Embed Size (px)
Citation preview

Phase synchronization analysis of prefrontal tissue oxyhemoglobin oscillations inelderly subjects with cerebral infarctionQingyu Han, Zengyong Li, Yuanjin Gao, Wenhao Li, Qing Xin, Qitao Tan, Manyu Zhang, and Yixun Zhang Citation: Medical Physics 41, 102702 (2014); doi: 10.1118/1.4896113 View online: http://dx.doi.org/10.1118/1.4896113 View Table of Contents: http://scitation.aip.org/content/aapm/journal/medphys/41/10?ver=pdfcov Published by the American Association of Physicists in Medicine Articles you may be interested in Spectral analysis of near-infrared spectroscopy signals measured from prefrontal lobe in subjects at risk forstroke Med. Phys. 39, 2179 (2012); 10.1118/1.3696363 Noninvasive, in vivo imaging of the mouse brain using photoacoustic microscopy J. Appl. Phys. 105, 102027 (2009); 10.1063/1.3116134 The Alzheimer’s β amyloid ( A β 1 – 39 ) monomer in an implicit solvent J. Chem. Phys. 128, 165102 (2008); 10.1063/1.2907718 Spatiotemporal dynamics of networks of excitable nodes Chaos 16, 015110 (2006); 10.1063/1.2177569 PIXE analysis of low concentration aluminum in brain tissues of an Alzheimer’s disease patient AIP Conf. Proc. 475, 468 (1999); 10.1063/1.59261

Phase synchronization analysis of prefrontal tissue oxyhemoglobinoscillations in elderly subjects with cerebral infarction
Qingyu Han, Zengyong Li,a) Yuanjin Gao, and Wenhao LiKey Laboratory of High Efficiency and Clean Mechanical Manufacture, School of Mechanical Engineering,Shandong University, Jinan 250061, China
Qing XinHospital of Shandong University, Jinan 250061, China
Qitao Tan, Manyu Zhang, and Yixun ZhangKey Laboratory of High Efficiency and Clean Mechanical Manufacture, School of Mechanical Engineering,Shandong University, Jinan 250061, China
(Received 30 April 2014; revised 3 September 2014; accepted for publication 9 September 2014;published 30 September 2014)
Purpose: This study aims to assess the phase relationship of prefrontal tissue oxyhemoglobinoscillations using wavelet phase coherence analysis of cerebral Delta [HbO2] signals in cerebralinfarction (CI) patients during the resting state.Methods: Continuous recordings of near-infrared spectroscopy signals were obtained from the leftand right prefrontal lobes in 21 subjects with CI (Group CI, age: 76.6 ± 8.5 yr) and 21 healthy elderlysubjects (Group Healthy, age: 69.0 ± 7.4 yr) during the resting state. The Group CI was furtherdivide into two groups: CI with hypertension and CI without hypertension. The phase synchronizationbetween left and right prefrontal Delta [HbO2] oscillations in four frequency intervals (I, 0.6–2 Hz;II, 0.145–0.6 Hz; III, 0.052–0.145 Hz; and IV, 0.021–0.052 Hz) was analyzed using wavelet phasecoherence method.Results: The phase coherences in intervals III and IV were significantly lower in CI with hypertensionthan in healthy elderly subjects (F = 12.974, p= 0.001 for III and F = 10.073, p= 0.004 for intervalIV). The phase coherence of CI without hypertension in interval III was significantly lower than inhealthy elderly subjects (F = 9.909, p= 0.004). Also, the phase coherence in interval IV was signif-icantly lower in CI with hypertension than in CI without hypertension (F = 5.665, p= 0.028). Also,the phase agreement in interval IV showed evident difference between Group CI with hypertensionand without hypertension.Conclusions: The difference in phase characteristics of prefrontal tissue oxyhemoglobin oscillationsbetween the CI patients and healthy elderly indicates altered phase synchronization. Moreover, theCI combined with hypertension would aggravate this process. This study provides new insight intothe phase dynamics of cerebral oxygenation and may be useful in assessing the risk for stroke.C 2014 American Association of Physicists in Medicine. [http://dx.doi.org/10.1118/1.4896113]
Key words: near-infrared spectroscopy, wavelet phase coherence, functional connectivity, cerebralinfarction, cerebral oxygenation, spontaneous oscillations
1. INTRODUCTION
Spontaneous oscillations in the low frequency range (<0.1 Hz)have been demonstrated to exhibit strong correlations in dis-tinct regions of the brain in the resting state.1 This correlationis defined as “resting state functional connectivity,” which hasbeen well reproduced in many studies using functional mag-netic resonance imaging (fMRI) (Refs. 2–4) and near-infraredspectroscopy (NIRS).5–7
NIRS is an increasingly popular technology for studyingbrain function. NIRS is based on measuring changes in localoxygenated and deoxygenated hemoglobin concentrations.8,9
While brain NIRS shares a common physiological basisto fMRI, it offers several potential advantages in terms oflogistics (cost, equipment portability, and patient compati-bility) and data quality (temporal sampling density >10 vs<1 Hz).10 NIRS has become a suitable and easily manageable
method to monitor cerebral cortical oxygenation continu-ously and noninvasively at rest or brain activation.7,8,11
Functional connectivity has been successfully observedduring the resting state in both adult and infant participantsusing NIRS.6–8,12 NIRS has high temporal resolution and ithas revealed a temporal relationship of signals obtained atdifferent brain regions.13,14 The correlations in cortical net-works concentrate within ultralow frequencies (0.01–0.06 Hz)and it shows distinct frequency-specific features in the func-tional networks.15 By decomposing fluctuations of oxygenatedhemoglobin and deoxygenated hemoglobin signals into vari-ous frequency bands, Sasai et al.16 investigated the frequencydependency of functional connectivity between diverse re-gions in the cerebral cortex. The functional connectivity be-tween homologous cortical regions of the contralateral hemi-sphere showed high coherence in the frequency range of0.009–0.1 Hz.16
102702-1 Med. Phys. 41 (10), October 2014 0094-2405/2014/41(10)/102702/8/$30.00 © 2014 Am. Assoc. Phys. Med. 102702-1

102702-2 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-2
Spontaneous activity in prefrontal cerebral oxygenationshas been demonstrated to be disturbed in elderly persons,17
in persons with cerebral infarction (CI),18 and in elderlysubjects with hypertension.12 Clinical studies demonstratedthat resting-state connectivity is altered in disorders such asstroke,19 and stroke lesions cause neural dysfunction both atthe lesion site and in remote brain regions.20 However, it isunclear what patterns of phase relationships in the left andright prefrontal regions are most closely associated with CI,especially in the CI patients with hypertension.
The power spectra of Delta [HbO2] signals have beenfound to exhibit oscillations in various frequency bands.18,21–24
Wavelet analysis can detect these oscillations with logarithmicfrequency resolution.12,18,25 Different characteristic frequen-cies of Delta [HbO2] signals have been identified using waveletanalysis, which indicate possible regulatory mechanisms ofthe tissue oxygenation signal.18,25,26 The oscillations in inter-vals I (0.6–2 Hz) and II (0.15–0.6 Hz) reflect the effects of car-diac and respiratory activities, respectively.18,25,27 The cerebraloscillations in interval III (0.05–0.15 Hz) might originate lo-cally from intrinsic myogenic activity of smooth muscle cellsin resistance vessels and this may be partly under autonomiccontrol.22,27 The interval IV (0.02–0.05 Hz) is considered tobe closely regulated through tight neurovascular coupling andpartial autonomic control within the brain.28
The cross spectrum and wavelet coherence are often usedin bivariate data analysis to detect phase synchrony betweenparticular frequency components that are common to bothof the signals under consideration.29,30 In general, the quan-tification of phase synchrony can be estimated by using thecross spectrum obtained from the Fourier transforms, conceptof analytic signal, or complex wavelet transform. The differ-ences between these methods have been demonstrated to beminor, and they are fundamentally mathematical equivalentwhen typically applied in spectral analyses.31,32 However,the cross spectrum obtained from the Fourier transformsof the whole time series is uninformative, and the truecross spectrum must be estimated by use of windowing andaveraging.30 Also, the coherence approach based on wavelettransform is best suited for treatment of nonstationary data oftime series, while the cross spectrum analysis obtained fromthe Fourier transforms implies stationarity of time series.22
The wavelet phase coherence (WPCO) can identify pos-sible phase relationships by evaluating the match betweenthe instantaneous phases of two signals in various frequencybands.33,34 WPCO has been successfully used to analyze therelationships between oscillations in skin blood flow, temper-ature and oxygen saturation, and intracranial pressure and ar-terial blood pressure (ABP) signals within certain frequencyranges.34–37 In this study, we used the wavelet transform,rather than the Fourier transform or Hilbert transform, ap-proach to the phase coherence as this offers a more intuitivevisualization of time–frequency behavior. We hypothesizethat the phase synchronization in the left and right prefrontalregions would be altered due to CI. The aim of this study wasto assess the phase relationships of left and right prefrontaloxygenations in CI patients during resting state using WPCOanalysis.
2. METHODS AND MATERIALS
2.A. Subjects
A total of 42 subjects were recruited from ShandongUniversity and local rehabilitation center to participate inthis study. Of the 42 subjects, 21 were elderly with cerebralinfarction (CI) (age: 76.6 ± 8.5 yr; Group CI). Among them,8 were subjects with hypertension and 13 subjects with-out hypertension. Twenty-one were healthy subjects [age:69.09 ± 7.4 yr; Group Health (G1)]. The CI group wasfurther divide into two groups: CI without hypertension(G2) and CI with hypertension (G3). The affected area ofcerebral infarction was different in each subject. Twelve ofthe affected areas were localized in the left side of the headand nine was in the right side.
Healthy subjects had no history of neurological or vasculardisease. Patients included in the study were subjects havinginfarcts on computed tomography (CT) scan and CI occurredmore than 12 months ago. Excluded from the study weresubjects with diabetes mellitus; subarachnoid hemorrhage;insufficiency of the heart, lungs, kidneys, and liver; smokingor drinking habits; and additional medications (angiotensin-converting enzyme, inhibitors/angiotensin II-receptor block-ers, and calcium-channel blockers). A diagnosis of hyperten-sion was made when systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mm Hg.38 This wasperformed in the course of study. A diagnosis of diabetes mel-litus was based on clinical assessment or fasting serum glucoselevel.
Prior to the experiment, basic subject information, in-cluding age, weight, height, and BP was recorded (Table I).Informed consent was obtained from all subjects. The experi-mental procedures were approved by the Human Ethics Com-mittee of Shandong University and were in accordance withthe ethical standards specified by the Helsinki Declaration of1975 (revised in 1983).
2.B. Measurement
Data for the NIRS signals in left and right prefrontal lobeswere obtained from simultaneous measurements. After theage, height, and body mass of the participants were recorded,NIRS measurements were performed on the subjects usingthe cerebral tissue saturation monitor (TH-200, developedby Tsinghua University, China). As spontaneous oscillationsare posture-dependent,39 NIRS measurements were collectedin their supine position. The TH-200 sensor consisted ofa two-wavelength light-emitting diode (LED) and two PINdiodes. The LED component served as the source of emittedlight at 760 and 850 nm, whereas the PIN diodes served asthe detectors. Photons can penetrate the overlying tissuesinto the cerebral cortex (gray matter) when the distancebetween the detector and the source is ≥30 mm. Moreover,the penetration depth can reach the maximum value whenthe distance is 40 mm.40 Therefore, the distances betweenthe light source and the two detectors were set to 30 mm(S1) and 40 mm (S2), respectively. The differential signal(S1−S2) in the optical density (OD) was recorded by the two
Medical Physics, Vol. 41, No. 10, October 2014

102702-3 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-3
T I. Characteristics of the participants.
HealthyCI P for difference
Characteristics G1 G2 G3 G1 vs G2 G1 vs G3 G2 vs G3
Age (yr) 69.0(7.4) 76.6(8.9) 76.6(8.3) 0.052 0.121 0.998Body mass index (BMI) 24.2(2.8) 21.3(1.9) 22.7(2.9) 0.007∗∗ 0.495 0.669Female sex 57.1% 30.8% 62.5% 0.363 0.993 0.454Systolic blood pressure (mm Hg) 124.5(11.6) 131.3(7.8) 160.6(27.0) 0.603 0.000§§ 0.000##
Diastolic blood pressure (mm Hg) 73.7(8.2) 72.5(8.0) 81.0(11.1) 0.997 0.193 0.132
Note: G1, healthy; G2, CI without hypertension; and G3, CI with hypertension. Values are presented as means and standard deviations and percentages. The t-test wasused for means and standard deviations, and chi-square test for percentages. Significant differences are marked with ∗∗p < 0.01 between the G1 and G2. §§p < 0.01between the G1 and G3. ##p < 0.01 between the G2 and G3.
detectors and used to obtain the cortical signals includingchanges in oxyhemoglobin (HbO2) and deoxyhamoglobin(HHb) using differential spectroscopy based on the modifiedBeer–Lambert law. This configuration was validated by Dinget al.41 The forehead of each subject was cleaned using iso-propyl alcohol. Afterward, the sensors were carefully fixedusing a flexible adhesive fixation pad and an elastic band. Thesensors were placed on the left and right forehead 1.5 cmlateral to the cerebral midline to avoid the sagittal sinus andat least 2 cm above the eyebrow to avoid the frontal sinus.The sensors were carefully secured with a tensor bandagewrapped around the forehead while ensuring no admissionof background light. The sampling rate of the NIRS-derivedsignals was set to 20 Hz. The Delta [HbO2] signals weremonitored at the prefrontal lobes for 15 min using NIRS. Tohelp reduce movement artifact, the volunteers were asked toavoid sudden movements during the measurement.
2.C. Data preprocessing
Wavelet transform was applied to the NIRS time seriesto decompose the results into signal and uncorrelated noisecomponents in distinct scales. The wavelet transform wascalculated in the 0.021–2 Hz frequency intervals. Slow vari-ations defined as below 0.021 Hz and uncorrelated noisecomponents above 2 Hz were removed. The whole signalof 15 min was used to obtain wavelet amplitude and phasecoherences. In addition, the average Delta [HbO2] of allrecorded segments was used for signal normalization to avoidsystematic differences between subjects and groups.
2.D. Wavelet transform
Wavelet transform is a method that allows the complextransformation of a time series from the time domain to thetime–frequency domain. It involves convolving the time seriesg(u) with a family of generally nonorthogonal basis functionsthat are generated from the mother wavelet35,42
W (s,t)= 1√
s
+∞
−∞
Ψ
u− ts
g(u)du, (1)
where W (s,t) is a wavelet coefficient and Ψ is the Morletmother wavelet, scaled by the factor s and translated in time
by t. The Morlet mother wavelet is a complex sinusoidmodulated by the Gaussian function with basic frequency ω0
Ψ(u)= 14√π· e−iω0u · e−u
2/2, (2)
where i =√−1. The continuous wavelet transform is a map-
ping of the function g(u) onto the time–frequency plane.Wavelet scaling enables the detection of oscillations with dif-ferent frequencies, whereas wavelet translation in time allowsthe monitoring of spectra evolution over time. The translationfrom scale to frequency depends upon the particular choice ofwavelet. An approximate relationship between wavelet scaleand translated frequency, pseudofrequency, f s, was computedas43
f s =fc
s · δt, (3)
where fc is the center frequency and δt is the sampling period.The choice of ω0 is a compromise between localization intime and in frequency. For smallerω0, the shape of the waveletfavors localization of singular time events, whilst for largerω0 more periods of the sine wave in the window improve thefrequency localization.42,44 To detect a frequency, the signalmust be observed over at least one period of this frequency.In this study, we choose ω0= 5, in time, approximately six toseven periods. The wavelet transform was calculated in thefrequency interval of 0.021–2 Hz. The upper limit of 2 Hzwas set to include the heart rate frequency, whereas the lowerlimit was selected to include possible regulatory mechanismsof the tissue oxygenation signal.18,25,27
2.E. Wavelet phase coherence
The wavelet coefficients are complex numbers with thecomplex Morlet wavelet. These values define the absoluteamplitude and instantaneous relative phase for each fre-quency and time. Phase information can be used to inves-tigate the relationships between oscillations from differentsignals.35 The relationship between the phases of two oscilla-tory processes at a specific frequency is defined as the phasecoherence. If a characteristic phase difference is maintainedbetween two signals, they have high phase coherence.45
Medical Physics, Vol. 41, No. 10, October 2014

102702-4 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-4
WPCO identifies possible relationships by evaluating thematch between the instantaneous phases of two signals.35
The instantaneous phases, named φ1k,n and φ2k,n, werecalculated at each time tn and frequency fk for both signals.34
The indices k and n refer to discrete frequency and time,respectively. The basic frequency is scaled according toωk = 1.05ωk−1 and the time is discretized by tn = nτ; τ = 1s.34
The phase difference between the components at a givenfrequency is φt and varies as a function of time t (between1 and T). The mean phasor P is given by36
P=1T
Tt=1
eiϕt . (4)
T is the whole length of the time series. The phase coherenceis equal to the amplitude of P. The synchronization is definedas the magnitude of P, i.e., the phase coherence. The valueof the phase coherence is between 0 and 1. It quantifies thetendency of the phase difference between the two signals toremain constant at a particular frequency.35 If the phase coher-ence is high, the subject preserves a particular typical phasedifference between the wavelet transforms at this frequency.
The phase difference for each subject can be representedas a unit phasor and the phasors combined in the complexplane. The term phase agreement was introduced to indicatethe similarity between values of phase difference determinedfor different subjects.36 Subject n has a typical phase differ-ence φn. The sample averaged phasor M over all subjects isgiven by36
M =1N
Nn=1
eiϕn. (5)
The phase agreement is defined as the amplitude of M . Thephase shift is given by the phase of M .
2.F. Amplitude-adjusted Fourier transform (AAFT)surrogate signals
When two oscillations are unrelated, their phase differencecontinuously changes with time; thus, their phase coherenceapproaches zero. Significant coherence was determined dur-ing the evaluation of the coherence of two oscillatory timeseries that may have variable amplitude and frequency. Themethod of AAFT surrogates produces surrogates of a signal,in which any temporal relationship with another signal is de-stroyed but the spectrum of the original data is preserved. TheAAFT method is used to estimate the parameters of the nulldistribution produced by unrelated or uncoupled time serieswith the same spectral characteristics as the original timeseries.30 With this method, a distribution of coherence valuescan be generated by subjecting the surrogate signals to exactlythe same procedures as the real data. The actual coherencevalue can be characterized in terms of its rank relative to thisdistribution (i.e., how many of the surrogate coherence valuesit exceeds). If the rank is high (close or equal to 100% of thesurrogate values) then the actual coherence value is unlikelyto have arisen by chance from unrelated signals.30 AAFT
surrogate signals were generated by shuffling the phases ofthe original time series to create a new time series with thesame means, variances, and autocorrelation functions as theoriginal sequences but without any phase relations.35 We thenaveraged 100 WPCOs from surrogate signals. A WPCO fromthe original recording was considered statistically significantwhen it was two standard deviations above the mean surrogatecoherence.
2.G. Statistical analysis
The phase coherence, age, BMI and BP were expressed asthe means (standard deviations) and sex as percentages. Thedata of each subject were tested for normality (Kolmogorov–Smirnov test) at the group level and for homogeneity ofvariance (Levene test) to ensure that the values fulfilled theassumption required by the parameter analysis. Significantdifferences between the characteristics of healthy elderly sub-jects and of the CI patients with or without hypertension weredetermined using a t-test (for means and standard deviations),and chi-square test (for percentages). Two-way ANOVA withfactors CI and hypertension were used to determine the maineffects on the phase coherence. Post-hoc analyses of thetwo groups were performed using Bonferroni comparisontests. A difference with p < 0.05 was considered statisticallysignificant.
3. RESULTS
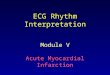
In this study, periodic oscillations of the Delta [HbO2] sig-nals in the left and the right prefrontal lobes were identified atfour frequencies intervals: (I, 0.6–2 Hz; II, 0.145–0.6 Hz; III,0.052–0.145 Hz; and IV, 0.021–00.052 Hz) (Fig. 1).
Figure 2 shows an example of the phase coherence the leftand right prefrontal Delta [HbO2] oscillations and the meanand two standard deviations of AAFT surrogate signals. Thephase coherence between the left and right prefrontal Delta[HbO2] oscillations was significant in the four intervals fromI to IV.
Figure 3 shows a comparison of the phase coherencesof the left and right prefrontal Delta [HbO2] signals amongthe three groups. The phase coherences in intervals III andIV were significantly lower in CI with hypertension thanin healthy elderly subjects (F = 12.974, p= 0.001 for III;F = 10.073, p= 0.004 for interval IV). Also, the phase co-herence in interval III was significantly lower in CI withouthypertension than in healthy elderly subjects (F = 9.909,p= 0.004). In addition, the phase coherence in interval IVshowed significant difference between CI with hypertensionand without hypertension (F = 5.665, p= 0.028).
As shown in Fig. 4, the phase agreement in intervalIII showed evident difference between Group Healthy andGroup CI with hypertension. Also, the phase agreement ininterval IV showed evident difference between Group CIwith hypertension and without hypertension. However, thephase shift did not show evident difference in these intervals(Fig. 5).
Medical Physics, Vol. 41, No. 10, October 2014

102702-5 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-5
F. 1. Typical time series of the simultaneous recordings of Delta [HbO2]signals from a healthy elderly person (a) in the left prefrontal lobe; (b)in the right prefrontal lobe; and (c) the average wavelet amplitude. Thevertical lines indicate the outer limits of the frequency intervals: I (0.6–2 Hz),II (0.145–0.6 Hz), III (0.052–0.145 Hz), and IV (0.021–0.052 Hz).
4. DISCUSSION
In this study, the phase relationship between simultane-ously measured left and right prefrontal Delta [HbO2] signalsof healthy elderly and CI patients with hypertension wasassessed using wavelet-based phase coherence analysis. Ourresults show that the phase coherence in intervals III andIV exhibited significantly lower level in the CI patients with
F. 2. Phase coherence (solid line) of the left and right prefrontal Delta[HbO2] signals, mean (dashed line) and two standard deviations (dotteddashed line) of AAFT surrogate signals.
F. 3. Comparison of the phase coherence among the Group Health,Group CI with hypertension and Group CI without hypertension. Fre-quency intervals: I (0.6–2 Hz), II (0.145–0.6 Hz), III (0.052–0.145 Hz), andIV (0.021–0.052 Hz). Significant differences are marked with ∗∗p < 0.01between the Group CI without hypertension and Group Healthy, §§p < 0.01between the Group CI with hypertension and Group Healthy, #p < 0.05between the Group CI with hypertension and without hypertension.
hypertension than in the healthy elderly subjects. Most strik-ingly, the hypertension combined with CI did show significanteffects on the phase coherence in the CI patients.
The WPCO indicates the consistency of the phase delaybetween two signals and can quantify the stability of phasedifference. It allows the identification of significant coher-ence even at low common power; this capability is particu-larly important when low-frequency components significantlycontribute to cardiovascular signals.35 The phase agreementindicates the similarity between values of phase differencedetermined for different subjects.36 If it is high, the subjectsagree about the typical phase difference between the wavelettransforms of left and right prefrontal Delta [HbO2] signalsat this frequency. The high agreement in these componentsindicates the synchronization of neural activation in the leftand right prefrontal regions in healthy elderly subjects duringresting state.
The cerebral oscillations in interval III originated locallyfrom intrinsic myogenic activity of smooth muscle cells andthese components reflect neural control of the cerebral circu-lation.22,27 It has been demonstrated that there is strong func-tional connectivity among spontaneous fluctuations of distinctregions of the brain in the low frequency range (interval III)in the resting state.1–7 Functional connectivity is characterized
F. 4. Phase agreement of the healthy elderly and the subjects with cerebralinfarction (CI) in the four frequency intervals. Frequency intervals: I (0.6–2 Hz), II (0.145–0.6 Hz), III (0.052–0.145 Hz), and IV (0.021–0.052 Hz).
Medical Physics, Vol. 41, No. 10, October 2014

102702-6 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-6
F. 5. Phase shift of the healthy elderly and the subjects with cerebral infarc-tion (CI) in the four frequency intervals. Frequency intervals: I (0.6–2 Hz),II (0.145–0.6 Hz), III (0.052–0.145 Hz), and IV (0.021–0.052 Hz).
by a temporal correlation between two raw time series in thelow frequency interval (0–0.1 Hz).46 Sasai et al.16 reported thatfunctional connectivity between homologous cortical regionsof the contralateral hemisphere showed high coherence over awide frequency range (0.009–0.1 Hz) based on Delta [HbO2]signals. In the present study, the phase coherence in intervalIII exhibited significantly lower level in the CI patients withor without hypertension than in the healthy elderly subjects.
Clinical studies have demonstrated that resting-state con-nectivity is altered in disorders such as stroke, suggesting adisruption of neuronal and/or vascular factors that contributeto high correlation in resting-state connectivity networks.19
Stroke lesions cause neural dysfunction both at the lesionsite and in remote brain regions.20 Our results show that thelesion resulted in an altered phase synchronization of theleft and right prefrontal oscillations. This further conformsa disruption of resting-state connectivity of left and rightprefrontal networks in the CI patients.
The oscillations in interval IV are closely regulated throughtight neurovascular coupling and partial autonomic control.28
In the present study, the high phase agreement in intervalIV indicated the consistency of the phase delay between leftand right prefrontal Delta [HbO2] oscillations under the con-trol neurogenic origins in healthy elderly subjects. However,the phase coherence in interval IV was significantly lower inGroup CI without hypertension than in the Group Healthy.This suggests a disruption of resting-state connectivity of leftand right prefrontal networks.
It has been demonstrated that hypertension has signifi-cant influence on the phase coherence of the left and rightprefrontal regions in elderly subjects.12 In the present study,the averaged phase coherence showed evident lower level ininterval IV in Group CI with hypertension than in Group CIwithout hypertension. These results showed that the hyper-tension did have significant effect on phase coherence. TheCI combined with hypertension would aggravate the processof weakened brain functional connectivity.
Since the oscillations in interval I reflect the effects ofthe cardiac activity, the cardiac pulsation should be in phaseregardless of the hemisphere. In fact, the phase of cardiacpulsation in the left and right hemispheres maybe not in fullsynchrony due to the different flow paths. According to ourprevious study, the cerebral oscillations measured from thefrontal lobe were closely related to the pulsatility of external
carotid artery (ECA) and middle cerebral artery (MCA).47
As there may be some differences in the vessel stiffness ofECA and MCA, the phase of cardiac pulsation in the left andhemisphere may be not in full synchrony.
4.A. Methodological considerations
NIR light must first pass through the superficial tissuelayers (scalp and skull) before reaching the cortex. Therefore,these superficial layers may provide noise as well as non-specific hemodynamic variations and this would contaminatethe measured signal.48 The interferences from superficiallayers are often referred to as “global interference.”49,50 Inthe present study, we used one light source and two detectorsplaced at 30 and 40 mm from the source to separate extrac-erebral (scalp and skull) and brain hemodynamic signals. Forsuch configurations, the differences in the OD as detected bythe two detectors were mainly attributed to the tissue (cortex)absorption.
Significant coherence was tested during the evaluation ofthe coherence of two oscillatory time series that may havevariable amplitude and frequency. The test was performedby generating AAFT surrogate signals via shuffling of thephases of the original time series to create a new timeseries with the same means, variances, and autocorrelationfunctions (and therefore the same power spectra) as theoriginal sequences but without any phase relations. When thecoherence value is equal to the standard deviations above themean surrogate coherence, a temporally constant interferencepossibly exists between the signals regardless of their spec-tral similarities or differences.35 The left and right prefrontaltissue oxyhemoglobin oscillations have been demonstrated toexhibit significant WPCO in intervals from I to IV in thehealthy elderly subjects using AAFT.12
A limitation of current study was the recordings period.Recordings are recommended to last at least ten times theperiod of the lower frequency boundary of the investigatedcomponent.51 The recordings lasted 900 s and oscillations withfrequency below 0.01 Hz would be represented with fewer thanten cycles. This may result in an unreliable detection of theamplitude within the interval. Due to the limited recordingsperiod, we did not analyze the oscillations in frequency inter-vals V (0.095–0.02 Hz) and VI (0.005–0.0095 Hz), which wereidentified and investigated by Stefanovska et al.42 and Kvandalet al.52
4.B. Summary
The phase relationship between simultaneously measuredleft and right prefrontal Delta [HbO2] signals of healthy elderlyand CI patients was assessed using wavelet-based phase co-herence analysis. Our results show that the phase coherence inintervals III and IV exhibited significantly lower level in the CIpatients with hypertension than in the healthy elderly subjects.Moreover, the hypertension did show significant effects on thephase coherence in the CI patients. This study provides newinsight into the phase dynamics of cerebral oxygenation andmay be useful in assessing the risk for stroke.
Medical Physics, Vol. 41, No. 10, October 2014

102702-7 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-7
ACKNOWLEDGMENT
This project was supported by the National NaturalScience Foundation of China (Grant Nos. 31371002 and81071223).
a)Author to whom correspondence should be addressed. Electronic mail:[email protected]; Telephone: +86-531-8839 5624; Fax: +86-531-88392863.
1B. Biswal, F. Z. Yetkin, V. M. Haughton, and J. S. Hyde, “Functional con-nectivity in the motor cortex of resting human brain using echo-planar MRI,”Magn. Reson. Med. 34, 537–541 (1995).
2J. S. Damoiseaux, S. A. Rombouts, F. Barkhof, P. Scheltens, C. J. Stam, S.M. Smith, and C. F. Beckmann, “Consistent resting-state networks acrosshealthy subjects,” Proc. Natl. Acad. Sci. U. S. A. 103, 13848–13853 (2006).
3M. De Luca, C. F. Beckmann, N. De Stefano, P. M. Matthews, and S. M.Smith, “fMRI resting state networks define distinct modes of long-distanceinteractions in the human brain,” NeuroImage 29(4), 1359–1367 (2006).
4M. D. Fox and M. E. Raichle, “Spontaneous fluctuations in brain activityobserved with functional magnetic resonance imaging,” Nat. Rev. Neurosci.8(9), 700–711 (2007).
5C. M. Lu, Y. J. Zhang, B. B. Biswal, Y. F. Zang, D. L. Peng, and C. Z. Zhu,“Use of fNIRS to assess resting state functional connectivity,” J. Neurosci.Methods 186(2), 242–249 (2010).
6B. R. White, A. Z. Snyder, A. L. Cohen, S. E. Petersen, M. E. Raichle, B.L. Schlaggar, and J. P. Culver, “Resting-state functional connectivity in thehuman brain revealed with diffuse optical tomography,” NeuroImage 47(1),148–156 (2009).
7H. Zhang, Y. Zhang, C. Lu, S. Ma, Y. Zang, and C. Zhu, “Functional connec-tivity as revealed by independent component analysis of resting-state fNIRSmeasurements,” NeuroImage 51, 1150–1161 (2010).
8S. Sasai, F. Homae, H. Watanabe, A. T. Sasaki, H. C. Tanabe, N. Sadato,and G. Taga, “A NIRS–fMRI study of resting state network,” NeuroImage63(1), 179–193 (2012).
9H. Obrig, M. Neufang, R. Wenzel, M. Kohl, J. Steinbrink, K. Einhäupl, andA. Villringer, “Spontaneous low frequency oscillations of cerebral haemo-dynamics and metabolism in human adults,” NeuroImage 12, 623–639(2000).
10R. Cheng, Y. Shang, Jr., D. Hayes, S. P. Saha, and G. Yu, “Noninvasiveoptical evaluation of spontaneous low frequency oscillations in cerebralhemodynamics,” NeuroImage 62, 1445–1454 (2012).
11M. Ferrari and V. Quaresima, “A brief review on the history of humanfunctional near-infrared spectroscopy (fNIRS) development and fields ofapplication,” NeuroImage 63(1), 921–935 (2012).
12Z. Y. Li, M. Zhang, R. Cui, Q. Xin, L. Lu, W. Zhou, Q. Han, and Y. Gao,“Wavelet coherence analysis of prefrontal oxygenation signals in elderlysubjects with hypertension,” Physiol. Meas. 35(5), 777–791 (2014).
13G. Taga, Y. Konishi, A. Maki, T. Tachibana, M. Fujiwara, and H. Koizumi,“Spontaneous oscillation of oxy-and deoxy-hemoglobin changes with aphase difference throughout the occipital cortex of newborn infants observedusing non-invasive optical topography,” Neurosci. Lett. 282(1), 101–104(2000).
14G. Taga, H. Watanabe, and F. Homae, “Spatiotemporal properties of corticalhemodynamic response to auditory stimuli in sleeping infants revealed bymulti-channel NIRS,” Philos. Trans. R. Soc., A. 369, 4495–4511 (2011).
15C. W. Wu, H. Gu, H. Lu, E. A. Stein, J. H. Chen, and Y. Yang, “Frequencyspecificity of functional connectivity in brain networks,” NeuroImage 42(3),1047–1055 (2008).
16S. Sasai, F. Homae, H. Watanabe, and G. Taga, “Frequency-specific func-tional connectivity in the brain during resting state revealed by NIRS,”NeuroImage 56, 252–257 (2011).
17A. Vermeij, A. S. Meel-van den Abeelen, R. P. Kessels, A. H. van Beek, andJ. A. Claassen, “Very-low-frequency oscillations of cerebral hemodynamicsand blood pressure are affected by aging and cognitive load,” NeuroImage15(85), 608–615 (2014).
18Z. Y. Li, Y. H. Wang, Y. Li, Y. Wang, J. P. Li, and L. L. Zhang, “Wavelet anal-ysis of cerebral oxygenation signal measured by near-infrared spectroscopyin subjects with cerebral infarction,” Microvasc. Res. 80, 142–147 (2010).
19A. R. Carter, S. V. Astafiev, C. E. Lang, L. T. Connor, J. Rengachary, M.J. Strube, D. L. Pope, G. L. Shulman, and M. Corbetta, “Resting inter-hemispheric functional magnetic resonance imaging connectivity predictsperformance after stroke,” Ann. Neurol. 67(3), 365–375 (2010).
20K. P. Westlake and S. S. Nagarajan, “Functional connectivity in relation tomotor performance and recovery after stroke,” Front. Syst. Neurosci. 5, 1–12(2011).
21T. Peng, P. N. Ainslie, J. D. Cotter, C. Murrell, K. Thomas, M. J. Williams,K. George, R. Shave, A. B. Rowley, and S. J. Payne, “The effects of age onthe spontaneous low-frequency oscillations in cerebral and systemic cardio-vascular dynamics,” Physiol. Meas. 29, 1055–1069 (2008).
22A. B. Rowley, S. J. Payne, I. Tachtsidis, M. J. Ebden, J. P. Whiteley, and D.J. Gavaghan, “Synchronization between arterial blood pressure and cerebraloxyhaemoglobin concentration investigated by wavelet cross-correlation,”Physiol. Meas. 28, 161–173 (2007).
23M. L. Schroeter, O. Schmiedel, and D. Y. Von Cramon, “Spontaneous low-frequency oscillations decline in the aging brain,” J. Cereb. Blood FlowMetab. 24, 1183–1191 (2004).
24V. Toronov, M. A. Franceschini, M. Filiaci, S. Fantini, M. Wolf, A. Michalos,and E. Gratton, “Near-infrared study of fluctuations in cerebral hemody-namics during rest and motor stimulation: Temporal analysis and spatialmapping,” Med. Phys. 27(4), 801–815 (2000).
25Z. Y. Li, M. Zhang, Q. Xin, G. Q. Chen, F. F. Liu, and J. P. Li, “Spectralanalysis of near-infrared spectroscopy signals measured from prefrontallobe in subjects at risk for stroke,” Med. Phys. 39(4), 2177–2179 (2012).
26Z. Y. Li, M. Zhang, Q. Xin, S. Luo, R. Cui, and L. Lu, “Age-related changesin spontaneous oscillations assessed by wavelet transform of cerebral oxy-genation and arterial blood pressure signals,” J. Cereb. Blood. Flow. Metab.33(5), 692–699 (2013).
27Y. Shiogai, A. Stefanovska, and P. V. E. McClintock, “Nonlinear dynamicsof cardiovascular ageing,” Phys. Rep. 488, 51–110 (2010).
28R. Zhang, J. H. Zuckerman, K. Iwasaki, T. E. Wilson, C. G. Crandall, and B.D. Levine, “Autonomic neural control of dynamic cerebral autoregulation inhumans,” Circulation 106, 1814–1820 (2002).
29T. Peng, A. B. Rowley, P. N. Ainslie, M. J. Poulin, and S. J. Payne, “Waveletphase synchronization analysis of cerebral blood flow autoregulation,” IEEETrans. Biomed. Eng. 57(4), 960–968 (2010).
30L. W. Sheppard, A. Stefanovska, and P. V. E. McClintock, “Testing fortime-localized coherence in bivariate data,” Phys. Rev. E 85(4), 046205(2012).
31M. Le Van Quyen, J. Foucher, J. P. Lachaux, E. Rodriguez, A. Lutz, J.Martinerie, and F. J. Varela, “Comparison of Hilbert transform and waveletmethods for the analysis of neuronal synchrony,” J. Neurosci. Methods111(2), 83–98 (2001).
32A. Bruns, “Fourier-, Hilbert-and wavelet-based signal analysis: Are theyreally different approaches?,” J. Neurosci. Methods 137(2), 321–332 (2004).
33L. W. Sheppard, V. Vuksanovic, P. V. E. McClintock, and A. Stefanovska,“Oscillatory dynamics of vasoconstriction and vasodilation identified bytime-localized phase coherence,” Phys. Med. Biol. 56, 3583–3601 (2011).
34A. Bandrivskyy, A. Bernjak, P. Mcclintock, and A. Stefanovska, “Waveletphase coherence analysis: Application to skin temperature and blood flow,”Cardiovasc. Eng. Int. J. 4(1), 89–93 (2004).
35A. Bernjak, A. Stefanovska, P. V. E. McClintock, P. J. Owen-Lynch, and P.B. M. Clarkson, “Coherence between fluctuations in blood flow and oxygensaturation,” Fluct. Noise Lett. 11(1), 1240013 (2012).
36P. Kvandal, L. Sheppard, S. A. Landsverk, A. Stefanovska, and K. A. Kirke-boen, “Impaired cerebrovascular reactivity after acute traumatic brain injurycan be detected by wavelet phase coherence analysis of the intracranial andarterial blood pressure signals,” J. Clin. Monit. Comput. 27(4), 375–383(2013).
37R. Cui, M. Zhang, Z. Li, Q. Xin, L. Lu, W. Zhou, Q. Han, and Y. Gao,“Wavelet coherence analysis of spontaneous oscillations in cerebral tissueoxyhemoglobin concentrations and arterial blood pressure in elderly sub-jects,” Microvasc. Res. 93, 14–20 (2014).
38W. J. Jones, L. S. Williams, A. Bruno, and J. Biller, “Hypertension andcerebrovascular disease,” Semin. Cerebrovasc. Dis. Stroke 3(3), 144–154(2003).
39I. Tachtsidis, C. E. Elwell, T. S. Leung, C. W. Lee, M. Smith, and D. T. Delpy,“Investigation of cerebral haemodynamics by near-infrared spectroscopy inyoung healthy volunteers reveals posture-dependent spontaneous oscilla-tions,” Physiol. Meas. 25, 437–445 (2004).
40Y. C. Teng, H. S. Ding, and Q. C. Gong, “Monitoring cerebral oxygen satura-tion during cardiopulmonary bypass using near-infrared spectroscopy: Therelationships with body temperature and perfusion rate,” J. Biomed. Opt.11(2), 024016 (2006).
41H. S. Ding, J. Liang, G. M. N’Guérékata, and T. J. Xiao, “Pseudo-almostperiodicity of some nonautonomous evolution equations with delay,” Non-linear Anal.: Theory, Methods Appl. 67(5), 1412–1418 (2007).
Medical Physics, Vol. 41, No. 10, October 2014

102702-8 Han et al.: Phase synchronization in elderly subjects with cerebral infarction 102702-8
42A. Stefanovska, M. Bracic, and H. D. Kvernmo, “Wavelet analysis of os-cillations in the peripheral blood circulation measured by laser Dopplertechnique,” IEEE Trans. Biomed. Eng. 46, 1230–1239 (1999).
43M. D. Papademetriou, I. Tachtsidis, M. J. Elliot, A. Hoskote, and C. E. El-well, “Multichannel near infrared spectroscopy indicates regional variationsin cerebral autoregulation in infants supported on extracorporeal membraneoxygenation,” J. Biomed. Opt. 17(6), 067008-1–067008-9 (2012).
44M. Bracic and A. Stefanovska, “Wavelet-based analysis of human blood-flow dynamics,” Bull. Math. Biol. 60(5), 919–935 (1998).
45C. A. Giller, “The frequency-dependent behavior of cerebral autoregula-tion,” Neurosurgery 27(3), 362–368 (1990).
46D. Cordes, V. M. Haughton, K. Arfanakis, J. D. Carew, P. A. Turski, C. H.Moritz, M. A. Quigley, and M. E. Meyerand, “Frequencies contributing tofunctional connectivity in the cerebral cortex in ‘resting-state’ data,” Am. J.Neuroradiol. 22, 1326–1333 (2001), PMID: 11498421.
47Z. Y. Li, M. Zhang, Q. Xin, J. Li, G. Chen, F. Liu, and J. Li, “Correlationanalysis between prefrontal oxygenation oscillations and cerebral arteryhemodynamics in humans,” Microvasc. Res. 82(3), 304–310 (2011).
48T. Takahashi, Y. Takikawa, R. Kawagoe, S. Shibuya, T. Iwano, and S. Ki-tazawa, “Influence of skin blood flow on near-infrared spectroscopy signalsmeasured on the forehead during a verbal fluency task,” NeuroImage 57(3),991–1002 (2011).
49Q. Zhang, E. N. Brown, and G. E. Strangman, “Adaptive filtering to reduceglobal interference in evoked brain activity detection: A human subject casestudy,” J. Biomed. Opt. 12, 064009 (2007).
50A. V. Medvedev, J. Kainerstorfer, S. V. Borisov, R. L. Barbour, and J. Van-Meter, “Event-related fast optical signal in a rapid object recognition task:Improving detection by the independent component analysis,” Brain Res.1236, 145–158 (2008).
51Task Force of the European Society of Cardiology and the North AmericanSociety of Pacing and Electrophysiology, “Heart rate variability: Standardsof measurement, physiological interpretation, and clinical use,” Circulation93, 1043–1065 (1996).
52P. Kvandal, S. A. Landsverk, A. Bernjak, A. Stefanovska, H. D. Kvernmo,and K. A. Kirkebøen, “Low frequency oscillations of the laser Dopplerperfusion signal in human skin,” Microvasc. Res. 72(3), 120–127 (2006).
Medical Physics, Vol. 41, No. 10, October 2014