Embed Size (px)
Citation preview
UNIVERSITY OF AGRICULTURAL SCIENCES AND VETERINARY MEDICINE
CLUJ-NAPOCA
DOCTORAL SCHOOL
VETERINARY MEDICINE FACULTY
COSMIN S. MUREŞAN
PHD THESIS SUMMARY
HEMODYNAMICS IN RESUSCITATED CARDIAC ARREST WITH
NEUROPROTECTION THROUGH THERAPEUTIC HYPOTHERMIA
AND MEMANTINE IN SWINE
SCIENTIFICAL ADVISOR
Prof. univ. Dr. LIVIU IOAN OANA
CLUJ-NAPOCA
2014

Table of contents
Keywords ...................................................................................................................... iii
1. Research motivation ..................................................................................................... iii
2. Thesis originality .......................................................................................................... iii
3. Research objectives ...................................................................................................... iii
4. Materials and method ................................................................................................... iv
5. Results and discussions ................................................................................................ vii
6. Conclusions and recommendations .............................................................................. xiv
iii
KEYWORDS: hemodynamic parameters, hemodynamic monitoring, cardiopulmonary arrest,
resuscitation, neuroprotection, therapeutic hypothermia, memantine.
1. RESEARCH MOTIVATION
Hemodynamic monitoring in cardiac arrest and resuscitation under neuroprotection is a
topical issue in emergency medicine and intensive care, which tries to bring more light on the
elucidation of pathophysiological mechanisms of cardiopulmonary arrest and consecutive
neuronal injury, on identification and update therapies with neuroprotective effects post
cardiopulmonary resuscitation, and on hemodynamic monitoring optimization and identification
of hemodynamic reference parameters in resuscitation and early goal-directed therapy.
In human medicine, post-resuscitation brain injury remains a professional challenge
requiring huge financial and human resources, and neuroprotective therapies devised or tested in
various preclinical studies and animal models still generate disappointing results. Controlled
hypothermia initiated post-resuscitation, although it has proven its neuroprotective effect in
comatose survivors of ventricular fibrillation, still raises some reticence about its usefulness on a
larger scale. In this context, the identification of new neuroprotective therapies or
complementary to hypothermia, once proven efficient, can be used in the usual clinical practice
(Gillies et al., 2010).
In veterinary medicine, the number of conclusive studies aimed at resuscitation, cerebral
ischemia and reperfusion neuronal injury, as well as hemodynamic monitoring in resuscitation
and post-resuscitation syndrome, is still very small. In addition, some of these studies are
performed on patients with often diversified pathology, others are experimental studies in
healthy patients, with hemodynamic parameters being chosen according to the addressed species,
the availability of monitoring equipment and preferences of the clinical staff involved, lacking an
overall hemodynamic monitoring which enables the identification of reference
methods/parameters and unequivocal demonstration of any correlation/non-correlations between
relevant parameters.
Thus it is necessary to further investigate the implementation of an updated strategy for
advanced hemodynamic monitoring during cardiopulmonary arrest and ischemia/reperfusion
injury in animals with experimental cardiac arrest, based on the findings of prospective clinical
trials.
2. THESIS ORIGINALITY
This study contributes to a better understanding of the evolution of hemodynamic
parameters during cardiopulmonary arrest, resuscitation and immediate post-resuscitation period,
potential correlations between them, the patient's response to resuscitation and influence of
neuroprotective therapy on the studied hemodynamic variables.
We believe that the findings in our study are significant, considering the following: the
study is based on cardiopulmonary arrest consecutive to induced ventricular fibrillation; there are
no differences between groups regarding CPR protocol or resuscitation medication; an essential
component of the study is the neuroprotection protocol (hypothermia and memantine); different
approach of categories of evaluated hemodynamic parameters; hemodynamic assessment from
post-ROSC to 120 minutes, etc.
3. RESEARCH OBJECTIVES
This paper aims to assess hemodynamic parameters during cardiac arrest, resuscitation
with neuroprotection, and during the return to spontaneous circulation, based on an experimental

iv
protocol of cardiac arrest by induction of ventricular fibrillation using an electric current of 50
Hz.
The study has the following objectives: to assess the dynamics of monitored
hemodynamic parameters; to identify potential correlations between monitored hemodynamic
parameters; to evaluate the influence of neuroprotection medication on monitored parameters.
To accomplish the objectives we monitored hemodynamic parameters using the
following classification (Edwards, 2002; Galli et al., 2000; Lopez-Herce et al., 2011a, 2011b;
LiDCO, 2003):
Global hemodynamic parameters – heart rate (HR), mean arterial pressure (MAP), central
venous pressure (CVP), pulmonary capillary wedge pressure (PWPC), cardiac output
(CO), stroke volume (SV), stroke volume variation (SVV), systemic vascular resistance
(SVR).
Oxygenation status parameters – partial pressure of oxygen (PO2) (arterial, venous and
jugular bulb blood), oxygen delivery (DO2), hematocrit (HCT – arterial, venous and
jugular bulb blood).
Acid-base status parameters – pH, base excess (BE(B)), bicarbonate (HCO3) and the
partial pressure of carbon dioxide (PCO2) – in arterial, venous and jugular bulb blood,
and the end tidal carbon dioxide (EtCO2).
Metabolic and tissue perfusion status parameters – glucose (GLU), serum potassium
(K+), lactatemia (LAC) and ionized calcium (Ca++) – in arterial, venous and jugular bulb
blood.
Hemodynamic parameters were assessed and recorded during four consecutive periods:
the period of stability (basal), during ventricular fibrillation (VF), during resuscitation (CPR) and
post resuscitation period (post-ROSC).
4. MATERIALS AND METHODS
Biological materials. The animals studied were the 25 pigs (Landrace/Large-White),
male and female, with an average weight of 65 ± 5 kg, all from the same breeder, a pig farm
from Cluj county. The pigs were brought to FMV Cluj-Napoca three days before the experiment
and hospitalized in separate boxes, with food and water regime ad libitum (fed a commercial diet
similar to that fed in the farm), and a normal lighting regimen (compliance of the day and night
cycle).
Equipment. Draeger Infinity Delta multiparameter monitor and Draeger Evita 1
ventilator (Dragerwerk AG Lubeck, Germany); Vigileo monitor, used with FloTrac sensor
(Edwards Life Sciences, USA); Primedic Defi Monitor XD1 defibrillator (Metrax GmbH,
Rottweil, Germany); Gem Premier 3000 blood gas and electrolyte analyzer (Instrumentation
Laboratory Company, Lexington, MA, USA); Infusomat B Braun FM and Injectomat B Braun
Compact S (B Braun Melsungen AG, Melsungen, Germany); Nikon D40, with a 18-55 mm
objective (Japan).
Working method. The experimental protocol was reviewed and approved for the project
PN-II/09.10.2007, „The development through interdisciplinary research of a new drug therapy
meant to ensure neuroprotection in cerebral ischemia (NEUROPROTER)” by the Committee on
Bioethics of UMF Iuliu Haţieganu Cluj-Napoca, and was in accordance with the European
legislation and also with the international guidelines on animal welfare involved in experimental
procedures, and is based on similar protocols found in several studies (Brücken et al., 2010;
Jeung et al., 2011; Wu et al., 2008; Koudouna et al., 2007; Liao et al., 2010; Lopez-Herce et al.,
2011a; 2011b; Schratter et al., 2010; Schwarzl et al., 2011; Xanthos et al., 2007a; 2007b; 2010;
Yannopoulos et al., 2011). Before being studied, the animals were diagnosed as clinically

v
healthy on a prior clinical consultation. 12 hours before the experiment they were subjected to
fasting, fluid administration remaining unchanged.
Anesthesia protocol. The anesthetic protocol used consisted in the administration of
atropine (0.04 mg/kg IM) and azaperone (4 mg kg IM) (premedication); propofol (3 mg/kg) i.v.
bolus (induction of anesthesia); sufentanil (0.2-0.3 mcg/kg IV every 20-30 minutes), Tracrium
(0.6 ml/kg IV every 30 minutes) and propofol (8-10 mg/kg/h) (maintenance). Ventilation was
maintained in a controlled manner with TV of 12-15 ml/kg I/E ratio of 2.1, 21% FiO2,
respiratory rate being adjusted to maintain EtCO2 between 30-40 mmHg and PaCO2 between 35-
45 mmHg.
Auxiliary protocol. Fluid therapy consisted of Hartmann's solution at a dose of 30 ml/kg
IV during the first hour, then 10 ml/kg/h, with interruption during ventricular fibrillation. 15 min.
before inducing the cardiac arrest all animals received heparin in order to prevent the potential
risk of thromboembolism.
Catheter placement. The marginal ear vein was catheterized with a 20G venous
catheter. The right carotid artery was surgically isolated and catheterized with a 20G arterial
catheter for continuous assessment of blood pressure, cardiac output and cardiac output derived
parameters. The pulmonary artery was catheterized with a 7F Swan-Ganz catheter, introduced
through the right jugular vein, right atrium, right ventricle, pulmonary artery and finally the
pulmonary capillary, the catheter position being monitored by visualizing the characteristic
waves on the monitor screen. For assessing central venous pressure, a central venous catheter
was inserted into the right jugular vein. The right internal jugular vein was also catheterized as
close as possible to the jugular bulb with a 22G intravenous catheter for blood gas and
electrolyte sampling. Bladder catheterization was performed using a urinary probe.
Monitoring of hemodynamic parameters. The following hemodynamic parameters
were monitored: HR, MAP, CVP, PWPC, CO, SV, SVV, SVR, PO2, DO2, HCT, pH, BE(B),
HCO3-, PCO2, EtCO2, GLU, K+, LAC and Ca++. Additionally, for quality purposes of the
experimental protocol, the following parameters were also monitored until patient extubation:
ECG in DII derivation, SpO2 and body temperature. After completing implementation of
catheters and monitoring, each animal was allowed to stabilize for 20 minutes before recording
baseline hemodynamic variables.
Registration of hemodynamic parameters was performed according to the following
protocol: baseline, 3 minutes from resuscitation; 5, 15, 30, 60 minutes and 120 minutes after
ROSC. The order of registration of these parameters was not random. For every measurement
set, blood sampling was performed after recording parameters on the screens of both monitors.
Blood samples for the analysis of blood gases, electrolytes and lactate were obtained at the same
time from the carotid artery, pulmonary artery and jugular bulb, according to the same protocol
applied for the rest of the hemodynamic variables. Analysis of blood gases, electrolytes, glucose
and lactate was performed immediately after blood sampling.
Methodology for the induction of cardiac arrest. Cardiac arrest was achieved by
induction of ventricular fibrillation (VF) by applying an alternating current of 40-60 V at a
frequency of 50 Hz, by means of two subcutaneous electrodes. The duration of cardiac arrest was
8 minutes, while mechanical ventilation and fluid therapy were stopped and the animals were left
without any treatment. The presence of ventricular fibrillation was confirmed by visualization of
the ECG characteristic waves and a significant drop in blood pressure.
Resuscitation protocol. After eight minutes of VF, resuscitation maneuvers were
initiated according to the human medicine ALS protocol. The CPCR protocol consisted of
manual external cardiac massage (standard) – chest compressions – at a rate of 100 per minute,
with the length of compression being equal to full relaxation, and the depth of compressions on
the anterior-posterior diameter being 25% of the height of the thorax, and controlled ventilation,
with a frequency of seven breaths per minute, 100% FiO2, and 30/2 ratio of chest

vi
compressions/breaths. After one minute of CPR, an IV bolus of vasopressin (0.5 IU/kg) was
administered. After five minutes of CPCR the patient was defibrillated by applying an electric
biphasic shock of 150 J. The success of resuscitation, ROSC (restoration of spontaneous
circulation), was considered a restoration of heart rate with an invasive SBP greater than 50-60
mmHg for more than 10 consecutive minutes. If ROSC was not achieved after the first shock, we
continued the CPCR with a minute of external cardiac massage and two electric shocks 150 J,
followed by another 2 minutes of ECM, a bolus of 30 mcg of epinephrine (0.02 mg/ kg) and after
another minute of ECM, two consecutive shocks of 200 J were applied. The absence of ROSC
after these shocks defines inefficiency of resuscitation. The resuscitation protocol was stopped
when ROSC was achieved or after 20 minutes of ineffective resuscitation. After restoring ROSC,
ventilation (i.e. maintaining PaCO2 and EtCO2 values before VF) fluid therapy and
hemodynamic monitoring were restarted. In addition, FiO2 was gradually decreased, so that after
60 minutes after ROSC, this parameter was reduced to 30%, and later maintained until patient
extubation. If SBP was less than 70 mmHg after ROSC, inotropic support with dobutamine was
initiated. At the end of the monitoring period extubation was performed. Before being transferred
to the box, each animal was observed for 20 minutes under SpO2 monitoring to ensure adequate
spontaneous breathing.
Neuroprotection protocol. Neuroprotection protocol was achieved through two distinct
methods, therapeutic hypothermia and administration of memantine.
Therapeutic hypothermia. Therapeutic hypothermia (32-34°C) (mild hypothermia), a
classical method in neuroprotection, was induced and maintained by a combination of two
methods, the endovascular method and the surface cooling method. The internal endovascular
method – "endovascular cooling" – was carried out by rapid intravenous bolus administration
(15-30 ml/kg) of cold crystalloid solution (Hartmann's solution at 4°C). The external method –
"surface cooling" – was carried out by placing cold compresses (wet towels) and polythene ice
packs on the ventral and lateral sides of the neck, thorax and abdomen (Gillies et al., 2010). The
duration of therapeutic hypothermia was 12 hours, and it was established in a single lot, starting
in the 1st minute post-ROSC. Throughout its length, the internal body temperature was measured
continuously at esophagus level (the lower third). Prevention of shivering was performed by
anesthetic management, neuromuscular blocking being added as needed. Finally, the reheating
procedure has been carried out by passive methods using hot blankets, and the room temperature
was adjusted to 22-23°C.
Administration of memantine. Two lots received memantine for neuroprotection – 5
mg/kg and 10 mg/kg i.v. in the 1st minute post-ROSC (in the Swan-Ganz introducer catheter).
Studied lots
Lot I (5 pigs) – anesthesia without cardiac arrest, without CPCR, without
neuroprotection;
Lot II (5 pigs) – anesthesia, cardiac arrest, CPCR, without neuroprotection;
Lot III (5 pigs) – anesthesia, cardiac arrest, CPCR, memantine 10 mg/kg;
Lot IV (5 pigs) – anesthesia, cardiac arrest, CPCR, therapeutic hypothermia;
Lot V (5 pigs) – anesthesia, cardiac arrest, CPCR, memantine 5 mg/kg.
After complete registration of the studied hemodynamic variables, animals that achieved
ROSC were kept alive for three days, during which they were examined neurologically at 24, 48
and 72 hours. Daily therapeutic protocol during this period consisted of antibiotic and analgesic/
anti-inflammatory drugs; diet and fluid intake remained unchanged. At the end of the
experiment, the animals were euthanized and necropsied, with sampling for histopathologic
examination.
Statistical analysis of the results. Recorded hemodynamic variables are presented as
mean ± SD. As we found in the literature only separate assessments of the dynamics and
potential correlations of blood variables (arterial, central venous, jugular bulb), in our study we

vii
preferred the combined appraisal, and therefore we introduced these hemodynamic variables in
the statistical analysis as an arithmetic mean.
Statistical interpretation of the test results was based on ANOVA (Analysis of Variance
One-way) and Tuckey Kramer for the dynamic evolution and the comparative evolution of
monitored hemodynamic parameters. A p value of <0.001 indicates highly significant differences
(marked with ***); a p value of <0.01 indicates significant differences (marked with **); a p
value of <0.05 was indicative for significant differences (marked with *); a p value of ≥0.05 was
indicative for differences statistically insignificant (marked with ns).
To assess the relationship between recorded hemodynamic variables we used Pearson's
correlation (Pearson Product Moment Correlation Coefficient (r) – correlation coefficient). A
correlation coefficient equal to 0 was an indicator for the absence of linear relationship, while a
correlation coefficient equal to 1 (±) has been an indicator for a perfect linear relationship
(positive/ negative). Correlation coefficient values between 0 and 0.3 (±) are indicators for a low
linear relationship (positive/negative); r values between 0.3 and 0.7 (±) were indicators for
moderate linear relationship (positive/negative) (significant error of prediction); r values between
0.7 and 0.9 (±) were indicators for a strong linear relationship (positive/negative) (moderate error
of prediction); correlation coefficient values between 0.9 and 1.0 (±) were indicators for a very
strong linear relationship (positive/negative) (with good accuracy of prediction) (Marion, 2004;
Stockburger, 1996; Dean et Illowsky, 2012). Additionally, for a correct interpretation of the
correlation coefficient we determined the linear regression between the same hemodynamic
variables by calculating the coefficient of determination (R2) (Brown, 2003; Dean et Illowsky,
2012; Roberts, 2014).
5. RESULTS AND DISCUSSIONS
DYNAMIC EVOLUTION OF HEMODYNAMIC PARAMETERS
Global hemodynamic parameters. In the control group, heart rate, blood pressure,
central venous pressure and pulmonary capillary wedge pressure remained relatively constant
throughout the experiment. Cardiac output and stroke volume were constant around 6 L/min. and
65 mL/beat. In addition, stroke volume variation had a similar pattern. In the resuscitated groups,
compared to basal period, heart rate dropped to 0 during the ventricular fibrillation period (Fig.
1), and simultaneously extreme hypotension was noticed (10% of basal value). During
resuscitation, heart rate increased sharply, as determined practically by cardiac massage, with
concomitant arterial hypotension (maximum 50% of basal value), even if resuscitation was
instituted accordingly. During the return of spontaneous circulation we recorded tachycardia,
heart rate values being the highest in the first 30 minutes, after which they had a tendency to
decrease and normalize. After 5 minutes of ROSC we observed a peak of hypertension, with a
subsequent trend of normalization, and at the end of the experiment the mean arterial pressure
was slightly increased compared to baseline. Central venous pressure and pulmonary capillary
wedge pressure were increased within 30 min after ROSC, after which there was a tendency to
normalization, baseline values being the smallest recorded. Due to technical reasons, CVP was
not recorded during ventricular fibrillation and CPR. The highest cardiac output was recorded in
resuscitated lots immediately after return to spontaneous circulation (5-15 min); at the end of the
experiment CO was lower than baseline; post-ROSC stroke volume variation had a downward
trend towards the end of the monitoring period, the values during ROSC 120 being superior to
baseline. However, during ventricular fibrillation and resuscitation periods, values generated by
the Vigileo monitor for CO, SV and SVV were identical with basal values, since the monitor
sensor could not detect an interpretable pulse wave, and we therefore believe that they do not
reflect the clinical reality of those moments, and were erroneously overestimated. Systemic

viii
vascular resistance was decreased during baseline and had a tendency to increase towards 120
min. post-ROSC; its values were not influenced by resuscitation.
Acid-base status parameters. In the control group, acid-base status parameters had a
linear trend which was constant throughout the experimental period - the base excess between
8.1 mmol/L, SD = 1.89 and 9.35 mmol/L, SD = 3.11; end-tidal carbon dioxide between 24.33
mmHg, SD = 1.08 and 29 mmHg, SD = 1.41; blood bicarbonate concentration between 31.45
mmol/L (SD = 1.7) and 33.74 mmol/L (SD = 3.87); partial pressure of carbon dioxide in the
range of 35.77 mmHg (SD = 3.16) and 44 mmHg (SD = 14.07); blood pH in the range of 7.48
(SD = 0.07) and 7.53 (SD = 0.02, 0.03, 0.005). In the lots where we induced ventricular
fibrillation, as compared to the basal values base excess and blood bicarbonate concentrations
were normal, but they decreased during CPR and return to spontaneous circulation, suggesting a
base deficit (metabolic compensation). Base excess had a negative peak 15 minutes after ROSC
(-6.1, SD = 0.73 and -10.32, SD = 4.1), and, starting 30 minutes post-ROSC, HCO3- and BE(B)
had recorded an upward trend in all resuscitated lots; as a whole, the recorded values for these
two parameters were lower than baseline (statistically insignificant) at the end of monitoring
(Fig. 2). End-tidal carbon dioxide decreased sharply up to 0 during ventricular fibrillation, then
rose sharply during resuscitation, reaching values of nearly 50% of baseline values, and
continued to grow during ROSC 5, when we registered values approximately equal to baseline.
Maximum values were found 15 minutes after return to spontaneous circulation, subsequently
we recorded a downward slope, where values recorded at the end of the monitoring period were
being almost similar to baseline. Basically EtCO2 showed an inversely proportional relationship
to BE(B) 15 minutes after return to spontaneous circulation. Partial pressure of carbon dioxide
showed almost identical values at the beginning and end of monitoring in resuscitated groups,
being increased in 15 minutes after ROSC. Basically PCO2 and EtCO2 were maximally increased
at the same time, 15 minutes after ROSC. Compared to baseline, the blood pH in resuscitated
lots decreased until 15 minutes after return to spontaneous circulation, at which point metabolic
acidosis was maximal. Subsequently it has registered an improvement, baseline pH and final pH
being quite similar.
Oxygenation status parameters. In the control group, oxygenation status parameters
had a linear trend throughout the experimental period. Oxygen delivery was between 661
mL/min (SD = 18.7) and 843 mL/min (SD = 180.71); partial pressure of oxygen in the blood
between 109.44 and 256.33 mmHg and hematocrit – between 25.44% (SD = 2.13) and 27.33%
(SD = 3.52). In resuscitated groups, during VF, these parameters were not registered. During
CPR, compared to baseline, PO2 and HCT increased. DO2 was maximally increased up to 5-15
minutes after return to spontaneous circulation, after which the declining trend was gradual-
minimum values were found at the end of the monitoring period (Fig. 3). Generally, the PO2
registered an increasing trend from baseline up to 60 minutes post-ROSC (hyperoxia), followed
by a sharp decline until the end of the monitoring period, ROSC 120 values did remain higher
than baseline. DO2 and PO2 were directly influenced by FiO2 evolution during resuscitation,
respectively 100% during CPR and then gradually reduced to 30% at 60 minutes. HCT in
resuscitated lots increased from baseline until 5 minutes post-ROSC, followed by a slow decline
within the next 60 minutes, the final values (ROSC 120) remaining similar to baseline.
Metabolism and tissue perfusion status parameters. In the control group, the
metabolic and tissue perfusion status markers remained constant throughout the experiment.
Glycaemia – between 5.22 mmol/L (SD = 0.92) and 6.05 mmol/L (SD = 1.84); blood lactate –
from 1.92 mmol/L (SD = 0.43) to 3.15 mmol/L (SD = 0.67); blood potassium – between 3.67
mmol/L (SD = 0.05) and 3.83 mmol/L (SD = 0.16); ionized calcium – between 1.37 mmol/L and
1.39 mmol/L during baseline. In resuscitated lots, compared to baseline, glycaemia and
lactatemia increased during CPR, and potassium levels reached a maximum peak. Post-ROSC,
blood glucose peaked at 5 minutes, blood lactate only after 5-15 minutes (Fig. 4), while

ix
potassium levels returned to baseline 15 minutes after return to spontaneous circulation. Serum
calcium was minimal 60 minutes after ROSC, but the evolution of this parameter was still
modest compared with other metabolic and tissue perfusion parameters.
CORRELATIONS BETWEEN HEMODYNAMIC PARAMETERS
Correlations between the global hemodynamic parameters. In the five studied lots,
few correlations were observed between monitored global hemodynamic parameters. Thus, we
identified a strong positive correlation between heart rate and mean arterial pressure in terms of
hemodynamic stability, but the correlation was inconstant in terms of hemodynamic instability.
In groups resuscitated under neuroprotection, we identified a strong positive correlation between
heart rate and cardiac output. Only in the lots resuscitated with memantine we have identified a
strong negative correlation between systemic vascular resistance and two other variables – heart
rate and cardiac output. In the group with hypothermia, we have identified a strong positive
correlation between cardiac output and mean arterial pressure, which remained very strong in the
group with memantine 10 mg/ kg, but not in the other groups. Cardiac output was not correlated
with global pressure parameters, such as central venous pressure and pulmonary capillary wedge
pressure.
Correlations between acid-base status parameters. Among the acid-base parameters
there are few strong correlations. In all groups we identified a strong positive correlation
between blood base excess and bicarbonate, both in terms of hemodynamic stability and
instability. We observed that during hemodynamic stability conditions, there was a strong
positive correlation between the partial pressure of carbon dioxide and base excess (blood), and
between partial pressure of carbon dioxide and blood bicarbonate, but the correlation becomes
strongly negative in all groups resuscitated under neuroprotection. Inconstantly, in the
hypothermic group and the group with memantine 10 mg/kg we found a strong positive
correlation between pH and base excess, and respectively bicarbonate. Only in the lots treated
with memantine, and in no other lots, we identified a strong positive correlation between the
partial pressure of carbon dioxide in the blood and the end-tidal carbon dioxide.
Correlations between oxygenation status parameters. Within the parameters of
oxygenation status there are no strong correlations. Inconstantly, in the hypothermic group and
the group with memantine 10 mg/kg we found a strong positive correlation between oxygen
delivery and hematocrit.
Correlations between metabolism and tissue perfusion status parameters. In the
metabolism and tissue perfusion status parameters there are little correlations. In all resuscitated
lots (with/without neuroprotection) we identified a strong positive correlation between blood
glucose and lactate.
Correlations between global hemodynamic parameters, acid-base status
parameters, oxygenation status parameters and metabolic and tissue perfusion status
parameters. Overall, taking into account all hemodynamic parameters in all lots studied, we
identified potential correlations which describes from a pathophysiological point of view
cardiopulmonary arrest, resuscitation period and the return to spontaneous circulation.
Between global hemodynamic variables and oxygenation status variables, we found a
strong positive correlation only between cardiac output and oxygen delivery in terms of
hemodynamic stability, which becomes very strong in the groups resuscitated under
neuroprotection.
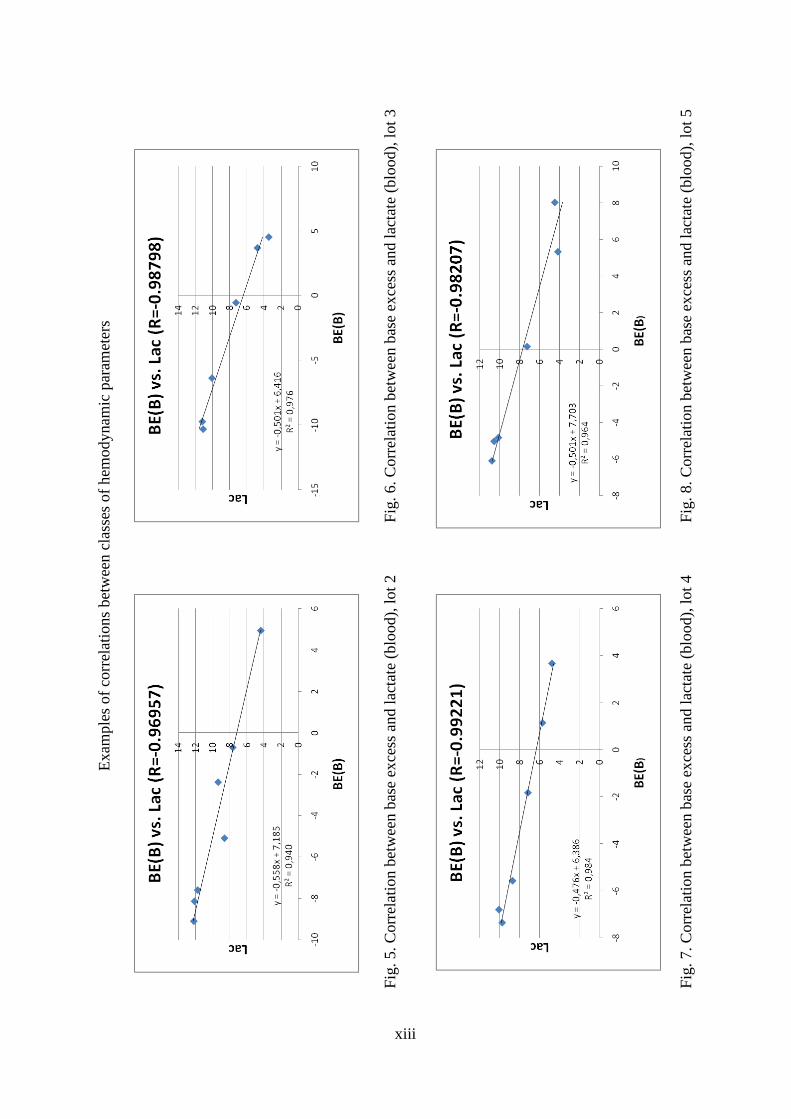
In all 4 resuscitated lots, we noticed a strong positive correlation between heart rate and
glycaemia, a strong negative correlation between blood base excess and blood lactate (Fig. 5, 6,
7, 8), and a very strong negative correlation between hydrogen ion concentration and blood
lactate. Additionally, in terms of hemodynamic stability, we revealed a strong negative
x
correlation between heart rate and blood lactate, which becomes very strong positive correlation
in resuscitated lots, except the hypothermic lot where this relationship was not maintained. We
identified a strong positive correlation between base excess and glycaemia, and between blood
bicarbonate and glycaemia in the lot without cardiac arrest and without neuroprotection (during
hemodynamic stability), but this correlation becomes reversed (negative) in all resuscitated lots.
Comparing hemodynamic variables in resuscitated lots, we found a strong negative
correlation between heart rate and base excess (blood), which becomes very strong in the groups
resuscitated under memantine. This correlation is not maintained in the group with hypothermia.
Also in resuscitated lots we identified a strong positive correlation between glucose and oxygen
delivery, between blood lactate and oxygen delivery, and a very strong correlation between heart
rate and oxygen delivery with one exception – the lot with therapeutic hypothermia. Similarly,
we found a strong negative correlation between blood base excess and oxygen delivery, between
bicarbonate ion concentration and oxygen delivery, and a very strong correlation between blood
bicarbonate concentration and heart rate in all resuscitated lots, but with the same exception – the
lot with hypothermia.
In lots resuscitated under neuroprotection, we have identified a strong positive correlation
only between cardiac output and glycaemia, and between the partial pressure of carbon dioxide
and blood lactate.
Only in the lots with memantine we noticed a strong positive correlation between heart
rate and end-tidal carbon dioxide, between cardiac output and blood lactate, and between oxygen
delivery and end-tidal carbon dioxide, but a strong negative correlation between cardiac output
and base excess and between cardiac output and blood bicarbonate concentration.
Through the fact that we found only a few correlations between monitored hemodynamic
parameters, our study confirms on the one hand the possibility that neuroprotective (hypothermia
and memantine) and resuscitation (epinephrine and vasopressin) medication might influence
hemodynamics. On the other hand, we must bear in mind that cardiopulmonary arrest and
resuscitation represent, in essence, a state of shock and consecutive hemodynamic instability,
with altered dynamics and interrelationships between hemodynamic variables, supplemented by
the influence of other external factors such as artificial ventilation, cardiac massage, etc.
Additionally, we mention the possibility of a correlation between two hemodynamic variables
without a causal relationship. On the other hand, the absence of monitored hemodynamic
parameter values during certain moments (especially VF) may mask or influence the dynamics
and interrelations between certain variables studied in this thesis. However, we believe that
further studies are needed to evaluate these hypotheses.
NEUROPROTECTIVE MEDICATION INFLUENCE ON MONITORED PARAMETERS
From a hemodynamic point of view, the neuroprotection strategy used yielded results that
are comparable to those from previous studies. Compared with other lots, hypothermia resulted
in lower heart rate and increased mean blood pressure starting from 5 minutes from the return to
spontaneous circulation. Throughout ROSC period, cardiac output and stroke volume variability
were more constant, and systemic vascular resistance was increased, the highest values being
found 5 to 30 minutes from ROSC. Hypothermia triggered the lowest values of EtCO2 and PCO2
of all resuscitated groups and less severe degree of metabolic acidosis, hyperlactataemia being
the lowest among all groups (15 to 30 minutes post-ROSC). Throughout CPR and ROSC,
hematocrit had the lowest values in hypothermic pigs, and compared with the other resuscitated
lots oxygen delivery was lower within 15-60 post-ROSC.
Resuscitation under memantine involved elevated heart rates post-ROSC, and with the
dose of 10 mg/ kg, cardiac output and stroke volume peaked (compared to other resuscitated
lots); base excess had the lowest values within 5-30 minutes post-ROSC. Metabolic acidosis was
xi
the most serious in the range of 5-30 min post-ROSC, with an elevated lactate level when
compared with the hypothermic lot. Only in the memantine receiving lots we identified a strong
positive correlation between the partial pressure of carbon dioxide and end-tidal carbon dioxide,
strong positive correlations between heart rate and end-tidal carbon dioxide, between cardiac
output and blood lactate and between the oxygen delivery and the end-tidal carbon dioxide. Also
we identified strong negative correlations between cardiac output and base excess, and between
cardiac output and bicarbonate ion concentration.
The hypothermic lot was an exception for many correlations. Thus, among the
resuscitated lots we identified strong positive correlations between glycaemia and oxygen
delivery, between blood lactate and oxygen delivery, as well as a very strong correlation between
heart rate and oxygen delivery in lots with hemodynamic instability, with one exception – the lot
with therapeutic hypothermia. Similarly, we found strong negative correlations between blood
base excess and oxygen delivery, between bicarbonate ion concentration and oxygen delivery,
and a very strong correlation between blood bicarbonate ion concentration and heart rate in lots
with hemodynamic instability with the same exception, the lot resuscitated with therapeutic
hypothermia.
Potential limitations of the study. This study also has some limitations. First, the rather
small number of pigs per lot, which still constitutes minimum requirements in terms of statistics,
to which the costs of related material are added. The experiment was based on healthy pigs,
where we induced VF to study hemodynamics in resuscitation and post resuscitation with
neuroprotection, in contrast to patients entering cardiac arrest consecutive to underlying
pathologies, who present by default pathophysiological particularities and specific hemodynamic
particularities. On the other hand, such a study provides a basis for comparison targeting the
development of hemodynamic variables in patients with specific pathologies, and simultaneously
the possibility of hemodynamic guidance of therapeutic maneuvers. Anesthesia and controlled
ventilation may influence certain hemodynamic parameters values, leading to significant changes
compared to normal patients, unsedated and with spontaneous breathing. However, they
represent an important goal to meet welfare of animals used in these experimental studies. We
have not reviewed CPP (coronary perfusion pressure) although other studies have successfully
rated this parameter, but our study did not initially propose to study hemodynamic differences
between successfully resuscitated animals versus unsuccessfully resuscitated animals (animals
with no return to spontaneous circulation). We evaluated the dynamics and potential correlations
of blood variables (arterial, central venous, jugular bulb) as average, and from a statistical point
of view we consider that it is necessary to supplement the research with a separate distinct
assessment. We used a method of determining cardiac output validated only in humans
(FloTrac/Vigileo), and still not yet validated in pigs, therefore we believe that it would be
necessary that values obtained by this method should be compared with a validated method (e.g.
transpulmonary thermodilution or LiDCO). However, given that cardiovascular physiology in
pigs is similar to the human model, we believe that the values obtained in this study may be
considered.

xii
E
xam
ple
of
the
evolu
tion
of
hem
odynam
ic v
aria
ble
s in
the
five
studie
d l
ots
Fig
. 2. B
ase
exce
ss (
blo
od)
dynam
ics
Fig
. 4. B
lood l
acta
te d
ynam
ics
Fig
. 1. H
eart
rat
e dyn
amic
s
Fig
. 3. O
xygen
del
iver
y d
ynam
ics
xiii
Exam
ple
s of
corr
elat
ions
bet
wee
n c
lass
es o
f h
emodynam
ic p
aram
eter
s
Fig
. 6. C
orr
elat
ion b
etw
een b
ase
exce
ss a
nd l
acta
te (
blo
od),
lot
3
Fig
. 8. C
orr
elat
ion b
etw
een b
ase
exce
ss a
nd l
acta
te (
blo
od),
lot
5
Fig
. 5. C
orr
elat
ion b
etw
een b
ase
exce
ss a
nd l
acta
te (
blo
od),
lot
2
Fig
. 7. C
orr
elat
ion b
etw
een b
ase
exce
ss a
nd l
acta
te (
blo
od),
lot
4

xiv
6. CONCLUSIONS AND RECOMMENDATIONS
Conclusions regarding dynamic evaluation of monitored hemodynamic parameters
The studied hemodynamic parameters had a constant linear evolution during all four pre-
established experimental moments in the control group, and only during baseline in the
four resuscitated lots.
Ventricular fibrillation period was characterized by the collapse of blood flow
parameters – heart rate was 0, extreme arterial hypotension (10% of baseline value), low
cardiac output and end-tidal carbon dioxide abruptly decreasing to 0.
Resuscitation period involved heart rate and cardiac output dependent on resuscitation
maneuvers, arterial hypotension (maximum 50% of baseline value), decreased base
excess and bicarbonate, increasing end-tidal carbon dioxide (nearly to 50% of baseline
values), increased partial pressure of oxygen, glycaemia, hematocrit, hyperlactatemia as
well as hyperkalemia.
The return to spontaneous circulation period was characterized by an initial growth of
most global hemodynamic parameters – tachycardia and hypertension, cardiac output,
central venous pressure and pulmonary capillary wedge pressure were all increased –
after which the trend was towards normalization.
15 minutes post-ROSC base deficit was greatly accentuated (15 minutes after ROSC) and
bicarbonate ion concentration minimal, and starting with 30 minutes post-ROSC their
evolution was ascending and became normal at the end of monitoring.
Immediately post-ROSC mixed acidosis (metabolic and respiratory) was severe, and end-
tidal carbon dioxide and partial pressure of carbon dioxide were elevated, but both
become normal after 120 minutes post-ROSC.
Partial pressure of oxygen and oxygen delivery were highly elevated (hyperoxia
consecutive 100% FiO2, gradual decreased to 30%); hematocrit, glycaemia and
lactatemia were increased immediate post-ROSC, with a decreasing trend towards
normalization after 120 minutes.
15 minutes after ROSC, there was an inverse proportional relationship between EtCO2
and BE(B). At the same time, PCO2 and EtCO2 peaked, and metabolic acidosis was the
most severe.
Although still not validated in pigs, Vigileo FloTrac method has potential for an accurate
assessment of CO in terms of hemodynamic stability; under extreme hemodynamic
instability – ventricular fibrillation and then resuscitation – it is less accurate, since it is
virtually impossible to assess the arterial pressure wave.
Conclusions regarding correlations between monitored hemodynamic parameters
During ventricullar fibrillation, CPR and ROSC periods, significant correlations were
disturbed.
Among monitored global hemodynamic parameters, only heart rate and mean arterial
pressure were positively correlated in terms of hemodynamic stability.
Between acid-base parameters only base excess and blood bicarbonate correlate
positively under hemodynamic stability and also instability; however, most existing
correlations during hemodynamic stability conditions were not maintained during
ventricular fibrillation, resuscitation and return to spontaneous circulation.
We have not identified correlations within the oxygenation status parameters.

xv
Within metabolic and tissue perfusion parameters there was only one strong positive
correlation – blood glucose and blood lactate in all resuscitated lots (with and without
neuroprotection).
Overall, taking into account all studied hemodynamic parameters in the four periods, we
identified few strong correlations:
Between cardiac output and oxygen delivery – a strong positive correlation in conditions
of hemodynamic stability, which became very strong in the groups resuscitated under
neuroprotection.
In all four resuscitated lots – strong negative correlations between blood lactate and base
excess, as well as with bicarbonate ion concentration.
In lots resuscitated with neuroprotection – strong positive correlations between cardiac
output and glycaemia, and between partial pressure of carbon dioxide and blood lactate.
Conclusions regarding the influence of neuroprotective medication on monitored
parameters
The dynamic of assessed variables and the identified correlations were influenced by
neuroprotective medication (therapeutic hypothermia and memantine).
Therapeutic hypothermia had a beneficial effect on the development of studied
hemodynamic variables, favorably influencing the evolution of resuscitated animals.
Therapeutic hypothermia influenced the evolution of hemodynamic parameters, leading
to a change of relations between them (correlations are not maintained).
Resuscitation under memantine directly influenced cardiac activity (positive
cronotropism, increased cardiac output and stroke volume), emphasized blood lactate
level and exacerbated metabolic acidosis immediately post-ROSC.
Because at certain moments (especially during induced ventricular fibrillation), due to
technical reasons, some hemodynamic parameters were not recorded, we cannot exclude the
possibility of a partial interpretation from a statistical point of view.
We consider it necessary to continue studies on hemodynamics during resuscitation in
order to confirm the results and to evaluation of these hypotheses.
Recommendations. Since we have identified only a few strong correlations (with good
predictive accuracy) between studied hemodynamic parameters in the four distinct periods, we
recommend:
Cautionary interpretation of the patient's hemodynamic status in each of the three
critical periods – cardio-pulmonary arrest period, resuscitation period, and return
to spontaneous circulation period;
Complex approach of the hemodynamic variables as a whole in the deployment of
the resuscitation strategy and post cardio-pulmonary arrest hemodynamic
optimization.
As neuroprotective therapy, given the beneficial effects on the evolution of studied
hemodynamic variables, we suggest using both therapeutic hypothermia as well as memantine.
However, we do consider supplemental clinical investigations necessary, in order to complete
the study of hemodynamic effects of the two neuroprotective strategies.