Embed Size (px)
Citation preview

PHASE II COMMITTEE THURSDAY, MAY 31, 2018, 8:00AM – 9:00AM
• Welcome & Introductions: Kohn/Mirza
• COI declarations
• Approval of Minutes/Report: November 2017 (posted on GCIG website)
• Closed/Published Trials: Kohn/Mirza
• Ongoing Clinical Trials:
• NRG GY005 phase 2 component Lee (NCI US)
• STICs and STONEs; NEO; eVOLVE, OLALA Lheureux (PMHC)
• EN2; FANDANGO; PALEO; AVANOVA; AVANOVA-Immune1; UMB1; MaRuC Mirza (NSGO)
• GTAC updates Kohn, Mirza, All
• GEICO; PMHC; CCTG; GOTIC; GGOC; ANZGOG; NRG; NSGO

Trial name/Group name and number
Trial setting: tumour type/stage: recurrent platinum-resistant or –refractory
ovarian cancer
Study Design: Phase II/III randomized trial
Sponsor(s): CTEP/NCI U.S.
Planned No. of patients: 208 (Phase II), 236-472 (Phase III)
Current accrual: Phase II accrual complete, end of phase II analysis pending
Other important information: To re-open in 3Q 2018 for Phase III
Ongoing Trials – status updateNRG CCTGKGOGNRG-J

NRG GY005: Randomized Phase II/III study of the combination of
Cediranib and Olaparib compared to Cediranib or Olaparib alone, or
Standard of care chemotherapy in women with platinum-resistant
recurrent Ovarian Cancer
PRR OvCa patients
ECOG 0-2
Measurable disease
< 2 prior regimens in the
recurrent setting
No prior bevacizumab in
the recurrent setting
gBRCAm status is not
required at study entry
n=208*52 per arm
for Phase II
Appx. 400
for Phase III
1:1:1:1
C + O
C 30 mg daily
O 300 mg bid
PLD
wkly Paclitaxel
Topotecan
PF
S
GY005to be followed by
Ph III OS/PFS trial

NEO: Olaparib Window of Opportunity
Archival tissue
Somatic DNAprofiling
RNASequencing
ctDNAprofiling
IHC

Trial Update
5
• 12 patients enrolled – 1 patient in screening
• 3 Sites open - 5 Sites pending
• First patient enrolled 14 months ago
• Clinical: no PD – no patient off trial
• Correlatives: 1st batch to be sent for analysis

EVOLVE: A proof of concept trial of combination of Olaparib + Cediranib
Platinum SENSITIVE disease
Platinum RESISTANT disease
Prior PARPi progression, treated with further chemo
11/11 pts
8/10 pts
9/10 pts 6
Archival Baseline
Somatic DNAprofiling
RNASequencing
ctDNAprofiling
IHC

Preliminary results
7
- Median age: 57 years (range 43-76)
- BRCA mut status: 6 gBRCA1; 3 gBRCA2; 1 sBRCA1; 1WT sBRCA
- # prior chemotherapy lines: median 2 (range 2-5)
- Prior PARPi: duration - median 7 cycles (range 4-33)
3Ttt (15,21,31 mths) – 8 Maintenance (med duration 13 mths [4-33])
Platinum Sensitive Cohort

STICs and STONES: OV.25 A randomized phase II double-blind placebo-controlled
trial of Acetylsalicylic acid (ASA) in prevention of ovarian cancer in women with BRCA1/2 mutations
Co Chairs: Oza A – Lheureux S
Trial committee: Eisen A, Cormier B, McAlpine J, Weberpals J,
Philips k, Bernardini M, Fung Kee Fung M, Kim R
Pathology Chair: Patricia Shaw
Senior Investigator: Wendy Parulekar
Biostat: Dongsheng Tu
Study coordinator: WenLing Liu
Sponsor: CCTG
Support: Apotex

Study DesignInternational, multicentre, randomized, double-blind, placebo controlled phase II in women with germline BRCA1/2 mutations, scheduled to undergo risk reducing surgey within 6 months to 2 years.
• 2:1 Randomization
• Stratification• Age (<40 vs 40-50 vs >50)• Current (last dose <6 mths) combined oral contraceptive use (Yes vs No)• BRCA status (BRCA1 vs BRCA2)
ctDNA collection (LSARP application)
women with
BRCA1/2
mutations
scheduled to
undergo risk-
reducing
surgery
R
A
N
D
O
M
I
Z
E
↗
ASA
81 mg po daily
Treatment
for a
minimum of
6 months to a
maximum of
2 years
Risk-reducing
surgery
↗
Acetylsalicylic
Acid
(ASA)
↘
↘ ASA
325 mg po daily
Placebo
One tablet po daily
N=414 women

Update / Timelines
• Centrally Activated in Canada April 6 2018
• First Centre Opened in Canada May 17 2018
• Publicity efforts ongoing
• Australian activation pending: ANZGOG
• International Collaborators Identified (including UK, Israel)
– Israeli Sites 4-8: Feasibility Assessment Jun2 2018
– Planning Investigator meeting Oct 2018.

OLALA: long-term vs short-term response to Olaparib (PARPi)
11
Enrolled
19/50 pts
19/50 pts
Multicentres - Canada - International
Somatic DNAprofiling
RNASequencing
ctDNAprofiling IHC

OLALA Objectives
12
• Molecular profiling, genomic and immune profile changes between ST and LT
• Signature of PARP response vs resistance
• Pharmacokinetics and pharmacogenomics of olaparib for patients on treatment

ENGOT- N2-DGCGSponsor: DGCG
A phase II Trial of postoperative chemotherapy or no further treatment for patients with node-negative stage I-II
intermediate or high risk endometrial cancer.
Study Design:
Sponsor(s): NSGO
Planned No. of patients: 240
Current accrual: 199
Other important information: Status - recruiting
Ongoing Trials – status update
Endometrioid:Stage I - G3; II
Non-endometrioid:Stage I-II
ChemotherapyCarboplatin-Paclitaxel x 6+ Brachytherapy
Observation+ Brachytherapy
1:1 randomization
Supported by

ENGOT-EN2-DGCG
Ongoing Trials – status update
Group PI Country No. of Institutions ActivatedTotal nb of pts
randomizedMay 2018
DGCG Mirza Denmark 6 6 63
The Netherlands Netherland 4 4 2
UK United Kingdom 9 9 31
NSGO Lundgren Sweden 4 4 30
Finland 6 5 9
BGOG Kridelka Belgium 10 8 13
MITO Greggi Italy 7 1 7
C-GOG (MDACC) Soliman US 1 1 1
MaNGO Ferrero Italy 6 2 3
NOGGO Sehouli Germany 9 5 11
AGO Chr. Marth Austria 1 1 1
ISGO Levy Israel 7 3 0
GEICO Santabella Spain 14 12 21
CEEGOG Cibula Czech rep. 5 2 6
Total 89 63 199

EN1/FANDANGOSponsor: NSGO
A randomised double-blind placebo-controlled phase II trial of first line combination chemo-therapy
with nintedanib/placebo for patients with advanced or recurrent endometrial cancer
Study Design:
Planned No. of patients: 148
Current accrual: 100
Other important information: Status - recruiting
Ongoing Trials – status updateR
and
om
izat
ion
1:1
N =
14
8
Stratification:• Stage of disease (stage 3C 2 vs. stage 4 vs. recurrent disease) • Prior adjuvant chemotherapy (yes/no) • Disease status (Measurable vs. non-measurable disease according to RECIST 1.1)

ENGOT-EN1-FANDANGO - Overall Summary
16
Group NCNumber
ofSites
Number of Sites
Activated
Screened Patients
Randomized Patients
NSGO Mirza 11 11 37 34
GINECO Berton-Rigaud12 12 41 33
NOGGO Sehouli12 11 23 21
BGOG Altintas6 6 10 9
TOTAL 41 40 111 100
05
1015202530354045
Okt16
Nov16
Dec16
Jan17
Feb17
Mar17
Apr17
May17
Jun17
Jul17
Aug17
Sep17
Oct17
Nu
mb
er
of
site
s
Expected Activated sites Activated sites 41 Sites in total
40 Activated SitesScreening/Recruitment Status per group
100 Randomized patients
020406080
100120140160
No
v 1
6
De
c 1
6
Jan
17
Feb
17
Mar
17
Ap
r 1
7
May
17
Jun
17
Jul 1
7
Au
g 1
7
Sep
17
Okt
17
No
v 1
7
De
c 1
7
Jan
18
Feb
18
Mar
18
Ap
r 1
8
May
18
Nu
mb
er
of
pat
ien
tsExpected Randomized patients Randomized patients
148 Patients in total

EN3-NSGO/PALEOSponsor: NSGO
A randomized, double-blind, placebo-controlled, phase II trial of Palbociclib in combination with Letrozole versus
Placebo in combination with Letrozole for patients with Estrogen Receptor Positive advanced or recurrent Endometrial
cancer.
Study Design:
Planned No. of patients: 78
Current accrual: 42
Other important information: Slow recruitment in the PALEO study. MITO still pending regarding approvals from CA and EC
Ongoing Trials – status update
Endometrial Cancer
Primary stage 4 or relapsed disease
ER positive endometrioid
adenocarcinoma
Randomize
ARM ALetrozole, 2.5mg d 1-28 every 28 daysPlacebo 125mg d 1-21 every 28 days
Until progression
ARM BLetrozole, 2.5mg d 1-28 every 28 days
Palbociclib 125mg d 1-21 every 28 days
Until progression
Stratification:• Number of prior lines (primary adv disease vs. 1st relapse vs. ≥2 relapses)• Measurable vs. evaluable disease• Prior use of MPA/Megace
Randomization: 1:1N=78
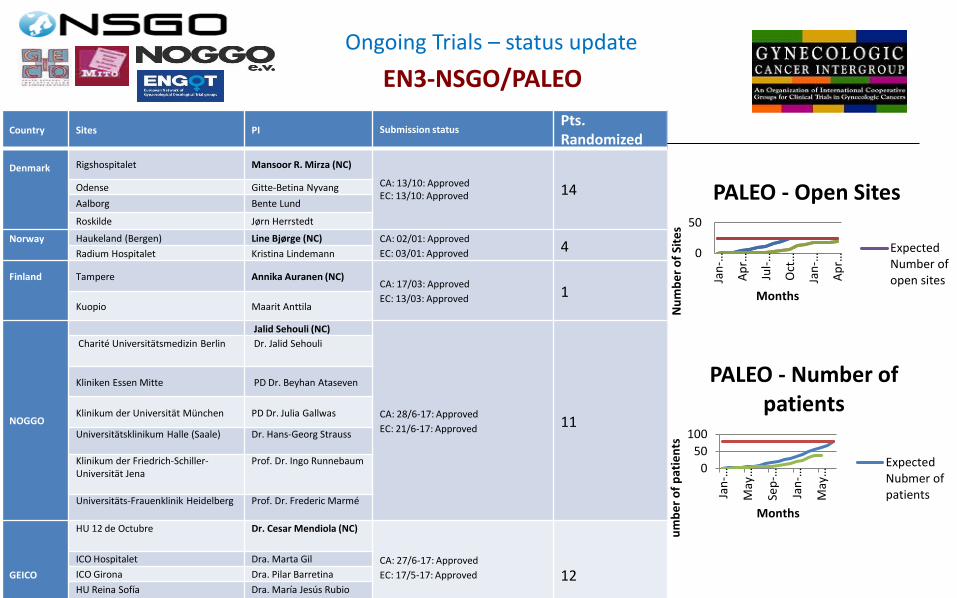
EN3-NSGO/PALEO
Ongoing Trials – status update
Country Sites PI Submission statusPts. Randomized
Denmark Rigshospitalet Mansoor R. Mirza (NC)
CA: 13/10: ApprovedEC: 13/10: Approved 14Odense Gitte-Betina Nyvang
Aalborg Bente Lund
Roskilde Jørn Herrstedt
Norway Haukeland (Bergen) Line Bjørge (NC) CA: 02/01: Approved
EC: 03/01: Approved 4Radium Hospitalet Kristina Lindemann
Finland Tampere Annika Auranen (NC)CA: 17/03: Approved
EC: 13/03: Approved 1Kuopio Maarit Anttila
NOGGO
Jalid Sehouli (NC)
CA: 28/6-17: Approved
EC: 21/6-17: Approved 11
Charité Universitätsmedizin Berlin Dr. Jalid Sehouli
Kliniken Essen Mitte PD Dr. Beyhan Ataseven
Klinikum der Universität München PD Dr. Julia Gallwas
Universitätsklinikum Halle (Saale) Dr. Hans-Georg Strauss
Klinikum der Friedrich-Schiller-Universität Jena
Prof. Dr. Ingo Runnebaum
Universitäts-Frauenklinik Heidelberg Prof. Dr. Frederic Marmé
GEICO
HU 12 de Octubre Dr. Cesar Mendiola (NC)
CA: 27/6-17: Approved
EC: 17/5-17: Approved 12ICO Hospitalet Dra. Marta Gil
ICO Girona Dra. Pilar Barretina
HU Reina Sofía Dra. María Jesús Rubio
0
50
Jan
-…
Ap
r…
Jul-
…
Oct
…
Jan
-…
Ap
r…
Nu
mb
er
of
Site
s
Months
PALEO - Open Sites
ExpectedNumber ofopen sites
0
50
100
Jan
-…
May
…
Sep
-…
Jan
-…
May
…
Nu
mb
er
of
pat
ien
ts
Months
PALEO - Number of patients
ExpectedNubmer ofpatients

Investigator’s choice
(without niraparib)
ARM 1Niraparib
ARM 2Bevacizumab
+Niraparib
Platinum-sensitive
Ovarian Cancer
HGSOCHGEOC
orAny BRCAmut
OC
Randomize
Treat to PD/toxic
ity
Treat to PD/toxic
ity
Randomization: 1:1n=94Hypothesis: Arm 1: niraparib median PFS 8mdr
Arm2: Nir + Bev median PFS 14mdrHR 0.57Power 80%alpha 0.1 inclusion 18 months
Stratification factors:HRD positive/negative
TFI: 6-12 mo vs. >12 mo
19
ENGOT-OV24-NSGO / AVANOVA part 3Sponsor: NSGO
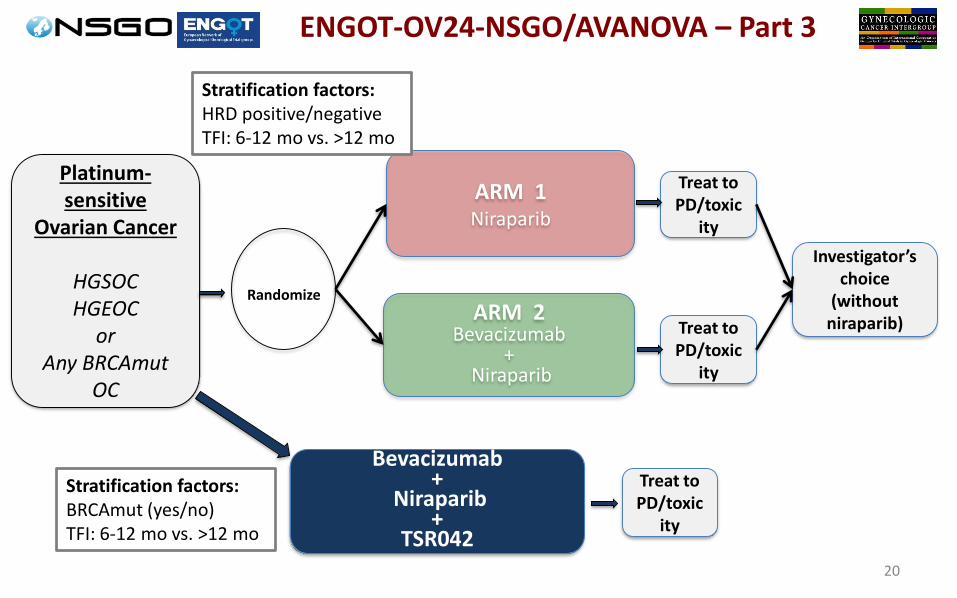
Investigator’s choice
(without niraparib)
ARM 1Niraparib
ARM 2Bevacizumab
+Niraparib
Platinum-sensitive
Ovarian Cancer
HGSOCHGEOC
orAny BRCAmut
OC
Randomize
Treat to PD/toxic
ity
Treat to PD/toxic
ity
Stratification factors:HRD positive/negativeTFI: 6-12 mo vs. >12 mo
20
ENGOT-OV24-NSGO/AVANOVA – Part 3
Bevacizumab +
Niraparib +
TSR042
Treat to PD/toxic
ity
Stratification factors:BRCAmut (yes/no)TFI: 6-12 mo vs. >12 mo

Same Inclusion / exclusion criteriaSame sitesNumber of BRCAmut patients capped to the same ratio as in part 2
Trial statistics:To detect a PFS hazard ratio of 0.7 between dublet and triplet treatmentPower: 80% one-sided significance level: 20%Accrual: 18 months Follow-up: 18 months The doublet arm has included 55 patients which are already in follow-up.
The aim is to have additionally 72 (65+dropouts) patients in follow-up after treatment with triplet.The below scenario is for 1:1 randomization between dublet and triplet, but since the dublet has already been included this is just a guide.
ENGOT-OV24-NSGO / AVANOVA part 3Sponsor: NSGO

ENGOT-OV42 / NSGO AVANOVA-Immune1
A randomized phase II trial of atezolizumab, niraparib and bevacizumab combination for patients with recurrent ovarian cancer.
ENGOT-OV42 / NSGO / AVANOVA-Immune1
Sponsor: NSGOStudy Chair: Mansoor Raza Mirza

ENGOT-OV42 / NSGO AVANOVA-Immune1
Design

ENGOT-OV42 / NSGO AVANOVA-Immune1
Objectives
Primary objective: Compare Progression-Free Survival (PFS) of niraparib-bevacizumab-atezolizumabagainst Standard of care (SoC) therapy in both cohorts (TFI 1-6months and TFI >6months).
Secondary objectives: Safety and tolerability of atezolizumab when given in combination with niraparib-bevacizumab. PFS according to trial stratification factors in both cohorts. Objective response rate according to RECIST (ORR) both in cohort 1 and cohort 2Objective response rate according to irRECIST (irORR) both in cohort 1 & cohort 2Disease control rate (DCR) (CR+PR+SD)Patient Reported Outcomes (PROs)PFS1 + PFS2
Exploratory objectives: Overall survival (OS) in each group according to trial stratification factors
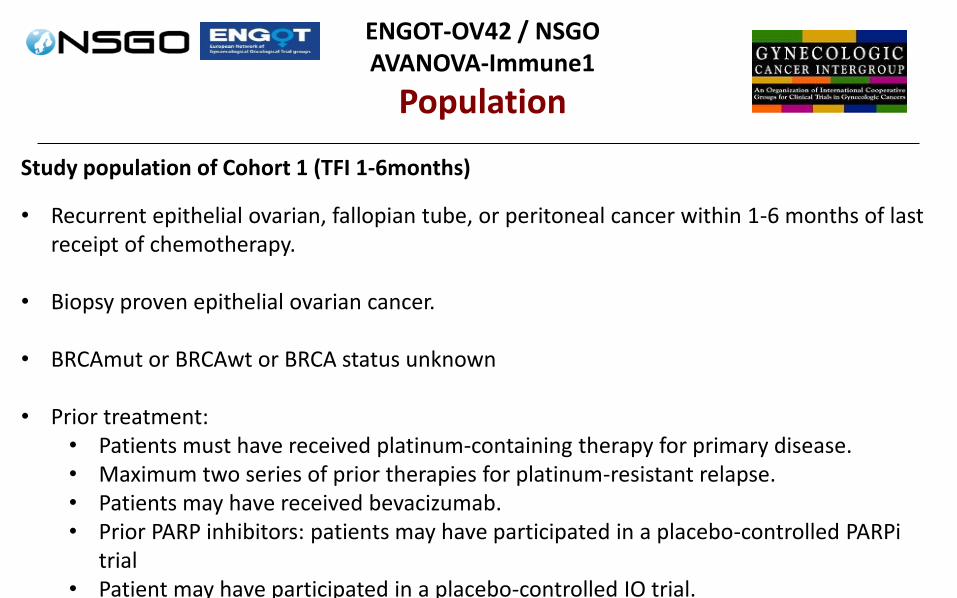
ENGOT-OV42 / NSGO AVANOVA-Immune1
Population
Study population of Cohort 1 (TFI 1-6months)
• Recurrent epithelial ovarian, fallopian tube, or peritoneal cancer within 1-6 months of last receipt of chemotherapy.
• Biopsy proven epithelial ovarian cancer.
• BRCAmut or BRCAwt or BRCA status unknown
• Prior treatment: • Patients must have received platinum-containing therapy for primary disease.• Maximum two series of prior therapies for platinum-resistant relapse.• Patients may have received bevacizumab.• Prior PARP inhibitors: patients may have participated in a placebo-controlled PARPi
trial • Patient may have participated in a placebo-controlled IO trial.

ENGOT-OV42 / NSGO AVANOVA-Immune1
Population
Study population of Cohort 2 (TFI >6months)
• Recurrent epithelial ovarian, fallopian tube, or peritoneal cancer and no recurrence within 6 months of last receipt of chemotherapy.
• Biopsy proven epithelial ovarian cancer.
• BRCAmut or BRCAwt or BRCA status unknown
• Prior treatment: • Patients must have received platinum-containing therapy for primary disease.• Maximum two series of prior platinum-based therapies for relapse.• Patients may have received bevacizumab.• Prior PARP inhibitors: patients may have participated in a placebo-controlled PARPi
trial • Patient may have participated in a placebo-controlled IO trial

ENGOT-OV42 / NSGO AVANOVA-Immune1
Treatment arms
Experimental arm:Arm B combination: • Niraparib 200mg PO once daily until disease progression.• Bevacizumab 15mg/kg IV q 21 days until disease progression• Atezolizumab until progression (dose to be added)
Standard armCohort 1• Arm A: chemotherapy alone (weekly paclitaxel or PLD or gemcitabin) or chemotherapy + bevacizumab.Cohort 2
• Arm A: platinum combination chemotherapy (carboplatin-PLD or carboplatin-paclitaxel or carboplatin-gemcitabine) or platinum combination chemotherapy with concomitant and maintenance bevacizumab or platinum combination chemotherapy followed by maintenance parp inhibitor.

GTAC: GCIG-wide Targeted therapy Against Cervical cancer
Gr ADrug A
Gr EDrug E
Gr BDrug B
Gr DDrug D
Gr CDrug C
GCIG
post CRTCaCx maintenance
therapyR
BSC,OBSERVATION
selected AGENT(s)

ENGOT-CX7 / NSGO / MaRuC
Arm ARucaparib 600mg BID for 24 months
Arm BPlacebo BID for 24 months
No residual disease
n = 162Randomization: 2:1Cervical cancer
Squamous, Adenosquamous, adenocarcinoma
Stage 2B, 3 & 4Or any stage withpara-aortic nodes
Patients have successfully completed definitive
treatment
Stratification factors• Histology (squamous vs adenosquamous, adenocarcinoma)• FIGO stage (2b-pos. nodes vs. 3 vs 4)
Enrolment of patients with squamous cell histology will be capped once 60% patients with this histo-type are enrolled

ENGOT-CX7 / NSGO / MaRuC
Sponsor: NSGO
A randomized double-blind placebo-controlled phase II trial of Rucaparib maintenance therapy for patients with locally advanced
cervical cancerENGOT-CX7 / NSGO / MaRuC
Study Status• Participating groups: NOGGO, PGOG, CEEGOG, PMHC, NCRI, BGOG
• Q3 18: submissions
• Expected FPI: Q4 2018

Standard Concurrent Chemo-Radiation
R2:1
Observation for 24 months
*TSR-0428 for 24 months≤14 weeks
*TSR-042: is an anti-PD1 IgG4 humanized monoclonal antibody that binds with high affinity to PD-1. TSR-042 will be administered using a 30 minute IV
infusion (with a -5 minute and +15 minute window permitted). Patients will receive a fixed 500 mg TSR-042 dose Q3W for the first 4 doses followed by a fixed 1000 mg TSR-042 dose Q6W for the remainder of the study.
PI: Ana Oaknin on behalf of GEICO
No Residual Disease
Stratification Factors• Histology( squamous vs adenosquamous,
adenocarcinoma)• FIGO Stage: IB2, IIA2, IIB w pos.nodes vs III/IVA vs
any Stage with positive ParaAortic Lymph nodes
N=132
A randomized double-blinded, placebo controlled , phase II trial of Anti-PD1, TSR-042, as maintenance therapy for patients with high-risk locally advanced
cervical cancer after chemo-radiation.
G-TAC: Targeted Agents in CxCa: GEICO Study design
G-TAC: GCIG - Targeted Agents in CxCaGEICO Statistical Analysis Plan
Design:Phase 2 randomized, two-arm trial (control vs. experimental treatment with TSR-042).1º End-Point: DFS@2 years:✓ We estimate 50% probability of surviving disease-free for at least 2 years in the
control arm and expect an increase to 63.7% with experimental treatment, which corresponds to a hazard ratio (HR) of 0.65.
✓ Using a 2:1 randomization a total of 138 evaluable patients are required (46 control/ 92 experimental treatment); total 10% drop-out rate is assumed.
✓ This study will be considered sufficiently mature for final analysis when there are at least 66 evaluable patients with events. This number of events provides 80% power with one-sided type I error of 0.2 for detecting significant superiority of the experimental arm using a log-rank test.
✓ The total expected study duration is 3.5 years; planned recruitment duration is 1 years with a minimum follow-up of 2.5 years.

GCIG Strategic Planning
PHASE 2 COMMITTEE
GOALS:•Advancing new opportunities through collaborative phase 2 multi-group studies
•Fostering communication regarding early phases study results to inform of new opportunities
•Collaborate with site committees in focused development
•Collaborate with Rare Tumors committee where phase 2 studies may be the target
•Moving GTAC forward
GCIG Strategic Planning – June 1, 2018, Chicago