Embed Size (px)
Citation preview

ucsovu
CAOG Papers www.AJOG.org
Phenazopyridine does not improve catheterdiscomfort following gynecologic surgeryCharles Anderson, MD; Maryann Chimhanda, MD; Jayme Sloan, MD; Suzanne Galloway, MD;James Sinacore, PhD; Linda Brubaker, MD, MS
OBJECTIVE: We sought to determine if phenazopyridine improves painin catheterized patients recovering from gynecologic surgery.
STUDY DESIGN: This trial randomized 240 adult women, who werendergoing gynecologic surgery and requiring an indwelling Foleyatheter, to placebo or phenazopyridine hydrocholoride. Group as-ignment was masked by instillation of orange dye in the Foley bagf both groups. The primary outcome was the mean postoperativeisual analog score (VAS). Secondary outcomes were pain medicinetilization and blinding efficacy.
RESULTS: In all, 219 patients received study medications (112
phenazopyridine and 107 placebo). There was no significant differ-Gynecol 2011;204:267.e1-3.
tnrdcsmF
dwelling Foley cathetedoi: 10.1016/j.ajog.2010.12.045
ence in demographics, procedure type, bladder VAS, overall VAS,and pain medication use. Only 25 of the 45 participants who re-sponded guessed their group assignment correctly, suggesting ad-equate blinding.
CONCLUSION: Postoperative VAS scores and pain medicine usage didnot change with using routine phenazopyridine following gynecologysurgery. Colored dye adequately masks visual side effects ofphenazopyridine.
Key words: bladder, blinding, catheter, gynecology, phenazopyridine
Cite this article as: Anderson C, Chimhanda M, Sloan J, et al. Phenazopyridine does not improve catheter discomfort following gynecologic surgery. Am J Obstet
Indwelling bladder catheters are com-monly used after pelvic surgery to
avoid bladder distension and bladder-related pain, and to allow urine outputassessment.1,2 Catheterization producesbladder irritation whose symptoms aresimilar to the symptoms of an overactivebladder caused by involuntary contrac-tions of the bladder mediated by musca-rinic receptors.3 This catheter-relatedbladder discomfort may exacerbatepostoperative pain because of the pres-ence of adjacent surgical wound.2
Techniques to relieve catheter-relateddiscomfort have not received much
From the Department of Obstetrics andGynecology, Loyola University MedicalCenter, Maywood, IL.
Presented at the 77th Annual Meeting of theCentral Association of Obstetricians andGynecologists, Las Vegas, NV, Oct. 27-30,2010. Recipient of the Young InvestigatorAward.
Received June 24, 2010; revised Dec. 6, 2010;accepted Dec. 23, 2010.
Reprints not available from the authors.
DISCLOSURE: Dr Brubaker received anhonorarium from Pfizer, New York, NY in 2009.
0002-9378/$36.00© 2011 Mosby, Inc. All rights reserved.
study. Tauzin-Fin et al4 demonstratedhe use of muscarinic receptor antago-ists in patients who had undergone aadical prostatectomy and reported a re-uction in postoperative bladder dis-omfort along with overall visual analogcore (VAS), and produced lower pain
edicine requirements. In contrast,rishman et al5 conducted a prospective
randomized double-blinded clinical trialcomparing a single dose of phenazopyri-dine to placebo prior to embryo transferin vitro fertilization in which the embryotransfer procedure requires a full blad-der. The mean VAS scores were not sig-nificantly different between the 2 groups.
As a commonly used clinical urinaryanalgesic, phenazopyridine hydrochlo-ride is an azo dye that exerts local anes-thetic or analgesic action on urinary tractmucosa through an unknown mecha-nism and causes a visible orange color tothe urine.6 Given the commonality ofcatheter usage associated with subjectivebladder discomfort in our patient popu-lation, we proposed a randomized clini-cal trial to determine whether routinephenazopyridine reduces catheter-re-lated bladder discomfort as well as painmedicine usage in women undergoinggynecologic surgery requiring an in-
r. We also sought
MARCH 2011 Americ
to prove that a novel blinding technique,colored dye, could be implemented toenhance masking of group assignment.
MATERIALS AND METHODSThis institutional review board–ap-proved, randomized trial was registeredat clinicaltrials.gov (NCT00771173)prior to the date enrollment com-menced. Participants were enrolled fromSeptember 2008 through December2009 at the 2 Loyola system hospitals:Loyola University Medical Center andLoyola at Gottlieb Hospital. Eligible can-didates were adult women undergoinggynecologic surgery who were expectedto require an indwelling catheter for aminimum of 12 postoperative hours andwho were expected to tolerate oral med-ication within 12 postoperative hours.Exclusion criteria included hypersensi-tivity to phenazopyridine products,known contraindications to phenazo-pyridine such as renal or hepatic failure,simultaneous suprapubic catheteriza-tion, anticipated inability to take oralmedication within 12 hours after sur-gery, and known pregnancy. Surgicalprocedure type was also recorded. Toconvey the mix of cases, we categorizedthe procedures broadly as laparoscopic,
abdominal, and vaginal and these werean Journal of Obstetrics & Gynecology 267.e1

CAOG Papers www.AJOG.org
expected to be equally distributed afterrandomization. Final eligibility of en-rollees was assessed prior to randomiza-tion to exclude patients with intraopera-tive urologic injury.
Enrolled participants who remainedeligible following surgery were random-ized (1:1) to receive either phenazopyri-dine 200 mg every 8 hours by mouth orplacebo while the Foley catheter was inplace or for 24 hours postoperatively,
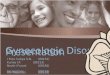
FIGUREConsort diagram displaying flow of
Received stud
(n = 2
No VAS recorded (n = 17)
Analyzed (n = 95)
Allocated to phenazopyridine (n = 112)
Women un
gynecologic sur
Randomized
Enrolled (
VAS, visual analog score.
Anderson. Phenazopyridine and catheter discomfort after gyn
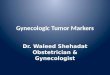
TABLE 1Demographic data and surgery typ
VariablePyridiumn � 112
Mean age, y 54...................................................................................................................
Caucasian 88 (79%)...................................................................................................................
African American 17 (15%)...................................................................................................................
Hispanic 3 (3%)...................................................................................................................
Other 4 (4%)...................................................................................................................
Abdominal surgery 93 (83%)...................................................................................................................
Vaginal surgery 22 (20%)...................................................................................................................
Laparoscopic surgery 36 (32%)...................................................................................................................
Anderson. Phenazopyridine and catheter discomfort after gyne
267.e2 American Journal of Obstetrics & Gynecolo
whichever came first. Group assign-ments were known to only the researchpharmacist who randomized subjectsonce an order for the study drug hadbeen placed by the investigator. Ran-domization was done using sequentiallynumbered opaque envelopes generatedby a randomized block permutation. Or-ange dye was instilled in the Foley bag ofboth groups in the operating suite priorto patient’s extubation to mask group as-
bjects through study
Not randomized (n = 18)
Didn’t receive
study drug (n = 21)
ication
Allocated to placebo (n = 107)
No VAS recorded (n = 15)
Analyzed (n = 92)
Not approached, ineligible or
declined (n = 470)
ing
n = 728)
240)
58)
ogic surgery. Am J Obstet Gynecol 2011.
cebo107
Overalln � 219
Test ofsignificance
54 .470..................................................................................................................
(80%) 174 (80%)..................................................................................................................
(14%) 32 (15%)..................................................................................................................
(0%) 3 (1.4%)..................................................................................................................
(6%) 10 (5%)..................................................................................................................
(83%) 182 (83%) .561..................................................................................................................
(20%) 43 (20%) .567..................................................................................................................
(38%) 77 (35%) .355..................................................................................................................
cologic surgery. Am J Obstet Gynecol 2011.
gy MARCH 2011
signment, as phenazopyridine is knownto color the urine dark orange. Surgicalpain was clinically treated by the pa-tient’s attending physician and residentswithout standardization.
The primary outcome was the meanVAS measurements during the postop-erative period. The scores were col-lected by nurses, residents, and mem-bers of the anesthesia team and wereextracted from the electronic medicalrecord. The sample size was deter-mined a priori to ensure 80% power todetect a clinically relevant difference of19% using the Pearson �2 test using a.05 alpha level. The reason we used19% as a clinically relevant differencewas based on the results of the priorseries by Tauzin-Fin et al4 and Frish-man et al.5 This was calculated to giveus adequate power for our anticipatedwithdraw of approximately 50 patientsand yielded us an even study number of240 patients. Randomized participantswho did not have at least 1 postopera-tive VAS score were not included in theanalysis.
Secondary outcomes were pain medi-cine utilization, both narcotic and nonnar-cotic, as well as assessments of blinding ef-ficacy. Pain medicine use was alsoquantified by the electronic medical re-cord. Blinding efficacy was assessed by ask-ing participants a series of standardizedquestions at the postoperative check. Inaddition to the primary VAS scores thatwere recorded by nursing staff per JointCommission on Accreditation of Health-care Organizations protocol, we also col-lected bladder-specific VAS scores thatwere collected by the house staff at thepostoperative check. At this time we alsoasked if they knew whether they were in themedication or placebo arm.
RESULTSIn all, 258 women were enrolled, 240were randomized, and 219 receivedstudy medications (112 phenazopyri-dine and 107 placebo). The Figure repre-sents the flow of subjects through thisstudy. Demographic data and surgerytype are presented in Table 1. The groupswere similar in age and race; most partic-
su
y med
19)
dergo
gery (
(n =
n = 2
ecol
e
Plan �
53.........
86.........
15.........
0.........
6.........
89.........
21.........
41.........
ipants (80%) were Caucasian, with a

s
gyne
www.AJOG.org CAOG Papers
mean age of 55 years. The groups werealso similar with respect to surgical type:abdominal procedures (83%), laparo-scopic procedures (35%), and vaginalsurgery (20%). For analytical purposes,patients who underwent a laparoscopicprocedure were categorized to both alaparoscopic group as well as the abdom-inal group. Our heterogeneous studypopulation consisted of general gyneco-logic, urologic, and oncologic patients.
Foley duration and VAS data are pre-sented in Table 2. In all, 188 patients(86%) had at least 1 VAS score recorded.The phenazopyridine group had 346VAS scores available compared to 301VAS scores in the control group. Themean Foley catheter duration was simi-lar between groups (17.8 hours, SD 6.0hours, vs 18.4 hours, SD 4.8 hours,P � .875). Catheter-specific bladder VASscores were obtained in 151 patients with86% having a VAS of �2. There was noignificant difference in bladder VAS
TABLE 2Foley duration and visual analog sc
VariablePyridium groupn � 112
Mean Foley duration, h 18 (SD � 6)...................................................................................................................
No. of VAS scores 346...................................................................................................................
Bladder VAS, mean 0.95...................................................................................................................
Overall VAS, mean 2.0...................................................................................................................
VAS, visual analog score.
Anderson. Phenazopyridine and catheter discomfort after
TABLE 3Pain medication utilization
Specific painmedication
Phenazopyridinevs placebo, testof significance
Morphine U .792...........................................................................................................
Norco 5 mg .874...........................................................................................................
Norco 10 mg .925...........................................................................................................
Darvocet N-100 .987...........................................................................................................
Tylenol no. 3 1.00...........................................................................................................
Nonnarcotic IV .262...........................................................................................................
Nonnarcotic PO .439...........................................................................................................
IV, intravenous; PO, by mouth.
Anderson. Phenazopyridine and catheter discomfort
after gynecologic surgery. Am J Obstet Gynecol 2011.means (.95, SD 1.8, vs .97, SD 1.7, P �.745). Approximately 1 in 5 participantsreported that their highest VAS score was0 (22%). Although the mean VAS wasslightly lower in the phenazopyridine (2.0)than in the placebo (2.4) group, this differ-ence was neither statistically nor clinicallysignificant (P � .820).
Pain medication utilization (narcoticand nonnarcotic) did not differ by group(P � .262-1.00) and is displayed in Table 3.Of the 140 subjects who were asked if theyknew their group assignment, 62% statedthey did not know. Among 45 patientswho believed they knew their group as-signed, only 25 guessed correctly (56%),suggesting that colored dye is an adequateblinding for the visual side effects of thestudy drug (kappa � .14, P � .231).
COMMENTOur finding that postoperative mean VASscores (both overall and bladder-specific)did not improve with the addition ofphenazopyridine hydrochloride followinggynecology surgery could be due to overalllow VAS scores secondary to excellentoverall surgical pain management, as evi-denced by the low VAS scores. Althoughthese data should not be used to withholdclinical treatment of catheter-associatedpain in any individual patient, we do notrecommend administering phenazopyri-dine on a routine basis. A subset of patientsmay benefit from bladder analgesics andphenazopyridine should be considered inpatients with acute bladder discomfortpostoperatively.
This trial also demonstrated the feasi-bility of blinding participants to the vi-sual side effect of phenazopyridine using
e data
cebo group107
Overalln � 219
Test ofsignificance
(SD � 5) 18 (SD � 5) .875..................................................................................................................
647..................................................................................................................
.97 0.96 .745..................................................................................................................
.4 2.0 .820..................................................................................................................
cologic surgery. Am J Obstet Gynecol 2011.
colored dye in the urinary bag. We dem-
MARCH 2011 Americ
onstrated the effectiveness of a novel andtrial-specific blinding technique thatmay be applicable to future trials.
One limitation of our study was incon-sistent collection of our primary outcomedata. Nursing staff and house staff failed tocollect VAS scores consistently as illus-trated in our consort diagram. This wasunexpected given the fact that our institu-tion considers the VAS score as the fifthvital sign and is actually a tool used forquality assurance and patient satisfaction.This led to a high number of participantsnot having any primary outcome data andrequired recruitment of 40 additional par-ticipants to ensure adequate power. An-other potential criticism of our study wasour methodology of categorizing surgicalcase types. Our main research questionwas the utility of phenazopyridine, ratherthan stratification by specific gynecologiccase. We categorized the proceduresbroadly as laparoscopic, abdominal, andvaginal and as expected with our random-ized design, these procedure “categories”were essentially equal between both studygroups. We did not test any secondary hy-pothesis regarding specific gynecologicprocedures or route of surgery and we arenot inclined to do so based on the results ofour primary study.
The strengths of this trial include theprospective design with group masking.The findings of this study can be general-ized to similar populations of gynecologicsurgical patients, given the distribution ofprocedure type and demographics. f
REFERENCES1. Jain P, Parada JP, David A. Overuse of theindwelling urinary tract catheter in hospitalizedmedical patients. Arch Intern Med 1995;155:1425.2. McMahon SB, Dmitrieva N, Koltzenburg M.Visceral pain. Br J Anaesth 1995;75:132-44.3. Andersson KE. Advances in the pharmaco-logical control of the bladder. Exp Physiol1999;14:195-213.4. Tauzin-Fin P, Sesay M, Svartz L, Krol-Houdek M, Maurette P. Sublingual oxybutyninreduces postoperative pain related to indwellingbladder catheter after radical retropubic prosta-tectomy. Br J Anaesth 2007;99:572-5.5. Frishman GN, Allsworth JE, Gannon JB,Wright KP. Use of phenazopyridine for reducingdiscomfort during embryo transfer. Fertil Steril2007;87:1010-4.6. UpToDate Online. Available at: http://
or
Plan �
18.........
301.........
0.........
2.........
www.utdol.com. Accessed Jan. 1, 2007.
an Journal of Obstetrics & Gynecology 267.e3