020
a, b
dual
-tas
k (s
) 17
17
(12
-39)
17
(12
-70)
22
(12
-83)
0
.137
TU
G d
iffe
renc
e
du
al-t
ask
– si
ngle
-tas
k (s
) 17
7
(-1-
25)
6 (8
1-53
) 11
(-1
-57)
0
.459
du
al-t
ask
cost
(%
) 17
79
84
96
Aer
obic
act
ivit
y le
vel
min
utes
/wee
k (m
inut
es)
21
332
(8-9
45)
285
(10-
670)
27
0 (1
0-60
0)
0.7
11
days
/wee
k w
ith
aero
bic
acti
vity
≥ 3
0 m
inut
es (
days
)
21
5
(0-7
)
4.5
(0-7
)
4 (0
-6.5
)
0.3
08
Tab
le 3
con
tinue
d on
pag
e 43
.

Tab
le 3
con
tinue
d fr
om p
age
42.
G
ait p
aram
eter
s
n m
ean±
SD
mea
n±SD
m
ean±
SD
p-
valu
e
Sing
le-t
ask
G
ait s
peed
(m
/s)
211.
14 ±
0.1
41.
10 ±
0.1
5 1.
01±
0.20
<0.
001a,
c
S
tep
leng
th (
m)
210.
62 ±
0.0
70.
60 ±
0.0
7 0.
57 ±
0.0
9<
0.00
1a, c
S
tep
wid
th (
m)
210.
08 ±
0.0
20.
08 ±
0.0
2 0.
09 ±
0.0
2 0
.801
D
oubl
e su
ppor
t (s)
21
0.27
± 0
.06
0.26
± 0
.07
0.29
± 0
.08
0.0
08c
S
tep
heig
ht (
m)
210.
22 ±
0.0
20.
21 ±
0.0
2 0.
21 ±
0.0
2<
0.00
1a, c
Dua
l-ta
sk
G
ait s
peed
(m
/s)
210.
74 ±
0.22
0.76
±0.
27
0.64
±0.
22 0
.007
a, c
S
tep
leng
th (
m)
210.
57 ±
0.09
0.55
±0.
09
0.51
±0.
11<
0.00
1a, c
S
tep
wid
th (
m)
210.
09 ±
0.03
0.09
±0.
04
0.10
±0.
03 0
.117
D
oubl
e su
ppor
t (s)
21
0.50
±0.
320.
43 ±
0.19
0.
49 ±
0.18
0.0
12c
S
tep
heig
ht (
m)
210.
21 ±
0.00
20.
20 ±
0.02
0.
20 ±
0.03
<0.
001a,
c
Fre
idm
an’s
tes
t w
as u
sed
to c
alcu
late
dif
fere
nces
in
wal
king
cap
acit
y, a
erob
ic a
ctiv
ity
leve
l, an
d do
uble
sup
port
. Po
st h
oc p
airw
ise
diff
eren
ces
wer
e ca
lcul
ated
by
the
Wil
coxo
n si
gned
-ran
k te
st.
Rep
eate
d m
easu
res
AN
OV
A w
as u
sed
to c
alcu
late
dif
fere
nces
for
all
oth
er g
ait
para
met
ers
(cor
rect
ed f
or m
ulti
ple
com
pari
sons
by
Bon
ferr
oni)
. a S
igni
fica
nt d
iffe
renc
es b
etw
een
base
line
and
2-y
ear
follo
w-u
p. b Si
gnif
ican
t dif
fere
nces
bet
wee
n ba
seli
ne a
nd 1
-yea
r fo
llow
-up.
c Sig
nifi
cant
dif
fere
nces
bet
wee
n 1-
year
fol
low
-up
and
2-ye
ar f
ollo
w-u
p.

44
Study IV - Subjective experiences of physical activity in individuals with AD The analysis of the interview data from the 14 participants with AD revealed three sub-themes that reflected interrelated perspectives on how people with mild AD reason about physical activity as part of everyday life (Figure 6). Specific focus was put on their ability to be physically active, and the mean-ing they attached to physical activity: Sub theme 1) Striving to be physically active, mirrors the participants’ approaches to cope with dementia-related barriers to physical activity by different strategies; Sub-theme 2) Under-standing in favour of physical activity, reflects how their thoughts and be-liefs regarding written and tacit norms encouraged them to remain physically active, and Sub-theme 3) Physical activity as a means to well-being, refers to how emotions and feelings related to the performance of physical activity inspired them to remain physically active. These emotions and feelings seemed to be achieved by movements in themselves and also by being out-doors while performing them.
Figure 6. The three sub-themes illustrating interrelated perspectives on how people with mild Alzheimer’s disease reason about physical activity, and one overarching theme that mirrors the common thread in the sub-themes interpreted against Harré’s framework of selfhood : Physical activity as a means of selfhood maintenance.
An analysis of the underlying meaning in the sub-themes revealed one over-arching theme that tied these three sub-themes together. This main theme emerged when the sub-themes were interpreted against Harré’s framework on selfhood: Physical activity as a means of selfhood maintenance. This main theme indicated that people with AD use physical activity as a means
Physical activity as a means to
well-being
Striving to be
physically active
Understanding
in favour of
physical activity
Selfhoodmaintenance

45
to shift the focus from attributes and social roles associated with the demen-tia diagnosis to activities and behaviours that could be considered associated with a healthy life. One of the participants described her views on this mat-ter.
“No, I think that keeping going is good for my whole mental state. I can tell. I feel so alive when I walk outside and manage on my own. So it’s, well, it feels really good, and then I don’t have that feeling that I’m ill.”
This quote can be interpreted as a statement that her ability to take walks independently gave her a sense of continuity in her selfhood. Thus, the find-ings suggest that physical activity may be highly valued in AD as it puts the focus on continuity in aspects linked to a healthy life, and that physical ac-tivity can constitute a means of sustaining well-being and selfhood in mild AD.

46
Methodological considerations
Sampling One main concern in this work is the study sample. The participants with AD were recruited to participate in a longitudinal study exploring different aspects of physical activity. The participants, and their cohabitants, may therefore have been specifically engaged in physical activity. Thus, it is pos-sible that the participants were systematically different from other individu-als with AD. However, the inclusion criteria did not comprise any specific claims about physical activity levels, or interest in physical activity. Still, a specific interest for physical activity may have influenced the positive atti-tude towards physical activity reported in Studies I and IV. On the other hand, the numeric data on aerobic activity levels (Study II) enabled a purpos-ive selection of informants for Study IV with a wide variety of physical ac-tivity levels ranging from less than 10 minutes a week to 10 hours a week. Therefore, the findings in Study IV are based on interviews with both physi-cally inactive and active participants.
The high level of education in the AD and in the control group was an-other factor that might have influenced the participants’ physical activity level and cognitive function. The level of education may explain why the participants in both groups reported higher aerobic activity levels than the general population (FHI, 2010).
Additionally, all participants with AD were community-dwelling with a cohabitant, and may therefore have been more active in everyday life than individuals with AD dwelling alone. It would not have been possible, how-ever, to have conducted the research project without a supporting cohabitant. It is to be noted that, despite the relatively high reported aerobic activity level in the AD group, they had a significantly lower cognitive function and walking capacity than the healthy controls. Moreover, the deteriorated cogni-tive function and walking capacity continued to decline during the study period.
The small sample sizes in Studies II and III is a limitation, which restricts the possibility of generalizing the results from these studies to a larger popu-lation. The study group was, however, comparable to previous cross-sectional studies that have demonstrated significant differences in walking capacity and gait function between people with mild AD and healthy con-trols (Ijmker et al., 2012; Maquet et al., 2010; Muir et al., 2012; Pettersson et

47
al., 2007), and significant changes of gait function during a one-year period among people with mild to moderate AD (Wittwer et al., 2010). It is likely that the lack of significant correlations between cognitive functions, gait parameters, and walking capacity could be due to the small sample size, in addition to the drop out of participants unable to perform some of the cogni-tive tests and the TUG tests at the two-year follow-up.
Data collection Aerobic activity level Our decision to use diary registration to measure aerobic activity levels was based on previous studies in which the questionnaires Physical Activity Scale for the Elderly (Burns et al., 2008) and the Frenchay Activity Index (Pettersson et al., 2002) were used. Both scales showed a decreased level of physical activity among people in the early stages of AD, but at the same time indicated a reasonable level of physical activities such as walking. A suggested explanation for the contradictory picture could be that question-naires such as those mentioned above commonly reward regular perfor-mance of a wide variety of physical activities. There is hence a risk that the habitual aerobic activity level of people with AD is underestimated, as indi-viduals with dementia tend to cease complicated activities early in the course of the disease. We therefore wanted to explore if people in the early stages of AD may still be physically active, but with a limited range of activities.
A limitation with diary registrations, and questionnaires, is that it is not possible to obtain the exact intensity, duration and frequency of physical activities. A strength is that an overall picture of the different types of per-formed physical activities can be attained. A complementation with an ob-jective measurement of physical activity, e.g. accelerometer, might have added interesting data to the diary registrations although accelerometers are insensitive to physical activities performed with the upper body, bicycling and swimming (FYSS, 2008). In order to ensure the validity of the diary registrations, careful instructions were given to the participants and the care-givers. The instructions included that the participants would continue with their habitual physical activities during the two-week registration period. Moreover, they were informed about what types of activities they would register, with regard to intensity and duration, i.e. activities of moderate in-tensity of bouts of at least 10 minutes. In addition, clarifications of recorded activities were obtained in direct dialogue with the caregivers and partici-pants. The recorded activities were finally classified according to the coding scheme proposed by Ainsworth (1993, 2000) to estimate the intensity of the recorded physical activities and thereby validate data.

48
Ability to divide attention Our intention regarding the dual-task tests (Studies II and III) was to exam-ine how walking capacity and gait function are influenced by a relatively simple cognitive task, and what changes can occur over an extended period of time, i.e. two years. Longitudinal changes in dual-tasking have to our knowledge, not been previously explored in people with AD. Assessing du-al-task ability might be a potential measurement to identify individuals who are at risk of falls during dual-task conditions. The participants were in-structed to name animals at their self-selected pace and prioritize the walking task if they did not come up with any words. We used the self-selected pace when wording to minimize the stress on the participants, but still distract their gait. This method has previously been used in cross-sectional studies including individuals with mild AD (Camicioli et al 1997; Pettersson et al. 2005; Muir et al 2012). The same method was used during both the TUG dual-task test (Study II) and the gait testing in the motor laboratory (Study III). A structured recording of wheather verbal cueing was given or not was performed during TUG testing to validate data (Study II), i.e. no cueing was given to encourage the participant to keep on walking if he/she hesitated or made occasional stops as this would have made it impossible to measure the “true” dual-task effect on the performance.
It is to be noted that even though the participants could choose the severi-ty of the cognitive task (i.e. naming animals at a self-selected pace), and were instructed to prioritize the walking task, we noticed that the participants made occasional stops when they did not come up with any words. This was likely due to their impaired working memory, which made them forget to prioritize the walking task, and also due to an impaired ability to divide at-tention between a motor task and a cognitive task. Our experiences are in accordance with Suttanon et al. (2011) who found that 4 out of 14 individu-als with mild-moderate AD in their study were unable to perform TUG cog-nitive, despite cueing.
During gait testing in the motor laboratory (Study III), no cueing was giv-en because the motor task consisted of a straight walk (i.e. no turning or sitting down as in the TUG test). However, we frequently observed dual-task gait disturbances that only occurred during dual-tasking. Therefore, the nu-meric data obtained from the gait testing were complemented by a systemat-ic visual examination of all motion capture files. Because of the observed dual-task gait disturbances during testing the purpose was to identify differ-ent characteristics of gait disturbances. During this procedure, all motion capture files were scrutinized several times, at different speeds and from different angles, which is an advantage in comparison to observing gait in “a real life situation”. A clear strength by complementing statistically calculat-ed gait variability with a visual examination of motion capture files (includ-ing a descriptive classification and video illustrations of dual-task gait dis-

49
turbances), is that it provides a potential explanation to calculated dual-task gait variability in early-stage AD. Moreover, the characteristics of such dis-turbances can easily be communicated to health care professionals, research-ers, caregivers and individuals with AD if illustrations are shown.
Comparison of the AD group’s gait function measured in the motor labor-atory to a healthy control group might have been of benefit. However, in Study II the healthy controls did not demonstrate any signs of walking dis-turbances while performing the TUG dual-task test, even if the TUG dual-task seemed to be more challenging than dual-tasking in the motor laborato-ry. This was shown by higher dual-task costs in TUG tests and more partici-pants in the AD-group unable to perform the TUG dual-task test at the two-year follow-up, in comparison to performance during gait testing in the mo-tor laboratory.
Fall registrations Falls were not a main focus of this project even though they are closely re-lated to physical activity among people with AD (Beauchet et al., 2009; Gleason et al., 2009). The intention with the fall registrations was to reflect the number of falls in the study groups and relate them to aerobic activity levels, walking capacity, gait function and subjective experiences to achieve a comprehensive descriptive picture of the participants’ functioning. Unfor-tunately, it proved difficult to draw any conclusions from the fall data. The main reason was the problems involved in fall registration by self-reports (i.e. cohabitants) of community-dwelling people with early-stage AD as they often spend time alone during the days and may not remember if they have fallen or not. Therefore, the fact that participants in the control group report-ed more falls than were reported among the participants in the AD group raises some questions (Study II). Did the participants with AD fall more often than was reported? Did the healthy controls engage in more risky types of activities and were therefore exposed to situations where one might fall (although not captured by the diary registration of aerobic activity)? Or was the high fall frequency in the control group just a coincidence? Another ex-planation may be that the number of falls increases until later on in the course of AD. This was suggested by Wittwer et al. (2010) who investigated gait function and falls in people with mild-moderate AD and found an al-most identical number of falls in the AD and control-group. However, Pitkälä et al. (2013) could demonstrate that physical exercises reduced the number of falls among community-living people with mild-moderate AD in comparison to a control group, by use of reports from informal partici-pants/cohabitants.
As mentioned previously, there may be validity problems involved in the self-reporting of falls from community-dwelling people with dementia. Therefore, studies are warranted using technical devices (e.g. body-worn sensors) (Schwickert et al., 2013), which can capture falls in everyday life,

50
indoor as well as outdoor to enable the accurate evaluation of fall interven-tions among community-dwelling individuals with dementia.
Analyses A qualitative approach was considered appropriate in Studies I and IV to answer the research questions furthering the understanding of experiences regarding the ability to be physically active from the perspective of individu-als with mild AD and their cohabitants, and the meaning they attach to phys-ical activity as part of their everyday life. Individual in-depth interviews are a feasible method of exploring the perspectives of people with mild AD (Clare, 2003; Hellström et al., 2007; Nygård, 2006). This method has be-come more common during the last decade and previous studies have shown that people with mild dementia are able to respond reliably to questions con-cerning, e.g. preferences, choices, feelings and other subjects related to qual-ity of life (Feinberg, 2001; Mozley et al., 1999; Öhman et al., 2008; Trigg et al., 2007). The benefits for a person with dementia to participate in an inter-view usually outweigh the risks if the interviewee has experience of people with cognitive impairments (Hellström et al., 2007; Nygård, 2006). This involves taking into account the specific problems a person with dementia might have (e.g. related to language and memory), and creating a safe con-text. In this project these precautions were made, and the fact that the inter-nal drop out was low in the longitudinal project indicates that participation was not experienced to be stressful by the participants.
Participant observation was used in Study I to collect data on walking performance (i.e. walking in the ordinary environment), and is a method that has previously been used in research involving people with dementia (Brorsson et al., 2011; Nygård, 2006). A benefit of this method is that the researcher can observe the individuals’ behaviour and abilities in their ordi-nary environment. The observations provided valuable data on the partici-pants’ daily routines, and performance in different familiar contexts, which had not been possible to obtain otherwise. During the observations, it was necessary as an observer to be part of the activities, as the participants nor-mally did not have any company on their activities that was of interest for observation, e.g. daily walks. The participants were also informed of the aims of the study. To minimize the impact of the presence of the observer (Y. Cedervall), no initiative was taken, or interference made with the partici-pants’ actions, but efforts were made to adopt a cautious approach and act in a casual manner.
Qualitative content analysis, as well as thematic analysis, is not philo-sophically bound to any specific philosophical tradition such as grounded theory or phenomenology (Braun et al., 2006; Danielsson, 2012). Qualitative content analysis and thematic analysis are described as suitable methods for the analysis and interpretation of text data grounded in the empirical-holistic

51
paradigm. Both methods have been widely used in health care research and have many similarities, even though the terminology of analysis patterns differs. The quality and richness of collected data is the main determining factor for whether it is possible to perform an analysis of the manifest (de-scriptive) or the latent (interpretive) content in the data (Braun et al., 2006; Danielsson, 2012; Hsieh et al., 2005). In Study I, the data was composed of written text from four interviews and four participant observations with the men with AD, and two interviews with their spouses. This enabled an analy-sis mainly of the manifest content of text and resulted in three separate cate-gories (Figure 4). In Study IV, the richness of data obtained from 28 individ-ual in-depth interviews made it possible to analyse the latent content and interpret the underlying meanings on a higher abstraction level, which re-sulted in three interrelated sub-themes and one overarching theme (Figure 6).
Trustworthiness To achieve trustworthiness of Studies I and IV a detailed description of the data collection and analysis procedures has been made (Graneheim et al., 2004; Lundman et al., 2008; Polit et al., 2008). The findings are illustrated by quotes from the interviews and observation notes enabling the readers to determine that the interpretations are based on data. We also used different kinds of triangulation to validate data (Polit et al., 2008). For example, in both Studies I and IV an informal member’s check was carried out by doing two individual interviews during a period of one to four weeks with the par-ticipant with AD. This method enabled the interviewer to obtain clarifica-tions of statements made in the first interview and probe deeper to ensure understanding of the participants’ statements and meanings. The two inter-connected interviews were also a way to achieve time triangulation, i.e. to ask similar questions at different time points to achieve a picture of consist-ence or inconsistence in the answers and statements made. Moreover, in Study I, data were collected by different methods and from different sources (participant observations of participants with AD, and interviews with them and their spouses), enabling a method, space and person triangulation and by that a multifaceted picture of the research question. In Study IV, text data from the interviews were complemented with numeric data from tests of walking capacity, cognitive function, and aerobic activity level to achieve a description of the participants with a focus on physical activity. Furthermore, the longitudinal design in the project as a whole, in combination with a per-son (Y. Cedervall) collecting all the data, enabled a prolonged engagement and possibilities to build trust with the participants. During the analysis and interpretation phase in Study IV, repeated peer debriefing sessions were held between the co-authors (S Torres and AC Åberg) and Y. Cedervall, in which preliminary analysis and interpretations were discussed and refined in an on-

52
going process. The co-authors are skilled researchers with long experience in performing qualitative research.
Mixed methods A clear strength of this thesis is the comprehensive approach involving data from diverse data sources, and that part of the data is collected under an ex-tended period of time. This design provided new perspectives on physical activity among people in the early stages of AD, and is in line with the pro-posed framework for organizing and identifying future directions for re-search in the area of dementia (O’Connor et al., 2007). The research frame-work proposed by O’Connor et al. is based on Kitwood’s definition of per-sonhood (see Abbreviations and definition section) and is the base for a per-son-centered care (Basun et al., 2013; SBU, 2008a; SoS, 2010). Research within this area encompasses three interrelated domains, namely subjective experiences of the person with dementia, the interactional environment and the broader socio-cultural context. The multi-perspectives used to investigate aspects of physical activity and AD in this thesis are in line with this re-search direction (O’Connor et al., 2007). The four studies included in this work involved a clinical-based picture of the prerequisites for being physi-cally active, habitual physical activity levels, and observations of being physically active in everyday life. In addition, subjective experiences related to these aspects and to physical activity in general were achieved. Thus, a comprehensive picture of the research problem was obtained. Moreover, data collected by one of these methods could compensate for weaknesses of, and add strengths to, the other methods used (Andrew, 2009; Creswell, 2009).
For example, the approach in this thesis, inspired by mixed methods re-search was probably decisive for the decision to perform a visual examina-tion of motion capture files when dual-task gait disturbances in the motor laboratory were observed. Thereby, we could identify specific characteristics of dual-task gait disturbances in AD. Statistically calculated gait variability has previously been reported (Allali et al., 2008; Sheridan et al., 2003; Wittwer et al., 2008) and clinical dual-task gait disturbances indicated (Camicioli et al., 1997), but to our knowledge specific types of gait irregular-ities related to dual-tasking have not been described or illustrated previously. Moreover, the interview and observation data complemented by numeric data on walking, aerobic activity levels and dual-task performance enabled understanding and explanations that we believe would not have been possi-ble with data from either of the sources alone.

53
General discussion
People in the early stages of AD have an impaired and declining walking capacity. A simple cognitive task can have a distinct impact on their walking performance. Their ability to walk can therefore vary substantially depend-ing on differing cognitive and environmental demands. Despite this, people with AD seem motivated and capable of maintaining a health-promoting level of physical activity. This could be understood as if physical activity provides them with “self-promoting benefits”, in addition to the common health-promoting benefits. In fact, in our study, being physically active was interpreted as a way to strengthen the participants’ sense of self associated with their lives before the dementia diagnosis. Physical activity hence con-tributed to reduce the sense of having dementia, and provided continuity and meaning to life.
Physical activity capacity and performance One of our main findings was that a simultaneously performed cognitive task, i.e. naming animals, appears to have a distinct impact on walking even in mild AD. This was shown by clinical (Study II) as well as laboratory-based measures (Study III). In Study II, the participants demonstrated diffi-culties in remembering the instructions for how to perform the mobility se-quence during the TUG test, and to prioritize the motor task. This resulted in the dual-task cost during the TUG test being significantly higher for the par-ticipants with AD than for the controls’ at baseline (89% vs 11%), and larger than in studies using only walking as the motor task (27%) (Muir et al., 2012). Similarly, in the motor laboratory setting (Study III), the dual-task cost for gait speed in our study was increased, but on a lower level than shown by the TUG test (35%). Thus, the lower dual-task cost shown in the laboratory setting most likely reflected the lower complexity of the motor task (only walking in comparison to the TUG test), however the dual-task cost in the motor laboratory setting was increased in comparison to healthy reference values (9%) (Muir et al., 2012). Previously, an increase of the complexity of the cognitive task (e.g. subtracting serials of 7s from 100) has been shown to raise the dual-task cost (Montero-Odesso et al., 2012a). Our findings suggest that even a more complex motor task, i.e. the TUG test, results in an increased dual-task cost. These observations demonstrate, that, cognitive function and gait are closely interrelated which is in line with an

54
emerging, alternative view on the relation between cognitive function and gait presented by Monter-Odasso et al. (2012b). They suggest that gait and cognitive function interact since cognitive impairments predict mobility de-cline and falls and, conversely, slow gait velocity and instability predict cog-nitive deterioration. Traditionally, cognitive function and gait have been viewed as separated geriatric entities related to dementia and falls, respec-tively. According to Montero-Odasso et al. (2012b) these two phenomena occur not in parallel, separated from each other, but in a concurrent manner.
In addition to the high dual-task cost for the TUG test described above (Study II), we also observed a clear effect on performance of the mobility sequence when a cognitive task was added. During baseline testing of the TUG dual-task test almost half of the participants with AD (12/25) needed verbal cueing such as “turn around” and/or “sit down”, but none in the healthy control group needed this. At the two-year follow-up, the proportion of participants in need for verbal cueing had increased (10/17). In addition, 5 of the 22 participants who completed the two-year study-period were unable to perform the TUG dual-task due to cognitive impairments, despite verbal cueing. Moreover, during gait testing in the laboratory setting (Study III), the participants presented irregular gait that only was observed during dual-tasking. The observed irregularities occurred occasionally and did not follow any consistent pattern. Thus, a participant could exhibit one distinct type of dual-task gait disturbance at just one of the dual-task trials, or two different types of gait disturbances at different dual-task trials. More than half of the participants exhibited at least one distinct type of dual-task gait disturbance at baseline (12/21), and there was a tendency of increased dual-task gait disturbances during the study period. Such descriptions and illustrations can provide a clarifying picture of the clinical characteristics of dual-task gait variability among people with AD, and constitute a valuable complement to previously reported statistically calculated gait variability (Allali et al., 2008; Sheridan et al., 2003; Wittwer et al., 2008). The dual-task conditions hence exposed clinically observable dual-task gait disturbances, which may be predictors of future falls (Bruce-Keller et al., 2012; Yogev-Seligmann et al., 2008). Longitudinal studies investigating the association between the preva-lence of these types of dual-task gait disturbances for the prediction of func-tional decline and falls are, therefore, warranted.
Moreover, we found that the walking capacity and gait function in terms of e.g. gait speed and step length, were deteriorated already in mild AD and continued to decline in the following two years. These findings are in line with previous cross-sectional studies including people with MCI and AD at different stages of dementia (Eggermont et al., 2010; Maquet et al., 2010; Pettersson et al., 2005; Wittwer et al., 2008), and with a longitudinal labora-tory-based study involving people with mild and moderate AD (Wittwer et al., 2010). In our study group, the dual-task costs for gait speed did not in-crease, but remained on a stable level during the two-year follow-up period,

55
even though the gait speed during both conditions declined significantly (Study III). One may speculate if this could reflect a “walking-too-fast-strategy”, indicating a lack of insight in declining cognitive functions and resulting in an inability to adapt walking to a cognitively demanding situa-tion, i.e. walking slower, but still too fast in relation to their capacity. Such a strategy has been reported among frail older people with dementia who showed a tendency to walk too fast in relation to their capacity and environ-mental factors (van Iersel et al., 2006). When we used the TUG tests (Study II), the dual-task cost appeared to remain relatively stable during the two-year study-period, but it is to be noted that 5 out of 22 were not able to per-form the test due to cognitive impairments, despite cueing. However, a com-parison of dual-task costs between healthy controls, people with MCI and those with mild AD shows inconsistent results. One study reported a gradual increase of dual-task costs as the cognitive function deteriorated (Pettersson et al., 2007), while another demonstrated equal dual-task costs among people with MCI and mild AD (Muir et al., 2012). Longitudinal studies evaluating dual-task costs in people with cognitive impairments are scarce, but are needed to clarify the relation between ability to divide attention when walk-ing and falls.
How did the participants perceive their impaired ability to walk? One may presume that they would restrict their physical activity levels in accordance to their deteriorated walking capacity. Rather surprisingly, their habitual aerobic activity levels by far exceeded the recommended health-promoting levels at baseline. Their activity levels additionally remained on a stable level during the study period, despite the decline of walking capacity and cognitive function. However, participating in structured exercises such as fitness and strength training in groups or individually was rare in the study group. The reason could be that these kinds of activities might be too chal-lenging for people in the early stages of AD since they require well-functioning executive, attention, and visuospatial functions. Probably, it also reflects a lack of organized exercise activities adapted for people with cogni-tive impairments in the community. In line with this assumption participants revealed that they had stopped doing more complicated physical activities (e.g. swimming in public pools, playing tennis), in favour of outdoor walks (Studies I and IV). Similarly, people with dementia have previously reported a preference for relatively undemanding physical activities such as outdoor walks (Duggan et al., 2008; Malthouse et al., 2013; Olsson et al., 2013).
In contrast to the measured and observed walking deteriorations described previously (see Results Studies I, II, and III) participants did not dwell on impaired walking capacity. Instead, they talked about barriers to being phys-ically active in a wider perspective. Frequently reported barriers were, for example, a decreased energy level, feelings of anxiety and impaired orienta-tion ability (Studies I and IV), which are in accordance with findings report-ed by Duggan et al. (2008). The decreased energy level involved an overall

56
sense of tiredness and difficulty in taking the initiative to undertake activities which, in addition to anxiety was described as a major hindrance to being active. These descriptions reflect common dementia symptoms (APA, 2000; Basun et al., 2013). Moreover, the impaired orientation ability limited the life space of the participants and increased the risk of them getting lost. They described different strategies they used to handle these orientation disabili-ties, for example, the use of specific landmarks on walking routes, only walking in well-known places, avoidance of crowded places, and having company walking. In previous studies, the use of landmarks have been de-scribed by people with dementia as an important strategy to orienteer them-selves in public places (Brorsson et al., 2011), along with the avoidance of specific problematic situations and the company of a caregiver (Duggan et al., 2008).
What was striking was that the participants with AD described and ex-posed a varying walking performance in daily life (Studies I). This was also reported by their spouses. The walking performance could differ markedly from one situation to another. One of the spouses described occasional inci-dences of “peculiar behaviour” in her husband (Study I). In certain situa-tions, he did not seem to notice objects in the environment and, therefore, could walk straight into them (e.g. a lamp post), which probably illustrated his impaired attention, perceptual or visual-spatial functions. This descrip-tion must be viewed in the light of this man’s routine to walk independently to the day-care centre several times a week. During the trip that he normally did on his own, he walked freely through public places and crossed crowded streets safely without any problems. During an observed walk, he gave the impression of being alert and to really enjoy walking. This kind of contradic-tory report concerning a person’s ability to move, mirror the different dual-task (or multiple-task) demands frequently involved in real life situations. Thus, the efficient and safe physical activity performance of people with AD is largely dependent on cognitive and environmental demands attached to a certain situation. A complicated activity that is well-known can function well, whereas a seemingly simple (unaccustomed) activity can imply signifi-cant difficulties. Additionally, a rapidly evolving distraction in a usual ac-tivity can severely interfere with a cognitively impaired person’s perfor-mance. This knowledge can be of great importance for health professionals in relation to the guidance and planning of interventions for people with AD.
Activity-promoting factors It was apparent that the participants had a strong driving force to overcome barriers in favour of sustaining physically active. The question is why they strived to remain physically active in everyday life, and why they committed themselves to outdoor activities. The answer might be that outdoor walks and recreational activities in natural environments are one of the most com-

57
mon leisure time physical activities reported by the Swedish population (FHI, 2010). Additionally, older people undergoing geriatric rehabilitation have strongly emphasized the ability to go out of doors as a key activity for their life satisfaction, irrespective of their physical functioning (Åberg et al., 2005; Åberg, 2008). In line with this, the participants in our studies also had a strong driving force to maintain physically active despite impaired walking capacity, declining cognitive functions, and other perceived barriers (Studies I and IV). Some of the participants needed assistance to take the initiative to go out and needed company for security reasons.
It was evident that the two participating spouses in Study I had a wish to support their husbands to maintain their physical activity routines. The spouses’ positive attitudes were mainly based on their perceptions that their partners benefitted from being physically active, which are opinions that also have been reported previously (Jansson et al., 2001; Pitkala et al., 2013). The spouses’ willingness to support activities and the desire to remain active expressed by the participants with AD (Studies I and IV) can explain why the AD-group reported a relatively high, and stable habitual aerobic activity level during the entire study period, despite limitations and deteriorations of walking and cognition (Study II).
There are several potential explanations for the participants’ positive atti-tudes towards physical activities such as outdoor walks, which may be inter-related. Firstly, in recent years, numerous research reports have focused on the positive effects of aerobic activity on brain structures and, subsequently, on cognitive function and depressive symptoms in older people, people with MCI, and dementia (Bherer et al., 2013; Erickson et al., 2013; Forbes et al., 2013; Tseng et al., 2011). It has been suggested that underlying neurobiolog-ical mechanisms can explain the positive effects. These effects are relatively widespread in the brain even though the prefrontal and hippocampal areas appear to be more influenced (Erickson et al., 2013). One may speculate that the well-being associated with being physically active reported in our studies (I and IV) and previous investigations (Malthouse et al., 2013) are in part results of these physiological effects of aerobic activity of the brain. On the other hand, positive subjective experiences associated with muscle strength exercise interventions among older people depending in activities of daily living, some with a dementia diagnosis, have also been reported to improve quality of life (Lindelöf et al., 2012). However, the studies that have ex-plored subjective experiences of different types of physical activities among people with dementia are scarce and include few participants. The im-portance of exploring these aspects has been highlighted not least to increase adherence to physical activity interventions aimed at maintaining independ-ence and preventing falls without increasing the total cost of health and so-cial services, and without increasing the informal caregivers’ burden (Bowes et al., 2013; Forbes, 2013; Lautenschlager et al., 2010).

58
Secondly, in addition to the potential positive effects of aerobic activity on brain health, it has been proposed that solitude in natural surroundings provides relaxation as well as relief from expectations and stress in cogni-tively healthy people (Daun et al., 1996; Korpela et al., 2001). Furthermore, exercising in natural environments has been associated with improvement in mental well-being compared to exercising indoors (Thompson Coon et al., 2011), and outdoor activities have been emphasised as being relatively un-demanding and, therefore, appreciated by people with dementia (Duggan et al., 2008; Olsson et al., 2013). These findings are supported by our results showing that the participants frequently stressed the importance of going out of doors for achieving general well-being, and for reducing feelings of stress and unease (Studies I and IV). Another aspect related to the fact that AD is a lethal disease is that being in nature, listening to the sounds of nature, enjoy-ing the scenery, and engaging in activities such as walking can be an effec-tive coping strategy to deal with severe illness (Ahmadi et al., 2013; Annerstedt et al., 2011; Gibson, 2007). These examples are in line with what participants in our study expressed as motivating and inspiring factors for being physically active in natural surroundings (Studies I and IV). The data on habitual aerobic activity additionally indicated that outdoor activities were a priority for the participants with AD, as well as for the healthy con-trols (Study II).
Thirdly, in addition to the positive experiences related to movements and outdoor activities reported by the participants, they seemed to have the fun-damental attitude that physical activity in general is good for the body and soul. Their perceptions regarding physical activity appeared to be based on their understanding of societal norms, both written and tacit (Studies I and IV). Additionally, they tended to compare themselves with others who were worse off or less active, which is a strategy described previously (Clare, 2002). We interpreted these attitudes as striving to sustain “normality”, when the dementia posed threats to their selfhood. Correspondingly, people with dementia have previously described how they actively strive to stay “nor-mal” by doing activities they associate with their former (healthy) life (Beattie et al., 2004; Hedman et al., 2013; Phinney, 1998). If the partici-pants’ statements in Study II are reflected in light of the data on aerobic ac-tivity levels, we can confirm that their efforts to maintain a physical activity level in accordance with “ordinary” healthy individuals were successful. On the other hand, a majority of the participants had marked walking capacity limitations, but seemed to regard them as minor, or overlooked them in eve-ryday life. A similar attitude to minimize problems due to the dementia and instead focus on abilities that function quite well has been described in pre-vious research (Caddell et al., 2011; Hedman et al., 2013; Kiyak et al., 1994). This attitude may reflect a deteriorated insight caused by cerebral neurodegeneration, but may also be understood as a strategy to handle the negative consequences of AD. We will discuss this in the next chapter.

59
Selfhood maintenance through physical activity At first sight, one may draw the conclusion that the participants’ preferences for being physically active were driven by a desire to maintain physical functioning and prevent illnesses. Instead, the participants emphasized a general sense of well-being attached to being physically active as their main motivation for maintaining regular physical activity routines (Studies I and II). Their descriptions of well-being involved a positive experience of body movements, nature, and open air. Participants with AD additionally ex-pressed general opinions that one should “keep moving” (Studies I and IV), as did the spouses (Study I). Thus, the maintenance of fitness and independ-ence were not mentioned as specific motivating factors for sustaining a phys-ically active lifestyle. How could we understand the well-being physical activity seemed to bring out in the participants? A significant finding emerged when we made a comprehensive interpretation of the results in the four studies against the backdrop of the theoretical perspectives chosen (Atchley, 1989, 1999; Harré, 1998). We found an underlying common thread, which indicated that, by being active, the participants were engaged in self-protective strategies to maintain normality and continuity in lifestyle and selfhood since AD posed a threat to their selfhood.
As suggested previously, the participants with AD had no difficulties in expressing their self of personal identity (Caddell et al., 2010). However, their self of physical and mental attributes, and their self of social roles had obviously undergone changes since the onset of dementia, which was in accordance with previous findings in the area (Caddell et al., 2010; Hedman et al., 2013). The participants acknowledged a range of alterations due to the dementia disease and told of actions they had taken, often with support from cohabitants, to overcome these barriers. In parallel, they appeared to be en-gaged in balancing self-maintenance with self-adjusting in order to achieve continuity in lifestyle and selfhood. Thus, they were involved in an on-going process of construction and re-construction of selfhood to give prominence to attributes and social roles associated with a past healthy life before they had AD. In this process of sustaining selfhood, physical activities such as outdoor walks appeared to be a significant and powerful tool.
Our interpretation identified several reasons why physical activity might be a specifically appropriate means to overcome the negative consequences on selfhood that AD might bring about. Firstly, physical activity was de-scribed as giving the participants well-being and joy (Studies I and IV), which corresponds with previous findings involving people with dementia (Duggan et al., 2008; Malthouse et al., 2013; Olsson et al., 2013). Secondly, physiological mechanisms that can enhance brain health and reduce stress may also play a part (Bowler et al., 2010; Erickson et al., 2013). Thirdly, regularly performed physical activity is stressed in societal norms as neces-sary for a healthy lifestyle. This was reflected in the participants’ positive

60
statements (Studies I and IV) and actions (Studies I and II) attached to being physically active. Altogether, these factors indicate that the participants per-ceived physical activity as a meaningful activity in daily life. This is in ac-cordance with findings in previous studies involving people with dementia (Duggan et al., 2008; Malthouse et al., 2013), and mental ill-health (Mason et al., 2012). The relatively stable health promoting aerobic activity level in the AD group (Study II) supports this interpretation and can be regarded as the participants’ ambitions to retain continuity in selfhood and in health as-pects linked to their past life.
Corresponding findings demonstrating that people with dementia strive to maintain continuity in life have been previously reported (Menne, 2002; Phinney, 1998; Steeman et al., 2006). Thus, the theoretical perspectives cho-sen (Atchley, 1989, 1999; Harré, 1998) could help to understand their moti-vation to be physically active, despite numerous barriers towards physical activity, such as anxiety, decreased ability to take initiative, and impaired orientation ability. In addition, the theories of selfhood and continuity can explain their statements regarding the importance of adhering to physical activity norms, tendencies to compare themselves to others (who are less active), and prominences given to attributes of themselves related to a good capacity, e.g. “I swim really fast”, “I keep up well” (Studies I and IV).
However, strategies to handle threats to selfhood may be misinterpreted by others as unawareness of dementia-related impairments. Bettie et al. (2004) described this as a tension between a desire in the person with de-mentia to maintain independence, and the caregivers’ perceptions of risks associated with certain situations. In line with this, participants in our Stud-ies (I and IV) stated that they sometimes weighted the risks and benefits in favour of doing an activity they used to do independently, but that now im-plied an element of risk taking. This tension described by Beattie et al. (2004) could also help to understand the contradiction found between the two spouses’ descriptions of their husbands (in)abilities to find their way around and the men’s routines to take long walks on their own. The spouses’ conflicting approaches, which might be viewed as hazardous from an exter-nal perspective, could be interpreted as if they were engaged in actions that support their husbands to remain independent.
The participants were hence able to strengthen their self-image by being physically active and thereby probably minimize the sense of having demen-tia. We noted that the two spouses (Study I) correspondingly supported their husbands in the process of maintaining continuity in selfhood. Thus, it ap-peared that the two men’s physical activity routines had the potential to rein-force also the cohabitants’ health in terms of well-being (Study I). This is consistent with previous findings that supporting a partner with dementia in physical activities can reduce the burden on the caregiver (Söderhamn et al., 2013; Vreugdenhil et al., 2012). The participating spouses in Study I both said that they wanted to support their husbands to have a meaningful every-

61
day life and it was clear that physical activity was also viewed in a meaning-ful way by the cohabitants. It is possible that physical activity helped the two men with AD to hold on to a social role associated with their old familiar self by their spouses, which may also have been vital for their interrelation-ships (Åberg et al., 2004).
To sum up, being physically active can be a strategy for people in the ear-ly stages of AD to shift focus from the social persona, “a dementia patient”, to a (physically) capable person, although with some cognitive impairments. People with AD who remain physically active may thereby gain “self-promotion benefits” in addition to the common “health-promoting benefits”. This may be one of the most important potential benefits of physical activity, as dementia severely threatens continuity in a person’s selfhood and life. Therefore, health professionals and informal caregivers should take into account the self-protective strategies that individuals with AD may be in-volved in and assist them to maintain normality and continuity in selfhood by supporting them to engage in meaningful undemanding physical activi-ties.

62
Main conclusions
A relatively simple cognitive task, i.e. naming animals, can have a sub-stantial impact on walking, even in mild AD. Additionally, specific dual-task gait disturbances during testing are frequent in this group. Such gait disturbances occur occasionally, are irregular, and possess different characteristics, i.e. temporal, spatial, and instable. Therefore, combining a cognitive task with a complex motor task such as the TUG test appears to be a sensitive test for detecting the early signs of cognitive impair-ment in clinical settings (Studies II and III).
Physical activity can be a meaningful activity that contributes to a conti-nuity of self and life for people with AD. The sense of meaning is sup-ported by written and tacit common norms about physical activity as well as experiences of well-being related to being physically active. Physical activities, in particular, those performed outdoors can be used by people with AD as a means to sustain their well-being and selfhood, and informal caregivers appear positive towards supporting them in this. Thus, beyond the common health-promoting benefits, people with AD can also gain “self-promoting benefits” from physical activity (Studies I, II, and IV).
Multi-perspective investigations by the use of mixed methods research
can generate valuable knowledge about physical activity and AD; knowledge contributing to a holistic picture of difficulties and possibili-ties related to being physically active, despite a dementia diagnosis (Studies I, II, III, and IV).

63
Clinical reflections
Can we use performance-based tests? The TUG test has been considered as a test of basic mobility, useful in the follow-up of clinical change over time (Podsiadlo et al., 1991), and for iden-tifying community-dwelling adults who are at risk of falls (Shumway-Cook et al., 2000). However, our results (Studies II and III) highlight the need to clarify whether the results of walking capacity tests in the early stages of AD, primarily reflect cognitive impairments or not (Study II). Namely, our findings demonstrate that the use of verbal cueing is an issue even when testing people with mild dementia (MMSE score 21-30 p). For this reason, evaluating physical activity interventions by performance-based tests should be carried out with cautiousness. Otherwise, there is a risk that the physical benefits achieved from a physical exercise intervention may not be captured because of the impact of the impaired cognitive function (Rockwood et al., 2000). However, if the intention is to evaluate dual-task ability specifically, the TUG might be feasible, but needs to be investigated in further studies.
The question to what extent verbal cueing is used in reality, and how this influences validity has been highlighted previously by Nordin et al. (2006), and should be considered in both the clinical setting and research. Van Iersel et al. (2007) and Ries et al. (2009) stressed that verbal cueing should be used when necessary in patients with dementia. In contrast, Hauer et al. (2008) stated that, when verbal cueing is needed, the patients’ results probably doc-ument the quality and quantity of the external cueing, not their walking ca-pacity. Our experience is that it is specifically important to identify if verbal cueing is given to encourage individuals to “keep going” if they walk slowly, hesitate or make occasional stops. In these cases, the validity of the test can be severely jeopardized. Our experiences are in line with those reported by Rockwood et al. (2000) and Pitkälä et al. (2013). Pitkälä et al. used a per-formance-based test, the Short Physical Performance Battery (SPPB) (Guralnik et al., 1994) in an intervention study and the community-dwelling participants with AD had problems following the instructions properly. Therefore, the SPPB mobility test was proven to be infeasible for them.
On the other hand, the distinct impact of a cognitive task on the perfor-mance of the TUG test, indicates that the TUG test (including dual-task test-ing) can be a sensitive test for detecting the early signs of cognitive impair-ment (Studies II and III). These thoughts correspond with Yogev et al.

64
(2008) who suggest that assessment of dual-task walking abilities, and exec-utive function should become a part of the routine examination among neu-rological patients to more fully evaluate gait disturbances and fall risk. In order to implement prevention strategies, the TUG test (including the dual-task test) may be a feasible screening test for physiotherapists in, for exam-ple, primary care and the community to identify individuals who are at in-creased risk of functional decline and falls. Based on our findings (Studies II and III), we suggest that in such testing focus should be placed on both the dual-task cost and the qualitative aspects, e.g. the need for verbal cueing and the prevalence of dual-task gait disturbances. However, further investigation is necessary to establish this.
One may speculate if it would be more accurate to evaluate exercise in-terventions designed for people with cognitive impairments with tests of body functions (e.g. cardiorespiratory fitness, muscle strength) in order to minimize the influence of their cognitive impairments on test results. We know from previous studies that people with dementia can manage to per-form for example cardiorespiratory testing on a tread mill (Billinger et al., 2011; Burns et al., 2008), or on a stationary cycle (Yu et al., 2011), and test of leg muscle strength by one repetition maximum test in leg-press (Hauer et al., 2012; Rosendahl et al., 2006). These types of measurements do not re-quire a large amount of cognitive ability, but reflect a general picture of fit-ness and physical capacity states, which are a prerequisite for physical func-tioning and independence.
Physical activity as a means to self-promotion Our findings place emphasis on the fact that people with early-stage AD may strive to maintain a physically active state for reasons that have not been previously highlighted by health care professionals. Commonly articulated motives for older people to be physically active are, for example, maintained muscle strength, independence in daily life, and a reduced risk of illnesses such as heart diseases and diabetes. It was clear in our study group that maintenance of fitness was not a significant reason for being physically ac-tive, instead, sustained well-being and selfhood were interpreted to be the main motives for the participants with AD to stay physically active.
Furthermore, our findings show that physical activities such as walking are feasible and viewed as meaningful by individuals with early-stage AD. Our findings and research over recent years demonstrate, on the one hand, the importance of a well-functioning cognitive function (especially executive and attention functions) to walk safely, and on the other hand, the benefits of aerobic activity on brain health (specifically executive functions). Altogeth-er, this shows that a new approach towards rehabilitation for individuals with AD, embracing aerobic activity is warranted.

65
A consequence of this reasoning is that physical activity should not be of-fered a limited period of time with the intention to improve fitness or reach a certain goal. Instead, health care professionals should support the person in being regularly active with physical activities they appreciate and attach to their past healthy life before they had AD. Thereby, the person might be able to maintain selfhood despite changes due to the dementia. This is in line with the common core principles for supporting people with dementia (e.g. to promote independence and encourage activity) proposed by WHO (2012).
An important aspect is the vast lack of structured activities in the commu-nity designed to meet people with impaired cognitive function who have the desire and capability for high intensity exercise. This will be a much larger problem in the future when people who are used to take part in, for example, fitness and muscle strength exercises for gaining general well-being, will reach the ages when the risk of dementia is a reality. Younger people with dementia have expressed an overwhelming need for activities appropriate for their age (Beattie et al., 2004). Have physiotherapists and other health pro-fessionals developed any strategies to meet their needs?
Is “self-promoting” by using physical activity an issue for physiothera-pists? I would say “Yes”. According to the World Confederation for Physi-cal Therapy (2011), physiotherapy is concerned with identifying and maxim-izing quality of life and movement potential in the fields of promotion and prevention, which comprises physical, psychological, emotional and social well-being. Moreover, rehabilitation, which is central for physiotherapists, is aimed at enabling people with disabilities to “maintain their optimal physi-cal, sensory, intellectual, psychological and social functional levels” (WHO, 2014). Thus, physical activity as a means for people with dementia to sustain well-being and selfhood should indeed be an issue for physiotherapists and other health professionals and should be an interesting focus in future re-search.

66
Sammanfattning på svenska (Summary in Swedish)
Bakgrund Personer med Alzheimers sjukdom (AD) har redan tidigt i sjukdomsförlop-pet ett långsammare, instabilare gångmönster än kognitivt friska individer. Orsakerna är inte klarlagda, men på senare år har väl fungerande kognitiva funktioner uppmärksammats som avgörande för att förflytta sig säkert i var-dagslivet. Exekutiva funktioner (att planera och genomföra en uppgift) och uppmärksamhetsfunktioner tros ha särskilt stor betydelse för att gå säkert och stabilt. Störningar i förmågan att dela uppmärksamheten mellan att gå och utföra en kognitiv uppgift (s k dual-tasking) ökar risken för fallinciden-ter och har påvisats hos personer med mild AD.
Även nedsättning av andra kognitiva funktioner som förekommer vid AD kan inverka negativt på förmågan att vara fysiskt aktiv, till exempel försäm-rad förmåga att orientera sig geografiskt. Känslomässiga reaktioner till följd av AD kan även det påverka aktivitetsnivån negativt.
Personer med AD riskerar således att få en alltför låg fysisk aktivitetsnivå och därmed att fysiska funktioner försämras, beroende tidigareläggs och livslängden förkortas. Regelbunden fysisk aktivitet rekommenderas därför för personer med demenssjukdom, men många behöver redan tidigt i sjuk-domsförloppet praktiskt stöd för att kunna utöva aktiviteter. Dessutom är det stor brist på träningsaktiviteter i samhället som är anpassade för personer med kognitiv nedsättning. För att möta deras behov av att träna och röra sig i vardagen behöver kunskapen öka om vilka begränsningar och förutsättningar de har för att vara fysiskt aktiva.
Det övergripande syftet med denna avhandling var därför att studera hur förmågan att vara fysiskt aktiv påverkas under två år i tidigt skede av AD. Dessutom var syftet att få förståelse för hur personer med AD och deras anhöriga resonerar kring fysisk aktivitet som en del i vardagen.
Metod och resultat Forskningsansatsen var explorativ och inspirerad av flermetodsforskning (s.k. mixed methods research). Både textdata och numerisk data samlades därför in parallellt för att belysa olika aspekter av fysisk aktivitet vid AD. Deltagarna med AD rekryterades från Minnes- och geriatrikmottagningen på Akademiska sjukhuset. Alla deltagare med AD uppfyllde gällande forsk-

67
ningskriterier för trolig AD. De hade vid studiens start mild AD (Mini Men-tal Test (MMT) 21-30 poäng), var mellan 55-79 år gamla, sammanboende i eget boende, och kunde gå utan hjälpmedel. Ingen av deltagarna hade någon annan sjukdom eller skada som påtagligt påverkade gångförmågan negativt.
Studie I En fallstudie där två par inkluderades. Männen i respektive par hade mild AD. Data samlades in med individuella djupintervjuer och delta-gande observationer. Två intervjuer och två deltagande observationer utför-des med respektive man med AD, och en intervju vardera med de båda ma-karna. Analys av textdata från intervjuer och observationer, analyserades med tematisk analys. Fysisk aktivitet i form av utomhuspromenader upplevdes som en betydelsefull rutin. Trots att flera demensrelaterade faktorer hindrade aktivitet, var deltagarna motiverade att använda anpassningsstrategier för att möjliggöra att männen med AD var fysiskt aktiva i vardagen. Både de två männen och deras makar beskrev att utomhuspromenaderna främjade deras hälsa och välbefinnande. Denna stu-die är att betrakta som en pilotstudie för planering och genomförande av Studie II-IV.
Studie II Vid baslinjen jämfördes 25 personer med AD med 25 kognitivt friska personer för att få en bild av AD-gruppens fysiska nivå. Personerna med AD följdes därefter under två år och data samlades in vid baslinje, efter ett och efter två år. 22 personer fullföljde den studien. Data avseende gång-kapacitet samlades in med kliniska tester (10 m bekväm gånghastighet, 6-minuters gång, Timed Up-and-Go (TUG) single- och dual task), fysisk akti-vitetsnivå med dagboksregistrering av anhöriga (eller under deras överinse-ende), och fallincidenter med rapport från anhöriga. Redan vid baslinjemätningen hade deltagarna med AD en nedsatt gångkapacitet jämfört med kontrollgruppen . Försämringen fortsatte under studiens två år. Särskilt framträdande var att gången påverkades påtagligt negativt av en samtidig kognitiv uppgift. Trots denna försämring var deltagarnas fysiska aktivitetsnivå jämförbar med kognitivt friska personer vid baslinjen, och förändrade inte nämnvärt under studietiden. Flertalet i AD-gruppen uppfyllde de gällande hälsorekommendationerna för aerob aktivitet (150 minuter/veckan).
Studie III Gånganalys i motoriklaboratorium genomfördes med deltagarna med AD för att identifiera skillnader i gångparametrar vid vanlig gång jäm-fört med gång då en kognitiv uppgift utfördes simultant (dual-tasking). Data-insamling utfördes vid baslinjen, efter ett och efter två år. 21 deltagare med AD fullföljde studien. Ett optiskt motion capture system (ProReflex, Quali-sys AB, Göteborg) användes. Förutom insamling av numerisk data om gångparametrar, gjordes en systematisk visuell analys av rörelsefilerna för att identifiera eventuella störningar i gångmönster. Gånghastigheten vid gång med samtidig kognitiv uppgift var redan vid baslinjen signifikant långsam-mare än hastighet vid vanlig gång, men ingen säker förändring av hastighets-skillnaden (dual-task cost) kunde ses under tvåårsperioden. Specifika gång-

68
störningar som förekom oregelbundet och endast under ”dual-tasking” iden-tifierades dessutom.
Studie IV Ett strategiskt urval av 14 personer gjordes från de 25 perso-nerna inkluderade i Studie II och III. En bred variation med avseende på bland annat aktivitetsnivå och självständighet eftersträvades i urvalet. Indi-viduella djupintervjuer gjordes med var och en av deltagarna vid två till-fällen inom en månads tid. Analys av textdata utfördes med kvalitativ inne-hållsanalys.
Fysisk aktivitet i vardagen beskrevs som en meningsfull aktivitet som gav kontinuitet i livet. Personerna med AD tycktes använda fysisk aktivitet för att stödja sitt välbefinnande och sin “jag-upplevelse” genom att fokusera på kapabla aspekter i sin person. Deras uppfattningar om normer och känsla av välbefinnade relaterade till fysisk aktivitet tolkades vara viktiga drivkrafter i denna process.
Slutsats Resultaten visar att gångförmågan är nedsatt hos personer med mild AD och fortsätter att försämras de följande åren. En enkel kognitiv uppgift kan ha en betydande negativ påverkan på gången redan vid mild AD. Det indikerar att testning av ”dual-tasking” med TUG skulle kunna vara en metod för att i klinik identifiera personer med kognitiv svikt. Trots dessa försämringar av gångförmågan tyder våra resultat på att personer med AD kan bibehålla en hälsofrämjande nivå av fysisk aktivitet. Dessutom kan fysisk aktivitet, sär-skilt utomhusaktiviteter, användas av dem inte bara för att främja fysisk hälsa, utan även som ett medel för att stärka välbefinnandet och upplevelser av ”jaget” som förknippas med hälsa och kontinuitet i livet.

69
Acknowledgements
Ni är många personer som på olika sätt har bidragit till att jag har kunnat genomföra min doktorandutbildning. Jag känner en stor tacksamhet mot er alla. Framför allt vill jag rikta ett varmt tack till deltagare, och anhöriga, som så generöst delade med sig av sin tid, sina tankar och erfarenheter. Utan ert engagemang hade denna forskning inte kunnat genomföras.
Jag vill också rikta ett särskilt tack till: Anna Cristina Åberg, min huvudhandledare, för din tro på mig och projektet, för att du lotsade mig in i forskningens snåriga värld, för din entusiasm, för intressanta diskussioner, och för alla inspirerande och roliga resor vi har gjort tillsammans. Ditt kunnande, engagemang och stöd är grunden för den här avhandlingen. Lars Lannfelt, professor i geriatrik, min handledare, för att du gjorde det möjligt för mig att bli doktorand, för ditt intresse, och för att du generöst delar med dig av dina erfarenheter. Jag har uppskattat våra samtal. Lena Kilander, min handledare, medförfattare i Studie II, för att du så själv-klart delar med dig av ditt gedigna kunnande inom demensområdet, för vär-defulla och klarsynta kommentarer på texter, och för uppmuntran under åren. Kjartan Halvorsen, medförfattare i Studie III, för gott samarbete och för att ditt tekniska kunnande tillförde något alldeles extra till studien. Sandra Torres, medförfattare i Studie IV, för inspirerande samarbete, för att du delade med dig av ditt stora kunnande och introducerade selfhood- och personhood-begreppen för mig. Margareta Falkeborn, tidigare verksamhetschef, och Lena Stigsdotter, nuva-rande verksamhetschef på Geriatriken, Akademiska sjukhuset för ert intresse och stöd. Susanna Tuvemo Johnson, min tidigare chef på Geriatrikens sjukgymnastik, Christine Bengtsson nuvarande chef, Jenny Boija Bennbom och Maria Knutsson Karlsson tidigare gruppchefer, Febe Sandqvist nuvarande grupp-

70
chef, för att ni så självklart har gjort det möjligt för mig att kombinera forsk-ning med kliniskt arbete under hela min doktorandtid. Catarina Färnstrand, för att du introducerade mig i motoriklabbet. Olga Tarassova för gott samarbete under datainsamling. Gunilla Elmgren Fryk-berg för roligt och inspirerande samarbete under huvudparten av datain-samlingen i motoriklabbet och för att du processade all data. Gunnel Cedervall, för noggrann och effektiv inmatning av all motoriklabs-data. Lars Berglund, för skicklig statistisk rådgivning. Ulla Nergård, för noggrann transkribering av mer än 100 djupintervjuer och Christina Ner-gård, för att du ordnade alla praktiska bestyr i samband med det. David De Boniface, and the late Maud Marsden for excellent linguistic revi-sions. Doktorander, forskare och andra kollegor på 14 B, för många roliga stunder och intressant prat i samband med dagens två höjdpunkter, fika och lunch. Tack också för er omtanke när det ibland har känts motigt. Breiffni Leavy, för att du räddat mig i språkliga nödsituationer (mer än en gång), men mest av allt för alla pratstunder, uppmuntran och glada skratt. Kristin Franzon och Malin Degerman Gunnarsson, mina rumskompisar det sista året, för behöv-liga och trevliga avbrott i forskningen med småprat om allt och inget. Vil-mantas Giedraitis, för att du alltid snabbt och självklart hjälper till när datorn trasslar. Doktorandkollegor och seniora forskare på Institutionen för folkhälso- och vårdvetenskap, för givande och intressanta diskussioner på seminarier, och för värdefulla råd om delarbeten och kappor. Doktorandkollegor och seniora forskare på Institutionen för neurovetenskap/fysioterapi, för givande och värdefulla diskussioner på seminarier. Doktorandkollegor från hela Sverige, för givande diskussioner och inspirerande möten på doktorandkurser i Jön-köping och Lund. Kollegor av olika slag som har gett värdefulla synpunkter på Kappan. Nina Mellberg och Birgitta Ohlson för att ni tog er tid att granska det sista utkastet så noggrant som bara ni kan. Mina arbetskamrater på Geriatrikens sjukgymnastik, för att ni tålmodigt stått ut med att jag inte alltid varit närvarande under doktorandtiden, för att ni alltid varit välkomnande och intresserade när vi har träffats, för alla roliga stunder, och inte minst för er omtanke. Jag har verkligen uppskattat att träffa er alla på fredagsfikan. Susanne Friman Vestlund, för att du med kort varsel

71
kunde gå in som sjukgymnast i Minnesteamet när jag behövde all tid för att skriva klart den här avhandlingen. Mina kollegor i Minnesteamet för inspirerande samarbete och för allt jag lär mig av er om demens och allt som hör till det. Tack också för ert intresse och stöd. Mina vänner utanför forskar- och arbetslivet (flera av er också mina kolle-gor) och mina släktingar, för att ni ger mig glädje, trygghet och kraft i livet. En stor varm kram till er alla! Mina föräldrar, min syster och bror med familjer, för ert aldrig sviktande intresse och stöd. Till sist, de som betyder allra mest för mig, Arvid, Gunnel, och Björn, för allt jag får uppleva tack vare er, för att ni är just de ni är ♥ ♥ ♥. Svante, min man och bästa vän, för all praktisk hjälp, kloka tankar, och för alla roliga år tillsammans, för allt ♥ Detta arbete finansierades med stöd från (i alfabetisk ordning): Agnes och Georg Johanssons stiftelse, Akademiska sjukhuset, Astrid Karlssons testa-mente, Demensfonden, Emma Petterssons testamente, Minnesfonden (Fysio-terapeuterna), Novartis, Sektionen för Äldres hälsa (Fysioterapeuterna), Stif-telsen Fondkistan, Stiftelsen för gamla tjänarinnor, Thuréus stiftelse för främjande av geriatrisk forskning, Uppsala Hemsysterskolas fond, Uppsala läns landsting, Uppsala universitet.
Uppsala, Maj 2014 Ylva Cedervall

72
References
Ahmadi, F., & Ahmadi, N. (2013). Nature as the Most Important Coping Strategy Among Cancer Patients: A Swedish Survey. J Relig Health. doi: 10.1007/s10943-013-9810-2
Ainsworth, B. E., Haskell, W. L., Leon, A. S., Jacobs, D. R., Jr., Montoye, H. J., Sallis, J. F., & Paffenbarger, R. S., Jr. (1993). Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc, 25(1), 71-80.
Ainsworth, B. E., Haskell, W. L., Whitt, M. C., Irwin, M. L., Swartz, A. M., Strath, S. J., & Leon, A. S. (2000). Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc, 32(9 Suppl), S498-504.
Alexander, N. B., Mollo, J. M., Giordani, B., Ashton-Miller, J. A., Schultz, A. B., Grunawalt, J. A., & Foster, N. L. (1995). Maintenance of balance, gait patterns, and obstacle clearance in Alzheimer's disease. Neurology, 45(5), 908-914.
Allali, G., Assal, F., Kressig, R. W., Dubost, V., Herrmann, F. R., & Beauchet, O. (2008). Impact of impaired executive function on gait stability. Dement Geriatr Cogn Disord, 26(4), 364-369.
Andrew, S., & Halcomb, E. J. (2009). Mixed methods research for nursing and the health sciences. Chichester, U.K.: Wiley-Blackwell Pub.
Annerstedt, M., & Wahrborg, P. (2011). Nature-assisted therapy: systematic review of controlled and observational studies. Scand J Public Health, 39(4), 371-388. doi: 10.1177/1403494810396400
APA. (2000). Diagnostic and statistical manual of mental disorders. 4th Ed. Text revision (DSM-IV-TR). Washington, DC: American Psychiatric Press.
Atchley, R. C. (1989). A continuity theory of normal aging. Gerontologist, 29(2), 183-190.
Atchley, R. C. (1999). Continuity and adaptation in aging : creating positive experiences. Baltimore, MD: Johns Hopkins University Press.
Basun, H., Skog, M., Wahlund, L. O., & Wijk, H. (2013). Boken om demens-sjukdomar (The book of dementia illnesses) (1st ed.). Stockholm, Sweden: Liber.
Bean, J. F., Kiely, D. K., Leveille, S. G., Herman, S., Huynh, C., Fielding, R., & Frontera, W. (2002). The 6-minute walk test in mobility-limited elders: what is being measured? J Gerontol A Biol Sci Med Sci, 57(11), M751-756.
Beard, R. L., Fetterman, D. J., Wu, B., & Bryant, L. (2009). The two voices of Alzheimer's: attitudes toward brain health by diagnosed individuals and support persons. Gerontologist, 49 Suppl 1, S40-49.
Beattie, A., Daker-White, G., Gilliard, J., & Means, R. (2004). 'How can they tell?' A qualitative study of the views of younger people about their dementia and dementia care services. Health Soc Care Community, 12(4), 359-368.

73
Beauchet, O., Annweiler, C., Dubost, V., Allali, G., Kressig, R. W., Bridenbaugh, S., Herrmann, F. R. (2009). Stops walking when talking: a predictor of falls in older adults? Eur J Neurol, 16(7), 786-795.
Bherer, L., Erickson, K. I., & Liu-Ambrose, T. (2013). A Review of the Effects of Physical Activity and Exercise on Cognitive and Brain Functions in Older Adults. J Aging Res, 2013, 657508. doi: 10.1155/2013/657508
Blankevoort, C. G., van Heuvelen, M. J., Boersma, F., Luning, H., de Jong, J., & Scherder, E. J. (2010). Review of Effects of Physical Activity on Strength, Balance, Mobility and ADL Performance in Elderly Subjects with Dementia. Dement Geriatr Cogn Disord, 30(5), 392-402.
Bowes, A., Dawson, A., Jepson, R., & McCabe, L. (2013). Physical activity for people with dementia: a scoping study. BMC Geriatr, 13, 129. doi: 10.1186/1471-2318-13-129
Bowler, D. E., Buyung-Ali, L. M., Knight, T. M., & Pullin, A. S. (2010). A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health, 10, 456. doi: 10.1186/1471-2458-10-456
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
Brorsson, A., Öhman, A., Lundberg, S., & Nygård, L. (2011). Accessibility in public space as perceived by people with Alzheimer's disease. Dementia, 10(4), 587-602. doi: 10.1177/1471301211415314
Bryman, A. (2004). Social Research Methods (2 ed.). Oxford: Oxford University Press.
Buchner, D. M., & Larson, E. B. (1987). Falls and fractures in patients with Alzheimer-type dementia. JAMA, 257(11), 1492-1495.
Burns, J. M., Mayo, M. S., Anderson, H. S., Smith, H. J., & Donnelly, J. E. (2008). Cardiorespiratory fitness in early-stage Alzheimer disease. Alzheimer Dis Assoc Disord, 22(1), 39-46.
Caddell, L. S., & Clare, L. (2010). The impact of dementia on self and identity: a systematic review. Clin Psychol Rev, 30(1), 113-126. doi: 10.1016/j.cpr.2009.10.003
Caddell, L. S., & Clare, L. (2011). I'm still the same person: The impact of early-stage dementia on identity. Dementia, 10(3), 379-398.
Camicioli, R., Howieson, D., Lehman, S., & Kaye, J. (1997). Talking while walking: the effect of a dual task in aging and Alzheimer's disease. Neurology, 48(4), 955-958.
Canonici, A. P., Andrade, L. P., Gobbi, S., Santos-Galduroz, R. F., Gobbi, L. T., & Stella, F. (2012). Functional dependence and caregiver burden in Alzheimer's disease: a controlled trial on the benefits of motor intervention. Psychogeriatrics, 12(3), 186-192. doi: 10.1111/j.1479-8301.2012.00407.x
Caspersen, C. J., Powell, K. E., & Christenson, G. M. (1985). Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep, 100(2), 126-131.
Clare, L. (2002). We'll fight it as long as we can: coping with the onset of Alzheimer's disease. Aging Ment Health, 6(2), 139-148. doi: 10.1080/13607860220126826
Clare, L. (2003). Managing threats to self: awareness in early stage Alzheimer's disease. Soc Sci Med, 57(6), 1017-1029.
Colcombe, S. J., Erickson, K. I., Scalf, P. E., Kim, J. S., Prakash, R., McAuley, E., . . . Kramer, A. F. (2006). Aerobic exercise training increases brain volume in aging humans. J Gerontol A Biol Sci Med Sci, 61(11), 1166-1170.

74
Cook, C., Fay, S., & Rockwood, K. (2008). Decreased initiation of usual activities in people with mild-to-moderate Alzheimer's disease: a descriptive analysis from the VISTA clinical trial. Int Psychogeriatr, 20(5), 952-963.
Creswell, J. W. (2007). Qualitative inquiry and research design: Choosing among five approaches. London, United Kingdom: Sage Publications Ltd.
Creswell, J. W. (2009). Research design: Qualitative, quantitative, and mixed methods approaches (3rd ed.). London , UK: SAGE.
Danielsson, E. (2012). Kvalitativ innehållsanalys (Qualitative content analysis). In M. Henricson (Ed.), Vetenskaplig teori och metod, från idé till examination inom omvårdnad (Scientific theory and method) (1 ed., Chapter 19): Studentlitteratur AB.
Daun, Å., & Teeland, J. (1996). Swedish Mentality (pp. 76-80). University Park, Pa.: Pennsylvania State Univ. Press.
Duggan, S., Blackman, T., Martyr, A., & Van Schaik, P. (2008). The impact of early dementia on outdoor life: A ‘shrinking world’. Dementia, 7(2), 191-204. doi: 10.1177/1471301208091158
Eggermont, L. H., Gavett, B. E., Volkers, K. M., Blankevoort, C. G., Scherder, E. J., Jefferson, A. L., Stern, R. A. (2010). Lower-extremity function in cognitively healthy aging, mild cognitive impairment, and Alzheimer's disease. Arch Phys Med Rehabil, 91(4), 584-588.
Erickson, K. I., Voss, M. W., Prakash, R. S., Basak, C., Szabo, A., Chaddock, L., Kramer, A. F. (2011). Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A, 108(7), 3017-3022.
Erickson, K. I., Gildengers, A. G., & Butters, M. A. (2013). Physical activity and brain plasticity in late adulthood. Dialogues Clin Neurosci, 15(1), 99-108.
Feinberg, L. F., & Whitlatch, C. J. (2001). Are persons with cognitive impairment able to state consistent choices? [Research Support, Non-U.S. Gov't]. Gerontologist, 41(3), 374-382.
FHI-Statens folkhälsoinstitut. (2010). (The Swedish National Institute of Public Health). Levnadsvanor, lägesrapport 2010 (Living habits, report 2010): Statens folkhälsoinstitut.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res, 12(3), 189-198.
Forbes, D., Thiessen, E., Blake, C., Forbes, S., & Forbes, S. (2013). Exercise program for people with dementia. Cochrane Database Syst rev(11:CD006489).
Freedman, M., & Leach, L. (1994). Clock Drawing: A Neuropsychological Analysis. New York: Oxford University Press Inc.
FYSS (2008). Fysisk aktivitet i sjukdomsprevention och sjukdomsbehandling (Phy-sical activity in the prevention and treatment of disease). - Statens Folkhälsoinstitut & Yrkesföreningar för fysisk aktivitet. (The Swedish National Institute of Public Health). Retrieved from http://www.folkhalsomyndigheten.se/publicerat-material/publikationer/FYSS-2008/
Föllesdal, D. (1994). Hermeneutics and the Hypothetic-Deductive Method. In M. Martin & L. McIntyre (Eds.), Readings in the Philosophy of Social Science: Bradford Book, the MIT Press.
Gibson, G. (2007). Housing and connection to nature for people with dementia. . Journal of Housing For the Elderly, 21(1-2), 55-72.
Gleason, C. E., Gangnon, R. E., Fischer, B. L., & Mahoney, J. E. (2009). Increased risk for falling associated with subtle cognitive impairment: secondary analysis of a randomized clinical trial. Dement Geriatr Cogn Disord, 27(6), 557-563.

75
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today, 24(2), 105-112.
Gruffydd, E., & Randle, J. (2006). Alzheimer's disease and the psychosocial burden for caregivers. Community Pract, 79(1), 15-18.
Grön, A., Husted, J., Lubeck, P., Rasmussen, S. A., Sandöe, P., Stefansen, N. C., & Bengtsson, J. (1988). Filosofilexikonet, filosofer och filosofiska begrepp från A till Ö (The philosophy dictionary, philosophers, philosophical concepts from A to Ö) (J. Hartman, Trans. 1 ed.). Stockholm: Bokförlaget Forum.
Guralnik, J. M., Simonsick, E. M., Ferrucci, L., Glynn, R. J., Berkman, L. F., Blazer, D. G., Wallace, R. B. (1994). A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol, 49(2), M85-94.
Harré, R. (1998). The singular self: An introduction to the psychology of personhood. London, UK: Sage.
Hauer, K., & Oster, P. (2008). Measuring functional performance in persons with dementia. J Am Geriatr Soc, 56(5), 949-950. doi: 10.1111/j.1532-5415.2008.01649.x
Hauer, K., Schwenk, M., Zieschang, T., Essig, M., Becker, C., & Oster, P. (2012). Physical training improves motor performance in people with dementia: a randomized controlled trial. J Am Geriatr Soc, 60(1), 8-15. doi: 10.1111/j.1532-5415.2011.03778.x
Hausdorff, J. M. (2005). Gait variability: methods, modeling and meaning. J Neuroeng Rehabil, 2, 19. doi: 10.1186/1743-0003-2-19
Hausdorff, J. M., Yogev, G., Springer, S., Simon, E. S., & Giladi, N. (2005). Walking is more like catching than tapping: gait in the elderly as a complex cognitive task. Exp Brain Res, 164(4), 541-548.
Hedman, R., Hansebo, G., Ternestedt, B. M., Hellström, I., & Norberg, A. (2013). How people with Alzheimer's disease express their sense of self: Analysis using Rom Harre's theory of selfhood. Dementia (London), 12(6), 713-733. doi: 10.1177/1471301212444053
Hellström, I., Nolan, M., Nordenfelt, L., & Lundh, U. (2007). Ethical and methodological issues in interviewing persons with dementia. Nurs Ethics, 14(5), 608-619. doi: 10.1177/0969733007080206
Heyn, P., Abreu, B. C., & Ottenbacher, K. J. (2004). The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil, 85(10), 1694-1704.
Horak, F. B., Wrisley, D. M., & Frank, J. (2009). The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits. Phys Ther, 89(5), 484-498.
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qual Health Res, 15(9), 1277-1288. doi: 10.1177/1049732305276687
Husband, H. J. (2000). Diagnostic disclosure in dementia: an opportunity for intervention? Int J Geriatr Psychiatry, 15(6), 544-547.
Ijmker, T., & Lamoth, C. J. (2011). Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture.
Ijmker, T., & Lamoth, C. J. (2012). Gait and cognition: the relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture, 35(1), 126-130. doi: 10.1016/j.gaitpost.2011.08.022
Jansson, W., Nordberg, G., & Grafström, M. (2001). Patterns of elderly spousal caregiving in dementia care: an observational study. J Adv Nurs, 34(6), 804-812.

76
Johnson, B. J., & Onwuegbuzie, A. J. (2004). Mixed Methods research: A Research Paradigm Whose Time Has Come. Educational Researcher(33), 14-26.
Kaplan, S. (1995). The restorative benefits of nature: Towards an integrative framework. Journal of Environmental Psychology 15(3), 169-182.
Kelly, F. (2010). Recognising and supporting self in dementia. a new way to facilitate a person-centered approach to dementia care. Ageing and Society, 30(01), 103-124.
Kirtley, C. (2009). Clinical Gait Analysis, Theory and Practice. London: Churchill Livingstone Elsevier.
Kitwood, T. (1997). Dementia Reconcidered: the Person Comes First. Philadelphia: Open University Press.
Kiyak, H. A., Teri, L., & Borson, S. (1994). Physical and functional health assessment in normal aging and in Alzheimer's disease: self-reports vs family reports. Gerontologist, 34(3), 324-330.
Korpela, K. M., Hartig, T., Kaiser, F. G., & Fuhrer, U. (2001). Restorative Experience and Self-Regulation in Favorite Places. Environment and Behavior, 33, 572-589.
Lamb SE, Jorstad-Stein EC, Hauer K, Becker C. (2005). Development of common outcome data set for fall injury prevention trials: the Prevention of Falls Net-work Europe consensus. J Am Geriatr Soc 53,1618-1622.
Lautenschlager, N. T., Cox, K., & Kurz, A. F. (2010). Physical activity and mild cognitive impairment and Alzheimer's disease. Curr Neurol Neurosci Rep, 10(5), 352-358.
Lezak, M. (1995). Neuropsychological assessment (3.ed ed.). New York: Oxford Univ. Press.
Lindelöf, N., Karlsson, S., & Lundman, B. (2012). Experiences of a high-intensity functional exercise programme among older people dependent in activities of daily living. Physiother Theory Pract. doi: 10.3109/09593985.2011.611217
Lundin-Olsson, L., Nyberg, L., & Gustavsson, Y. (1997). “Stops walking when talking” as a predictor of falls in elderly people. Lancet Neurol.
Lundman, B., & Graneheim, U. H. (2008). Kvalitativ innehållsanalys (Qualitative content analysis). In M. Granskär & B. Höglund-Nilsen (Eds.), Tillämpad forskning inom hälso- och sjukvård (Applied research in health care) (Chapter 10): Studentlitteratur.
Malthouse, R., & Fox, F. (2013). Exploring experiences of physical activity among people with Alzheimer's disease and their spouse carers: a qualitative study. Physiotherapy. doi: http://dx.doi.org/doi:10.1016/j.physio.2013.10.002
Maquet, D., Lekeu, F., Warzee, E., Gillain, S., Wojtasik, V., Salmon, E., Croisier, J. L. (2010). Gait analysis in elderly adult patients with mild cognitive impairment and patients with mild Alzheimer's disease: simple versus dual task: a preliminary report. Clin Physiol Funct Imaging, 30(1), 51-56.
Mason, O. J., & Holt, R. (2012). Mental health and physical activity interventions: a review of the qualitative literature. J Ment Health, 21(3), 274-284. doi: 10.3109/09638237.2011.648344
McCurry, S. M., Pike, K. C., Logsdon, R. G., Vitiello, M. V., Larson, E. B., & Teri, L. (2011). Predictors of short- and long-term adherence to a daily walking program in persons with Alzheimer's disease. Am J Alzheimers Dis Other Demen, 25(6), 505-512.
McGough, E. L., Kelly, V. E., Logsdon, R. G., McCurry, S. M., Cochrane, B. B., Engel, J. M., & Teri, L. (2011). Associations between physical performance and executive function in older adults with mild cognitive impairment: gait speed

77
and the Timed "Up & Go" test. Phys Ther, 91(8), 1198-1207. doi: 10.2522/ptj.20100372
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology, 34(7), 939-944.
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R., Jr., Kawas, C. H., Phelps, C. H. (2011). The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 7(3), 263-269.
Menne, H. L., Kinney, Jennifer M. (2002). Trying to continue to do as much as they can do - Theoretical insights regarding continuity and meaning making in the face of dementia. Dementia, 1, 367-382.
Montero-Odasso, M., Muir, S. W., & Speechley, M. (2012a). Dual-task complexity affects gait in people with mild cognitive impairment: the interplay between gait variability, dual tasking, and risk of falls. Arch Phys Med Rehabil, 93(2), 293-299. doi: 10.1016/j.apmr.2011.08.026
Montero-Odasso, M., Verghese, J., Beauchet, O., & Hausdorff, J. M. (2012b). Gait and cognition: a complementary approach to understanding brain function and the risk of falling. J Am Geriatr Soc, 60(11), 2127-2136. doi: 10.1111/j.1532-5415.2012.04209.x
Mozley, C. G., Huxley, P., Sutcliffe, C., Bagley, H., Burns, A., Challis, D., & Cordingley, L. (1999). 'Not knowing where I am doesn't mean I don't know what I like': cognitive impairment and quality of life responses in elderly people. Int J Geriatr Psychiatry, 14(9), 776-783.
Muir, S. W., Speechley, M., Wells, J., Borrie, M., Gopaul, K., & Montero-Odasso, M. (2011). Gait assessment in mild cognitive impairment and Alzheimer's disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture.
Muir, S. W., Speechley, M., Wells, J., Borrie, M., Gopaul, K., & Montero-Odasso, M. (2012). Gait assessment in mild cognitive impairment and Alzheimer's disease: the effect of dual-task challenges across the cognitive spectrum. Gait Posture, 35(1), 96-100. doi: 10.1016/j.gaitpost.2011.08.014
Mårdh, S. (2013). Weak central coherence in patients with Alzheimer's disease. Neural Regeneration Research, 8(8), 760-766. doi: 10.3969/j.issn.1673-5374.2013.08.011
Nakamura, T., Meguro, K., & Sasaki, H. (1996). Relationship between falls and stride length variability in senile dementia of the Alzheimer type. Gerontology, 42(2), 108-113.
Nelson, M. E., Rejeski, W. J., Blair, S. N., Duncan, P. W., Judge, J. O., King, A. C., Castaneda-Sceppa, C. (2007). Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc, 39(8), 1435-1445.
Nordin, E., Rosendahl, E., & Lundin-Olsson, L. (2006). Timed "Up & Go" test: reliability in older people dependent in activities of daily living--focus on cognitive state. Physical Therapy, 86(5), 646-655.
Nygård, L. (2006). How can we get access to the experiences of people with dementia? Suggestions and reflections. Scand J Occup Ther, 13(2), 101-112.
O'Connor, D., Phinney, A., Smith, A. D., Small, J., Purves, B., Perry, J., Beattie, L. (2007). Personhood in dementia care: Developing a research agenda for broading the vision. Dementia, 6(1), 121-142.

78
Olsson, A., Lampic, C., Skovdahl, K., & Engström, M. (2013). Persons with early-stage dementia reflect on being outdoors: a repeated interview study. Aging Ment Health. doi: 10.1080/13607863.2013.801065
Pearce, A., Clare, L., & Pistrang, N. (2002). Managing sense of self: Coping in the early stages of Alzheimer’s disease. Dementia, 1(2), 173-192.
Persson, J., & Sahlin, N.-E. (2012). Vetenskapsteori för sanningssökare (Philosophy of Science for truth seekers). Stockholm: Fri Tanke.
Pettersson, A. F., Engardt, M., & Wahlund, L. O. (2002). Activity level and balance in subjects with mild Alzheimer's disease. Dement Geriatr Cogn Disord, 13(4), 213-216.
Pettersson, A. F., Olsson, E., & Wahlund, L. O. (2005). Motor function in subjects with mild cognitive impairment and early Alzheimer's disease. Dement Geriatr Cogn Disord, 19(5-6), 299-304.
Pettersson, A. F., Olsson, E., & Wahlund, L. O. (2007). Effect of divided attention on gait in subjects with and without cognitive impairment. J Geriatr Psychiatry Neurol, 20(1), 58-62.
Phinney, A. (1998). Living with dementia from the patient's perspective. J Gerontol Nurs, 24(6), 8-15.
Pitkala, K. H., Poysti, M. M., Laakkonen, M. L., Tilvis, R. S., Savikko, N., Kautiainen, H., & Strandberg, T. E. (2013). Effects of the Finnish Alzheimer disease exercise trial (FINALEX): a randomized controlled trial. JAMA Intern Med, 173(10), 894-901. doi: 10.1001/jamainternmed.2013.359
Pless, M., & Granlund, M. (2011). Handbok i att använda ICF och ICF-CY (The handbook for using ICF and ICF-CY)) (1 ed.). Lund: Studentlitteratur AB.
Podsiadlo, D., & Richardson, S. (1991). The Timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc, 39(2), 142-148.
Polit, D. F., & Beck, C. T. (2008). Nursing research : generating and assessing evidence for nursing practice (8 ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Reisberg, B. (1988). Functional assessment staging (FAST). Psychopharmacol Bull, 24(4), 653-659.
Ries, J. D., Echternach, J. L., Nof, L., & Gagnon Blodgett, M. (2009). Test-retest reliability and minimal detectable change scores for the Timed "Up & Go" test, the six-minute walk test, and gait speed in people with Alzheimer disease. Phys Ther, 89(6), 569-579.
Rockwood, K., Awalt, E., Carver, D., & MacKnight, C. (2000). Feasibility and measurement properties of the functional reach and the timed up and go tests in the Canadian study of health and aging. J Gerontol A Biol Sci Med Sci, 55(2), M70-73.
Rosendahl, E., Lindelöf, N., Littbrand, H., Yifter-Lindgren, E., Lundin-Olsson, L., Haglin, L., Nyberg, L. (2006). High-intensity functional exercise program and protein-enriched energy supplement for older persons dependent in activities of daily living: a randomised controlled trial. Aust J Physiother, 52(2), 105-113.
Sabat, S. R., & Collins, M. (1999). Intact social, cognitive ability, and selfhood: A case study of Alzheimer's disease. The American Journal of Alzheimer's Disease and Other Dementias, 14(1), 11-19. doi: 10.1177/153331759901400108
Sabat, S. R. (2002). Surviving Manifestations of selfhood in Alzheimer's disease: A case study. Dementia, 1(1), 25-36.
SBU - Statens beredning för medicinsk utvärdering (Swedish Council on Health Technology Assessment). (2008a). Dementia – Caring, Ethics, Ethnical and Economical Aspects, A Systematic Review (Vol. 1). Mölnlycke.

79
SBU – Statens beredning för medicinsk utvärdering (Swedish Council on Health Technology Assessment). (2008b). Dementia - Etiology and Epidemiology, A Systematic Review (Vol. 1). Mölnlycke: The Swedish Council on Technology Assessment in Health Care, SBU Statens beredning för medicinsk utvärdering.
Scarmeas, N., Luchsinger, J. A., Brickman, A. M., Cosentino, S., Schupf, N., Xin-Tang, M., Stern, Y. (2011). Physical activity and Alzheimer disease course. Am J Geriatr Psychiatry, 19(5), 471-481.
Schwickert, L., Becker, C., Lindemann, U., Marechal, C., Bourke, A., Chiari, L., Klenk, J. (2013). Fall detection with body-worn sensors : a systematic review. Z Gerontol Geriatr, 46(8), 706-719. doi: 10.1007/s00391-013-0559-8
Sheridan, P. L., Solomont, J., Kowall, N., & Hausdorff, J. M. (2003). Influence of executive function on locomotor function: divided attention increases gait variability in Alzheimer's disease. J Am Geriatr Soc, 51(11), 1633-1637.
Sheridan, P. L., & Hausdorff, J. M. (2007). The role of higher-level cognitive function in gait: executive dysfunction contributes to fall risk in Alzheimer's disease. Dementia & Geriatric Cognitive Disorders, 24(2), 125-137.
Shumway-Cook, A., Brauer, S., & Woollacott, M. (2000). Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther, 80(9), 896-903.
Shumway-Cook, A., & Woollacott, M. H. (2012). Motor Control Translating Research into Clinical Practice (4 ed.). Philadelphia: Lippincott Williams & Wilkins.
Snijders, A. H., van de Warrenburg, B. P., Giladi, N., & Bloem, B. R. (2007). Neurological gait disorders in elderly people: clinical approach and classification. Lancet Neurol, 6(1), 63-74.
Solomon, P. R., & Pendlebury, W. W. (1998). Recognition of Alzheimer's disease: the 7 Minute Screen. Fam Med, 30(4), 265-271.
Steeman, E., de Casterle, B. D., Godderis, J., & Grypdonck, M. (2006). Living with early-stage dementia: a review of qualitative studies. J Adv Nurs, 54(6), 722-738. doi: 10.1111/j.1365-2648.2006.03874.x
Steffen, T. M., Hacker, T. A., & Mollinger, L. (2002). Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys Ther, 82(2), 128-137.
Suttanon, P., Hill, K. D., Dodd, K. J., & Said, C. M. (2011). Retest reliability of balance and mobility measurements in people with mild to moderate Alzheimer's disease. Int Psychogeriatr, 23(7), 1152-1159. doi: 10.1017/S1041610211000639
Söderhamn, U., Landmark, B., Eriksen, S., & Soderhamn, O. (2013). Participation in physical and social activities among home-dwelling persons with dementia - experiences of next of kin. Psychol Res Behav Manag, 6, 29-36. doi: 10.2147/PRBM.S46334
Tangen, G. G., Londos, E., Olsson, J., Minthon, L., & Mengshoel, A. M. (2012). A longitudinal study of physical function in patients with early-onset dementia. Dement Geriatr Cogn Dis Extra, 2(1), 622-631. doi: 10.1159/000345782
Ten Brinke, L. F., Bolandzadeh, N., Nagamatsu, L. S., Hsu, C. L., Davis, J. C., Miran-Khan, K., & Liu-Ambrose, T. (2014). Aerobic exercise increases hippocampal volume in older women with probable mild cognitive impairment: a 6-month randomised controlled trial. Br J Sports Med. doi: 10.1136/bjsports-2013-093184
Thompson Coon, J., Boddy, K., Stein, K., Whear, R., Barton, J., & Depledge, M. H. (2011). Does participating in physical activity in outdoor natural environments

80
have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ Sci Technol, 45(5), 1761-1772. doi: 10.1021/es102947t
Trigg, R., Jones, R. W., & Skevington, S. M. (2007). Can people with mild to moderate dementia provide reliable answers about their quality of life? Age Ageing, 36(6), 663-669. doi: 10.1093/ageing/afm077
Trost, J., & Levin, I. (2011). Att förstå vardagen med ett symbolisk interaktionistiskt perspektiv (Understanding everyday life from a symbolic interactionist perspective) (4th ed.). Lund: Studentlitteratur AB.
van Iersel, M. B., Verbeek, A. L., Bloem, B. R., Munneke, M., Esselink, R. A., & Rikkert, M. G. (2006). Frail elderly patients with dementia go too fast. J Neurol Neurosurg Psychiatry, 77(7), 874-876.
van Iersel, M. B., Ribbers, H., Munneke, M., Borm, G. F., & Rikkert, M. G. (2007). The effect of cognitive dual tasks on balance during walking in physically fit elderly people. Arch Phys Med Rehabil, 88(2), 187-191.
van Iersel, M. B., Benraad, C. E., & Rikkert, M. G. (2007). Validity and reliability of quantitative gait analysis in geriatric patients with and without dementia. J Am Geriatr Soc, 55(4), 632-634. doi: 10.1111/j.1532-5415.2007.01130.x
Vreugdenhil, A., Cannell, J., Davies, A., & Razay, G. (2012). A community-based exercise programme to improve functional ability in people with Alzheimer's disease: a randomized controlled trial. Scand J Caring Sci, 26(1), 12-19. doi: 10.1111/j.1471-6712.2011.00895.x
Watson, M. (2002). Refining the Ten-metre Walking Test fo Use with Neurologically Impaired People. Physiotherapy 88(7), 386-397.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L. O., Petersen, R. C. (2004). Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med, 256(3), 240-246. doi: 10.1111/j.1365-2796.2004.01380.x
Wittwer, J. E., Andrews, P. T., Webster, K. E., & Menz, H. B. (2008). Timing variability during gait initiation is increased in people with Alzheimer's disease compared to controls. Dement Geriatr Cogn Disord, 26(3), 277-283.
Wittwer, J. E., Webster, K. E., & Menz, H. B. (2010). A longitudinal study of measures of walking in people with Alzheimer's Disease. Gait Posture.
WHO - World Health Organization. (2008). International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization.
WHO - World Health Organisation. (2010). Global recommendations on physical activity for health. Switzerland: World Health Organization. Retrieved from http://www.who.int/dietphysicalactivity/publications/9789241599979/en/.
WHO - World Health Organization and Alzheimer Disease International. (2012). Dementia: A Public Health Priority. Retrieved from http://www.who.int/mental_health/publications/dementia_report_2012/en/
WHO - World Health Organization. (2014) Health Topics, Rehabilitation. Retrieved from http://www.who.int/topics/rehabilitation/en/
World Confederation for Physical Theapy. (2011). Policy statement. Description of Physical Therapy. Retrieved from http://www.wcpt.org/policy/ps-descriptionPT
Yogev-Seligmann, G., Hausdorff, J. M., & Giladi, N. (2008). The role of executive function and attention in gait. Mov Disord, 23(3), 329-342. doi: 10.1002/mds.21720

81
Yu, F., Savik, K., Wyman, J. F., & Bronas, U. G. (2011). Maintaining physical fitness and function in Alzheimer's disease: a pilot study. Am J Alzheimers Dis Other Demen, 26(5), 406-412. doi: 10.1177/1533317511414861
Yu, F., Thomas, W., Nelson, N. W., Bronas, U. G., Dysken, M., & Wyman, J. F. (2013). Impact of 6-Month Aerobic Exercise on Alzheimer's Symptoms. J Appl Gerontol. doi: 10.1177/0733464813512895
Åberg, A. C., Lindmark, B., & Lithell, H. (2003). Evaluation and application of the General Motor Function assessment scale in geriatric rehabilitation. Disabil Rehabil, 25(7), 360-368.
Åberg, A. C., Sidenvall, B., Hepworth, M., O'Reilly, K., & Lithell, H. (2004). Continuity of the self in later life: perceptions of informal caregivers. Qual Health Res, 14(6), 792-815.
Åberg, A. C., Sidenvall, B., Hepworth, M., O'Reilly, K., & Lithell, H. (2005). On loss of activity and independence, adaptation improves life satisfaction in old age--a qualitative study of patients' perceptions. Quality of Life Research, 14(4), 1111-1125.
Åberg, A. C. (2008). Care recipients' perceptions of activity-related life space and life satisfaction during and after geriatric rehabilitation. Qual Life Res, 17(4), 509-520.
Öhman, A., Josephsson, S., & Nygard, L. (2008). Awareness through interaction in everyday occupations: experiences of people with Alzheimer's disease. Scand J Occup Ther, 15(1), 43-51. doi: 10.1080/11038120701441080

App
endi
x
Ove
rvie
w o
f th
e 21
par
tici
pant
s an
d th
eir
iden
tifi
ed ty
pes
of d
ual-
task
ga
it d
istu
rban
ces
(Stu
dy I
II)
T
EM
PO
RA
L
DIS
TU
RB
AN
CE
SP
AT
IAL
D
IST
UR
BA
NC
E
INS
TA
BIL
ITY
IN
SIN
GL
E
ST
AN
CE
Partici-pants
MM
SE
sco
re
Gai
t spe
ed m
/s
Dou
ble
stan
ce
stop
S
ingl
e st
ance
st
op
Var
iabl
e st
ep
leng
th
Var
iabl
e S
tep
wid
th/
Dev
iati
ng
dire
ctio
n
Sta
nce
foot
co
rrec
tion
B
1y
2y
B
1y
2y
B
1y
2y
B
1y
2y
B
1y
2y
B
1y
2y
B
1y
2y
1 28
29
18
1.
17
1.05
0.
90
2
25
21
18
1.15
1.
17
1.05
●
●
● ●
● ●
● ●
●
3 23
16
15
0.
93
0.98
0.
67
●
● ●
● 4
25
24
21
0.86
0.
78
0.51
5 22
22
15
1.
33
1.28
1.
28
●
●
6
24
26
21
1.18
1.
19
1.26
●
●
7 23
22
14
1.
08
1.02
1.
07
● ●
●
●
●
8
22
20
17
1.37
1.
38
1.18
● ●
●
9 25
17
13
1.
33
1.26
1.
33
10
22
23
18
1.
22
0.98
1.
10
11
26
17
16
1.
23
1.01
0.
94
●
●
● ●
●
● ●
12
23
19
21
1.
02
1.22
1.
19
●
● 13
23
20
20
1.
12
0.96
0.
93
● ●
●
14
26
24
26
1.
26
1.26
0.
97
●
15
26
28
26
1.
22
1.06
0.
87
● ●
●
16
26
22
21
1.
00
1.01
0.
99
●
17
30
24
28
0.
92
0.90
0.
81
18
22
23
23
1.
28
1.16
1.
12
19
29
25
21
1.
11
1.17
1.
05
● ●
●
● ●
●
20
21
18
9
1.00
1.
00
0.80
21
28
27
25
1.16
1.
18
1.11
●
MM
SE
= M
ini M
enta
l Sta
te E
xam
inat
ion


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1008
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-223687
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2014