Embed Size (px)
DESCRIPTION
Phys Ther 2002 Bartlett 237 48
Citation preview

2002; 82:237-248.PHYS THER. Doreen J Bartlett and Robert J PalisanoClinical ReasoningChildren With Cerebral Palsy: Implications forInfluencing the Acquisition of Motor Abilities of Physical Therapists' Perceptions of Factors
http://ptjournal.apta.org/content/82/3/237found online at: The online version of this article, along with updated information and services, can be
Collections
Motor Development Diagnosis/Prognosis: Other
Cerebral Palsy (Pediatrics) Cerebral Palsy
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

Physical Therapists’ Perceptions ofFactors Influencing the Acquisition ofMotor Abilities of Children WithCerebral Palsy: Implications forClinical Reasoning
Background and Purpose. Evidence supporting factors predictingmotor change for children with cerebral palsy is minimal. A consensusexercise using focus groups and survey methods was conducted toidentify factors perceived to affect the acquisition of basic motorabilities among children with cerebral palsy from the time of diagnosisto 7 years of age. Subjects. Fifty-seven physical therapists participated inone of 12 focus groups, and 60 physical therapists participated in afollow-up questionnaire survey via mail. Methods. The nominal grouptechnique was used to conduct the focus groups. Results. Participantsreached consensus about 12 factors in 4 constructs, which we called:(1) primary impairments (muscle tone/movement patterns, distribu-tion of involvement, balance, and sensory impairment), (2) secondaryimpairments (range of motion/joint alignment, force production,health, and endurance), (3) personality characteristics (motivation),and (4) family factors (support to child, family expectations, andsupport to family). Discussion and Conclusion. The recognition ofpotential determinants of motor change could assist in the clinicalreasoning that physical therapists use when planning interventions forchildren with cerebral palsy. Participants identified a set of variables,some of which are found in the literature, that can provide foundationknowledge for decision making and research on factors that bringabout change in motor ability among children with cerebral palsy.[Bartlett DJ, Palisano RJ. Physical therapists’ perceptions of factorsinfluencing the acquisition of motor abilities of children with cerebralpalsy: implications for clinical reasoning. Phys Ther. 2002;82:237–248.]
Key Words: Cerebral palsy, Clinical reasoning, Consensus, Motor outcomes, Prognosis.
Doreen J Bartlett, Robert J Palisano
Physical Therapy . Volume 82 . Number 3 . March 2002 237
Rese
arch
Repo
rt �
������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
������
������
������
������
������
������
������
�����
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

Cerebral palsy is the sensory and neuromusculardeficit caused by a nonprogressive brain defector lesion occurring during the prenatal, intra-partum, perinatal, or early postnatal periods.1
At the time of diagnosis, most parents are concernedabout their child’s potential for motor developmentand, specifically, the prognosis for ambulation.2–5 Knowl-edge of factors that can be used to predict motoroutcomes in children with cerebral palsy is limited.6 Thisprognostic information is essential, however, when mak-ing collaborative decisions with families about rehabili-tation services for their children.7 The clinical reasoninginvolved in this decision-making process has been sug-gested as being at the core of effective practice8 and istherefore an important area for investigation.
“Clinical reasoning,” as we use the term, refers to themany ways a practitioner thinks about and interprets anidea and incorporates knowledge, experience, problemsolving, judgment, and decision making.9 Experiencedclinicians, especially those who practice in neurology,10
are thought by at least one group to apply their knowl-edge of multiple factors influencing outcomes in animplicit way to arrive rapidly at decisions for a plan ofcare.11,12 In a review of research on clinical reasoning inpediatric physical therapy, Palisano and colleagues13
argued that physical therapists largely use implicitthought processes and that the implicit knowledgemight not be organized into an effective framework.14
An explicit conceptual framework, therefore, might beuseful for physical therapists to reflect on their percep-tions of factors influencing motor outcomes of childrenwith cerebral palsy and could optimize clinicalreasoning.
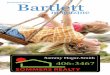
Previously, we described a multivariate model of acqui-sition of motor abilities in infants and children withcerebral palsy up to the age of 7 years.6 This model wasdeveloped to assist with decision making (Figure). Wedefined basic motor abilities as the child’s capacity toperform movements such as rolling, sitting, crawling,and walking. This definition is consistent with Touwen’suse of the term, which he differentiated from “motorskills” (eg, higher-level activities such as writing or play-ing sports or a musical instrument).15 Recent researchsuggests that the acquisition of basic motor abilitiesplateaus by 6 or 7 years of age in children with cerebralpalsy.16 Accordingly, the focus of the model is on chil-dren younger than 7 years of age. Development of themodel was guided by compatible theoretical frameworks(the disablement process using the International Classi-fication of Functioning, Disability, and Health [ICIDH-2],17 systems theory, and family-centered care), researchon prognostic factors for motor outcome in childrenwith cerebral palsy, literature on motor development ofinfants, and literature on the general health and devel-opmental outcomes of children who are at risk for adevelopmental disability.
The model contains 5 constructs (primary impairments,secondary impairments, child personality characteristics,family ecology, and health care services) that are pro-posed to interact to explain and predict the acquisitionof basic motor abilities among children with cerebralpalsy. Primary impairments were defined as organ- orsystem-level deficits that were apparent at the time ofdiagnosis. An example of a primary impairment is hyper-tonicity. Secondary impairments were defined as organ- orsystem-level deficits occurring over time. Contracturesare an example of secondary impairments. Child person-
DJ Bartlett, PT, PhD, is Assistant Professor, School of Physical Therapy, Faculty of Health Sciences, 1588 Elborn College, The University of WesternOntario, London, Ontario, Canada N6G 1H1 ([email protected]), and Associate Member, CanChild, Centre for Childhood Disability Research,McMaster University, Hamilton, Ontario, Canada. Address all correspondence to Dr Bartlett at the first address.
RJ Palisano, PT, ScD, is Professor, Programs in Rehabilitation Sciences, MCP Hahnemann University, Philadelphia, Pa, and Co-Investigator,CanChild, Centre for Childhood Disability Research, McMaster University.
Both authors provided concept/research design and writing. Dr Bartlett provided data collection and analysis, project management, fundprocurement, subjects, facilities/equipment, and institutional liaisons. Dr Palisano provided consultation (including review of manuscript beforesubmission). The authors thank the physical therapists from the Ontario Association for Children’s Rehabilitation Services Centres forparticipating in this project and Andrea Abbott for conducting the reliability portion of the content analysis. They also acknowledge the membersof CanChild, Centre for Childhood Disability Research, McMaster University, for providing a forum for the development of this work.
Part of the information in this manuscript was included in a presentation titled “Prognostic Indicators in Cerebral Palsy: A Consensus Exercise”at the Tri-joint Congress; May 25, 2000; Toronto, Ontario, Canada.
This project was approved by the Review Board for Health Sciences Research Involving Human Subjects at The University of Western Ontario.
This project was funded through a research grant from the Vice President (Research) at The University of Western Ontario.
This article was submitted April 2, 2001, and was accepted September 26, 2001.
238 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

ality characteristics were defined as any personalityattributes that are largely independent of having adiagnosis of cerebral palsy (ie, relates to a description ofchildren, regardless of diagnosis); temperament is anexample of a personality attribute. Family ecology wasdefined as anything related to the environment offamilies, such as resources and supports.
Possible indicators identified in the literature for the 4constructs in our study are presented in Table 1. Asindicated in the Figure, primary impairments arehypothesized to be a major influence on the acquisitionof motor abilities, both directly and by causing secondaryimpairments. Child personality characteristics are con-ceptualized by us as being independent of the primaryimpairments associated with cerebral palsy and as havingan effect on motor abilities through an effect on second-ary impairments. We viewed family ecology (ie, howfamilies function) as being influenced, at least in part, bythe personality characteristics of the child with cerebralpalsy and, in turn, as influencing the acquisition ofmotor abilities through variations in opportunities formovement exploration.
The nature of a child’s primary impairments and per-sonality characteristics are hypothesized by us to havemoderate and relatively minor influences, respectively,on the services provided by physical therapists. Thenature of the secondary impairments might also influ-ence services, which could affect the secondary impair-ments over time. The bidirectional arrows in the Figureindicate the relationship between the constructs ofhealth care services and family ecology, in keeping withthe philosophy of family-centered care.18 As indicated bythe dashed ovals and arrows in the Figure, the constructsof activity (as it applies to activities of daily living andplay) and participation (eg, attendance at preschool orschool) are not a part of the proposed model. They areincluded in the Figure to provide a perspective on howmotor abilities relate to activity and participation.6 Muchof the evidence we used to develop the model came fromliterature on development rather than solely from theliterature about children with cerebral palsy.
Streiner and Norman19 contended that, in the absenceof research-based evidence, clinicians with relevant expe-rience are a valuable source of knowledge. Oneapproach used to examine clinical reasoning and deci-
Figure.Model of determinants of motor change for children with cerebral palsy. The magnitude of the hypothesized influences is indicated by the differentthicknesses of the arrows. Solid lines and ovals are a part of the proposed model; dotted lines and ovals represent parts of an expanded model.Reprinted with permission of the American Physical Therapy Association from Bartlett DJ, Palisano RJ. A multivariate model of determinants of motorchange for children with cerebral palsy. Phys Ther. 2000;80:598–614.
Physical Therapy . Volume 82 . Number 3 . March 2002 Bartlett and Palisano . 239
������
������
������
������
�
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

sion making is the nominal group technique (NGT).20
The NGT is a method of obtaining group consensus thatis designed to stimulate the generation of critical ideas,to increase the creative productivity of group action, togive guidance in the aggregation of individual judg-ments, and to arrive at a desirable group decision, whileleaving participants with a sense of satisfaction. The NGTconsists of a 6-step process that involves: (1) silentgeneration of items, (2) round-robin recording of items,(3) serial discussion of items, (4) preliminary ranking ofitems, (5) discussion of ranking, and (6) final ranking ofitems. According to Boyce et al,21 when the NGT is usedfor planning a research agenda, clinicians’ participationmay increase because this method can provide a feelingof “ownership” of the results. The NGT has been used inrehabilitation research, including the development of ameasure of quality of movement15 and a classificationsystem for children with cerebral palsy.22
The purpose of our study was to use a conceptualframework and the NGT consensus process to: (1) identifyfactors that physical therapists perceive are important inthe acquisition of motor abilities in children with cere-bral palsy, (2) discuss implications for clinical reasoning,
(3) compare the results of the consensus process withcurrent knowledge, and (4) discuss how the results canassist research. The focus of this work is not on interven-tions, but it is in line with the approach of clarifyingprognostic factors before examining the effectiveness ofinterventions.23 We did not include the construct ofhealth care services in the consensus process.
MethodWe studied pediatric physical therapists working inthe Ontario Association for Children’s RehabilitationServices (OACRS) centers. The study had 3 phases:(1) consensus within focus groups, (2) compilation ofpotential determinants identified in the focus groups,and (3) consensus among all participants.
Selection of ParticipantsPhysical therapist participants were recruited from 18 ofthe 19 centers affiliated with OACRS; one chief execu-tive officer did not respond to an initial letter. Themajority of children with cerebral palsy in Ontarioreceive services through these centers. Informationpackages were mailed to 75 physical therapists; 64 con-sents were returned after a second mailing, for aresponse rate of 85%. Of the 64 initial respondents,57 physical therapists from 12 OACRS centers partici-pated in the focus groups (phase 1). Group sizes rangedfrom 2 to 7 participants. Although 5 to 9 participants pergroup is recommended for the NGT,20 groups wereconducted with fewer participants because this repre-sented the total number of eligible physical therapists atthese centers. Four additional physical therapists con-sented to participate in the third phase of the study,which involved completion of a questionnaire. Thequestionnaire was mailed to the 68 physical therapists.After one reminder, 60 survey questionnaires werereturned, for a response rate of 88%.
Fifty-six participants were women, and 4 participantswere men; the majority worked full-time. As a group,these therapists had worked in pediatric rehabilitationfor an average of 13.7 years (SD�7.4, range�1–35).Although the preferred interventions used by theseparticipants cannot be stated with certainty, serviceproviders in the OACRS centers usually provide family-centered services, particularly with respect to: enablingand partnership, providing specific information aboutthe child, and providing respectful and supportivecare.24 There is, in our view, a trend among physicaltherapists working at centers similar to these to a movefrom a neurodevelopmental treatment approach tofamily-centered functional therapy25 incorporatingmotor learning and cognitive strategies26 when workingwith children with cerebral palsy.
Table 1.Possible Determinants of Motor Change for Children WithCerebral Palsya
Construct Possible Determinant
Primary impairmentsMotor Aberrations in muscle tone
Type of motor disorderDistribution of motor disorderPrimitive reflexesAge of acquisition of motor
abilitiesSensory Visual impairment
Sensorimotor integration (vision,somatosensation, vestibular)
Cognitive Cognitive abilityEpilepsy
Secondary impairments Muscle hypoextensibilityJoint contractureSkeletal malalignmentImpaired force productionImpaired endurance
Inherent child characteristics TemperamentMovitationRisk taking
Family ecology Family resourcesQuality of the home environmentFamily supportParental expectationsFamily function
a Adapted and reprinted with permission of the American Physical TherapyAssociation from Bartlett DJ, Palisano RJ. A multivariate model ofdeterminants of motor change for children with cerebral palsy. Phys Ther.2000;80:598–614.
240 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

Phase 1: Consensus Within Focus GroupsA package of information containing a description of thestudy, the agenda for the focus group, a 2-page intro-duction to the model and the definitions of the 4constructs of interest, and a descriptive survey instru-ment was mailed to each physical therapist. Examples ofdeterminants were described in very broad terms, so asnot to constrain responses.20 Participants were asked tothink about what they believed influences the acquisi-tion of basic motor abilities of young children withcerebral palsy relative to the 4 constructs. They wereasked to record their ideas in the survey instrumentprovided in the information package in preparation forthe meeting. The focus groups lasted 60 to 90 minutes,and the NGT was used.20 Although the primary author(DJB) had not previously used this technique, the“Guidelines for Conducting NGT Meetings”20 was usedfor the sessions. Each focus group began with an intro-duction of the facilitator (DJB), a review of the agenda,and a brief overview of the model. This introductoryportion ended with the question “What are the impor-tant factors in the 4 constructs of child characteristicsrelating to the primary neurological impairments, childcharacteristics relating to the secondary impairments,child personality characteristics, and family ecology con-tributing to change in motor abilities of children withcerebral palsy?” Participants were assured that this wasnot a test. The facilitator reiterated the point that wewere interested in learning from them and theirexperiences.
Step 1 was completed in 5 to 10 minutes. During thistime, each participant independently generated a list ofdeterminants of motor outcomes for the 4 constructs.Next, a round-robin format was used to generate acomposite list of determinants of motor abilities. Eachparticipant was asked to suggest one determinant at atime in an effort to ensure equal participation. Partici-pants were encouraged not to repeat ideas, but tosuggest variations that they thought were important. Thegroup facilitator recorded ideas on a flip chart with aseparate page for each construct. This process lasted 30to 40 minutes. The round-robin format was conductedrapidly based the assumption that doing so would min-imize ideas being attributed to individual participants.20
After all potential determinants were recorded for the 4constructs, each determinant was reviewed for clarityand distinctiveness from other determinants throughdiscussion guided by the facilitator. Although many ofthe determinants might be partially correlated, the mainconsideration was whether each determinant couldpotentially affect the acquisition of motor abilities in aunique way. Ideas were grouped together only if allmembers of the group agreed. The average number ofdeterminants for each construct generated by the focus
groups were: primary impairments�13.9 (SD�2.8,range�9–17), secondary impairments�10.8 (SD�3.1,range�6–16), child personality characteristics�11.6(SD�4.2, range�6–20), and family ecology�14.8(SD�3.5, range�9–21).
Each focus group ended with the participants identifyingand ranking the 5 most important determinants for eachof the 4 constructs. As recommended by experts on theNGT,20 each participant first recorded the 5 most impor-tant determinants within a construct on 5 separate cardsand then identified the most important determinantfrom the 5 cards (rank�5), the least important determi-nant from the remaining 4 cards (rank�1), the mostimportant determinant from the remaining 3 cards(rank�4), and the least important determinant from theremaining 2 cards (rank�2). The last remaining cardreceived a rank of 3. Consensus within each focus groupwas established by determining the average rank foreach determinant generated by the participants.
Phase 2: Compilation of Determinants Identified byFocus GroupsTypically, the NGT includes steps 5 and 6 in which theresults of the preliminary vote are discussed and asecond vote is taken. In our study, the second vote wasconducted by having all participants complete a ques-tionnaire. In order to develop a questionnaire for com-pletion by all participants (phase 3 of the study), therank-ordered lists generated by the 12 focus groups wereintegrated into a single list. This task was accomplishedusing a strategy referred to as “the induction of catego-ries using content analysis”20 and was conducted first bythe primary author and then independently by anotherpediatric physical therapist who had 10 years of clinicalexperience and a Master of Science degree (ie, researchtraining beyond the entry-to-practice degree).
First, the rankings for each potential determinant gen-erated by each focus group were written on paper, andthe paper was cut into strips, with one determinant perstrip. The primary author then sorted the determinantsinto groups, with each group capturing one set of ideas.For example, the determinants of “muscle tone” and“spasticity” were included in one group. Participants insome groups elected to combine some issues (eg, musclecontracture and skeletal malalignment); when thisoccurred, these ideas were pooled for all similar items.Through this process, redefinitions of categories and thedevelopment of new categories occurred. Thus, allpotential determinants were categorized by new themes,and an average rank for each new theme was produced,reflecting input from the 12 groups. This average rankwas determined by dividing the sum of the rankingsprovided by each individual focus group by 12 (ie, thenumber of groups).
Physical Therapy . Volume 82 . Number 3 . March 2002 Bartlett and Palisano . 241
������
������
������
������
�
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

Only those items with average ranks above 0.7 wereselected for inclusion in the questionnaire. We arbi-trarily selected this cut-point of 0.7 in order to get about5 potential determinants for each construct. Althoughthis cut-point seems low in the context of the scale of 1through 5, many groups did not suggest some of thepotential determinants. That effectively contributed zeropoints to the ranking for that determinant. Accordingly,the value cannot be considered an estimate of impor-tance of the determinant; instead, this was simply thestrategy that was used to identify variables ranked mosthighly for the next phase. Our strategy resulted in5 potential determinants for primary impairments, 5potential determinants for secondary impairments, 4potential determinants for child personality characteris-tics, and 6 potential determinants for family ecology.The results of the average ranked values of these top 4 to6 determinants for each construct are shown in Table 2.
To examine interrater reliability, a second pediatricphysical therapist independently categorized the deter-minants generated from the focus groups (ie, shegrouped the determinants into categories withoutknowledge of the primary author’s categorization). Inde-pendent classification resulted in agreement on 17 of 20determinants (ie, 85% item agreement). The 2 physicaltherapists were in agreement on 4 of the top 5 determi-nants for the construct of primary impairments, on all 5
determinants for the construct of sec-ondary impairments, on 3 of the top 4determinants for the construct of childpersonality characteristics, and on allexcept the fifth ranked of 6 determi-nants for the construct of family ecol-ogy. The questionnaire was constructedusing the categorization by the primaryauthor.
Phase 3: Consensus Among ParticipantsIn the final phase, all participants com-pleted a questionnaire that was devel-oped for this study. The Appendix con-tains an example of one of the itemsunder construct of family ecology. Thepotential determinants for each of the4 constructs were presented in randomorder on the questionnaire. Questionswere focused on the importance of eachdeterminant in influencing the acquisi-tion of motor abilities, an estimate ofthe feasibility of collecting data in aclinical setting, and an indication ofwhat resources would be required beforethe data could be collected (eg, train-ing, time, “other” [for example, finan-cial reimbursement]). Participantswere asked to rate the question about
the importance of each item on a 10-point scale, with 10being “very important” and 0 being “unimportant.”Feasibility was rated on a 3-point scale, with 3 being“feasible” and 1 being “not at all feasible.”
In order to identify a set of variables for future researchto test the model, we selected a cut-point of greater than7. The intent was to identify a relatively small number ofvariables that therapists perceived to be important in theacquisition of basic motor abilities by children withcerebral palsy. We did not aim to identify all possiblevariables. In the context of testing the model in thefuture with structural equation modeling, we believe inthe principle of parsimony.27–29 In addition, we believethat when doing research in a clinical setting, it isimportant not to burden families and service providerswith data collection.
ResultsThe determinants that had ratings of importance of 7 orgreater out of 10 are shown in Table 3. The physicaltherapists identified the following 4 primary impair-ments as being potential determinants of motor abilities:muscle tone (which most groups referred to as “spastic-ity”) and movement patterns, distribution of involve-ment, balance, and sensory impairment. The 4 highestranked secondary impairments were: range of motion
Table 2.Average Ranking of Determinants for Each Construct Among 57 Physical Therapists From 12Centersa
Construct DeterminantAverageRanking
Primary impairments Muscle tone/movement patterns 4.4Cognition 1.8Distribution of involvement 1.6Sensory impairment (all types) 1.4Balance/postural reactions 0.8
Secondary impairments Muscle and joint contractures/skeletal malalignment
5.4b
General health/respiratory status 1.5Force production 1.4Endurance/fitness/efficiency 0.9Pain/effect of surgery 0.7
Child personality characteristics Motivation 4.6Temperament 1.7Separation anxiety 1.2Sociability 0.9
Family ecology Expectations/beliefs 3.5Support to child 2.3Response to diagnosis 2.2Family support 1.7Family functioning 1.5Family resources 1.5
a Values range from 1 (least important) to 5 (most important).b Values greater than 5 are possible as a result of independent items being pooled in the contentanalysis strategy.
242 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

and joint alignment, muscle force, health, and endur-ance. Only one determinant (motivation) in the con-struct of child personality characteristics had an averagerating of greater than 7. Finally, participants identified 3items under the construct of family ecology: family’ssupport to child, family expectations of their child, andthe support a family receives.
All of the potential determinants listed in Table 3 (withthe exception of sensory impairment) had median val-ues for feasibility of 3 (top value). More than half of therespondents judged assessment of sensory impairmentto be only “somewhat feasible” for young children withcerebral palsy.
DiscussionThe 3-phase process of obtaining consensus amongpracticing pediatric physical therapists on factors thatthey believe influence the acquisition of motor abilitiesin children with cerebral palsy was successful. The highresponse rates30 of 85% and 88% for 2 of the phases, inour opinion, attest to the enthusiasm of the physicaltherapists working in the OACRS centers in participatingin this project. In this discussion, we elaborate on thepotential implications of therapists’ beliefs of prognosticfactors on current clinical reasoning and decision mak-ing. We also discuss the similarities and differencesbetween the results of this consensus project for each ofthe 4 constructs with the theory- and evidence-basedmodel we previously developed. Finally, we state howthese results will guide us in the next stage toward testingthe model of determinants of motor abilities.
Implications for Clinical ReasoningThis consensus exercise was conductedwith 60 physical therapists with an aver-age of 13.7 years of experience in pedi-atrics. Although the participants nei-ther developed the conceptual modelillustrated in the Figure nor explicitlystated their assumptions about factorsinfluencing the acquisition of motorabilities outside of this study, we con-tend that the results shown in Table 3provide a rare glimpse of factors thatphysical therapists might use implicitlyin practice when making clinical deci-sions. These determinants can be usedin one of 2 ways. Determinants per-ceived as not likely to change haveimplications for prognosis, includingestablishment of realistic and attainablegoals. In contrast, determinants per-ceived as amenable to change arepotential areas for intervention.
Although the therapists in this study were not asked tomake this distinction, the results provide a foundationfor further inquiry on how knowledge of determinants isapplied in decision making.
Some of the primary impairments might be the factorsthat are least amenable to change through physicaltherapy intervention. Physical therapy intervention isnot likely to change either the distribution of involve-ment or the nature of the sensory impairment. Thesefactors, therefore, are unlikely to be the focus of inter-vention, but they could be taken into considerationwhen selecting intervention strategies and proceduresfor children with different attributes. Similarly, althoughmuscle tone (ie, “the force with which a muscle resistsbeing lengthened”31(p577)) has been a focus of physicaltherapy interventions in the past,32 current rehabilita-tion practice favors medical or surgical interventionssuch as use of intrathecal baclofen,33 use of botulinumtoxin A,34 or selective posterior rhizotomy35 for themanagement of spasticity. From this study, it is difficultto speculate how physical therapists would use the factorthey identified as “movement patterns” in decision mak-ing. Therapists using a neurodevelopmental frameworkbased on the work of the Bobaths would likely target thequality of movement as an area for intervention, albeit inwhat they consider a functional context.36–38 Conversely,therapists using what they call a functional approach25
might use information from the assessment of move-ment patterns to assist in establishing realistic functionalgoals. Finally, little information was obtained withrespect to balance or postural control; however, theconsensus statements of a conference on the manage-ment of cerebral palsy concluded that physical therapy is
Table 3.Determinants for Each Construct Rated as Most Important by 60 Physical Therapists in Phase3a
Construct Determinant
Estimate ofImportance
X SD
Primary impairments Muscle tone/movement patterns 9.4 1.0Distribution of involvement 9.4 1.0Balance 8.7 1.4Sensory impairment 7.5 2.0
Secondary impairments Range of motion/joint alignment 9.0 1.2Muscle strength/force production 7.9 1.6Health 7.5 1.9Endurance 7.0 2.0
Child personality characteristics Motivation 8.2 1.7
Family ecology Support to child 7.9 1.8Family expectations 7.3 2.1Family support 7.3 2.1
a Determinants were rated on a 10-point scale (1�unimportant, 10�very important).
Physical Therapy . Volume 82 . Number 3 . March 2002 Bartlett and Palisano . 243
������
������
������
������
�
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

effective in enhancing postural control,39 supportingtherapists’ focus on enhancing balance and posturalcontrol during intervention.
In contrast to the mixed picture under the construct ofprimary impairments, physical therapists try to preventsecondary impairments through interventions.7 The sec-ondary impairments identified in our study as determi-nants of motor change are currently recommended asareas for intervention by health care practitioners work-ing with children with cerebral palsy. These areas forintervention include prevention or minimization of mus-cle and joint contractures and skeletal malalignmentand promotion of general health, muscle force, fitness,and endurance.40,41
Motivation was the only child personality characteristicunrelated to the diagnosis of cerebral palsy that wasidentified as a determinant of change in motor abilities.Based on their experiences, participants might perceivethat children who are motivated to achieve motor abili-ties are more likely to actively participate in interventionthan children who are not motivated. That is, therapistsmight regard a child’s “motivation” as important duringthe goal-setting process. In addition, some therapistsmight use strategies during intervention that areintended to enhance motivation. Some people believethat motivation can be increased if the child perceivesthe activity to have some type of intrinsic reward.42
Campbell43 related the concept of “flow” (defined as anoptimal psychological experience) to a pediatric physicaltherapy session by suggesting that if a therapist is able toengage a child deeply in an activity, outcomes of therapymight be enhanced.
Finally, therapists identified a family’s support to thechild, expectations of the child, and the support that thefamily has as being important determinants of motorchange for children with cerebral palsy. We believe thatthese ideas reflect a philosophical approach related tofamily-centered service.44 Each of these determinants is apotential target for intervention or supportive care.Based on the assumption that optimal child functioningoccurs within a supportive family and community con-text, service providers should support families and encour-age the use of community supports, as necessary.44
In our study, therapists were not asked to describe howthey perceived these factors to influence acquisition ofmotor abilities of children with cerebral palsy; however,we believe that this is a useful area for future inquiry.Campbell43 recently emphasized the importance ofusing explicit decision-making paradigms in the contextof a conceptual framework to improve physical therapypractice and optimize outcomes of children with neuro-logical impairments. Conceptual models have been iden-
tified that influence daily practice by giving guidance onwhat to do, how to do it, and—most importantly—why todo it.45 Thus, although it has been argued that clinicalreasoning involves more than the ability to offer reasonsjustifying clinical decisions,46 we believe that explicitacknowledgement of the content and process of clinicaldecision making will improve both the outcomes amongchildren with cerebral palsy and the learning experi-ences of inexperienced physical therapists.
Comparison of Consensus Results With CurrentKnowledge
Primary impairments. Knowledge of factors used in pre-dicting acquisition of motor abilities among childrenwith cerebral palsy is limited to the type of involvement,2distribution of involvement,2–5,47,48 presence and inten-sity of primitive reflexes,2–5,48 and age of acquisition ofearlier motor abilities such as independent sit-ting,2,4,5,47–49 with ambulation being the only motoroutcome investigated. Historically, impairments in whatpeople have called muscle tone have been thought of asa key contributor to limitations in motor function ofchildren with cerebral palsy.33 Recent experience withprocedures such as selective dorsal rhizotomy suggestthat muscle weakness50 and other deficits associated withabnormal temporal organization of motor unit firing51
persist following surgery. Consensus participantsexpressed the belief that alteration in muscle tonecontributes to difficulties in acquiring motor abilities.We do not know, however, whether they shared acommon definition of muscle tone. Many participants inphase 1 suggested that more than muscle tone is im-plicated. They referred to “movement patterns,” a termincorporating other qualitative aspects of movementthat included type of motor disorder (eg, dystonic orathetoid) and expression of the motor disorder (eg, pres-ence and intensity of primitive reflexes). This fits withthe description of the motor deficits of cerebral palsy asinvolving one or more of the following impairments:increased latency of movement onset, poor temporalorganization of muscle contraction, poor force produc-tion, decreased speed of movement, and increasedco-contraction.52
Although alterations in muscle tone and movementpatterns emerged as most important in the preliminary“across focus groups” consensus, a second estimate ofconsensus across centers resulted in distribution ofinvolvement being ranked as equally important. Thephysical therapists’ views are supported by the researchliterature. For example, virtually all children with hemi-plegia walk independently during the preschool years,2–4
and children with diplegia have a much better prognosisfor ambulation than children with quadriplegia.3–5,47,48
244 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

Participants identified both sensory impairment andbalance as important in both first and final phases of ourstudy. Little is known about the influence of sensoryimpairment on the acquisition of motor abilities incerebral palsy,53 in part, because of difficulties in mea-suring sensory impairments (including modulation andprocessing of sensory information) in young children.This difficulty was reflected in participants’ rating offeasibility of collecting this information. Deficits in bal-ance and postural control have long been describedfrom clinical observations as fundamental problemsamong children with cerebral palsy.32 More recently,researchers using kinetic and kinematic data collectionmethods have described postural control in childrenwith cerebral palsy in greater detail.54 Nonetheless, littleis known about the relationship between balance andpostural control (and the influence of intersensoryconflict) and the acquisition of motor abilities in thisgroup of children.
During phase 2, cognition emerged as a potentiallyimportant influence on the acquisition of motor abili-ties; however, participants did not identify it as a poten-tially important influence in the third phase. Cognitiveability has been identified as an unimportant determi-nant of ambulation,55 although children with micro-cephaly48 and children with very low scores on intelli-gence tests4 have been shown to have poor motoroutcomes. These results suggest that the relationshipbetween cognitive ability and the acquisition of basicmotor abilities is nonlinear, but cognitive abilities belowa certain cut-point (but not above) clearly influencemotor development. This nonlinear relationship mightexplain therapists’ hesitancy to rank cognition as animportant determinant for all children with cerebralpalsy.
Secondary impairments. Impairments in range ofmotion and joint alignment were ranked as the mostimportant secondary impairments in both parts of thisconsensus process. Many participants wanted to com-bine listings involving muscle and joint extensibility andbone alignment because impairments in these tissueswere perceived to develop progressively. The researchliterature supports the observation that children withchronic hypertonicity are at risk for the development ofmuscle hypoextensibility,56 joint contracture,57 and skel-etal malalignment.58 Prevention of these secondaryimpairments is advocated to avoid long-term problemssuch as arthritis,59 repetitive motion disorders, and bur-sitis.40 Little is known about the influence of impair-ments in range of motion and joint alignment and theacquisition of motor abilities among children with cere-bral palsy, although participants ranked these secondaryimpairments as most influential.
Children with cerebral palsy have been shown to havedeficits in force production60,61 and endurance (as mea-sured by the Energy Cost Index).62,63 Participants rankedthese factors as potentially important determinants inthe acquisition of motor abilities. Force production hasbeen identified to be associated improved walking per-formance,64,65 but little is known about the influence ofmuscle force on the acquisition of other basic motorabilities or the influence of endurance on motor change.
Participants ranked general health as being an impor-tant determinant of motor abilities among children withcerebral palsy. To our knowledge, the role of generalhealth in motor development of children with cerebralpalsy has not been investigated. Finally, although partic-ipants initially identified pain (particularly postsurgicalpain) as an important determinant, it did not remainlisted as an important determinant in the second roundof consensus across focus groups.
Child personality characteristics. Research involvinginfants developing typically has indicated that childcharacteristics of temperament,66 motivation,67 and risktaking68 are potential influences on early motor devel-opment. Although the participants in our study ofchildren with cerebral palsy initially identified severaltemperamental attributes that they believed to be partic-ularly influential (eg, separation anxiety, sociability),upon reflection only motivation had an average impor-tance rating of greater than 7. Although children withphysical disabilities such as cerebral palsy have beenshown to have lower levels of motivation than childrenwithout physical disabilities,69 the role of persistence andmotivation in the acquisition of motor abilities has notyet been explored.
Family ecology. Based on our literature review ofaspects of families that support general child develop-ment, we identified global issues of family resources,quality of the home environment, family support, paren-tal expectations, and family functioning as being poten-tial important influences on motor development.6 Onlyparental expectation has some evidence about its role onmotor development. Specifically, caregiving practicesthat involve aggressive handling of infants and exposureof infants to frequent postural challenges are associatedwith motor advancement.70 Although participants ini-tially identified ideas similar to those we found in theliterature, the final consensus revealed only 3 potentialdeterminants that received an importance rating ofgreater than 7: the family’s ability to support the child’smotor development, the family’s expectations of motorperformance, and informal support available to thefamily (eg, extended family, friends, neighbors, churchcommunity). Currently, no research evidence existsregarding the role of these family attributes on the
Physical Therapy . Volume 82 . Number 3 . March 2002 Bartlett and Palisano . 245
������
������
������
������
�
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

acquisition of motor abilities of children with cerebralpalsy.
Informing Future ResearchThe determinants identified by the participants will beused, along with future research data, to test a multivar-iate model of determinants of motor change for chil-dren with cerebral palsy. Although practicing cliniciansreached consensus about potential determinants, thisdoes not mean that the identified factors are the mostinfluential. We believe that their perceptions must betested. Before this research can be conducted, measuresof some of the variables will need to be operationallydefined and developed, and the validity and reliability ofdata obtained with these measures will need to beexamined.
LimitationsSeveral limitations of this work exist. First, participatingclinicians might not have identified some critical factorsthat might influence the acquisition of basic motorabilities of young children with cerebral palsy. Somepracticing clinicians do not keep up with the researchliterature, and they are not necessarily aware of thebroader concepts being developed. However, many ofthe participants in this study are, in our view, reflectivepractitioners,71 and make the most of their practiceexperiences.
Second, because the therapists generated lists of deter-minants and a common set of operational definitionswas not used, the participants may actually have haddiffering views of the determinants. Muscle tone, forexample, may have been tested by multiple therapists,but they may not all have had the same idea as to whatthe term means.
Third, the model and this consensus exercise focus onthe acquisition of basic motor abilities such as rolling,crawling, and walking, and not motor skill acquisition,which relies on cognition to a greater extent.15 Amongchildren with cerebral palsy, these basic motor abilitiesare acquired by 7 years of age.16 The combined effect ofthese 2 limitations might explain the lack of consensusabout child characteristics. Variables such as cognition,attention, memory, anticipation, reasoning, and judg-ment are clearly important in acquiring new motorbehaviors that are described as “skills” versus “basicabilities.”
Summary and ConclusionPhysical therapists working in centers affiliated with theOACRS participated in a 3-phase consensus process toidentify important determinants of acquisition of motorabilities in children with cerebral palsy. The primaryimpairments identified by the therapists were muscle
tone and qualitative aspects of the movement disorder,distribution of involvement, balance, and sensoryimpairments. Important secondary impairments weredeviations in range of motion and joint alignment,muscle force, health, and endurance. The only childpersonality characteristic thought to be influential in theacquisition of motor abilities was motivation. Finally, thefamily variables judged to be important were familysupport to the child, family expectations, and support tofamily. The results are compatible with current knowl-edge or address gaps in knowledge of determinants ofmotor abilities for children with cerebral palsy. Thedeterminants identified by group consensus provideinsight into contemporary perspectives on children withcerebral palsy and how physical therapists might useinformation to make clinical decisions.
The results of our study could provide knowledge forfurther investigation. As might be expected for a lifelongcondition such as cerebral palsy that affects multiplesystems, understanding of complex relationships amongpotential determinants of motor ability is a complexprocess.23 Identification of prognostic factors has beenidentified as a priority for evaluating rehabilitation inter-ventions72,73 and motor interventions for children withcerebral palsy.74 Although this need was recognized overa decade ago,74 knowledge of prognostic factors is lim-ited. Clarification of determinants of motor abilities ofchildren with cerebral palsy will provide knowledge thathas direct implications for evidence-based decision mak-ing and outcomes research.75
References1 Scherzer AL, Tscharnuter I. Early Diagnosis and Therapy in CerebralPalsy: A Primer on Infant Developmental Problems. 2nd ed. New York, NY:Marcel Dekker; 1990.
2 Molnar GE, Gordon SU. Cerebral palsy: predictive value of selectedclinical signs for early prognostication of motor function. Arch Phys MedRehabil. 1976;57:153–158.
3 Bleck EE. Locomotor prognosis in cerebral palsy. Dev Med ChildNeurol. 1975;17:18–25.
4 Watt JM, Robertson CMT, Grace MGA. Early prognosis for ambula-tion of neonatal intensive care survivors with cerebral palsy. Dev MedChild Neurol. 1989;31:766–773.
5 Campos Da Paz AC, Burnett SM, Braga LW. Walking prognosis incerebral palsy: a 22-year retrospective analysis. Dev Med Child Neurol.1994;36:130–134.
6 Bartlett DJ, Palisano RJ. A multivariate model of determinants ofmotor change for children with cerebral palsy. Phys Ther. 2000;80:598–614.
7 Guide to Physical Therapist Practice. 2nd ed. Phys Ther. 2001;81:9–744.
8 Rivett D, Higgs J. Experience and expertise in clinical reasoning. NZJ Physiotherapy. 1995;23:16–21.
9 Flemming MH. The therapist with the three track mind. Am J OccupTher. 1991;45:1007–1014.
246 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

10 May BJ, Dennis JK. Expert decision making in physical therapy: asurvey of practitioners. Phys Ther. 1991;71:190–202.
11 Benner P. From Novice to Expert: Excellence and Power in ClinicalNursing Practice. Upper Saddle River, NJ: Prentice Hall Health; 2001.
12 Jasper MA. Expert: a discussion of the implications of the concept asused in nursing. J Adv Nurs. 1994;20:769–776.
13 Palisano RJ, Campbell SK, Harris SR. Decision-making in pediatricphysical therapy. In: Campbell SK, VanderLinden DW, Palisano RJ,eds. Physical Therapy for Children. Philadelphia Pa: WB Saunders Co;2000:198–224.
14 Larin HM. Knowledge in Practice: Motor Learning Theories in PediatricPhysiotherapy [unpublished doctoral dissertation]. Toronto, Ontario,Canada: University of Toronto; 1992.
15 Touwen BCL. The brain and the development of function. Dev Rev.1998;18:504–526.
16 Palisano RJ, Hanna SE, Rosenbaum PL, et al. The validation of amodel of motor development for children with cerebral palsy. PhysTher. 2000;80:974–985.
17 International Classification of Functioning, Disability, and Health [Prefi-nal Draft]. Geneva, Switzerland: World Health Organization; 2000.
18 Law M, ed. Family-Centered Assessment and Intervention in PediatricRehabilitation. Birmingham, NY: The Haworth Press Inc; 1998.
19 Streiner DL, Norman GR. Health Measurement Scales: A Practical Guideto Their Development and Use. 2nd ed. Oxford, United Kingdom: OxfordUniversity Press; 1995.
20 Delbecq AL, Van de Ven AH, Gustafson DH. Group Techniques forProgram Planning: A Guide to Nominal Group and Delphi Processes. Middle-ton, Wis: Green Briar Press, 1986.
21 Boyce WF, Gowland C, Hardy S, et al. Development of a quality-of-movement measure for children with cerebral palsy. Phys Ther. 1991;71:820–832.
22 Palisano RJ, Rosenbaum PL, Walter S, et al. Development andreliability of a system to classify gross motor function in children withcerebral palsy. Dev Med Child Neurol. 1997;39:214–223.
23 Gordis L. Epidemiology. Philadelphia, Pa: WB Saunders Co; 1996.
24 Children With Disabilities in Ontario: A Profile of Children’s Services, Part1: Children, Families, and Services. Hamilton, Ontario, Canada: CanChild,Centre for Childhood Disability Research; 2000.
25 Law M, Darrah J, Pollock N, et al. Family-centered functionaltherapy for children with cerebral palsy: an emerging practice model.Physical & Occupational Therapy in Pediatrics. 1998;18:83–102.
26 McDougall J, King GA, Malloy-Miller T, et al. A checklist to deter-mine the methods of intervention used in school-based therapy:development and pilot testing. Physical & Occupational Therapy inPediatrics. 1999;19(2):53–77.
27 Hayduk LA. Structural Equation Modeling With LISREL: Essentials andAdvances. Baltimore, Md: Johns Hopkins University Press; 1987.
28 Kleinbaum DG, Kupper LL, Muller KE, Nizam A. Applied RegressionAnalysis and Other Multivariable Methods. Pacific Grove, Calif: DuxburyPress; 1998.
29 Raykov T, Marcoulides GA. On desirability of parsimony in struc-tural equation model selection. Structural Equation Modeling. 1999;6:292–300.
30 Portney LG, Watkins MP. Foundations of Clinical Research: Applicationsto Practice. East Norwalk, Conn: Appleton & Lange; 1993.
31 Gordon J, Ghez C. Muscle receptors and spinal reflexes: the stretchreflex. In: Kandel ER, Schwarz JH, Jessell JM, eds. Principles of NeuralScience. 3rd ed. New York, NY: Elsevier; 1991.
32 Bobath B. Abnormal Postural Reflex Activity Caused by Brain Lesions.2nd ed. London, United Kingdom: Heinemann; 1981.
33 Almeida GL, Campbell SK, Girolami GL, et al. Multidimensionalassessment of motor function in a child with cerebral palsy followingintrathecal administration of baclofen. Phys Ther. 1997;77:751–764.
34 Flett PJ, Stern LM, Waddy H, et al. Botulinum toxin A versus fixedcast stretching for dynamic calf tightness in cerebral palsy. J PaediatrChild Health. 1999;35:71–77.
35 Gul SM, Steinbok P, McLeod K. Long-term outcome after selectiveposterior rhizotomy in children with spastic cerebral palsy. PediatrNeurosurg. 1999;31:84–95.
36 Valvano J, Long T. Neurodevelopmental treatment: a review of thewritings of the Bobaths. Pediatric Physical Therapy. 1991;3:125–129.
37 Bly L, Whiteside A. Facilitation Techniques Based on NDT Principles.San Antonio, Tex: Therapy Skill Builders; 1997.
38 Bly L. Baby Treatment Based on NDT Techniques. San Antonio, Tex:Therapy Skill Builders; 1999.
39 Campbell SK. Consensus statements. Proceedings of the ConsensusConference on the Efficacy of Physical Therapy in the Management ofCerebral Palsy. Pediatric Physical Therapy. 1990;2:175–176.
40 Campbell SK. Therapy programs for children that last a lifetime.Physical & Occupational Therapy in Pediatrics. 1997;17(1):1–15.
41 Lollar DJ. Preventing Secondary Conditions Associated With Spina Bifidaor Cerebral Palsy. Washington, DC: Spina Bifida Association of America;1994.
42 Morgan GA, MacTurk RH, Hrncir EJ. Mastery motivation: overview,definitions, and conceptual issues. In: MacTurk RH, Mogan GA, eds.Mastery Motivation: Origins, Conceptualizations, and Applications. Nor-wood, NJ: Ablex; 1995:1–17.
43 Campbell SK. Models for decision making in pediatric neurologicphysical therapy. In: Campbell SK, ed. Decision Making in PediatricNeurologic Physical Therapy. New York, NY: Churchill Livingstone Inc;1999:1–22.
44 Rosenbaum P, King S, Law M, et al. Family-centered service: aconceptual framework and research review. Physical & OccupationalTherapy in Pediatrics. 1998;18:1–20.
45 Krefting LH. The use of conceptual models in clinical practice. CanJ Occup Ther. 1985;52:173–178.
46 Mattingly C. What is clinical reasoning? Am J Occup Ther. 1991;45:979–986.
47 Scrutton D, Rosenbaum P. Locomotor development in childrenwith cerebral palsy. In: Connolly KJ, Forssberg H, eds. Neurophysiologyand Neuropsychology of Motor Development. London, United Kingdom:MacKeith Press; 1997:101–123.
48 Trahan J, Marcoux S. Factors associated with the inability ofchildren with cerebral palsy to walk at six years: a retrospective study.Dev Med Child Neurol. 1994;36:787–795.
49 Badell-Ribera A. Cerebral palsy: postural-locomotor prognosis inspastic diplegia. Arch Phys Med Rehabil. 1985;66:614–619.
50 Lin J-P. Dorsal rhizotomy and physical therapy [editorial]. Dev MedChild Neurol. 1998;40:219.
51 Giuliani CA. Dorsal rhizotomy for children with cerebral palsy:support for concepts of motor control. Phys Ther. 1991;71:248–259.
Physical Therapy . Volume 82 . Number 3 . March 2002 Bartlett and Palisano . 247
������
������
������
������
�
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

52 Campbell SK. Central nervous system dysfunction in children.In: Campbell SK, ed. Pediatric Neurologic Physical Therapy. New York, NY:Churchill Livingstone Inc; 1991:1–17.
53 Nashner LM, Shumway-Cook A, Marin O. Stance posture control inselect groups of children with cerebral palsy: deficits in sensoryorganization and muscular coordination. Exp Brain Res. 1983;49:393–409.
54 Brogren E, Hadders-Algra M, Forssberg H. Postural control inchildren with spastic diplegia: muscle activity during perturbations insitting. Dev Med Child Neurol. 1996;38:379–388.
55 Beals RK. Spastic paraplegia and diplegia: an evaluation of non-surgical and surgical factors influencing the prognosis for ambulation.J Bone Joint Surg Am. 1966;48:827–846.
56 Tardieu C, Tardieu G, Colbeau-Justin P, et al. Trophic muscleregulation in children with congenital cerebral lesions. J Neurol Sci.1979;42:357–364.
57 Hufschmidt A, Mauritz KH. Chronic transformation of muscle inspasticity: a peripheral contribution to increased tone. J Neurol. 1985;48:676–685.
58 Bax MCO, Brown JK. Contractures and their therapy [editorial].Dev Med Child Neurol. 1985;27:423–424.
59 Sutherland DH, Davids JR. Common gait abnormalities of the kneein cerebral palsy. Clin Orthop. 1993;288:139–147.
60 Olney SJ, MacPhail HA, Heeden DM, Boyce WF. Work and power inhemiplegic cerebral palsy gait. Phys Ther. 1990;70:431–438.
61 Wiley ME, Damiano DL. Lower-extremity strength profiles in spasticcerebral palsy. Dev Med Child Neurol. 1998;40:100–107.
62 Rose J, Medeiros JM, Parker R. Energy cost index as an estimate ofenergy expenditure of cerebral-palsied children during assisted ambu-lation. Dev Med Child Neurol. 1985;27:485–490.
63 Rose J, Gamble JG, Medeiros J, et al. Energy cost of walking innormal children and in those with cerebral palsy: comparison of heartrate and oxygen uptake. J Pediatr Orthop. 1989;9:276–279.
64 Kramer JF, MacPhail HEA. Relationships among measures of walk-ing efficiency, gross motor ability, and isokinetic strength in adoles-cents with cerebral palsy. Pediatric Physical Therapy. 1994;6:3–8.
65 Damiano DL, Kelly LE, Vaughn CL. Effects of quadriceps femorismuscle strengthening on crouch gait in children with spastic diplegia.Phys Ther. 1995;75:658–671.
66 Werner EE. Vulnerable but invincible: high-risk children from birthto adulthood. Acta Paediatr. 1997;422:103–105.
67 Thelen E, Smith LB. A Dynamic Systems Approach to the Development ofCognition and Action. Cambridge, Mass: The MIT Press; 1994.
68 Cintas HL. The relationship of motor skill level and risk-takingduring exploration in toddlers. Pediatric Physical Therapy. 1992;4:165–170.
69 Jennings KD, Connors RE, Stegman CE. Does a physical handicapalter the development of mastery motivation during the preschoolyears? J Am Acad Child Adol Psych. 1988;27:312–317.
70 Cintas HL. Cross-cultural similarities and differences in develop-ment and the impact of parental expectations on motor behavior.Pediatric Physical Therapy. 1995;7:103–111.
71 Schon DA. The Reflective Practitioner. New York, NY: Basic Books;1983.
72 Andresen EM, Lollar DJ, Meyers AR. Disability outcomes research:Why this supplement, on this topic, at this time? Arch Phys Med Rehabil.2000;81(12 suppl 2):S1–S4.
73 Gray DB, Hendershot GE. The ICIDH-2: developments for a newera of outcomes research. Arch Phys Med Rehabil. 2000;81(12 suppl2):S10–S14.
74 Piper MC. Efficacy of physical therapy: rate of motor developmentin children with cerebral palsy. Pediatric Physical Therapy. 1990;2:126–130.
75 Kane RL. Understanding Health Care Outcomes Research. Gaithersburg,Md: Aspen; 1997.
Appendix.Family Ecology
Family ExpectationsChild Improvement Locus of Control: to be completed by a parent;estimated time to complete is 10 minutesa) Importance (0 is unimportant, 10 is very important—please circle)
0 1 2 3 4 5 6 7 8 9 10b) Feasibility (1 is not feasible at all, 3 is feasible—please circle)
1 2 3c) Additional resources required (circle all that apply)
1 training2 time3 other (please indicate)
248 . Bartlett and Palisano Physical Therapy . Volume 82 . Number 3 . March 2002 by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from

2002; 82:237-248.PHYS THER. Doreen J Bartlett and Robert J PalisanoClinical ReasoningChildren With Cerebral Palsy: Implications forInfluencing the Acquisition of Motor Abilities of Physical Therapists' Perceptions of Factors
References
http://ptjournal.apta.org/content/82/3/237#BIBLfor free at: This article cites 42 articles, 10 of which you can access
Cited by
http://ptjournal.apta.org/content/82/3/237#otherarticles
This article has been cited by 5 HighWire-hosted articles:
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on June 26, 2012http://ptjournal.apta.org/Downloaded from