-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
1/28
PhenytoinVS
levetiracetamfor seizure prophylaxis
in secondary seizure
Kristy WuMedicine Rotation
Western University of Health SciencesCollege of Pharmacy,
PSIII
Preceptor: Doreen Pon, PharmD
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
2/28
Objectives
Introduce patient case
Brief review of secondary CNS lymphoma andsecondary seizure
Brief review of phenytoin and levetiracetam Discuss the clinical
trials of phenytoin and
levetiracetam comparisons in seizure prophylaxis
Advantages of levetiracetam over phenytoin
Evaluation of the patient case
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
3/28
Patient CaseRH is a 69 year-old male with aggressive diffuse
large B-cell non-
Hodgkinlymphoma who is being admitted for autologous stem
cell
transplantationwith conditioning chemotherapy of BEAM
(carmustine, etoposide,cytarabine, melphalan)
HPI: Diagnosed in 10/2009 Bone marrow biopsy showed involvement
with lymphoma on
10/14/2009 The cytogenetics were normal
Had 3 cycles of R-CHOP with 3rd cycle given on 11/30/2009
Developed new onset seizure on 12/15/2009 MRI of the brain: mass in
the right occipital lobe Treated with phenytoin and dexamethasone
Received 2 cycles of high-dose methotrexate with cytarabine in
12/2009 and had complete remission
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
4/28
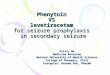
Patient Case
Brain MRI of 12/2009:
3 x 2.2 x 2.2 cm mass in the right
occipital lobe extending toward the corpuscallosum without
midline shift or evidenceof herniation
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
5/28
Patient Case
PMH Type 2 DM
Hypertension
Hypercholesterolemia
Sleep apnea Benign prostatic hypertrophy.
FH
There is no cancer history in the family
Father heart problem; paternal uncle heartproblem; maternal
grandfather heart attackyears ago
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
6/28
Patient Case
Medications
Phenytoin PO 500mg/400mg at bedtimealternating every other
day
trazodone, buspirone, fluconazole, nystatin,acyclovir, ursodiol,
famotidine, metformin,Flomax
Allergies: NKDA
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
7/28
Clinical Question
Can levetiracetam (Keppra) beused as 1st line option for
seizureprophylaxis in secondary seizure?
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
8/28
Secondary CNS lymphoma ~ 10-30% of systemic lymphoma have
secondary CNS
involvement.
Almost all CNS lymphoma are non-Hodgkin B-cell tumors
Typically develops in the subcortical and subependymal
whitematter and the corpus striatum, and may extend to
corpuscallosum
Spinal cord is frequently affected
Clinical presentation is nonspecific, may involve focal
neurologicimpairment, headache, confusion and seizures.
Zee CS, Neuroradiology: A Study Guide. 1996:158-60.Gerstner ER,
et al. Blood. Sep 2008;112(5):1658-61.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
9/28
Secondary Seizure
Symptomatic epilepsy Secondary to known structural or
metabolic
diseases adversely affecting the brain Disorders included:
drug-induced, alcohol related,
stroke, trauma, brain infection, neurosurgery,neoplasm,
metabolic disorders, degenerative CNSconditions
Seizure due to CNS metastases: should receiveanticonvulsive
treatment with phenytoin
Fauci, AS, et al. Harrisons principles of internal medicine,
17th edition. Chap 270, Sec 4, Oncologic Emergencies.World Health
Organization.
http://www.who.int/mediacentre/factsheets/fs999/en/index.html
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
10/28
Phenytoin FDA indications: management of generalized
tonic-clonic and
complex partial seizures; prevention of seizures following
head
trauma/neurosurgery
Mechanism of Actions: Neuronal sodium channel blocker
PK profile:
Absorption depends on the formulation Highly protein bound: >
90% Half-life: 12-36 hours (average 24 hours) Elimination:
dose-dependent; metabolized to inactive
metabolite and excreted in the urine
Monitoring parameters: Therapeutic plasma level: 10-20 mcg/mL
>20 mcg/mL: Far lateral nystagmus >30 mcg/mL: 45 lateral gaze
nystagmus and ataxia >40 mcg/mL: Decreased mentation >100
mcg/mL: Death
Katzung, BG, et al. Basic & Clinical Pharmacology, 11 th
Edition. Chapter 24, Antiseizure Drugs.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
11/28
Levetiracetam FDA indications: Adjunctive therapy in the
treatment of partial
onset, myoclonic, and/or primary generalized tonic-clonic
seizures
Mechanism of Action: binds selectively to the synaptic
vesicularprotein SV2A
function of this protein is not understood
modifies the synaptic release of glutamate and GABA.
PK profile:
Oral absorption: rapid and unaffected by food
Protein bound: < 10%
Half-life: 6-8 hours Elimination: 2/3 excreted unchanged in the
urine
Monitoring parameters:
- Renal adjustment is required
Katzung, BG, et al. Basic & Clinical Pharmacology, 11 th
Edition. Chapter 24, Antiseizure Drugs.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
12/28
Abbreviations and Terminologies
GCS = Glasgow coma score: trauma scoring; scoredbetween 3-15; 3
being the worst and 15 the best
GOS = Glasgow outcome score: score for the long-termfollow-up
after severe brain injuries; scored between 1-5; 5being the best
outcome and 1 the worst.
GOSE
DRS = disability rating score; scored 1-20;
1-3 (mild), 4-6 (moderate), 7-20(severe)
LEV = levetiracetam
PHT = phenytoin
Teasdale G., Jennett B., LANCET (ii) 81-83, 1974.Center for
outcome measurement in brain injury.
http://www.tbims.org/combi/drs/drsprop.html
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
13/28
Levetiracetam versus phenytoin forseizure prophylaxis
in severe traumatic brain injury
Design: Non-randomized, open label, historical control
Site: University of Pittsburgh Medical Center
Subjects:
Prospective cohort: 32 patients with severe traumatic brain
injury (TBI) 11/2006 12/2007 were admitted and
receivedlevetiracetam 500mg IV Q12H for the 1st 7 days
aftertraumatic injury
Historical cohort from severe TBI database: 41 patients withTBI
from 07/2005-06/2006 received phenytoin for 7 days aftertrauma.
Inclusion Diagnostic criteria:
GCS score of 3-8
Hospital standard protocol: not defined in the study
Only patients who received an EEG examination were includedin
the analysis.
Jones, K.E., et al. Neurosurg. Focus. Volume 25(4):E3, 2008
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
14/28
Results
Patient baseline characteristics: No significantdifferences
Patients with EEG examinations: 15/32 in the
levetiracetam cohort vs. 12/41 in the phenytoincohort
Levetiracetam cohort: total 19 EEG examinations
4 patients had2 EEG studies Phenytoin cohort: total 19 EEG
examinations
4 patients had 2 EEG studies
1 patient had 3 EEG studies
Jones, K.E., et al. Neurosurg. Focus. Volume 25(4):E3, 2008
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
15/28
Results
Jones, K.E., et al. Neurosurg. Focus. Volume 25(4):E3, 2008
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
16/28
Prospective, Randomized, single-Blinded Comparative Trial
ofIntravenous Levetiracetam Versus Phenytoin for Seizure
Prophylaxis
Design: prospective, single-center, randomized,
single-blindedcomparative trial
Site: University of Cincinnati hospital
Subjects:
Randomization occurred after admission up to 24 hours in the
NSICU at 2:1 ratio of LEV to PHT 52 patients was enrolled: 18
patients in the PHT arm and 34
patients in the LEV arm.
Inclusion diagnostic criteria:
Patients with severe TBI or subarachnoid hemorrhageadmitted to
the hospital < 24 hours prior to randomization
GCS score 3-8 or GCS motor score < 5 with abnormaladmission
CT scan showing intracranial pathology
Hemodynamically stable with sBP 90mmHg; at least 1reactive
pupil
17 years of age
Szaflarski JP, et al. Neurocrit Care. 2010 Apr;12(2):165-72.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
17/28
Exclusion criteria:
No venous access
Spinal cord injury
History of or CT confirmation of previous brain injury
Hemodynamically unstable
Suspected anoxic events; other peripheral trauma likely
resultliver failure
Age < 17 yo
CI treatment with LEV or PHT
Intervention:
PHT group: loading dose of fos-PHT 20mg/kg PE IV, max of2gm;
maintenance dose (5mg/kg/day, IV Q12H). PHT serum
levels check at days 2 and 6 after randomization and
doseadjustments to maintain therapeutic serum levels of
10-20mcg/mL.
LEV group: loading dose of 20mg/kg IV; maintenance dose(1gm, IV
Q12H). Dose was adjusted to max 3gm/day ifseizure occurred.
Szaflarski JP, et al. Neurocrit Care. 2010 Apr;12(2):165-72.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
18/28
Results Baseline characteristics: no differences
There were no differences in early seizure occurrencebetween the
PHT vs. LEV groups (3/18 vs. 5/34; P = 1.0)or death (4/18 vs.
14/34; P = 0.227)
There were no differences in PHT vs. LEV groups in GCS at7 days
(6 vs. 7; P = 0.58) and GOS at discharge (2 vs. 2;P = 0.33), 3
months (3 vs. 3; P = 0.61), and 6 months
(3 vs. 3; P = 0.89) LEV-treated patients experienced less
worsening
neurological status (P = 0.024) and GI problems (P =0.043)
Tendency toward lower incidence of anemia in PHT group (P
= 0.076) Surviving patients treated with LEV experienced
better
outcomes than surviving patients treated with PHTincluding lower
DRS at 3 and 6 months (P = 0.006 and P =0.037) and higher GOSE at 6
months (P = 0.016).
Szaflarski JP, et al. Neurocrit Care. 2010 Apr;12(2):165-72.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
19/28
Studies have 6 months follow-up period
In Jones, et al., levetiracetam isassociated with higher seizure
tendencyshowing on EEGs than phenytoin.
Both levetiracetam and phenytoin do nothave evidence in
prevention of lateepilepsy.
Comparisons in the studies were in IV
formulation for 7-day use. Efficacy of long-term use in PO
formulation has not been compared.
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
20/28
Safety and feasibility of switching from phenytoin
tolevetiracetam monotherapy for glioma-related seizure control
following craniotomy: a randomized phase II pilot study
Design: randomized phase II
Subjects:
Prior to randomization, patients were stratified into: noprior
craniotomy and history of one craniotomy
Within each stratification group, patients wererandomized in a
2:1 ratio to receive LEV or PHT
Inclusion diagnostic criteria:
Seizure history attributable to supratentorial glioma
PHT monotherapy for seizure prophylaxis
Planned craniotomy
Karnofosky performance scale of >70
> 18 yo
Lim, DA et al. J neurooncol 2009, 93:349-354
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
21/28
Exclusion Criteria Non-glioma cancer Pregnancy or
breast-feeding
Seizures unrelated to the suspected glioma Use AEDs other than
PHT >1 generalized seizure per day Prior interstitial
brachytherapy.
Intervention PHT: serum levels confirmed at therapeutic
range
at postoperative day1 (POD1); PHT dose adjustedas needed.
LEV: started LEV 1000mg PO BID with 24 hours ofsurgery and PHT
was tapered off as following:
100% of preoperative PHT regimen on POD0, 75%on POD1, 50% on
POD2, and PHT was discontinuedon POD3.
Primary end point: proportion of patients who wereseizure free 6
months after tumor resection
Lim, DA et al. J neurooncol 2009, 93:349-354
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
22/28
Results
29 patients enrolled: 20 in LEV vs. 9 in PHT
Baseline characteristics:
majority of patients were male
Female: 6 in LEV vs. 0 in PHT
Seizure type at presentation: Generalized: 8 in LEV vs. 3 in
PHT
Simple partial: 6 in LEV vs. 1 in PHT
Complex partial: 1 in LEV vs. 4 in PHT
Lim, DA et al. J neurooncol 2009, 93:349-354
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
23/28
Results
Lim, DA et al. J neurooncol 2009, 93:349-354
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
24/28
Phenytoin
ADRs: blood dyscrasias, dermatologic reactionsincluding toxic
epidermal necrolysis and SJS,hepatotoxcicity, bradycardia,
hypotension,cardiac arrhythmia, headache, insomnia,
tremor,paresthesia; idosyncratic (gingival hyperplasia,
hirsutism, coarse features)
DDIs with patients current medication: CYP4A3 substrates:
BusPirone, tamsulosin,
trazodone Fluconazole
Lexi-comp.com
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
25/28
Levetiracetam
ADRs: Somnolence, ataxia, headache, Lesscommon are complaints of
agitation or anxiety,emotion labile Idiosyncratic reactions are
rare.
Levetiracetam is not metabolized by CYP450
DDIs with patients current medication: None
Lexi-comp.com
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
26/28
Advantages of Levetiracetamover Phenytoin
Non-enzyme inducing AED
No serum level monitoring
Not induce drug fever or cutaneoushypersensitivity reactions
Less ADRs
Less DDIs
No food-drug interactions
IV:PO = 1:1
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
27/28
Back to Patient Case
Currently on Phenytoin PO 500mg/400mg at bedtimealternating
every other day
Phenytoin serum level:
3/8: 10.2 mcg/ml (corrected with albumin: 15 mcg/ml)
3/15: 10.3 mcg/ml (corrected with albumin: 14.7mcg/ml)
No seizure activity observed
Repeat MRI: not available
-
8/2/2019 Phenytoin Versus Levetiracetam for Seizure
Prophylaxis
28/28
Reference
Fauci, AS, et al. Harrisons principles of internal medicine,
17th edition (online version).Chapter 270, Section 4, Oncologic
Emergencies.http://www.accessmedicine.com.proxy.westernu.edu/content.aspx?aID=2880754.Accessed
03/22/2010
Gerstner ER, et al. CNS Hodgkin lymphoma. Blood. Sep
2008;112(5):1658-61.
Jones, K.E., et al. Levetiracetam versus phenytoin for seizure
prophylaxis in severetraumatic brain injury. Neurosurg. Focus.
Volume 25(4):E3, 2008
Katzung, BG, et al. Basic & Clinical Pharmacology, 11th
Edition. Chapter 24,
AntiseizureDrugs.http://www.accessmedicine.com.proxy.westernu.edu/content.aspx?aID=4512306.Accessed
03/23/2010.
Lexi-comp.com
Lim, DA et al. Safety and feasibility of switching from
phenytoin to levetiracetammonotherapy for glioma-related seizure
control following craniotomy: a randomizedphase II pilot study.
Journal neurooncol 2009, 93:349-354.
Szaflarski JP, et al. Prospective, Randomized, single-Blinded
Comparative Trial ofIntravenous Levetiracetam Versus Phenytoin for
Seizure Prophylaxis. Neurocrit care April2010 (2):165-72
Uptodate.com Zee CS, Neuroradiology: A Study Guide. McGraw Hill
1996:158-60.