Embed Size (px)
Citation preview

I nvestigational New Drugs 2, 311-314 (1984) �9 1984, Martinus Nijhoff Publishers. Printed in the Netherlands
Phase I evaluation of AT-125 single dose every three weeks
Sarah Taylor, Robert J. Belt, U. Joseph, Charles D. Haas and Barth Hoogstraten Department o f Medicine, Division o f Clinical Oncology, University o f Kansas Medical Center, Kansas City, Kansas 66103 and Kansas City Veterans Administration Medical Center, Kansas City, Missouri, U.S.A.
Key words: AT-125, acivicin, Phase I
Summary
A Phase I trial of AT-125 was completed for the bolus dose every three week schedule. Dose limiting toxicity was primarily central nervous system (CNS) in the form of ataxia, confusion, hallucinations and dysarthria. Although this was most severe at doses of 150 m g / m 2, lesser symptoms were reported at all dose levels.
Nausea and vomiting were moderate to severe at higher doses. Myelosuppression did not occur. This schedule is not recommended for Phase II studies until methods are developed to reduce drug-related CNS toxicity.
Introduction
AT-125((s, 5s) - amino-3-chloro-4,5 dihydro-5- isoxazole acetic acid, NSC 163501) - is a fermenta- tion derived amino acid antimetabolite isolated f rom streptomyces sviceus. Its biochemical mecha- nism of action is not fully understood. However, it has been found to be a potent inhibitor of a number of enzymes including cytidine 5 ' -triphosphate syn- thetase and L-glutamine dependent xanthine 5 ' - monophosphate aminase. AT-125 is structurally similar to glutamine and has been found to be a po- tent inhibitor of glutamine utilization by L-aspara- gine synthetase as well as several other glutamine
requiring enzymes (1). Ant i tumor activity against L1210 leukemia was
first shown in 1973 with optimal in vitro cell killing after continuous 72 h exposure (1). Results of murine tumor therapy showed a wide range of ac- tivity against P388 and L1210 leukemias as well as M5076 ovarian carcinoma. Anti tumor activity was also seen against a human breast and lung tumor xenograft, but not against colon tumor xenografts (2).
Drug related toxicities in large animals included vomiting, diarrhea, dehydration, anorexia and weight loss. Labora tory abnormalities included lymphocytopenia and thrombocytopenia. Single
doses were tolerated better than divided doses over several days. The toxic low dose in the dog on a daily • 1 schedule was 125 m g / m z (1). Based upon this a dose of 40 m g / m z was chosen as a starting dose. However, further preclinical data in large animals f rom Upjohn suggested this might be a tox- ic dose, therefore, we initiated our study at 20
2 m g / m . The only neurotoxicity observed in the dog and monkey testing done prior to the clinical trial was sedation and disorientation occurring at lethal and supralethal doses which caused death due to gastroinestinal toxicity (3).
Materials and methods
Phase I studies with AT-125 were initiated at the University of Kansas in 1979 at 20 m g / m 2 given in- travenously over 15 min and repeated every three weeks. Subsequent groups of three or more patients
Address for reprints: Sarah A. Taylor, M.D., University of Kansas Medical Center, Division of Clinical Oncology, 39th and Rainbow Blvd., Kansas City, KS 66103, U.S.A.

312
were escalated according to a modified Fibronacci schema to a final dose of 150 mg/m 2. Individual patient doses were escalated provided excessive toxicity was not observed. Patients experiencing ex- cessive toxicity had doses reduced by one dose level. Courses were given every three weeks. AT-125 was provided by the NCI in 25 mg vials of lyophilized drug.
Requirements for patient eligibility were histol- ogic proof of malignancy in which established forms of treatment were ineffective, solid tumor, life expectancy of 12 weeks or more, no treatment for three weeks prior to entry, recovery from any toxicity of prior treatment, adequate liver function with a bilirubin of less than 2.0 mg% and no clinical evidence of biliary obstruction, serum creatinine less than 2 mg%, and signed informed consent in keeping with the policies of the Human Experimen- tation Committees of the University of Kansas Medical Center and the Kansas City Veterans Ad- ministration Hospital.
Pretreatment evaluation included 1) a complete history and physical examination, which included documentation of measurable disease and signs and symptoms as well as performance status; 2) labora- tory studies which included complete blood count with white blood cell differential; platelet and reticulocyte count, urinalysis, BUN, creatinine, SGOT, LDH, alkaline phosphatase, uric acid, calcium, phosphorus, bilirubin (direct and total), bone marrow aspiration, and stool hematest; 3) in- dicated x-rays or scans. Evaluation during the study included weekly blood count with white blood cell differential and platelet count, weekly stool hema- test, SGOT, alkaline phosphatase, LDH, total and direct bilirubin, uric acid, calcium, phosphorus, urinalysis, BUN, and creatinine. Every three weeks and off study all weekly studies, history, physical and weight were repeated.
Plasma and urine samples were collected for pharmacokinetic analysis conducted by Upjohn Company. The results have been published sepa- rately (4).
A partial response was defined as a 50% or greater decrease in the sums of the products of all measurable tumors with no evidence of increasing disease for at least four weeks. No changes or stable
disease included lesions that decreased in size by less than 50~ or enlarging lesions that increased less than 25% in size. Increasing disease was de- fined as an unequivocal increase of at least 25~ in size of measured lesions and /o r the appearance of new lesions.
Results
Seventeen patients received 42 evaluable courses of AT-125 (range 1-8) . The median performance status was 60 Karnofsky (30-100) and the median age was 60 years (range 40-78) . Fourteen men and three women were treated. Seven patients had received prior chemotherapy and eight patients had received both prior chemotherapy and radiothera- py. Patients had a variety of solid tumors: colorec- tal carcinoma (5), squamous cell carcinoma of the head and neck (1), pancreatic carcinoma (1), pros- tate carcinoma (1), renal cell carcinoma (2), non small cell carcinoma of the lung (3), small cell car- cinoma of the lung (2), squamous cell carcinoma unknown primary (1) and fibrosarcoma (1).
Dose limiting CNS toxicity was seen in three of four patients (3/5 courses) treated at 150 mg/m 2. This consisted of dysarthria, lethargy, ataxia, con- fusion, and visual hallucinations which began 24 hours after a dose and lasted three to four days. Pa- tients were completely disabled during this time but recovered without treatment. CNS evaluations in- cluding EEG's, CAT scans and lumbar punctures were unremarkable. One patient with the most severe CNS toxicity had no measurable AT-125 in the CSF approximately 48 hours after a 150 mg/m 2 dose. Lesser degrees of CNS toxicity including nightmares, 'large thoughts ' , confusion, headaches and hallucinations were encountered at the lowest doses (Table 1). One patient on Valium was treated at 150 mg/m 2 and had no CNS symptoms. Two pa- tients at 120 mg/m 2 were given Valium in an at- tempt to prevent neurotoxicity. Both patients had confusion and hallucinations.
Other toxicities included dose dependent mode- rate to occasionally severe nausea and vomiting (11 courses), mild diarrhea (2 courses), and occasional transient rises in liver function tests (3 courses).
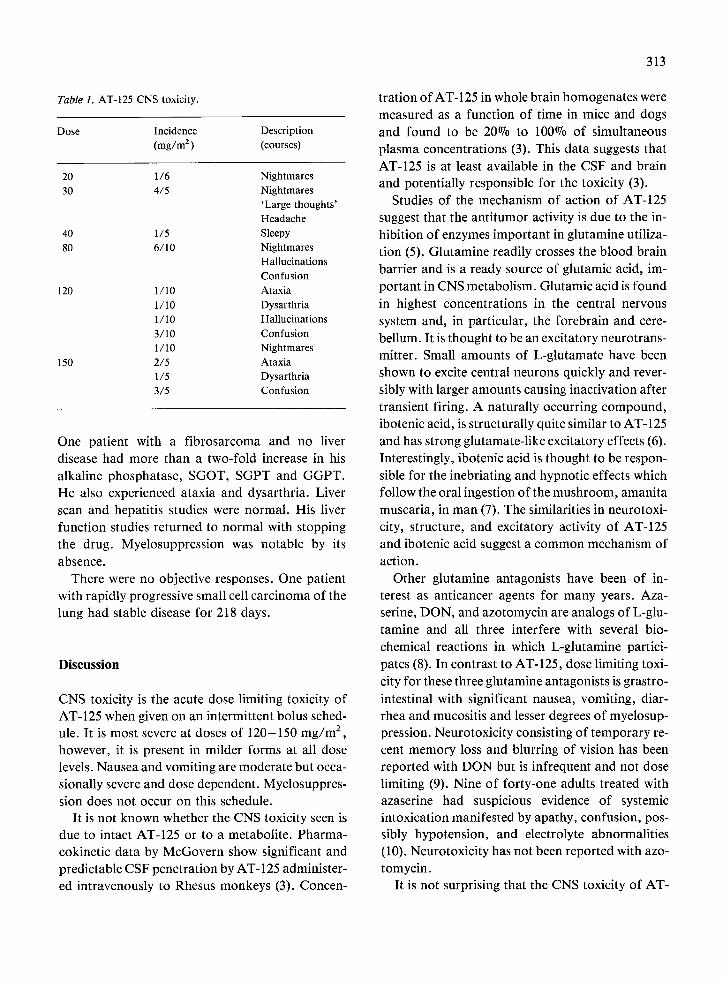
Table 1. AT-125 CNS toxicity.
Dose Incidence Description (mg/m 2 ) (courses)
20 1/6 Nightmares 30 4/5 Nightmares
'Large thoughts' Headache
40 1/5 Sleepy 80 6/l 0 Nightmares
Hallucinations Confusion
120 1/10 Ataxia 1 / 10 Dysarthria 1 / 10 Hallucinations 3/10 Confusion 1 / 10 Nightmares
150 2/5 Ataxia 1/5 Dysarthria 3/5 Confusion
One patient with a fibrosarcoma and no liver disease had more than a two-fold increase in his alkaline phosphatase, SGOT, SGPT and GGPT. He also experienced ataxia and dysarthria. Liver scan and hepatitis studies were normal. His liver function studies returned to normal with stopping the drug. Myelosuppression was notable by its absence.
There were no objective responses. One patient with rapidly progressive small cell carcinoma of the lung had stable disease for 218 days.
Discussion
CNS toxicity is the acute dose limiting toxicity of AT-125 when given on an intermittent bolus sched- ule. It is most severe at doses of 120-150 mg/m 2, however, it is present in milder forms at all dose levels. Nausea and vomiting are moderate but occa- sionally severe and dose dependent. Myelosuppres- sion does not occur on this schedule.
It is not known whether the CNS toxicity seen is due to intact AT-125 or to a metabolite. Pharma- cokinetic data by McGovern show significant and predictable CSF penetration by AT-125 administer- ed intravenously to Rhesus monkeys (3). Concen-
313
tration of AT- 125 in whole brain homogenates were measured as a function of time in mice and dogs and found to be 20% to 100% of simultaneous plasma concentrations (3). This data suggests that AT-125 is at least available in the CSF and brain and potentially responsible for the toxicity (3).
Studies of the mechanism of action of AT-125 suggest that the antitumor activity is due to the in- hibition of enzymes important in glutamine utiliza- tion (5). Glutamine readily crosses the blood brain barrier and is a ready source of glutamic acid, im- portant in CNS metabolism. Glutamic acid is found in highest concentrations in the central nervous system and, in particular, the forebrain and cere- bellum. It is thought to be an excitatory neurotrans- mitter. Small amounts of L-glutamate have been shown to excite central neurons quickly and rever- sibly with larger amounts causing inactivation after transient firing. A naturally occurring compound, ibotenic acid, is structurally quite similar to AT-125 and has strong glutamate-like excitatory effects (6). Interestingly, ibotenic acid is thought to be respon- sible for the inebriating and hypnotic effects which follow the oral ingestion of the mushroom, amanita muscaria, in man (7). The similarities in neurotoxi- city, structure, and excitatory activity of AT-125 and ibotenic acid suggest a common mechanism of action.
Other glutamine antagonists have been of in- terest as anticancer agents for many years. Aza- serine, DON, and azotomycin are analogs of L-glu- tamine and all three interfere with several bio- chemical reactions in which L-glutamine partici- pates (8). In contrast to AT-125, dose limiting toxi- city for these three glutamine antagonists is grastro- intestinal with significant nausea, vomiting, diar- rhea and mucositis and lesser degrees of myelosup- pression. Neurotoxicity consisting of temporary re- cent memory loss and blurring of vision has been reported with DON but is infrequent and not dose limiting (9). Nine of forty-one adults treated with azaserine had suspicious evidence of systemic intoxication manifested by apathy, confusion, pos- sibly hypotension, and electrolyte abnormalities (10). Neurotoxicity has not been reported with azo- tomycin.
It is not surprising that the CNS toxicity of AT-
314
125 was not predicted by the preclinical studies. Neurologic toxicity in man is not in general well predicted by the animal screens. The central ner- vous toxicity of the alkylating agents in man was predicted by preclinical studies while the CNS toxi- city and peripheral neuropathy due to the vinca alkaloids was not (11).
Two separate Phase I studies of AT-125 as well as an additional Phase II study found more toler- able neurotoxicity using the five day schedule (12-14). It is not known whether the CSF levels seen would be cytotoxic to an intracranial malig- nancy. However, Phase II testing of AT-125 using the more tolerable five day schedule should be undertaken and particularly in CNS malignancies. We do not recommend the intermittent bolus schedule for Phase II testing.
Acknowledgment
This study was supported by NCI grant # NCI- CM-RFP-74-01.
References
1. Clinical brochure for AT-125(NSC-163501,(L-( 5, 5S)-ami- no-3-chloro-4, 5-dihydro-5-isoxazole acetic acid)) April 1979
2. Houchens DP, Ovejera AA, Sheridan MA, Johnson RK, Bogden AE, Neil GL: Therapy for mouse tumors and human tumor xenografts with the antitumor antibiotic AT-125. Cancer Treat Rep 63:473-475, 1979
3. McGovern JP, Stewart JC, Elfring GL, Smith RB, Soares
N, Wood JH, Poplack DG, Von Hoff DD: Plasma and cere- brospinal .quid pharmacokinetics of acivicin in Ommaya reservoir-bearing Rhesus monkeys. Cancer Treat Rep 65: 1333-1341, 1982
4. McGovern P, Pratt EA: Pharmacokinetics of acivicin (AT-125) in the phase I clinical trials. (Abstract) Proc Am Soc Clin Oncol 22:356, 1981
5. Jayaram NH, Cooney DA, Ryan JA, Neil GL, Dion RL, Bono VH: L-[ 5,5S]-amino-3 chloro-4,5-dihydro-5 isoxazole acetic acid (NSC 163501): a new amino acid antibiotic with the properties of an antagonist of L-glutamine. Cancer Chemother Rep 59:481-491, 1975
6. Physiological Reviews (2) 54:418-540, 1974 7. Waser PG: The pharmacology of amanita muscaria. In:
Efron DH, Holmstedt B, Kline NS (eds): Ethnopharmacol- ogic Search for Psychoactive Drugs. U.S. Public Health Ser- vices Publication No. 1645, Washington D.C., pp 419-439, 1967
8. Catane R, Von Hoff DD, Glaubiger DL, Muggia FM: Azaserine, DON, and Azotomycin: three diazo analogs of L- glutamine with clinical antitumor activity. Cancer Treat Rep 63:1033-1038, 1979
9. Kovach JS, Eagan RT, Powis G, Rubin J, Creagan EG, Moertel CG: Phase I and pharmacokinetics of DON. Cancer Treat Rep 65:1031-1036, 1981
10. Ellison RR, Karnofsky DA, Sternberg SS, Murphy ML, Bur- chenal JH: Clinical trials of O-Diazoacetyl-L-Serine (Azaserine) in neoplastic disease. Cancer 7:801-814, 1954
11. Woolley PV, Schein PS: Clinical pharmacology and phase I trial design. In: Methods in Cancer Research, Vol. XVII, Academic Press, 1979, pp 177-198
12. Murphy WK, Burgess MA, Valdivieso M, Bodey GP: Phase I evaluation of acivicin (AT-125). (Abstract) Proc Am Soc Clin Oncol 1:23, 1982
13. Adolphson C, Bedikian AY, Stroehlein JR, Karlin DA, Bodey GP, Hickey RC: Phase II evaluation of acivicin (AT-125, NSC 163501) in patients with advanced colorectal cancer. (Abstract) Proc Am Soc Clin Oncol 1:96, 1982
14. Ohnuma T, Sridhar K, Goldsmith M, Bruckner H, Chahi- nian AP, Holland JF: A phase I study of acivicin (AT-125). (Abstract) Proc Am Soc Clin Oncol 22:382, 1981