Embed Size (px)
Citation preview

PHASE 3 RANDOMISED TRIAL
EVALUATING 2 SHORT RADIATION
SCHEMES FOR PROSTATE CANCER: impact of bladder dose on acute urinary toxicity
Sebastian Wilhelm Robert Benque Student number: 01303297
Supervisor(s): Prof. Dr. Valérie Fonteyne, Dr. Karel Decaestecker
A dissertation submitted to Ghent University in partial fulfillment of the requirements
for the degree of Master of Medicine in Medicine
Academic year: 2017 – 2018


“The author and the promotor give the permission to use this thesis for consultation
and to copy parts of it for personal use. Every other use is subject to the copyright
laws, more specifically the source must be extensively specified when using results
from this thesis.”
Date
Sebastian Wilhelm Robert Benque Prof. Dr. Valérie
Fonteyne (Student) (promotor)


Table of Contents Abbreviations ............................................................................................................................ 1
Abstract ..................................................................................................................................... 2
Background ........................................................................................................................... 2
Materials and Methods ........................................................................................................ 2
Results ................................................................................................................................... 3
Conclusion ............................................................................................................................ 3
Samenvatting ............................................................................................................................ 4
Inleiding ................................................................................................................................. 4
Methode en materialen ....................................................................................................... 4
Resultaten ............................................................................................................................. 5
Conclusie ............................................................................................................................... 5
Introduction ............................................................................................................................... 6
Anatomy ................................................................................................................................ 6
Epidemiology ........................................................................................................................ 6
Classification and Prognosis .............................................................................................. 6
External Beam Radiotherapy Techniques ....................................................................... 8
Hypofractionated Radiotherapy ....................................................................................... 10
Radiotherapy Induced Toxicity ........................................................................................ 11
Research Question ............................................................................................................ 12
Materials and Methods .......................................................................................................... 13
Study Design ...................................................................................................................... 13
Treatment ............................................................................................................................ 16
Regions of Interest ............................................................................................................. 18
Dosimetric Parameters ..................................................................................................... 20
Statistical Considerations ................................................................................................. 21
Results ..................................................................................................................................... 23

Patients ............................................................................................................................... 23
Acute Urinary Toxicity ....................................................................................................... 25
Clinical Risk Factors ......................................................................................................... 26
Hypotheses Generating: Deriving Bladder Dose-Volume Constraints ..................... 28
Cut-Off Analysis ................................................................................................................. 29
Discussion .............................................................................................................................. 32
Patient related risk factors ............................................................................................... 32
Dosimetric parameters ..................................................................................................... 33
Conclusion .............................................................................................................................. 37
References ............................................................................................................................. 38

1
Abbreviations
3D-CRT 3D conformal radiotherapy
ADT Androgen deprivation therapy
BED Biological equivalent dose
BEV Beam’s eye view
BPH Benign prostatic hyperplasia
CT Computer tomography
CTCAE v4.0 Common Terminology Criteria for Adverse Effects 4.0
DVH Dose-volume histogram
EAU European Association of Urology
EBRT External beam radiotherapy
GI Gastro-intestinal
HFRT Hypofractionated radiotherapy
IBD Inflammatory bowel disease
IMAT Intensity modulated arc therapy
IMRT Intensity modulated radiotherapy
IPL Intraprostatic lesion
LHRH Luteinizing hormone-releasing hormone
LINAC Linear accelerator
LQ Linear quadratic
MLC Multi-leaf collimator
MRI Magnetic Resonance Imaging
NSAA Non-steroidal anti-androgen therapy
OAR Organs at risk
PC Prostate cancer
PSA Prostate specific antigen
PTV Planning target volume
QoL Quality of life
RT Radiotherapy
RTOG Radiation Therapy Oncology Group
SIB Simultaneous integrated boost
TURp Trans-urethral resection of the prostate
WHO World Health Organization

2
Abstract
Background
Randomised trials, comparing conventional dose radiotherapy with hypofractionated
radiotherapy (HFRT), demonstrated the non-inferiority of HFRT regarding relapse free survival
for low and intermediate risk prostate cancer (PC) patients. The risk of developing toxicity
remains acceptable with HFRT. Based on the results of these trials, HFRT can be considered
as a standard of care for localized PC. With proven effectiveness of different HFRT schedules,
side effects determine which HFRT schedule to apply. Therefore, a prospective phase III trial
was started at the Ghent University Hospital in 2013 in which two different hypofractionated
schemes in PC are studied:
- 56 Gy delivered in 4 weeks (Arm A)
- 67 Gy delivered in 5 weeks (Arm B).
An interim safety analysis of the first 160 patients demonstrated the safety of both regimens.
Nevertheless, the incidence of GI (gastro-intestinal) and urinary toxicity is not negligible and
warrants further follow up and research.
This thesis focuses on the evaluation of correlations between dose received by different parts
of the bladder and incidence of acute urinary toxicity. For those regions of the bladder in which
a correlation was found, dose-volume histogram (DVH) and constraints are derived.
Materials and Methods
A phase III trial started at Ghent University Hospital in 2013 and 346 patients are to be included
in the trial. Patients with localised PC are randomly assigned to two groups. The first group
receives 16 fractions with four fractions (3.5 Gy per fraction, total dose of 56 Gy) per week.
The second group receives 25 fractions with 5 fractions (2.69 Gy per fraction, total dose of
67.25 Gy) per week. The correlation between patient characteristics and urinary toxicity was
examined. For the evaluation of dose-volume associations from different parts of the bladder
and urinary toxicity, the following structures were delineated on CT-scans: urethra, bladder
wall (which was further subdivided into anterior, posterior, left and right bladder wall), trigone,
left and right ureter orifices. The dosimetric data up to 65 Gy was considered because higher
dose-volume parameters were not always available. Afterwards the volume receiving dose x
(Vx) from each treatment were converted to the corresponding biological equivalent dose
(BED). As a result, the Vx expressed as BEDs for both groups could be pooled for further
analysis.
Hypotheses generating was done with a student’s t-test. The variables that were found to be
significant with the student’s-t test were further analysed with a logistic regression to find the

3
optimal dosimetric cut-off points to define dose volume constraints. The results of the logistic
regression were used to create the DVHs of the bladder sub volume.
Results
Nicotine usage and trans-urethral resection of the prostate (TURp) procedure decreased the
overall risk of urinary toxicity. Anticoagulation medication and hypercholesterolemia
medication however increased the risk of developing acute urinary toxicity.
For generating hypotheses, the following toxicities were evaluated: retention, incontinence and
nocturia at three months post-RT with cut-offs at grade ≥ 2.
Significant correlation between the dose of the bladder and bladder wall (V25-V65) and
retention grade ≥ 2 three months post-RT was found. These results were used to create the
DVHs of the bladder wall for 5%, 10%, 15% and 20% probability for retention three months
post-RT.
Conclusion
Further research is needed to define robust predictive parameters for acute urinary toxicity
after HFRT.

4
Samenvatting
Inleiding
Recent onderzoek toont aan dat gehyrofractioneerde radiotherapie (HFRT) niet inferieur is aan
conventionele radiotherapie (RT) met betrekking tot de ziektevrije overleving van
prostaatkankerpatiënten met een laag en gemiddeld risico. Het risico op toxiciteit bij HFRT is
aanvaardbaar. Op basis van deze onderzoeken kan het gebruik van HFRT als
standaardbehandeling voor gelokaliseerde prostaatkanker overwogen worden. De effectiviteit
van verschillende HFRT-schema’s is aangetoond. De bijwerkingen moeten nu bepalen welk
HFRT-schema het best wordt toegepast. Hiervoor werd in 2013 een fase III trial gestart in het
universitaire ziekenhuis Gent (UZ Gent), waarbij twee gehypofractioneerde schema’s worden
vergeleken:
- 56 Gy toegediend gedurende 4 weken (Arm A)
- 67 Gy toegediend gedurende 4 weken (Arm B)
De veiligheid van die twee HFRT-schema’s is aangetoond door een tussentijdse
veiligheidsanalyse. De incidentie van gastro-intestinale en urinaire toxiciteit is echter niet
verwaarloosbaar en noodzaken verdere opvolging en onderzoek.
In deze masterproef wordt de correlatie tussen de stralingsdosis op verschillende regio’s van
de blaas en het voorkomen van acute urinaire toxiciteit bestudeerd. Voor de regio’s waar een
correlatie gevonden wordt, worden dosis-volume histogrammen (DVH) en constraints
opgesteld.
Methode en materialen
In 2013 is een fase III onderzoek van start gegaan in het universitaire ziekenhuis Gent (UZ
Gent), waarbij 346 patiënten met gelokaliseerde prostaatkanker geïncludeerd zijn. Tot nu toe
is het onderzoek op 160 patiënten uitgevoerd. De patiënten zijn over twee groepen
gerandomiseerd. De eerste groep ondergaat 16 fracties met vier fracties (3,5 Gy per fractie en
een totale dosis van 56 Gy) per week. De tweede groep ondergaat 25 fracties met 5 fracties
(2,69 Gy per fractie en een totale dosis van 67,25 Gy) per week. De correlatie tussen de
patiënten karakteristieken en de urinaire toxiciteit worden onderzocht. Voor de evaluatie van
de dosis-volume parameters van verschillende delen van de blaas en de urinaire toxiciteit
worden de volgende structuren afgelijnd op CT-scans: urethra, blaaswand (verder
onderverdeeld in anterieure, posterieure, linker en rechter blaaswand), trigonum en linker en
rechter ureteropeningen. De dosimetrische gegevens tot 65 Gy worden in de analyse
opgenomen, omdat de hogere dosis-volume parameters niet altijd beschikbaar waren. Daarna
worden de volumes die dosis x krijgen (Vx) van elke arm omgerekend tot de biologisch

5
equivalente dosis (BED). De Vx van beide armen, uitgedrukt als BED, worden hierdoor
vergelijkbaar en zijn samengevoegd voor verder onderzoek.
Het genereren van hypothesen wordt met de student’s t-toets gedaan. De variabelen die
significant zijn, worden met behulp van een logistische regressie geanalyseerd om de optimale
dosimetrische cut-off’s te vinden. Aan de hand van die resultaten worden DVH's van de
blaasregio’s opgesteld.
Resultaten
Nicotinegebruik en transurethrale resectie van de prostaat (TURp) verminderen het risico op
acute urinaire toxiciteit. Anticoagulatie medicatie en hypercholesterolemie verhogen echter het
risico op acute urinaire toxiciteit. Volgende toxiciteitparameters worden voor het genereren van
hypothesen gebruikt: retentie, incontinentie en nocturie op drie maanden na de RT met cut-
off’s van graad ≥ 2.
Er wordt een significante correlatie tussen de dosis op de blaas en blaaswand (V25-V65) en
de retentie graad ≥ 2 op drie maanden na HFRT gevonden. Aan de hand van die resultaten
worden DVHs opgesteld van de blaaswand voor 5%, 10%, 15% en 20% kans op retentie drie
maanden na HFRT.
Conclusie
Verder onderzoek is nodig naar voorspellende parameters voor acute urinaire toxiciteit na
HFRT.

6
Introduction
Anatomy
The prostate is an organ situated inferior of the bladder, anterior of the rectum and posterior
of the prostatic venous plexus. It surrounds the urethra while it passes through the
genitourinary diaphragm. The seminal vesicles are located posterior superior of the prostate
(1). A fibrous capsule surrounds the prostate. The cavernous nerves are situated at the
posterior and at the anterior lateral sides (2). The anatomical position around the urethra as
well as the vicinity of the bladder causes urinary symptoms in case of disease.
Epidemiology
PC is the most frequent cancer, besides skin cancer, in men with an incidence of more than
200 cases per 100000 men in Northern and Western Europe. There has been a recent
increase in incidence in all European countries and mostly in the younger age group (35-64
years) (3).
Classification and Prognosis
PC is staged according to the 2009 TNM classification of malignant tumours of PC and the
European Association of Urology (EAU) risk group classification (Table 1) (4,5). Relapse free
survival and mortality is correlated with the EAU risk group classification (6).
Table 1: The table of the risk groups for localized prostate cancer as defined in the report of the
European Association of Urology (EAU) and D’amico et al. (8). The table is borrowed from Nicolas
Mottet et al. (4).
Low-risk Intermediate-risk High-risk
Definition
PSA < 10 ng/mL
and GS < 7
and cT1-2a
PSA 10–20 ng/mL
or GS 7
or cT2b
PSA > 20 ng/mL
or GS >7
or cT2c
any PSA
any GS
cT3–4 or cN+
Localised Localised Localised Locally advanced
Abbreviations: GS = Gleason score; PSA = prostate-specific antigen.
Localised prostate cancer (PC) is cancer which is confined to the prostate and has not yet spread to
other parts of the body.
Locally advanced PC is cancer which has spread to other parts of the body.

7
Overall, PC has a good prognoses with a cancer-specific survival of 100% for low risk PC, 96%
for medium risk and 91% for high risk patients as seen in Figure 1 (7).
Treatment
There are different treatment options for patients with PC, depending on the risk group. The
possibilities are active surveillance, surgery, or radiotherapy (RT).
For patients with low-risk PC who have a 20 years PC-specific survival of 80-90% active
surveillance is a valuable option to avoid toxicity inherent to most treatment options. It is
important that this patient group receives close follow-up (4).
Patients with low-, intermediate- and high-risk PC may receive a radical prostatectomy as
treatment. If there is a risk of more than 5% of nodal metastases (Briganti nomogram, MSKCC,
or Roach formula), a pelvic lymph node dissection is indicated.
An alternative to surgery is radiotherapy (RT) such as external beam radiotherapy (EBRT) or
brachytherapy. In EBRT the radiation source is located outside the patient. Contrary to
brachytherapy, where the radiation source is implanted in the patient.
Figure 1: shows that the European Association of Urology (EAU) risk group classification is
correlated with the cancer-specific mortality post-radiotherapy (RT). The figure is borrowed from
D’Amico et al. (6).

8
For patients with intermediate-risk or high-risk PC, as defined in Table 1, androgen deprivation
therapy (ADT) is added in combination with EBRT (4).
In this thesis we will focus on RT and more specifically EBRT.
External Beam Radiotherapy Techniques
RT uses ionizing radiation to kill cancerous cells. The ionizing radiation transfers some of its
energy to the tissue it passes through. The dose delivered to the tissue is given in Gray (Gy).
The unit Gray is defined as the radiation energy (in Joule) that is absorbed by 1 kg of mass.
The ionizing radiation can damage the cell’s deoxyribonucleic acid (DNA). Double strand
breaks (DSB) of the DNA are implicated in the cell killing. If a cell has more than one DSB it is
difficult for the cell to repair the damage. This can as a consequence lead to apoptosis (8).
In EBRT medical linear accelerators (LINACs) are being used. Medical LINACs can generate
electron or photon beams between 1 MeV and 25 MeV. The LINACs work through accelerating
electrons. The LINAC can create a photon beam by directing the electrons onto a target (high
atomic number) where they are transformed to bremsstrahlung or braking radiation. This
bremsstrahlung is then used to irradiate the target. The electron beam is used for superficial
located tumours, whilst the photon beam can be used for deeper targets (9). For the treatment
of PC photon beams are being used.
Because it is difficult to compare the dose distribution of all the regions of interest between
different radiation schemes, the data is reduced to dose-volume histograms (DVHs). DVHs
represent the volume of a target or organ at risk that receives a certain dose. Ideally 100% of
the tumour region receives 100% of the dose. In contrast, the dose to the organs at risk should
be as low as possible to reduce the risk of inducing toxicity. Figure 2 shows an example of a
DVH of the bladder, the rectum and the planning target volume (PTV).

9
To minimize the dose to healthy tissue, different methods of delivering the radiation dose have
been developed.
3D-conformal RT (3D-CRT), intensity modulated RT (IMRT) and intensity modulated arc
therapy (IMAT) are different forms of EBRT. In 3D-CRT a multi-leaf collimator (MLC) and a
variable number of beams is used. The MLC mimics the shape of the tumour in beam’s eye
view (BEV). Consequently, the dose on the surrounding organs at risk (OAR) can be reduced,
while the dose to the tumour can be increased. With IMRT further dose escalation to the targets
can be obtained. IMAT is a form of IMRT in which the LINAC rotates around the patient. IMRT
implies the use of multiple beams with different beam angles and per beam angle different
segments. IMRT also allows to perform a Simultaneous Integrated Boost (SIB) to the dominant
intraprostatic lesion (IPL) resulting in further dose escalation to the tumour bearing site (10).
Summation of dose delivered by different beams with different shapes due to changes in MLC
results in an optimal dose distribution with high dose to the target volume, in our case the
prostate, while minimizing the dose to the normal tissue surrounding the target volume (11).
When compared to 3D-CRT the risk of developing rectal toxicity is significantly decreased with
IMRT. The impact of 3D-CRT versus IMRT on urinary toxicity is less clear (12).
IMRT is the standard technique used for treating patients with PC at Ghent university Hospital.
Figure 2: The planning target volume (PTV) receives almost 100% of the delivered dose,
while the organs at risk (OAR), bladder and rectum, receive a lower dose per volume. This
dose volume histogram (DVH) is borrowed from Cheng et al. (11).

10
Hypofractionated Radiotherapy
Randomised trials demonstrate that a higher radiation dose (dose ≥ 74 Gy) shows better long-
term biochemical outcomes when compared to low dose RT (13,14).
Traditionally a dose of 74-80 Gy in 2 Gy fractions has been used in the treatment of PC. This
results in a treatment time of 7-8 weeks. However, in recent years evidence has shown that a
shorter treatment time with a higher dose per fraction might be as effective as the traditional
approach. This is more convenient for the patient and lowers the treatment cost while rate of
tumour control is not compromised. High doses per fractions might unfortunately be associated
with higher late-term complications, such as vascular injury and chronic inflammation. But
recent developments such as IMRT and IMAT have increased the dose that can be delivered
to the target, whilst minimizing the dose to the OAR. This made hypofractionation a new safe
possibility for some tumours.
To compare different treatment RT schemes linear-quadratic (LQ) formalism is used. The LQ-
model is
𝑆 = exp (−𝐷 (α +β𝐷
𝑛)).
Where S is survival of the cells, D is the total dose and n is the number of fractions. The α/β-
ratio is the dose needed for which the linear term (α) and the quadratic term (β) are responsible
for the same amount of cell deaths.
The equation shows that the linear term is independent of the fraction rate, whereas the
quadratic term depends on the fraction rate (8,15).
To quantify the dose/fractions dependencies, the α/β-ratio is used in the LQ model. Early
responding normal tissues with a high α/β-ratio are less sensitive to changes in number of
fractions than late responding tissues with low α/β-ratio (15). There is evidence that the α/β-
ratio values for PC are between 1.0 and 1.7 Gy, which is lower than for other tumours (16).
Therefore, it might be possible to use hypofractionated RT (HFRT) treatments and shorten the
treatment duration while maintaining the high biological equivalent tumour doses.
Recently, four randomised trials, comparing conventional dose radiotherapy with HFRT,
demonstrated the non-inferiority of HFRT regarding biochemical and clinical relapse free
survival for low- and intermediate-risk PC patients (17–20).
Although increased toxicity is reported, the risk of developing toxicity remains acceptable with
HFRT (17–19). Based on the results of these trials, HFRT can be considered as a standard of
care for localized PC.

11
Radiotherapy Induced Toxicity
The major OAR to take into consideration when irradiating the prostate are the bladder and
rectum. Many studies have investigated the correlation between dose and toxicity.
For gastro-intestinal (GI) complications, a clear dose volume relationship has been described
and long-term reduction in toxicity has been achieved by using appropriate rectal constraints
(21). Data concerning impact of dose on urinary toxicity or erectile function, in contrast, are
scarce (22).
The relationship between the dose to the bladder and the urinary toxicity is still unclear (23).
There is some evidence that the bladder DVHs have an impact on the acute and late urinary
toxicity, but there are also studies that show no relationship (24,25).
As the incidence of urinary toxicity is higher than the incidence of GI toxicity it is of importance
to perform further research to minimize the rate of urinary toxicity for patients who receive
EBRT for PC (26). A better understanding of factors that are associated with urinary toxicity
might reduce the incidence of it.
Patient related factors such as diabetes mellitus and smoking, have been linked to urinary
toxicity (27–29). Anticoagulation therapy has also been associated with an increased risk of
developing late urinary toxicity (30). The presence of baseline symptoms increases the
probability of having post-RT symptoms which correlates with late urinary toxicity (31–33). A
prior transurethral resection of the prostate (TURp) and acute urinary toxicity for example
contribute to the late GU toxicity (31).
Therapy related factors, such as radiation dose, have been shown to have an impact on the
acute urinary toxicity as well (23,33). It is evident that different parts of the bladder receive
different doses (23,34). Studies show that the urinary symptoms are mainly related to
irradiation of the trigone, the urethra and the bladder neck and not the bladder itself (22,35,36).
Alterations in fraction dose, as is the case in HFRT, is also accompanied by an increased risk
of developing acute and to a lesser extend late urinary toxicity (19,37).
With proven effectiveness of different HFRT schedules, side effects determine which HFRT
schedule to apply. Therefore, a prospective phase III trial was started at the Ghent University
Hospital in 2013 in which two different hypofractionated schemes in PC are studied:
- 56 Gy delivered in 4 weeks (Arm A)
- 67 Gy delivered in 5 weeks (Arm B).
An interim safety analysis was planned after inclusion of the first 160 patients to decide whether
the study could be continued. This interim analysis demonstrated the safety of both regimens

12
regarding GI toxicity. Nevertheless the incidence of GI and urinary toxicity is not negligible and
warrants further follow up (38).
Research Question
As part of the above mentioned interim safety analysis of a phase III trial urinary toxicity was
evaluated. This thesis focuses on evaluation of correlation between the dose received by
different parts of the bladder and incidence in acute urinary toxicity. For those regions of the
bladder were a correlation is found, DVH constraints are derived. Also, patient related factors
are taken into account.

13
Materials and Methods
This study was done as part of a randomized controlled phase III trial. In this paper the
correlation between spatial dose predictors, clinical characteristics and acute urinary toxicity
was studied. Acute urinary toxicity was defined as the toxicity occurring during or within the
first three months post-RT.
Study Design
Eligibility
The primary inclusion criterium was a histological proven adenocarcinoma of the prostate
without clinical evidence of positive lymph nodes or metastases (cT1-cT4cN0cM0). The
patients must be eligible to receive EBRT as primary treatment with or without ADT depending
on tumour characteristics. The World Health Organization (WHO) performance status had to
be two or less. Another primary tumour was an exclusion criterion, except for basal cell
carcinoma or a diagnosis of other primary tumours more than five years ago. All patients had
to sign an informed consent.
Endpoints of the Study
The primary endpoint was GI toxicity occurring during the first three months after HFRT.
Secondary endpoints were acute and late urinary (including erectile dysfunction), late GI
toxicity, where late toxicity was defined as toxicity occurring within the first two years post-RT.
Toxicity was scored by the Common Terminology Criteria for Adverse Effects 4.0 (CTCAE
v4.0) and the Radiation Therapy Oncology Group (RTOG) criteria as defined in Table 2 (39).
The definition for nocturia and dysuria can be found in Table 3.
Quality of life (QoL), biochemical control, disease free survival, distant metastasis free survival,
PC specific survival and overall survival were also secondary endpoints.

14
Tab
le 2
: T
he t
oxic
ity d
efin
itio
n a
ccord
ing to
th
e C
om
mo
n T
erm
inolo
gy C
rite
ria o
f A
dvers
e E
ffe
cts
4.0
(C
TC
AE
) (3
9).
G
rad
e
1
2
3
4
5
Urg
en
cy
Pre
sen
t L
imitin
g in
str
um
enta
l A
DL
;
me
dic
al m
anag
em
ent
ind
ica
ted
- -
-
Fre
que
ncy
Pre
sen
t L
imitin
g
instr
um
enta
l A
DL
;
me
dic
al m
anag
em
ent
ind
ica
ted
- -
-
Ha
em
atu
ria
Asym
pto
matic;
clin
ica
l o
r d
iag
nostic
obse
rva
tion
s
only
;
inte
rve
ntio
n
not
indic
ate
d
Sym
pto
ma
tic;
urin
ary
ca
thete
r o
r
bla
dd
er
irrig
ation
in
dic
ate
d;
limitin
g in
str
um
enta
l A
DL
Gro
ss h
em
atu
ria
; tr
ansfu
sio
n,
IV
me
dic
ation
s
or
hospita
liza
tion
indic
ate
d;
ele
ctive
e
nd
osco
pic
,
radio
log
ic o
r o
pera
tive
inte
rve
ntio
n
indic
ate
d;
limitin
g s
elf c
are
AD
L
Life-t
hre
ate
nin
g
co
nse
qu
ence
s;
urg
ent
radio
log
ic o
r o
pera
tive
inte
rve
ntio
n in
dic
ate
d
De
ath
Incon
tine
nce
Occa
sio
na
l (e
.g., w
ith
co
ug
hin
g,
sn
ee
zin
g,
etc
.),
pad
s
not
indic
ate
d
Sp
on
tan
eou
s;
pad
s
indic
ate
d;
limitin
g in
str
um
enta
l A
DL
Inte
rve
ntio
n in
dic
ate
d (e
.g., c
lam
p,
co
llag
en
inje
ctio
ns);
o
pe
rative
inte
rve
ntio
n in
dic
ate
d;
limitin
g s
elf
care
AD
L
- -
Re
ten
tio
n
Urin
ary
, su
pra
pu
bic
or
inte
rmitte
nt
ca
the
ter
pla
cem
ent
not
indic
ate
d;
to v
oid
with
so
me r
esid
ua
l
Pla
cem
ent of u
rina
ry, sup
rap
ubic
or
inte
rmitte
nt
ca
the
ter
pla
cem
ent
indic
ate
d;
med
ica
tion
indic
ate
d
Ele
ctive
o
pe
rative
o
r ra
dio
log
ic
inte
rve
ntio
n i
ndic
ate
d;
su
bsta
ntia
l
loss o
f aff
ecte
d k
idne
y f
unctio
n o
r
ma
ss
Life-
thre
ate
nin
g
co
nse
qu
ence
s;
org
an
failu
re;
urg
ent
ope
rative
in
terv
entio
n
indic
ate
d
De
ath
Ab
bre
via
tion
s:
AD
L=
activitie
s o
f d
aily
liv
ing.

15
Tab
le 3
: T
he t
oxic
ity d
efin
itio
n o
f n
octu
ria
an
d d
ysu
ria.
Gra
de
1
2
3
4
5
No
ctu
ria
Tw
ice
B
ladd
er
vo
idin
g
at
nig
ht
pre
-
thera
py o
r 2-3
tim
es
post-
thera
py
Bla
dd
er
vo
idin
g
4-6
tim
es
at
nig
ht
(le
ss
than
on
ce p
er
hou
r)
Bla
dd
er
vo
idin
g m
ore
than
6 t
imes
- D
eath
Dysu
ria
Slig
ht
dis
com
fort
durin
g m
ictio
n a
nd n
o
me
dic
ation
ne
ede
d
Loca
l a
na
esth
etic
nee
de
d (
incl. b
ladd
er
sp
asm
)
Na
rco
tics
nee
de
d
(in
cl. b
ladd
er
sp
asm
,
pelv
ic
pain
) a
nd
se
ve
re
ste
no
sis
wh
ere
T
UR
o
r
dila
tatio
n is n
ee
de
d
Bla
dd
er
obstr
uctio
n
(no c
lot)
De
ath
Ab
bre
via
tion
s:
TU
R =
tra
nsure
thra
l re
se
ction
.

16
Sample Size Calculations
The study was designed to include 2 stages. The sample size for both stages was calculated
separately. An upper limit of 40% of acute CTCAE v4.0 and RTOG GI toxicities grade ≥ 2 with
an expected rate of 25% was chosen for stage 1. This was done with a one-stage Fleming-
A’Hern design. A power β of 0.83 (with a one-sided α-level of 0.0038) was obtained with 72
patients per group. A sample size of 160 patients was set for stage 1 to account for a dropout
of 10%. If a GI toxicity grade ≥ 2 in 22/72 patients was observed the treatment arm was to be
rejected.
For stage 2 a upper limit of 35% of acute GI toxicities grade ≥ 2 was chosen with an expected
rate of 25%. A power β of 0.86 (with a one-sided α-level of 0.0049) was obtained with 155
patients per group. If a GI toxicity grade ≥ 2 in 45/155 patients was observed the treatment
arm was to be rejected. A sample size of 346 patients was set for stage 1 and stage 2 combined
to account for a dropout of 10%.
Toxicity Assessment
The patients’ medical history was taken at admission with a standardised questionnaire. It
included the following: colitis, Crohn disease, inflammatory bowel disease (IBD),
haemorrhoids, diabetes mellitus, hypertension, nicotine usage and previous abdominal
surgeries.
The GI and urinary toxicity was evaluated pre-RT, during and at the end of EBRT as well as
one and three months post-RT. Every urinary symptom that occurred was scored.
The overall acute toxicity was defined as the highest-grade toxicity of all individual toxicities
during and post-RT up to 3 months pooled together.
Treatment
Radiation Therapy
All patients underwent pre-treatment imaging, consisting of a planning computer tomography
(CT) scan and Magnetic Resonance Imaging (MRI) unless the patient could not have an MRI
due to medical contraindications. Image fusion wass needed to aid the delineation. To facilitate
the image fusion process, all patients were scanned in treatment position. The images were
taken after filling their bladder and after active emptying of the rectum. The Syntegra® (version
1.2b, Philips) software packet was used for image fusion. The fusions were based on the pelvic
bone structure and prostate anatomy. The planning in both treatment groups was equivalent.
The clinical target volume (CTV) was defined as the prostate and the seminal vesicles. The
seminal vesicles were excluded from the CTV at 50 Gy if the probability of invasion was less
than 15%. The Roach equation was used to calculate the probability of invasion (40). The PTV

17
was a 5 mm isotropic expansion around the CTV. If an IPL was visualized on MRI, it was
delineated separately for a SIB without an additional margin. No patient received radiation to
the pelvic lymph nodes. Additionally, the following OAR were delineated: rectum, sigmoid
colon, small intestines, bladder, urethra and the femoral heads.
Two different treatment schemes were used. The first group received 16 fractions with four
fractions (3.5 Gy per fraction, total dose of 56 Gy) per week (Monday, Tuesday, Thursday and
Friday). The second group received 25 fractions with 5 fractions (2.69 Gy per fraction, total
dose of 67.25 Gy) per week (Monday to Friday).
As explained above we can assume an α/β-ratio of 1.5 Gy (16). Using the following formula,
we can calculate the equivalent dose in 2 Gy fractions.
𝐵𝐸𝐷2 𝐺𝑦 =𝐷𝑡𝑜𝑡𝑎𝑙 (𝐷𝑓𝑟𝑎𝑐𝑡𝑖𝑜𝑛 + 𝛼/𝛽)
2 + 𝛼/𝛽
𝐵𝐸𝐷2 𝐺𝑦 is the biological equivalent dose (BED) for 2 Gy fractions, 𝐷𝑡𝑜𝑡𝑎𝑙 is the total dose in the
original fraction scheme, 𝐷𝑓𝑟𝑎𝑐𝑡𝑖𝑜𝑛 is the dose per fraction and 𝛼/𝛽 is 1.5 Gy. The equivalent
dose for 16 fractions is 80 Gy and for 25 fractions 80.5 Gy. Therefore, the doses in both arms
can be considered to be biochemically equivalent.
The planning objectives for both targets and organs at risk can be found in Table 4 and Table
5.
Table 4: Planning objectives for both protocols.
16 fractions 25 fractions
Minimum Median Minimum Median
PTV (Gy) 52.6(72)/50.8(68) 56 62.8(72)/60.6(68) 67
CTV (Gy) 55 (78) 56 66 (78) 67
IPL (Gy) 56 (80) 57.6 (84) 67 (80) 69 (84)
The numbers between brackets represent the equivalent dose in 2 Gy fractions (𝐵𝐸𝐷2 𝐺𝑦)
calculated for an α/β ratio of 1.5 for the IPL, CTV and PTV.
Abbreviations: PTV=planned target volume; CTV=clinical target value; IPL=intraprostatic
lesion.

18
Table 5. Planning constraints for both protocols. Maximum dose allowed in organs at risk
(OAR).
OAR 16 fractions 25 fractions
Maximum Mean Maximum Mean
Rectum (Gy) 57.6 43.3 (52) 66.9 51.4 (52)
Sigmoid (Gy) 57.6 43.3 (52) 66.9 43.3 (52)
Small intestine
(Gy)
51.7 63.3
Bladder (Gy) 59.5 69.3
Femoral heads
(Gy)
43.6 50
The numbers between brackets represent the equivalent dose in 2 Gy fractions (BED2 Gy)
calculated for an α/β ratio of 1.5.
Abbreviations: PTV=planned target volume.
Patients were treated on an Elekta LINAC (Crawley, UK) using 6 MV-photons with a MLC. The
patients were asked to use a daily rectal suppository and to have a filled bladder before
treatment. During treatment, the patients were positioned in supine position with knee support.
The positioning was controlled with a daily cone-beam CT.
Androgen Deprivation Therapy
Patients with intermediate-risk or high-risk PC, as defined in Table 1, were eligible for ADT in
combination with EBRT. ADT should be used concomitantly and start simultaneously with or
before EBRT. In a neo-adjuvant setting it may start 2-3 months before the first irradiation.
Duration of the ADT is 6 or 24 months depending on the risk group.
Luteinizing hormone-releasing hormone (LHRH) agonists are the first choice for ADT. Patients
that are ineligible to or refuse to take LHRH agonists may receive non-steroidal anti-androgen
therapy (NSAA). Orchiectomy is another possibility.
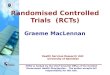
Regions of Interest
For evaluation of dose-volume associations between different parts of the bladder and urinary
toxicity, the following structures were delineated: urethra, bladder wall (which was further
subdivided into anterior, posterior, left and right bladder wall), trigone, left and right ureter
orifices according to the bladder map, used for evaluation of the bladder at cystoscopy (Figure
3) (41).

19
Pinnacle³ was used for delineating these regions of interest (ROI) on the planning-CT.
The bladder and the clinical target volume (CTV) were prospectively delineated. In most cases,
the urethra within the CTV was also prospectively delineated.
The urethra outside of the CTV, bladder wall, left and right walls, anterior and posterior walls,
distal ureters and the trigone were retrospectively delineated using the following definitions:
1) Urethra
We looked at the prostatic urethra, which is limited by the upper and lower border of
the prostate. The prospectively delineated urethra was taken and limited superiorly by
the upper border of the CTV and inferiorly 1 cm below the CTV. If the urethra outside
of the CTV was not prospectively delineated, the MRI was used for the delineation.
2) Bladder wall
The total bladder wall is a hollow structure created in 2 steps. First an aid structure, the
inner bladder wall, was made by contracting the delineated whole bladder volume with
5 mm. Thereafter this aid structure was substracted from the delineated whole bladder
volume (42). Although the normal thickness of the bladder is less (43,44). The mean
bladder wall thickness in men is 3.33 mm and in men with lower urinary tract symptoms
(LUTS) and benign prostate hypertrophy (BPH) 3.67 mm (43). We assumed a greater
Figure 3: The interior of the bladder seen from anterior. The figure is borrowed from
European Association of Urology (43).

20
thickness because of the possible movement of the bladder between treatments (45).
An important remark is that the trigone and the bladder neck show relatively little
movement (45). We also didn’t account for the fact that the bladder wall thickness
changes with changing volumes of the bladder (44).
3) Left and right bladder wall
The bladder wall was split in half by measuring the bladder at its broadest point latero-
laterally. This point was then used to mark the middle line. We then delineated the right
bladder wall by contouring the bladder up to the defined middle line and contracted it
whilst avoiding the interior of the inner bladder wall and the exterior of the outer bladder
wall to get the right bladder wall. Again a 5 mm thickness between inner and outer
bladder volume was applied. The left bladder wall was delineated by contracting the
right bladder wall from the total bladder wall.
4) Anterior and posterior bladder wall
The same procedure as for the creation of the left and right bladder wall was applied
after defining a midline based on the highest point cranio-caudally.
5) The ureter orifices
The distal ureters were defined as the ureteral orifices and the ureter 1 cm more cranial.
6) Trigone of the bladder
The volume between the ureteral orifices and the urethral orifice was manually
delineated and defined as the trigone (35,46).
Dosimetric Parameters
The volume receiving a certain dose is expressed as Vx, where x is the dose received by the
volume. The volume is expressed relatively to the total volume of the delineated region. For
each patient and each ROI, the Vx for 1 to 65 Gy was calculated from the planning CTs. The
dosimetric data only up to V65 was considered because a higher Vx was not always available.
Afterwards the Vx from each treatment arm was mapped with the corresponding Vx converted
to BED, calculated with the formula
𝐵𝐸𝐷2 𝐺𝑦 =𝐷𝑡𝑜𝑡𝑎𝑙 (𝐷𝑓𝑟𝑎𝑐𝑡𝑖𝑜𝑛+𝛼/𝛽)
2+𝛼/𝛽,
as explained earlier. For the acute toxicity of the bladder a 𝛼/𝛽-ratio of 10 Gy may be assumed
(47). After this mapping the dosimetric data of both arms was expressed in BED for 2 Gy and
was therefore comparable.
When we look at both arms, we see that the highest BED that we can calculate in both arms
is 68 Gy (Table 6). And because we studied the dosimetric data in 5 Gy steps, only toxicity up
to 65 Gy could be considered.

21
The Vx expressed as BEDs for both groups was pooled for further analysis.
Statistical Considerations
The following acute urinary toxicity scores were analysed: urgency, dysuria, frequency,
haematuria, incontinence, nocturia and retention and overall toxicity. The toxicity data was
dichotomized with a cut-off of grade ≥ 2 and grade ≥ 3.
The impact of clinical risk factors on the overall urinary toxicity after three months was studied
with a univariate logistic regression. For binary variables dummy variables were generated.
Clinical characteristic that were evaluated are: age at diagnosis, weight at diagnosis,
abdominal surgery, diabetes, hypertension, haemorrhoids, nicotine use, TURp,
antihypertensive medication, anticoagulation, hypercholesterolemia medication, CTV volume,
PTV volume , PSA, pelvic lymph node dissection and ADT. CTV volume, PTV volume, prostate
specific antigent (PSA), age and weight were seen as continuous variables. A p-value ≤ 0.05
was considered significant.
Table 6: The dose for both arms (16 and 25 fractions) expressed as biological equivalent
dose (BED).
25 fractions (Arm B) 16 fractions (Arm A)
Dose (Gy) BED (Gy) Dose (Gy) BED (Gy)
65 68 65 76
60 62 60 69
55 56 55 62
50 50 50 55
45 44 45 48
40 39 40 42
35 33 35 36
30 28 30 30
25 23 25 24
20 18 20 19
15 13 15 14
10 9 10 9
5 4 5 4
1 1 1 1
Abbreviations: BED = biological equivalent dose.

22
Because it was not known which ROI correlates with which type of urinary toxicity, we aimed
to generate hypotheses. First the normality of all dosimetric variables was checked with the
Shapiro-Wilk’s test. Then the student’s t-test was used to compare the different types of toxicity
as categoric group variable and the continuous dose-volume parameters as independent
variables. We considered a two-tailed p-value ≤ 0.05 to be statistically significant
The variables that were found to be significant with the student’s-t test were further analysed
to find the optimal dosimetric cut-off points for dose-volume constraints. A univariate logistic
regression was used to calculate the probabilities of having 5%, 10%, 15% and 20% toxicity.
These probabilities were used to create the DVHs of the significant ROI. The odds ratio (OR)
of showing toxicity were also calculated.
R version 3.4.1 and SPSS version 22 were used for the analysis.

23
Results
Patients
Of the 160 patients included in this analysis it was only possible to retrieve the dosimetric
parameters of 140 patients, 71 in arm A and 69 in arm B. One patient died before the one-
month follow-up.
The patient and tumour characteristics of these 140 cases are shown in Table 7.
Table 7: Summary of patient and tumour characteristics for 16 and 25 fractions and both
groups combined.
16 fractions 25 fractions All Patients
n = 71 n = 69 n = 140
Patient characteristics
Age at diagnosis (years)
Median (range) 71 (51-83) 71 (50-84) 71 (50-84)
Karnofsky Performance Score
Median (Range) 90 (70-100) 90 (70-100) 90 (70-100)
Weight (kg)
Median (Range) 80 (58-116) 80.5 (58-118) 80 (58-118)
IBS
Yes 1 (1%) 2 (3%) 3 (2%)
No 70 (99%) 67 (97%) 137 (98%)
Abdominal Surgery
Yes 26 (37%) 28 (41%) 54 (39%)
No 45 (63%) 41 (59%) 86 (61%)
Diabetes
Yes 15 (21%) 9 (13%) 24 (17%)
No 56 (79%) 60 (87%) 116 (83%)
Hypertension
Yes 40 (56%) 42 (71%) 82 (59%)

24
No 31 (44%) 27 (39%) 58 (41%)
Haemorrhoids
Yes 16 (23%) 15 (22%) 31 (22%)
No 55 (77%) 54 (78%) 109 (78%)
Nicotine use
Yes 8 (11%) 6 (9%) 14 (10%)
No 63 (89%) 63 (91%) 126 (90%)
Medication: antihypertensive
Yes 38 (54%) 40 (58%) 78 (56%)
No 33 (46%) 29 (42%) 62 (44%)
Medication: anticoagulation
Yes 29 (41%) 29 (42%) 58 (41%)
No 42 (59%) 40 (58%) 82 (59%)
Medication: hypercholesterolemia
Yes 32 (45%) 28 (41%) 60 (43%)
No 39 (55%) 41 (59%) 80 (57%)
Tumour characteristics
Stage
T1 27 (38%) 25 (36%) 52 (37%)
T2 30 (42%) 30 (44%) 60 (43%)
T3 14 (20%) 12 (18%) 26 (18%)
T4 - 1 (1%) 1 (1%)
Unknown - 1 (1%) 1 (1%)
PSA (ng/ml)
Median (range) 10.93 (4-83) 11.98 (0.8-77) 11.15 (0.8-83)
CTV (cc)
Median (range) 58 (27-263) 64 (21-144) 63.5 (21-263)

25
PTV (cc)
Median (range) 139 (80-413) 144 (67-224) 141.0 (67-413)
ADT
Yes 58 (82%) 48 (70%) 106 (76%)
No 13 (18%) 21 (30%) 34 (24%)
ADT (months)
Median (range)
PLND
Yes 36 (51%) 28 (41%) 64 (46%)
No 35 (49%) 41 (59%) 76 (54%)
TURp
Yes 11 (16%) 7 (10%) 18 (13%)
No 60 (84%) 62 (90%) 122 (87%)
Abbreviations: IBS = inflammatory bowel syndrome, PSA = prostate specific antigen, CTV =
clinical target volume, PTV = planned target volume, ADT = androgen deprivation therapy,
PLND = pelvic lymph node dissection, TURp = transurethral resection of the prostate.
Acute Urinary Toxicity
Table 8 gives an overview of the observed toxicities. 94 patients (67.1%) showed symptoms
of acute ≥ 2 urinary toxicity, and only 14 patients (10.0%) had grade ≥ 3 toxicity. No grade 4
toxicity was observed. Because of the limited amount of grade ≥ 3 toxicity, only grade ≥ 2
toxicity was considered in the further analysis. The most frequently seen acute urinary toxicity
grade ≥ 2 three months post-RT was nocturia with 31 cases (22.1%). Retention was observed
in 13 patients (9.3%) and incontinence in 7 patients (5.0%) three months post-RT. Because
the small number of events for urgency, dysuria, frequency and haematuria, it was chosen to
exclude those parameters from the further analysis.

26
Important to notice is that the prevalence of urinary toxicity during RT was much higher than
the toxicity pre-RT and toxicity observed in the months following RT. During RT retention was
the most frequent toxicity (53 patients, 37.8%).
Clinical Risk Factors
Clinical risk factors were studied with univariate logistic regression to see if they influence the
incidence of overall urinary toxicity during the first three months. The results are shown in Table
9. For one patient was the overall toxicity not available.
Table 8: The number and percentage of patients with acute urinary toxicity (Grade ≥ 2) for
the different analysed toxicity types. Overall toxicity is shown for grade ≥ 2 and grade ≥ 3.
The 140 patients used for the analysis were included.
Toxicity Pre-RT During RT One Month Post-
RT
Three Months Post-
RT
Urgency (≥2) 2 (1.4%) 19 (13.6%) 9 (6.5%) 4 (2.9%)
Dysuria (≥2) - 22 (15.7%) 7 (5.0%) 4 (2.9%)
Frequency (≥2) 4 (2.9%) 40 (28.6%) 13 (9.4%) 4 (2.9%)
Haematuria (≥2) 3 (2.1%) 1 (0.7%) - 2 (1.4%)
Incontinence
(≥2)
9 (6.4%) 8 (5.7%) 6 (4.3%) 7 (5.0%)
Nocturia (≥2) 16 (11.4%) 51 (36.4%) 41 (29.5%) 31 (22.1%)
Retention (≥2) 18 (12.9%) 53 (37.8%) 25 (18.0%) 13 (9.3%)
Overall Toxicity (≥2) 94 (67.1%)
Overall Toxicity (≥3) 14 (10.0%)
We used a cut-off of ≥ 2 for the different urinary toxicities. For the overall toxicities we looked
at the cut-offs of ≥ 2 and ≥ 3.
Abbreviations: RT = radiotherapy

27
Table 9: Univariate logistic regression of patient characteristics with acute overall urinary
toxicity ≥ 2 at three months post-RT.
Variable Comparison n OR (95% CI) p-value
Age Continuous - 1.048 (0.996-1.102) 0.069
Weight Continuous - 1.008 (0.979-1.039) 0.582
Abdominal Surgery Yes 54 1.000 -
No 85 0.813 (0.389-1.698) 0.582
Diabetes Yes 24 1.000 -
No 115 0.650 (0.239-1.768) 0.389
Hypertension Yes 81 1.000 -
No 58 0.649 (0.317-1.330) 0.237
Haemorrhoids Yes 30 1.000 -
No 109 0.708 (0.287-1.742) 0.452
Nicotine use Yes 14 1.000 -
No 125 3.171 (1.028-9.778) 0.045
TURp Yes 18 1.000 -
No 122 3.071 (1.119-8.427) 0.029
Antihypertensive Yes 78 1.000 -
No 61 0.649 (0.317-1.327) 0.236
Anticoagulation Yes 58 1.000 -
No 81 0.379 (0.175-0.823) 0.014
Hypercholesterolemia Yes 60 1.000 -
No 79 0.348 (0.161-0.756) 0.008
CTV Continuous - 1.015 (0.999-1.032) 0.062
PTV Continuous - 1.009 (0.999-1.018) 0.068
PSA Continuous - 0.988 (0.962-1.015) 0.394
PLND Yes 64 1.000 -
No 75 1.351 (0.663-2.756) 0.407
ADT Yes 106 1.000 -
No 33 0.561 (0.250-1.258) 0.160
Abbreviations: IBS = inflammatory bowel syndrome, PSA = prostate specific antigen, CTV
= clinical target volume, PTV = planned target volume, ADT = androgen deprivation therapy,
PLND = pelvic lymph node dissection, TURp = transurethral resection of the prostate.
Variables in bold are significant.

28
Nicotine usage decreased the overall risk for urinary toxicity. The TURp procedure also
decreased the risk. Anticoagulation medication and hypercholesterolemia medication however
increased the risk of developing acute urinary toxicity.
Hypotheses Generating: Deriving Bladder Dose-Volume Constraints
To calculate the DVHs the patients of both arms were pooled. This was done because of the
low prevalence of urinary symptoms in both arms separately (Table 8). The BED for 2 Gy is
used in both arms. Therefore, the doses were biochemically equivalent, and can be compared.
Because of the data available and the formula for the BED, V65 is the highest dosimetric
parameter (Table 6).
The impact of dose-volume parameters of different bladder regions on urinary toxicity was
unknown. Therefore, we looked for possible correlations between the bladder dose-volume
parameters and different urinary toxicities. Because the small number of events for urgency,
dysuria, frequency and haematuria, it was chosen to exclude those parameters from the further
analysis and only retention, incontinence and nocturia were considered for analysis.
First, the normality of all continuous volume-dose variables was tested with the Shapiro-Wilk’s
test. Normality was seen for all dosimetric parameters. Therefore, the student’s t-test was used
for further analysis and hypotheses generating.
The following toxicities were evaluated: retention, incontinence and nocturia at three months
post-RT with cut-offs at grade ≥ 2. A cut-off of grade ≥ 3 was not considered for analysis
because there were too few events during the first 3 months post-RT.
Because one patient died before the first post-RT follow-up, only 139 patients were considered
in the analysis.
Retention grade ≥ 2 three months post-RT is correlated with the anterior wall (V20-V65), the
posterior wall (V60-V65), the right wall (V25-V65), the left wall (V25-V65), the bladder (V25-
V65), the bladder wall (V20-V65) and the right ureteral orifice (V60-V65). Because of the
similarities in pattern between anterior and posterior wall, right and left wall and the bladder
and bladder wall, it was chosen to only use the bladder wall as surrogate for the other
structures. The bladder wall was chosen rather than the bladder given that a higher level of
significance is found for the bladder wall.
It appears that only the urethra (V35-V50) significantly correlated with nocturia grade ≥ 2 at 3
months post-RT. For incontinence grade ≥ 2 at 3 months post-RT only the left ureteral orifice
(V45-V50) is significantly correlated.

29
In the further analysis, only retention and nocturia grade ≥ 2 three months post-RT were
considered, because only retention and nocturia showed statistical and clinical significant
results.
Cut-Off Analysis
The dose-volume parameters that were found to be significant with the student’s t-test were
further analysed as continuous variables with univariate logistic regression. This way, the
impact of a change in the dose volume-parameters of the bladder wall on the occurrence of
retention grade ≥ 2 at three months post-RT could be analysed. The impact of a change in the
dose volume-parameters of the urethra on the occurrence of nocturia grade ≥ 2 at three months
post-RT was also analysed.
Table 10 illustrates the correlation between the bladder wall (V20-V65) and the retention grade
≥ 2 three months post-RT. There was no significant effect of the bladder wall V20 on the
retention.
Table 10: Univariate logistic regression models for acute grade ≥ 2 retention: relative
volume of the bladder wall receiving a certain dose (V20-V65). The logistic regression for
V20 is not significant.
Variable OR (95% CI) p-value AUC (95% CI)
V20 1.036 (1.000-1.073) 0.052 0.692 (0.536-0.848)
V25 1.042 (1.007-1.079) 0.019 0.714 (0.555-0.873)
V30 1.044 (1.010-1.079) 0.011 0.724 (0.568-0.881)
V35 1.005 (1.019-1.093) 0.003 0.751 (0.594-0.907)
V40 1.059 (1.020-1.098) 0.002 0.763 (0.613-0.914)
V45 1.058 (1.017-1.100) 0.005 0.745 (0.595-0.894)
V50 1.062 (1.019-1.106) 0.004 0.728 (0.579-0.878)
V55 1.066 (1.020-1.114) 0.005 0.737 (0.588-0.886)
V60 1.080 (1.030-1.132) 0.001 0.766 (0.613-0.919)
V65 1.096 (1.037-1.159) 0.001 0.759 (0.607-0.912)
Abbreviation: OR = odds ration from the logistic regression, CI = confidence interval, AUC =
area under the curve.
Variables in bold are significant.

30
Table 11 illustrates the correlation between the urethra (V35-V50) and the nocturia grade ≥ 2
three months post-RT. There were no significant results found with univariate logistic
regression.
The urethra was not considered for generating DVHs, because no significant results were
found as seen in Table 11. The significant results in Table 10 are the rational of creating DVHs
for the bladder wall.
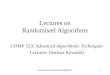
Figure 4 shows the DVH’s of the dose delivered to the bladder wall, so that 5%, 10%, 15% and
20% of the patients get retention grade ≥ 2 at three months post-RT. Ideally no irradiation
should be delivered to this ROI. Logistic regression was used to calculate the probabilities for
retention. These probabilities were used to create the DVHs for 5%, 10%, 15% and 20%
probability for retention three months post-RT. For example, when the V25 of the bladder wall
is < 53.5%, the V30 is < 45.5%, the V35 is < 39.6% etc, then the probability of getting grade ≥
2 retention is < 5% (the diamond line in Figure 4).
Table 11: Univariate logistic regression models for acute grade ≥ 2 nocturia: relative volume
of the urethra receiving a certain dose (V35-V50). No significant result was found.
Variable OR (95% CI) p-value AUC (95% CI)
V35 0.846 (0.646-1.107) 0.223 0.465 (0.345-0.585)
V40 0.901 (0.712-141) 0.387 0.459 (0.338-0.579)
V45 0.931 (0.802-1.097) 0.341 0.492 (0.373-0.611)
V50 0.954 (0.891-1.021) 0.174 0.460 (0.342-0.577)
Abbreviation: OR = odds ration from the logistic regression, CI = confidence interval, AUC
= area under the curve.
Variables in bold are significant

31
Figure 4: A cumulative dose volume histogram (DVH) for the bladder wall for 5%, 10%, 15%
and 20% probability of getting grade ≥ 2 retention three months post-RT.
0
10
20
30
40
50
60
70
80
90
100
2 5 3 0 3 5 4 0 4 5 5 0 5 5 6 0 6 5
VO
LUM
E (%
)
DOSE (GY)
5% 10% 15% 20%

32
Discussion
Recently, four randomised trials, comparing conventional dose radiotherapy with HFRT,
demonstrated the non-inferiority of HFRT regarding biochemical and clinical relapse free
survival for low and intermediate risk PC patients (17–20). Also the risk of developing toxicity
remains acceptable with HFRT. Based on the results of these trials, HFRT can be considered
a standard of care for localized PC.
Urinary toxicity is the most frequent form of toxicity experienced by PC patients post-RT. The
risk of developing acute urinary toxicity is further increased with HFRT. This makes it vital to
create robust models of dosimetric predictors as well as models of patient-related risk factors
of urinary toxicity in HFRT.
In this analysis we looked at the impact of patient related factors on urinary toxicity as well as
correlation between spatial dose predictors of the bladder and acute urinary toxicity
experienced by the patients receiving HFRT.
Patient related risk factors
Studies have shown conflicting results regarding the correlation between acute urinary toxicity
and different patient-related risk factors like smoking and TURp. However, all studies agree
that use of anticoagulation therapy is an important risk factor for developing urinary toxicity.
Smoking
The literature about smoking in association with urinary toxicity after EBRT is scarce and the
evidence goes both ways. It is shown that smoking increases the risk of late urinary toxicity
(28). There is also evidence that smoking increases the risk of acute urinary toxicity (27,33).
Proposed mechanisms to explain this increase in risk are that smoking induces contractions
of the bladder or that there is an ischemic effect on the detrusor muscle (48,49). But it is also
reported that smoking decreases the risk of late urinary toxicity (50). And in our study smoking
decreases the risk of acute urinary toxicity as seen in Table 9.
We recognize the limitation that there were only 14 smokers (10%) and 125 non-smokers
(90%) included in the analysis. Because of this, a small change in the number of smokers
might have had a large impact on the odds ratio (OR) of the logistic regression (51).
Because of contradicting evidence about smoking as risk factor for acute as well as late urinary
toxicity, it might be interesting to continue considering smoking in future research.
TURp
TURp is a surgical treatment of benign prostatic hyperplasia (BPH) where prostatic tissue is
removed through the urethra. We found reduced acute urinary toxicity after a TURp procedure

33
as seen in Table 9. This can be expected because acute toxicity symptoms arise from swelling
of the prostate. Which is mitigated by TURp (52). We might expect an increased incidence of
late urinary toxicity because of a decrease in swelling.
We must note that only 18 patients (13%) of the 140 underwent TURp prior to the treatment.
Because of this, again a small change in the number of patients who had a TURp might have
had a large impact on the OR of the logistic regression (51).
Most published articles show that there is an increase in acute urinary toxicity post-RT if patient
underwent TURp prior to EBRT. Some articles show no correlation (53). One article shows
that TURp decreased the risk (54). Most of those studies used old irradiation techniques. TURp
increases the risk of late urinary toxicity (31,52).
Because of the conflicting opinions it is interesting to look at the impact of TURp on different
forms of toxicity with modern irradiation techniques and alternative fractionation regimens.
Anticoagulation
Elderly often uses anticoagulation medication. It is given for cardiovascular disease such as
atrial fibrillation, acute coronary syndrome, myocardial infarction, and deep vein thrombosis.
Because PC presents at higher age, we can assume that the prevalence of anticoagulation
usage is high in this patient group.
Evidence shows that anticoagulation therapy has a strong correlation with the acute and late
urinary toxicity, especially haematuria (30,55). In this cohort the same significant result is found
for overall acute toxicity, as seen in Table 9. Because anticoagulation medication is a
confounding variable for urinary toxicity, it might be interesting to exclude the patient group
receiving anticoagulation medication in future research. This makes it possible to model the
effect of HFRT without anticoagulation as confounding variable. It is also a possibility to include
this variable in the logistic regression model.
Dosimetric parameters
HFRT and Urinary Toxicity
Randomised trials demonstrate that a higher radiation dose shows good long-term biochemical
outcomes (13,14).
There is evidence that patients receiving HFRT have a higher risk of acute urinary toxicity than
patients with conventional treatment (15,56). The types of toxicity are similar between HFRT
and conventional treatment (15,56). We found that nocturia, incontinence and retention are
frequent forms of acute urinary toxicity (Table 8).

34
Other types of toxicity like haematuria, frequency, dysuria and urgency have a significant
impact on the QoL especially on social functioning (57). In this study only few of the patients
presented these symptoms. Consequently, it is not possible to consider them in this analysis
(Table 8). It might therefore be interesting to study these types of toxicity in future research.
High doses per fractions are unfortunately associated with higher late-term complications, such
as vascular injury and chronic inflammation. There is evidence that supports this fact (58). But
there is big range in incidence of late toxicity between different studies (37).
DVHs
To calculate the DVHs the patients of both arms were pooled. This was done because of the
low prevalence of urinary symptoms in both arms. Although the question rises if the number of
fractions doesn’t have an influence on the acute toxicity. Alterations in fraction dose, as is the
case in HFRT, are also accompanied by an increased risk of developing acute and to a lesser
extend late urinary toxicity (19,37).
Another limitation of the DVHs we created is the use of relative volumes instead of absolute
volumes. Evidence shows that absolute DVHs are more invariant to changes in bladder filling
(59). It might be interesting to use relative as well as absolute histograms in future research to
make the results more robust (60).
Figure 4 shows as expected that a lower dose to the bladder wall leads to less retention grade
≥ 2 at three months post-RT. Retention was the only significantly correlated dosimetric factor
with the dose to the bladder and the bladder wall. In the analysis only the retention at three
months was considered. This means that the time factor was ignored, which can lead to biased
results. In further research, a Cox risk analysis might be more appropriate if acute and late
toxicity are analysed together. This might make it possible to do the analysis not just on the
retention, but also on other individual toxicities. The Cox risk analysis also considers temporal
factors.
The symptom ‘retention’ has also a high prevalence pre-RT and is the highest during RT (Table
8). We saw earlier that the retention is correlated with the dose to the bladder. In this study the
impact of the symptoms pre-RT was not included. This is a limiting factor and it could be
interesting to exclude patients who have symptoms grade ≥ 2 pre-RT in future research or
include the toxicity pre-RT in the logistic regression model.
Trigone
The bladder is an organ that is subject to changes in positioning due to different factors such
as bladder filling, bowel filling and positioning. There is interfraction movement of up to 4 cm
(35,61), as well as movement during treatment. The introduction of IMRT and IMAT has made

35
it possible to deliver a high dose distribution conforming to the prostate. However, when the
bladder moves, the dose can shift to the bladder during treatment (62).
The movement of the bladder is mostly found in the anterior-cranial region (45,61). The dose
to the anterior-cranial region is small and therefore probably of little clinical relevance. The
trigone and the base of the bladder are not subject to bladder filling variations They are
relatively stable in respect to the prostate. They might therefore be regarded as robust
predictors of urinary toxicity (45).
Although the trigone seems to be robust regarding movement and dose distribution, we didn’t
find it to be significant in this analysis. One reason might be that the dose difference between
patients with toxicity and patients without is too low. Another study has also shown that the
dose difference between patients with or without urinary toxicity in the posterior bladder, and
therefore also in trigone is only approximately 2 Gy (34).
The trigone and the base of the bladder are in close vicinity of the CTV and receive a higher
dose than other parts of the bladder. Therefore, another possibility could be that the dose to
the trigone is higher than 65 Gy, which is the highest dose we evaluated. This way we might
have missed the impact of the higher doses.
Because the trigone is responsible for sphincter opening, it can be assumed that a high dose
and therefore damage to the trigone might lead to incontinence (34,63). Studies have shown
that the dose to the trigone has a greater impact on toxicity than the dose to the whole bladder
(22,33,35,36). In our study the following definition of the trigone was used for delineation: the
trigone is the volume between the ureteral orifices and the urethral orifice. On CT scans the
trigone, as defined above, is often difficult to identify (35). Therefore, there might be some inter
patient variability in the delineation. An easier region to delineate and also robust region of the
bladder is the region up to 2.5 cm cranially from the base (45).
Taking into account the movement of bladder, it might be interesting to take a planning CT
during each treatment session and to delineate all ROI. Afterwards the actual dose received
by each individual ROI can be calculated.
Urethra
The prostate surrounds the urethra, and therefore the urethra receives a high dose in EBRT.
There is evidence that the prostatic urethra and the prostate is responsible for most urinary
symptoms, because people have less symptoms after a TURp procedure (35). This
corresponds with our findings.
We found that nocturia is influenced by the dose received by the urethra (V35-V50). Although
this could not be quantified with the univariate logistic regression, it seems feasible that a high

36
dose to the urethra may lead to nocturia. Because of the radiation, we can see urethral and
prostatic swelling which in turn can lead to nocturia (64).
These results suggest that a reduction of the dose to the urethra might lead to less urinary
symptoms, which is substantiated by literature (65).

37
Conclusion
As part of an interim safety analysis of a phase III trial, urinary toxicity was evaluated. This
thesis focused on evaluation of correlation between dose received by different parts of the
bladder and incidence in acute urinary toxicity. For those regions of the bladder were a
correlation was found, DVH constraints were derived. Also, patient related factors were
considered.
The results were not conclusive, and it is evident that further research is needed to define
robust predictive parameters for acute urinary toxicity.

38
References
1. Lee CH, Akin-Olugbade O, Kirschenbaum A. Overview of Prostate Anatomy, Histology,
and Pathology. Endocrinol Metab Clin North Am. 2011 Sep 1;40(3):565–75.
2. Walz J, Graefen M, Huland H. Surgical anatomy of the prostate in the era of radical robotic
prostatectomy: Curr Opin Urol. 2011 May;21(3):173–8.
3. Arnold M, Karim-Kos HE, Coebergh JW, Byrnes G, Antilla A, Ferlay J, et al. Recent trends
in incidence of five common cancers in 26 European countries since 1988: Analysis of the
European Cancer Observatory. Eur J Cancer. 2015 Jun 1;51(9):1164–87.
4. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-
ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local
Treatment with Curative Intent. Eur Urol. 2017 Apr 1;71(4):618–29.
5. Stelloo S, Nevedomskaya E, van der Poel HG, de Jong J, van Leenders GJ, Jenster G, et
al. Androgen receptor profiling predicts prostate cancer outcome. EMBO Mol Med. 2015
Nov;7(11):1450–64.
6. D’Amico AV, Moul J, Carroll PR, Sun L, Lubeck D, Chen M-H. Cancer-Specific Mortality
After Surgery or Radiation for Patients With Clinically Localized Prostate Cancer Managed
During the Prostate-Specific Antigen Era. J Clin Oncol. 2003 Jun 1;21(11):2163–72.
7. Di Blasio CJ, Rhee AC, Cho D, Scardino PT, Kattan MW. Predicting clinical end points:
treatment nomograms in prostate cancer. Semin Oncol. 2003 Oct 1;30(5):567–86.
8. Brenner DJ. Point: The linear-quadratic model is an appropriate methodology for
determining iso-effective doses at large doses per fraction. Semin Radiat Oncol. 2008
Oct;18(4):234–9.
9. Halperin EC, Perez CA, Brady LW. Principles of Radiologic Physics. In: Perez and Brady’s
Principles and Practice of Radiation Oncology. Lippincott Williams & Wilkins; 2008. p. 130–
54.
10. Bansal A, Kapoor R, Singh SK, Kumar N, Oinam AS, Sharma SC. Dosimetric comparison
of standard three-dimensional conformal radiotherapy followed by intensity-modulated
radiotherapy boost schedule (sequential IMRT plan) with simultaneous integrated boost–
IMRT (SIB IMRT) treatment plan in patients with localized carcinoma prostate. Indian J
Urol IJU J Urol Soc India. 2012;28(3):300–6.

39
11. Yu CX. Intensity-modulated arc therapy with dynamic multileaf collimation: an alternative
to tomotherapy. Phys Med Biol. 1995;40(9):1435.
12. Wortel RC, Incrocci L, Pos FJ, van der Heide UA, Lebesque JV, Aluwini S, et al. Late Side
Effects After Image Guided Intensity Modulated Radiation Therapy Compared to 3D-
Conformal Radiation Therapy for Prostate Cancer: Results From 2 Prospective Cohorts.
Int J Radiat Oncol. 2016 Jun 1;95(2):680–9.
13. Pollack A, Zagars GK, Starkschall G, Antolak JA, Lee JJ, Huang E, et al. Prostate cancer
radiation dose response: results of the M. D. Anderson phase III randomized trial. Int J
Radiat Oncol. 2002 Aug 1;53(5):1097–105.
14. Zietman AL, DeSilvio ML, Slater JD, Rossi CJ, Miller DW, Adams JA, et al. Comparison of
Conventional-Dose vs High-Dose Conformal Radiation Therapy in Clinically Localized
Adenocarcinoma of the Prostate: A Randomized Controlled Trial. JAMA. 2005 Sep
14;294(10):1233–9.
15. Benjamin LC, Tree AC, Dearnaley DP. The Role of Hypofractionated Radiotherapy in
Prostate Cancer. Curr Oncol Rep [Internet]. 2017;19(4). Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5366169/
16. Dasu A, Toma-Dasu I. Prostate alpha/beta revisited – an analysis of clinical results from
14 168 patients. Acta Oncol. 2012 Nov 1;51(8):963–74.
17. Dearnaley D, Syndikus I, Mossop H, Khoo V, Birtle A, Bloomfield D, et al. Conventional
versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer:
5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol.
2016 Aug 1;17(8):1047–60.
18. Catton CN, Lukka H, Gu C-S, Martin JM, Supiot S, Chung PWM, et al. Randomized Trial
of a Hypofractionated Radiation Regimen for the Treatment of Localized Prostate Cancer.
J Clin Oncol. 2017 Mar 15;35(17):1884–90.
19. Lee WR, Dignam JJ, Amin MB, Bruner DW, Low D, Swanson GP, et al. Randomized Phase
III Noninferiority Study Comparing Two Radiotherapy Fractionation Schedules in Patients
With Low-Risk Prostate Cancer. J Clin Oncol. 2016 Jul 10;34(20):2325–32.
20. Arcangeli G, Saracino B, Arcangeli S, Gomellini S, Petrongari MG, Sanguineti G, et al.
Moderate Hypofractionation in High-Risk, Organ-Confined Prostate Cancer: Final Results
of a Phase III Randomized Trial. J Clin Oncol. 2017 Mar 29;35(17):1891–7.

40
21. Fonteyne V, Sadeghi S, Ost P, Vanpachtenbeke F, Vuye P, Lumen N, et al. Impact of
changing rectal dose volume parameters over time on late rectal and urinary toxicity after
high-dose intensity-modulated radiotherapy for prostate cancer: A 10-years single centre
experience. Acta Oncol. 2015 Jul 3;54(6):854–61.
22. Fiorino C, Valdagni R, Rancati T, Sanguineti G. Dose–volume effects for normal tissues in
external radiotherapy: Pelvis. Radiother Oncol. 2009 Nov;93(2):153–67.
23. Improta I, Palorini F, Cozzarini C, Rancati T, Avuzzi B, Franco P, et al. Bladder spatial-
dose descriptors correlate with acute urinary toxicity after radiation therapy for prostate
cancer. Phys Med [Internet]. [cited 2016 Oct 3]; Available from:
http://www.sciencedirect.com/science/article/pii/S1120179716309000
24. Zelefsky MJ, Kollmeier M, Cox B, Fidaleo A, Sperling D, Pei X, et al. Improved Clinical
Outcomes With High-Dose Image Guided Radiotherapy Compared With Non-IGRT for the
Treatment of Clinically Localized Prostate Cancer. Int J Radiat Oncol. 2012 Sep
1;84(1):125–9.
25. Rosewall T, Catton C, Currie G, Bayley A, Chung P, Wheat J, et al. The relationship
between external beam radiotherapy dose and chronic urinary dysfunction – A
methodological critique. Radiother Oncol. 2010 Oct 1;97(1):40–7.
26. Zelefsky MJ, Levin EJ, Hunt M, Yamada Y, Shippy AM, Jackson A, et al. Incidence of Late
Rectal and Urinary Toxicities After Three-Dimensional Conformal Radiotherapy and
Intensity-Modulated Radiotherapy for Localized Prostate Cancer. Int J Radiat Oncol. 2008
Mar 15;70(4):1124–9.
27. Stankovic V, Džamic Z, Pekmezovic T, Tepavcevic DK, Dozic M, Saric M, et al. Acute and
Late Genitourinary Toxicity after 72 Gy of Conventionally Fractionated Conformal
Radiotherapy for Localised Prostate Cancer: Impact of Individual and Clinical Parameters.
Clin Oncol. 2016 Sep;28(9):577–86.
28. Yahya N, Ebert MA, Bulsara M, Haworth A, Kennedy A, Joseph DJ, et al. Dosimetry,
clinical factors and medication intake influencing urinary symptoms after prostate
radiotherapy: An analysis of data from the RADAR prostate radiotherapy trial. Radiother
Oncol. 2015 Jul;116(1):112–8.
29. Kalakota K, Liauw SL. Toxicity After External Beam Radiotherapy for Prostate Cancer: An
Analysis of Late Morbidity in Men With Diabetes Mellitus. Urology. 2013 Jun;81(6):1196–
201.

41
30. Pederson AW, Fricano J, Correa D, Pelizzari CA, Liauw SL. Late Toxicity After Intensity-
Modulated Radiation Therapy for Localized Prostate Cancer: An Exploration of Dose–
Volume Histogram Parameters to Limit Genitourinary and Gastrointestinal Toxicity. Int J
Radiat Oncol. 2012 Jan 1;82(1):235–41.
31. Budäus L, Bolla M, Bossi A, Cozzarini C, Crook J, Widmark A, et al. Functional Outcomes
and Complications Following Radiation Therapy for Prostate Cancer: A Critical Analysis of
the Literature. Eur Urol. 2012 Jan;61(1):112–27.
32. Kim S, Moore DF, Shih W, Lin Y, Li H, Shao Y-H, et al. Severe Genitourinary Toxicity
Following Radiation Therapy for Prostate Cancer: How Long Does it Last? J Urol [Internet].
2013 Jan [cited 2016 Nov 30];189(1). Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3819428/
33. Cozzarini C, Rancati T, Carillo V, Civardi F, Garibaldi E, Franco P, et al. Multi-variable
models predicting specific patient-reported acute urinary symptoms after radiotherapy for
prostate cancer: Results of a cohort study. Radiother Oncol. 2015 Aug;116(2):185–91.
34. Palorini F, Cozzarini C, Gianolini S, Botti A, Carillo V, Iotti C, et al. First application of a
pixel-wise analysis on bladder dose–surface maps in prostate cancer radiotherapy.
Radiother Oncol. 2016 Apr;119(1):123–8.
35. Viswanathan AN, Yorke ED, Marks LB, Eifel PJ, Shipley WU. Radiation Dose–Volume
Effects of the Urinary Bladder. Int J Radiat Oncol. 2010 Mar 1;76(3, Supplement):S116–
22.
36. Carillo V, Cozzarini C, Rancati T, Avuzzi B, Botti A, Borca VC, et al. Relationships between
bladder dose–volume/surface histograms and acute urinary toxicity after radiotherapy for
prostate cancer. Radiother Oncol. 2014 Apr;111(1):100–5.
37. Incrocci L, Wortel RC, Alemayehu WG, Aluwini S, Schimmel E, Krol S, et al.
Hypofractionated versus conventionally fractionated radiotherapy for patients with
localised prostate cancer (HYPRO): final efficacy results from a randomised, multicentre,
open-label, phase 3 trial. Lancet Oncol. 2016 Aug 1;17(8):1061–9.
38. Fonteyne V. Four-weeks versus 5-weeks hypofractionated high dose radiotherapy as
primary therapy for prostate cancer: interim safety analysis of a randomized phase 3 trial.
Int J Radiot Oncol Biol Phys. 2017;

42
39. Common terminology criteria for adverse events : (CTCAE). v4.03. [Bethesda, Md.] : U.S.
Department of Health and Human Services,; 2010.
40. Diaz A, Roach M, Marquez C, Coleman L, Pickett B, Wolfe JS, et al. Indications for and
the significance of seminal vesicle irradiation during 3D conformal radiotherapy for
localized prostate cancer. Int J Radiat Oncol. 1994 Sep 30;30(2):323–9.
41. Professionals S-O. Non-muscle-invasive Bladder Cancer [Internet]. Uroweb. 2015 [cited
2017 Dec 2]. Available from: https://uroweb.org/guideline/non-muscle-invasive-bladder-
cancer/#5
42. Cheung MR, Tucker SL, Dong L, de Crevoisier R, Lee AK, Frank S, et al. Investigation of
bladder dose and volume factors influencing late urinary toxicity after external beam
radiotherapy for prostate cancer. Int J Radiat Oncol. 2007 Mar 15;67(4):1059–65.
43. Hakenberg OW, Linne C, Manseck A, Wirth MP. Bladder wall thickness in normal adults
and men with mild lower urinary tract symptoms and benign prostatic enlargement.
Neurourol Urodyn. 2000;19(5):585–93.
44. Rosewall T, Bayley A, Catton C, Chung P, Currie G, Heaton R, et al. Delineating the inner
bladder surface using uniform contractions from the outer surface under variable bladder
filling conditions. Br J Radiol [Internet]. 2015 Sep [cited 2016 Nov 7];88(1053). Available
from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4743562/
45. Palorini F, Botti A, Carillo V, Gianolini S, Improta I, Iotti C, et al. Bladder dose–surface
maps and urinary toxicity: Robustness with respect to motion in assessing local dose
effects. Phys Med [Internet]. [cited 2016 Apr 17]; Available from:
http://www.sciencedirect.com/science/article/pii/S1120179716300011
46. Ghadjar P, Zelefsky MJ, Spratt DE, Munck af Rosenschöld P, Oh JH, Hunt M, et al. Impact
of Dose to the Bladder Trigone on Long-Term Urinary Function After High-Dose Intensity
Modulated Radiation Therapy for Localized Prostate Cancer. Int J Radiat Oncol. 2014 Feb
1;88(2):339–44.
47. Di Franco R, Borzillo V, Ravo V, Ametrano G, Falivene S, Cammarota F, et al.
Rectal/urinary toxicity after hypofractionated vs conventional radiotherapy in
low/intermediate risk localized prostate cancer: systematic review and meta analysis.
Oncotarget. 2017 Jan 22;8(10):17383–95.

43
48. Nuotio M, Jylhä M, Koivisto A-M, Tammela TLJ. Association of Smoking with
Urgency in Older People. Eur Urol. 2001;40(2):206–12.
49. Bump RC, McClish DK. Cigarette smoking and urinary incontinence in women. Am J
Obstet Gynecol. 1992 Nov;167(5):1213–8.
50. Chennupati SK, Pelizzari CA, Kunnavakkam R, Liauw SL. Late toxicity and quality of life
after definitive treatment of prostate cancer: redefining optimal rectal sparing constraints
for intensity-modulated radiation therapy. Cancer Med. 2014 Aug;3(4):954–61.
51. Nemes S, Jonasson JM, Genell A, Steineck G. Bias in odds ratios by logistic regression
modelling and sample size. BMC Med Res Methodol. 2009 Jul 27;9:56.
52. Kollmeier MA, Stock RG, Cesaretti J, Stone NN. URINARY MORBIDITY AND
INCONTINENCE FOLLOWING TRANSURETHRAL RESECTION OF THE PROSTATE
AFTER BRACHYTHERAPY. J Urol. 2005 Mar 1;173(3):808–12.
53. Ishiyama H, Hirayama T, Jhaveri P, Satoh T, Paulino AC, Xu B, et al. Is There an Increase
in Genitourinary Toxicity in Patients Treated With Transurethral Resection of the Prostate
and Radiotherapy?: A Systematic Review. Am J Clin Oncol. 2014 Jun;37(3):297.
54. Schultheiss TE, Lee WR, Hunt MA, Hanlon AL, Peter RS, Hanks GE. Late GI and GU
complications in the treatment of prostate cancer. Int J Radiat Oncol. 1997 Jan 1;37(1):3–
11.
55. Choe KS, Jani AB, Liauw SL. External Beam Radiotherapy for Prostate Cancer Patients
on Anticoagulation Therapy: How Significant is the Bleeding Toxicity? Int J Radiat Oncol.
2010 Mar 1;76(3):755–60.
56. Aluwini S, Pos F, Schimmel E, van Lin E, Krol S, van der Toorn PP, et al. Hypofractionated
versus conventionally fractionated radiotherapy for patients with prostate cancer
(HYPRO): acute toxicity results from a randomised non-inferiority phase 3 trial. Lancet
Oncol. 2015 Mar 1;16(3):274–83.
57. Fransson P, Damber J-E, Tomic R, Modig H, Nyberg G, Widmark A. Quality of life and
symptoms in a randomized trial of radiotherapy versus deferred treatment of localized
prostate carcinoma. Cancer. 2001 Dec 15;92(12):3111–9.
58. Aluwini S, Pos F, Schimmel E, Krol S, van der Toorn PP, de Jager H, et al.
Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate

44
cancer (HYPRO): late toxicity results from a randomised, non-inferiority, phase 3 trial.
Lancet Oncol. 2016 Apr 1;17(4):464–74.
59. Hoogeman MS, Peeters STH, Bois J de, Lebesque JV. Absolute and relative dose–surface
and dose–volume histograms of the bladder: which one is the most representative for the
actual treatment? Phys Med Biol. 2005;50(15):3589.
60. Kusumoto C, Ohira S, Miyazaki M, Ueda Y, Isono M, Teshima T. Effect of various methods
for rectum delineation on relative and absolute dose-volume histograms for prostate IMRT
treatment planning. Med Dosim. 2016 Jun 1;41(2):136–41.
61. Yee D, Parliament M, Rathee S, Ghosh S, Ko L, Murray B. Cone Beam CT Imaging
Analysis of Interfractional Variations in Bladder Volume and Position During Radiotherapy
for Bladder Cancer. Int J Radiat Oncol. 2010 Mar 15;76(4):1045–53.
62. Happersett L, Mageras GS, Zelefsky MJ, Burman CM, Leibel SA, Chui C, et al. A study of
the effects of internal organ motion on dose escalation in conformal prostate treatments.
Radiother Oncol. 2003 Mar;66(3):263–70.
63. Dorschner W, Stolzenburg JU, Dieterich F. A new theory of micturition and urinary
continence based on histomorphological studies. 2. The musculus sphincter vesicae:
continence or sexual function? Urol Int. 1994;52(3):154–8.
64. Weiss JP, Blaivas JG. NOCTURIA. J Urol. 2000 Jan 1;163(1):5–12.
65. Shimizu S, Nishioka K, Suzuki R, Shinohara N, Maruyama S, Abe T, et al. Early results of
urethral dose reduction and small safety margin in intensity-modulated radiation therapy
(IMRT) for localized prostate cancer using a real-time tumor-tracking radiotherapy (RTRT)
system. Radiat Oncol Lond Engl. 2014 May 21;9:118.