Embed Size (px)
Citation preview

DOI:10.1093/jnci/dju283First published online September 25, 2014
JNCI | Article 1 of 10
© The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: [email protected].
jnci.oxfordjournals.org
Article
Pharmacological relevance of endoxifen in a laboratory Simulation of Breast cancer in Postmenopausal PatientsPhilipp Y. Maximov, Russell E. McDaniel, Daphne J. Fernandes, Puspanjali Bhatta, Valeriy R. Korostyshevskiy, Ramona F. Curpan, V. Craig Jordan
Manuscript received December 13, 2013; revised July 24, 2014; accepted August 1, 2014.
Correspondence to: V. Craig Jordan, OBE, PhD, DSc, FMedSci, Oncology and Pharmacology, Georgetown University Medical Center, 3970 Reservoir Rd NW, Research Building, Suite E501, Washington, DC 20057 (e-mail: [email protected]).
Background Tamoxifen is metabolically activated via a CYP2D6 enzyme system to the more potent hydroxylated derivatives 4-hydroxytamoxifen and endoxifen. This study addresses the pharmacological importance of endoxifen by simu-lating clinical scenarios in vitro.
Methods Clinical levels of tamoxifen metabolites in postmenopausal breast cancer patients previously genotyped for CYP2D6 were used in vitro along with clinical estrogen levels (estrone and estradiol) in postmenopausal patients determined in previous studies. The biological effects on cell growth were evaluated in a panel of estrogen recep-tor–positive breast cancer cell lines via cell proliferation assays and real-time polymerase chain reaction (PCR). Data were analyzed with one- and two-way analysis of variance and Student’s t test. All statistical tests were two-sided.
Results Postmenopausal levels of estrogen-induced proliferation of all test breast cancer cell lines (mean fold induc-tion ± SD vs vehicle control: MCF-7 = 11 ± 1.74, P < .001; T47D = 7.52 ± 0.72, P < .001; BT474 = 1.75 ± 0.23, P < .001; ZR-75-1 = 5.5 ± 1.95, P = .001. Tamoxifen and primary metabolites completely inhibited cell growth regardless of the CYP2D6 genotype in all cell lines (mean fold induction ± SD vs vehicle control: MCF-7 = 1.57 ± 0.38, P = .54; T47D = 1.17 ± 0.23, P = .79; BT474 = 0.96 ± 0.2, P = .98; ZR-75-1 = 0.86 ± 0.67, P = .99). Interestingly, tamoxifen and its primary metabolites were not able to fully inhibit the estrogen-stimulated expression of estrogen-responsive genes in MCF-7 cells (P < .05 for all genes), but the addition of endoxifen was able to produce additional anties-trogenic effect on these genes.
Conclusions The results indicate that tamoxifen and other metabolites, excluding endoxifen, completely inhibit estrogen-stimulated growth in all cell lines, but additional antiestrogenic action from endoxifen is necessary for complete blockade of estrogen-stimulated genes. Endoxifen is of supportive importance for the therapeutic effect of tamox-ifen in a postmenopausal setting.
JNCI J Natl Cancer Inst (2014) 106(10): dju283 doi:10.1093/jnci/dju283
Tamoxifen, a nonsteroidal antiestrogen, is a pioneering therapy for the treatment of breast cancer targeted to the tumor estrogen receptor (ER) (1). The laboratory strategy (2) of targeting tumor ER with long-term antihormone therapy accurately translated to clinical practice with enhanced control of disease recurrence fol-lowing long-term adjuvant therapy in both pre- and postmenopau-sal patients. This targeted adjuvant treatment strategy ultimately resulted in a 30% decrease in mortality (3–6). Indeed, long-term (five years) adjuvant tamoxifen therapy contributes substantially to national statistics with the reduction in death rate from breast can-cer during the past decade (7).
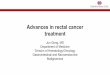
Early findings demonstrated that tamoxifen is metabolically activated to 4-hydroxytamoxifen (Figure 1) that has a hundred-fold increase in affinity for the ER (8,9). However, high affinity of a ligand for the ER is an advantage but not a requirement
for antiestrogenic activity (10,11). Indeed, studies comparing the antitumor activity of tamoxifen and 4-hydroxytamoxifen (4OHT) in vivo demonstrated that tamoxifen was the supe-rior agent for clinical development (10). 4-Hydroxytamoxifen is cleared from the body faster than tamoxifen while the par-ent drug tamoxifen accumulates (12). Nevertheless, the sub-sequent identification of 4-hydroxy-N-desmethyltamoxifen (13–15) (later called endoxifen) (Figure 1) and the demonstra-tion of a reduction of endoxifen production in women taking Selective Serotonin Reuptake Inhibitors (SSRI) (for reduction of hot flashes), which block the enzymatic activity of CYP2D6 (16), suggested that this important drug interaction reduces tamoxifen’s efficacy. Subsequently, a hypothesis was developed and connected with genotypic aberrations in CYP2D6 alleles (17). The hypothesis depends on the concept that different
October 8 dju283
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

Vol. 106, Issue 10 | dju283 | October 8, 20142 of 10 Article | JNCI
polymorphisms of CYP2D6 can result in altered enzymatic activity of the cytochrome P450 2D6, which results in differ-ent rates of tamoxifen metabolism and thus different levels of tamoxifen metabolites N-desmethyltamoxifen (NDMTAM) and endoxifen. Some clinical studies have shown association between the CYP2D6 genotypes and the clinical outcomes (18–20), and some have not found any association (21–23). Numerous papers using retrospective clinical data presented convincing cases for or against the hypothesis. However, the low incidence of poor metabolizers (PM) (24), and the known poor compliance rate (25) of long-term antihormone therapies make the hypothesis difficult to validate in retrospective patient samples.
In this article we address the role of the CYP2D6 genotype dur-ing tamoxifen treatment of breast cancer in a laboratory simulation. We have characterized a panel of four representative ER-positive breast cancer cell lines, MCF-7, T47D, BT474, and ZR-75-1, and carefully calibrated their concentration responsiveness to both estradiol (E2) and estrone (E1). We selected concentrations of total estrogen (E1/E2) corresponding to the previously reported circu-lating levels in postmenopausal breast cancer patients (26,27). We address two hypotheses: 1) that tamoxifen is a prodrug that needs to be metabolically activated to NDMTAM and 4OHT, and 2) that circulating concentrations of tamoxifen and its two metabolites NDMTAM and 4OHT are sufficient to block estrogen-stimulated breast cancer cell growth and gene expression in a postmenopausal patient simulation. Our chosen concentrations of tamoxifen and metabolites have been determined recently for postmenopausal patients genotyped for CYP2D6 as extensive metabolizers (EM), intermediate metabolizers (IM), and PM (28). The experiment was repeated with all cell lines to address the second hypothesis with and without relevant concentrations of endoxifen for each
genotype. Overall, metabolic activation to endoxifen appears to play a supportive role in blocking estrogen-induced cell replication in breast cancer cell lines in a simulated model of postmenopausal breast cancer. Conversion to endoxifen is perhaps consolidating the long-term benefits of antiestrogen therapy but is not essential for the immediate antiestrogenic antitumor actions of tamoxifen in the postmenopausal setting.
MethodsCells and Culture ConditionsThe ER-positive human breast cancer cell lines MCF-7, T47D, BT474, and ZR-75-1 were used in this study. All cells were obtained from American Type Culture Collection (ATCC) and were main-tained in phenol-red RPMI 1640 medium. All cultures were grown in 5% CO2 at 37°C. All cell lines were verified using DNA finger-printing analysis performed at the tissue culture shared resource at the Lombardi Comprehensive Cancer Center (29).
Cell Proliferation AssaysAll cells were cultured in estrogen-free medium (phenol red-free Roswell Park Memorial Institute 1640 media supplemented with 10% charcoal-stripped fetal bovine serum) for three days before beginning the proliferation assay. The proliferation assays were performed after a seven-day treatment as previously described (BibXref) using a fluorescent DNA quantification kit and calf thymus DNA for the standard curve. To study the pharmacologi-cal importance of endoxifen we simulated the postmenopausal estrogen setting for patients in each of our cell lines and used the actual clinical concentrations of tamoxifen and its metabo-lites found in patients previously genotyped for CYP2D6 and
Figure 1. The chemical structures of all metabolites of tamoxifen in this study and their metabolism pathways and metabolizing cytochrome P450 (CYP) enzymes with relative binding affinities (RBAs) for the estrogen receptor (ER). Tamoxifen is metabolically activated to 4-hydroxytamoxifen (4OHT) and endoxifen (N-desmethyl-4-hydroxytamoxifen) by the CYP2D6 enzyme system. Tamoxifen is also metabolized into N-desmethyltamoxifen (NDMTAM), which has a similar RBA for the ER as tamoxifen. 4OHT = 4-hydroxytamoxifen; ER = estrogen receptor; RBA = relative binding affinity.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

JNCI | Article 3 of 10jnci.oxfordjournals.org
treated with tamoxifen (Supplementary Table 1, available online). To simulate the clinical setting in vitro we selected a panel of ER-positive human breast cancer cell lines: MCF-7, T47D, BT474, and ZR-75-1; all were previously shown to be ER-positive (31) by western blotting and estrogen-responsive for growth. Experiments, each consisting of three replicates, were performed at least three times.
Real-Time Polymerase Chain ReactionReal-time polymerase chain reaction (PCR) was performed as previously described (32). Primers sequences that were used for human pS2 cDNA amplification are: 5’-CAT CGA CGTCCCTCCAGAAGA-3’ sense, and 5’-CTCTGGGACT AATCACCGTGCTG-3’ anti-sense; human GREB1 gene: 5’-CAAAGAATAACCTGTTGGCCCTGC-3’sense, 5’-GA CAT GCCTGCGCTCTCATACTTA-3’ anti-sense; human proges-terone receptor (PgR): 5’-CGTGCCTATCCTGCCTCTCAA-3’ sense, 5’-CCGCCGTCGTAACTTTCGT-3’ anti-sense; the ref-erence gene 36B4: 5’-GTGTTCGACAATGGCAGCAT-3’ sense, 5’-GACAC CCTCCAGGAAGCGA-3’ anti-sense. All primers were obtained from Integrated DNA Technologies Inc. (Coralville, IA). Experiments, each consisting of three replicates, were per-formed at least three times.
ImmunoblottingImmunoblotting was performed as previously described (30). The membranes were probed with rabbit polyclonal anti-ERα antibody at 1:500 dilution (Santa Cruz Biotechnology, Santa Cruz, CA) and with mouse monoclonal anti-β-actin antibody at 1:40,000 dilution (Sigma-Aldrich, St. Louis, MO) antibodies, as recommended by the supplier. All protein levels were analyzed by densitometry using ImageJ software (NIH). Experiments, each consisting of three rep-licates, were performed at least three times.
Molecular ModellingThe experimental X-ray structures of ERα LBD to be used for docking were selected from Protein Databank (33) based on the three-dimensional shape similarity between the compounds to be docked and cocrystallized ligands extracted from the recep-tor-ligand complex similarity. The three-dimensional shape was computed using the Rapid Overlay of Chemical Structures utility of Openeye. The ligands of interest were used as the query data-set while the screening library was compiled from the ligands extracted from all of the available crystal structures of human ERα deposited in the Protein Data Bank (PDB). ShapeTanimoto parameter was used for scoring with a cutoff value of 0.8, and four ligands met this criterion. The 3D coordinates of the correspond-ing ERα complexes were extracted from PDB entries 3ERT (34). Subsequently, the structures were prepared for docking using the Protein Preparation Workflow (Schrödinger, LLC, New York, NY, 2011) accessible from within the Maestro program (Maestro, version 9.2; Schrödinger, LLC, New York, NY, 2011). Briefly, the hydrogens were properly added to the complexes, water mol-ecules beyond 5Å from a heteroatom were deleted, bond correc-tions were applied to the cocrystallized ligands, the orientation of hydroxyl groups, Asn, Gln and the protonation state of His were optimized to maximize hydrogen bond formation. All Asp,
Glu, Arg, and Lys residues were left in their charged state. In the final stage, a restrained minimization on the ligand-protein com-plexes was carried out with the OPLS_2001 force field, and the default value for root-mean-square deviation of 0.30Å for non-hydrogen atoms was used. Docking simulations were performed with Glide software (Glide, version 5.7; Schrödinger, LLC, New York, NY, 2011), a grid-based docking method that can be run rigid or fully flexible for the ligand (35,36). To some extent, a degree of flexibility was allowed to the X-ray structures of ERα in agonist conformation by scaling down the van der Waals radii of nonpolar atoms with a scale factor of 0.8 and allowing the free rotation of hydroxyl groups.
Statistical AnalysisTo test the interactions between treatment and genotype in the pro-liferation assays, we used analysis of variance (ANOVA) with a bal-anced two-factor design. When a statistically significant interaction was present, we used one-way ANOVA to investigate simple effects of the independent factors. A P value less than .05 was considered significant. All computations were carried out using R, Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria). For testing the signifi-cance of treatment in RT-PCR experiments, the Student’s t test was used. All statistical tests were two-sided.
resultsEffects of Estrogens, Tamoxifen and Metabolites, and Endoxifen on Cell ProliferationConcentration response curves for all cell lines with increasing concentrations of either E1 or E2 are shown in Figure 2. The estrogen levels in postmenopausal patients treated with tamoxifen alone that were used are based on the calculated levels of E1 and E2 in patient plasma reported in the literature (26,27). The recal-culated concentrations used for all assays were 7.8x10-11M for E1 (which corresponds to the average 21 pg/mL in patient plasma) and 4.7x10-11M for E2 (which corresponds to the average 13 pg/mL in patient plasma); these concentrations combined were used in subsequent treatments of the cells to simulate the postmenopau-sal setting. Estrogen levels were also consistent with plasma levels reported by other groups (37,38) for postmenopausal patients. To simulate the clinical setting of postmenopausal patients treated with tamoxifen, we used concentrations of tamoxifen and all its metabolites previously published for a clinical study of differ-ent CYP2D6 genotypes (28) (Supplementary Table 1, available online). The metabolic activation of tamoxifen to endoxifen by different CYP2D6 genotypes occurs at different rates, resulting in different plasma levels of endoxifen, NDMTAM, and tamox-ifen itself. 4OHT remains consistently low. Using the published concentrations of tamoxifen and its metabolites, along with the calculated concentrations of estrogens, we treated all cell lines and assessed the biological effect on growth using a seven-day proliferation assay.
All cell lines (Figure 3) were responsive to treatment with the estrogen combination (E1/E2) alone (mean fold induction ± SD vs vehicle control: MCF-7 = 11 ± 1.74, P < .001 [Figure 3A]; T47D = 7.52 ± 0.72, P < .001 [Figure 3B]; BT474 = 1.75 ± 0.23,
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

Vol. 106, Issue 10 | dju283 | October 8, 20144 of 10 Article | JNCI
P < .001 [Figure 3C]; ZR-75-1 = 5.5 ± 1.95, P = .001 [Figure 3D]; all P by one-way ANOVA).
The addition of tamoxifen plus primary metabolites NDMTAM and 4OHT (TPM) to E1/E2 (Figure 3) completely inhibited estrogen-stimulated cell growth (mean fold induction ± SD vs vehicle control: MCF-7 = 1.57 ± 0.38, P = .54 [Figure 3A]; T47D = 1.17 ± 0.23, P = .79 [Figure 3B]; BT474 = 0.96 ± 0.2, P =. 98 [Figure 3C]; ZR-75-1 = 0.86 ± 0.67, P = .99 [Figure 3D]; all P by one-way ANOVA).
Addition of endoxifen to the TPM and E1/E2 treatment (Figure 3, A-D, col. 6) did not produce a further antiestrogenic effect in any of the genotype groups (P = .82 for MCF-7, P = .95 for T47D, P = .95 for BT474, and P = .99 for ZR-75-1; one-way ANOVA compared with TPM + E1/E2). Assessment of endoxifen’s pharmacological impact when added to the TPM + E1/E2 treat-ment in all tested cell lines using a two-way ANOVA approach did not reveal any statistically significant antiestrogenic effect enhancement in any of the genotype categories, with all P values higher than .05.
To assess the importance of the active metabolite 4OHT, we performed proliferation assays in our panel of cells after treatment with postmenopausal concentrations of estrogens and estrogens in combination with tamoxifen and NDMTAM, and estrogens
in combination with tamoxifen and its primary metabolites. The results demonstrate that treatment with tamoxifen plus the pri-mary metabolite NDMTAM at concentrations corresponding to patients with EM genotype (Supplementary Table 1, available online) inhibited the estrogen stimulated growth of MCF-7 cells by 39.62 ± 2.26% (P = .02, Student’s t test) (Figure 4A, col. 3); however, addition of 4OHT in the EM genotype concentration (Supplementary Table 1, available online) completely inhibited the proliferation action of estrogens (94.72 ± 0.06% average inhibition vs E1/E2 treatment (P = .15 vs vehicle control, Student’s t test) (Figure 4A).
Additionally, we assessed the biological effect of tamoxifen metabolites in a postmenopausal setting in hypothetical osteoporo-tic women. To simulate an osteoporotic scenario, we used estrogen concentrations 10-fold lower than the average concentrations used in our study, which coincides with estrogen plasma levels in post-menopausal patients from the clinical study of osteoporotic women determined in the results for the analysis of the Multiple Outcomes of Raloxifene Evaluation study (39). The results demonstrated that treatment of the MCF-7 breast cancer cell line with a combina-tion of tamoxifen and primary metabolites without endoxifen com-pletely inhibit estrogen action (Supplementary Figure 1, available online).
Figure 2. Dose response cell-growth curves to estrone (E1) and estradiol (E2) in A) MCF-7, B) T47D, C) BT474, and D) ZR-75-1 cell lines. Data represent means and error bars are SD from three independent experiments with three replicates.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

JNCI | Article 5 of 10jnci.oxfordjournals.org
Effect of Endoxifen on Estrogen-Stimulated GenesTo assess the estrogenic and antiestrogenic effect on the tran-scriptional activity of ER and estrogen-responsive gene expres-sion in MCF-7 cells, we focused on the contribution to the overall effect of estrogen and the antiestrogenic effect of either or both of the active metabolites 4OHT and endoxifen. We performed RT-PCR as described in the Methods section and used primers for GREB1, pS2, and PgR estrogen-responsive genes. Results for all genes were similar. We demonstrated that GREB1 (Figure 4B), a regulator of hormone response in breast cancer (40), was activated 333.42 ± 58.18-fold by estrogens compared with vehicle control (P = .005, Student’s t test). Addition of tamoxifen and NDMTAM reduced the estrogenic effect by 73 ± 5.3% of E1/E2 treatment, P = .015 compared with E1/E2 treatment alone, but was statistically significantly different from vehicle control (P = .007). Addition of 4OHT in EM concentration reduced the fold change in GREB1
mRNA levels even more when compared with the tamoxifen and NDMTAM combination treatment (down to 90 ± 1.08% of E1/E2 treatment, P = .022). Addition of endoxifen to tamoxifen and its pri-mary metabolite mix (TPM) completely inhibited the estrogenic effect, bringing the fold change down to control levels (P = .34). Additionally, we studied the effects of these treatments on other estrogen-responsive genes, such as pS2 (Figure 4C) and PgR (Figure 4D). Estrogens induced both genes; however, in both cases, addition of tamoxifen and NDMTAM to the E1/E2 mix elevated the average mRNA expression of these genes; however, this was not statistically significant (P = .26 for pS2, and P = .24 for PgR). Addition of 4OHT to tamoxifen and NDMTAM in both genes reduced mRNA expression (78.9 ± 1.34%, P = .006 for pS2; and 91 ± 2.4%, P = .04 for PgR compared with estrogen treatment). Addition of endoxifen (EN) to tamoxifen and primary metabolites (TPM) further inhibited the estrogen-stimulated expression of
Figure 3. Biological response to clinical levels of metabolites of tamoxifen with and without endoxifen, and in presence of postmen-opausal levels of estrogens in the media in A) MCF-7, B) T47D, C) BT474, and D) ZR-75-1 cell lines. All cells lines were treated for seven days with the indicated treatments after a three-day starvation in the estrogen-free media. The biological effect was assessed by DNA quantification assay. Treatments were made as follows in all cell lines (panels A-D): 1 = vehicle control, 2 = postmenopausal concentration
of E1/E2, 3 = tamoxifen plus primary metabolites (NDMTAM and 4OHT) (TPM), 4 = E1/E2 plus TPM, 5 = TPM plus endoxifen (EN), 6 = E1/E2 plus TPM plus EN. Data represent means and error bars are SD from three independent experiments with three replicates. P values from one-way analysis of variance. All statistical tests were two-sided. EM = extensive metabolizer; EN = endoxifen; IM = inter-mediate metabolizer; PM = poor metabolizer; TPM = tamoxifen plus primary metabolites.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

Vol. 106, Issue 10 | dju283 | October 8, 20146 of 10 Article | JNCI
the mRNAs but not statistically significantly vs TPM treatment (P = .23 for pS2, and P = .48 for PgR).
Effect of Tamoxifen and Metabolites on ERα Protein StabilityWe assessed the effect of tamoxifen and metabolites on ERα pro-tein stability after 24 hours of treatment in MCF-7 cells. Our results indicated that MCF-7 cells in a postmenopausal estrogen (E1/E2) environment reduced the levels of ERα protein by approx-imately 15% as measured by densitometry compared with vehicle control (Figure 5A, lane 2). Tamoxifen plus primary metabolites (TPM) at EM concentrations stabilized the levels of ERα by approximately 27% when compared with vehicle control as meas-ured by densitometry (Figure 5A, lane 3). In combination with E1/E2, TPM reversed the effect of estrogens on ERα, consistent with the antiestrogenic effect of tamoxifen (Figure 5A, lane 4) and stabilized the levels of the ERα protein by about 37% when com-pared with vehicle control. We compared the effects of endoxifen
from different sources (Dr. Margarete Fischer-Bosch-Institute of Clinical Pharmacology, Stuttgart, Germany; Indiana School of Medicine, Indaniapolis, IN; and the Mayo Clinic, Rochester, MN) in concentrations reported for patients with an EM genotype (Figure 5A). Results showed clear differences in the stabilization of the ERα protein, but we did not find any reduction in protein levels (Figure 5A). 4-Hydroxytamoxifen clearly stabilized the ERα protein levels at EM genotype concentrations by approximately 36% when compared with vehicle control. TPM and endoxifen prevented the estrogen-induced degradation of the ERα protein. ICI 182780 (fulvestrant) was used as a positive control for ER deg-radation at a 1µM concentration.
We assessed the effects of 4OHT and endoxifen on ERα pro-tein stability in MCF-7 cells at high concentrations of 1µM with 1nM E2 after 24 hours of treatment (Figure 5B). Treatment with 1 nM E2 treatment resulted in downregulation of the ERα protein by 50% compared with vehicle control as measured by densitom-etry. Treatments with 1 µM 4OHT alone and 1 µM endoxifen alone
Figure 4. The pharmacological importance of 4-hydroxytamoxifen (4OHT) in MCF-7 cells in the postmenopausal setting. A) The prolifera-tion assay after treatment of MCF-7 cells with tamoxifen plus primary metabolites (TPM) at extensive metabolizer (EM) concentrations to assess the importance of 4OHT. B) Real-time polymerase chain reac-tion (RT-PCR) results for GREB1 gene after treating MCF-7 cells with EM concentrations of TPM to assess the importance of 4OHT and endoxifen in regulating estrogen responsive gene expression. RT-PCR results for
the same treatments for C) pS2 and D) PgR. Treatments were made as follows in all cell lines (panels A-D): 1 = vehicle control, 2 = postmeno-pausal concentration of E1/E2, 3 = E1/E2 plus tamoxifen and NDMTAM, 4 = E1/E2 with tamoxifen plus primary metabolites NDMETAM and 4OHT (TPM), 5 = E1/E2 plus TPM plus endoxifen (EN). Data represent means and error bars are SD from three independent experiments with three replicates. P values from Student’s t test. All statistical tests were two-sided. EN = endoxifen; TPM = tamoxifen plus primary metabolites.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

JNCI | Article 7 of 10jnci.oxfordjournals.org
each stabilized the ERα protein by 100% and 90%, respectively, when compared with vehicle control as measured by densitometry. A combination of 1 nM E2, with either 1 µM 4OHT or endoxifen, reversed the estrogen-induced degradation of ERα (ERα protein stabilization by 92% with 4OHT and 54% with endoxifen when compared with vehicle control as measured by densitometry), show-ing the consistent antiestrogenic regulation of ERα protein stability with endoxifen.
Molecular Modelling of 4OHT and Endoxifen With the Ligand-Binding Domain of the ERThe superimposition of the top-ranked, induced-fit docking pose of endoxifen onto the ERα-4OHT complex shows a predicted binding alignment of endoxifen similar to that of 4OHT. The same H-bond network is recapitulated, which engages contacts between the phenolic hydroxyl group of endoxifen and E353, R394, and a crystallized water molecule. The core structures of both ligands overlap almost perfectly, the major difference being in the ami-noalkyl side chain. The positioning of the flexible methylaminoe-thyl group of endoxifen and the side chain of D351 is shifted when compared with the 4OHT complex. Thus, the carboxylate group of D351 is moved towards the aminomethyl group, lying 2.6 Å away, compared with 3.8 Å in the case of the 4OHT complex and being involved in a salt bridge formation. This indicates that the
conformation of the ER in complex with endoxifen is very similar to the known conformation of the ER-4OHT complex.
DiscussionTo our knowledge, this study is the first to employ the actual cir-culating concentrations of tamoxifen and its metabolites measured in tamoxifen-treated postmenopausal patients and used to block estrogen action from clinically derived plasma levels using a panel of human breast cancer cell lines. We found that tamoxifen and its primary metabolites in concentrations found in three CYP2D6 gen-otypes (EM, IM, and PM) are sufficient to inhibit estrogen-induced replication in the postmenopausal setting. We also established the importance of 4OHT as the active primary metabolite in the anti-estrogenic action of tamoxifen in the postmenopausal setting. The estrogenic steroids would be anticipated to accumulate in the cell by binding to the ER. However, at premenopausal levels of estrogens, we show an association between the antiestrogenic effect and the lev-els of endoxifen corresponding to different CYP2D6 genotypes (41).
Estrogens activate the ER and induce its transcriptional activ-ity via interaction with the estrogen-responsive gene promoters. Estrogen receptor protein turnover is required (42) to maintain the continuous transcription of mRNA. This turnover is achieved by proteosomal degradation of the ER protein. Binding of antiestro-gens, in particular 4OHT, blocks the ER and promotes stabilization
Figure 5. Effect of tamoxifen and metabolites on ERα protein sta-bility and molecular model of 4-hydroxytamoxifen (4OHT) action. A) Protein levels of ERα in MCF-7 cells after 24-hour treatment with extensive metabolizer (EM) concentrations of tamoxifen metabolites with and without endoxifen. The levels of ERα protein after treatment with tamoxifen metabolites are similar to upregulation after treatment
with 4OHT at EM concentration (Supplementary Table 1, available online). B) Protein levels of ERα in MCF-7 cells after treatment with 1nM E2, and tamoxifen primary metabolites 4OHT and endoxifen at 1µM indi-vidually and in combination. C) Endoxifen is docked within the same pocket that binds 4OHT in the antagonist conformation of ERα ligand binding domain. 4OHT = 4-hydroxytamoxifen.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

Vol. 106, Issue 10 | dju283 | October 8, 20148 of 10 Article | JNCI
of the ER protein (43). In contrast, Wu et al. (44) reported that endoxifen targets ERα protein for degradation in MCF-7 and T47D cells at higher concentrations (100 and 1000 nM) (44). However, these concentrations are not comparable with circulat-ing endoxifen concentrations in patients. The same authors used (44) circulating EM and PM genotype concentrations of endox-ifen with circulating concentrations of tamoxifen and its primary metabolites in MCF-7 cells and demonstrated ERα degradation only at EM levels of endoxifen. Endoxifen is biologically very simi-lar to 4OHT in breast cancer cells (45). According to the molecular model of 4OHT action (Figure 5C) (34), the structurally similar endoxifen should bind to the ER and induce a similar conforma-tion of the ER. The fact that the lone pair of electrons on the free nitrogen of endoxifen now interacts with the Asp351 means that it is not available to interact with the appropriate amino acid at Helix 12. This means that it is less likely to create a closed Helix 12, and the instability will result in destruction of accumulated ERα compared with 4OHT (Figure 5, A and B). This contrasts with the selective estrogen receptor modulators raloxifene and bazedoxifene that completely shield Asp351 and prevent Helix 12 closure. This is why the unstable complex is degraded (46,47). Fulvestrant, which completely disrupts the complex, is the extreme case of complex destruction (48).
Wu et al. (49) proposed a link between endoxifen-mediated destruction of ERα protein and levels of ERβ in the cells. However, the artificial overexpression of ERβ in cells may not accurately depict the natural mechanism of ERα degradation in tumors. MCF-7 cells have very low levels of ERβ expression compared with ERα. Breast tumors have very low expression of ERβ protein or mRNA (50–52) compared with ERα.
Tamoxifen and its metabolites regulate the transcriptional activity of estrogen-responsive genes. GREB1 plays a substantial role in breast cancer cell hormone-dependent proliferation (40). We demonstrate that tamoxifen and NDMTAM partially inhibit GREB1 estrogen-induced mRNA synthesis; however, addition of 4OHT and endoxifen statistically significantly enhances the anti-estrogenic activity of the tamoxifen metabolite pool (Figure 4B). These results show that endoxifen, unlike the short-term cell growth end point, actually plays a substantial role in inhibiting the estrogen-mediated activation of responsive genes. We further examined the role of endoxifen in the estrogen regulation of pS2 and PgR gene expression (Figure 4, C and D). Although these genes are not important for proliferation, they illustrate the diversity of responsiveness to tamoxifen and its metabolites. The addition of tamoxifen and NDMTAM elevated both pS2 and PgR, an effect that has been noted previously (53,54). Adding the other tamox-ifen metabolite 4OHT partially decreased gene expression of pS2 and PgR, but endoxifen suppressed gene expression further. It may be that these observations are relevant during prolonged adjuvant therapy (6) as incomplete suppression of gene function may lead to estrogen-stimulated proliferation, development of resistance, and, ultimately, recurrence. These conclusions are supported by a recent report by Hawse et al. (55).
This study also had some limitations. Although these data in vitro model the antiestrogen environment in postmenopausal patients taking tamoxifen in the short term, there are other dimen-sions to consider for therapeutic efficacy during adjuvant therapy.
Tamoxifen and metabolites are competitive inhibitors of estrogen-induced cell proliferation (56). Therefore, circulating and tumor cell estrogen levels are critical for successful antiestrogen therapy. We have demonstrated (41) that the efficacy of the metabolite mix for tamoxifen, and the role of endoxifen, is critically dependent upon the circulating estrogen levels. The studies that titrate endox-ifen in a parallel premenopausal model, ie, much higher circulating levels of estrone and estradiol, show that only by titrating down estrogen levels can the positive role of endoxifen be defined (41).
There is no laboratory model that can simulate the action of a decade of adjuvant therapy. It is now emerging that tamox-ifen and metabolites are not simply acting just as inhibitors of estrogen action, but there is a dynamic change in breast cancer cell population over years as selection pressure creates acquired resistance in micrometastases. The principle has recently been illustrated by the extended cell culture of aromatase inhibitor–resistant breast cancer cells incubated in a cytostatic environment for eight weeks. Cell populations change dramatically (57). For the future, we propose to monitor the evolution of breast cancer cell populations under the selection pressure of appropriate anti-estrogenic therapy for years. This will stimulate the evolution of cell populations during adjuvant therapy that become vulnerable to a woman’s own estrogen to trigger estrogen-induced apoptosis. This approach was originally used with tamoxifen to describe the evolution of acquired resistance of tumors in the athymic mouse model over years of treatment (58). This cytostatic mechanism of tamoxifen and its metabolites needs time, compliance and high endoxifen levels to create effective selection pressure in different estrogen environments over years. It is these interlocking factors that expose the vulnerability of breast cancer to estrogen-induced apoptosis that results in a decrease in mortality in the decade after tamoxifen is stopped (59). However, to extrapolate appropriately to clinical care it is important to appreciate the requirement to validate methodologies to determine the CYP2D6 genotyping, as there is a profound loss of heterozygosity of the gene in breast cancer tissue. This quality control issue in genotyping was empha-sized recently (60). In conclusion, based on the experimental data in vitro, in a panel of breast cancer cell lines in a postmenopausal setting, the presence of endoxifen in any concentration is second-ary for blocking growth but necessary to block estrogen-regulated genes completely.
references 1. Jordan VC. Tamoxifen: a most unlikely pioneering medicine. Nat Rev Drug
Discov. 2003;2(3):205–213. 2. Jordan VC. Tamoxifen: catalyst for the change to targeted therapy. Eur J
Cancer. 2008;44(1):30–38. 3. EBCTCG. Tamoxifen for early breast cancer: an overview of the ran-
domised trials. Lancet. 1998;351(9114):1451–1467. 4. Davies C, Godwin J, Gray R, et al. Relevance of breast cancer hormone
receptors and other factors to the efficacy of adjuvant tamoxifen: patient-level meta-analysis of randomised trials. Lancet. 2011;378(9793):771–784.
5. EBCTCG. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717.
6. Davies C, Pan H, Godwin J, et al. Long-term effects of continuing adju-vant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oes-trogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet. 2013;381(9869):805–816.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

JNCI | Article 9 of 10jnci.oxfordjournals.org
7. Berry DA, Inoue L, Shen Y, et al. Modeling the impact of treatment and screening on U.S. breast cancer mortality: a Bayesian approach. J Natl Cancer Inst Monogr. 2006;(36):30–36.
8. Jordan VC, Collins MM, Rowsby L, et al. A monohydroxylated metab-olite of tamoxifen with potent antioestrogenic activity. J Endocrinol. 1977;75(2):305–316.
9. Jordan VC, Dix CJ, Naylor KE, et al. Nonsteroidal antiestrogens: their biological effects and potential mechanisms of action. J Toxicol Environ Health. 1978;4(2–3):363–390.
10. Allen KE, Clark ER, Jordan VC. Evidence for the metabolic activation of non-steroidal antioestrogens: a study of structure-activity relationships. Br J Pharmacol. 1980;71(1):83–91.
11. Lieberman ME, Jordan VC, Fritsch M, et al. Direct and reversible inhibi-tion of estradiol-stimulated prolactin synthesis by antiestrogens in vitro. J Biol Chem. 1983;258(8):4734–4740.
12. Furr BJ, Jordan VC. The pharmacology and clinical uses of tamoxifen. Pharmacol Ther. 1984;25(2):127–205.
13. Mauvais-Javis P, Baudot N, Castaigne D, et al. trans-4-Hydroxytamoxifen concentration and metabolism after local percutaneous administration to human breast. Cancer Res. 1986;46(3):1521–1525.
14. Lien EA, Solheim E, Kvinnsland S, et al. Identification of 4-hydroxy-N-desmethyltamoxifen as a metabolite of tamoxifen in human bile. Cancer Res. 1988;48(8):2304–2308.
15. Lien EA, Solheim E, Lea OA, et al. Distribution of 4-hydroxy-N-desmeth-yltamoxifen and other tamoxifen metabolites in human biological fluids during tamoxifen treatment. Cancer Res. 1989;49(8):2175–2183.
16. Stearns V, Johnson MD, Rae JM, et al. Active tamoxifen metabolite plasma concentrations after coadministration of tamoxifen and the selective seroto-nin reuptake inhibitor paroxetine. J Natl Cancer Inst. 2003;95(23):1758–1764.
17. Jin Y, Desta Z, Stearns V, et al. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst. 2005;97(1):30–39.
18. Schroth W, Goetz MP, Hamann U, et al. Association between CYP2D6 polymorphisms and outcomes among women with early stage breast can-cer treated with tamoxifen. JAMA. 2009;302(13):1429–1436.
19. Lammers LA, Mathijssen RH, van Gelder T, et al. The impact of CYP2D6-predicted phenotype on tamoxifen treatment outcome in patients with metastatic breast cancer. Br J Cancer. 2010;103(6):765–771.
20. Madlensky L, Natarajan L, Tchu S, et al. Tamoxifen metabolite concen-trations, CYP2D6 genotype, and breast cancer outcomes. Clin Pharmacol Ther. 2011;89(5):718–725.
21. Lash TL, Cronin-Fenton D, Ahern TP, et al. CYP2D6 inhibition and breast cancer recurrence in a population-based study in Denmark. J Natl Cancer Inst. 2011;103(6):489–500.
22. Regan MM, Leyland-Jones B, Bouzyk M, et al. CYP2D6 Genotype and Tamoxifen Response in Postmenopausal Women with Endocrine-Responsive Breast Cancer: The Breast International Group 1–98 Trial. J Natl Cancer Inst. 2012;104(6):441–451.
23. Rae JM, Drury S, Hayes DF, et al. CYP2D6 and UGT2B7 Genotype and Risk of Recurrence in Tamoxifen-Treated Breast Cancer Patients. J Natl Cancer Inst. 2012;104(6):452–460.
24. Zanger UM, Fischer J, Raimundo S, et al. Comprehensive analysis of the genetic factors determining expression and function of hepatic CYP2D6. Pharmacogenetics. 2001;11(7):573–585.
25. Jordan VC, Obiorah I, Fan P, et al. The St. Gallen Prize Lecture 2011: evolution of long-term adjuvant anti-hormone therapy: consequences and opportunities. Breast. 2011;20 Suppl 3:S1–11.
26. Jordan VC, Fritz NF, Tormey DC. Endocrine effects of adjuvant chemo-therapy and long-term tamoxifen administration on node-positive patients with breast cancer. Cancer Res. 1987;47(2):624–630.
27. Ravdin PM, Fritz NF, Tormey DC, et al. Endocrine status of premenopau-sal node-positive breast cancer patients following adjuvant chemotherapy and long-term tamoxifen. Cancer Res. 1988;48(4):1026–1029.
28. Murdter TE, Schroth W, Bacchus-Gerybadze L, et al. Activity levels of tamoxifen metabolites at the estrogen receptor and the impact of genetic polymorphisms of phase I and II enzymes on their concentration levels in plasma. Clin Pharmacol Ther. 2011;89(5):708–717.
29. Balaburski GM, Dardes RC, Johnson M, et al. Raloxifene-stimulated experimental breast cancer with the paradoxical actions of estrogen to pro-mote or prevent tumor growth: a unifying concept in anti-hormone resist-ance. Int J Oncol. 2010;37(2):387–398.
30. Maximov P, Sengupta S, Lewis-Wambi JS, et al. The Conformation of the Estrogen Receptor Directs Estrogen-Induced Apoptosis in Breast Cancer: A Hypothesis. Horm Mol Biol Clin Investig. 2011;5(1):27–34.
31. Sweeney EE, McDaniel RE, Maximov PY, et al. Models and Mechanisms of Acquired Antihormone Resistance in Breast Cancer: Significant Clinical Progress Despite Limitations. Horm Mol Biol Clin Investig. 2012;9(2):143–163.
32. Sengupta S, Sharma CG, Jordan VC. Estrogen regulation of X-box bind-ing protein-1 and its role in estrogen induced growth of breast and endo-metrial cancer cells. Horm Mol Biol Clin Investig. 2010;2(2):235–243.
33. Berman HM, Westbrook J, Feng Z, et al. The Protein Data Bank. Nucleic Acids Res. 2000;28(1):235–242.
34. Shiau AK, Barstad D, Loria PM, et al. The structural basis of estrogen receptor/coactivator recognition and the antagonism of this interaction by tamoxifen. Cell. 1998;95(7):927–937.
35. Friesner RA, Banks JL, Murphy RB, et al. Glide: a new approach for rapid, accurate docking and scoring. 1. Method and assessment of docking accu-racy. J Med Chem. 2004;47(7):1739–1749.
36. Halgren TA, Murphy RB, Friesner RA, et al. Glide: a new approach for rapid, accurate docking and scoring. 2. Enrichment factors in database screening. J Med Chem. 2004;47(7):1750–1759.
37. Cauley JA, Gutai JP, Kuller LH, et al. The epidemiology of serum sex hor-mones in postmenopausal women. Am J Epidemiol. 1989;129(6):1120–1131.
38. Hankinson SE, Willett WC, Manson JE, et al. Plasma sex steroid hormone levels and risk of breast cancer in postmenopausal women. J Natl Cancer Inst. 1998;90(17):1292–1299.
39. Cummings SR, Duong T, Kenyon E, et al. Serum estradiol level and risk of breast cancer during treatment with raloxifene. JAMA. 2002;287(2):216–220.
40. Rae JM, Johnson MD, Scheys JO, et al. GREB 1 is a critical regulator of hormone dependent breast cancer growth. Breast Cancer Res Treat. 2005;92(2):141–149.
41. Maximov PY, McDaniel RE, Fernandes DJ, et al. Simulation with cells in vitro of tamoxifen treatment in premenopausal breast cancer patients with different CYP2D6 genotypes. Br J Pharmacol. 2014; In press.
42. Lonard DM, Nawaz Z, Smith CL, et al. The 26S proteasome is required for estrogen receptor-alpha and coactivator turnover and for efficient estrogen receptor-alpha transactivation. Mol Cell. 2000;5(6):939–948.
43. Wijayaratne AL, McDonnell DP. The human estrogen receptor-alpha is a ubiquitinated protein whose stability is affected differentially by ago-nists, antagonists, and selective estrogen receptor modulators. J Biol Chem. 2001;276(38):35684–35692.
44. Wu X, Hawse JR, Subramaniam M, et al. The tamoxifen metabolite, endoxifen, is a potent antiestrogen that targets estrogen receptor alpha for degradation in breast cancer cells. Cancer Res. 2009;69(5):1722–1727.
45. Johnson MD, Zuo H, Lee KH, et al. Pharmacological characterization of 4-hydroxy-N-desmethyl tamoxifen, a novel active metabolite of tamoxifen. Breast Cancer Res Treat. 2004;85(2):151–159.
46. Levenson AS, Jordan VC. The key to the antiestrogenic mechanism of raloxifene is amino acid 351 (aspartate) in the estrogen receptor. Cancer Res. 1998;58(9):1872–1875.
47. Lewis-Wambi JS, Kim H, Curpan R, et al. The selective estrogen receptor modulator bazedoxifene inhibits hormone-independent breast cancer cell growth and down-regulates estrogen receptor alpha and cyclin D1. Mol Pharmacol. 2011;80(4):610–620.
48. Pike AC, Brzozowski AM, Walton J, et al. Structural insights into the mode of action of a pure antiestrogen. Structure. 2001;9(2):145–153.
49. Wu X, Subramaniam M, Grygo SB, et al. Estrogen receptor-beta sensitizes breast cancer cells to the anti-estrogenic actions of endoxifen. Breast Cancer Res. 2011;13(2):R27.
50. Roger P, Sahla ME, Makela S, et al. Decreased expression of estrogen receptor beta protein in proliferative preinvasive mammary tumors. Cancer Res. 2001;61(6):2537–2541.
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from

Vol. 106, Issue 10 | dju283 | October 8, 201410 of 10 Article | JNCI
51. Iwao K, Miyoshi Y, Egawa C, et al. Quantitative analysis of estrogen recep-tor-alpha and -beta messenger RNA expression in breast carcinoma by real-time polymerase chain reaction. Cancer. 2000;89:1732–1738.
52. Shaaban AM, O’Neill PA, Davies MP, et al. Declining estrogen receptor-beta expression defines malignant progression of human breast neoplasia. Am J Surg Pathol. 2003;27:1502–1512.
53. Horwitz KB, Koseki Y, McGuire WL. Estrogen control of progester-one receptor in human breast cancer: role of estradiol and antiestrogen. Endocrinology. 1978;103:1742–1751.
54. May FE, Johnson MD, Wiseman LR, et al. Regulation of progesterone receptor mRNA by oestradiol and antioestrogens in breast cancer cell lines. J Steroid Biochem. 1989;33:1035–1041.
55. Hawse JR, Subramaniam M, Cicek M, et al. Endoxifen’s molecular mech-anisms of action are concentration dependent and different than that of other anti-estrogens. PLoS One. 2013;8:e54613.
56. Jordan VC. Biochemical pharmacology of antiestrogen action. Pharmacol Rev. 1984;36:245–276.
57. Fan P, Agboke FA, McDaniel RE, et al. Inhibition of c-Src blocks oes-trogen-induced apoptosis and restores oestrogen-stimulated growth in long-term oestrogen-deprived breast cancer cells. Eur J Cancer. 2014;50:457–468.
58. Yao K, Lee ES, Bentrem DJ, et al. Antitumor action of physiological estra-diol on tamoxifen-stimulated breast tumors grown in athymic mice. Clin Cancer Res. 2000;6:2028–2036.
59. Jordan VC. Linking estrogen-induced apoptosis with decreases in mor-tality following long-term adjuvant tamoxifen therapy. J Natl Cancer Inst. 2014; In press.
60. Brauch H, Schwab M. Prediction of tamoxifen outcome by genetic varia-tion of CYP2D6 in post-menopausal women with early breast cancer. Br J Clin Pharmacol. 2014;77:695–703.
FundingThis work was supported by the Department of Defense Breast Program (award number W81XWH-06-1-0590) Center of Excellence, the Susan G. Komen for the Cure Foundation (award number SAC100009), and the Lombardi Comprehensive Cancer Center Support Grant (core grant NIH P30 CA051008). The views and opinions of the authors do not reflect those of the US Army or the Department of Defense.
Affiliations of authors: Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC (PYM, REM, DJF, PB, VRK, CJ); Institute of Chemistry, Romanian Academy, Timisoara, Romania (RFC).
at Universitaetsbibliothek G
iessen on June 23, 2015http://jnci.oxfordjournals.org/
Dow
nloaded from











![Introduction aux études médico-économiques · 2016. 5. 25. · Source : Health Technology Assessment 2007 Mitmann JNCI 2009 26 Étude Ligne Traitement AVG QALY’s RCE [avg] RCE](https://img.pdfslide.us/doc/110x75/6149c35712c9616cbc68f91d/introduction-aux-tudes-mdico-conomiques-2016-5-25-source-health-technology.jpg)











![Welcome! [] · the niersity o Kentucy author o Black Faces, White Spaces: Reimagining the Relationship of African Americans to the Great Outdoors will resent the - tegner Lecture](https://img.pdfslide.us/doc/110x75/5ec50e11aaeead42803a37c8/welcome-the-niersity-o-kentucy-author-o-black-faces-white-spaces-reimagining.jpg)




