Embed Size (px)
Citation preview

European Journal of Pharmacology 613 (2009) 39–45
Contents lists available at ScienceDirect
European Journal of Pharmacology
j ourna l homepage: www.e lsev ie r.com/ locate /e jphar
Neuropharmacology and Analgesia
Pharmacological modulation of movement-evoked pain in a rat modelof osteoarthritis
Prasant Chandran a,⁎, Madhavi Pai a, Eric A. Blomme b, Gin C. Hsieh a, Michael W. Decker a, Prisca Honore a
a Neuroscience Research, Global Pharmaceutical Research and Development, Abbott Laboratories, Dept. R4N5, Bldg. AP9A-LL, 100 Abbott Park Road, Abbott Park, Illinois 60064-6115, USAb Advanced Technology, Global Pharmaceutical Research and Development, Abbott Laboratories, Abbott Park, Illinois 60064, USA
⁎ Corresponding author. Tel.: +1 847 936 3537; fax: +E-mail address: [email protected] (P. Ch
0014-2999/$ – see front matter © 2009 Elsevier B.V. Adoi:10.1016/j.ejphar.2009.04.009
a b s t r a c t
a r t i c l e i n f oArticle history:Received 25 November 2008Received in revised form 23 March 2009Accepted 7 April 2009Available online 16 April 2009
Keywords:Animal modelOsteoarthritisPain
This study was conducted to characterize movement-induced pain in a rat model of knee joint osteoarthritisand validate this behavioral assessment by evaluating the effects of clinically used analgesic compounds.Unilateral intra-articular administration of a chondrocyte glycolytic inhibitor monoiodoacetate, was used toinduce knee joint osteoarthritis in Sprague–Dawley rats. In this osteoarthritis model, histologically erosivedisintegration of the articular surfaces of the ipsilateral joint are observed which closely mimic the clinicalpicture of osteoarthritis. Movement-induced pain behavior was measured using hind limb compressive gripforce evaluation. The animals exhibited pain behaviors epitomized by a long-lasting decrement in bilateralcompressive hind limb grip force following unilateral knee injury. The effects of clinically used referenceanalgesics were evaluated 20 days following i.a. injection of monoiodoacetate. Full analgesic activity wasobserved for tramadol, celecoxib and diclofenac; moderate effects for indomethacin, duloxetine andgabapentin but weak or no effects for acetaminophen, ibuprofen and lamotrigine. As morphine reduced gripforce in naïve rats, its analgesic effects could not be accurately evaluated in this model. Finally, the effects ofcelecoxib were maintained following chronic dosing. The results indicate that this in vivo model utilizing amovement-induced pain behavior spawned by knee joint osteoarthritis may provide a valuable tool inexamining the role of potential analgesic targets in osteoarthritic pain. As the model is clinically relevant, itwill further enhance the mechanistic understanding of chronic arthritic joint pain and help in developingnewer and better therapeutic strategies to manage osteoarthritis pain.
© 2009 Elsevier B.V. All rights reserved.
1. Introduction
Osteoarthritis is by far the most common type of degenerativearthritis and afflicts millions of people worldwide including anestimated 20 million people in the US (Lawrence et al., 1998). Painworsened by weight bearing activity is one of the cardinal symptomsof osteoarthritis and is the leading cause of disability and quality of lifeimpairment due to functional limitations (O'Reilly et al., 1998;American College of Rheumatology Subcommittee on OsteoarthritisGuidelines, 2000). In the US, the percentage of people withosteoarthritis-induced functional limitation is projected to increasefrom 2.8 in 1990 to 3.6% of the population in 2020 (Yasmin et al.,2000). Therefore, pain management is a challenging but criticalcornerstone for the pharmacotherapy of osteoarthritis, which in effectfacilitates maintaining or improving joint mobility and minimizingfunctional impairment.
Relief from chronic joint pain secondary to osteoarthritis is oftenrefractory to currently available pharmacological interventionsincluding non-steroidal anti-inflammatory drugs and opioid formula-
1 847 938 0072.andran).
ll rights reserved.
tions, posing a challenge for the clinicians (Kidd, 2006). Osteoarthritispain is complex as its etiology is often from multiple sources and canbe either inflammatory or non-inflammatory in origin (Pinals, 1996).Clinically, the patients afflicted with osteoarthritis describe their jointpain as being a deep and dull ache that is exacerbated with motion oractivity. Movement-induced pain is a characteristic early symptomhowever, with the progression of the disease, a continuous achingpain or pain at rest is the main clinical presentation (Sinkov andCymet, 2003). Recent clinical studies have reported a difference inpharmacological profile for relief of pain at rest versus movement-induced pain in osteoarthritic patients (Petrella et al., 2002). There-fore, a thorough understanding of the mechanisms of actions ofcurrently used analgesics and their utility in treating the differentqualities of pain is vital.
Evaluation of hind limb compressive grip force in animal models ofosteoarthritis may reproduce clinically observed symptoms of move-ment-induced pain in osteoarthritis patients. There have been reportsof several animal models of osteoarthritis evaluating the pathogenesisand potential therapeutic modulation of the disease (Bendele, 2001).Intra-articular administration (i.a.) of sodium monoiodoacetate inrodents causes a disruption of the articular cartilage by inhibitingchondrocyte metabolism (Guingamp et al., 1997; van der Kraan et al.,

40 P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
1992). The progressive joint degeneration and functional impairmentfollowing monoiodoacetate injection mimics clinical signs andsymptoms of osteoarthritis (van der Kraan et al., 1992; Clarke et al.,1997; Guingamp et al., 1997). However, the emphasis for the study ofpain in this rodent osteoarthritis model has been a recent phenom-enon with all the reports in the literature assessing hind limb weightbearing as an index for resting pain behavior (Schött et al., 1994; Boveet al., 2003; Kobayashi et al., 2003; Fernihough et al., 2004; Pomoniset al., 2005; Vermeirsch et al., 2007).
The purpose of this study is to pharmacologically characterize anovel compressive grip force movement-induced pain behavior inosteoarthritic rats and validate this model using clinically availableanalgesics.
2. Materials and methods
2.1. Animals
All experiments have been approved by the Institutional AnimalCare and Use Committee at Abbott Laboratories and are in strictaccordance with the ethical guidelines laid down by the InternationalAssociation for the Study of Pain (Zimmermann,1983) for the care anduse of laboratory animals. Male Sprague–Dawley rats (Charles RiverLabs, Portage, MI) group housed (5 per cage) and with free access tofood and water, were used for the study (150–175 g at the start of theexperiment). The animals were housed in temperature and humiditycontrolled animal rooms and on a 12 h light/dark cycle in anAssociation for Assessment and Accreditation of Laboratory AnimalCare International accredited facility.
2.2. Induction of knee joint osteoarthritis
Unilateral knee joint osteoarthritis was induced in the rats by asingle intra-articular (i.a.) injection of Sodium monoiodoacetate(Sigma-Aldrich, St. Louis, MO) (3 mg in 0.05 ml sterile isotonic saline)into the joint cavity under light (1–3%) isoflurane (Hospira, LakeForest, IL) anesthesia using a 26 gauge needle (Pomonis et al., 2005).Following injection, the animals were allowed to recover from theeffects of anesthesia (usually 5–10 min) before returning to theirhome cages. To maintain uniformity across the study, the right kneejoint of each animal was injected with monoiodoacetate. Hind limbgrip force assessment was carried out 20 days following monoiodoa-cetate injection as discussed below. The dose of the monoiodoacetate(3 mg/i.a. injection) was selected based on results obtained frompreliminary studies (Chandran et al., 2004; Pomonis et al., 2005).
2.3. Pain behavior assessment: grip force
Assessment of bilateral hind limb compressive grip force followingunilateral injection of monoiodoacetate was used as a behavioralmeasure of movement evoked pain in adult osteoarthritic rats (bodyweight 20 days following monoiodoacetate injection: 325–350 g).Measurements of peak bilateral hind limb grip force were conductedby recording the maximum compressive force exerted on the hindlimb strain gauge setup, in a commercially available grip forcemeasurement system (Columbus Instruments, Columbus, OH). Duringtesting, each rat was gently restrained and allowed to grasp the wiremesh frame (10×12 cm2) attached to the strain gauge, with their hindlimbs. The rats were restrained in such a way that their forelimbs didnot touch the strain gauge. The experimenter then moved the animalin a rostral-to-caudal direction until the grip was broken. Each rat wassequentially tested twice at approximately 2–3 min interval to obtaina bilateral rawmean grip force (CFmax) for the hind limbs. For the timecourse experiment, the assessment of hind limb grip force wasconducted for 20 days following the i.a. injection of monoiodoacetate/saline (control)/non-injected (age-matched naïve rats) groups. Base-
line measurements were acquired a day prior to the injections ofmonoiodoacetate/saline. Additional tests were performed 4, 7, 11, 15and 20 days following the injections. A group mean±SEM for CFmax
was calculated at each time point for the 6 animals in themonoiodoacetate, saline injected and the naïve (non-injected) groups,respectively.
For evaluating the effects of reference analgesic drugs, theevaluation of hind limb grip force was conducted 20 days followingthe i.a. injection of monoiodoacetate. Since other studies havedemonstrated the presence of the joint destruction consistent withclinical osteoarthritis by day 20 following monoiodoacetate injection,we selected this time point for conducting the pharmacologicalstudies (Chandran et al., 2004; Pomonis et al., 2005). A group of agematched naïve animals were added to each experiment and the dataobtained from the different dose groups for the compound beingtested were compared to the naïve group. The vehicle control groupfor each compound being tested was assigned 0% whereas the naïvegroup was assigned as being 100% (normal). The % effects for eachdose-group was then expressed as % return to normalcy compared tothe naïve group (=[100÷% increase from vehicle for naive group]×% increase from vehicle for treatment group); (% increase fromvehicle=[Treatment CFmax−Vehicle CFmax)/Vehicle CFmax]×100. Allexperiments evaluating drug effects in this model were conducted in arandomized blinded fashion.
2.4. Drugs, vehicles, and dosing
Morphine sulfate pentahydrate, acetaminophen, ibuprofen, diclo-fenac, indomethacin, haloperidol, dimethyl sulfoxide, hydroxypropyl-β-cyclodextrin, and polyethylene glycol-400 were acquired fromSigma-Aldrich (St Louis, MO). Celecoxib was purchased from TorontoResearch Chemicals, Inc. (Toronto, ON, Canada). Tramadol, lamotrigineand gabapentinwere synthesized in-house at Abbott Laboratories. Thedoses, route of administration, vehicles and the injection volumes forthe different compounds were as follows: morphine (1, 3, 8 and13 μmol/kg, s.c.) dissolved in 0.9% sterile saline (Abbott Laboratories,IL) (1 ml/kg); tramadol (10, 30 and 100 μmol/kg, i.p.) (2 ml/kg) andcelecoxib (10, 30 and 100 μmol/kg, p.o.) (2 ml/kg) in 100%polyethylene glycol-400; ibuprofen (30, 100 and 300 μmol/kg, p.o.)and diclofenac (10, 30 and 100 μmol/kg, p.o.) were dissolved inpolyethylene glycol-400/sterile water (30:70 v/v) (5 ml/kg); acet-aminophen (30, 100 and 300 μmol/kg, p.o.) suspended in 0.5% methylcellulose (Eastman Kodak Co., Rochester, NY) (2 ml/kg); lamotrigine(10, 30 and 100 μmol/kg, p.o.) (2 ml/kg) and haloperidol (1, 3 and10 μmol/kg, i.p.) were dissolved in dimethyl sulfoxide /polyethyleneglycol-400 (5:95 v/v); gabapentin (100, 250 and 500 μmol/kg, p.o.)and duloxetine (30, 90 and 150 μmol/kg, p.o.) were dissolved in sterilewater (2 ml/kg); indomethacin (10, 30 and 100 μmol/kg, p.o.)was dissolved in 100% polyethylene glycol-400 (2 ml/kg). Thoseanimals receiving oral dosageof the respective compoundswere fastedovernight. The assessment of grip force was carried out 20, 30or 60 min following the administration of the compounds either bys.c., i.p., or p.o. routes respectively, 20 days following the i.a. injectionof monoiodoacetate. The analgesic effects following the administra-tion of duloxetine were assessed 180 min following p.o. dosing. Forthe chronic dosing study, two doses of celecoxib (10 and 30 μmol/kg)(2 ml/kg in 100% polyethylene glycol-400) was administered orallytwice daily starting 7 days following the induction of osteoarthritis bymonoiodoacetate. The rats were tested 1 h following the morningdosing on the 12th day following chronic dosing (20 days followinginduction of osteoarthritis). The doses for all the compounds wereselected based on their efficacy data in several pain models andmodels of catalepsy (haloperidol) used in-house and from theliterature (Nakamura-Craig and Follenfant, 1994; Dirig et al., 1998;Chandran et al., 2004; Combe et al., 2004; Fernihough et al., 2004;Jones et al., 2005; Pomonis et al., 2005).

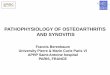
Fig. 1. Time course of changes in hind limb grip force in monoiodoacetate and salineinjected rats (mean±SEM; n=6). Data expressed as hind limb compressive force(CFmax) (gram force) for each animal. Long lasting compressive force-induced painbehavior is observed in the rats injected with monoiodoacetate. (F (21,131)=14.56,Pb0.0001) ⁎Pb0.05, ⁎⁎Pb0.01, versus saline injected rats, +Pb0.05, ++Pb0.01 versusuntreated naïve rats.
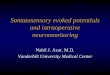
Fig. 2. (A) Effects of morphine (s.c.) and tramadol (i.p.) on grip force in rats 20 daysfollowing injection of monoiodoacetate. Tramadol was efficacious in reversing thereduced grip force in osteoarthritic rats. Morphine was weakly active in osteoarthriticrats in reversing the decreased grip force. Data represented as % effects for grip force (g)(mean±SEM; n=12/dose group). ⁎Pb0.05, ⁎⁎Pb0.01 versus vehicle treated rats.(B) Effects of morphine (s.c.) and haloperidol (i.p.) on grip force in naïve rats. Bothmorphine and haloperidol reduced grip force in naïve (no monoiodoacetate-inducedosteoarthritis) rats. Data represented as % reduction of grip force (g) (mean±SEM;n=12/dose group). +Pb0.05, ++Pb0.01 versus untreated naïve rats.
41P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
2.5. Data analysis
The statistical analysis was carried out using GraphPad Prism(version 4.03; GraphPad Software, Inc., San Diego, CA) and JMP(version 5.0.1a; SAS Institute, Inc., Cary, NC). The analyses for the timecourse effects on hind limb grip force following injection ofmonoiodoacetate versus saline controls and the % return to normalcyfollowing administration of the different analgesic compounds wereconducted using repeated measures analysis of variance. Fisher'sProtected Least Significant Difference analysis was performed as apost hoc comparison. The values were represented as mean±SEM. Inall cases Pb0.05 was assumed as the level for statistical significance.ED50 values (Effective Dose, 50%) (GraphPad Prism) were alsocalculated by linear regression analysis and reported with the 95%confidence interval (CI95%).
3. Results
3.1. Time course of pain behavior assessment
Intra-articular administration of either monoiodoacetate or salinehad no effect on the general health of the animals. The animals in boththe saline and monoiodoacetate injected groups gained body weightnormally and there was no statistically significant difference in bodyweight gain between the two groups.
The rats following i.a. administration ofmonoiodoacetate exhibitedlong lasting compressive grip force movement-induced pain behaviorthroughout the 20-day study period (Fig. 1). When compared to thesaline injected and the non-injected (naïve) group, the monoiodoa-cetate injected group exhibited a significant decrement in hind limbgrip force (F (19, 95)=124, Pb0.0001). In the monoiodoacetateinjected group, grip force decreases from 357.50±11.38 g beforeunilateral monoiodoacetate injection to 121.25±8.18 g at 20 daysfollowing injection. When compared to the saline injected group, themonoiodoacetate-injected group exhibited a significant decrement ingrip force (Pb0.01 for treatment, time and time⁎ treatment) onall testing days. The baseline grip force values for the saline injectedand naive groups were 337.50±13.02 g and 334.17±14.63 g respec-tively; on day 20 the respective grip force valueswere 425.83±12.24 gand 407.92±7.89 g. In the saline-injected and the naive groupsno difference in grip force was observed on days 4 and 7. However,on days 11,15 and 20, the grip force values observed for both the salineand naïve groups were significantly higher than the corresponding
baseline values (Pb0.05). This observation of increased grip forcevalues for the naïve and control (saline injected) rats is due tothe increasing raw mean grip force values (CFmax) as the rats growstronger with gains in body weight. The naïve rats' and saline controlgroup's day 20 values for the rawmean grip force (CFmax) increased to407.92±7.92 g and 425.83±12.24 g respectively. Post hoc analysisrevealed a significant effect formonoiodoacetate-injected groupwhencompared to the saline control and naïve groups from days 4–20(Pb0.01).
3.2. Pharmacological modulation of the compressive force-induced painbehavior
The analgesic effects of morphine, tramadol, celecoxib, diclofenac,indomethacin, acetaminophen, ibuprofen, gabapentin, duloxetine,and lamotrigine were determined on compressive force-inducedpain behavior as evaluated by grip force assessment, observed20 days following the i.a. injection of monoiodoacetate. In order toensure that the doses of the compounds used above were notimpairing grip force assessment on their own, pilot studies wereconducted wherein the highest doses of each drug used in doseresponse studies were administered in naïve rats and evaluated if theyreduced grip force (data not shown). None of the compounds (butmorphine) had any significant effects on grip force readouts in naïverats.

Fig. 4. Effects of gabapentin (p.o.) and lamotrigine (p.o.) on grip force in rats 20 daysfollowing injection of monoiodoacetate. Gabapentin demonstrated efficacy whilelamotrigine had weak effects on reversing the reduced grip force in osteoarthritic rats.Data represented as % effects for grip force (g) (mean±SEM; n=12/dose group).⁎Pb0.05, ⁎⁎Pb0.01 versus vehicle treated rats for lamotrigine; +Pb0.05, ++Pb0.01versus vehicle treated rats for gabapentin, #Pb0.05, ##Pb0.01 versus vehicle treated ratsfor duloxetine.
42 P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
3.2.1. OpioidsMorphine produced weak effects in monoiodoacetate-injected rats
(36±3% effect at 8 μmol/kg). Vehicle CFmax for morphine was 95.83±4.29 g (Fig. 2A). On the otherhand, 8 μmol/kg (6mg/kg) and13 μmol/kg(10 mg/kg) of morphine reduced grip force in naïve rats (non-monoiodoacetate injected rats) by 3±5% and 52±3% % respectivelycompared to age-matched naïve untreated rats (CFmax=351.25±9.18 g)(Fig. 2B). To further understand the weak effects of morphine in thismodel, we evaluated the effects of haloperidol when administered innaïve rats. In naïve rats, haloperidol (8±6, 44±9 & 71±2% for the 1, 3and 10 μmol/kg doses respectively) reduced hind limb grip force whencompared to the corresponding untreated age-matched group of rats(CFmax=319.92±28.30 g) (Fig. 2B) (⁎⁎Pb0.01 dose groups versusvehicle). Tramadol demonstrated dose-dependent reversal of thedecreased grip force (ED50=40 μmol/kg, CI95%=32–54 μmol/kg with79±5%effect at 100 μmol/kg) (Fig. 2A) inmonoiodoacetate injected rats.Vehicle CFmax for tramadol was 93.75±7.89 g (⁎⁎Pb0.01 dose groupsversus vehicle).
3.2.2. Non-steroidal anti-inflammatory drugs and acetaminophenAmong the non-steroidal anti-inflammatory drugs, celecoxib
(ED50=27 μmol/kg, CI95%=16–42 μmol/kg with 91±5% effect at
Fig. 3. (A) Effects of acetaminophen (p.o.) and non-steroidal anti-inflammatory drugs:diclofenac (p.o.), ibuprofen (p.o.), celecoxib (p.o.) and indomethacin (p.o.) on grip forcein rats 20 days following injection of monoiodoacetate. Celecoxib and diclofenacdemonstrated good efficacy in reversing compressive force-induced pain behavior inosteoarthritic rats. Partial efficacy observed with indomethacin. ⁎Pb0.05, ⁎⁎Pb0.01versus vehicle treated rats for celecoxib; +Pb0.05, ++Pb0.01 versus vehicle treated ratsfor diclofenac, #Pb0.05, ##Pb0.01 versus vehicle treated rats for indomethacin.(B) Chronic dosing of celecoxib (3, 10, 30 and 100 μmol/kg p.o., twice daily) for12 days beginning 7 days after monoiodoacetate injection produced similar efficacy assimilar acute dose groups (10, 30 and 100 μmol/kg p.o.) (administered on day 20)improving the reduced grip force. Data represented as % effects for grip force (g) (mean±SEM; n=12/dose group). ⁎Pb0.05, ⁎⁎Pb0.01 versus vehicle treated rats for acutecelecoxib dose groups; +Pb0.05, ++Pb0.01 versus vehicle treated rats for chroniccelecoxib dose groups (B).
100 μmol/kg) and diclofenac (ED50=29 μmol/kg, CI95%=22–38 μmol/kg with 74±3% effect at 100 μmol/kg) fully reversed thedecreased grip force, whereas weaker effects were observed foribuprofen (31±8% effect at 300 μmol/kg) and indomethacin (41±5%effect at 85 μmol/kg) (Fig. 3A). Vehicle CFmax for diclofenac, ibuprofen,indomethacin and celecoxib were 107.92±12.85 g, 126.67±19.42 g,146.25±9.71 g and 112.14±5.43 g respectively (⁎⁎Pb0.01 dosegroups versus vehicle). Orally administered acetaminophen exhibitedno effects (28±10% effect at 300 μmol/kg) (Fig. 3A).
Following chronic oral dosing (twice daily) of the 3, 10, 30 and100 μmol/kg doses of celecoxib for 7 days, the analgesic efficacy ismaintained (0.13±4%, 22±13%, 48.58±1% and 80±4% effects respec-tively) with statistical significance at the 10, 30 and 100 μmol/kg doses(++Pb0.01 vs. vehicle). Corresponding acutely dosed 10, 30 and100 μmol/kg doses produced 9±3%, 47±3% and 97±4% analgesiceffects respectively) (statistical significance at the 30 and 100 μmol/kgdoses, ⁎⁎Pb0.01 versus vehicle). Vehicle CFmax for this study was130.83±17.72 g (Fig. 3B).
3.2.3. Anti-neuropathic pain drugsGabapentin decreased grip force-induced painwith 47±5% effect at
500 μmol/kg. Duloxetine was also moderately efficacious in reversingthe osteoarthritis-induced reduction in grip force (50±4% effect at150 μmol/kg). Lamotrigine had weak effects (32±4% effect at100 μmol/kg) (Fig. 4). Vehicle CFmax for gabapentin, duloxetine andlamotriginewere 185.23±5.95 g,153.96±20.23 g and 104.58±13.33 grespectively (⁎⁎Pb0.01 dose groups versus vehicle) (Fig. 4).
4. Discussion
Assessment of pain associated with osteoarthritis in animals is achallenging task. Intra-articular (i.a.) injection of monosodiumiodoacetate, a cellular glycolytic inhibitor has been used to induceosteoarthritis-like changes in the articular cartilage of rodents toexamine the pathophysiology of the disease (Kalbhen, 1987; Guin-gamp et al., 1997; van der Kraan et al., 1992). A lesioning of thearticular cartilage is observed and there is a marked depletion ofproteoglycans as indicated by the loss of safranin O staining(Gustafson et al., 1992; van der Kraan et al., 1992). Pain being one ofthe cardinal symptoms of osteoarthritis, recent studies in osteoar-thritic rats have focused on analyzing hind limb weight bearingdistribution as an index for resting or static pain behavior as the ratsare immobilized during the measurement (Bove et al., 2003;Kobayashi et al., 2003; Pomonis et al., 2005). In the present study

43P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
using intra-articular injection of monoiodoacetate to induce osteoar-thritis in rats, one of the chief symptoms of osteoarthritic pain,dynamic pain or movement-elicited pain, determined by compressivegrip force assessment was characterized throughout a 20-dayobservation period. The efficacy and potency of clinically-usedanalgesics in ameliorating this pain behavior were also evaluated.
Patients with osteoarthritis have pain that typically worsens withactivity but improves with rest. If the patient experiences continuouspain at rest, this signifies an increase in disease severity. Thus,movement-induced pain is clinically relevant to the early stageosteoarthritis and measuring this dynamic endpoint, instead of painat rest, could be a better early predictor of pharmacological efficacy inpreclinical animal models. Recently it has been demonstrated thatthese pain behaviors observed in osteoarthritis patients responddifferently to pharmacological interventions. Resting pain respondedequally well to both oral non-steroidal anti-inflammatory drugs andintra-articular sodium hyaluronate. However, pain following physicalactivity responded well to intra-articular sodium hyaluronate and thisimproved with time compared with the effects of non-steroidal anti-inflammatory drugs, which do not show improvement over the courseof treatment (Petrella et al., 2002). Thus it is imperative to look atpreclinical models of osteoarthritis that incorporate the differentaspects of pain and then evaluate the effects of different treatments.
Our results demonstrate that movement-evoked joint pain (illu-strated by decrease in grip force measurement) secondary to thedevelopment of osteoarthritis can be reproducibly quantified in rats.The histological picture was archetypical of osteoarthritis-likechanges characterized by a disruption of the articular cartilageintegrity (Guzman et al., 2003; Fernihough et al., 2004). Grip strengthassessment in rodents has been developed and used in the literatureas part of the functional observation battery in toxicological studies toassess the integrity of the neuromuscular system (Meyer et al., 1979;Tilson, 1990). Only recently has this technique been used to measurepain in rodent models of bone cancer and muscle pain (Kehl et al.,2000; Wacnik et al., 2003). Our study is among the first to use a gripforce assessment system to evaluate movement-evoked pain in ananimal model of osteoarthritic pain and to demonstrate a long lastingmovement-induced pain behavior following unilateral monoiodoace-tate injection. While establishing this model in rodents, the assess-ment of tensile grip force of the fore and hind limbs in rats followingthe induction of osteoarthritis was also evaluated. However, theresults for tensile grip force were not as consistent as the compressivegrip force in hind limbs of rats with osteoarthritis.
In order to further validate this behavioral endpoint, we evaluatedthe effects of several clinically used analgesics. Morphine only hadweak effects (tested up to 8 μmol/kg or 6 mg/kg dose) in this model,contrasting with recent data demonstrating full efficacy on weightbearing in monoiodoacetate-induced osteoarthritic pain model in rats(Pomonis et al., 2005). This lack of efficacy of morphine seems to be anartifact of the measure and illustrates the limitations of suchapproach. Morphine decreased grip force in naïve rats, these effectscounteracting its analgesic effects at reversing the monoiodoacetate-induced reduction in grip force (Fig. 2B). On the other hand, tramadolproduced a complete dose-dependent reversal of the reduced gripforce in osteoarthritic rats. Tramadol has recently been shown toproduce only mild reversal of the weight-bearing deficit in themonoiodoacetate-induced osteoarthritic pain model (Combe et al.,2004). Tramadol's effects in this model highlight the difference inpharmacology for pain at rest as measured by the weight-bearingassay versus movement-evoked pain as measured in the grip forceassay. We have further highlighted the limitation of this model byevaluating effects of haloperidol on grip force in naïve ratsdemonstrating a dose-dependent reduction in grip force. Thuscompounds producing significant sedative/hypomobility effects inaddition to muscle weakness cannot be accurately evaluated usingassessment of grip force. Clinically, µ-opioid agonists including
morphine alone or combined with a non-opioid are the treatment ofchoice for moderate to severe osteoarthritis pain (American PainSociety,1996). Tramadol, a centrally acting analgesic, has a low affinityto the µ-opioid receptor in addition to inhibiting norepinephrine andserotonin reuptake (Raffa et al., 1992). Clinicians are increasinglyusing tramadol to treatmoderate pain (Visual Analog Scale of 4–6 on a0–10 scale) (American Pain Society, 1996) and have demonstrated itsefficacy for the treatment of breakthrough flare pain in patients whowere on non-steroidal anti-inflammatory drug therapy. In the clinic,as observed in rodents in the present study, significant improvementswere noticed for pain on motion (Roth, 1998).
Acetaminophen and non-steroidal anti-inflammatory drugs forman important therapeutic option for the treatment of mild tomoderateosteoarthritis pain. Acetaminophen was ineffective while bothcelecoxib and diclofenac showed dose-dependent effects in alleviatingmovement-induced pain in osteoarthritic rats. Furthermore, theeffects of celecoxib were maintained following chronic dosing. Incontrast, Pomonis et al. (2005) showed that following acute oraladministration of celecoxib (100 μmol/kg or 30 mg/kg), no significanteffects were observed on the resting pain behavior in osteoarthriticrats. However, the same dose following chronic oral dosing (twice aday) produced significant efficacy in reversing osteoarthritis-inducedresting pain (Pomonis et al., 2005). These data demonstrate that forthe same pain model, different pharmacological effects can beobserved depending on the behavioral endpoint (movement-inducedversus resting pain) and the dosing regimen (acute versus chronicdosing). These results outline the importance of testing severalendpoints in the same chronic pain disease model and the usefulnessof testing the efficacy following repeated dosing. Ibuprofen wasineffective in reversing the pain behavior in this model. However,similar doses have been shown to be effective in reducing prosta-glandin synthesis and reducing inflammatory hyperalgesia (Diriget al., 1998). While immediately following monoiodoacetate injectionthere is an elevation in the levels of prostaglandins, a return to basallevels by day 7 post monoiodoacetate injection was observed(Pulichino et al., 2006). Histological assessment also demonstratesthe presence of inflammation early on following monoiodoacetateinjection and a subsequent resolution of the inflammation (Guzmanet al., 2003; Fernihough et al., 2004). This absence of inflammation atthe 20 day time pointmay explain the lack of efficacy of indomethacin,ibuprofen and acetaminophen in this model. However, the robustefficacy observed following dosing with celecoxib and diclofenac maybe speculated to be due to pharmacokinetic parameters pendingfurther investigation. Intriguingly, the various cyclooxygenase inhibi-tors show different profiles in the varied animal pain models. This isillustrated by Torres-Lopez et al. (2002) who have demonstrated theperipheral analgesic efficacy of selective cyclooxygenase-1 inhibitor(resveratrol) and the non-selective cyclooxygenase inhibitor (diclo-fenac) in the rat formalin model of inflammatory pain. In contrast, theselective cyclooxygenase-2 inhibitor (celecoxib) was not able toproduce antinociception. This data disagrees with results from otherinflammatory pain models, leading the authors to suggest thatperipheral cyclooxygenase-1 is a bigger player than peripheralcyclooxygenase-2 in formalin-induced inflammatory pain. This under-lines the important caveat to pre-clinical pain studies which may notalways be predictive of clinical pain conditions in terms of efficacy ofnon-steroidal anti-inflammatory drugs.
Gabapentin, an anticonvulsant drug used extensively to treatneuropathic pain (Backonja and Glanzman, 2003) producedmoderateanalgesic activity in this model. Although gabapentin is rarely usedclinically, preclinical studies have shown that tactile allodynia but notmechanical hyperalgesia 14 days following the induction of osteoar-thritis (2 mg MIA) was reversed by gabapentin (Fernihough et al.,2004). Reduction in weight bearing asymmetry is also observed 14–28 days following monoiodoacetate-induced (1 mg) osteoarthritis(Ivanavicius et al., 2007). Duloxetine, a serotonin-norepinephrine

44 P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
reuptake inhibitor used clinically to treat neuropathic pain is alsoefficacious in the treatment of acute and chronic inflammatory pain(Jones et al., 2005). In this current study evaluating duloxetine'seffects on osteoarthritis-induced chronic pain, moderate analgesiceffects were also observed. New clinical data from Eli Lilly and Co.suggests that patients with osteoarthritis pain of the knee treatedwith 60 mg and 120 mg duloxetine once daily reported significantpain relief (throughout the 13-week trial) when compared to placebo.These clinical study findings from 231 osteoarthritis patients werepresented at the Annual Congress of the European League AgainstRheumatism in Paris, France (June, 2008) (http://newsroom.lilly.com/ReleaseDetail.cfm?ReleaseID=316480). While current treat-ment regimen to control osteoarthritis-induced pain does not includethe use of drugs used to control neuropathic pain, these results couldsuggest their potential efficacy. The issue of concern is how much ofosteoarthritis pain is neuropathic in origin. It may be a relatively smallbut important contributor when compared to other mechanisms orsites of origin, for instance, inflammatory pain from the synovium andperi-articular structures and bone pain among others (Kidd, 2006). Arecent pre-clinical study has demonstrated an increased ActivatingTranscription Factor-3 immunoreactivity (neuronal injury marker) inthe L5 dorsal root ganglion between days 8 and 14 post mono-iodoacetate injection (1 mg) (Ivanavicius et al., 2007). We observedminimal effects with lamotrigine, another anti-epileptic drug that isclinically (off label) used to treat neuropathic pain (di Vadi andHamann, 1998). Pre-clinically, analgesic effects of orally administeredlamotrigine have been demonstrated in the acute model of prosta-glandin E2 and chronic diabetic neuropathy induced hyperalgesia(Nakamura-Craig and Follenfant, 1994).
The emphasis currently is on therapies directed toward treatingjoint pain, which is the main presenting symptom in osteoarthritis,without taking into account the physical functional status of thepatient. We have characterized a novel movement-induced painbehavior in an animal model of osteoarthritis where it is possible toexamine the impact of different pharmacological interventions on afunctional measure of osteoarthritis pain. Our results demonstrate apharmacological difference for movement-induced versus restingpain behavior, suggesting that the different stages of osteoarthritispain viz., movement-induced or pain at rest could require differentpain relief approaches. With the push to develop novel and effectivepharmacological agents to treat pain in osteoarthritis patients, it isimperative not to ignore pain at the different physiological states suchas at rest and that induced by physical activity and functionalperformance. This may ultimately affect the clinical performance ofthe drug in question. Thus, grip force measurement is a simplebehavioral assessment used in an osteoarthritis pain model providinga valuable preclinical tool in examining the role of novel analgesictargets.
Acknowledgements
The authors wish to thank Brenda Weaver and Dr. Robert S. Bitnerfor their assistance on the histological evaluation.
References
American College of Rheumatology Subcommittee on Osteoarthritis Guidelines, 2000.Recommendations for the medical management of osteoarthritis of the hip andknee. Arthritis Rheum. 43, 1905–1915.
American Pain Society, 1996. The Use of Opioids for the Treatment of Chronic Pain: AConsensus Statement from American Academy of PainMedicine and American PainSociety. From htttp://www.ampainsoc.org/advocacy/opioids.htm.
Backonja, M., Glanzman, R.L., 2003. Gabapentin dosing for neuropathic pain: evidencefrom randomized, placebo-controlled clinical trials. Clin. Ther. 25, 81–104.
Bendele, A.M., 2001. Animal models of osteoarthritis. J. Musculoskelet. NeuronalInteract. 1, 363–366.
Bove, S.E., Calcaterra, S.L., Brooker, R.M., Huber, C.M., Guzman, R.E., Juneau, P.L., Schrier,D.J., Kilgore, K.S., 2003. Weight bearing as a measure of disease progression and
efficacy of anti-inflammatory compounds in a model of monosodium iodoacetate-induced osteoarthritis. Osteoarthr. Cartil. 11, 821–830.
Chandran, P., Hsieh, G.C., Honore, M.P., 2004. Pharmacological characterization ofmonoiodoacetate-induced osteoarthritic pain in rats. Poster Presentation at the34th Annual Meeting of the Society for Neuroscience (SFN), San Diego, CA, October2004. Published in Abstract Form.
Clarke, K.A., Heitmeyer, S.A., Smith, A.G., Taiwo, Y.O., 1997. Gait analysis in a rat model ofosteoarthrosis. Physiol. Behav. 62, 951–954.
Combe, R., Bramwell, S., Field, M.J., 2004. The monosodium iodoacetate model ofosteoarthritis: a model of chronic nociceptive pain in rats? Neurosci. Lett. 370,236–240.
di Vadi, P.P., Hamann, W., 1998. The use of lamotrigine in neuropathic pain. Anaesthesia53, 804–809.
Dirig, D.M., Isakson, P.C., Yaksh, T.L., 1998. Effects of COX-1 and COX-2 inhibition oninduction and maintenance of carrageenan-evoked thermal hyperalgesia in rats.J. Pharmacol. Exp. Ther. 285, 1031–1038.
Fernihough, J., Gentry, C., Malcangio, M., Fox, A., Rediske, J., Pellas, T., Kidd, B., Bevan, S.,Winter, J., 2004. Pain related behaviour in two models of osteoarthritis in the ratknee. Pain 112, 83–93.
Guingamp, C., Gegout-Pottie, P., Philippe, L., Terlain, B., Netter, P., Gillet, P., 1997. Mono-iodoacetate-induced experimental osteoarthritis. A dose-response study of loss ofmobility, morphology, and biochemistry. Arthritis Rheum. 40, 1670–1679.
Gustafson, S.B., Trotter, G.W., Norrdin, R.W., Wrigley, R.H., Lamar, C., 1992. Evaluation ofintra-articularly administered sodium monoiodoacetate-induced chemical injuryto articular cartilage of horses. Am. J. Vet. Res. 53, 1193–1202.
Guzman, R.E., Evans, M.G., Bove, S., Morenko, B., Kilgore, K., 2003. Mono-iodoacetate-induced histologic changes in subchondral bone and articular cartilage of ratfemorotibial joints: an animal model of osteoarthritis. Toxicol. Pathol. 31, 619–624.
Ivanavicius, S.P., Ball, A.D., Heapy, C.G., Westwood, F.R., Murray, F., Read, S.J., 2007.Structural pathology in a rodent model of osteoarthritis is associated withneuropathic pain: Increased expression of ATF-3 and pharmacological character-ization. Pain 128, 272–282.
Jones, C.K., Peters, S.C., Shannon, H.E., 2005. Efficacy of duloxetine, a potent andbalanced serotonergic and noradrenergic reuptake inhibitor, in inflammatory andacute pain models in rodents. J. Pharmacol. Exp. Ther. 312, 726–732.
Kalbhen, D.A., 1987. Chemical model of osteoarthritis — a pharmacological evaluation.J. Rheumatol. 14, 130–131.
Kehl, L.J., Trempe, T.M., Hargreaves, K.M., 2000. A newmodel for assessing mechanismsand management of muscle hyperalgesia. Pain 85, 333–343.
Kidd, B.L., 2006. Osteoarthritis and joint pain. Pain 123, 6–9.Kobayashi, K., Imaizumi, R., Sumichika, H., Tanaka, H., Goda, M., Fukunari, A., Komatsu,
H., 2003. Sodium iodoacetate-induced experimental osteoarthritis and associatedpain model in rats. J. Vet. Med. Sci. 65, 1195–1199.
Lawrence, R.C., Helmick, C.G., Arnett, F.C., Deyo, R.A., Felson, D.T., Giannini, E.H., Heyse, S.P.,Hirsch, R., Hochberg,M.C.,Hunder, G.G., Liang,M.H., Pillemer, S.R., Steen,V.D.,Wolfe, F.,1998. Estimatesof theprevalenceof arthritis and selectedmusculoskeletal disorders inthe United States. Arthritis Rheum. 41, 778–779.
Meyer, O.A., Tilson, H.A., Byrd, W.C., Riley, M.T., 1979. A method for the routineassessment of fore- and hindlimb grip strength of rats and mice. Neurobehav.Toxicol. 1, 233–236.
Nakamura-Craig, M., Follenfant, R.L., 1994. Effect of lamotrigine in the acute and chronichyperalgesia induced by PGE2 and in the chronic hyperalgesia in rats withstreptozotocin-induced diabetes. Pain 63, 33–37.
O'Reilly, S.C., Muir, K.R., Doherty, M., 1998. Knee pain and disability in the Nottinghamcommunity: associated with poor health status and psychological distress.Br. J. Rheumatol. 37, 870–873.
Petrella, R.J., DiSilvestro, M.D., Hildebrand, C., 2002. Effects of hyaluronate sodium onpain and physical functioning in osteoarthritis of the knee. Arch. Intern. Med. 162,292–298.
Pinals, R.S., 1996. Mechanisms of joint destruction, pain and disability in osteoarthritis.Drugs 52, 14–20.
Pomonis, J.D., Boulet, J.M., Gottshall, S.L., Phillips, S., Sellers, R., Bunton, T., Walker, K.,2005. Development and pharmacological characterization of a rat model ofosteoarthritis pain. Pain 114, 339–346.
Pulichino, A.M., Rowland, S., Wu, T., Clark, P., Xu, D., Mathieu, M.C., Riendeau, D., Audoly,L.P., 2006. Prostacyclin antagonism reduces pain and inflammation in rodentmodelsof hyperalgesia and chronic arthritis. J. Pharmacol. Exp. Ther. 319, 1043–1050.
Raffa, R.B., Friderichs, E., Reimann, W., Shank, R.P., Codd, E.E., Vaught, J.L., 1992. Opioidand nonopioid components independently contribute to the mechanism of actionof tramadol, an “atypical” opioid analgesic. J. Pharmacol. Exp. Ther. 260, 275–285.
Roth, S.H., 1998. Efficacy and safety of tramadol HCl in breakthrough musculoskeletalpain attributed to osteoarthritis. J. Rheumatol. 25, 1358–1363.
Schött, E., Berge, O.-G., Ängeby-Möller, K., Hammarström, G., Dalsgaard, C.-J., Brodin, E.,1994. Weight bearing as an objective measure of arthritic pain in the rat.J. Pharmacol. Toxicol. Methods 31, 79–83.
Sinkov, V., Cymet, T., 2003. Osteoarthritis: understanding the pathophysiology, geneticsand treatment. J. Natl. Med. Assoc. 95, 475–482.
Tilson, H.A., 1990. Behavioral indices of neurotoxicity. Toxicol. Pathol. 18, 96–104.Torres-Lopez, J.E., Ortiz, M.I., Castaneda-Hernandez, G., Alonso-Lopez, R., Asomoza-
Espinosa, R., Granados-Soto, V., 2002. Comparison of the antinociceptive effect ofcelecoxib, diclofenac and resveratrol in the formalin test. Life Sci. 70 (14),1669–1676.
van der Kraan, P.M., Vitters, E.L., van Beuningen, H.M., van den Berg, W.B., 1992.Proteoglycan synthesis and osteophyte formation in ‘metabolically’ and ‘mechani-cally’ induced murine degenerative joint disease: an in-vivo autoradiographicstudy. Int. J. Exp. Pathol. 73, 335–350.

45P. Chandran et al. / European Journal of Pharmacology 613 (2009) 39–45
Vermeirsch, H., Biermans, R., Salmon, P.L., Meert, T.F., 2007. Evaluation of pain behaviorand bone destruction in two arthritic models in guinea pig and rat. Pharmacol.Biochem. Behav. 87, 349–359.
Wacnik, P.W., Kehl, L.J., Trempe, T.M., Ramnaraine, M.L., Beitz, A.J., Wilcox, G.L., 2003.Tumor implantation in mouse humerus evokes movement-related hyperalgesiaexceeding that evoked by intramuscular carrageenan. Pain 101, 175–186.
Yasmin, S., Fayazzadeh, H., Takami, S., Gong, W.C., Gill, M.A., 2000. Update onpathophysiology and treatment of osteoarthritis. Pharm. Times 75–85 (July).
Zimmermann, M., 1983. Ethical guidelines for investigations of experimental pain inconscious animals. Pain 16, 109–110.