Embed Size (px)
Citation preview

Int. J. Radiation Oncology Biol. Phys., Vol. 78, No. 5, pp. 1407–1412, 2010Copyright � 2010 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$–see front matter
jrobp.2009.10.012
doi:10.1016/j.iCLINICAL INVESTIGATION Esophagus
PHASE II STUDY OF CONCURRENT CHEMORADIATION IN COMBINATION WITHERLOTINIB FOR LOCALLY ADVANCED ESOPHAGEAL CARCINOMA
GANG LI, M.D.,* WEI HU, M.D.,y JIANHUA WANG, M.D.,y XIA DENG, M.D.,* PING ZHANG, M.D.,*
XUEBANG ZHANG, M.D.,* CONGYIN XIE, M.D.,* AND SHIXIU WU, M.D.*
*Department of Radiation Oncology, The first affiliated hospital of Wenzhou Medical College, WenZhou, ZheJiang, People’s Republicof China; and yDepartment of Radiation Oncology, Taizhou Hospital, Wenzhou Medical College, Taizhou, Zhejiang, People’s Republic
of China
ReprinMedical Cince, P.R88069372
Purpose: To investigate the feasibility and efficacy of concurrent chemoradiation in combination with erlotinib forlocally advanced esophageal carcinoma.Methods and Materials: Twenty-four patients with locally advanced esophageal carcinoma were treated with con-current chemoradiotherapy. A daily fraction of 2.0 Gy was prescribed to a total dose of 60 Gy over 6 weeks. Con-current paclitaxel (135 mg/m2, d1) and cisplatin (20 mg/m2, d1-3) were administered on Day 1 and Day 29 of theradiotherapy. Erlotinib, an oral epidermal growth factor receptor–tyrosine kinase inhibitor, was taken by everypatient at the dose of 150 mg daily during the chemoradiotherapy.Results: The median follow-up of the 24 patients was 18.6 months (range, 7.1–29.6 months). The 2-year overallsurvival, local-regional control, and relapse-free survival were 70.1% (95% CI, 50.4–90%), 87.5% (95% CI,73.5–100%), and 57.4% (95% CI, 36.3–78.7%), respectively. During the chemoradiotheapy, the incidences of acutetoxicities of Grade 3 or greater, such as leucopenia and thrombocytopenia, were 16.7 % (4/24) and 8.3% (2/24).Conclusions: Application of concurrent chemoradiotherapy in combination with erlotinib for locally advancedesophageal carcinoma yielded satisfactory 2-year overall survival and local-regional control. The toxicities werewell tolerated. � 2010 Elsevier Inc.
Chemoradiation, Esophageal carcinoma, EGFR inhibition, Radiosensitization.
INTRODUCTION
Esophageal carcinoma is the sixth most common cause of
cancer-related death, and 462,000 new cases were diagnosed
during 2002 (1, 2). However, the optimal treatment approach
for esophageal carcinoma still needs to be elucidated. Surgery
is the cornerstone in treatment for esophageal carcinoma. Data
fromtwocontemporary randomizedstudies indicatedamedian
survival ranged from 13.6 to 16 months and 2-year survival of
34% to 37% (3, 4). In these two trials, nearly half of the patients
could not achieve R0 resection. After resection alone, approx-
imately 58% of patients experienced local-regional recur-
rence. It is unknown whether surgery after neoadjuvant
chemoradiation is of benefit, although improvement in
survival was reported in several series (5, 6).
Concurrent chemoradiation has been widely recognized as
a viable option for locally advanced esophageal carcinoma.
The Radiation Therapy Oncology Group (RTOG) 8501 trial
showed that concurrent chemoradiation is superior to radiation
alone as primary therapy (7). The combination of radiotherapy
t requests to: Shixiu Wu, M.D., First hospital,Wenzhouollege, No.2 Fuxue Lane, WenZhou City, ZheJiang prov-
.China, 325000. Tel: +86-577-88069372; Fax: +86-577-; E-mail: [email protected]
1407
and concurrent chemotherapy with cisplatin and fluorouracil
has led to a long-term survival rate of approximately 25%,
an outcome similar to that associated with surgery alone.
The patterns of failure observed after definitive chemoradia-
tion showed that local-regional control is poor, with approxi-
mately 52% patients in the RTOG 8501 study experiencing
local failure. Local-regional recurrence of cancer after surgery
or radiotherapy alone remains a common problem.
The epidermal growth factor receptor (EGFR) is a member
of the erb-B family of receptors with intrinsic tyrosine kinase
activity. The EGFR is activated on binding of ligand to its
extracellular domain, resulting in autophosphorylation and
activation of downstream molecules, such as Ras, ErK,
PI3K, and Akt. In tumorigenesis EGFR plays an important
role in that it promotes growth of cells and is highly expressed
in a variety of solid tumors, with overexpression observed in
29% to 90% of esophageal cancers, which may be correlated
with poor prognosis and inferior response to therapy (8).
Oral tyrosine kinase inhibitors (TKIs) compete with adenosine
triphosphate for binding to the receptors of tyrosine kinase
Presented in part at the 44th American Society of Clinical Oncol-ogy Annual Meeting, May 30–June 3, 2008, Chicago, IL.
Conflict of interest: none.Received March 26, 2009, and in revised form Sept 10, 2009.
Accepted for publication Oct 7, 2009.

1408 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 5, 2010
domain, inhibit the enzyme’s ability to autophosphorylate, and
block the receptor-dependent signaling cascade (9).
Early preclinical work showed that radiation-induced EGFR
phosphorylation and tumor proliferation could be effectively
blocked by the addition of an EGFR-signaling inhibitor (10).
Further work in cell culture and xenograft models showed the
capacity of EGFR inhibition to enhance radiation response in
several tumor types (11). Bonner et al. demonstrated that radio-
therapy plus cetuximab improved median and overall survival
and significantly enhanced local tumor control in squamous-
cell carcinoma of the head and neck (12). Dobelbower et al.reported safety and tolerability of erlotinib delivered at
150 mg/day with concurrent 5-FU, cisplatin, and thoracic
radiation in a Phase I study of esophageal carcinoma (13).
Currently, preclinical and limited clinical data suggest that
there may be significant potential for epidermal receptor
inhibitors to enhance the effectiveness of radiation. The
EGFR inhibitors are among the most promising molecular
targeting agents in combination with radiotherapy. The
potential advantage of EGFR-TKIs includes ease of adminis-
tration and no issues with infusion reactions. The aim of our
study was to evaluate the feasibility and efficacy of erlotinib
added to concurrent chemoradiation in patients with locally
advanced esophageal squamous cell carcinoma.
METHODS AND MATERIALS
PatientsTwenty-four patients with squamous cell carcinoma of the esoph-
agus between January 1, 2007, and October 31, 2008, were enrolled
in this trial. All patients had pathologically confirmed esophageal
squamous cell carcinoma. The 24 patients were staged according
to the International Union Against Cancer (UICC, 2002)TNM stage
criteria. Patients were clinically staged T1–4 Nx, M0–1a excluding
patients with a tracheoesophageal fistula.
Pre-entry computed tomography (CT) of the thorax and abdomen
with transesophageal ultrasound (EUS) was required for accurate
staging. Patients were to be of $18 years of age with a Karnofsky
Performance Status $60. White blood cell counts had to be
$3,000/mm, platelet counts $100,000/mm, hemoglobin $10 g%,
serum creatinine at or less than the institutional upper limit of
normal, and/or creatinine clearance $50 cc/min.
Bronchoscopy was required for patients with T3 or T4 lesions near
the carina, to exclude tracheoesophageal fistula. Patients must not
have had a second malignancy, other than curable nonmelanoma
skin cancer or cervical cancer in situ, unless they were disease free
for $5 years. No prior chest radiation or chemotherapy was allowed.
Informed consent was signed before enrollment. This study and col-
lateral translational research were approved by the institutional re-
view board at the first hospital of Wenzhou Medical College.
ChemotherapyPaclitaxel 135 mg/m2 was administered intravenously over
3 hours on Day 1 and Day 29 with standard premedications. Cis-
platin 20 mg/m2 was administered as an i.v. infusion on Days 1,
2, and 3 and Days 29, 30, and 31. Chemotherapy was given concur-
rently with radiation for two cycles. The drug dosage was adjusted
according to the acute toxicities occurring in the first cycle. Erlotinib
was administrated at the beginning of chemoradiation with 150 mg/
d from Day 1 to Day 42.
RadiotherapyRadiotherapy started on the first day of the first cycle of chemo-
therapy; 6 MV of X-ray energy was used. Before the start of the
irradiation, a planning CT scan was made from the cricoid to L1
vertebra with a slice thickness of 5 mm, with the patient in treatment
position. The gross tumor volume (GTV) was defined as the primary
tumor and any enlarged regional lymph nodes as defined by transe-
sophageal ultrasound, esophagram, or CT scan (whichever was
larger). The planning target volume (PTV) provided a 2-cm radial
margin and a proximal and distal margin of 5 cm around the
GTV. A barium swallow was obtained at the time of simulation to
confirm the location of the esophagus. If the primary tumor was
above the carina (proximal esophagus), the supraclavicular nodes
were included in the initial field (40 Gy). If the primary was in the
lower third of the esophagus, the celiac nodes were included in
the initial field (40 Gy). Initially 40 Gy (20 fractions at 2 Gy per frac-
tion) was given in the anteroposterior fields over 4 weeks. A 20-Gy
boost was then delivered through parallel opposed lateral or oblique
portals. However, the superior and inferior fields were decreased to
2 cm beyond the tumor. The maximum dose to the spinal cord was
limited to 40 to 45 Gy. A total of 60 Gy of radiation delivered over
30 fractions in 6 weeks. The prescription dose was specified at the
International Commissions of Radiation Units and Measurements
(ICRU) 50/62 reference point. The daily prescription dose was
2 Gy at the ICRU reference point, and the 95% isodose had to
encompass the entire planning target volume (PTV). For the upper
thoracic and cervical esophageal carcinoma, a three-dimensional
conformal radiation technique was adopted in the boost phase.
Follow-UpAll of the patients were monitored weekly during the treatment
for acute treatment toxicity. At completion of treatment, patients
underwent CT, endoscopy, and biopsy to evaluate response to treat-
ment. The follow-up was carried out at 3-monthly intervals in the
first 2 years and at 6-monthly interval after 2 years.
Evaluation of early treatment efficacyPatients were required to have bidimensionally measurable or
assessable disease. Bidimensionally measurable disease was defined
as tumor masses that could be evaluated by radiography, CT, or
physical examination in which two perpendicular dimensions could
be obtained and monitored serially. A complete response required
disappearance of all evidence of tumor, and for patients with the pri-
mary tumor in place, endoscopic confirmation of a complete
response with normal endoscopic biopsy specimens or brushings
was required. A partial response was defined as a greater than
50% reduction in the sum of the products of the longest perpendic-
ular diameters of indicator lesions. A minor response was defined as
a greater than 25% but less than 50% reduction in measurable tumor
area. Assessable disease was defined as radiographically distinct,
unidimensional tumor that could be evaluated serially by radio-
graphic studies (i.e., the primary tumor evaluated by double-contrast
barium esophagram). Response in assessable disease was defined as
a more than 50% improvement in unidimensional disease as
determined by at least 2 observers (14).
Statistical analysisAll of the statistical analyses were performed using SPSS version
10.0 software (SPSS Inc., Chicago, IL). Toxicity was graded using
the National Cancer Institute Common Toxicity Criteria 3.0. Overall
survival was determined as the time (in months) between the first
day of therapy and the date of death.

Table 1. Patient characteristics
Characteristic n %
Age (y)$60 13 54.2<60 11 45.8
PathologySquamous 24 100Adenocarcinoma 0 0
Primary tumorCervical 1 4.2Upper thoracic 8 33.3Middle thoracic 12 50Lower thoracic 3 12.5
TNM classificationStage I–II 7 29.2Stage III–IV 17 70.8
Pretreatment weight lossNormal 15 62.5<10% 7 29.2>10% 2 8.3
Chemoradiotherapy plus Erlotinib for esophageal carcinoma d G. LI et al. 1409
Local-regional control survival was calculated as the time (in
months) from the date of therapy to the date of local-regional recur-
rence as the first site of recurrence (radiologic or pathologic). Overall
survival, local-regional control survival, and relapse-free survival
were calculated using the Kaplan-Meier method (15), and patients
of different stages were compared with the log-rank test. Our previ-
ous study indicated the incidence of persistent disease was 35.7% in
101 patients of esophageal cancer treated by radiotherapy with con-
current chemotherapy containing paclitaxel and cisplatin (16). When
the same chemoradiotherapy regimen was added with erlotinib we
hope the incidence of persistent disease can be decreased to 10%.
The statistical design was intended to allow us to detect a response
percentage of at least 20%, it was calculated that a sample size of
24 patients was needed.The primary end point of this study was lo-
cal-regional control survival and overall survival. The secondary ob-
jectives included response rate, toxicit,y and tolerability.
RESULTS
Patient characteristicsTwenty-four patients were enrolled, with a median age of
61 years (range, 40–72 years) and median Karnofsky Perfor-
mance Status of 90 (range, 80–90). One patient had T2, 17
had T3, and 6 had T4 disease diagnosed by EUS with refer-
ence of CT and MRI scans. Sixteen patients had N0, 8 had
N1, and 8 had M1a. One patient’s lesion was in cervical,
8 in upper, 12 in mid, and 3 in lower locations. Among these
24 patients, 7 had pretreatment weight loss of less than 10%,
and 2 of more than 10% (Table 1).
ToxicitiesIn all, 83% (20/24) of patients completed both cycles of
chemotherapy. In the first cycle of chemotherapy, 4 patients
had Grade 3 or greater leucopenia. The second cycle of che-
motherapy was held in 3 patients for severe depression of
bone marrow function and impairment of liver function.
The other patient required dose reduction by 25% in the
second cycle of chemotherapy for hematological toxicities.
All patients completed radiation on schedule except
1 patient who had a radiation delay for 7 days. Acute esoph-
agitis in Grade 1, Grade 2, and Grade 3 occurred in 9, 10, and
5 patients, respectively. Among the 24 patients, 54.2% (13/
24) had acute tracheitis with 12 in Grade 1 and 1 patient in
Grade 2, and none had acute tracheitis of Grade 3 or more.
During the chemoradiation, 21 patients developed skin rash
on the face and chest, with 1 patient in Grade 3, 8 in Grade
2, and 12 in Grade 1. The other 3 patients had no rash until
the end of chemoradiotherapy (Table 2).
Treatment resultsThe last date of follow-up was August 31, 2009. The median
follow-up of the 24 patients was 18.7 months (range, 7.1–29.6
months). Of the 24 patients, 11 (45.8%) attained a partial re-
sponse, and 11 (45.8%) attained a complete response as con-
firmed by chest CT scan and barium swallow. All patients
underwent upper endoscopy and biopsy. Two patients (8.3%)
had persistent disease after completion of chemoradiotherapy.
Until the date of analysis, 8 patients had distant recurrence,
1 in the bone, 3 in the liver, and 4 in lung. Among them,
1 patient also experienced failure at the site of the original le-
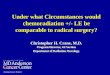
sion. Kaplan-Meier analysis showed that 2-year local-regional
control in the 24 patients was 87.5% (95% CI, 73.5–100%)
(Fig. 1), and the 2-year disease-free survival was 57.4%
(95% CI, 36.2–78.7%). At the time of analysis, 7 patients
had died. One patient, who had persistent disease at the comple-
tion of chemoradiothrepy, died of hemorrhage of esophagus,
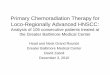
and the other 6 patients died of tumor recurrence. The 2-year
survival was calculated as 70.1% (95% CI, 50.4–90 %) (Fig. 2).
DISCUSSION
Radiotherapy or chemoradiotherapy, in combination with
target therapy, had been tried in limited fashion. The intro-
duction of targeted agents against the EGFR pathway has
been shown to improve overall survival in locally advanced
head and neck carcinomas. The results of the first randomized
clinical Phase III trial on simultaneous fractionated irradia-
tion and EGFR inhibition by the monoclonal antibody
(mAb) cetuximab (Erbitux) were promising. The landmark
study demonstrated the application of cetuximab during
primary radiotherapy of patients with head and neck squa-
mous cell carcinoma led to a significant improvement of local
tumor control and survival compared with radiotherapy
alone. The median survival was 28 months for the radiation
alone vs. 54 months for the cohort receiving cetuximab.
Three-year overall survival was also significantly improved
by the addition of cetuximab (44 vs. 57%, respectively).
The treatment was well tolerated with minimal enhancement
in the toxicity profile associated with radiotherapy. However,
it is notable that the addition of cetuximab to radiation ther-
apy had not reduced the risk of distant metastases compared
to radiotherapy alone (12). These data support the incorpora-
tion of chemotherapy into radiotherapy plus target therapy
when applied in locally advanced esophageal carcinoma,
which will facilitate further decrease of distant metastases.
Pfister et al. tested it in a Phase II trial. The results observed
that addition of cetuximab to cisplatin-based

Table 2. Acute toxicities during chemoradiation
Grade 0 1 2 3 4
Leucopenia 0 5 (20.8%) 15 (62.5%) 4 (16.7%) 0Hemoglobin 16 (66.7%) 5 (20.8%) 3 (12.5%) 0 0Platelets 17 (70.8%) 4 (16.7%) 1 (4.2%) 2 (8.3%) 0Vomiting 0 17 (70.8%) 7 (29.2%) 0 0Alopecia 3 (12.5%) 7 (29.2%) 14 (58.3%) 0 0Esophagitis 0 9 (37.5%) 10 (41.2%) 5 (20.8%) 0Tracheitis 11 (45.8%) 12 (50.0%) 1 (4.2%) 0 0Skin rash 3 (12.5%) 12 (50.0%) 8 (33.3%) 1 (4.2%) 0
1410 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 5, 2010
radiochemotherpy in head and neck carcinoma patients
achieved promising overall survival rates of 76% and local
tumor control rates of 71% after 3 years (17). However, it
cannot be taken for granted that addition of EGFR inhibitors
to combined chemoradiotherapy will necessarily further im-
prove treatment outcomes. A Phase I/II trial on neoadjuvant
radiochemotherapy with capecitabine/oxaliplatin combined
with cetuximab in patients with rectal carcinoma showed
complete tumor response rates of only 9% in the pathohisto-
logical specimens, which was less than in historical data on
radiochemotherapy without cetuximab (18).
Our data showed the addition of erlotinib to radiation with
concurrent chemotherapy containing paclitaxel and cisplatin
was effective in locally advanced esophageal carcinoma.
Although most of patients were in Stage III to IV, the
2-year overall survival and 2-year disease-free survival
were 70.1% and 57.4%, respectively. The clinical outcomes
were comparable to latest results of surgical series (3). In con-
trast to the results of the RTOG 8501 study (7), the 2-year
local control in our series was excellent, reaching 87.5%.
Our previous study indicated the incidence of persistent
disease was 35.7% in 101 patients of esophageal carcinoma
treated by radiotherapy with concurrent chemotherapy con-
taining paclitaxel and cisplatin. Although it is sometimes mis-
Fig. 1. Kaplan-Meier plots of local-regional control survival rate of24 patients with esophageal squamous cell carcinoma.
leading in the assessment of the presence of residual
carcinoma, the incidence of persistent disease significantly
decreased from 35.7% to the present 8.3% as evaluated by en-
doscopic biopsy in combination with fluorography (16). The
protocol design, including radiation dose, field arrangements,
and chemotherapy regimen, was as same as in our present trial
except for the addition of erlotinib. The results suggested that
erlotinib in addition to chemoradiation may significantly en-
hance the local control in esophageal carcinoma.
With the addition of synchronous chemotherapy to radio-
therapy, acute treatment-related toxicity is significantly
increased. In the RTOG 8501 trial (7), 29% of patients ran-
domized to the chemoradiation arm experienced Grade 3 or
4 toxicity, primarily with esophagitis, myelosuppression,
and pneumonitis. The profile of acute toxicity during concur-
rent erlotinib and chemoradiotherapy was consistent with
that reported in our previous chemoradiotherapy trials (16).
The most frequent Grade 3 to 4 toxicities in the regimen
were leucopenia, esophagitis, and skin rash. The incidences
of leucopenia and thrombocytopenia of Grade 3 or more
were 16.7% (4/24) and 8.3% (2/24), respectively. The pa-
tients tolerated the treatment well. Erlotinib does not seem
to increase chemoradiotherapy-induced acute toxicities, in-
cluding mucositis and skin reactions. However the effect of
Fig. 2. Kaplan-Meier plots of overall survival rate of 24 patientswith esophageal squamous cell carcinoma.

Chemoradiotherapy plus Erlotinib for esophageal carcinoma d G. LI et al. 1411
erlotinib combined with cisplatin and concurrent radiother-
apy in locally advanced head-and-neck carcinomas was re-
ported in a Phase II study with a high incidence (45%) of
Grade 3 to 4 in-field dermatitis (19). An interim analysis of
the Tarceva Lung Cancer Survival Treatment(TRUST) study
for patients with advanced non–small-cell lung cancer
showed that of 4,965 patients for whom safety data were
available, erlotinib-related rash was observed in 70% of pa-
tients, and 16% of these cases were Grade 3 or 4. Although
erlotinib-related rash was observed in 82% of patients in
a Chinese series, only 10% of these cases were Grade 3 or
4 (20). A retrospective case-control study has compared ge-
fitinib vs. platinum-containing doublet chemotherapy as
a first-line treatment in clinically selected non-small cell
lung cancer(NSCLC) patients (Stage IIIB or IV adenocarci-
noma) in China. The most commonly recorded adverse event
in the gefitinib arm was rash or acne (9.1%), which was lower
than in other gefitinib studies recruiting patients of different
origins: 49.4% in an Iressa Non-Small Cell Lung Cancer
Trial Evaluating Responses & Survival against Taxotere(IN-
TEREST) study, 37.0% in an IRESSA Survival Evaluation
in Lung Cancer (ISEL) study, and even 66.1% in an IRESSA
Pan-ASia Study (IPASS) in Asia (21). Rudin et al. conducted
a prospective study of 80 patients with lung, head and neck,
and ovarian cancer receiving standard dose (150 mg daily) er-
lotinib to assess the pharmacogenomic and pharmacokinetic
determinants of skin rash and diarrhea, the two major adverse
reactions associated with erlotinib. The results demonstrated
that some gene polymorphisms may be involved in the mech-
anism underlying development of skin rashes. The genotype
of these genes may affect the incidence of skin rashes among
patients of different racial/ethnic backgrounds (22).
The EGFR is overexpressed in approximately 80% of
esophageal carcinoma (23). Studies have also shown overex-
pression of EGFR in up to 88% of lymph node metastases
(24). Overexpression of EGFR has been correlated with
poor prognosis in esophageal carcinoma patients (25–29);
however, not all studies have found such a connection (30).
In NSCLC, there is strong evidence supporting the presence
of mutations in the catalytic domain of EGFR with sensitivity
to EGFR-directed therapy. The finding that EGFR kinase do-
main mutations were not detected in esophageal squmaous
cell carcinoma may be a result of the low frequency of
EGFR mutations detected in tumors other than NSCLC. In
this setting we did not consider it necessary to detect expres-
sion or mutation of EGFR in enrollment of patients. Cis-
platin-based concurrent chemoradiotherapy was the
standard regimen as established in the RTOG 8501 trial
(7). Paclitaxel had significant antineoplastic activity in the
treatment of advanced, unresectable esophageal carcinoma
(31). Response rates of up to 100% have been reported for
paclitaxel-based combination chemotherapy regimens (32,
33). Paclitaxel was prescribed in weekly regimen instead of
in full dose in most of studies of concurrent radiochemother-
apy (34, 35). The toxicities were of major concern. However,
the efficacy of weekly vs. full-dose regimen had never been
compared. Chemoradiotherapy with low-dose weekly carbo-
platin and paclitaxel, as widely adopted, may not be optimal
and may be inferior to regimens using systemic doses of che-
motherapy. The results of concurrent chemoradiotherapy con-
taining full doses of paclitaxel in esophageal carcinoma were
encouraging (16). We found that toxicities associated with
therapy were significant but manageable. The rationale for
the choice of a full dose of paclitaxel was based on the follow-
ing: first, it is helpful for maintaining adequate systemic cyto-
toxic effect compared to weekly dosage; and second, daily oral
erlotinib can result in a better radiosensitization effect.
Given promising results in NSCLC, single-agent TKIs
have been studied in several different pretreated carcinoma
types, including esophageal carcinoma. Tew et al. demon-
strated a disease control rate of 54.5% (partial response
(PR), 9%; stable disease(SD), 45.5%) with erlotinib in a 22-
patient cohort with metastatic, pretreated esophageal squa-
mous cell carcinoma or adenocarcinoma. Both patients with
PRs had squamous cell histology and EGFR overexpression
(36). Ferry et al. reported on a Phase II trial of gefitinib in ad-
vanced adenocarcinoma of the esophagus, revealing that gefi-
tinib is an active treatment with a disease control rate (PR or
SD) of 58% (37).There was no correlation found between re-
sponse to gefitinib and the level of EGFR expression (38).
These studies described similar modest response rates with ei-
ther erlotonib or gefitinib in esophageal squamous cell carci-
noma. The TKIs were well tolerated, with the most common
side effects being Grade 1 to 2 (skin rash and diarrhea). De-
spite the relatively poor activity in esophageal carcinoma
treated by TKIs alone, EGFR inhibitors have demonstrated ra-
diosensitizing effects in head and neck carcinomas, suggest-
ing that these may interact with intracellular pathways in
ways that are significant only in the context of concurrent ad-
ministration of radiotherapy.
CONCLUSION
Chemoradiotherapy in combination with erlotinib can be
safely delivered in esophageal carcinoma. It has potential
to enhance local control and to improve 2-year overall sur-
vival in esophageal carcinoma. The toxicities associated
with therapy, although manageable, were significant.
REFERENCES
1. Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74–108.
2. Devesa SS, Blot WJ, Fraumeni JF, Jr. Changing patterns in theincidence of esophageal and gastric carcinoma in the UnitedStates. Cancer 1998;83:2049–2053.
3. Fok M, Sham JS, Choy D, et al. Postoperative radiotherapy forcarcinoma of the esophagus: A prospective, randomized con-trolled study. Surgery 1993;113:138–147.
4. Medical Research Council Oesophageal Cancer WorkingGroup. Surgical resection with or without preoperative

1412 I. J. Radiation Oncology d Biology d Physics Volume 78, Number 5, 2010
chemotherapy in oesophageal cancer: A randomized controlledtrial. Lancet 2002;359:1727–1733.
5. Walsh TN, Noonan N, Hollywood D, et al. A comparison ofmultimodal therapy and surgery for esophageal adenocarci-noma. N Engl J Med 1996;335:462–467.
6. Bosset JF, Gignoux M, Triboulet JP, et al. Chemoradiotherapy fol-lowed by surgery compared with surgery alone in squamous-cellcarcinoma of the esophagus. N Engl J Med 1997;337:161–167.
7. Cooper JS, Matthew D, Herskovic Arnold, et al. Chemoradio-therapy of locally advanced esophageal cancer: Long-termfollow-up of a prospecitve randomized trial (RTOG 85-01).J Am Med Assoc 1999;281:1623–1627.
8. Kuwano H, Kato H, Miyazaki T, et al. Genetic alterations inesophageal cancer. Surg Today 2005;35:7–18.
9. Herbst RS, Fukuoka M, Baselga J. Gefitinib—a novel targetedapproach to treating cancer. Natl Rev Cancer 2004;4:956–965.
10. Balaban N, Moni J, Shannon M, et al. The effect of ionizingradiation on signal transduction: Antibodies to EGF receptorsensitize A431 cells to radiation. Biochim Biophys Acta 1996;1314:147–156.
11. Chinnaiyan P, Huang S, Vallabhaneni G, et al. Mechanisms ofenhanced radiation response following epidermal growth factorreceptor signaling inhibition by erlotinib (Erlotinib). CancerRes 2005;65:3328–3335.
12. Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetux-imab for squamous-cell carcinoma of the head and neck. N EnglJ Med 2006;354:567–578.
13. Dobelbower MC, Russo SM, Raisch KP, et al. Epidermalgrowth factor receptor tyrosine kinase inhibitor, erlotinib, andconcurrent 5-fluorouracil, cisplatin and radiotherapy for patientswith esophageal cancer: A phase I study. Anti-Cancer Drugs2006;17:95–102.
14. Ilson DH, Saltz L, Enzinger P, et al. Phase II trial of weeklyirinotecan plus cisplatin in advanced esophageal cancer.J Clin Oncol 1999;17:3270–3275.
15. Kaplan EL, Meier P. Nonparametric estimation of incompleteobservations. J Am Stat Assoc 1958;53:457–481.
16. Zhang P, Xie CY, Wu SX, et al. Concurrent chemoradiationwith paclitaxel and platinum for locally advanced esophagealcancer. Zhonghua Zhong Liu Za Zhi 2007;29:773–777.
17. Pfister DG, Su YB, Kraus DH, et al. Concurrent cetuximab,cisplatin, and concomitant boost radiotherapy for locoregion-ally advanced, squamous cell head and neck cancer: A pilotphase II study of a new combined-modality paradigm. J ClinOncol 2006;24:1072–1078.
18. Rodel C, Grabenbauer GG, Papadopoulos T, et al. Phase I/IItrial of capecitabine, oxaliplatin, and radiation for rectal cancer.J Clin Oncol 2003;21:3098–3104.
19. Herchenhorn D, Dias FL, Pineda RM, et al. Phase II study oferlotinib combined with cisplatin and radiotherapy for locallyadvanced squamous cell carcinoma of the head and neck(SCCHN) [Abstract]. J Clin Oncol 2007;25(Suppl 18): S307.
20. Ardizzoni A, Evangelia R, Mikhail L, et al. Interim safetyresults from TRUST, a global open-label study of erlotinib inpatients with advanced non-small-cell lung cancer (NSCLC)[Abstract]. J Thorac Oncol 2007;2: S342.
21. Xu Y, Zhou Y, Huang M, et al. Gefitinib versus platinum con-tained doublet chemotherapy in chemotherapy-naive patientswith stage IIIb or IV non-small cell lung cancer of adenocarci-noma histology: A retrospective case control study [Abstract].2009 ASCO Annual Meeting: e19070.
22. Rudin CM, Liu W, Desai A, et al. Pharmacogenomic and phar-macokinetic determinants of erlotinib toxicity. J Clin Oncol2008;26:1119–1127.
23. Dassonville O, Formento JL, Francoual M, et al. Expression ofepidermal growth factor receptor and survival in upper aerodi-gestive tract cancer. J Clin Oncol 1993;11:1873–1878.
24. Shiozaki H. Mechanism of the lymph node metastasis in humanesophageal cancer (epidermal growth factor causes the dysfunc-tion of cadherinmediated cell-cell adhesion). Hum Cell 1996;9:31–36.
25. Ueda M. New prognostic factors in patients with esophagealsquamous carcinoma. Gan To Kagaku Ryoho 1992;19:20–25.
26. Itakura Y, Sasano H, Shiga C, et al. Epidermal growth fac-tor receptor overexpression in esophageal carcinoma. Animmunohistochemical study correlated with clinicopatho-logic findings and DNA amplification. Cancer 1994;74:795–804.
27. Iihara K, Shiozaki H, Tahara H, et al. Prognostic significance oftransforming growth factor-alpha in human esophageal carci-noma. Implication for the autocrine proliferation. Cancer1993;71:2902–2909.
28. Ozawa S, Ueda M, Ando N, et al. Prognostic significance ofepidermal growth factor receptor in esophageal squamous cellcarcinomas. Cancer 1989;63:2169–2173.
29. Gibson MK, Abraham SC, Wu TT, et al. Epidermal growthfactor receptor, p53 mutation, and pathological response predictsurvival in patients with locally advanced esophageal cancertreated with preoperative chemoradiotherapy. Clin CancerRes 2003;9:6461–6468.
30. Friess H, Fukuda A, Tang WH, et al. Concomitant analysis ofthe epidermal growth factor receptor family in esophagealcancer: Overexpression of epidermal growth factor receptormRNA but not of c-erbB-2 and cerbB-3. World J Surg 1999;23:1010–1018.
31. Ajani JA, Ilson DH, Daugherty K, et al. Activity of Taxolin patients with squamous cell carcinoma and adenocarci-noma of the esophagus. J Natl Cancer Inst 1994;86:1086–1091.
32. Ilson DH, Ajani J, Bhalla K, et al. Phase II trial of paclitaxel,fluorouracil, and cisplatin in patients with advanced carcinomaof the esophagus. J Clin Oncol 1998;16:1826–1834.
33. Lokich JJ, Sonneborn H, Anderson NR, et al. Combined pacli-taxel, cisplatin and etoposide for patients with previouslyuntreated esophageal and gastroesophageal carcinomas. Cancer1999;85:2347–2351.
34. Brenner B, IlsonD H, Minsky BD, et al. Phase I trial ofcombined-modality therapy for localized esophageal cancer:Escalating doses of continuous-infusion paclitaxel withcisplatin and concurrent radiation therapy. J Clin Oncol 2004;22:45–52.
35. Adelstein DJ, Rice TW, Rybicki LA, et al. Does paclitaxelimprove the chemoradiotherapy of locoregionally advancedesophageal cancer? A nonrandomized comparison with fluoro-uracil-based therapy. J Clin Oncol 2000;18:2032–2039.
36. Tew W, Shah M, Schwartz G, et al. Phase II trial of erlotinib forsecond-line treatment in advanced esophageal cancer[Abstract]. Proc Am Soc Clin Oncol GI Cancers Symposium2005;23: 5a.
37. Ferry DR, Anderson M, Beddows K, et al. Phase II trial ofgefitinib (ZD1839) in advanced adenocarcinoma of the oesoph-agus incorporating biopsy before and after gefitinib [Abstract].J Clin Oncol 2004;22(Suppl 14): 4021.
38. Teraishi F, Kagawa S, Watanabe T, et al. ZD1839 (Gefitinib,‘Iressa’), an epidermal growth factor receptor-tyrosine kinaseinhibitor, enhances the anti-cancer effects of TRAIL in humanesophageal squamous cell carcinoma. FEBS Lett 2005;579:4069–4075.








![Development of [ C]erlotinib Positron Emission Tomography ...clincancerres.aacrjournals.org/content/clincanres/19/1/183.full.pdf · Imaging, Diagnosis, Prognosis Development of [11C]erlotinib](https://img.pdfslide.us/doc/110x75/5a9efa4b7f8b9a8e178c2b60/development-of-cerlotinib-positron-emission-tomography-diagnosis-prognosis.jpg)

![Preoperative chemoradiation versus radiation alone for stage II … · 2017-12-19 · [Intervention Review] Preoperative chemoradiation versus radiation alone for stage II and III](https://img.pdfslide.us/doc/110x75/5f0251f77e708231d403afe0/preoperative-chemoradiation-versus-radiation-alone-for-stage-ii-2017-12-19-intervention.jpg)