Embed Size (px)
Citation preview

Phase I, open-label, multi-ascending dose trial of avelumab (MSB0010718C), an anti-PD-L1 monoclonal antibody, in Japanese patients with advanced solid tumorsK. Shitara,1 Y. Yamada,2 K. Yoh,1 Y. Naito,1 S. Iwasa,2 N. Yamamoto,2 A. von Heydebreck,3 H. Achiwa,4 T. Doi1 1National Cancer Center Hospital East, Kashiwa, Chiba, Japan; 2National Cancer Center Hospital, Chuo-ku, Tokyo, Japan; 3Merck KGaA, Darmstadt, Germany; 4Merck Serono Co., Ltd., Meguro-ku, Tokyo, Japan
INTRODUCTION
Immune-based therapies in cancer: PD-1/PD-L1 pathway1
• Increased progression-free survival (PFS) and overall survival (OS) have been demonstrated in NSCLC and melanoma with immune checkpoint inhibitors2,3
– Durable antitumor responses and manageable safety profiles have been reported in a growing list of tumor types
• The programmed death-1 receptor (PD-1) and its ligand (PD-L1) are key therapeutic targets in the reactivation of the immune response against multiple cancers
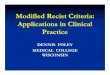
Avelumab* (MSB0010718C)• Key attributes (Figure 1)4
– Fully human anti-PD-L1 IgG1 antibody – Binds PD-L1
• Inhibits PD-1/PD-L1 interactions• Leaves PD-1/PD-L2 pathway intact
• ADCC may contribute to activity, as shown in preclinical models5
• Preliminary (n=28) safety, pharmacokinetic (PK), and efficacy data from a phase I dose-escalation trial (JAVELIN Solid Tumor; NCT01772004) have been previously reported – Doses up to 20 mg/kg once every 2 weeks were safely administered – Antitumor activity in lung, gastric, bladder, and other malignancies
• Here we report on the safety and tolerability of avelumab in a phase I dose-escalation study in Japanese patients with advanced solid tumors
Figure 1. Mechanism of action of avelumab
Immunemediators
T-cell mediatedimmune response
PD-1
PD-1PD-L1
PD-L1
AvelumabAvelumab
FcγRTumorCell
T Cell
NK Cell
Potential ADCCactivity
* Avelumab is the proposed international nonproprietary name (INN) for the anti-PD-L1 monoclonal antibody (MSB0010718C).
OBJECTIVES
• Primary objectives of this phase I, open-label, dose-escalation study: – Assess the safety and tolerability of avelumab in Japanese patients with metastatic
or locally advanced solid tumors, including gastric cancer – Determine the maximum tolerated dose (MTD) administered as monotherapy by
investigating the occurrence of dose-limiting toxicities (DLTs)• Select secondary objectives:
– Characterize PK profile of avelumab – Evaluate tumor PD-L1 expression – Assess best overall response (BOR) and PFS time
METHODS
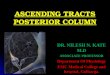
• JAVELIN Solid Tumor JPN (NCT01943461) is a phase I, open-label, multiple-ascending dose trial of avelumab in patients with metastatic or locally advanced solid tumors (ECOG PS 0-1 at trial entry) and consecutive parallel-group expansion in patients with gastric cancer (Figure 2)
• Avelumab dose escalation (standard 3+3 design) was performed at 3 doses (3, 10, and 20 mg/kg)
Figure 2. Study design
3.0 mg/kg
Dose levels
Dose-escalation part (standard 3 + 3 design)*
10.0 mg/kg
20.0 mg/kg
Up to 18 patients Up to 20 patients
10.0 mg/kg
Expansion part†
* After the first 3 weeks (ie, DLT observation period), the same dose of avelumab was administered once every 2 weeks until confirmed complete response (CR), confirmed progression, unacceptable toxicity, or withdrawal occurred.
† Until CR, confirmed progression, unacceptable toxicity, or withdrawal occurred.
• Dose-limiting toxicity (DLT) – Any grade ≥3 treatment-related adverse event (AE) occurring during the DLT evaluation
period – Confirmed by the safety monitoring committee to be relevant for the study-drug treatment – The DLT evaluation period was 3 weeks
• Treatment continued once every 2 weeks until confirmed complete response, progression, unacceptable toxicity, or withdrawal
• AEs were graded using NCI-CTCAE v4.0• Responses were assessed according to RECIST 1.1 and modified immune-related response
criteria (irRC)• Blood samples for analysis of PK parameters were collected within 6 hours before infusion
(trough value) and immediately after infusion was completed (peak value) on Days 15, 29, 43, 85, 127, and 169, as well as more frequently on Day 1 and during the first 2-week dosing period
RESULTS
• In total, 17 patients with advanced solid tumors were enrolled and treated with avelumab during the dose-escalation part of the trial (Table 1)
• Median treatment duration: 14.1 weeks (range, 4.0-56.0) – At least 6 weeks follow-up by October 29, 2014 – 5 patients remain on treatment at data cutoff, including 2 patients (11.8%) with durable
partial responses by RECIST of >18 weeks• Five, 6, and 6 patients were treated with 3, 10, and 20 mg/kg, respectively• All patients were evaluable for PK analysis
Table 1. Patient demographics and disease characteristics
Characteristics n=17
Median age, years (range) 62 (30, 74)
Gender, n (%) Male Female
10 (58.8)7 (41.2)
ECOG PS, n (%) 0 1
14 (82.4)3 (17.6)
Primary tumor, n (%) Gastric cancer Melanoma Non-small cell lung cancer Colorectal cancer Gastrointestinal stromal tumor Esophageal squamous-cell carcinoma Metastatic breast cancer
4 (23.5%)4 (23.5%)3 (17.6%)2 (11.8%)2 (11.8%)1 (5.9%)1 (5.9%)
Median time since first diagnosis, years (range) 2.9 (1.3, 22.3)
Median time since metastatic disease, months (range) 30.8 (3.75, 174.8)
Number of prior anticancer therapies, n (%) 1 2 3 ≥4
1 (5.9)2 (11.8)5 (29.4)9 (52.9)
Safety • There were no DLTs reported in the DLT analysis set (n=15) and a maximum tolerated dose
was not reached
• Table 2 provides a summary of the safety results
Table 2. Summary of safety results
Events TEAEs (n=17), n (%)
TEAE 16 (94.1)
TEAE, grade ≥3 2 (11.8)
Related TEAE 11 (64.7)
Related TEAE, grade ≥3 0
TEAE leading to permanent treatment discontinuation 0
Related TEAE leading to permanent treatment discontinuation 0
Serious TEAE 2 (11.8)
Related serious TEAE 0
TEAE leading to death 0
Related TEAE leading to death 0
TEAE of special interest 5 (29.4)
Related TEAE of special interest 5 (29.4)
TEAE, treatment-emergent adverse event
• Treatment-related treatment-emergent AEs (TEAEs; all grades) occurred in 64.7% (11/17) of patients (Table 3)
• No grade ≥3 TEAEs related to avelumab were reported
– Three grade ≥3 TEAEs deemed unrelated to avelumab occurred in 2 patients: increased aspartate aminotransferase, increased blood bilirubin, and hyponatremia
• TEAEs of special interest (potentially immune-related)
– Treatment-related infusion-related reactions (5)
– Maculopapular rash (1)
• There were no treatment-related deaths
Table 3. Treatment-related TEAEs, all grades
Events, n (%)Most common (>10%) treatment-related TEAEs,
all grades* (n=17)
Infusion-related reaction 5 (29.4)
Stomatitis 4 (23.5)
Maculopapular rash 4 (23.5)
Decreased WBC count 3 (17.6)
Pyrexia 2 (11.8)
Headache 2 (11.8)
Anemia 2 (11.8)
* All treatment-related TEAEs were grade 1 or 2.
PK profile• The PK profile of avelumab is summarized in Table 4
Table 4. PK parameters after first dose
Parameter, mean (SD) 3 mg/kg (n=5) 10 mg/kg (n=6) 20 mg/kg (n=6)
Cmax (µg/mL) 65.2 (13.7) 182 (35) 462 (61)
AUC0-tau (µg/mL*h) 5,586 (1,422) 21,400 (8,500) 48,300 (11,200)
t1/2 (h) 92 (26) 127 (34) 115 (14)
CL (L/h/kg) 0.524 (0.153) 0.453 (0.201) 0.377 (0.084)
Vz (L/kg) 67.2 (19.6) 75.7 (21.1) 61.8 (13.1)
Data as of October 10, 2014.
Figure 3. Comparison of PK parameters by ethnicity
1000
100
10
1240 48
Con
cent
ratio
n (m
g/m
L)
Time (h)
72 96 128 144 168 192 216 240 264 288 312 336
Mean concentration-time profiles following first infusion of avelumab
1.2
1.1
0.8
0.6
0.4
0.2
00
Mea
n cl
eara
nce
(SD;
mL/
h/kg
)
Dose (mg/kg)
5 10
Relationship between clearance and dose following first infusion of avelumab
A. B.
15 20
Japanese, 3 mg/kgJapanese, 10 mg/kgJapanese, 20 mg/kgCaucasian, 3 mg/kgCaucasian, 10 mg/kgCaucasian, 20 mg/kg
JapaneseCaucasian
• Serum concentration of avelumab over time and by dose (Figure 3A) and systemic clearance (Figure 3B) showed similar responses between Japanese and Caucasian patients
• The observed PK profile of avelumab was linear over the investigational dose range
Clinical activity of avelumab by dose• Confirmed partial responses to avelumab monotherapy (RECIST criteria) were observed in
11.8% (2/17) of patients (Table 5) – Tumor type of patient with PR at 3 mg/kg dose was melanoma – Tumor type of patient with PR at 10 mg/kg dose was esophageal squamous-cell
carcinoma (ESCC; Figure 5)• Stable disease was observed in an additional 12 patients (70.6%)
Table 5. Best overall response (BOR)
Confirmed BOR by RECIST
3 mg/kg (n=5)
n
10 mg/kg (n=6)
n
20 mg/kg (n=6)
n
Total (n=17)n (%)
Complete response (CR) 0 0 0 0
Partial response (PR) 1 1 0 2 (11.8)
Stable disease (SD) 3 5 4 12 (70.6)
Progressive disease (PD) 0 0 2 2 (11.8)
Not evaluable (NE) 1 0 0 1
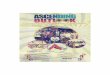
Figure 5. Complete response by irRC to avelumab in patient with ESCC
Baseline/screening Week 7 Week13
20.0 mm 11.0 mm 0.0 mm
• History: 59-year-old male patient with stage IV progressive disease after 3 prior lines of chemotherapy (5-FU/cisplatin; 5-FU/nedaplatin; paclitaxel)
• Outcome: irCR (PR by RECIST) for >18 weeks at cutoff
CONCLUSIONS
• Avelumab can be safely administered to Japanese patients in doses up to 20 mg/kg Q2W
• There were no DLTs reported in the DLT analysis set and a maximum tolerated dose was not reached
• The parameters Cmax and AUC were approximately proportional with dose, showed low variability, and were similar to those previously obtained in Caucasian patients3
• Durable partial responses (>18 weeks) were observed in 2 patients (11.8%)
• Avelumab 10 mg/kg Q2W has been studied in a phase Ib dose-expansion trial of Japanese patients with gastric cancer (JAVELIN Solid Tumor JPN [NCT01943461]; abstract #4047)
• Additional phase II/III studies to evaluate the clinical activity of avelumab at 10 mg/kg Q2W in select tumor types are currently underway
REFERENCES
1. Hamid O, Carvajal RD. Expert Opin Biol Ther. 2013;13(6):847-61.
2. Robert C, et al. N Engl J Med. 2015;372(4):320-30.
3. Rizvi NA, et al. Lancet Oncol. 2015;16(3):257-65.
4. Heery CR, et al. J Clin Oncol. 2014;32(Suppl 15):Abstract 3064.
5. Lepone LM, et al. AACR Annual Meeting. 2015:Abstract 1316.
ACKNOWLEDGMENTS
This trial was sponsored by Merck KGaA, Darmstadt, Germany and is part of an alliance between Merck KGaA and Pfizer. The authors would like to thank the patients, investigators, co-investigators, and the study teams at each of the participating centers and at Merck KGaA, Darmstadt, Germany and Merck Serono, Tokyo, Japan*. Medical writing support was provided by ClinicalThinking, Hamilton, NJ and funded by Merck KGaA, Darmstadt, Germany.
* A Japanese subsidiary of Merck KGaA, Darmstadt, Germany
DISCLOSURES
AvH is an employee and stockholder of Merck KGaA, Darmstadt, Germany; HA is an employee of Merck Serono Co., Ltd.*, Tokyo, Japan. These authors disclose the following relationships with Merck KGaA: YY, SI, and TD have received research funding; TD has provided consulting. All other authors have nothing to declare in relation to Merck KGaA.
*Merck Serono Co., Ltd. is a subsidiary of Merck KGaA, Darmstadt, Germany
Correspondence: K. Shitara, [email protected]
GET POSTER PDF
Copies of this poster obtained through Quick Response (QR) Code are for personal use only and may not be reproduced without permission from ASCO® and the author of this poster. For questions, please contact [email protected]
Poster Presentation at the 51st ASCO Annual Meeting, May 29-June 2, 2015; Chicago, Illinois. Abstract No. 3023.