Embed Size (px)
Citation preview

lACC Vol 8. No. bDecember 1986 21 B-32B
Pharmacology of Platelet Inhibitors
LAURENCE A. HARKER, MD,* VALENTIN FUSTER, MD, FACCt
La Jolla. California and New York, New York
21B
Although many drugs have inhibitory effects on plateletfunction, none of them inhibits all of the mechanismsthat may be involved in the various forms of thrombosis.Choice of suitable drugs is hampered by lack of fullknowledge concerning the reactions that make the majorcontributions to the formation ofarterial thrombi at sitesof repeated vessel wall injury or on atherosclerotic lesions. Drugs such as aspirin that inhibit the arachidonatepathway in platelets can only be expected to be effectiveagainst thromboembolic events in which the generationof thromboxane A2 plays a major part. If thrombin andfibrin formation are dominant, oral anticoagulant agentsor heparin should be beneficial; thus, experimental evidence indicates that with repeated vessel wall injury, theformation of platelet fibrin thrombi on the vessel wall isprobably influenced more by inhibitors of thrombin generation than by the subendothelial constituents such ascollagen.
Phannacologic modification of platelet function reduces thethromboembolic complications in a number of arterial vascular disorders and in patients with prosthetic cardiovasculardevices (1-3). However, the indications for the clinical useof antiplatelet agents are not entirely clear despite extensivebasic experimental animal and clinical studies. This uncertainty is explained, at least in part. by our lack of knowledgeof the precise pathogenesis of many clinical vascular syndromes, by the lack of suitable phannacologic agents fordefinitive clinical testing and by the inconclusive resultsobtained in some of the clinical studies. In this study, thecurrent pharmacologic status of antiplatelet drugs used inclinical practice is reviewed.
From the *Roon Center for Artenosclerosis and ThrombosIs. Department of Basic and Climcal Research, Scnpps Climc and Research Foundation. La Jolla. California and tMount Sinai Medical Center, New York,New York. ThiS work was supported m part by U.S. Public Health ServiceGrants HL 31950 and RR 0833 from the National Institutes of Health.Bethesda, Maryland. ThiS study is publication no. 4355 BCR from theResearch InstItute of Scripps Climc. Scripps Climc and Research FoundatIon, La Jolla, California.
Address for reprint>. Laurence A. Harker, MD, Roon Center for Arteriosclerosis and Thrombosis. Department of BaSIC and ClImcal Research.Scripps Climc and Research FoundatIOn. La Jolla. California 92037
©1986 by the Amencan College of CardIology
Agents like prostacyclin that raise platelet cyclicadenosine monophosphate (AMP) levels in platelets bystimulating adenylate cyclase are potent inhibitors of thereaction of platelets to all aggregating and releaseinducing stimuli, but these agents are not suitable forlong-term administration. The effect of dipyridamole onplatelet cyclic AMP levels is weak, and this drug mayact through other effects on platelets or on other cells.Indeed, several of the drugs that have been tested inclinical trials may exert their effects through unrecognized mechanisms. Many combinations of drugs havebeen used to affect platelets or platelets and coagulation.This practice has been based on the theory that becauseseveral mechanisms may be involved in thrombus formation, combinations of drugs that inhibit differentmechanisms may be beneficial.
(J Am Coil CardioI1986;8:21B-32B)
Ideally, a clinically useful, platelet-modifying drug shouldbe nontoxic, orally effective, have sustained action and havegood antithrombotic potency without excessive risk of abnormal bleeding. None of the currently available clinicalagents satisfies all these requirements. Aspirin, sulfinpyrazone, dipyridamole, suloctidil, ticlopidine and prostacyclinhave been the agents evaluated in clinical trials to date.Many agents with more defined pharmacologic actions havebeen synthesized for evaluation and are presently at variousstages of development.
The disorders for which antiplatelet therapy has beenstudied may have quite different pathogenetic mechanisms.Because the effects of a given drug may be different foreach pathogenetic process, it is probably inappropriate toextrapolate the results for a given drug from one clinicalsetting to another. In general, however, kinetic studies (4)in patients using radioactively labeled platelets and fibrinogen indicate that arterial thrombosis is characterized byselective platelet consumption that can be interrupted bysome inhibitors of platelet function but not by heparin, whereasvenous thrombosis produces combined and equivalent consumption of both platelets and fibrinogen that is blocked byanticoagulant therapy but not by drugs that modify plateletfunction.
0735-1097/86/$3.50

228 HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
JACC Vol 8, No (,December 1986 21B-32B
Pathways of Platelet Activation andTheir Modulation
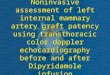
Process of platelet adhesion and aggregation (Fig. 1).Vascular injury with endothelial denudation exposes subendothelial structures to circulating blood and induces platelets to adhere to subendothelial collagen (5). The processof platelet adhesion involves interaction of the platelet membrane glycoprotein receptor GPlb, subendothelial collagenand plasma von Willebrand factor and fibronectin (6). Platelet interaction with collagen leads to the release of adenosinediphosphate (ADP) and activation of the prostaglandinarachidonate pathway (7,8) to release thromboxane A2 • BothADP and thromboxane A2 recruit circulating platelets (9,10)to change shape and aggregate with the layer of alreadyadherent platelets on the subendothelial surface (Fig. I). Athird pathway of platelet recruitment involves thrombin generation. Thrombin formation is produced through both extrinsic and intrinsic coagulation processes at the injury siteand around the aggregating platelet mass. Although thrombin induces the release of both ADP and thromboxane A2 ,
more importantly, thrombin induces platelet aggregation andrelease through a direct mechanism that is independent ofADP release or the formation of thromboxane A2 (11-13).In addition, the formation of polymerizing fibrin in closeproximity to the platelet aggregate by the action of thrombinon fibrinogen stabilizes the aggregate through the adherenceof polymerizing fibrin to the platelet surface (14). Plateletaggregates that are not stabilized by fibrin deaggregate readily and are broken up under the force of blood flow.
IHepa rlnas~
All platelet recruitment requires the rapid expression ofthe platelet-membrane complex GPllb/GPIlIa as the fibrinogen receptor (6,9,15). That is, platelet-platelet aggregatesare formed through calcium-dependent fibrinogen bindingwith the expressed receptor. This reaction may also be modulated by platelet alpha-granule proteins, fibronectin, vonWillebrand factor or thrombospondin (16).
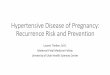
Limitation of thrombus formation. Intact endotheliumactively limits thrombus formation and its extension by multiple mechanisms including I) inactivation of released ADP(17), 2) active clearance of vasoactive amines (18), 3)thrombin-mediated release of prostacyclin (19), 4) directinactivation of circulating thrombin by plasma protease inhibitors (20), 5) inactivation of thrombin by enhancementof the endothelial surface thrombin-antithrombin III complex formation (21), 6) thrombin complexing with thrombomodulin on the endothelial cell surface to activate proteinC (which reduces thrombin formation by destroying factorsVa and Villa both in plasma and bound to the plateletsurface) (22), and 7) thrombin-mediated release of tissueplasminogen activator from intact vascular wall (23) (Fig.2). Thus, thrombin initiates important negative feedbackmechanisms to control its own generation and extent ofeffect.
Calcium-dependent platelet activation. There is increasing evidence that some platelet responses occur throughcalcium-regulated contractile processes (24), which are intum modulated by cyclic adenosine monophosphate (AMP)(25) and prostaglandin or arachidonic acid products (26).In general, contractile and secretory processes are thought
Figure 1. Pathways of platelet recruitment. Endothelial disruption initiates the attachment of plateletsto the subendothelium through the interaction of aplatelet receptor (GPIb), subendothelial collagen anda plasma cofactor VIII/von Willebrand factor (vWF).Fibronectin and thrombospondin derived from plasma,platelets and endothelium may also play roles in thisprocess. An unstable platelet mass forms through several interactive but independent recruitment mechanisms, including the generation of thromboxane (TX)A2 release of dense granule, adenosine diphosphate(AOP) and thrombin-mediated platelet activation.Aggregation requires the rapid expression of plateletmembrane fibrinogen receptor complex (GPIIb andGPIIIa) and calcium-dependent interplatelet bridgingby fibrinogen. Thrombin is generated locally on theplatelet surface through both extrinsic and intrinsicpathways. Thrombin-modified factor V (factor Vm)binds to platelets. Platelet-bound factor Vm serves asa high affinity platelet receptor for factor Xa in thefinal convetsion of prothrombin to thrombm. Thus,the generation of thrombin initiates potent positivefeedback mechanisms on the platelet surface for explosive activation of the coagulation cascade and fibrin formation. f3TG = f3-thromboglobulin; FOP =fibrin degradation products; POGF = platelet-de-rived growth factor; PF4 = platelet factor 4.

lACC Vol 8. No.6December 1986'2IB-32B
Figure 2. Mechanisms limiting throm-bus extension. Intact endothelium actively resists thrombus formation. Platelet aggregate formation is prevented bythe endothelium despite the presence ofADP, epinephrine or thrombin throughthe inactivation of ADP, active clearanceof vasoactive amines, facilitated complexing of thrombin with antithrombin IIIand the explosive thrombin-mediatedsynthesis and release of inhibitory POb.These mechanisms markedly decrease thepossibility of thrombus forming in thepresence of intact endothelium. The potent effects of thrombin are also activelylimited to the site of vascular injury byplasma protease inhibitors, enhancementof the endothelial surface of thrombinantithrombin III complex formation,binding of circulating thrombin to thrombomodulin (a receptor of luminal surfaceof the endothelial cells) thereby activatingprotein C to destroy factors V and VIIIand induced release of tissue plasminogenactivator from vascular endothelium. Thus,thrombin initiates negative feedbackmechanisms controlling its own generation. Abbreviations as in Figure I.
HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
23B
to be mediated by an increase in the concentration of cytoplasmic calcium derived from intracellular storage sitesor from the extracellular environment. Calcium-dependentplatelet activation occurs through actomyosin-mediated contractile mechanisms including pseudopod formation, aggregation, release and clot retraction. It appears that the releasereaction is triggered by release of calcium from an intracellular storage site, possibly the dense tubular system, intothe cytoplasm. Calcium regulation of contractile proteins inplatelets is similar to the processes of contraction in muscle.Calcium and the calcium-binding protein calmodulin areinvolved in activation of the specific enzyme myosin lightchain kinase and, hence, promotion of the interaction between platelet actin and myosin (27).
Platelet cyclic AMP. This compound inhibits both platelet secretion and aggregation (28). The amount of cyclicAMP in the platelet is determined both by the activity ofmembrane adenyl cyclase and by the specific phosphodiesterase that hydrolyzes cyclic AMP to adenosine triphosphate (ATP); that is, platelet cyclic AMP is increased byagents that either increase the activity of adenyl cyclase ordecrease the activity of phosphodiesterase. The basal levelof cyclic AMP appears to modulate release and aggregationby controlling the storage and release of calcium from platelet intracellular storage sites.
Role of prostaglandins. As discussed in more detail inthe first section of the symposium by Vermylen et al. (29)(also see Fig. I and 2 in reference 29), prostaglandins (PG)
are important in the regulation of platelet activation for tworeasons (26,30). First, as mentioned, stimulated plateletsproduce biologically active prostaglandins and derived substances that regulate platelet function. Second, other prostaglandins produced by other cells (such as PGh by vascularcells) may either inhibit or activate platelets. Platelet stimulation results in the hydrolysis of arachidonic acid frommembrane phospholipid, possibly through a calmodulinmediated process. Both phosphatidylinositol (through hydrolysis by phospholipase C) and phosphatidylcholine (throughhydrolysis by phospholipase Az) may serve as the sourceof arachidonic acid. The arachidonic acid thus liberatedbecomes converted by cyclooxygenase to labile prostaglandin endoperoxide intermediates (PGGz and PGHz), whichare potent platelet-aggregating agents, or through the Iipoxygenase pathway to other prostaglandin derivates. Bymeans of thromboxane synthetase, the most important conversion of PGHz is to the highly labile nonprostaglandinsubstance thromboxane Az, which is the most potent platelet-aggregating agent derived from arachidonic acid yet discovered. In addition, thromboxane Az is a potent vasoconstrictor. PGHz is also converted to several other (stable)prostaglandins, namely, PGEz and PGFza , which do notdirectly affect platelets but may potentiate aggregation byother substances, and PGDz, which inhibits aggregation andcould play the role of a negative feedback mechanism inregulating aggregation.
On the other hand, vascular tissue, cultured endothelial

248 HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
lACC Vol H. No 6December 19H6 21 B-32B
cells and postinjury neomtIma synthesize POlz from thearachidonic acid pathways (26,31,32). Moreover, endothelial cells can utilize POOz(Hz) derived from platelets tosynthesize POIz (33). POIz is about 30 to 40 times morepotent than POE) as an inhibitor of platelet aggregationinduced by ADP, epinephrine, collagen, thrombin and arachidonic acid. Its inhibitory effects are mediated throughelevation of platelet cyclic AMP through activation of adenylcyclase (34).
Finally, prostaglandins, cyclic AMP and Ca2+ interactin a number of complex ways to enhance platelet function(7,8,35). For example, both phospholipase Az and phospholipase C are activated by Caz + , and the inhibitory effectof cyclic AMP on platelet aggregation may act by maintaining calcium in a bound form, thereby preventing activation of phospholipases. Thromboxane A2 also has properties resembling those of a calcium ionophore, and someof the platelet-stimulatory effects of thromboxane Az maybe related to its ability to mobilize intracellular calcium fromstorage sites.
Drug TestingThe first assessment of a new compound to test for plate
let-inhibitory activity usually involves adding it to citratedplatelet-rich plasma in vitro and examining the effect onaggregation and the release of granule contents in responseto such substances as ADP, epinephrine, collagen and arachidonic acid. Suspensions of washed or gel-filtered platelets are more suitable for tests with thrombin and also permitexperiments in the presence of physiologic concentrationsof ionized calcium and magnesium. Unfortunately, theseresults have little predictability regarding antiplatelet efficacy in vivo, and it is for this reason that the effects of theseagents on in vitro testing will not be addressed in detail inthis review. Thus, although many agents that strongly inhibitaggregation and release in vitro have been identified, fewhave proved useful in human patients, particularly for longterm administration. Most of the drugs that have been usedin clinical trials were in use long before their effects onplatelets were recognized, and their value as antithromboticagents would not have been recognized by the type of routinescreening systems now being used. There have been noreports of major trials of new drugs that have been designedspecifically as inhibitors of platelet function. Other in vitrotests of platelet function of uncertain interpretation includestudies of platelet adherence to glass beads, artificial surfaces, collagen or subendothelium and examination of thecontribution of platelets to the acceleration of coagulation.In vivo testing in experimental animals has a number ofadvantages: 1) the drug is tested at concentrations that canbe achieved clinically, 2) active metabolites of the drug arealso assessed, 3) the time during which effective concentrations of the drug or its metabolites remain in the circu-
lation can be determined, and 4) side effects of the drugmay become apparent.
The most common tests of in vivo platelet function inhuman beings after drug administration involve bleedingtime (36), platelet survival and turnover (37), examinationof plasma for materials released from platelets (platelet factor 4 and beta-thromboglobulin) (38) and determination ofthe number of circulating platelet aggregates (39,40). Inaddition, there are suggestions of platelet hypersensitivity,circulating platelet aggregates or circulating materials released from platelets associated with clinical complicationsof atherosclerosis (41). In almost all of these conditions,administration of drugs that inhibit the arachidonate pathwayin platelets decreases their sensitivity to aggregating agentsand reduces the number of circulating platelet aggregates.These variables, however, may be a result of the clinicalcomplications rather than the cause. If so, drugs that depressthe sensitivity of the platelets may have little effect on theclinical complications.
Pharmacology of Drugs That ModifyPlatelet Function
The pharmacology of the drugs that inhibit platelet function and thrombus formation will be considered in four broadcategories: I) drugs that inhibit the arachidonate pathway,2) drugs that affect platelet cyclic AMP levels, 3) drugs thatinhibit thrombin formation and action, and 4) drugs that actthrough less well defined mechanisms.
Drugs that inhibit the arachidonate pathway. Drugsthat affect this prostaglandin pathway include agents thatinhibit platelet cyclooxygenase, drugs that block the actionof phospholipases and drugs that inhibit thromboxane synthetase. Because these drugs affect only thrombus formationthat is dependent on thromboxane Az, thrombus formationthat is predominately mediated by the other pathways andstimuli (that is, thrombin) will be largely unaffected by thisclass of drug.
Drugs that inhibit cyclooxygenase include the nonsteroidanti-inflammatory drugs such as aspirin, indomethacin, ibuprofen and many others (1-3,42). (Although the uricosuricagent sulfinpyrazone has effects on cyclooxygenase, its antithrombotic mechanism is unclear and is, therefore, discussed later.)
Aspirin and platelet function. Aspirin inhibits the secondbut not the first wave of ADP-induced platelet aggregation.Aspirin affects, in part, collagen-induced platelet aggregation caused by its inhibitory effect on platelet secretion.In addition to inhibiting the release of ADP, aspirin in vitroand in vivo inhibits the collagen-induced release of ATP,serotonin and platelet antiheparin activity (platelet factor 4).Similar results have been obtained with epinephrine-inducedaggregation. The effects of aspirin on thrombin-induced

lACC Vol S. No 6December 1986 21 B-32B
HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
258
aggregation and secretion are dose-related. Inhibition occursat low but not high concentrations of thrombin (43). Finally,the inhibitory effects of aspirin on platelet aggregation todifferent agents are detected for 4 to 7 days after a singleoral dose when salicylate is no longer detectable in theblood. This period of inhibition reflects an irreversible effectof aspirin on the platelet.
Aspirin irreversibly acetylates the cyclooxygenase inplatelets (44). Because platelets are unable to synthesizenew enzyme to replace that which has been inactivated, itis not until new platelets enter the circulation that plateletfunction is restored. However, aspirin also acts on megakaryocyte cyclooxygenase. This is shown by the finding thathuman platelets harvested at times up to 48 hours afteradministration of aspirin cannot be acetylated in vitro withradiolabeled aspirin (45), and also by direct experimentswith megakaryocytes that indicate that aspirin administration abolishes their ability to synthesize prostaglandins (46).The long-term administration of I mg/kg of aspirin once aday effectively inhibits platelet cyclooxygenase and thromboxane A~ formation in humans.
In contrast, aspirin inhibition of the cyclooxygenase ofthe cells of the vessel wall is not irreversible because thesecells synthesize new cyclooxygenase. Regeneration of theability of cultured human endothelial cells from umbilicalveins to synthesize PGI~ requires many hours (47). Indeed,long-term administration of I mg/kg of aspirin once a daywill also effectively inhibit vascular cyclooxygenase andprostaglandin production in humans (48). Thus, the notionthat low dose, infrequently administered aspirin exerts itsantithrombotic effects by preferentially sparing vascularprostacyclin production may not be correct. Furthermore,high doses of aspirin over prolonged periods to patients withrheumatoid arthritis may decrease thrombosis despite inhibition of PGI~ production (49). Earlier data concerningthe low incidence of myocardial infarction as a cause ofdeath of patients with rheumatoid arthritis who consumedlarge amounts of aspirin also support this view (50).
Under physiologic conditions of flow and protein concentration and hematocrit, aspirin does not inhibit adherenceof the initial layer of platelets to the subendothelium (51 ,52).Aspirin and indomethacin also do not inhibit the release ofamine storage granule contents from platelets that adheredirectly to collagen or the subendothelium (53), and releasedADP and serotonin from these platelets contribute to thrombus formation in the presence of the cyclooxygenase inhibitors. Because aspirin does not inhibit release of plateletderived growth factor from the alpha granules of the adherent platelets, it is not surprising that these drugs do notprevent smooth muscle cell proliferation in response to vessel damage (54). However, these drugs may inhibit plateletaggregate formation on the layer of adherent platelets (52),presumably by blocking thromboxane A~ release.
In some experimental animal studies, aspirin has par-
tially inhibited thrombus formation. In other studies no significant effects have been observed and, in a few, aspirinhas been reported to potentiate thrombus formation (55).The last effect has been attributed to aspirin inhibiting PGI~
production by the vessel wall.Aspirin in unstable angina and ischemia. In the myo
cardial and cerebral circulations, platelet aggregate formation and, perhaps, associated vasospasm (related to the release of thromboxane A2 or platelet-derived growth factor[56,57]) may lead to the acute coronary syndromes (that is,unstable angina, myocardial infarction, arrhythmia-relatedsudden death) or transient ischemic attacks, respectively.In dogs with experimentally stenosed coronary arteries, aspirin inhibits the formation of platelet plugs and the occurrence of fatal arrhythmias (58). Studies (59,60) with ischemic dog and cat myocardium have shown that aspirin canprevent ventricular fibrillation caused by ischemia. The beneficial effects of aspirin in patients with unstable angina ortransient ischemic attacks and in the experimental preparations just referred to, may be related not only to its abilityto inhibit platelet aggregation, but also to the inhibition ofrelease of thromboxane A~ and platelet-derived growth factor, preventing vasoconstriction so that thromboemboli donot readily lodge and persist in the microcirculation.
Aspirin and thromboembolism. Aspirin has been shownto be clinically effective in reducing thromboembolic complications of artificial heart valves in one study (61), thrombotic occlusion of arteriovenous cannulas in uremic patients(62), stroke and death in patients with transient ischemicattack (63), myocardial infarction in men with unstable angina (64,65), and, possibly, the occlusion of saphenous veincoronary artery bypass grafts (66). It may be important inthis context to note that an additional hemostatic abnormalitywas associated with the beneficial effect of aspirin in thestudies of artificial heart valves (oral anticoagulation) andarteriovenous cannulas (platelet dysfunction in uremic patients treated with long-term hemodialysis). The reportedantithrombotic effect of aspirin in patients undergoing saphenous vein coronary artery bypass surgery is provisionalin that the study involved a relatively small number of patients with an unusually high frequency of graft occlusionin the control group. Thus, aspirin may exert limited antithrombotic effects unless it is used in association withanother antithrombotic drug or perturbation of the hemostatic mechanism.
Regarding aspirin dose, the beneficial effects of low dosesof aspirin (100 to 150 mg/day) reported to prevent thrombosis in saphenous vein aortocoronary bypass grafts andarteriovenous shunts must be considered to be provisionalbecause, as already mentioned, the former study requiresconfirmation because of questions regarding the control group,and the conclusions of the latter study may not be extrapolated to other clinical settings because of the associatedplatelet dysfunction in those patients undergoing long-term

268 HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
JACC Vol X. No 6December I'!X6 21B-32B
hemodialysis. On the other hand, there are clinical reportsof high dose-dependent antithrombotic effects of aspirin. Inthis context, recent studies (67) in experimental thromboembolism indicate that aspirin has antithrombotic effectsthat are independent of its effect on cyclooxygenase andthat these effects occur at high doses.
Nonsteroid anti-inflammatory drugs. Other nonsteroidanti-inflammatory drugs also inhibit platelet activation throughinhibition of platelet cyclooxygenase (67). However, theseagents differ in potency and duration of action because theyinhibit competitively. In addition, some of these drugs mayhave other effects on platelets besides inhibiting cyclooxygenase. For example, indomethacin may inhibit phospholipase activation. At equimolar concentrations, meclofenamic acid, aspirin and indomethacin and ibuprofen werethe most active, whereas phenylbutazone was a relativelyweak inhibitor (68).
Other agents. Drugs that affect the generation of arachidonate from the cell membrane have been considered tobe inhibitors of phospholipase Az; they include the antimalarial drug quinacrine hydrochloride (mepacrine hydrochloride) and some of the steroid anti-inflammatory drugs.None of these agents has been shown to have clinicallyuseful antithrombotic effects in humans (42).
Inhibitors that block thromboxane synthetase include imidazole and its derivatives. Although a number of thesecompounds have been synthesized and have undergone testing in animal models and human subjects (69), none ofthese agents has been shown to prevent thrombosis in humans.
Drugs that increase platelet cyclic AMP levels. Whenthe cyclic AMP level in platelets is elevated, many plateletfunctions are inhibited (42). Platelet cyclic AMP is increasedby agents that stimulate adenylate cyclase and, to a lesserextent, by drugs that inhibit platelet phosphodiesterase (79)and, thus, prevent the breakdown of cyclic AMP in platelets(42). Adenylate cyclase is stimulated by PGlz, PGFz andPGE!. The combination of PGIz or PGE, with a phosphodiesterase inhibitor such as dipyridamole or theophyllinestrongly inhibits platelet functions (71,72).
PGE1 and PGIz. Agents that increase cyclic AMP levelsdiminish rabbit platelet adherence to damaged vessel walls(72), inhibit platelet aggregation induced by all stimuli andinhibit the release of platelet granule contents induced byall stimuli (26,42,74). When cyclic AMP levels are raised,the change in platelet shape in response to aggregating andrelease-inducing agents is also inhibited. This prevents plateletmembrane sites involved in the intrinsic coagulation pathway from becoming available to accelerate the generationof thrombin on the platelet surface. Agents such as PGE 1
or PGIz, when given in high doses, have been shown to bestrong inhibitors of platelet aggregation, thrombus formationand their consequences under a variety of situations in hu-
mans and experimental animals (75-80). PGIz is the mostpotent inhibitor of platelet aggregation thus far described,and it is 30 to 40 times more potent than PGE, in inhibitingplatelet aggregation by ADP. The duration of these effectsin vivo is very short; they disappear within 30 minutes ofdosing. PGh is a strong dilator in several vascular beds suchas those of the heart, kidney, mesenteric and skeletal muscle(81,82). Intravenous infusion of relatively small amounts(5 ng/kg per min) of PGlz in human patients produces vasodilation of peripheral blood vessels in the head, neck andpalms, a decrease in diastolic but not systolic blood pressureand an increase in heart rate (83). Platelet aggregation inresponse to ADP and the number of circulating aggregatesdecrease during PGIz infusion, while the bleeding time increases. One hour after termination of the infusion, theresponsiveness of the platelets to ADP returns to normal.
Dipyridamole. Dipyridamole is another platelet-inhibitordrug. It has been proposed that it acts to elevate plateletcyclic AMP by both blocking platelet phosphodiesterasedependent breakdown and increasing cyclic formation byPGIrmediated stimulation of platelet adenylate cyclase (72).It seems more likely that an increase in blood adenosinelevels may be involved because dipyridamole is a potentinhibitor of vascular and erythrocyte adenosine uptake (84,85)and produces an elevation in plasma adenosine levels (86).The higher plasma concentrations of adenosine could mediate the inhibition of platelet reactivity by stimulating platelet adenylate cyclase activity (87). For example, 10 fLM ofdipyridamole in vivo markedly inhibits the uptake of adenosine by endothelial cells and produces potent antiaggregating activity that is not blocked by aspirin (that is, in theabsence of prostacyclin). The vasodilating effects of dipyridamole also appear to be related to the elevation of plasmaadenosine levels. Indeed, vasodilation may account for itsactions in some experimental situations in which it has beenshown to be beneficial (88).
Dipyridamole, when given experimentally at a very highdose, does inhibit platelet adherence to collagen (89) andthe subendothelium (90), but most importantly, when givenat a dose more comparable with that used in humans, dipyridamole inhibits platelet activation over artificial surfaces(67,91). Indeed, the capacity of dipyridamole to decreaseexperimental thromboembolism in a dose-dependent fashioncorrelates well with its ability to normalize platelet survivalin patients with artificial heart valves (92,93) and arteriovenous cannulas (94) and its efficacy in preventing thromboembolism in patients with prosthetic heart valves (95).Moreover, the dose (10 mg/kg per day) and resulting bloodlevels that produce complete interruption of experimentalthromboembolism at prosthetic surfaces are in reasonableaccord with the dose (5 to 7 mg/kg per day) reported tonormalize platelet survival (92,94,96) and prevent thromboembolism in patients with artificial heart valves.

JACC Vol. 8, No 6December 1986.21B-32B
HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
27B
Aspirin potentiates the efficacy of dipyridamole in experimental thromboembolism on prosthetic surfaces (67).Moreover, the full potentiation depends on administering arelatively high dose of aspirin simultaneously with everydose of dipyridamole (20 mg/kg per day). These results inbaboons are in accord with the capacity of the combinationof aspirin and dipyridamole to prolong platelet survival inpatients with Dacron vascular grafts (96). On the other hand,the data regarding the beneficial effects on platelet survivaland thromboembolism of the combination of aspirin anddipyridamole in biologic surfaces such as in coronary arteryatherosclerosis (97-99), renal microvascular disease (100)and saphenous vein bypass grafting (10 I, 102) has raisedthe possibility of aspirin being the main effective component. That is, in four other different trials (103-106), thecombination of aspirin and dipyridamole was as effectiveas aspirin alone; in only one trial (107) addressing the rateof progression of peripheral vascular disease did this combination appear to be more effective than aspirin alone, butthis remains to be confirmed.
The mechanism whereby aspirin potentiates the antithrombotic activity of dipyridamole. particularly in experimental prosthetic surfaces. is not: I) mediated through aspirin's conversion to salicyclic acid; 2) due to alteredpharmacokinetic results; or 3) dependent on inhibition ofthe cyclooxygenase-thromboxane Az pathway since the specific blockage of thromboxane Az formation with dazoxibendoes not by itself produce detectable antithrombotic activityor potentiation of dipyridamole's antithrombotic activity (67),
Drugs that inhibit thrombin. The effects of thrombinon platelets and' fibrin formation can be prevented by inhibiting its action with heparin. Heparin, through its effecton antithrombin III, also inhibits other serine proteasesproduced during activation of the coagulation cascade, suchas factors IXa, Xa and XIa (108).
Heparin. Reports of the effects of heparin on plateletreactions are complex and contradictory (109,110) perhaps,in part, because of the variability among different commercially available heparin preparations. In vitro, heparinprevents the effects of thrombin on platelets, but may potentiate or inhibit aggregation and release induced by otheraggregating agents (109,110). It may itself cause plateletaggregation.
It is now recognized that heparin is heterogeneous withrespect to its molecular size and its affinity for antithrombinIII (111,112). More than 60% of some commercial formsof heparin are practically inactive as an anticoagulant. Inone study (109), heparin induced platelet aggregation incitrated platelet-rich plasma, Fractions of high molecularweight (approximately 20,000 daltons) were more reactivewith platelets than were fractions of low molecular weight(approximately 7,000 daltons). These findings raise the possibility that it may be feasible to select fractions of low
molecular weight and high antithrombin III activity for antithrombotic therapy without the undesirable effects of unfractionated heparin on platelets.
Heparin combined with prostaglandins. Two observations should be considered in the relation between the effectsof heparin and PGIz on platelet function. In the presence ofPGlz, the inhibitory effect of heparin on coagulation shouldbe enhanced (113). On the other hand, heparin has beenshown to inhibit the activation of adenylate cyclase by PGlz(114). Thus, a combination of heparin with one of theseprostaglandins might prove beneficial in preventing the formation of thrombi to which the coagulation pathway makesa major contribution, but might be less useful if plateletaggregation in response to collagen, ADP and thromboxaneAz has a dominant role and PGlz acts in a regulatory role.Overall, when well defined anticoagulant fractions of heparin become available for more extensive testing, it will beimportant to reassess the antiplatelet effects of heparin in avariety of experimental and clinical situations.
An alternative strategy being developed to block thrombin-mediated platelet thrombus formation involves the synthesis of peptides that show specificity for the inhibition ofthrombin (115-117). A number of these agents have beenstudied in vitro and in experimental animals. No clinicalexperience is available.
Agents that inhibit platelet function by other mechanisms. Many other agents have been shown to inhibitplatelet reactions and thrombus formation, although theirmechanisms of action remain to be defined (1-3,42).
Suljinpyrazone. Sulfinpyrazone inhibits platelet aggregation and secretion in vitro, but at concentrations higherthan that achieved after standard clinical doses (42). Inhibition of platelet aggregation and secretion after oral administration of high doses of sulfinpyrazone has also been reported (118). However, the concentration of collagen usedin performing in vitro tests is critical in demonstrating aninhibitory effect of sulfinpyrazone after oral administrationof the drug in humans (119). Although it has been suggestedthat sulfinpyrazone, in contrast to aspirin, is a competitiveinhibitor of platelet cyclooxygenase, present data suggestthat other mechanisms are more relevant in vivo (42,67).The inhibitory effects of sulfinpyrazone on collagen-inducedaggregation in rabbits has persisted for many hours after thedrug was cleared from the blood. This prolonged inhibitoryeffect has been attributed to mediated drug metabolites inplasma (120). Sulfinpyrazone has also been found to inhibitthe formation of thrombi on subendothelium (121) and toprotect endothelium from chemical injury in vitro and possibly in vivo (122). No mechanism has been identified forthis postulated endothelial protective effect. In addition, adose-dependent inhibition by sulfinpyrazone of experimental thromboembolism has been reported (67) that correlateswith its capacity to normalize platelet survival in patients

28B HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
lACC Vol 8. No 6December 1986 21B-32B
with artificial heart valves (123) and with its ability to reducethrombotic events in patients with arteriovenous cannulas(124). Experimentally on prosthetic surfaces, aspirin alsopotentiates this antithrombotic effect of sulfinpyrazone, witha maximal effect at 20 mg/kg per day, the same dose foundto optimally potentiate dipyridamole (67). These results withsulfinpyrazone on prosthetic surfaces have been more consistent than with biologic surfaces. Thus, despite a beneficialtrend in decreasing vascular events after myocardial infarction (125) and saphenous vein coronary artery bypass (126),the results were negative in the Canadian stroke study (63)and in the Canadian unstable angina study (65).
Ticlopidine. Ticlopidine is unusual in two respects: 1)
its effects are only manifest 24 to 48 hours after administration, but they last for several days after the drug is stopped;and 2) it is an inhibitor of the primary phase of ADP-inducedaggregation (127,128). It also inhibits aggregation and release induced by collagen, epinephrine, arachidonic acidand thrombin, prolongs the bleeding time, prolongs shortened platelet survival (129) and inhibits intimal proliferation(130) in the rabbit aorta from which the endothelium hasbeen removed. As well as being an inhibitor of plateletreactions in its own right, ticlopidine has been shown toenhance the inhibitory effect of PGh on platelets (13!).Thus, of the antiplatelet drugs currently available for clinicalinvestigation, ticlopidine is one of the most potent and hasseveral important theoretical advantages over existing drugs.Ticlopidine is chemically unrelated to other antiplatelet drugsand appears to have a unique, albeit unknown, mechanismof action. It is neither a prostaglandin synthesis inhibitornor a cyclic AMP-phosphodiesterase inhibitor. There aredata that indicate that ticiopidine may act on the plateletmembrane to alter its reactivity to activating stimuli (128).Clinical evaluation of this drug is underway in a number ofEuropean and American trials.
Antibiotics. In high doses, carbenicillin and penicillinproduce a bleeding tendency in patients (132). Studies withhuman volunteers have shown that these antibiotics alsoprolong the bleeding time and inhibit platelet aggregationinduced by a variety of agents. The drugs also inhibit plateletactivation in vitro at concentrations greater than those obtained in vivo (133). Similar findings have been describedfor ticarcillin. In vitro studies suggest that these drugs interfere with the binding of substances such as ADP, epinephrine and factor VIII/von Willebrand factor with theirspecific receptors on the platelet membrane, perhaps as aresult of properties that permit them to bind to membraneproteins or, as shown with artificial phospholipid bilayers,to platelet membrane lipids (134). The inhibitory effects invitro are observed immediately, but the prolongation of thebleeding time occurs after 12 to 24 hours of parenteraladministration (132,133). Therefore, either a metabolite orprolonged contact of platelets with lower concentrations ofthe antibiotics may account for the inhibition of platelet
activation observed in subjects who received the drugs (134).Although these antibiotics appear to have platelet-inhibitingeffects, no studies have been performed demonstrating thatthey prevent clinical thrombosis.
Dextran infusions. Dextran of a molecular weight of65,000 to 80,000 daltons produces a prolonged bleedingtime after patients receive one or more liters (135-137).The inhibitory effects of dextran infusions on platelet function are dose-related and are more pronounced with dextranof high molecular weight. The finding that platelets absorbdextran, with resultant changes in electrophoretic mobility,suggests that the inhibitory effect of dextran on plateletfunction might be due to some alteration of platelet membrane function. Other findings suggest that dextran maytemporarily impair platelet function by interfering with thefactor VIII/von Willebrand factor complex (138). Antithrombotic effects of dextran have been shown by experimental and clinical studies (3,42).
Suloctidil. This compound, originally introduced to prevent vasospasm at high concentrations, has been reportedto have a weak effect on platelet aggregation and secretion(139). Although it has been reported to be antithromboticin some thrombotic models and to prolong shortened plateletsurvival time in patients with artificial heart valves (140,141),suloctidil is ineffective in the secondary prevention of stroke(142) and in experimental arterial thromboembolism (143).
Vitamin E. This agent inhibits collagen-induced aggregation and the second phase of aggregation induced by ADPor epinephrine in citrated human platelet-rich plasma (144).It has been suggested that vitamin E may prevent the internalcalcium flux that mediates internal platelet contraction andsecretion induced by aggregating and release-inducing agents(145). However. the clinical antithrombotic usefulness ofvitamin E remains unproved.
Other drugs. A variety of other drugs have been reportedto have in vitro antiplatelet effects (1-3,42): calcium channel blockers, clofibrate and halofenate, furosemide and otherdiuretic drugs, serotonin antagonists, anesthetics, phenothiazines, tricyclic antidepressants, antihistamines, propranolol and other beta-adrenergic blocking agents, glycerylguaiacolate, furadantin, monoamine oxidase inhibitors, pyridinal carbamate, hydroxychloroquine, alcohol, pyrizadinederivates, pyridoxal phosphate and chlortetracycline. Clinically useful antithrombotic effects have not been demonstrated using any of these agents.
Summary of Drug EffectsThe principal antithrombotic effects of those drugs ad
equately evaluated are summarized as follows:Aspirin. This nonsteroid anti-inflammatory agent po
tently and irreversibly inactivates platelet cyclooxygenaseby acetylation. Although all of aspirin's antithrombotic effects have been attributed to this blockade of thromboxane

lACC Vol 8, NO.6December 1986.2IB-32B
HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
298
A2 formation by platelets, there is evidence for anti thrombotic effects independent of its inactivation of cyclooxygenase. At present, there is intense interest in aspirin therapyfor vascular disease.
Aspirin has been shown in well designed clinical trialsto be beneficial in at least five and possibly six clinicalsettings: I) reduction of thromboembolic complications associated with artificial heart valves; 2) prevention of strokeand death in patients with transient ischemic attacks; 3)decrease in thrombotic occlusion of arteriovenous Silasticcannulas in uremic patients undergoing hemodialysis; 4)reduction in myocardial infarction and cardiac death in patients with unstable angina; 5) probable effect in the secondary prevention of myocardial infarction; and 6) possibleincrease in the patency of saphenous vein coronary bypassgrafts. These reported benefits of aspirin require some comment. First, the antithrombotic effects of aspirin in patientswith prosthetic mitral valves are evident in association withoral anticoagulant therapy, and this combination is associated with an unacceptably high frequency of gastrointestinalbleeding. Second, the capacity of aspirin in low doses toreduce the thrombotic complications of arteriovenous cannulas was shown in patients undergoing long-term hemodialysis and, thus, associated with significant platelet dysfunction. It cannot be assumed that a similar dose wouldbe antithrombotic in the absence of associated platelet dysfunction.
Sulfinpyrazone. This urocosuric agent has weak antiinflammatory properties. The mechanism of antithromboticaction remains to be defined. Sulfinpyrazone reduces arteriovenous cannula occlusion and early coronary artery saphenous vein graft occlusion. Since the claimed benefit inreducing mortality in the secondary prevention of myocardial infarction remains controversial, no recommendations can be made regarding that possible indication. Thereports that it may also decrease thromboembolism in patients with artificial heart valves require confirmation.
Dipyridamole. This agent, a coronary vasodilator withweak inhibitory effects on phosphodiesterase activity, appears to increase inhibitory cyclic AMP levels in plateletsby elevating blood adenosine levels through the blockadeof adenosine uptake by red blood cells and vascular wallcells. Experimentally, on artificial surfaces, aspirin potentiates the antithrombotic effects of dipyridamole by mechanisms independent of platelet inactivation of platelet cyclooxygenase. Dipyridamole decreases thromboembolismin patients with artificial heart valves (in combination withanticoagulants). Dipyridamole in association with aspirinmay be more effective than aspirin alone in reducing theprogression of peripheral vascular disease, but this remainsto be confirmed. When used in combination with aspirin,it has been shown to decrease coronary mortality and nonfatal myocardial infarction in patients who have previouslysustained a myocardial infarction, to reduce both early and
late coronary artery saphenous vein graft occlusion and topreserve renal function in patients with membranoproliferative glomerulonephritis. However, the benefit of addingdipyridamole to aspirin in these latter settings of biologicsurfaces remains to be established.
Ticlopidine. This agent exhibits global antiplatelet activity of prolonged duration through some apparently novelmechanism of action. The fact that ticlopidine does notinhibit prostacyclin synthesis in the arterial wall, but canstill inhibit aggregation induced by thromboxane Az andprostaglandin endoperoxide, gives it a theoretical advantageover aspirin. A number of important weB designed multicenter trials are in progress. These trials should determinethe ultimate clinical role of ticlopidine.
ReferencesGenton E, Gent M, Hirsh 1, Harker LA. Platelet-inhibiting drugs inthe prevention of clinical thrombotic disease. N Engl 1 Med1975;293: 1174-8.
2 Braunwald E, Firedewald WT, Furberg CD. Proceedings of the workshop on platelet-active drugs in the secondary prevention of cardiovascular events. CIrculation 1980;62 (suppl V):V-I-135
3. Weiss H1. Platelets. Pathophysiology and Antiplatelet Drug Therapy.New York: Alan R. LISS, 1982.
4, Harker LA, Slichter S1. Platelet and fibrinogen consumption in man.N Engl1 Med 1972;287'999-1005.
5 Baumgartner HR, Muggli R, Tschopp TB, Turritto VT Platelet adhesion, release and aggregation In flowing blood: effects of surfaceproperties and platelet function. Thromb Haemost 1976;35:124-38.
6. George 1N, Nurden AT, Phillips DR, Molecular defects in interactionsof platelets with the vessel wall. N Engl1 Med 1984;311:1084-98.
7 Bell RL. Kennerly DA, Stanford N, Majerus PW. Diglyceride lipase:a pathway for arachidonate release from human platelets. Proc Nat!Acad SCI USA 1979;76:3238-41.
8. Rittenhouse-Simmons S. ProductIOn of diglyceride from phosphatidylinositol In activated human platelets 1 Clin Invest 1979;63:580-7
9. Zucker MB. The functioning of blood platelets. Sci Am 1980;242(6):86-103
10 Holmsen H Prostaglanding endoperoxide-thromboxane synthesis anddense granule secretion as positive feedback loops in the propagationof platelet responses dunng "the baSIC platelet reactiOn." ThrombHaemost 1977,38: I030-41.
II. Bills TK, Smith lB, Silver M1. Selective release of arachidonic acidfrom the phospholipids of human platelets in response to thrombin. 1Clin Invest 1970;60: 1-6.
12. Kinlough-Rathbone RL, Packham MA, Reimers H-1. Cazenave 1-P.Mustard 1F. Mechamsms of platelet shape change, aggregation andrelease Induced by collagen, thrombin or A23, 187. 1 Lab Clin Med1977;90:707-19.
13 Charo IF, Feinman RD, Detwiler TC Interrelations of platelet aggregation and secretion 1 Clin Invest 1977;60:866-73.
14. Nlewiarowski S, Regoeczi E, Stewart G1, Senyi AF, Mustard 1F.Platelet Interaction With polymerizing fibrin. 1 Clin Invest1972;51.685-700.
15, Kloczewiak M, Timmons S, Lukas n, Hawlger 1. Platelet receptorrecogmtIOn site on human fibrinogen. Synthesis and structure-functionrelationship of peptIdes corresponding to the carboxy-tenninal segmentof the gamma-chain. Biochemistry 1984;23.1767-74.
16. Houdijk WPM, de Groot PG. Nievelstein PFEM, Sakariassen KS,Sixma 11. Subendothelial proteins and platelet adhesion. von Wille-

30B HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
lACC Vol X. No 6December 1986 21B-32B
brand factor and fibnnectin, not thrombospondin, are mvolved mplatelet adhesIOn to extracellular matnx of human va,cular endothelialcells Arteriosclerosis 1986;6:24-33.
17. LIeberman GE, LewIs GP, Peters TJ. A membrane-bound enzymein rabbit aorta capable of inhibIting adenos1Oe-dIphosphate-inducedplatelet aggregation. Lancet 1977;2:330-2.
18. Johnson AR, Erdos EG. Metabolism of vasoactive peplldes by humanendothelial cells m culture. J Clin Invest 1977;59:684-95
19. Weksler BB, Ley CW, Jaffe EA. Stimulallon of endothelial cell prostacyclin producllon by thrombin, trypsin and the ionophore A 23187.J Clin Invest 1978;62:923-30.
20. Rosenberg RD. Heparin-antithrombin system. In: Colman RW, HIrshJ, Marder VJ, Salzman EW, eds. Hemostasis and Thrombosis: BasIcPrinciple, and Cl10ical Practice. Philadelphia: JB Lippmcott,1982:962-85.
21. Lollar P, Owen WG. Clearance of thrombin from CIrculation in rabbItsby high affimty bind10g sites on endothelium. J Clin Invest1980;66.1222-30
22. Esmon CT, Owen WG. Identification of an endothelial cell cofactorfor thrombin-catalyzed aCllvation of protein C Proc Nat! Acad SciUSA 1981 ;78:2249-52.
23. Levin EG. Marzec U, Anderson J, Harker LA. Thrombin sllmulate,tissue pla,minogen activator release from cultured human endothelialcells. J Clin Invest 1984;74:1988-95.
24. Zucker MB, Nachmias VT. Platelet activation. ArteriosclerosIs1985;5:2-18.
25. Salzman EW Cyclic AMP and platelet function N Engl J Med1972;286:358-63.
26. Moncada S, Vane JR. ArachIdonic acid metabolites and the interactions between platelets and blood-vessel walls N Engl J Med1979;300.1142-7
27. Hathaway DR, Eaton CR, Adelstein RS. Regulation of human plateletmyosm kmase by calcium-calmodulm and cyclic AMP. In: Mann KG,Taylor FB eds. The Regulation of Coagulation. New York: Elsevier/North Holland, 1980:271.
28. Haslam RJ, Davidson MML, Cajnham JA. Cyclic nucleotides 10 platelet function. Thromb Haemost 1978;40:232-40.
29. Vermylen J, Verstraete M, Fuster V. Role of platelet acllvation andfibrin formation in thrombogenesis. J Am Coli Cardlol 1986;8:2B-9B
30. Marcus AJ. The role of prostaglandins in platelet functIOn. Prog Haematol 1979;11: 147-71.
31. Marcus AJ, Weksler BB, Jaffe EA. SyntheSIS of prostaglandm h(prostacyclin) by cultured human and bovine endothelial cells ProcNatl Acad Sci USA 1977;74:3922-6.
32. Eldor A, Falcone OJ, Hajjar DP, Minick CR, Weksler BB. Recoveryof prostacyclin production by de-endothelialized rabbit aorta: crillcalrole of neomtimal smooth muscle cells. J Clin Invest 1981;67:735-41
33. Marcus AJ, Weksler BB, Jaffe EA, Broekman MJ. Synthesis of prostacyclin from platelet-derived endoperoxides by cultured human endothelial cell; J Clin Invest 1980;66:979-86.
34. Tateson JE, Moncada S, Vane JR. Effects of prostacyclin (pGX) oncyclic AMP concentrallons in human platelets. Prostaglandins1977;13:389-97.
35. Gerrard JM, White JF. Prostagland1Os and thromboxanes: "middlemen" modulat1Og platelet function 10 hemostasIs and thrombosis. ProgHemost Thromb 1978;4:87-125.
36. Harker LA, Slichter SJ. The bleed10g lime as a screening te,t forevaluatIon of platelet function. N Engl J Med 1972;287:155-9.
37. Mustard JF. Platelet survival. Thromb Haemost 1978;40:154-62.
38. Kaplan KL, Nossel HL, Lesznik G. Radioimmunoassay of plateletfactor 4 and beta-thromboglobulin: development and application to
,tudle, of platelet release in relallon to fibnnopepllde A generation.Br J Haematol 1978;39'129-46.
39. Hornstra G, ten Hoor F The filtragometer: a new deVice for measunngplatelet aggregation 10 venous blood of man Thromb Diath Haemorrh1975;34.531-44.
40. Wu KK, Hoak Jc. Increased platelet aggregate, m pallents with transient IschemiC attach Stroke 1975,6:521-24.
41 Packham MA. Method, fordetecllon of hypersensItive platelet,. ThrombHaemost 1978;40: 175-95.
42. Packham MA, Mustard JF. Pharmacology of platelet-affect1Og drugs.Circulallon 1980;62 (suppl V):V26-41
43. Holmsen H, Setkowsky CA, Lages B, Day JH, Weiss JH, ScruttonMC. Content and thrombin-induced relea,e of acid hydrolase, in gelfiltered platelets from patients WIth storage pool deficiency Blood1975;46:131-42
44. Roth GL, Majerus PW. The mechamsm of the effect of aspmn onhuman platelets I. Acetylation of a particulate fractIon protem. J ClinInvest 1975;56:624-32.
45 Burch JW, Stanford N, Majerus PW. InhIbillon of platelet prostaglandm synthetase by oral aspmn. J Clin Invest 1978;61:314-9.
46. Demers LM, Budm R, Shaikh B. The effects of aspinn on megakaryocyte prostaglandin productIOn. Blood 1977;50 239-47.
47. Jaffe EA, Weksler BB. Recovery of endothelial cell prostacyclin producllon after inhibition by low doses of aspirin. J Clin Invest1979;63:532-5.
48 Weksler BB, Pett SB. RIchter RC, et al. Differential 1OhIbitlOn byaspmn of vascular and platelet prostaglandin synthesis 10 atherosclerotic pallents. N Engl J Med 1983;308:800-5
49 Linos A, Worth1Ogton JW, O'Fallon W, Fuster V, Whlstnant JP.Kurland LT Effect of aspIrin on preventIOn of coronary and cerebrovascular disease in patients WIth rheumatoid arthntis. A long-termfollow-up study. Mayo Clin Proc 1978,53:581-6.
50. Wood L Aspirin and myocardIal infarcllon. Lancet 1972;2.1021-2
51 Tschopp TB. Aspmn 10hibits platelet aggregallon on but not adhesionto collagen fibnls: an assessment of platelet adheSIOn and depositedplatelet mass by morphometry and 51-Cr-Iabeling. Thromb Res1977;11.619-32.
52 Weiss HJ, Tschopp TB, Baumgartner HR. Impalfed 1Oteracllon (adhesion-aggregatIOn) of platelet, WIth the subendothelium 10 storage-pooldIsease and after asplfin ingestion. A comparison WIth von Willebrand's disease. N Engl J Med 1975;293:619-23.
53. K1Olough-Rathbone RL, Cazenave J-P, Packham MA, Mustard JFEffect of 1Ohibltors of arachidonate pathway on the release of granulecontents from rabbit platelets adherent to collagen. Lab Invest1980,42.28-34.
54. Clowes AW, Karnovsky MJ. Failure of certain anllplatelet drugs toaffect myointimal thickening followmg arterial endothelial injUry 10the rat Lab Invest 1977;36:452-64.
55. Kelton JG, HIrsh J, Carter CJ, Buchanan MR. Thrombogenic effectof high-dose aspmn m rabbIts. RelationshIp to mhIbitlOn of veSi>elwall syntheSIS of prostaglandin Ie-like actIVIty. J Clin Invest 1978;62:892-5.
56 Needleman P, Kulkarni PS, Raz A. Coronary tone modulallon: formallon and acllons of prostagland1Os, endoperoxide, and thromboxanes. Science 1977,195:409-12.
57. Berk BC, Alexander RW, Brock TA, Gimbrone MA Jr, Webb RC.Vasoconstncllon: a new activity for platelet-denved growth factor.Science 1986;232:87-90.
58. Folts JD, Crowell EB, Rowe GG. Platelet aggregatIOn 10 partiallyobstructed vessels and Its elimmation WIth aspIrin. CIrculation1976;54:365-70.
59 Vik-Mo H. Effects of acute myocardial ischaemIa on platelet aggregallon m the coronary sinus and aorta in dogs. Scand J Haematol1977,19:68-74.

lACC Vol. 8, No 6December 1986:21 B-32B
HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
31B
60. Vik-Mo H. Platelet accumulatIon in the myocardium dunng acutenonthrombotic coronary artery occlusIon in dogs. Scand 1 Haematol1978,21:225-32.
61. Dale 1, Myhre E, Storstem 0, Stonnorkew H, Efskmd L. PreventIonof arterial thromboembolIsm with acetylsalIcyclic acid. A controlledclinical study m patients wIth aortic ball valves. Am Heart 11977;94:101-11.
62 Harter HR, Burch lW, Majerm PW, et al. Prevention of thrombosIsin patIents on hemodIalysis by low-dose aspmn N Engl 1 Med1979;301577-9.
63. Canadian Cooperative Study Group. A randomized tnal of aspinn andsulfinpyrazone m threatened stroke. N Engll Med 1978;299.53-9.
64. Lewis HD, DaVIS lW, Archibald DG, et al. ProtectIve effects of aspirinagainst acute myocardial mfarcllon and death in men with unstableangina. N Engl 1 Med 1983;309:396-403
65. Caims lA, Gent M, Singer 1, et al. Aspinn, sultinpyrazone or bothin unstable angina. results of a Canadian multIcenter trial. N Engl 1Med 1985:313:1369-75.
66. Lorenz RL, Weber M, Kotzur 1. et al. Improved aortocoronary bypasspatency by low-dose aspIrin (100 mg/dally) Effects on platelet aggregatIon and thromboxane formatIOn. Lancet 1984; I: 1262-4
67. Hanson SR, Harker LA, BJomsson TD Effects of platelet-modIfyingdrugs on artenal thromboembolism in baboons. Aspmn potenllatesthe antIthrombollc actIOns of dipyndamole and sulfinpyrazone bymechamsm(s) independent of platelet cyclooxygenase mhlbition. JClin Invest 1985;75:1591-9.
68. SImon LS, Mills JA. Non-steroIdal anti-inflammatory drugs N Engl1 Med 1980;302: 1179-85.
69. Moncada S, Bunting S, Mullane K, et al. ImIdazole-selectIve inhIbItorof thromboxane synthetase. Prostaglandins 1977;13:611-8.
70. Mills DCB, Smith lB. The mfluence on platelet aggregatIOn of drugsthat affect the accumulation of adenosme 3'-5' -cyclIc monophosphatem platelets. BIochemIstry J 1971;121:185-96.
71. Haslam Rl, Davidson MML, DaVies T, Lynham lA, McClenaghanMD. Regulation of blood platelet functIon by cyclic nucleotldes AdvCyclic Nucleotide Res 1978:9'533-52.
72. Moncada Sand Korbut R Dipyndamole and other phosphodiesterasemhibitors act as antithrombotIc agents by potentiatmg endogenousprostacyclin Lancet 1978; I: 1286-9.
73. Cazenave l-P, DeJana E, Kinlough-Rathbone RL, et al. Prostaglandins1-2 and E-I reduce rabbit and human platelet adherence Without inhibiting serotonm release from adherent platelets. Thromb Res1979;15:273-9.
74 Lefer AM, Ogletree ML, Smith lB, et al. ProstacyclIn: a potentIallyvaluable agent for preserving myocardial tissue in acute myocardialischemia. Science 1978:200:52-4.
75. Aiken lW, Gonnan RR, Shebuski RJ Prevention of blockage ofpartially obstructed coronary arteries WIth prostacyclin correlates WIthinhibition of platelet aggregatIOn. Prostaglandins 1979,17:483-94
76. Gryglewskl RJ, Szceklik A, Nizankowskl R Anti-platelet action ofintravenous mfusion of prostacyclin m man. Thromb Res1978;13:153-63.
77. Woods HF, Ash G, Weston Ml, Bunting S, Moncada S, Vane lRProstacyclin can replace hepann m haemodialysls in dogs. Lancet1978;2: 1075-7.
78. Rosenblum WI, EI-Sabban F. TopIcal prostacyclin (PGb) mhibltsplatelet aggregatIon in pial venules of the mouse. Stroke1979;10:399-401
79. Bourgain RH. The mhibitory effect of PGb (prostacyclIn) on whiteplatelet artenal thrombus formation. Haemostasis 1979;8:117-9.
80. Coppe D, Wonder T, Snider M, Salzman E. Preservation of plateletnumber and functIOn durmg extracorporeal membrane oxygenation(ECMO) by regional infusion of PGI-2 (abstr). CIrculation 1978;58(suppl1I):II-207.
81. Bolger PM, Eisner GM, Ramwell PW, Slotkoff LM, Corey El. RenalactIons of prostacyclin. Nature 1978;271 :467-9.
82. Needleman P, Bronson SD, Wyche A, Sivakoff M, Nicolaou KC.Cardiac and renal prostaglandin b. BIOsynthesIs and biological effectin isolated perfused rabbit tissues. 1 Clin Invest 1978;61:839-49.
83. Szezeklik A, Gryglewski Rl, Nlzankowski R, Musial 1, Pieton R,Murk 1. Circulatory and ant Iplatelet effects of mtravenous prostacyclinin healthy men Phannacol Res Commun 1978,10:545-66.
84. Crutchley Dl, Ryan US, Ryan lW. Effects of aspirin and dipyridamoleon the degradation of adenosme diphosphate by cultured cells derivedfrom bovine pulmonary artery. 1 Ciin Invest 1980;66:29-35.
85 Gresele P, Zoja C. Deckmyn H, Amout 1, Vermylen 1. Verstaete MDipyndamole inhIbits platelet aggregation m whole blood. ThrombHaemost 1983;50:852-6.
86. Klabunde RE. Dipyridamole inhibItion of adenosme metabolism mhuman blood Eur 1 Pharmacol 1983;93:21-6
87. Sattim A, Rail T. The effect of adenosine and adenine nucleotldes onthe cyclIc adenosine 3'-5'-phosphate content of gumea pig cerebralcortex slices Mol Pharmacol 1970;6:13-23.
88. Roberts A1. lacobstem lG. Clpnano PR, Alonso DR, Combes lR,Gay WA Jr. Effecllveness of dlpyndamole in reducmg the size ofexpenmental myocardial mfarction. Circulation 1980,61:228-36.
89 Cazenave l-P, Packham MA, Kmlough-Rathbone RL, Mustard RF.Platelet adherence to the vessel wall and to collagen-coated surfaces.Adv Exp Med BIOI 1978;102:31-49.
90. Kmlough-Rathbone RL, Groves HM, Cazenave l-P, RIchardson M,Mustard IF Effect of dipyridamole and aspmn on platelet adherenceto damaged rabbit aortas in VItro and m vivo (abstr). Fed Proc1978;37:260.
91. Harker LA, Hanson SR, Kirkman TR Expenmental arterial thromboembolIsm m baboons. Mechamsm, quanlltation, and pharmacologICprevention. 1 Clm Invest 1979;64:559-69
92. Harker LA, Slichter Sl. Studies of platelet and fibrinogen kmetics inpallents wIth prosthetic heart valves. N Engll Med 1970;283: 1302-5
93. Weily HS, Steele PP, Davies H. Pappas G, Genton E Platelet survivalm patIents WIth substitute heart valves. N Engll Med 1974;290:534-6
94. Harker LA Platelet surVIval tIme: Its measurement and use. ProgHemost Thromb 1978;4:321-47.
95. Sullivan 1M, Harken DE, Gorlin R. Pharmacologic control of thromboembolIc complications of cardiac-valve replacement. N Engll Med1971 ;284: 1391-4
96. Harker LA. Slichter S1. Sauvage LR Platelet consumption by arterialprostheses: the effects of endothelialization and pharmacologIC inhlblllon of platelet function Ann Surg 1977;158:594-601
97. Ritchie lL, Harker LA. Platelet and fibrinogen survival in coronaryatheroscleroSIS response to medICal and surgIcal therapy. Am 1Cardiol1977;39:595-8.
98. Fuster V, Chesebro lH, Frye RL, Elveback LR. Platelet surVival andthe development of coronary artery disease in the young: the effectsof cIgarette smoking, strong family history, and medical therapy.CIrculation 1981 ;63.546-5 I
99. Klimt CR, Knatterud GL, Stamler 1, Meier P and the PersantineAspmn ReinfarctIon Study Research Group. Part II. Secondary coronary prevention WIth persantme and aspinn. 1 Am Coli Cardiol1986;7'251-69.
100. Donadio lV lr, Anderson CF, MitchelllC III, et al. MembranoproIIferatIve glomerulonephntis. A prospective climcal trial of plateletmhlbltor therapy. N Engll Med 1984;310:1421-6
101. Chesebro lH, Clements IP, Fuster V, et al. A platelet inhibitor-drugtnal m coronary-artery bypass operatIOns. Benefit of perioperativedlpyndamole and aspinn therapy on early postoperative vem-graftpatency. N Engl J Med 1982.307.73-8.
102. Chesebro lH. Fuster V, Elveback LR, et al. Effect of dipyridamole

328 HARKER AND FUSTERPHARMACOLOGY OF PLATELET INHIBITORS
lACC Vol X. No 6December 19X6 21B-32B
and aspirin on late veIn-graft patency after coronary bypass operations. N Engl J Med 1984;310:209-14.
103. The PersantIne-Aspinn ReInfarction Study Group. Persantine andaspinn In coronary heart disease Circulation 1980;62:449-61
104. Bousser MG, Eschwege E, Haugenau M, et al. "AICLA" controlledtrial of aspirin and dipyridamole in the secondary prevention of athero-thrombotic cerebral ischemia. Stroke 1983;14:5-14.
105 American-CanadIan Cooperative Study Group. Persantine-aspirin tnalIn cerebral Ischemia. Part II: endpOInt results. Stroke 1985;16:406-15.
106. Brown BG, CukIngman RA, DeRouen T, et al. Improved graft patency in patients treated with platelet-Inhibiting therapy after coronarybypass surgery. Circulation 1985;72: 138-46.
107. Hess H, Mletaschk A, Deichsel G. Drug-induced Inhibition of plateletfunctIOn delays progression of penpheral occlusive arterial disease.A prospective double-blind arteriographically controlled trial Lancet1985;1:415-21.
108. Rosenberg RD. Heparin, antithrombin, and abnormal clotting. AnnRev Med 1978;29:367-78.
109. Salzman EW, Rosenberg RD, SmIth MH, LIndon IN. Favreau L.Effect of hepann and heparin fractions on platelet aggregation. J ClInInvest 1980;65:64-73.
110. Zucker MB. Effects of heparin on platelet function. Thromb DlathHaemorrh 1975;33.63-5.
III. Lam LH, Silbert JE, Rosenberg RD. The separatIOn of active andInactive forms of heparin. Biochem Blophys Res Commun1976;69:570-7.
112. Andersson L-O, Barrowcliffe TW, Holmer E, Johnson EA, SimsGEe. Anticoagulant properties of heparin fractIOnated by affinitychromatography on matrix-bound antithrombin III and by gel filtratIOn. Thromb Res 1976;9:575-83
113. Miletich JP, Jackson CM, Majerus PW. Properties offactor Xa bIndIng site on human platelets J Bioi Chern 1978;253:6908-16.
114 Saba HI, Saba SR, Blackburn CA, Hartmann RC, Mason RG. Heparin neutralization of PGI-2: effects upon platelets Science1979;205:499-50 I.
I IS Okamoto S, Hijikata A. Potent inhIbition of thrombin by the newlysynthesized arginine derivative No 805. The Importance of stereostructure of its hydrophobic carboxamide portion. Biochem BlophysRes Commun 1981;10 I:440-6.
116. Kumada T, Ablko Y Comparative study on heparin and a syntheticthrombin Inhibitor No 805 (MD-805) In expenmental antithrombinIII-defiCient animals Thromb Res 1981;24:285-92
117. Sturzebecher J, Markwardt F, VOIgt B, Wagner G, Walsmann P.Cyclic amides of N-alpha-arylsulfonylaminoacylated 4-amldinophenylalanine-tight bmding inhibitors of thrombIn. Thromb Res198329:635-42.
118 Butler KD, Wallis RB, White AM. A study of the relationship between ex vivo and in vivo effects of sulphInpyrazone in the guineapig. Haemostasis 1979;8:353-60.
119. Ali M, McDonald JWD. Effects of sulfinpyrazone on platelet prostaglandIn synthesis and platelet release of serotonin. J Lab Clin Med1977:89:868-75.
120. Buchanan MR, Rosenfeld J, HIrSch J. The prolonged effect of sulfinpyrazone on collagen-induced platelet aggregation in vivo ThrombRes 1978;13:883-92.
121. Baumgartner HR. Effects of acetylsalIcylIc acid, sulfinpyrazone anddipyndamole on platelet adhesion and aggregation in flowing nativeand anticoagulated blood Haemostasis 1979;8:340-52.
122. Harker LA, Harlan JM, Ross R. Effect of sulfinpyrazone on homocysteIne-induced endothelial injury and arteriosclerosis In baboons. Circ Res 1983;53:731-9.
123. Steele P, Rainwater J, Vogel R. Platelet suppressant therapy in patients with prosthetic cardIac valves: relationship of clInical effec-
tlveness to alteration of platelet surVival time CirculatIOn1979;60'910-3
124 Kaegi A, PIneo GF, Shimizu A, Tnvedl H, Hirsh J, Gent M. Artenovenous-shunt thrombosis: prevention by sulfinpyrazone. N EnglJ Med 1974,290:304-6.
125. Report from the Anturane ReinfarctlOn Study. Sulfinpyrazone in postmyocardial infarction. Lancet 1982: I:237-42.
126. Baur HR. Van Tassel RA, Pierach CA, Gobel RL. Effects of sulfinpyrazone on early graft closure after myocardial revascularizatlon.Am J CardlOl 1982:49'420-4
127. O'Brien JR Ticlopldine: a promISe for the prevention and treatmentof thrombOSIS and ItS complIcations. Haemostasls 1983;13:1-54.
128 Gordon JL Overview' pharmacology of tlclopidine. In: TlclopldIne:Quo Vadls" Agents and Actions Supplements, Vol 15. Germany'Blrkhauser Verlag, 1984:1-312.
129 WilkInson AR, Hawker RJ, Hawker JM. The Influence of antlplateletdrugs on platelet survival after aortic damage or implantation of adacron arterial prosthesIS. Thromb Res 1979; IS: 181-9
130. Reece AH. Walton PL Inhibition of intimal proliferation of rabbitaorta by tlclopldIne(abstrl. Thromb Haemost 1979;42:367.
131. Johnson M, Heywood 18 POSSible mode of actIOn of ticlopldine. anovel Inhibitor of platelet aggregatlOn(abstr). Thromb Haemost1979.42.367
132. Brown CH III, Bradshaw MW, Natelson EA, Alfrey CP Jr, WillIamsTW Jr Defective platelet function following the admimstratlon ofpemciliin compounds. Blood 1976;47:949-56.
133. Cazenave J-P, GuccIOne MA, Packham MA, Mustard JF. Effects ofcephalothIn and pemcIllin G on platelet functIOn in Vitro. Br J Haematol 1977;35: 135-52.
134. Shattil SJ. Bennett JS, McDonaugh M, Turnbull J Carbenicillin andpenicillIn G inhibit platelet function in vitro by Impairing the InteractIOn of agonists With the platelet surface. J Clin Invest1980,65 329-37.
135. Ewald RA, Eichelberger JW, Young AA, Weiss HJ, Crosby WHoThe effect of dextran on platelet factor 3 actiVity: In vitro and in VIVOstudies. TransfUSIOn 1965;5: 109-19.
136. Bygdeman S. Eliasson R. Effect of dextrans on platelet adhesivenessand aggregation. Scand J Clin Lab Invest 1967;20: 17-23
137. Weiss HJ. The effect of clinical dextran on platelet aggregation,adheSion and ADP release in man: In VIVO and In Vitro stUdies. J LabClin Med 1967:69:37-46
138. Oberg M, Hedner U, Bergentz S-E Effect of dextran 70 on factorVIII and platelet function In von Willebrand's disease. Thromb Res1978.12:629-34
139. Roba J, Defreyn G. Biagi G. Antlthrombotlc actiVity of suloctidilThromb Res 1983;4:53-8.
140. Col-Debeys C, Ferrant A, Monau M. Effects of suloctldil on plateletsurvival time following cardiac valve replacement. Thromb Haemost1981;46:550-3.
141. Ciavarella N, Antoncecchl S, E'ElIa N, Ettorre C, Raniere P, ManZIni A. NormalIzation by suloctldil of decreased platelet surVival Inpatients with heart prosthetIC valves in randomized controlled doublehlInd trial(abstr). Thromb Haemost 1981.46:308
142. Gent M, Blakely JA, HachinskI V, ct al. A secondary preventionrandomized tnal of suloctidil in patients with a recent history ofthromboembolIc stroke. Stroke 1986;16'416-24
143. Hanson SR, Harker LA. Studies of suloctidil In expenmental thrombosIS in baboons. Thromb Haemost 1985.53:423-7.
144. Steiner M, Anastasi J. Vitamin E. An inhibItor of the platelet releasereactIOn J CIIn Invest 1976:57:732-7.
145. Butler AM, Gerrard JM, Peller 1, Stoddard SF, Rao GHR, WhiteJG. Vitamin E inhibits the release of calcium from a platelet membrane fraction in vitro Prostaglandins Med 1979,2'203-16