Embed Size (px)
Citation preview

PHOTO OFDr. Thomas
1
Summary of Guidelines Summary of Guidelines
• JNC VI guidelines focus on: - Absolute risks and benefits used in compiling recommendations - Strong emphasis on risk stratification of patients including awareness of the importance of isolated systolic blood pressure - Re-emphasis on importance of lifestyle modification in prevention and treatment - First line drugs for uncomplicated patient are diuretics and beta-blockers
• JNC VI guidelines focus on: - Absolute risks and benefits used in compiling recommendations - Strong emphasis on risk stratification of patients including awareness of the importance of isolated systolic blood pressure - Re-emphasis on importance of lifestyle modification in prevention and treatment - First line drugs for uncomplicated patient are diuretics and beta-blockers
2
4
Blood Pressure Classification Blood Pressure Classification
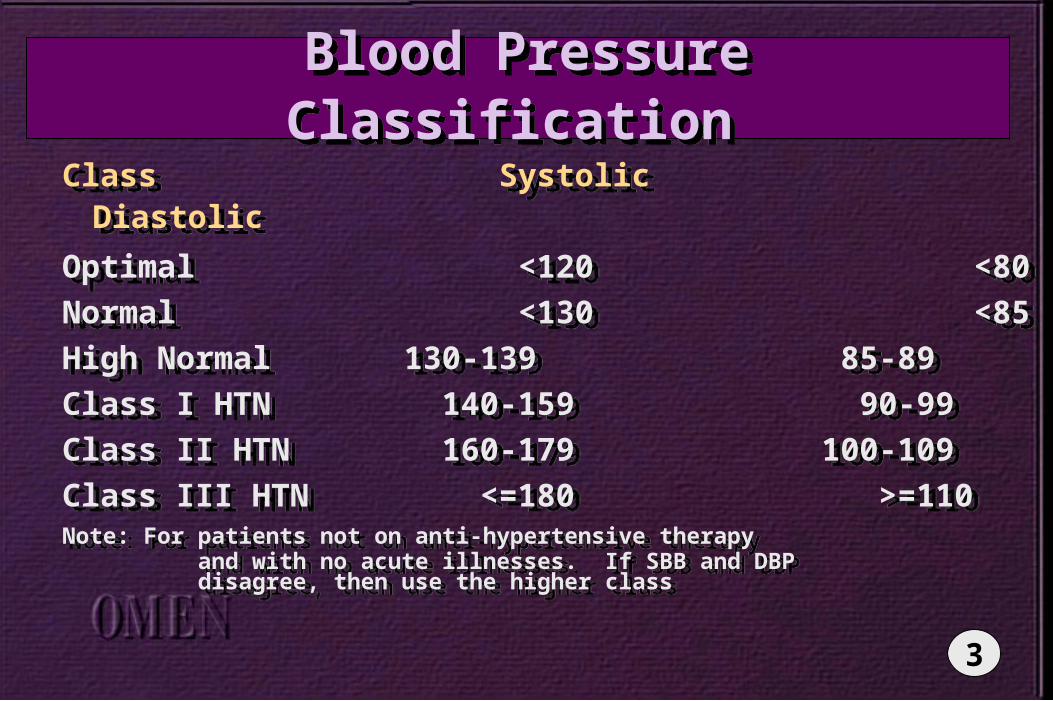
Class Systolic Diastolic
Optimal <120 <80
Normal <130 <85
High Normal 130-139 85-89
Class I HTN 140-159 90-99
Class II HTN 160-179 100-109
Class III HTN <=180 >=110Note: For patients not on anti-hypertensive therapy and with no acute illnesses. If SBB and DBP disagree, then use the higher class
Class Systolic Diastolic
Optimal <120 <80
Normal <130 <85
High Normal 130-139 85-89
Class I HTN 140-159 90-99
Class II HTN 160-179 100-109
Class III HTN <=180 >=110Note: For patients not on anti-hypertensive therapy and with no acute illnesses. If SBB and DBP disagree, then use the higher class
3
Blood Pressure Follow-Up Blood Pressure Follow-Up
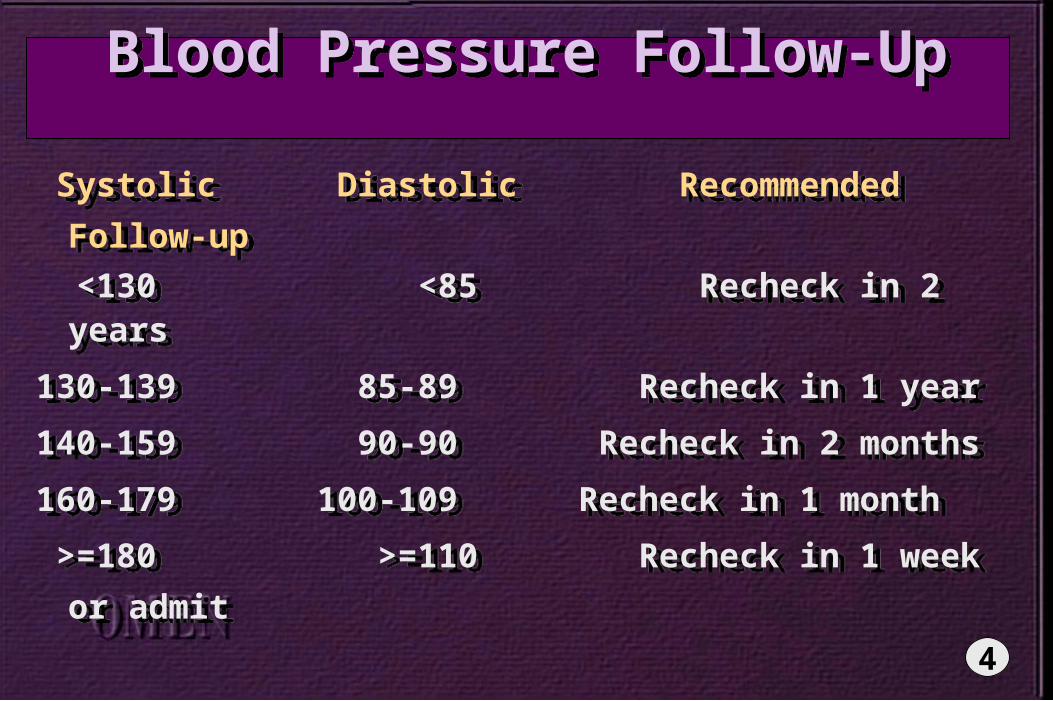
Systolic Diastolic Recommended Follow-up
<130 <85 Recheck in 2 years
130-139 85-89 Recheck in 1 year
140-159 90-90 Recheck in 2 months
160-179 100-109 Recheck in 1 month
>=180 >=110 Recheck in 1 week or admit
Systolic Diastolic Recommended Follow-up
<130 <85 Recheck in 2 years
130-139 85-89 Recheck in 1 year
140-159 90-90 Recheck in 2 months
160-179 100-109 Recheck in 1 month
>=180 >=110 Recheck in 1 week or admit
4

Ambulatory BP Monitoring Ambulatory BP Monitoring
• Correlates more closely with target organ damage
• Helpful in certain populations: - Suspected “white coat hypertension” - Suspected drug resistance - Hypotensive symptoms on therapy - Episodic HTN - Autonomic dysfunction - NOT for use in basic diagnosis or screening for HTN
• Correlates more closely with target organ damage
• Helpful in certain populations: - Suspected “white coat hypertension” - Suspected drug resistance - Hypotensive symptoms on therapy - Episodic HTN - Autonomic dysfunction - NOT for use in basic diagnosis or screening for HTN
5
Risk-based Treatment Groups Risk-based Treatment Groups
• Risk Group A: - No risk factors, no target organ disease, no known cardiovascular disease
• Risk Group B: - At least one risk factor but NOT diabetes, no target organ disease or cardiovascular disease
• Risk group C: - Target organ disease and / or cardiovascular disease and / or diabetes, with or without other risk factors
• Risk Group A: - No risk factors, no target organ disease, no known cardiovascular disease
• Risk Group B: - At least one risk factor but NOT diabetes, no target organ disease or cardiovascular disease
• Risk group C: - Target organ disease and / or cardiovascular disease and / or diabetes, with or without other risk factors
6
Initial Evaluation Initial Evaluation
• Assess for target organ damage at baseline
• Identify any other cardiovascular risk factors
• Identify any potential secondary causes
• Assess for target organ damage at baseline
• Identify any other cardiovascular risk factors
• Identify any potential secondary causes
7
Lab Evaluation Lab Evaluation
• Recommended tests to screen for target organ damage - Urinalysis - Renal function - CBC - Electrolytes - HDL - 12 lead EKG
• Optional tests to screen for target organ damage (not all-inclusive): - Creatinine clearance - Hemoglobin A1C - Urine microalbumin - TSH - 24 hour urine for protein - Fasting, full lipid panel
• Recommended tests to screen for target organ damage - Urinalysis - Renal function - CBC - Electrolytes - HDL - 12 lead EKG
• Optional tests to screen for target organ damage (not all-inclusive): - Creatinine clearance - Hemoglobin A1C - Urine microalbumin - TSH - 24 hour urine for protein - Fasting, full lipid panel
8
Cardiovascular Risk Factors Cardiovascular Risk Factors
• Major Risk Factors:
- Smoking
- Dyslipidemia
- Diabetes
- Age >60 years
- All males and postmenopausal females
- Family history of CAD in women < 65 or men < 55 years old
• Major Risk Factors:
- Smoking
- Dyslipidemia
- Diabetes
- Age >60 years
- All males and postmenopausal females
- Family history of CAD in women < 65 or men < 55 years old
9
Target Organ / Cardiovascular Disease Target Organ / Cardiovascular Disease
• Heart Disease - Left ventricular hypertrophy (LVH) - Angina or prior myocardial infarction - Prior coronary revascularization - Heart failure
• Stroke or transient ischemic attack• Nephropathy• Peripheral Vascular Disease• Hypertensive retinopathy
• Heart Disease - Left ventricular hypertrophy (LVH) - Angina or prior myocardial infarction - Prior coronary revascularization - Heart failure
• Stroke or transient ischemic attack• Nephropathy• Peripheral Vascular Disease• Hypertensive retinopathy
10
Risk-Based Treatment Options Risk-Based Treatment Options
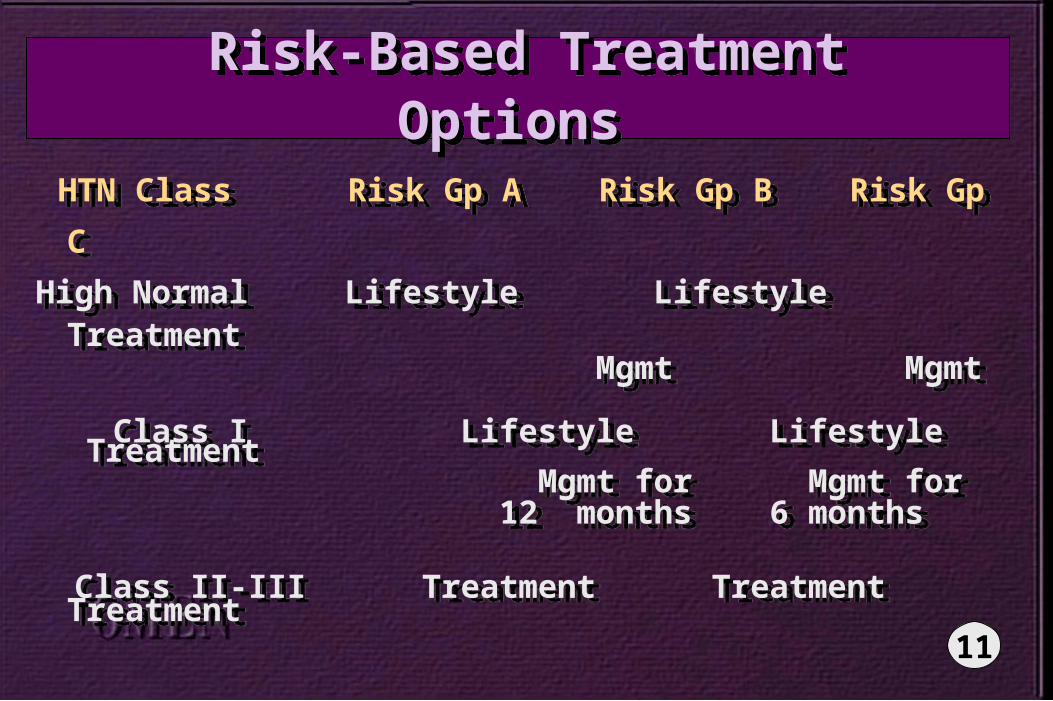
HTN Class Risk Gp A Risk Gp B Risk Gp C
High Normal Lifestyle Lifestyle Treatment Mgmt Mgmt
Class I Lifestyle Lifestyle Treatment Mgmt for Mgmt for 12 months 6 months
Class II-III Treatment Treatment Treatment
HTN Class Risk Gp A Risk Gp B Risk Gp C
High Normal Lifestyle Lifestyle Treatment Mgmt Mgmt
Class I Lifestyle Lifestyle Treatment Mgmt for Mgmt for 12 months 6 months
Class II-III Treatment Treatment Treatment
11
Clues for Secondary Causes Clues for Secondary Causes
• Age, history, severity of HTN do not correlate with clinical picture
• Poor response to therapy
• Previously well-controlled
• Class III hypertension
• Sudden onset of hypertension
• Age, history, severity of HTN do not correlate with clinical picture
• Poor response to therapy
• Previously well-controlled
• Class III hypertension
• Sudden onset of hypertension
12
Lifestyle Modification Lifestyle Modification
Should be seen as part of bothprevention and treatment
•
Diet modification - DASH diet
• Weight reduction
• Increased physical activity
Should be seen as part of bothprevention and treatment
•
Diet modification - DASH diet
• Weight reduction
• Increased physical activity
13
Lifestyle Modification Lifestyle Modification
• Moderation of sodium intake• Maintain appropriate intake of: - Potassium - Calcium - Magnesium
• Improve modifiable CV risk factors• Questionable benefit - caffeine reduction, relaxation / biofeedback
• Moderation of sodium intake• Maintain appropriate intake of: - Potassium - Calcium - Magnesium
• Improve modifiable CV risk factors• Questionable benefit - caffeine reduction, relaxation / biofeedback
14
Treatment Steps Treatment Steps
• Step 1: If no other added indication, start with either diuretic or beta-blocker
• Step 2: If no response, increase dose
• Step 3a: If tolerated at higher dose, add a second drug
• Step 3b: If not tolerated at higher, substitute a new drug in its place
• Step 1: If no other added indication, start with either diuretic or beta-blocker
• Step 2: If no response, increase dose
• Step 3a: If tolerated at higher dose, add a second drug
• Step 3b: If not tolerated at higher, substitute a new drug in its place
15
Treatment Steps Treatment Steps • Step 4: If still not controlled then: - Continue adding agents from other classes - Consider referral to a hypertensive specialist
• Resistant HTN: - Defined as BP > 140 / 90 or isolated systolic > 160 on three drugs (including a diuretic) at max dose
- Often still related to volume overload - Consider referral to hypertensive specialist
• Step 4: If still not controlled then: - Continue adding agents from other classes - Consider referral to a hypertensive specialist
• Resistant HTN: - Defined as BP > 140 / 90 or isolated systolic > 160 on three drugs (including a diuretic) at max dose
- Often still related to volume overload - Consider referral to hypertensive specialist
16
Treatment Steps Treatment Steps • For Stage III hypertensive patient: - Start pharmacologic therapy sooner - Increase the dose or add a second agent sooner - Look for secondary causes sooner
• Step-down therapy: - Begin slowly weaning medications after adequate control for one year
- May be able to accelerate decrease in medications if also adherent to lifestyle modifications
• For Stage III hypertensive patient: - Start pharmacologic therapy sooner - Increase the dose or add a second agent sooner - Look for secondary causes sooner
• Step-down therapy: - Begin slowly weaning medications after adequate control for one year
- May be able to accelerate decrease in medications if also adherent to lifestyle modifications
17
Special Populations Special Populations • African-Americans:
- More effective: diuretics, calcium antagonists
- Less effective: beta-blockers, ACE inhibitors as mono-therapies
- Okay to use less effective if have an additional indication
• African-Americans:
- More effective: diuretics, calcium antagonists
- Less effective: beta-blockers, ACE inhibitors as mono-therapies
- Okay to use less effective if have an additional indication
18
Special Populations Special Populations • Children / Adolescents:
- Aggressively identify secondary causes - Lifestyle modification very important - Treat with smaller doses of medication - Avoid ACE and Angiotensin-II receptor blockers in sexually active / pregnant women - Check for use of anabolic steroids - No need to prohibit from exercise if asymptomatic
• Children / Adolescents:
- Aggressively identify secondary causes - Lifestyle modification very important - Treat with smaller doses of medication - Avoid ACE and Angiotensin-II receptor blockers in sexually active / pregnant women - Check for use of anabolic steroids - No need to prohibit from exercise if asymptomatic
19
Special Populations Special Populations • Females: - Contraceptive use: If BP increase seems related to OCP use, discontinue OCP and BP should normalize
- Pregnancy: Defined as essential HTN if BP elevated before pregnant or before the 20th week of gestation - Avoid ACE, A-II receptor blockers - Use diuretics, alpha-methyl dopa, beta-blockers (after the 1st trimester)
• Females: - Contraceptive use: If BP increase seems related to OCP use, discontinue OCP and BP should normalize
- Pregnancy: Defined as essential HTN if BP elevated before pregnant or before the 20th week of gestation - Avoid ACE, A-II receptor blockers - Use diuretics, alpha-methyl dopa, beta-blockers (after the 1st trimester)
20
Special Populations Special Populations • Elderly: - Isolated systolic HTN an important, more common problem
- Pulse pressure (SBP-DBP) a good predictor of risk in this population
- More effective: thiazide diuretic, thiazide + beta-blocker, and long acting dihydropyridine calcium antagonists
- Avoid postural hypotensive symptoms - Avoid cognitive symptoms
• Elderly: - Isolated systolic HTN an important, more common problem
- Pulse pressure (SBP-DBP) a good predictor of risk in this population
- More effective: thiazide diuretic, thiazide + beta-blocker, and long acting dihydropyridine calcium antagonists
- Avoid postural hypotensive symptoms - Avoid cognitive symptoms
21
Additional Indications Additional Indications
• Coronary Artery Disease: - Avoid aggressive, quick lowering of BP
- Added benefit: beta-blocker, long-acting calcium antagonists
- Avoid: short-acting calcium antagonists
- ACE inhibitors may be useful after MI with LV function dysfunction
• Coronary Artery Disease: - Avoid aggressive, quick lowering of BP
- Added benefit: beta-blocker, long-acting calcium antagonists
- Avoid: short-acting calcium antagonists
- ACE inhibitors may be useful after MI with LV function dysfunction
22

Additional Indications Additional Indications
• Heart Failure: - ACE inhibitors are standard therapy
- May substitute vasodilator and nitrate or A-II receptor blocker if not tolerated
- Carvedilol and other beta-blockers are showing more benefit in these patients
- Long-acting dihydropyridines are safe to use in these patients for the treatment of angina
• Heart Failure: - ACE inhibitors are standard therapy
- May substitute vasodilator and nitrate or A-II receptor blocker if not tolerated
- Carvedilol and other beta-blockers are showing more benefit in these patients
- Long-acting dihydropyridines are safe to use in these patients for the treatment of angina
23

Additional Indications Additional Indications
• Diabetes:
- Blood pressure control an imperative for preventing target organ damage from DM
- ACE inhibitors help prevent / reduce proteinuria
- Avoid beta-blockers only if hypoglycemia is a significant risk or past history
• Diabetes:
- Blood pressure control an imperative for preventing target organ damage from DM
- ACE inhibitors help prevent / reduce proteinuria
- Avoid beta-blockers only if hypoglycemia is a significant risk or past history
24
Additional Indications Additional Indications
• Dyslipidemia: - High dose thiazide and loop diuretics can induce increases in total cholesterol, LDL and triglycerides
- Low dose thiazides can be appropriate - Diet modification can reduce this effect - Beta-blockers may transiently increase triglycerides and lower HDL
- Alpha-blockers may slightly reduce total cholesterol and increase HDL
• Dyslipidemia: - High dose thiazide and loop diuretics can induce increases in total cholesterol, LDL and triglycerides
- Low dose thiazides can be appropriate - Diet modification can reduce this effect - Beta-blockers may transiently increase triglycerides and lower HDL
- Alpha-blockers may slightly reduce total cholesterol and increase HDL
24 A
Additional Indications Additional Indications
• Reactive / Obstructive Airway Disease:
- Avoid beta-blockers and alpha-beta- blockers (carvedilol) unless only minimal lung disease and tolerated well by the patient
- Check for any OTC remedies for asthma since may exacerbate blood pressure
• Reactive / Obstructive Airway Disease:
- Avoid beta-blockers and alpha-beta- blockers (carvedilol) unless only minimal lung disease and tolerated well by the patient
- Check for any OTC remedies for asthma since may exacerbate blood pressure
24 B
Summary Points Summary Points • Focus on risk-adjusting each patient to better meet that patient’s needs• Consider additional indications / added benefits or risks in your choice of therapy• Emphasize lifestyle modification focusing on cardiovascular healthy habits for both treatment and prevention• Remember the importance of isolated systolic hypertension especially in the elderly
• Focus on risk-adjusting each patient to better meet that patient’s needs• Consider additional indications / added benefits or risks in your choice of therapy• Emphasize lifestyle modification focusing on cardiovascular healthy habits for both treatment and prevention• Remember the importance of isolated systolic hypertension especially in the elderly
24 C
PHOTO OFDr. Dennis
25
Profile Profile
Ms. Barile
• 45 year old female• Presented 2 years ago with BP 150 / 100 at routine exam• Previous BP had been in high-normal range
Initial Diagnosis• Hypertension
• BP 150 / 90
Ms. Barile
• 45 year old female• Presented 2 years ago with BP 150 / 100 at routine exam• Previous BP had been in high-normal range
Initial Diagnosis• Hypertension
• BP 150 / 9026
Profile Profile
Ms. BarileDiagnostic Tests• Comprehensive history and physical• Urinalysis• EKG• Blood tests for glucose, BUN, creatinine, electrolytes and cholesterol profile
Diagnosis• Essential hypertension without diabetes or target organ abnormalities
Ms. BarileDiagnostic Tests• Comprehensive history and physical• Urinalysis• EKG• Blood tests for glucose, BUN, creatinine, electrolytes and cholesterol profile
Diagnosis• Essential hypertension without diabetes or target organ abnormalities 26 A
Profile Profile
Ms. BarileTreatment• Referred to nutritionist for dietary counseling
• Salt-restricted, low-fat diet with reduced calories
• Lose weight through increased regular exercise
• Lisinopril - 10mg daily
Ms. BarileTreatment• Referred to nutritionist for dietary counseling
• Salt-restricted, low-fat diet with reduced calories
• Lose weight through increased regular exercise
• Lisinopril - 10mg daily
26 B

27

Classification of BP for AdultsAge 18 Years and Older
Classification of BP for AdultsAge 18 Years and Older
Systolic Diastolic Category (mmHg) (mmHg)
Optimal <120 <80 Normal <130 <85 High normal 130 - 139 85 - 89
Hypertension Stage I 140 - 159 90 - 99 Stage 2 160 - 179 100 - 109 Stage 3 > 180 > 110
Systolic Diastolic Category (mmHg) (mmHg)
Optimal <120 <80 Normal <130 <85 High normal 130 - 139 85 - 89
Hypertension Stage I 140 - 159 90 - 99 Stage 2 160 - 179 100 - 109 Stage 3 > 180 > 110
28
Optimal Blood Pressure Optimal Blood Pressure
Optimal blood pressure is
that value below which further
reduction garners no additional
benefit to morbidity or mortality
Optimal blood pressure is
that value below which further
reduction garners no additional
benefit to morbidity or mortality
29
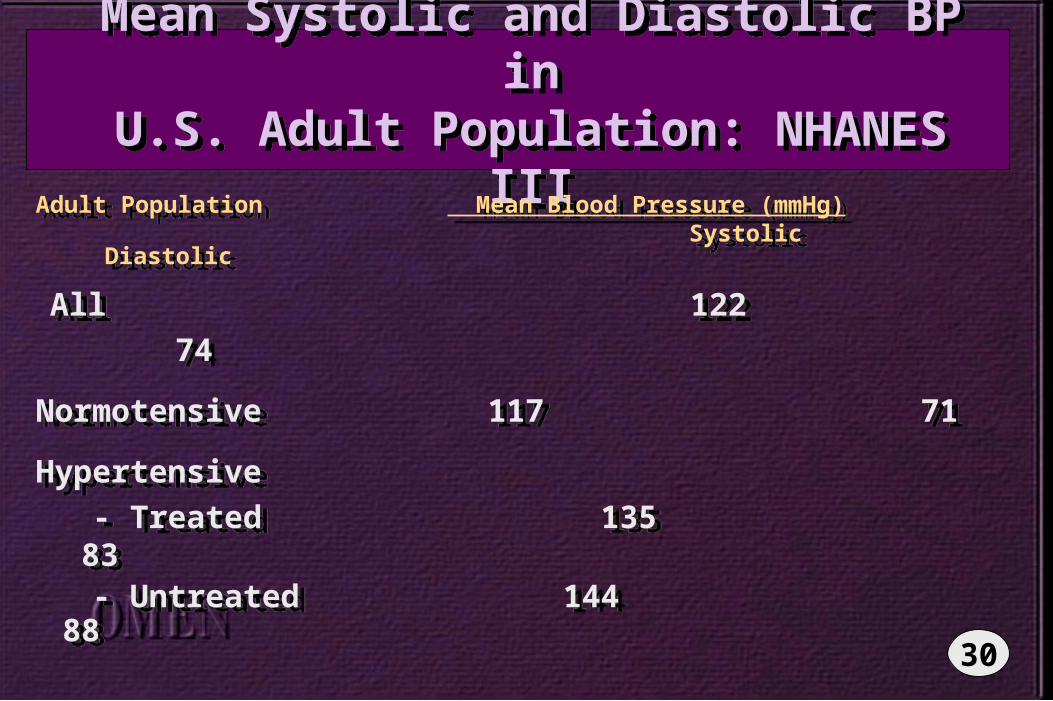
Mean Systolic and Diastolic BP inU.S. Adult Population: NHANES IIIMean Systolic and Diastolic BP inU.S. Adult Population: NHANES III
Adult Population Mean Blood Pressure (mmHg) Systolic Diastolic
All 122 74
Normotensive 117 71
Hypertensive
- Treated 135 83 - Untreated 144 88
Adult Population Mean Blood Pressure (mmHg) Systolic Diastolic
All 122 74
Normotensive 117 71
Hypertensive
- Treated 135 83 - Untreated 144 88
30

Office, Home and Ambulatory BloodPressure in 1438 Subjects
Age 25-64 Years: PAMELA Study
Office, Home and Ambulatory BloodPressure in 1438 Subjects
Age 25-64 Years: PAMELA Study
Blood Pressure (mmHg) Pulse SBP DBP Rate
Office 127 ± 17 82 ± 9.8 72 ± 8.6
Home 119 ± 17 75 ± 10 73 ± 10
24-hr mean 118 ± 11 74 ± 7 77 ± 8
Daytime 123 ± 11 79 ± 8 82 ± 9
Nighttime 108 ± 11 64 ± 8 67 ± 8
Blood Pressure (mmHg) Pulse SBP DBP Rate
Office 127 ± 17 82 ± 9.8 72 ± 8.6
Home 119 ± 17 75 ± 10 73 ± 10
24-hr mean 118 ± 11 74 ± 7 77 ± 8
Daytime 123 ± 11 79 ± 8 82 ± 9
Nighttime 108 ± 11 64 ± 8 67 ± 8
31
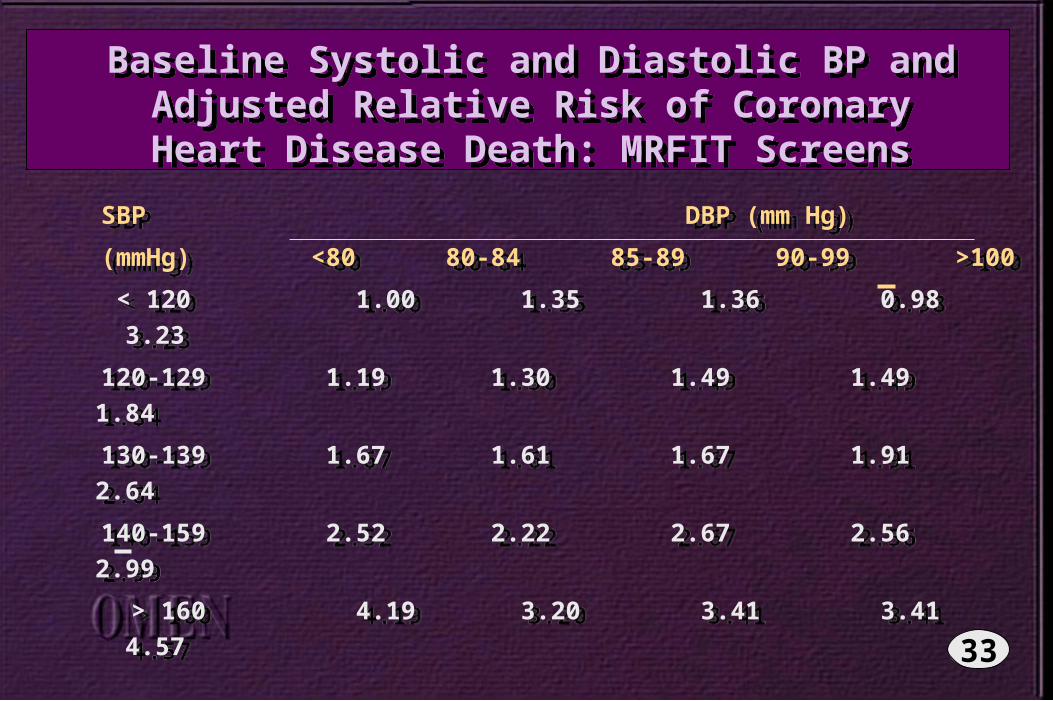
Baseline Systolic and Diastolic BP andAdjusted Relative Risk of Coronary
Heart Disease Death: MRFIT Screens
Baseline Systolic and Diastolic BP andAdjusted Relative Risk of Coronary
Heart Disease Death: MRFIT Screens
SBP DBP (mm Hg)
(mmHg) <80 80-84 85-89 90-99 >100
< 120 1.00 1.35 1.36 0.98 3.23
120-129 1.19 1.30 1.49 1.49 1.84
130-139 1.67 1.61 1.67 1.91 2.64
140-159 2.52 2.22 2.67 2.56 2.99
> 160 4.19 3.20 3.41 3.41 4.57
SBP DBP (mm Hg)
(mmHg) <80 80-84 85-89 90-99 >100
< 120 1.00 1.35 1.36 0.98 3.23
120-129 1.19 1.30 1.49 1.49 1.84
130-139 1.67 1.61 1.67 1.91 2.64
140-159 2.52 2.22 2.67 2.56 2.99
> 160 4.19 3.20 3.41 3.41 4.5733
34
35

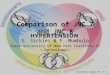
TOMHS TOMHS
n
Acebutolol 132 Active
Amlodipine 131 Treatment Placebo
Chlorthalidone 136 Total (n=234)
Doxazosin 134 (n=668)
Enalapril 135
n
Acebutolol 132 Active
Amlodipine 131 Treatment Placebo
Chlorthalidone 136 Total (n=234)
Doxazosin 134 (n=668)
Enalapril 135
36
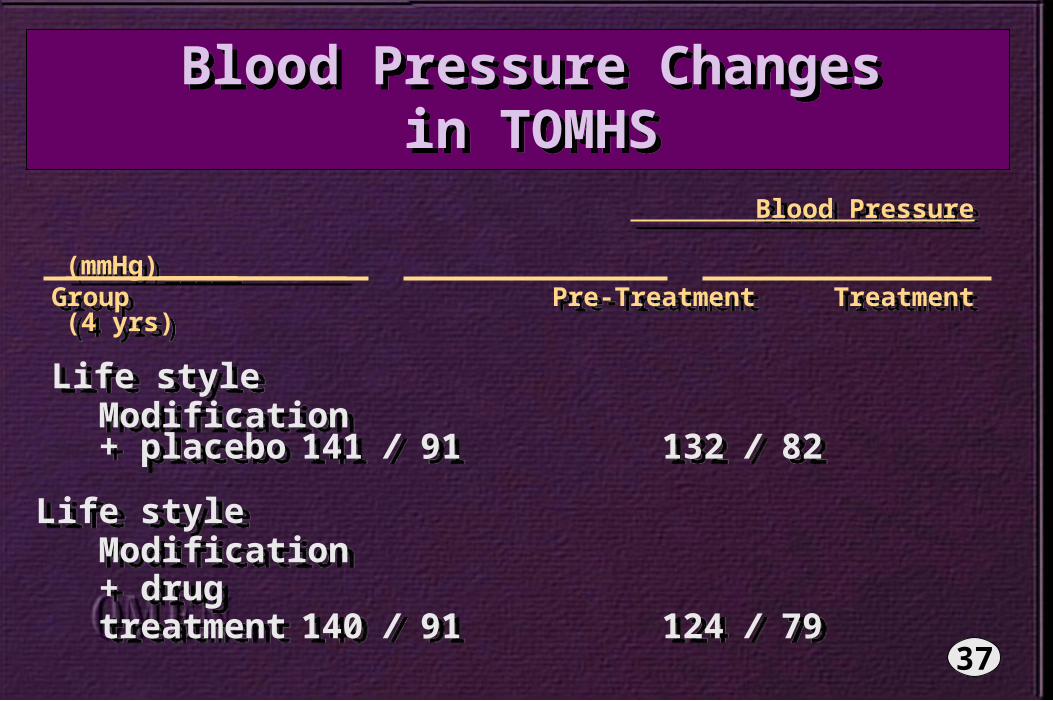
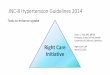
Blood Pressure Changesin TOMHS
Blood Pressure Changesin TOMHS
Blood Pressure (mmHg)_____ Group Pre-Treatment Treatment (4 yrs)
Life style Modification + placebo 141 / 91 132 / 82
Life style Modification + drug treatment 140 / 91 124 / 79
Blood Pressure (mmHg)_____ Group Pre-Treatment Treatment (4 yrs)
Life style Modification + placebo 141 / 91 132 / 82
Life style Modification + drug treatment 140 / 91 124 / 79
37
38
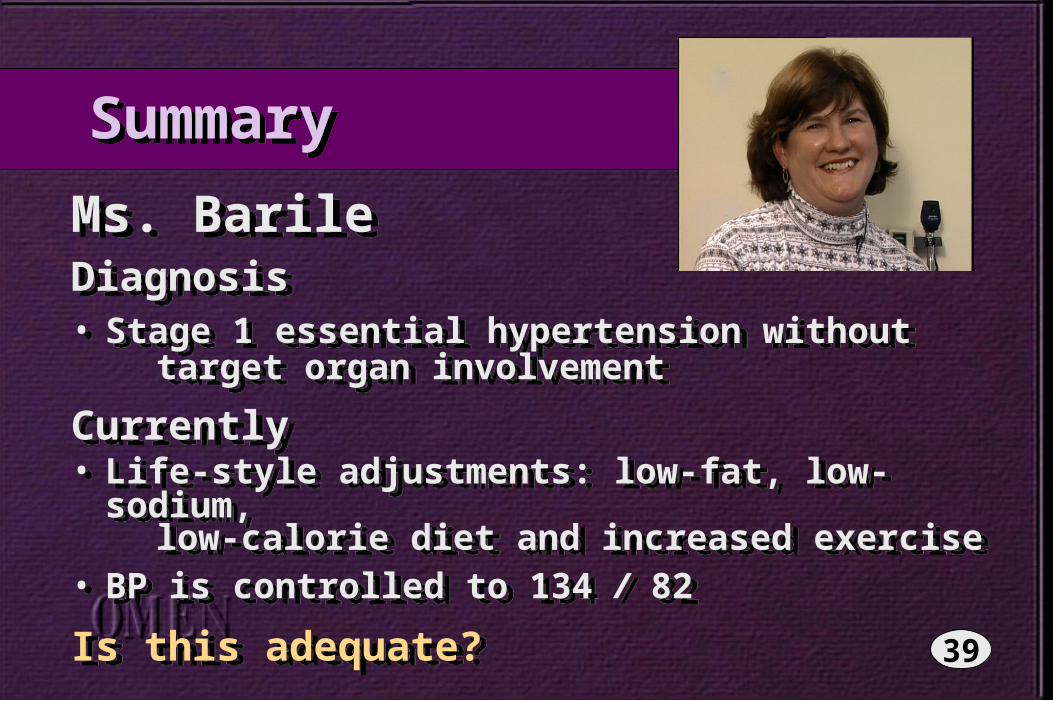
Summary Summary
Ms. BarileDiagnosis• Stage 1 essential hypertension without target organ involvement
Currently• Life-style adjustments: low-fat, low-sodium, low-calorie diet and increased exercise• BP is controlled to 134 / 82
Is this adequate?
Ms. BarileDiagnosis• Stage 1 essential hypertension without target organ involvement
Currently• Life-style adjustments: low-fat, low-sodium, low-calorie diet and increased exercise• BP is controlled to 134 / 82
Is this adequate? 39