Embed Size (px)
Citation preview

Philips in CPR
New Technologies Supporting AHA Guidelines
Jim HendrixEMS Marketing ManagerPhilips Medical Systems

Section 4: Adult Basic Life Support
(Circulation. 2005;112:IV-18-IV-34.)© 2005 American Heart Association.

Leading the Way in Intelligent Resuscitation
• CPR Coaching
• Step-by-Step instructions for bystander-initiated CPR and the minimally-trained rescuer
• SMART CPR for trained first responders• First AED to analyze presenting VF rhythm & advise
initial therapy of either a defibrillation shock or CPR followed by a shock
• Q-CPR• CPR Measurement and Feedback for ALS
professionals
• Quick Shock on all HeartStart Defibrillators• Shock after CPR in <10s, while heart is still
“primed”

CPR Coaching Since 2002
• Available on HeartStart FRx, HeartStart OnSite and HeartStart Home Defibrillators
• After shock, user is instructed to begin CPR and “for help with CPR press the flashing blue button”
• Step-by-step instructions including: • Airway Opening• “Timed” Breath Prompts• Compression Metronome
• Two minute CPR timer

What is SMART CPR?
• SMART CPR offers the opportunity for CPR first, before a shock
• Evaluates heart rhythm, automatically advises rescuer on initial therapy– Immediate shock for hearts that
are likely to benefit – CPR first for the hearts less likely
to benefit from a shock
• An alternative to “one-size fits all” therapy

Defibrillating VF Doesn’t Always Restore Circulation
Likely return ofcirculation witha shock
Time after collapse: ~4-5 min ~10 min
Traditional AED Therapy: Shocks then CPR No shock advised
Unlikely to return to circulation with shock
Asystole or “Flatline”

The Responder’s Dilemma
• The responder doesn’t know on arrival if the patient’s heart is receptive to a shock• What should they do? Shock first or CPR first?
Short or long duration VF? Did she already
receive bystander CPR?
Was it good, productive CPR?
Is her rhythm effected by medication?
Overdose?Does she have a diseased heart?
What is th
e cause of
arrest?
Exactly how many minutes did it take me to get here?
How long ago?

Applying the Latest Clinical Research to Help More Patients
• Designed to advise CPR first to patients with rhythms typical of long-duration arrest, without altering treatment for the most successful patient group*
• More informed, refined treatment decisions
• Supports a protocol the literature suggests may have better outcome
*Snyder, DE, et al. Wolf Creek Conference on Resuscitation. June 2005

Promising Alternative Therapy Protocol
Unlikely to return to circulation with shock
Asystole or “Flatline”
Therapy of choice:
Likely return ofcirculation witha shock
Shock first CPR first, then shock No shock; perform CPR
Wik L, et al. JAMA, 2003, 289;1389-1395Cobb LA, et al. JAMA,1999, 281;1182-1188Weisfeldt & Becker JAMA, 2002, 288; 3035-3038
Time: ~4-5 min ~10 min

What is Q-CPR?
• Q-CPR is the first and only CPR measurement and feedback tool seamlessly integrated into an ALS monitor/defibrillator (Philips HeartStart MRx) to promote high-quality CPR delivery by professional emergency responders in hospitals and EMS.

Real-Time Feedback
Compressions:1. Incomplete Release2. Compression depth shallow3. Compression rate slow or fast4. Compression depth5. Duty Cycle Ventilations:1. Volume low2. Frequency high or low3. Inflation time fast or slow

New Studies Validate the Value of Q-CPR Monitoring and Feedback Technology to Improve CPR Delivery by Trained Responders...
(Studies presented AHA)
• Dr. Jo Kramer-Johansen of Ulleval University Hospital, Oslo, Norway, reported on 108 cardiac arrests in three ambulance services in Europe, where the automatic verbal and visual feedback features of Q-CPR improved the quality of CPR delivered by the paramedics and emergency medical technicians (EMTs). With the use of Q-CPR, the median percentage of chest compressions within guidelines more than doubled from 24% to 53%. Additionally, there was a significant increase in the mean depth of compressions in those utilizing Q-CPR (34+9 mm to 38+6 mm), and a reduction in mean compression rate (121+18 to 109+12), which means that the performance was closer to current AHA guidelines for compression depth of 38 to 51mm and compression rate of 100 per minute

New Studies Validate the Value of Q-CPR Monitoring and Feedback Technology to Improve CPR Delivery by Trained Responders(continued)
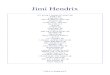
• Dr. Ben Abella, from the University of Chicago, presented results showing that Q-CPR also improved multiple parameters of CPR quality for cardiac arrest patients treated in-hospital. A related study on how the quality of CPR affects the success rates of defibrillation, by his colleague Dr. Dana Edelson, reported that a modest increase in the depth of chest compressions doubled the chance of defibrillation success, which is associated with more patients leaving the hospital alive. Dr. Edelson’s study garnered her the Resuscitation Science Symposium’s (ReSS) Young Investigator of the Year award

Shock success by compression depth Edelson et. al
50%
62%
93% 100%
0%10%20%30%40%50%60%70%80%90%
100%
<1 1-1.5 1.5-2 >2
Sh
ock
Su
cces
s, P
erce
nt
Compression Depth, Inches
n=10 n=5n=14n=13
P=0.02

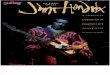
System Components
Therapy/CPR Cable
MRx Defib Pads
Compression Sensor

What is Quick Shock?
• All Philips HeartStart AEDs can deliver a shock less than 10 seconds after CPR
• A unique feature offered only by Philips• CPR primes the pump and Quick Shock
allows the rescuer to quickly deliver a shock

CPR is an Important Part of Resuscitation
• CPR Helps– CPR prior to defibrillation shock can help restore normal
heartbeat in more patients, especially those with longer duration VF1,2
– Beneficial effect of CPR disappears in seconds, so time to shock is very important 3,4
• Quick Shock maximizes benefits of CPR – Minimizes interruption of CPR
– Increases the chance that a shock will result in a successful return of circulation & may improve survival
1Cobb LA, et al. JAMA. 1999; 281(13):1182-11882Wik L, et al. JAMA. 2003 Mar 19; 289(11):1389-13953 Yu T, et al. Circulation. 2002; 106:368-3724 Eftestol T, et al. Circulation. 2002;105:2270-2273

Effect of stopping compressions on hemodynamics
Kern et al Resuscitation 1998;39:179-88
Blo
od
pre
ssu
re
Time
= chest compression
Illustration : Ben Abella

Peer-reviewed Research Supports Quick Shock
• “Interruptions of precordial compression for rhythm analyses that exceed 15 seconds before each shock compromise the outcome of CPR and increase the severity of post resuscitation myocardial dysfunction.”
• “The interval between discontinuation of chest compressions and delivery of a shock should be kept as short as possible.”
• Simply put, getting a shock to the heart as soon as possible after CPR can save more lives
Yu T, et al. Circulation. 2002; 106:368-372
Eftestol T, et al. Circulation. 2002;105:2270-2273

Shock success by pre-shock pauseEdelson et. al
100%
74%67%
38%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
=<10 10.1-20 20.1-30 >30
Pre-Shock Pause, Seconds
Sh
ock
Su
cces
s, P
erce
nt
P<0.01

HeartStartFR2+10 seconds
100%
80%
60%
20%
5 10 15 20 2500%
Survival
Time to shockin seconds
40%
30
Auto
Times measured from end of Stop-CPR prompt, with AEDs at maximum energy
HeartStart OnSite, Home & FRx, MRx 5 seconds
Survival Closely Linked to Speed of Shock Delivery After CPR
Survival data: Swine; 7 minutes of VF Yu T, et al. Circulation. 2002; 106:368-372

In Summary
• CPR Coaching • Step-by-Step instructions for bystander-initiated CPR
and the minimally-trained rescuer
• Q-CPR• CPR Measurement and Feedback for ALS
professionals
• SMART CPR for trained first responders• First AED to analyze presenting VF rhythm & advise
initial therapy of either a defibrillation shock or CPR followed by a shock
• Quick Shock on all HeartStart Defibrillators• Shock after CPR in <10s, while heart is still “primed”

Thank You!






















![₪[martin gardner] aha aha insight](https://img.pdfslide.us/doc/110x75/568cad201a28ab186daa6515/martin-gardner-aha-aha-insight.jpg)


