Embed Size (px)
Citation preview

Clinical Radiology (1993) 47, 183-188
Phase III Trial of Oral Magnetic Particles in MRI of Abdomen and Pelvis D. MacVICAR, T. F. JACOBSEN*, R. GUY and J. E. HUSBAND
Cancer Research Campaign Magnetic Resonance Research Group, Royal Marsden Hospital, Sutton, Surrey, UK and *Nycomed ~s, Clinical Research and Development, Oslo, Norway
A prospective Phase III trial was performed to evaluate the efficacy in clinical practice of a new gastro-intestinal contrast agent, Oral Magnetic Particles (OMP), for use in abdominal and pelvic magnetic resonance imaging (MRI). This was an open study comprising 35 patients each given 800 ml of OMP at a concentration of 0.5 g/I. Distribution of the agent was most reliable in the small bowel. General contrast effect was satisfactory, and image quality and diagnostic confidence were enhanced. Administration of O M P increased diagnostic information in the magnetic resonance (MR) image in 50% of patients. No clinically significant adverse effects were observed. The results confirm in a clinical setting a potential role for this new contrast agent. MacVicar, D., Jacobsen, T.F., Guy, R. & Husband, J.E. (1993). Clinical Radiology 47, 183-188. Phase III Trial of Oral Magnetic Particles in MRI of Abdomen and Pelvis
Accepted for Publication 5 October 1992
While magnetic resonance (MR) imaging has become firmly established in neurology and orthopaedic practice, a number of factors have hindered progress in abdominal and pelvic imaging. Scan times on most machines remain too long to allow imaging on a single breath hold and respiratory artefacts degrade image quality. On T2- weighted (T2W) imaging, bowel fluid is of high signal, giving little contrast with surrounding fat, and may result in artefacts due to peristaltic motion. Use of T l weighting (T1W) results in better gut to fat contrast, but the signal intensity ofgastro-intestinal tract remains similar to other intra-abdominal organs. Despite introduction of fast gradient echo imaging and fat saturation sequences, a need for a bowel marking agent remains. In an attempt to improve abdominal and pelvic image quality, oral con- trast agents are being developed. Gas, water, barium, clays and oils have been used, but none have proved entirely satisfactory [1-2]. Paramagnetic agents such as Gadolinium diethylene triamine pentacetic acid (Gd- DTPA) have been used. This gastro-intestinal contrast agent produces a shortening in the T1 relaxation time, which increases signal within the bowel on T l W imaging and therefore gives positive contrast [3]. Superparamag- netic agents shorten T2 relaxation time, reduce signal within marked bowel on T2W imaging and thus result in negative contrast. Crystalline iron oxide is a prototypic example of such an agent. The mechanism of action of these ferrite particles and early clinical trials of this group of agents have been described previously [4-9].
We report a Phase III trial of Oral Magnetic Particles (OMP), an oral contrast agent composed of ferrite-type crystalline iron oxide, bound to a carrier matrix of monodisperse polymer particles. The aim of the trial was to evaluate the contrast effect of OMP, its distribution through the gastro-intestinal tract, its influence on lesion detection and diagnostic information, and its acceptabi- lity to patieffts in a clinical setting.
Correspondence to: Dr A. D. MacVicar, Department of Radiology, Royal Marsden Hospital, Downs Road, Sutton, Surrey SM2 5PT.
PATIENTS AND M E T H O D S
Patients
The trial involved 35 patients (25 male, 10 female) aged 21-81 years (mean 51.7) whose body weight ranged from 45 to 102 kg (mean 68.0 kg). The patients were referred from the practice of an oncological hospital. The diagnoses (suspected or confirmed) and indications for magnetic resonance imaging (MRI) are summarized in Tables 1 and 2. Absolute contraindications to MR imaging such as cardiac pacemakers and intracranial aneurysm clips excluded patients from the trial. The following exclusions were added: pregnancy, known positive hepatitis or human immunodeficiency virus serology, abdominal or pelvic metal implants, phenylke-
Table 1 - Patient diagnoses (suspected or confirmed) at time of scanning
Diagnosis Number of patients
Lymphoma 22 Teratoma 4 Cancer of colon 3 Cancer of prostate 3 Cancer of rectum 1 Cancer of stomach 1 Cancer of bladder 1
Table 2 - Indications for MRI with disease site
Indication Number of patients
Evaluation of nodal and abdominal masses* 29 Mesenteric 11 Retroperitoneal 11 Pelvic (below aortic bifurcation) I0 Mass excluded 4
Evaluation of local disease recurrence 6 Pelvic 5 Stomach/pancreas 1
* Some patients had more than one site of disease.

184 CLINICAL RADIOLOGY
Table 3 - Distribution of contrast in areas of alimentary tract in region of interest
Site Contrast distribution
No distribution Partial but Partial and Complete insufficient sufficient
Percen rage suJficient or complete (%)
Stomach 3 1 3 0 44 Duodenum 0 4 7 1 67 Jejunum 0 I 15 3 95 Ileum 0 1 22 8 97 Ascending Colon 0 11 17 I 64 Descending Colon 0 11 17 1 64 Trans. colon 0 I 15 0 94 Sigmoid "0 8 11 I 60 Rectum 2 7 6 1 43
tonuria and previous entry into the trial. All patients had a clinical indication for MRI, gave informed written consent and were conscious and co-operative throughout. The trial was approved by the ethical committee of the Royal Marsden Hospital and conducted in accordance with the current revision of the Helsinki declaration (1964) and the UK Good Clinical Practice guidelines (1988).
Contrast Material
The active component of OMP is ferrite-type crystal- line iron oxide particles less than 50 nm in diameter, composed of an intermediate between Fe203 and Fe304. These are coated onto monodisperse polymer resin particles approximately 3.7/zm in diameter which act as a carrier matrix.
The iron content of OMP is 20-27% by weight. The toxicology data, obtained from studies in mice and rats, have been reported previously [9]. Phase I and Phase II trials have optimized the iron concentration and common food additives have been introduced as viscosity increas- ing agents [7,8]. The OMP supplied for our study was presented as granules which were resuspended in 200 ml of water, giving a viscosity of 700 kPa.s. After a fast of 4 h, four portions of 200 ml each were given to the patient at 40 rain intervals, each portion being consumed within 3 rain of resuspension.
Imaging Technique
All patients were imaged prior to OMP administration with Tl-weighted (TR 500-700 ms, TE 17-20 ms) and double echo T2-weighted (TR 2000-2500 ms, TE 25-30/ 70-90 ms) spin echo sequences, in a Siemens Magnetom operating at 1.5 Tesla. Scan orientations were selected to enable optimal demonstration of pathology. Only the relevant region of clinical interest was scanned. Gradient echo imaging (TR 242 ms, TE 11 ms, flip angle 68 ~ was performed in one patient. Scans were repeated without alteration of protocol within 30 rain of completing ingestion of OMP. No gut relaxing agents were used.
Image Assessment
Pre- and post-contrast images were read by a single radiologist. The following criteria were considered: con- trast distribution and general contrast effect, image quality, diagnostic information and artefacts. Contrast distribution was assessed for separate regions of the gastro-intestinal tract (stomach, duodenum, jejunum,
ileum, colon, sigmoid and rectum) and distribution was graded 'none', 'partial but insufficient', 'partial but sufficient' or 'complete'. General contrast effect and image quality were graded 'insufficient', 'sufficient' or 'excellent'. Diagnostic information was categorized as more, equal or less than pre-contrast MRI. Specific questions were answered regarding the usefulness of OMP in (a) delineating the GI tract, (b) facilitating diagnosis, (c) disclosing additional findings, (d) providing increased confidence in interpretation of the scans, and (e) leading to change in diagnosis or management. Artefacts were grouped into respiratory, vascular or peristaltic and graded non-disturbing or disturbing. Images were scruti- nized for effects directly related to the contrast medium such as blurring and metallic artefacts.
Adverse Events and Patient Acceptability
Patients were asked to report any adverse events they experienced during ingestion, whether the contrast agent was pleasant or unpleasant, and if they would be prepared to take it again. They were allowed to leave the hospital 30 rain after completion of the scan and asked to report, by telephone, any untoward subsequent event. All observed or reported adverse events were recorded whether or not they were considered related to the contrast agent.
RESULTS
Pre- and post-contrast scans were available in 34 patients. One patient only took one mouthful of OMP and was not rescanned.
Contrast Distribution and General Contrast Effect
Contrast distribution is summarized in Table 3. The general contrast effect was deemed insufficient in three patients, sufficient in 23 and excellent in eight on T2W imaging, and insufficient in three, sufficient in 25 and excellent in six on T1W imaging. The contrast effect was noted to be more pronounced on T2W imaging.
Image Quali ty and Diagnostic Information
After OMP, image quality was categorized as excellent in six scans compared to one before OMP. No scans deteriorated after OMP. Two scans were of 'insufficient' quality before and after OMP. More diagnostic informa- tion was present post-OMP in 17 patients (50%), and equal information was present in 17. None of the post- OMP scans contained less diagnostic information. Re- sponses to the specific questions (a-e, methods) about the contrast agent are summarized in Table 4.

OMP IN MRI OF ABDOMEN AND PELVIS 185
Table 4 - Questions about the contrast agent (total patient no. = 34)
Questions Yes No
Improved delineation of the GI tract? 32 2 Facilitation of diagnosis o f patient? 20 14 Revelation of previously undisclosed findings? 8 26 Increased confidence in MR? 24 10 Change in diagnosis? 1 33
Peristaltic motion artefacts were seen in nine patients pre-contrast and three post-contrast. Only three patients had disturbing peristaltic artefacts pre-contrast, all of which were reduced by administration of contrast. Dis- turbing respiratory motion artefact was observed in seven patients, reduced to five on post-OMP imaging. Vascular motion artefacts were unaffected by OMP. No blurring or metallic artefacts were reported in this study. Minor susceptibility effects were observed in relation to contrast- filled gut loops but these were not clinically significant on spin echo sequences. More obvious artefact was observed on a single patient of whom gradient echo images were obtained.
Adverse Events and Patient Acceptability
Three patients were unable to ingest the entire volume, as a result of nausea, although no vomiting occurred. No other adverse effects were noted. Thirty-four patients said they would take the contrast again, 30 found the taste acceptable and five found it unpleasant or bad, one of whom refused to take more than a mouthful.
DISCUSSION
Progress in abdominal MRI has been relatively slow, this is partly due to the variety and complexity of the movement artefacts generated by respiration, cardiac motion, blood flow and peristalsis. In addition, bowel loops may mimic abdominal masses. A contrast agent should mark bowel loops, but to do this reliably it must be distributed evenly through the gastro-intestinal tract. It must not create additional artefacts, and in this respect a negative contrast agent has theoretical advantages. On T2W sequences, fluid-filled bowel loops are of high signal and this signal is propagated as part of respiratory or peristaltic artefact onto other parts of the image. OMP is intended to reduce or abolish the signal without distorting the anatomy of the bowel loops, thus enabling identifica- tion of the gut and reducing artefact. OMP has the incidental advantage of influencing signal on all pulse sequences, although the effect is maximal on T2W imaging. The fundamental purpose of the contrast agent is to increase the diagnostic information available from MRI while causing no troublesome side effects to the patient and minimal inconvenience in administration.
Our experience shows that OMP is satisfactory in most of these functions. Diagnostic information was equal in 17 patients and more information was available on the post-contrast scan in 17 patients (50%). It should be stressed that the subjective nature of this assessment is a potential source of observer bias, so it is reassuring that this figure is almost identical to that reported by Rinck et al. [9], and similar to the results of Boudghene et al. [10]. The distribution was best in small bowel and transverse colon, and least reliable in the stomach and rectosigmoid.
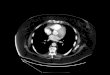
(b)
Fig. 1 (a) T2W image (SE 2300/90) of a patient with a large retroperitoneal and mesenteric mass of non-Hodgkin's lymphoma. Fluid-filled gut loops at the anterolateral margins of the mass mimic nodules of lymphoma (arrows). (b) After OMP, the gut loops are of low signal intensity on the same pulse sequence. The negative contrast effect shows the mass to be less extensive than would be deduced from the precontrast image.
It was frequently difficult to differentiate colonic gas from the contrast agent, but this did not cause any practical diagnostic problems. Administration of contrast did not deteriorate image quality on any spin echo sequence, although significant susceptibility artefact was produced on gradient echo imaging. The contrast was well tolerated and caused no serious side effects.
Although our patients did not represent a generalized cross-section of pathology our study suggests that OMP should be useful for a broad spectrum of clinical indica- tions. All patients came from the practice of an oncologi- cal hospital and were being investigated for recurrence of abdomino-pelvic tumours or evaluation of nodal disease. MRI is frequently used to assess lymphoma masses, as there is growing evidence that change in the MR signal may indicate fibrosis in tumour masses in response to treatment [11,12]. OMP was effective in clearly demon- strating loops of fluid-filled bowel which can mimic

186 CLINICAL RADIOLOGY
(a) (a)
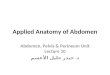
(b)
Fig. 2 - (a) Proton density image (SE 2000/23) of pelvis showing a right external iliac node involved by metastatic prostatic carcinoma. (b) Post- OMP image (SE 2000/23) with contrast marking of pelvic ileal loops increases lesion conspicuity.
mesenteric and para-aortic lymphoma masses (Fig. 1). Nodal disease in the retroperitoneum and pelvis may be difficult to assess on CT, even with intravenous contrast [13] and in this area a 'problem solving' role is developing for MRI, although CT and ultrasound remain unchal- lenged as the primary cross-sectional techniques in abdo- mino-pelvic imaging. OMP increased lesion conspicuity in the pelvis (Fig. 2) and even when lesions were clearly visible before contrast, image quality and diagnostic confidence were increased (Fig. 3). In only one patient was the diagnosis altered by administration of OMP (Fig. 4) but in our centre investigation is frequently a part of follow-up rather than initial diagnosis. In centres where a higher proportion of MRI is performed as part of a diagnostic work up, it may be anticipated that more patients will fall into the 'diagnosis altered' category.
A significant problem of conducting a trial such as this is a lack of objective criteria by which to assess contrast effect and its clinical utility. Responses to questions regarding parameters such as facilitation of diagnosis and confidence in diagnosis are inevitably subjective, espe- cially when scans are viewed by a single radiologist. However, our assessment of the contrast agent has been
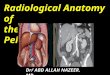
(b)
Fig. 3 - (a) T2W image (SE 2500/80) before OMP. Recurrent non- Hodgkin's lymphoma in left common iliac nodes (arrow) medial to psoas. (b) After OMP, the gut in the upper pelvis is clearly marked. Image quality is improved, although the diagnostic information was present pre-contrast.
broadly similar to those at nine other centres conducting Phase III trials of OMP in Europe [14].
A drawback of OMP administration identified during the trial was the difficulty in obtaining satisfactory gradient echo images of the abdomen after contrast in one patient. The field inhomogeneities caused by OMP led to disturbing susceptibility artefacts in one patient (Fig. 5). It may be necessary to adjust the way in which OMP is applied with the fast and ultrafast sequences now being developed, although it has been reported that shortening echo times may reduce the artefact caused by OMP on gradient echo images [15]. Our experience of a single patient, scanned on an 'ad hoc' basis, does not imply that OMP prevents the use of gradient echo sequences, but does indicate that further investigation will be useful to optimize pulse sequence selection. Also, the consumption of OMP takes 2 h, which caused some inconvenience to staff and patients. Further trials may help to demonstrate whether the timing of contrast ingestion couldbe short- ened, or if it could be consumed by the patient at home or on the ward. Rectal administration of OMP is of potential utility, but as yet has not been formally assessed.

OMP IN MRI OF ABDOMEN AND PELVIS 187
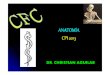
(a) (a)
(b) Fig. 4 - (a) Proton density (SE 2000/25) image at level of pancreatic head. A partial gastrectomy had been performed previously for stomach carcinoma, with a 'roux en Y' procedure. The patient presented with jaundice and pre-contrast MRI appeared to show a recurrent mass (arrows). (b) Post-contrast image (SE 2000/25) shows the roux loop of duodenum marked by OMP (arrows), demonstrating that the suspected mass is duodenum and pancreatic head. The jaundice was caused by a common bile duct calculus.
Despite these factors, OMP shows considerable pro- mise as a gastro-intestinal contrast agent for MRI of the abdomen and pelvis. OMP yielded more diagnostic information in 50% of patients, increasing confidence in diagnosis and decreasing artefact while being safe and well tolerated by patients.
Acknowledgements. The authors wish to thank Pauline Kennedy, Janet MacDonald and Jackie Seckel for help in preparation of the manuscript, and the Cancer Research Campaign and the Daniel Marks Fund for continuing financial support.
REFERENCES
1 Weinreb JC, Maravilla KR, Redman HC, Nunnally R. Improved MR imaging of the upper abdomen with glucagon and gas. Journal of ComputeroAssisted Tomography 1985;8:835-838.
2 Li KCP, Tart RP, Storm B. Rolfes P, Ang P, Ros PR. MR oral contrast agents: comparative study with five agents in humans [abstract]. In: Society of Magnetic Resonance in Medicine, 1989, Vol. 2, Berkeley, CA: Society of Magnetic Resonance in Medicine, 1989:791.
(b)
Fig. 5 - (a) Post-OMP T2W image (SE 2500/80) of a patient with a para- aortic and mesenteric lymphoma mass. (b) Post-OMP gradient echo sequence (TR 242 ms/TE 11 ms, flip angle 68~ The contrast agent causes inhomogeneity in the local magnetic field. Magnetic susceptibi- lity effects result in signal voids around marked gut which obscure diagnostic detail.
3 Lainado M, Kornmesser W, Hamm B, Clauss W, Weinmann H J, Felix R. MR imaging of the gastrointestinal tract: value of Gd DTPA. American Journal of Roentgenology 1988; 150:817-821.
4 Craik DJ. Magnetic oxides. New York: Wiley, 1975. 5 Hahn PF, Stark DD, Saini S, Lewis JM, Wittenberg J, Ferrucci JT.
Ferrite particles for bowel contrast in MR imaging: Design issues and feasibility studies. Radiology 1987; 164:3741.
6 Lonnemark M, Hemmingson A, Carlsten J, Ericsson A, Holtz F, Klaveness J. Superparamagnetic particles as an MRI contrast agent for the gastrointestinal tract. Acta Radiologica (Diagnosis) 1989;29:599-602.
7 Hahn PF, Stark DD, Lewis JM, Saini S, Elizondo G, Weissleder R et al. First clinical trial of a new superparamagnetic iron oxide for use as an oral gastrointestinal contrast agent in MR imaging. Radiology 1990; 175:695-700.
8 Lonnemark M, Hemmingson A, Ericsson A, Gundersen HG, Bach- Gansmo T. Oral magnetic particles for magnetic resonance imaging. Effect in plain and viscous aqueous suspension. Acta Radiologica (Diagnosis) 1991;31:303 307.
9 Rinck PA, Smevik O, Nilsen G, Klepp O, Onsrud M, Oksendal Aet al. Oral magnetic particles in MR imaging of the abdomen and pelvis. Radiology 1991;178:775-779.
10 Boudghene F, Faintuch JM, Wallays C, Bach-Gansmo T, Lam- brechts M, Bigot JM. Superparamagnetic particles as oral gastro-

188 CLINICAL RADIOLOGY
intestinal contrast agent in MRI of the abdomen (abstract). European Radiology 1991;1 (suppl.):216.
11 Glazer HS, Lee JKT, Levitt RG, Heiken J, Ling D, Totty WG et al. Radiation fibrosis from recurrent tumour by MR imaging. Radio- logy 1985;156:721-726.
12 Nyman RS, Rehn SM, Glimelius BLG, Hagberg HE, Hemmingsson AL, Sundstrom CJ. Residual mediastinal masses in Hodgkin Disease: prediction of size with MR imaging. Radiology 1989; 170:435-440.
13 Husband JE, Robinson L, Thomas G. Contrast enhancing lymph
nodes in bladder cancer. A potential pitfall in CT. Clinical Radiology 1992;45:395-398.
14 Jacobsen TF, Bach-Gansmo T, Borseth A, Haugen I, Lunby B, Fvaland Met al. Oral magnetic particles (OMP) as an oral contrast agent for abdominal and pelvic MRI. Results from clinical trials (abstract). European Radiology 1991;1 (suppl):216.
15 Rummeny E, Stoeber U, Wiessmann W, Unbehaun B, Vassalo P, Jacobsen TF et al. Value of gradient echo pulse sequences for Oral Magnetic Particle enhanced MR imaging of abdominal tumours (abstract). Radiology 1991;181 (suppl.):94.