Embed Size (px)
Citation preview

[CANCER RESEARCH 50, 6302-6310. October I. 1990]
Phase I Trial of Intraperitoneal Recombinant Interleukin-2/Lymphokine-activatedKiller Cells in Patients with Ovarian Cancer1
James A. Stewart,2 Jerome L. Belinson, Ann L. Moore, John A. Dorighi, Barbara W. Grant, Larry D. Haugh,
John D. Roberts, Richard J. Albertini, and Richard F. BrandaVermont Regional Cancer Center [J. A. S.. J. L. B., A. L. M., B. W. G., J. D. R., R. J. A.. R. F. B.¡,Department of Medicine ¡J.A. S.. B. W. G., J. D. R., J. A. D.. R. J. A.,R. F. B.J, Department of Obstetrics and Gynecolog)' [J. L. BJ, and Department of Mathematics and Statistics [L. D. H.), University of Vermont, Burlington, Vermont 05405
ABSTRACT
Ten patients with ovarian cancer refractory to conventional therapywere treated with intraperitoneal (i.p.) recombinant interleukin-2 (rIL-2)and lymphokine-activated killer cells (LAK). The 28-day protocol consisted of 6 priming i.p. rIL-2 infusions on days 0, 4, 6, 8, 10, and 12.Leukapheresis was performed for mononuclear cell collection on days15, 16, 17, and 18 and lymphokine-activated killer cells were given i.p.with the rIL-2 on days 19 and 21. Three additional i.p. rIL-2 infusionswere given on days 23, 25, and 27. Three dose levels of rIL-2 were tested:5 x IO9, 2 x IO6, and 8 x 10'' units/in2 body surface area. The dose-
limiting toxicity was abdominal pain secondary to ascites accumulationwith significant weight gain. Other toxic effects included decreasedperformance status, fever, nausea and vomiting, diarrhea, and anemia.Peripheral lymphocytosis and eosinophilia were seen at all dose levels.The maximum tolerated dose is 8 x 1(1''units/m2/dose.
Peripheral and peritoneal IL-2 levels were measured with a bioassayusing an IL-2-dependent cell line. At the highest dose level, serum IL-2was >10 units/ml for 18 h. After the first infusion, a 2-log dilution of thei.p. IL-2 was measured in the serum. In the postleukapheresis i.p. IL-2-dosing period less IL-2 was detected in the serum than in the earlier i.p.IL-2-priming period.
The induction and persistence of LAK activity were studied. PeritonealLAK activity was detected as early as 4 days after the first i.p. infusion,by day 11 in all évaluablepatients, and persisted for the 6-day intervalbetween priming IL-2 and LAK/IL-2 infusion. Peritoneal lytic activitypersisted until day 28 in 5 tested patients. These peritoneal cells retainedlytic activity 48 h in culture medium without rIL-2 present. PeritonealLAK activity correlated with the percentage of mononuclear cells and thepercentage of CDS6-positive mononuclear cells in the peritoneum. Theyield of peripheral lymphocytes after the six i.p. priming doses of rIL-2correlated with the dose level of rIL-2 infused. Peripheral blood LAKactivity showed a minimal, however progressive, increase during thetreatment protocol. LAK activity could be enhanced if rIL-2 was presentduring the 4-h assay. These studies indicate that i.p. rIL-2 infusioninduced durable regional LAK activity and primes peripheral blood cellsfor LAK activity if exposed briefly to additional IL-2.
INTRODUCTION
Current approaches to the treatment of ovarian cancer include cytoreductive surgery, radiotherapy, and the administration of systemic agents given p.o., i.V., or i.p. A theoreticadvantage of the i.p. route is the increased ratio of peritonealto systemic exposure of the drug or agent used. This advantagemay be exploited in a disease such as ovarian cancer which formost of its natural history is confined to the abdominal cavity.Using this rationale in numerous clinical trials investigatorshave administered i.p. immunotherapy to patients with regional
Received 2/5/90; accepted 7/2/90.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This work was supported by grants from the National Cancer Institute (P30CA22435). The Division of Research Resources (M01-RR-109). the AmericanCancer Society, VT Division. Lake Champlain Cancer Research Organization(ACS Institutional Research Grant IN-156C). and the Vermont Regional CancerCenter.
: To whom requests for reprints should be addressed, at Vermont RegionalCancer Center, One South Prospect Street. Burlington. VT 05401.
tumors using single-agent cytokines such as IL-23 (1-7), interferons (8-13), or combinations of cytokines (14).
Interleukin-2 activates a population of lymphocytes which isthen capable of lysing natural killer-resistant tumor cells without major histocompatibility complex restriction (15). ThisLAK phenomenon has been utilized in adoptive immunotherapy with rIL-2 to produce antitumor responses in animalmodels (16-18) and in patients with advanced metastatic cancer(19). High-dose intermittent bolus rIL-2 given i.v. has yieldeddurable responses in renal cancer and melanoma but is associated with significant hypotension and fluid retention as treatment-limiting toxicities (19). The administration of LAK alongwith rIL-2 may enhance the therapeutic effect of systemic rlL-2 alone (20).
Comparison of i.v. and i.p. routes of IL-2 administration inmurine models showed that i.p. administration of IL-2 andLAK was more effective than systemic treatments in reducingintraperitoneal tumors (21). The bioavailability of IL-2, determined by the in vivo growth of adoptively transferred T-cells,correlates better with the duration of time IL-2 is detectable inserum than the peak IL-2 levels achieved (22).
Initial clinical trials of i.p. rIL-2 have resulted in in vivodevelopment of LAK as well as toxicities of weight gain anddiarrhea ( 1). To better understand the rIL-2 and cellular kineticsof i.p. administered rIL-2 and LAK we conducted a phase Itrial in patients with advanced ovarian cancer. The objectiveswere to determine the maximum tolerated dose of i.p. rIL-2, toevaluate the feasibility of peripheral LAK harvest using i.p. rlL-2 priming, to describe serum and peritoneal IL-2 kinetics, andto study the induction and persistence of peripheral and regionalLAK activity.
MATERIALS AND METHODS
Patient Eligibility. Patients with persistent or recurrent unresectableepithelial ovarian cancer were candidates for this trial. Eligibility requirements included age £70years. Eastern Cooperative OncologyGroup performance status 0 or 1, lack of other serious medical illnesses,adequate organ function defined by WBC count >4,000/mm3, platelets
>100,000/mm\ serum creatinine <1.4 mg/dl, forced vital capacity>70% of predicted, forced expiratory volume in l s >70% predicted,and serum bilirubin <1.2 mg%. Prior immunotherapy, chemotherapy,or radiation therapy within the previous 4 weeks and prior rIL-2 werenot permitted. All patients provided written informed consent approvedby the University of Vermont Institutional Review Board.
Treatment Plan. Single-cuff Tenckhoff intraperitoneal catheters wereplaced using an incision large enough to lyse adhesions. In some cases,the catheters were placed at the time of the laparotomy documentingrecurrent or residual disease. Isotope or other imaging studies todetermine the distribution of fluid in the peritoneum were not done;however, the relatively large volumes instilled resulted in apparent
s The abbreviations used are: IL-2. interleukin-2: rIL-2, recombinant IL-2:LAK, lymphokine-activated killer cells; AUC, area under the curve: MNC,mononuclear cells; HBSS. Hanks' balanced salt solution: LU. lytic unit; PBS.phosphate-buffered saline.
6302
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL ML-2/LAK
symmetric distribution in the abdomen as assessed by physical examination.
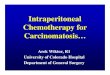
Fig. 1 describes the treatment protocol. Baseline serum and peritoneal fluid samples were obtained on day 0, just prior to the first infusionof rIL-2. At the completion of the IO min drug infusion serum sampleswere collected at 15, 30, 45, 60, and 90 min; 2, 3, and 6 h; and thenevery 6 h for 4 days (96 h). For the first and last rIL-2 infusionperitoneal samples were obtained when possible at 1,2, 4, and 8 h andthen every 24 h for 4 days. Peritoneal samples were often not obtained48-96 h after rIL-2 infusion because of lack of adequate ascites forsampling or difficulty removing fluid through the Tenckhoff catheter.On days 4, 6, 8, 10, and 12 i.p. rIL-2 was infused and serum sampleswere collected as described above. In addition i.p. fluid samples werecollected when possible prior to each rIL-2 infusion. Heparinized bloodand peritoneal fluid were periodically collected and assayed for mono-nuclear cell LAK activity and determination of LAK precursors. Ondays 15, 16, 17, and 18 leukapheresis for lymphocyte harvest was donevia a subclavian vein double-lumen catheter. Lymphocytes were activated in vitro for 3-4 days with rIL-2 and infused with rIL-2 on day 19(day 15-16 leukapheresis) and 21 (day 17-18 leukapheresis). Recombinant IL-2 alone was infused i.p. on days 23, 25, and 27.
The initial dose level was selected in an effort to obtain a descriptionof peripheral levels of rlL-2 and to achieve dose-limiting toxicity withrelatively few escalation steps and numbers of patients. RecombinantIL-2 was provided by Hoffman-LaRoche as a lyophilized powder in 5-ml vials containing 1x10" units. According to a bioassay Hoffman-La
Roche rlL-2 units corresponded with human IL-2 (Jurkat) BiologicResponse Modifiers Program reference units (supplied by the BRMPthrough Hazelton Biotech Co., Vienna, VA) which had a specificactivity of 13.1 x 10* reference units/mg (23). Three dose levels weretested: 5 x 10', 2 x IO6,or 8 x IO6units/m2 body surface area for eachi.p. infusion of rIL-2. Reconstituted rIL-2 was initially administered in1 liu-r m ' body surface area of lactated Ringers. Commercially available
peritoneal dialysis fluids were not used after the first patient because ofinhibition of LAK activity (24). In patients in whom therapy-relatedascites accumulation became a problem, particularly at the highestdose, lesser volumes of fluid were used for rIL-2 administration. Afterthe initial 2 patients all patients received routine acetaminophen, 650mg, P.O., every 4 h; indomethacin, 25 mg, p.o. every 6 h; and rannidine,150 mg, p.o. at bedtime to reduce rIL-2-related toxicity. Meperidine25 mg, i.V., was used as needed to control rIL-2-related rigors.
All patients were evaluated for response by physical examination,radiological tests, and serum CA-125 as appropriate.
IL-2 Pharmacokinetics. Recombinant IL-2 was measured in a standard bioassay using an IL-2-dependent cell line, CTLL-2 (AmericanType Culture Collection TIB214). Dilutions (1:5) of heat-treated (50°C,
20 min) serum, peritoneal fluid, or standard rIL-2 in medium wereincubated with IO4cells/well in 96-well plates for 18 h before labeling
for 4 h with 1 nC\ tritiated iIHinuline Cells were then harvested ontoglass filters and counted in a liquid scintillation counter. Units of IL-2were calculated using a probit analysis computer program of the IL-2titration data.
Given the difficulties of analysis of intraperitoneal therapy kineticswe adopted a unique nonparametric curve-fitting approach to determinethe AUC. A cubic spline interpolant (CSAKM), designed to be smoothand minimize oscillations, was fit to the data (25). An iterative algo-
IL2 IL2 IL2 IL2 IL2 IL2
I I I I I I: I0
I I I4 6
I I I I10 12
LAK LAKIL2 IL2 IL2 IL2 IL2
I , , . .I I I I I I I I I I I I I I
15 1819 21 23 25 27
Fig. 1. Treatment protocol for intraperitoneal IL-2/LAK: IL-2 was given i.p.on day 0 and then every 48 h on days 4, 6. 8. 10. and 12. LAK activated for 3and 4 days were given i.p. with IL-2 on days 19 (from leukapheresis days 15 and16) and 21 (from days 17 and 18). IL-2 alone was given i.p. on days 23. 25. and27.
rithm was written, calling this interpolant, in order to locate an endpoint in time for each curve beyond which the concentration is treatedas zero. Beginning initially with very large trial end points, and successively decreasing the end point, the first value of time which guaranteeda non-negative interpolant over the complete range was selected. Thearea under the curve could then be determined by an integration(CSITG) of the fitted interpolant (25).
A comparison of AUC values across days and among dosage groups(low, 5x10' units/m2; medium, 2x10" units/m2; high, 8x10" units/m2) was done by a repeated measures univariate analysis of variance
and attendant multiple comparisons using SAS software (GLM) (26).Transformations (log or square root) of AUC values were analyzedalternatively to ensure that the nonconstant variance among dosagelevels did not affect the results of the multiple comparisons.
In order to contrast the total AUC for the first and second halves ofthe study it was necessary to calculate imputed values for patients 1(day 10), 4 (day 4), 8 (day 12), and 10 (day 27).
Mulinimi k-ar Cell Separation. Patients underwent leukapheresis us
ing a continuous flow cell separator (Travenol celltrifuge II). Acidcitrate dextrose (NIH formula A, 15 ml) and 3000 units of heparinwere added to the collection bag at the time of leukapheresis. Thenumber of MNC obtained was counted after each apheresis. Mononu-clear cells from leukapheresis, heparinized blood, or peritoneal fluidwere isolated by centrifugation over a 5- or 20-ml discontinuous Ficoll-Paque gradient (Pharmacia, Piscataway, NJ) in 15- or 50-ml conicalcentrifuge tubes. For the last four patients leukapheresed MNC wereseparated over Ficoll-Paque and washed using a Fenwal CS-3000 bloodcell separator (27). Separated MNCs were washed twice with HBSSand resuspended in medium either for activation of LAK or to assaydirectly for LAK activity. In some cases in order to remove residualeosinophils the peritoneal cell population was further separated on acontinuous density gradient formed by centrifugation of a 1:2 mixtureof peritoneal cells in HBSS and Sepracell-MN (Sepratech, OklahomaCity, OK). Occasionally unscheduled peritoneal samples were obtainedand the peritoneal cell pellet after centrifugation was resuspended inAIM V medium (28) (Gibco, Grand Isle, NY) without rIL-2 andincubated 24-48 h prior to Ficoll-Paque and Sepracell MNC separationand determination of lytic activity. Cytospin preparations were stainedwith Wright-Giemsa to determine cellular composition by morphology
before and after separation procedures.LAK Activation. For the first five patients LAK activation medium
consisted of RPMI 1640 (low endotoxin), 2% autologous serum, glu-tamine, antibiotics (Gibco), and 1500 units/ml rIL-2. Early in the studyautologous serum was used for in vitro LAK generation because commercially available human serum used in prior LAK trials was suspectfor hepatitis infection. Phlebotomy to obtain the serum was done everyweek for 3 weeks beginning 1 month prior to therapy. Autologousserum was tested prior to the start of treatment to ensure that serumdid not inhibit LAK generation in vitro. For the last four patients AIMV was used.
Mononuclear cells from the first five patients were activated in tissueculture flasks (800 ml) containing 300 ml of MNC (1.5 x 106/ml) andincubated for 3-4 days at 37'C in 5% CO2. After activation the cells
were centrifuged and washed twice with HBSS in 50-ml tubes. TheMNC from the last four patients were activated in culture bags undersimilar conditions and then pooled and washed with HBSS using theFenwal CS 3000.
The resulting LAK were resuspended in infusion medium consistingof 200ml of 0.9% sodium chloride containing 5% normal human serumalbumin (American Red Cross Blood Services, Washington, DC) and75,000 units of rIL-2. An aliquot of the final cell suspension was shown
to be sterile by Gram stain prior to infusion into the patient. Aliquotsof cells were also assayed for lytic activity.
Lytic Assay. LAK activity was assayed in a standard 4-h chromiumrelease assay as we have previously described (24) using the tumor cellline Daudi as the target cell. Effector cells were resuspended in RPMI1640 medium with 10% heat-inactivated fetal calf serum. Percentageof specific lysis was calculated for each effectortarget ratio and expressed as LU (numbers of effectors in 10" MNC lysing 30% of 5000
6303
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rlL-2/LAK
targets). In some assays the effector cells were incubated with 100 units/ml rIL-2 during the 4-h assay period (29).
Mononuclear Cell Phenotyping. Mononuclear cells (IO6) were labeledwith 20 f/l of fluorescein-conjugated anti-Leu 4 (CD3) and 20 //' ofphycoerythrin-conjugated anti-Leu 19 (CD56) (Becton Dickinson,Mountain View, CA) in 50 M' PBS containing 0.5% bovine serumalbumin and 0.1% azide for 30 min at 4°C.MNCs were washed twice
with PBS and resuspended in PBS/bovine serum albumin/azide containing I% paraformaldehyde. Correlated two-color fluorescent analysis was acquired from the gated lymphocyte fraction using an OrthoDiagnostic Cytofluorograf 50-H (Ortho Diagnostics Systems, Inc.,Westwood, MA).
RESULTS
Ten patients were enrolled in this trial and all were évaluablefor toxicity. Patient characteristics including dose level andtotal rIL-2 given are shown in Table 1. Patient 9 received onlysix infusions of rIL-2 because of intraperitoneal infection priorto leukapheresis.
Toxicky. The dose-limiting toxicity was the accumulation ofascites. All patients gained weight (Table 2). The median percentage increase in weight was 9% (range, 1-42%). Abdominalgirth was measured daily and increased in all patients with amedian increase of 12% (range, 7-42%). The clinical impression was that weight gain was primarily from ascites and notperipheral edema. Weight gain was greater for higher doses ofrIL-2. Subjectively, abdominal fullness and discomfort fromascites was the most distressing toxicity.
Given the duration and intensity of the treatment periodgeneral fatigue and confinement to bed were common complaints. Eastern Cooperative Oncology Group performance status was determined on a daily basis (Table 2). Ascites, fatigue,nausea, and diarrhea were the major toxicities resulting in adecreased performance status. A common but relatively minorcomplaint was of nasal congestion after the initial infusion ofrIL-2. Hypotension occurred but was not dose or schedulelimiting.
RBC transfusion was needed in all patients. The first 6patients underwent phlebotomy for the collection of serumneeded for LAK culture. With the availability of serum-freemedium the phlebotomy procedure prior to treatment waseliminated. Patients received a median of 5 units of packedRBCs (range, 2-10). An effort was made to keep the hemoglobin >9 g/dl. Patients 7-10, who did not undergo phlebotomyfor serum collection, required 5, 5, 4, and 2 units of RBCs,respectively.
Thrombocytopenia occurred as a result of both i.p. rIL-2 and
the leukapheresis procedure. The lowest platelet counts tended
to occur on days 17 and 18 just after apheresis and were thoughtto be due to the leukapheresis procedure. Two patients receivedplatelet transfusions during this period. Platelet counts greaterthan baseline were recorded toward the end of therapy. Fivepatients had platelet counts >400,000/mm' at the end of thetrial on days 26-28.
Significant WBC count changes occurred during the courseof treatment (Table 3). A dose-related lymphopenia occurredafter the first i.p. rIL-2 infusion. All patients experienced alymphocyte rebound usually occurring on days 14-15 after theinitial six infusions of rIL-2. Peripheral eosinophilia was dramatic with an approximately 100-fold increase in three patientsat the highest dose level.
Liver and renal toxicities, as measured by serum chemistrywere mild and transient. Only one patient had an aspartateaminotransferase >2 times normal and 5 patients had serumalkaline phosphatase >2 times normal. The highest bilirubinwas 1.1 mg/dl on day 23, in a patient treated at the lowest doselevel. Significant changes in serum creatinine did not occur.
One patient (patient 4) experienced abdominal wall extravasation of rIL-2 resulting in an area of skin hyperemia. Replace
ment of the catheter allowed intraperitoneal therapy withoutdifficulty. One patient (patient 9) developed Staphylococcusaureus peritonitis after six infusions of i.p. rIL-2. Treatmentwith rIL-2 was stopped and i.v. and i.p. antibiotics were given.
Clinical Response. Nine patients had progressive disease despite rIL-2/LAK. One patient (patient 7) demonstrated reduction of a tumor nodule in the uterosacral ligament assessed byphysical examination (from 0.5 to 0.2 cm) accompanied by atransient reduction of serum CA-125 (257 units/ml pretreatment, 155 units/ml immediately posttreatment, and 113 units/ml 1 month posttreatment). Disease progression in this patientoccurred at 3 months posttreatment. The median survival ofthe 10 patients is >11 months (range, 2-27+ months). Twopatients are currently alive with evidence of disease.
Two patients underwent laparotomy after therapy with rlL-2/LAK. One patient (patient 8) had placement of anotherTenckhoff catheter for i.p. cisplatin treatment 8 months afterrIL-2. Peritoneal adhesions more extensive than those seen atthe earlier catheter placement were present. Another patient(patient 9) underwent exploratory laparotomy 8 months afterrIL-2 for treatment of bowel obstruction. Obstruction wasbecause of tumor and although adhesions were present theywere not believed to be unusual in amount or quality.
rIL-2 Kinetics. The initial dose of rIL-2 was followed by 4days without therapy allowing for prolonged sample collectionso as to fully describe the kinetics of rIL-2 given i.p. IL-2 couldbe detected in the serum within 15 min in all patients except
Table 1 Patient characteristics
Patient Age(yr)1
41254
3604
565556707
558 509 46
10 44Largest
tumormass(cm)>2
<2>2>2
>2>2<2
<2>2>2Prior
therapy"a
(3), b, c, d, e, f, ha (2), d, e, fa(l), b, d, e,fa
(2), d. e, fa (2), d, e, fa (2). d, e,fa
(2), d, e, f, ga (2), d, e, fa (4), d, e. f. g. ha (3), e, fDose
level(units/m2)5
x 10*5x 10*5 x10*2x
IO62 x 10"2xIO68x
10'8x 10'8x IO68 x 10'Infusions
(dayheld)11
111110
(day 4)111111
10 (day 12)6 (days 19-27)
10 (day 27)Total
rIL-2 given(x 10'units)9.1
9.19.434
3534123
12877
120" a, abdominal surgical procedures prior to study (no. of operations); b. hormonal therapy (tamoxifen +/—megestrol acetate); c, interferon (i.p.); d. doxorubicin; e.
cyclophosphamide; f, cisplatin (i.v.); g, cisplatin (i.p.); h, VP-16.
6304
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rlL-2/LAK
Table 2 Toxicity
Performance statusEastern Cooperative
Wl Oncology GroupPatient gain* (days at PS 2 3)
rIL-2related
Nausea" Vomiting" Diarrhea" fever
12.1456789"1013'0,103223378171411248è131010102
112222
221212
200120221222122222222" By National Cancer Institute Common Toxicity Criteria.* Weight gain: O, <5C¿;1. 5-9.9"^; 2. I0-I9.9ré:3. ==20%.c Ascites thought to be tumor associated, rather than treatment related.J Abbreviated course (6 doses) because of peritonitis, treatment related.
two receiving the lowest dose. Peak serum levels were usuallyreached within 3-6 h.
Fig. 2 shows the serum and peritoneal rIL-2 levels measuredfrom two representative patients receiving the highest andlowest doses of rIL-2. Serum levels followed peritoneal levelsover time. Generally, a 2-log dilution of the i.p. IL-2 level wasmeasured in the serum. Peritoneal IL-2 levels were still detectedat 72-96 h in patients receiving the highest dose level of rIL-2,but ascites was often not obtainable after 24-48 h in patientsreceiving lower doses.
Fig. 3 shows the mean (±SE)of serum rIL-2 levels for eachdose level at the various sampling times. As depicted by Figs.2 and 3 the duration after infusion that serum rIL-2 wasdetected was <18 h at the lowest dose of i.p. rIL-2 and <30 hfor the patients receiving the higher doses of i.p. rIL-2. Peaklevels of serum rIL-2 were dose related. Serum levels >10 units/ml were maintained for 18 h at the highest dose level.
Early in the treatment schedule there was a clear correlationbetween i.p. IL-2 dose level and peripheral IL-2 exposure asmeasured by the calculated AUC (Fig. 4). Interestingly, therewas a dramatic decrease in peripheral IL-2 levels in the secondhalf of the treatment, particularly in patients receiving thehighest rIL-2 dose. Most notably, patient 8 had no detectableserum IL-2 during the period of the last five infusions. Thiswas accompanied by high i.p. IL-2 levels, reaching >25,000units/ml, and ascites accumulation. Except for patient 5 therewas a higher peripheral AUC for days 0-12 compared to days13-27.
A repeated measures analysis of variance of the AUC values
indicates that the three dose level groups do not follow thesame pattern over days of administration, since there was astatistically significant interaction (P < 0.05) between dose levelgroups and days for either days 0-12 or 0-27. The only statistically significant differences among dose level groups in AUClevels at each day appeared at day 0 (even if nonconstantvariances among the groups are compensated by an appropriatedata transformation). At day 0 the high-dose level group hadsignificantly higher mean AUC than the medium- or low-doselevel groups. Fig. 4 indicates that the AUC on average tends tofollow the expected pattern of higher AUC values with higherdose level given.
A contrast can be drawn between the rIL-2 levels of the firsthalf of the study, in which rIL-2 was given on days 0, 4, 6, 8,10, and 12, and the second half of the study, postleukapheresis.Fig. 4 illustrates that the AUC drops significantly from day 0through day 12, particularly at high doses. There are statisticallysignificant negative correlations between AUC and day for boththe high and medium doses with r = —0.62(P = 0.002) for highand r = —0.69(P = 0.002) for medium. That correlation is not
just due to the initial drop after day 0 but is also significantfrom days 4 through 12 for the high and medium doses (r =-0.46, P = 0.048, for high and r = -0.56, P = 0.036, formedium). The negative trend for high- and medium-dose levelsalso appears during the second half of the study (r = -0.42, P= 0.13, for high and r = -0.52, P = 0.045, for medium) although
it is not as statistically significant.In order to judge whether the overall level of AUC has
decreased during the second half of the study the differencesand percentage of differences in total AUC for the 5 doses (days4-12) and the total AUC for the 5 doses (days 19-27) werecompared with a paired t test. On average the AUC levels werelower in the second half, but the difference was not significant.
Peritoneal Cells. The generation of peritoneal LAK activityis detailed in Table 4. LAK assays were done with cells obtainedjust prior to rIL-2 infusions. Some patients could not be evaluated on particular days because either there was no peritonealfluid or the Tenckhoff catheter would not drain. Usual MNCseparation methods using a Ficoll-Hypaque discontinuous gradient were not successful in removing peritoneal eosinophils.When peritoneal cells after separation methods contained<30% MNC the absence of lytic activity was considered notévaluable.Occasionally, on later days in the protocol schedule,peritoneal fluid could be obtained but was essentially acellular.LAK activity was not detected in peritoneal MNC obtainedprior to or immediately after the first i.p. rIL-2 infusion on day0 (5 évaluablepatients. Table 4). Four days after the first
Table 3 Peripheral H'BC changes
Lymphocytes(/pi)Patient
Day01
1,65321,58433964
824585666367
1.80088199
1.443101.180Day
17031.6173602922131202198818645Day
1Day
00.431.020.910.350.250.190.120.110.130.04High(day)2.944(14)2.806(15)1.715(15)2.013(15)3.861
(14)1,800(15)3.451
(14)2.310(14)4.788(12)3.750(16)HighDay
01.81.84.32.44.52.81.92.83.33.2Day028572(11030531003999947Eosinophils
(/n\)High
(day)3,960
(22)1.584(25)2.050
(23.24)874
(26)4,077(24)1.276(24)11.328(22)6.283
(26)1.664(15)8.400(16)HighDay
0142247"924°24113161<2179
' On day 0 when no eosinophils were reported in the differential a value of 1% was used in order to calculate a ratio.
6305
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rIL-2/LAK
10000•
Fig. 2. Serum (5) and peritoneal (P) IL-2 glevels on day 0 for two representative patients. \
. patient 1 (dose, 5 x 10*units/m2); -°-, patient 7 (dose, 8x10' units/m2). pj
I
Day 0
io
Hours
100 Day 0
Fig. 3. Serum IL-2 on day Oforali patientsat each dose level. Dose levels: •,5 x 10*units/m2; D, 2 x 10' units/m2; A, 8 x 10'units/m2; points, means; bars, ±SE.
1
infusion, 4 of 5 évaluablepatients had peritoneal cells expressing low levels of LAK activity (<5 LU). By day 7 (24 h afterthe third infusion of IL-2), peritoneal MNC from 5 of 8évaluablepatients exhibited a wide range of LAK activity (<5-288 LU). By day 11 peritoneal MNC from all 6 évaluablepatients demonstrated lytic activity (10-375 LU). This activitywas persistent even after incubation for 24-48 h in mediumwithout rIL-2. Addition of rIL-2 (100 units/ml) to the assaydid not increase the lytic activity. On day 18, 6 days followingthe last primary infusion, peritoneal cells from 3 of 4 patientscontinued to manifest the capacity to lyse Daudi targets. Following rIL-2/LAK infusion on days 19 and 21, peritonealMNC from all évaluablepatients had LAK activity on days25-28.
The initial pretreatment peritoneal cell analysis varied considerably among patients. Only 2 patients had peritoneal fluidobtainable prior to treatment. For other patients the initialanalysis was done on cells obtained by lavage immediately afterrIL-2 infusion. The majority of the pretreatment peritonealcells were eosinophils in 4 patients, neutrophils in 2 patients,
Hours
and MNC in 3 patients. Cellular populations varied considerably during the treatment for each patient and from patient topatient. There did not seem to be a correlation between rIL-2
dose level and cell type or numbers of peritoneal cells obtained.MNC tended to predominate during days 7-14, followed by aninflux of eosinophils, often making up >80% of the cells by theend of the treatment. A rise in the percentage of MNC in theperitoneal fluid correlated with an increase in the percentage ofCD56-positive MNC and enhanced lytic activity.
Peripheral MNC Priming from ¡.p.rIL-2. The number ofWBCs obtained from the 4 days of leukapheresis, the cell yieldfollowing ex vivo IL-2 incubation, and the total i.p. infused lyticunits of LAK generally correlated with rIL-2 dose (Table 5).Patients 2 and 8 were exceptions. Patient 2 had large numbersof adherent cells in the ex vivo activated cultures. Becausepatient 8 was not administered the sixth infusion of IL-2 (day12), 5 days instead of 3 elapsed between the last i.p. rIL-2infusion and leukapheresis. This delay may explain the slightlylower leukapheresis and LAK yields obtained and the considerably decreased number of lytic units generated for this patient.
6306
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rIL-2/LAK
1000-
Fig. 4. AUC (units'h/ml) of serum IL-2levels after each IL-2 infusion for each of threedose levels given: •.5 x 10s units/m2: Q, 2 x10' units/m2; A, 8 x 10* units/m2; points.
means: bars, ±SE.
—1—
83
—1—
MT
28
Doy
Table 4 Peritoneal lytic activity (LU/10* peritonealMNC)°
Study day
11 14 18 21" 25 28
Patients12345678910%
Evaluable patients with lytic activity0NONONO000NO0NO0NOC0NONONO<5<5<5<5NO80V0288NO072"8NO39"<563NO38"NONO13"107"81"10NE'375"100NE'10NONONO218"350NE7NE'144100NO<50"NONONO53"NE'Off
study<5"75NE'IS5838461429NE'364100NO<5NE'<51399NE'NE'175100<530NE'30085459NE'NE'NO100
°0 LU. <10% specific lysis at effectontarget ratio of 40:1; <5 LU, >IO-<30% specific lysis at effectortarget ratio of 40:1.'Cells obtained before LAK/IL2 infusion.' NO, not obtained."Cells cultured 24-48 h in media without IL2 before assayed for lytic activity.' Due to eosinophilia; NE, not évaluable(ascites collected but not assayed because of insufficient numbers of MNC).'Acellular ascites; NE. not évaluable(ascites collected but not assayed because of insufficient numbers of MNC).
Table 5 IL-2, ¡.p.,priming of peripheral lymphocytes for ex vivo LAK activation
Total LAKTotal leukopak yield (4
cell yield (4 days) xdays) x 10' 10'
Mean LU/10' Total LULAK (4-day infused x
range) IO3
Dose: 5 x 10'units/m2Patient
1Patient2Patient
3Dose:
2 x 10*units/m2Patient
4Patient5Patient
6Dose:
8 x 10*units/m2Patient
7Patient8Patient
1024282335474069547016121020182248366348(21-82)<5116(18-355)158(99-152)155(80-189)426
(355-470)381
(373-389)107(97-117)396(301-494)8264630413223.3487,16718.0003.75825,448
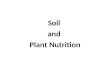
Peripheral MNC LAK Activity. Fig. 5 illustrates the percentage of specific lysis of Daudi targets by peripheral MNC fromall 10 patients after i.p. infusions of rIL-2. There was a pro-
6307
gressive increase in lytic activity (mean percentage of specificlysis), reaching a peak on day 18 and persisting until day 28.The inducibility of peripheral LAK activity did not appear tocorrelate with i.p. rIL-2 dose, since patients from each of the 3dose levels had >20% specific lysis on days 25 and 27. Onepatient (patient 3) who was receiving the lowest dose of rIL-2(5 x IO5 units/m2) had high levels of peripheral LAK activityafter the First i.p. infusion of IL-2 and maintained this throughout the study. The large standard error of the mean percentageof specific lysis of all patients (Fig. 5) reflects this patient's high
peripheral LAK activity. Lytic activity of peripheral MNCscould be greatly enhanced after several i.p. IL-2 treatments(from 8 to 60% specific lysis) when rIL-2 (100 units/ml) wasadded during the 4-h assay. Peripheral MNC from 10 normalindividuals exhibited a similar enhancement of lytic activity ifIL-2 was present during the assay (from <5% specific lysis to20 ±11%), however, not as dramatic as the patients' peripheral
MNC after i.p. IL-2 priming. The increase in these primedperipheral lymphocytes coincided with an increase in the per-
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rIL-2/LAK
ininiuU-LüCL
(/)50
-,4540^^-
35-o•*30-£25-^20-¿15-105-0-IL2«•
m•A*•
"%*»—
J-^•• X^^• A. ———irf A"-^-^
« * -**^^ •» - . 'JÉ ..^ .„::'..««••0
4 6 8 10 12 19 21 23 25 27
DAYS LAK LAK
Fig. 5. Peripheral MNC LAK activity [% specific lysis Daudi effectortarget(E:T)40:I| during i.p. IL-2/LAK from patients receiving doses: •.5 x 10' units/m2: •.2 x 10* units/m2; A, 8 x 10' units/m2: *, mean % specific lysis of allpatients assayed that day: bars, ±SE;shaded area, mean rl specific lysis ofperipheral MNC from 10 normal individuals not receiving II.-2 treatment.
centage of CD3-negative, CD56-positive MNC during the treatment course.
DISCUSSION
Optimal treatment with biological response modifiers ultimately requires knowledge of the dose resulting in the greatestdesired biological effect. First, however, it is important to havean understanding of the dose range tolerable in humans, thekinds of toxicities encountered, and a description of the kineticbehavior of the agent used. In this trial we evaluated three doselevels of rIL-2, given i.p. as repeated infusions, with the additionof autologous LAK.
The dose-limiting toxicity of rIL-2 given on this schedule wasdiscomfort secondary to ascites accumulation. Patients at thehighest dose level gained from 19 to 42% of their baselineweight from fluid retention manifested as ascites and peripheraledema. Because of increasing ascites many rIL-2 infusions weregiven in volumes of lactated Ringers' solution smaller than theinitially prescribed 1 liter/m2. The three patients at the highestdose level who received the full 28-day course of therapy allexperienced the need for ascites drainage, dose elimination, orreduction of rIL-2 volume infused. The discomfort from thefluid gain and abdominal distension seen with repeated infusions of 8 x 10* units/rrr suggested that at higher dose levels
few patients would tolerate even a majority of infusions on thisschedule. Therefore, the maximum tolerated dose is consideredto be at or near 8 x IO6units/m2.
The infusion of LAK did not seem to directly increase toxicity. There were no episodes of wheezing, urticaria, or otheranaphylactic type reactions and no increase in nausea or diarrhea over that seen with i.p. rIL-2 alone. Fluid gain did notcompletely resolve during days 13-18 prior to the second courseof rIL-2, so it is difficult to determine whether LAK influencedascites accumulation.
Lurie et al. (2) reported a lack of weight gain or ascitesaccumulation in a trial of i.p. rIL-2 using a daily times fiveschedule every 2 weeks in which total doses ranged from 4.0 xIO4 to 15.6 x IO6 units/patient. In contrast, using three times
a day dosing and a higher individual dose level Lotze et al. (1)reported that all patients gained weight. It is also worth noting
that these studies used Cetus rIL-2 (Emeryville, CA) which hasbeen shown, on a unit for unit basis, to be more potent thanRoche rIL-2. Clearly, ascites will limit dose and frequency oftreatment particularly when the peritoneum is already abnormalas in patients with advanced ovarian cancer or other malignancies metastatic to the peritoneum.
Other authors have raised concerns about the potential development of peritoneal fibrosis following i.p. biological therapy (30). Such Fibrosis could lead to either bowel obstructionrequiring surgical intervention or significant occlusion of theperitoneal cavity precluding continued i.p. therapy. D'Acquisto
et al. (11) noted evidence of peritoneal inflammation in a trialof i.p. recombinant 7-interferon and postulated a direct effectof the interferon as a cause. Our trial experience suggests that,although rIL-2-related fibrosis may be a problem, it should beevaluated in the context of the clinical setting. Ovarian canceris a disease that naturally produces bowel obstruction, andfibrosis at second- or third-look laparotomies is not uncommonin this population. Evaluation of the fibrogenic pathogenesisand development of preventive measures are needed.
A potential kinetic advantage of i.p. over i.v. therapy includesa high i.p. to peripheral ratio of drug with resulting reductionin systemic toxicity (31). Indeed, in this trial the dose-limitingtoxicity of hypotension seen with high-dose i.v. bolus rIL-2 wasavoided. The 2-log advantage of i.p. over serum IL-2 levels seen
in this trial is similar to that of other studies (3, 30). Thus, thetoxicity profile is altered and high IL-2 levels in the peritoneumand maintenance of modest but prolonged serum levels areachieved. In fact, peripheral levels of IL-2 approximated thatnecessary for LAK activation in vitro (32).
We noted an initial lymphopenia, a rebound lymphocytosis,and marked eosinophilia similar to that reported for i.v. IL-2(33). Based on this trial leukapheresis might be more productiveif started 48 rather than 72 h after the last rIL-2 primaryinfusion. Leukapheresis was scheduled for day 15 which forsome patients was 1-2 days after peak lymphocytosis. MNCyields from apheresis at our highest i.p. rIL-2 dose level approximated those obtained after high-dose i.v. bolus rIL-2 byRosenberg et al. (19). The latter investigators reported a 66.5x IO9median total cell yield from 5 days of leukapheresis afteran i.v. dose of IO5units/kg, 3 times/day, for 5 days, comparedwith a cell yield of 69, 54, and 70 x IO9from our three patientsreceiving high-dose rIL-2 i.p. (Table 5). In a previously reportedi.p. rIL-2/LAK trial (30) patients were initially primed i.v. for3 days in their first cycle and then administered rIL-2 withLAK i.p. followed by a second cycle of leukapheresis and i.p.rIL-2/LAK. Thus, that protocol differed from ours in rIL-2
dose, timing, and source. They obtained a mean LAK yieldfrom each day of leukapheresis of 10.8 x 10' (cycle 1 i.v.priming) and 7.7 x IO9 (cycle 2 i.p. priming). Our mean LAKyield for each day of leukapheresis was 3.2, 5, or 12.3 x IO9forlow-, medium-, and high-dose levels of rIL-2 in our protocol.The range of total number of LAK generated in our patientsreceiving the highest dose was 36-63 x IO9,while those administering high-dose rIL-2 i.v. report a range of 20-152 x IO9(mean 76 x 10") (33). We conclude that i.p. rIL-2 can ade
quately generate sufficient peripheral cells for ex vivo generationof LAK.
Enriched populations of CD3-negative large granular lymphocytes are efficiently activated by rIL-2 and demonstrateLAK activity within hours. This is in contrast to CD3-positiveMNC requiring 2-3 days exposure to IL-2 to generate maximal activity (34). Although peripheral LAK activity was high
6308
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rlL-2/LAK
in only one patient, we could show that the peripheral MNCfrom patients receiving i.p. rIL-2 were "primed" for lytic killing
and only needed additional exposure to rIL-2 (100 units/ml)during the short assay period to effect lysis. Furthermore, thisincrease in primed peripheral MNC coincided with an increasein the percentage of CD3-negative, CD56-positive MNC duringthe treatment course.
This study confirms other clinical reports (5, 7, 30) thatfollowing i.p. IL-2 there are large numbers of MNC in theperitoneal cavity which are activated to kill tumor in vitro. Ourfindings show that this LAK activity corresponded to increasesin the CD3-negative CD56-positive population of large granularlymphocytes rather than CD3-positive T-cells.
We found that rIL-2 i.p. every 48 h induced peritoneal LAKactivity, and this activity persisted for several days after the lasti.p. rIL-2 infusion. Although LAK are reportedly dependenton continued exposure to IL-2 for effective killing function (35,36), these endogenously activated cells retained lytic activityeven after being incubated in culture media for 48 h withoutIL-2. Our findings also indicate that i.p. rIL-2 does not need tobe given by continuous infusion (6) or even every 8 h (1, 30) tomaintain adequate IL-2 levels to support localized LAK activity.Based on our observations, we suggest that 2 or 3 i.p. rIL-2infusions/week could maintain cellular lytic activity and perhaps avoid severe toxicities such as ascites, abdominal pain,and intraperitoneal fibrosis.
Another approach to i.p. immunotherapy has been to primewith low doses of rIL-2 i.p., expand the intracavitary lymphocytes ex vivo with IL-2, and then reinfuse cells i.p. (2). However,using this approach, total doses of ex vivo activated intracavitarylymphocytes given ranged from only 2 to 20 x IO8. It may bethat judicious scheduling of i.p. IL-2 can induce endogenouslylarge numbers of LAK and obviate the need for the technicallymore demanding ex vivo activation of peritoneal cells.
Previous reports of therapy with i.p. or i.v. IL-2/LAK (30,33) have shown that neither in vitro LAK activity nor numbersof LAK infused were predictive of clinical efficacy or toxicity.We observed one partial response in a patient receiving thehighest dose of i.p. rIL-2, but we could not discern a correlationbetween clinical or laboratory findings (such as LAK activity,MNC numbers and phenotypes) and tumor response. Encouraging clinical responses have been reported with very low dosesof rIL-2 (6) but a laboratory correlation to response has notbeen demonstrated.
We had anticipated that for a given patient and dose levelrepeated infusions would result in increasing ascites cellularityand because of "vascular leak" increasing serum levels of IL-2.
Unexpectedly, three of four patients at the highest dose level(patients 7, 8, and 9) experienced the accumulation of largevolumes of essentially cell-free ascites after receiving severalinfusions of i.p. rIL-2. This phenomenon was observed prior tothe infusion of LAK. This reduction of peripheral IL-2 levelsover time is in contrast to that seen by others with three timesa day dosing, where during a second cycle of i.p. rIL-2 peripheral levels were actually higher than during the first cycle despitethe same treatment dose (30). The therapy-induced ascites weobserved was associated with low levels (AUC <10, peak <1unit/ml) or an absence of detectable IL-2 in the serum and highi.p. IL-2 levels (2000->25,000 units/ml 48 h post-IL-2 infusion). It is possible but not likely that this extreme hypocellu-larity is due to simple dilution or sampling error from peritonealpockets of fluid. Another possible explanation for the absenceof cells in the fluid is that the activated MNC become adherent
to the peritoneal surface. A subpopulation of IL-2-activatedMNC (1-4%) are known to become adherent. This enrichedpopulation of cells has been shown to be CD3 negative CD56positive, to have higher proliferative potential, and to be morecytotoxic (37). Another possibility was that ascites fluid wastoxic to the cells. To test this, we activated normal lymphocyteswith rIL-2 in the presence of this ascites fluid but toxic effectson normal MNC were not detected (data not shown). Thehypocellularity of ascites in our patients may be related to thelow peripheral IL-2 levels noted, but the mechanism of such aninteraction is unclear.
In conclusion, this trial of i.p. rIL-2 with LAK resulted in adose-limiting toxicity of symptoms related to ascites accumulation. In a subsequent phase II trial using this schedule a doseno greater than 8 x IO6units/m2 body surface area/dose should
used. Leukapheresis could perhaps be more productive if starteda day earlier. Peripheral IL-2 levels generally varied with doselevel and i.p. levels early in the treatment period. Later measurements demonstrated decreasing peripheral IL-2 levels despite maintenance of the same i.p. dose. Intraperitoneal IL-2induced durable regional LAK activity which correlated withan increase in the percentage of MNC as well as the percentageof CDSo-positive MNC in the peritoneum. In addition, peripheral blood MNC were primed by i.p. IL-2 for lytic activity whichwas inducible with brief in vitro exposure to IL-2. This primingcorrelated with an increase in CD56-positive peripheral MNCand with a rebound lymphocytosis 48-72 h after i.p. rIL-2. Aclearer understanding of peritoneal changes after several infusions of i.p. rIL-2 will help improve the design of further clinicaltrials using i.p. immunotherapy.
ACKNOWLEDGMENTS
We wish to thank Pamela Vacek, Chris Blair, and Greg Goodwinfor computer and statistical support, Cheryl Chabot and the ClinicalResearch Center nurses for the care given the patients, and CathyLarsson, Franny Matthias, Cassandra Vertone, and Eva Champoux fortheir assistance in this project.
REFERENCES
1. Lotze. M. T., Cusler, M. C., and Rosenberg, S. A. Intraperitoneal administration of interleukin-2 in patients with cancer. Arch. Surg.. 121:1373-1379,1986.
2. Lurie, H., Rakovsky, E., Fenig. E., Davidovitz, J., and Adler. A. A pilotstudy of intraperitoneal recombinant interleukin-2 and ex vivo activatedintracavitary lymphocytes in patients with malignant peritoneal spread: I.Clinical aspects. Mol. Biother.. /: 163-169, 1989.
3. Chapman, P. B., Kolitz, J. E.. Hakes, T. B., Gabrilove, J. L., Weite, K.,Merluzzi, V. J., Engert A., Bradley, E. C., Konrad, M., and Mertelsmann,R. A phase I trial of intraperitoneal recombinant interleukin 2 in patientswith ovarian carcinoma. Invest New Drugs. 6: 179-188. 1988.
4. Lembersky. B., Baldisseri, M.. Kunschner. A., Seski, J., Zook, D.. Hammond.R.. Kowal, C.. and Kirkwood, J. Phase I-I1 study of intraperitoneal (IP) lowdose interleukin-2 (IL-2) in refractory stage III ovarian cancer (OC). Proc.Am. Soc. Clin. Oncol., S: 636. 1989.
5. Sugarbaker, P. H.. Oliff, L., and Graves, T. Phase I and pharmacokineticstudies—with intraperitoneal (IP) interleukin-2 (IL-2) in patients with peritonea) carcinomatosis from colon cancer. Proc. Am. Soc. Clin. Oncol.. 30:1500, 1989.
6. Roth. A., Lembersky, B., Kowal, C., Whiteside, T., Herberman, R., andKirkwood, J. Immunologie studies of loco-regional therapy with low doseinterleukin-2 (IL-2) in refractory stage III ovarian carcinoma (OC) and intransit metastatic melanoma (ITMM). Proc. Am. Soc. Clin. Oncol., 30:1461, 1989.
7. Melioli, G., Baldini. E.. Mingari. M. C., DeMaria, A., Sertoli, M. R.,Badellino F., Percivale, P.L., Catturich, A.. Bertoglio, S., Civalleri, D., Santi,L.. and Moretta, L. Phenotypic and functional characteristics of tumor-associated lymphocytes in patients with malignant ascites receiving intraperitoneal infusions of recombinant interleukin-2 (rII-2). Int. J. Cancer, 43:231-234. 1989.
8. Einhorn, N., Ling, P.. Einhorn, S., and Strander, H. A phase II study on
6309
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRAPERITONEAL rlL-2/LAK
escalating ¡nterferondoses in advanced ovarian carcinoma. Am. J. Clin. 22.Oncol.. 11:3-6, 1988.
9. Rambali. A.. Introna, M.. Coletta, F.. Landolfo, S., Colombo. N.. Mangioni.C., and Mantovani A. Intraperitoneal administration of interferon in ovarian 23.cancer patients. Cancer (Philadelphia). 56; 294-301. 1985.
10. Berek, J. S., Hacker, N. F.. Lichtenstein. A., Jung. T.. Spina, C.. Knox, R. 24.M., Brady, J., Greene. T., Ettinger. L. M.. Lagasse. L. D., Bonnern. E. M..Spiegel, R. J.. and Zighelboim, J. Intraperitoneal recombinant alpha-inter-feron for "salvage" immunotherapy in stage III epithelial ovarian cancer: agynecological oncology group study. Cancer Res.. 45: 4447-4453. 1985. 25.
11. D'Aquisto, R.. Markman, M., Hakes. T.. Rubin. S., Hoskins. W.. and Lewis, 26.J. L. A phase 1 trial of intraperitoneal recombinant gamma-interferon in 27.advanced ovarian carcinoma. J. Clin. Oncol., 6: 689-695. 1988.
12. Willemse. P. H., de Vries. E. G.. Oosterhuis. B. E.. Aalders. J. G.. Bouma.J., Mulder, N. H.. and Sleijfer. D. T. Intraperitoneal human r-lFN-2ab in 28.patients with stage III minimal residual ovarian cancer. Proc. Am. Soc. Clin.Oncol., S: 602. 1989.
13. Nardi, M., Cognetti. F., DellaGiulia. M.. Sternberg, C., Lombardi. A.. 29.Atlante. G.. Mottolese, M.. Natali. P. G.. and Calabresi. F. Intraperitonealr 2-interfcron (IFN) alternating wilh cisplatin (DDP) as salvage therapy forminimal residual disease ovarian cancer. Proc. Am. Soc. Clin. Oncol.. 8:612. 30.1989.
14. Repetto, L.. Alama. A., Chiara, S., Guido. T.. Conte, P. F., and Rosso. R.Intraperitoneally administered cytokines (IFN alpha2b and rHuTNF) inrefractory ovarian cancer: a clinical and biological evaluation. Proc. Am. Soc. 31.Clin. Oncol.. A:639. 1989.
15. Grimm. E. A., Mazumder. A.. Zhang. H. Z., and Rosenber, S. A. Lympho-kine- activated killer cell phenomenon. J. Exp. Med.. /55: 1823-1841. 1982. 32.
16. Mule, J. J.. Shu, S., Schwarz. S. S., and Rosenberg. S. A. Adoptive immunotherapy of established pulmonary métastaseswith LAK cells and recom- 33.binant interleukin-2. Science (Washington DC). 225: 1487-1489. 1984.
17. Mule, J. J., Shu, S.. and Rosenberg. S. A. The anti-tumor efficacy oflymphokine-activated killer cells and recombinant interleukin-2 in vivo. J.Immunol.. 135: 646-652, 1985.
18. Lafreniere. R.. Rosenstein, M. S., and Rosenberg. S. A. Optimal methods 34.for generating expanded lymphokine activated killer cells capable of reducingestablished murine tumors in vivo. J. Immunol. Methods. 94: 37-49, 1986.
19. Rosenberg. S. A., Lotze, M. T., Muul, L. M.. Chang. A. E., Avis, F. P., et 35.al. A progress report on the treatment of 157 patients with advanced cancerusing lymphokine-activated killer cells and interleukin-2 or high-dose interleukin-2 alone. N. Engl. J. Med.. 316: 889-897. 1987. 36.
20. Hawkins. M. IL-2/LAK: current status and possible future directions. Principles Pracl. Oncol. Updates, 3: 1-14, 1989.
21. Ottow, R. T., Steller, E. P., Sugarbaker. P. H.. Wesley. R. A., and Rosenberg. 37.S. A. Immunotherapy of intraperitoneal cancer with interleukin-2 and lymphokine-activated killer cells reduces tumor load and prolongs survival inmurine models. Cell. Immunol., 104: 366-376. 1987.
Cheever, M. A.. Thompson, J. A.. Kern. D. E., and Greenberg, P. D.lnterleukin-2 (IL-2) administered in vivo: influence of 1L-2 route and timingon T cell growth. J. Immunol.. 134: 3895-3900. 1985.Rossio. J. L.. Thurman, G. B.. Long, C., et al. The BRMP IL-2 referencereagent. Lymphokine Res., 5: 513-518, 1986.Moore, A. L., Grant. B. W., Dorighi, J. A., Belinson, J. A., Stewart, J. A.,and Alberimi. R. J. Effect of commercial peritoneal dialysis fluids on thelytic function of lymphokine-activated killer cells. J. Biol. Response Modif.,7.-401-408. 1988.Users Manual. Houston. TX: Math/Library IMSL, April 1987.SAS User's Guide: Statistics. Cary. NC: SAS Institute. 1985.
Muul. L. M. Director. E. P.. Hyatt. C. D.. and Rosenberg. S. A. Large scaleproduction of human lymphokine actived killer cells for use in adoptiveimmunolherapy. J. Immunol. Methods. 88: 265-275, 1986.Jadus, M. R.. Thurman. G. B., Mrowca-Bastin. A., and Yannelli. J. R. Thegeneration of human lymphokine-activated killer cells in various serum-freemedia. J. Immunol. Methods. 109: 169-174. 1988.Itoh. K., Tilden, A. B.. and Balch, C. M. Lysis of human solid tumor cellsby lymphokine-activated natural killer cells. J. Immunol.. 136: 3910-3915.1986.Urba. W. J.. Clark. J. W., Steis. R. G., Bookman, M. A.. Smith. J. W., II, etal. Intraperitoneal lymphokine-activated killer cell/interleukin-2 therapy inpatients with intra-abdominal cancer: immunologie Considerations. J. Nati.Cancer Inst.. 81: 602-611. 1989.Dedrick. R. L., Myers, C. E., Bungay, P. M., and DeVita, V. T. Pharmaco-kinetic rationale for peritoneal drug administration in the treatment ofovarian cancer. Cancer Treat. Rep., 62: 1-11, 1978.Grimm, E. A., and Wilson. D. J. The human lymphokine-activated killer cellsystem. Cell. Immunol.. 94: 568-578. 1985.Bold!. D. H., Mills. B. J.. Gemlo, B. T., Holden. H.. Meier. J.. Paietta, E.,McMannis, J. D.. Escobedo, L. V.. Sniecinski. I., Rayner, A. A., Hawkins.M. J., Atkins, M. B.. Ciobanu. N., and Ellis, T. M. Laboratory correlates ofadoptive immunotherapy with recombinant intcrlcukin-2 and lymphokine-activated killer cells in humans. Cancer Res.. 48: 4409-4416. 1988.Ortaldo. J. R.. and Longo D. L. Human natural lymphocyte effector cells:definition, analysis of activity, and clinical effectiveness. J. Nati. Cancer Insl..«0:999-1010. 1988.Yagita. M.. and Grimm. E. A. Current understanding of the lymphokine-activated killer cell phenomenon. Prog. Exp. Tumor Res., 32: 213-226,1988.Sondel, P. M., Hank, J. A., and Kohler. P. C. Status and potential ofinterleukin-2 for the treatment of neoplastic disease. Oncology, /: 41-48.1987.Melder. R. J., Whiteside, T. L.. Vujanovic, N. L., Hiserodt, J. C.. andHerberman. R. B. A new approach to generating antitumor effectors foradoptive immunotherapy using human adherent lymphokine-activated killercells. Cancer Res.. 48: 3461-3469. 1988.
6310
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1990;50:6302-6310. Cancer Res James A. Stewart, Jerome L. Belinson, Ann L. Moore, et al. Ovarian CancerInterleukin-2/Lymphokine-activated Killer Cells in Patients with Phase I Trial of Intraperitoneal Recombinant
Updated version
http://cancerres.aacrjournals.org/content/50/19/6302
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/50/19/6302To request permission to re-use all or part of this article, use this link
on August 3, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from