Embed Size (px)
Citation preview

REVIEW Open Access
Pharmacokinetics–pharmacodynamicsissues relevant for the clinical use of beta-lactam antibiotics in critically ill patientsRui Pedro Veiga1,2,3* and José-Artur Paiva1,2,3
Abstract
Antimicrobials are among the most important and commonly prescribed drugs in the management of criticallyill patients and beta-lactams are the most common antibiotic class used. Critically ill patient’s pathophysiologicalfactors lead to altered pharmacokinetics and pharmacodynamics of beta-lactams.A comprehensive bibliographic search in PubMed database of all English language articles published from January2000 to December 2017 was performed, allowing the selection of articles addressing the pharmacokinetics orpharmacodynamics of beta-lactam antibiotics in critically ill patients.In critically ill patients, several factors may increase volume of distribution and enhance renal clearance, inducinghigh intra- and inter-patient variability in beta-lactam concentration and promoting the risk of antibiotic underdosing.The duration of infusion of beta-lactams has been shown to influence the fT >minimal inhibitory concentration and animproved beta-lactam pharmacodynamics profile may be obtained by longer exposure with more frequent dosing,extended infusions, or continuous infusions.The use of extracorporeal support techniques in the critically ill may further contribute to this problem and werecommend not reducing standard antibiotic dosage since no drug accumulation was found in the availableliterature and to maintain continuous or prolonged infusion, especially for the treatment of infections caused bymultidrug-resistant bacteria.Prediction of outcome based on concentrations in plasma results in overestimation of antimicrobial activity at thesite of infection, namely in cerebrospinal fluid and the lung. Therefore, although no studies have assessed clinicaloutcome, we recommend using higher than standard dosing, preferably with continuous or prolonged infusions,especially when treating less susceptible bacterial strains at these sites, as the pharmacodynamics profile mayimprove with no apparent increase in toxicity.A therapeutic drug monitoring-guided approach could be particularly useful in critically ill patients in whomachieving target concentrations is more difficult, such as obese patients, immunocompromised patients, thoseinfected by highly resistant bacterial strains, patients with augmented renal clearance, and those undergoingextracorporeal support techniques.
Keywords: Critical care or intensive care or critically ill, Sepsis or septic shock, Antibiotics, Pharmacokinetics,Pharmacodynamics
* Correspondence: [email protected] Hospitalar São João, EPE – Intensive Care Department, Porto,Portugal2Faculty of Medicine – University of Porto, Porto, PortugalFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Veiga and Paiva Critical Care (2018) 22:233 https://doi.org/10.1186/s13054-018-2155-1

BackgroundAntimicrobials are among the most important and com-monly prescribed drugs in the management of criticallyill patients and beta-lactams are the most common anti-biotic class used because of their broad spectrum of ac-tivity and high tolerability [1, 2].Early and appropriate antibiotic administration im-
proves clinical outcome of septic patients [3–7]. In thepresence of septic shock, besides conflicting results [8,9], each hour delay is associated with a measurable in-crease in mortality and other negative endpoints (e.g.,length of stay in ICU, acute kidney injury, acute lung in-jury, and global organ injury assessed by theSepsis-Related Organ Assessment score) [10, 11].Choosing the appropriate antimicrobial for the bacter-
ial activity spectrum is crucial but the correct dosageregimen (both dose and frequency) is, at least, of thesame importance for successful clinical cure and micro-biological eradication [11].Unlike organotropic drugs, where it is easy to titrate dose
to achieve a clinical response, antibiotics may take 24–72 hto present signs of resolution of infection, making it diffi-cult to determine the most appropriate dosage [1, 2].We conducted a comprehensive bibliographic search
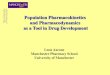
in the PubMed database of all English language articlespublished from January 2000 to December 2017, usingthe following keywords: critical care or intensive care orcritically ill and sepsis or septic shock and antibioticsand pharmacokinetics or pharmacodynamics. Articlesnot addressing beta-lactam pharmacokinetics (PK) orpharmacodynamics (PD) in critically ill patients were ex-cluded. A small number of articles derived from refer-ences in the articles selected were also reviewed. In theend, 214 studies were included in our review (Fig. 1).
Beta-lactam PD characteristicsKnowledge of the antimicrobial PD characteristics (in-hibition of growth, rate and extent of bactericidal action,and post-antibiotic effect (PAE)) provides a more ra-tional basis for determination of optimal dosing regi-mens in terms of the dose and the dosing interval.The antimicrobial activity of drugs is usually assessed
by determination of the minimum inhibitory concentra-tion (MIC) and the minimum bactericidal concentration(MBC) of the drug under specific conditions in vitro.These in vitro conditions are very different from thoseexpected at the site of infection, where the milieu is fre-quently acidic and anaerobic, and tissue protein maybind a variable amount of the drug. Additionally, theseparameters do not provide information on the timecourse of the antimicrobial effect—the fluctuating levelsthat are present in a patient treated with the drug—andare measured against a standard bacterial inoculum(about 10 colony-forming units (CFU) per millilitre [5])
that does not necessarily correspond to bacterial dens-ities at site of infection (10 CFU per gram of tissue orpus [8–10]). For bactericidal drugs, the MBC is generallynot more than fourfold higher than the MIC. The size ofthe residual bacterial population at the end of each dos-ing interval, and ultimately the efficacy of the antimicro-bial regimen, depends on the interplay of a variety ofbacterial, drug, and host factors that include the size ofthe initial bacterial population, the potency (MIC andMBC) and PK characteristics of the antimicrobial agent,the rate and extent of any bactericidal effect, the pres-ence of a post-antibiotic effect (PAE), the rate ofre-growth of persistent organisms, and the state of hostdefences [13].Three PD indices describe optimal killing associated
with antibiotics: fT >MIC, which is the amount of timethat the unbound drug concentration remains above theMIC of the infecting organism; Cmax/MIC, which is theratio between the maximum concentration of the drugand the MIC of the infecting organism; and AUC0–24/MIC, which is the ratio between total area under theconcentration–time curve (AUC) over 24 h and the MICof the infecting organism.Beta-lactams are time-dependent antimicrobials whose
efficacy is mainly related to fT >MIC [1, 2, 12–14].
299 Articles Reviewed
209 Articles Selected
3 articles selected from references of
these 211
212 Articles Selected
90 Articles Excluded: 45 addressing PK-PD issues of other classes of antibiotics;
1 addressing lesion consecutive to adverse event
11 not evaluating PK-PD issues;
3 addressing study protocols;
1 addressing prophylactic therapy;
1 addressing empirical therapy
19 addressing non-critically ill patients;
4 corresponding letters;
1 book chapter
3 in vitro studies;
1 addressing PK-PD issues of non-antibiotics.
Fig. 1 Articles reviewed, included, and excluded
Veiga and Paiva Critical Care (2018) 22:233 Page 2 of 34

Increasing drug concentrations much above the MBCdoes not enhance bacterial killing and the bactericidalaction of these drugs is relatively slow. When druglevels at the site of infection fall below the MIC, therelatively large residual population can resume growthquickly because most beta-lactams either have no oronly a short PAE [12]. McKinnon et al. compared thePD of cefepime and ceftazidime and observed that pa-tients with fT >MIC of 100% had significantly greaterrates of clinical cure and bacteriological eradicationthan patients with fT >MIC of < 100% [15].It is suggested that 50% fT >MIC of the dosage inter-
val is needed to ensure standard efficacy with these anti-microbials, whereas 100% fT >MIC of the dosageinterval should be ensured for optimal exposure in im-munocompromised patients. A further improvement inefficacy is observed when antibiotic concentrations arefour to five times greater than MIC [2, 12, 13]. The per-centage of time above MIC that correlates with efficacyvaries among different beta-lactam groups, being greaterfor cephalosporins and aztreonam than for penicillins,and greater for penicillins than for carbapenems. Also,variations occur among different bacterial species, beingless for staphylococci, for which beta-lactams have aPAE, than for streptococci and Gram-negative bacilli, forwhich beta-lactams do not have a PAE [2, 13].
Beta-lactam PK issues in the critically illDiscovered antibiotics are evaluated in vitro and testedin animals, initially for toxicity and subsequently for effi-cacy. The antibiotic dose and frequency are based onthese in vitro or animal in vivo PK/PD studies. Thesedosing regimens are then tested on healthy human vol-unteers for tolerability, with clinical efficacy studiesundertaken in non-critically ill patients. After the launchof the drug onto the general market, the same dosingregimen is used in critically ill patients; however, this islikely to lead to suboptimal outcomes in the ICU [5], es-pecially with more resistant bacterial strains [16] and inthe immunocompromised population [17].Beta-lactams are hydrophilic drugs and so their vol-
ume of distribution (Vd) is low and similar to that ofextracellular water. Variations in the extracellular fluidcontent and/or in renal or liver function may be consid-ered the most relevant and frequent pathophysiologicalmechanisms possibly affecting drug disposition in critic-ally ill patients. Other factors may contribute to alteredantibiotic concentrations: an interesting case-report byTaccone et al. [18] related the case of an obese septic pa-tient with Pseudomonas aeruginosa pneumonia treatedwith meropenem. The PD target (t > 4 × MIC > 40% ofthe dosing interval) was only achievable by dosing 3 gq6h at 3 h extended infusion and was associated withclinical improvement.
Compared with healthy volunteers and non-critically illpatients, in critically ill patients capillary leakage andedema, fluid therapy, pleural effusion, ascites, indwellingpost-surgical drainage, and hypoalbuminemia may in-crease Vd and cause antibiotic dilution in plasma andextracellular fluids. Some pathophysiological factors mayalso enhance (trauma, burns, the hyperdynamic conditionof the early phase of sepsis, the use of hemodynamicallyactive drugs) or reduce (renal failure, muscular wastage,bedridden patients) renal clearance and consequently mayalter plasma and extracellular antibiotic concentrations(with implications on time over MIC), induce high intra-and inter-patient variability, and promote the risk of anti-biotic underdosing [1, 2, 12, 14, 19–35]. Extracorporealsupport techniques also contribute to antibiotic concen-tration variability [36].PK studies on ICU septic patients reported, overall, in-
creased Vd with significant daily concentration fluctua-tions between and within patients [5, 36–41]. Clearanceof drugs is also affected and usually related to creatinineclearance [1, 42–44]. A single-center study of 17 ICUpatients with ventilator-associated pneumonia (VAP) de-scribed the PK profile of ertapenem and concluded that,because of its highly protein-bound profile, hypoalbu-minemia resulted in a higher protein-unbound fractionwith consequences for drug distribution and elimination[38]. Ulldemolins et al. [39] found the same while study-ing the PK profile of flucloxacillin. Ramon-Lopez et al.[45] described high PK variations (between and withinpatients) for meropenem in 12 burn ICU patients thatwere mostly related to age, body weight, and serum al-bumin. Carlier et al. [37] investigated the adequacy ofpiperacilin/tazobactam dosing and its trough variabilityduring an entire 7-day antibiotic course in 11 ICUpatients with pneumonia and normal renal function. Sixof them failed to achieve the PK/PD target of 100% fT >MIC at least once during the treatment course and con-siderable antibiotic concentration variability was foundwithin and between patients. The DALI study, a largemulticenter prospective study evaluated 248 ICU pa-tients treated for infection with beta-lactams and foundlarge variations on beta-lactam blood concentrations.The achievement of the PK/PD targets was highly incon-sistent, with one fifth of the patients not achieving theirmost conservative PK/PD target of 50% fT >MIC andbetter outcomes were described with higher drug expos-ure, at least for less severely ill patients [5].Septic patients with acute renal failure may have sub-
optimal antibiotic concentrations in the first days oftherapy when the recommended dosing adjustment forrenal failure is used [46]. Taconne et al. [40] studied thePK profiles of four beta-lactams (ceftazidime, cefepime,piperacilin/tazobactam, and meropenem) over the first24 h of treatment in 80 septic ICU patients. They
Veiga and Paiva Critical Care (2018) 22:233 Page 3 of 34

concluded that, besides high intra- and inter-patient PKvariability, standard first doses of broad-spectrumβ-lactams provided inadequate levels to achieve targetserum concentrations for extended periods of time.Augmented renal clearance has probably more impact
than altered Vd on the PK of beta-lactams [25, 27, 47–54].Roberts et al. [23] described the PK of cefazolin in plasmaand interstitial fluid of subcutaneous tissue in post-traumacritically ill patients and demonstrated that increasing cre-atinine clearance (ClCr) or decreasing serum albuminconcentrations will reduce the likelihood of achieving op-timal cefazolin exposure in subcutaneous interstitial tis-sue. In the presence of augmented renal clearance (ClCr> 130 mL/min), a much higher dose of cefazolin is re-quired to obtain similar relative drug exposures [23]. Conilet al. [43] found that higher ClCr values (> 50 mL/min)did not provide trough concentrations of piperacilin (4 gthree times a day) sufficient enough to attain the MIC formany pathogens in many of the patients studied.Hypoalbuminemia has also been associated with altered
PK. Wong et al. [55] described a linear correlation be-tween the percentage protein binding of flucloxacillin andthe plasma albumin concentration, though this was nottrue for ceftriaxone. Also, plasma albumin concentrationsand in vitro binding data from healthy volunteers shouldnot be used to predict unbound concentrations of ceftri-axone in ICU patients [56].
Use of extracorporeal support techniques incritical careAcute kidney injury (AKI) occurs in 50 to 65% ofcritically ill patients and in approximately two-thirdsof patients within the first 24 h after admission tothe intensive care unit (ICU) [57]. Critically ill pa-tients are usually supported with one of the forms ofcontinuous renal replacement therapy (CRRT)—con-tinuous venous-venous hemofiltration, hemodiafiltra-tion, hemodialysis (CVVHF, CVVHDF, CVVHD,respectively)—or with sustained low-efficiency dialysis(SLED). Molecules are transported across the filtermembrane by the mechanism of convection (drivenby the pressure gradient—CVVHF), diffusion (drivenby the concentration gradient—CVVHD, SLED), orboth (CVVHDF).Employing CRRT complicates antibiotic dosing to a
significantly higher extent than standard hemodialysisdue to the high number of variables, including Vd, flowof the dialysis fluid, replacement fluid infusion site (pre-or post-dilution mode), type and surface of the usedmembrane, and the difference between delivered andprescribed RRT dose.Vd in AKI may be significantly different from published
population estimates derived from healthy subjects.Besides the decreased plasma protein concentrations in
acutely ill patients, uremic solutes, such as hippurate andindoxyl sulfate, alter drug binding to albumin in chronicrenal failure and might do so in acute renal failure, al-though this has not been tested. The free fraction of manydrugs is increased in renal failure, even though the Vd fortotal drug may increase due to movement of unbounddrug into interstitial or total body water [57–59].Overall, a tendency for antibiotic underdosing in critic-
ally ill patients on CRRT or SLED likely exists. The modeand dose of CRRT vary quite widely from center to centerand from report to report, making it very difficult to cre-ate generally applicable beta-lactam dosing guidelines forcritically ill patients under CRRT. Additionally, antibioticconcentrations may vary depending on the degree of ex-traction and residual renal function, which is variable, dif-ficult to assess, and rarely considered despite its relevantcontribution to antibiotic clearance in patients undergoingCRRT (Tables 1 and 2) [60–96].Globally, we recommend not reducing standard anti-
biotic dosage since no drug accumulation was found inthe available literature and to maintain continuous or pro-longed infusion in critically ill patients on CRRT, SLED, orEDD, especially for the treatment of multidrug-resistantbacteria. Although usually not available in clinical rou-tines, a therapeutic drug monitoring (TDM)-guided strat-egy has potential benefit to ensure appropriate antibiotictherapeutic targets.Extracorporeal membrane oxygenation (ECMO) has
become an essential tool for severe cardiorespiratoryfailure in critically ill patients. It is thought to introduceadditional confounding factors to the already altered PKproperties of beta-lactams in this subset of patients.Sequestration of antibiotics in the ECMO circuit and theassociated systemic inflammation can further increasethe antibiotic Vd and reduce clearance [74, 97–99].However, very few in vivo studies have been performedin this subset of patients (Table 3). Globally, they showno significant statistical variation in Vd and clearance,but while probability of target attainment (PTA) withstandard ICU dosage regimens was achieved when treat-ing for highly susceptible Gram-negative bacteria, anti-biotic concentrations were below those desired to treatmore resistant strains.
Longer exposure regimens: continuous infusion,extended infusion, or reduced-interval dosingThe duration of infusion of beta-lactams has been shownto influence their fT >MIC. Improved PD profiles ofbeta-lactams may be obtained by longer exposure withmore frequent dosing, extended infusions, or continuousinfusions. Several studies reported PD benefits for targetattainment of extended and continuous infusions,especially considering highly resistant bacterial strains,even using smaller daily doses [1, 2, 36, 41, 103–143].
Veiga and Paiva Critical Care (2018) 22:233 Page 4 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
Fish
etal.[67]
Tomorefully
characterizePK
disposition
ofim
ipen
emin
critically
illadultpatientsdu
ringcurren
tlyused
CVV
Hor
CVV
HDFregimen
s
Imipen
em-cilastatin
Prospe
ctiveop
en-labe
lstudy
ofim
ipen
em-cilastatin
administeredas
thecombinatio
nprod
uctin
afixed
1:1ratio
Adu
ltICUpatientswith
CVV
H(n
=6
patients)or
CVV
HDF(n
=6patients)
Imipen
emadministeredat
0.5g
every8to
12h(totaldaily
dosesof
1to
1.5g/day)
byintraven
ous
infusion
over
30min
Pre-
andpo
st-m
embraneplasma
andcorrespo
ndingultrafiltrate
ordialysatesamples
werecollected
at1,2,4,and8or
12h(dep
ending
ondo
sing
interval)aftercompletionof
thedrug
infusion
Patientson
CVV
HDFhadsign
ificantly
high
erCLs
comparedto
patientson
CVV
H(P
=0.01),bu
tthisdifference
was
notsign
ificant
whe
nno
rmalized
fortotalb
odyweigh
t(P
=0.477)
Theob
served
t1/2
was
overallsim
ilar
betw
eenbo
thpatient
grou
ps(P
=0.860)
Nosign
ificant
differzen
ceswere
foun
din
Vd,S,and
Sa,or
ultrafiltratio
nrates
MeanCmax,C
min,and
AUC0–24
values
inpatientsreceiving0.5gbid
durin
gCVV
Hversus
CVV
HDFwere
17.5g/mLvs
14.1g/mL,1.1g/mLvs
1.0g/mL,and129.5g·h/mLvs
110.3g·h/mL,respectively,andin
patientsreceiving0.5gtid
they
were
18.5g/mLvs
17.1g/mL,1.9g/mLvs
1.1g/mL,and183.3g·h/mLvs
140.6g·h/mL,respectively
Doses
of0.5gbidand0.5gtid
gene
rally
provided
T>MIC
ofat
least
40to
50%and50
to60%,respectively
(MICsof
<2g/mL)Doses
of0.5g
every6h(2.0g/day)weremod
eled
basedon
thePK
parametersob
served
inthisstud
yandtheT>MIC
calculated:at2.0g/day,organism
swith
aMIC
of<4g/mLhadaT>MIC
ofatleast50
to80%.And
fortho
sewith
MIC
<8g/mL,T>MIC
rang
edfro
m34
to62%
CVV
HandCVV
HDFcontrib
uteto
imipen
emclearanceto
agreater
degree
than
previouslyrepo
rted
.Im
ipen
emdo
sesof
1.0g/dayappe
arto
achieveconcen
trations
adeq
uate
totreatmostcommon
Gram-
negativepathog
ens(MICup
to2g/mL)
butdo
sesof
2.0g/dayor
moremay
berequ
iredto
adequatelytreatand
preventresistanceinpathog
enswith
high
erMICs(M
IC>4to
8g/mL)
Malon
eet
al.
[68]
Tomorefully
characterizethe
PKdisposition
ofcefepimein
critically
illadultICUpatientsdu
ring
CVV
Hor
CVV
HDF
Cefep
ime
Prospe
ctive,ob
servationalstudy
12adultICUpatientsreceivingCRR
Tforsevere
renalfailure
(5patientson
CVV
H,7
patientson
CVV
HDF)
Cefep
imeregimen
sinclud
edeither
1gor
2gdo
sesadministered
intraven
ouslyevery12
or24
h(total
daily
dosesof
1to
4g/day)
Samplingwas
perfo
rmed
assoon
aspo
ssibleafterinitiationof
theCRR
Tanddrug
therapy.Pre-
andpo
st-
mem
braneveno
usbloo
dsamples
wereob
tained
1,2,4,and8hafter
thecompletionof
thedrug
infusion
andjustbe
fore
administrationof
the
next
dose
Drugclearancedu
ringCRR
T(CL
CRR
T)and%CLS
weresign
ificantly
high
er(P
=0.002and0.018,
respectively),and
t1/2
was
sign
ificantlylower
(P=0.005)
amon
gpatientsreceivingCVV
HDFthan
inpatientsreceivingCVV
H.
ThemeancefepimeSdu
ringCVV
HandSa
durin
gCVV
HDFwere
estim
ated
at0.86
±0.04
and0.78
±0.10,respe
ctively,indicatin
gthat
cefepimeisextensivelycleared
across
theCRR
Tmem
brane
App
roximately40
and59%
ofcefepimeCLs
was
attributed
tomem
braneclearancedu
ringCVV
HandCVV
HDF,respectively,indicatin
gthat
theclearanceof
cefepimewas
Itappe
arsthat
CVV
HDFismore
efficient
than
CVV
Hin
elim
inating
cefepime.How
ever,the
presen
tstud
yinclud
edtoofew
subjectsand
toomuchvariabilitywas
observed
with
inthedata
tode
mon
strate
this
conclusively.
Cefep
imeregimen
sof
0.25
to1.0g/
dayas
recommen
dedby
the
manufacturerforanuricpatientsor
thosereceivingconven
tional
hemod
ialysiswou
ldlikelybe
subthe
rape
uticagainstallb
utthe
mosthigh
lysuscep
tiblepathog
ens
whe
nadministeredto
patients
receivingCRR
TTheauthorsrecommen
dcefepime
dosesof
2gdaily
unde
rmost
Veiga and Paiva Critical Care (2018) 22:233 Page 5 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
substantially
enhanced
durin
gbo
thCRR
Ttechniqu
esValues
forcefepimeVd
werealso
statisticallydifferent
(P=0.03)
betw
eenCVV
HandCVV
HDFgrou
ps,
butchange
sin
Vdwereon
lyweakly
correlated
with
change
sin
t1/2
(Spe
arman’srank
correlation
coefficient
of0.641;P=0.133)
Allpathog
ensisolated
from
stud
ypatientshadcefepimeMICsof
<4g/mL,anddo
sesas
low
as1g/day
wou
ldpred
ictablyprovideadeq
uate
treatm
entdu
ringeither
CVV
Hor
CVV
HDF
Cefep
imedo
sesof
2g/daywou
ldbe
expe
cted
toachievefavorable
concen
trations
inserum
against
suscep
tiblepathog
ens(M
IC<8
g/mL)
with
T>MIC
greaterthan
50%.C
efep
ime(2
g/day)du
ring
either
CVV
Hor
CVV
HDFwou
ldalso
bepred
ictedto
achievefavorable
T>MIC
>80%
againstpathog
ens
with
interm
ediate
suscep
tibility
(MIC
<16
g/mL)
circum
stancesin
critically
illpatients
receivingCR
RT.H
owever,con
sidering
moreresistant
strains,do
sesof
4g/dayshou
ldbe
considered
for
empiricaltherapyinlife-threatening
nosocomialinfectio
ns,w
hileaw
aitin
gresults
ofcultu
reandsusceptib
ility
testing
Muelleret
al.
[69]
Tode
term
inethePK
ofpipe
racillin-
tazobactam
incritically
illpatients
with
acuteanuricrenalfailure
treatedby
CVV
H
Pipe
racilin-tazob
actam
Prospe
ctive,ob
servationalstudy
8adultICUpatientson
CVV
HD
Doses
anddo
sing
sche
duleswere
chosen
empiricallyby
theattend
ing
physicians
andwereadministered
intraven
ouslyover
15min
Pre-dialyzer
bloo
dsamples
and
dialyzer-outletdialysatesamples
weretakenbe
fore
drug
administration,
at10
and30
min
afterinfusion
,and
at1,2,4,6,8,12,
20,22,and24
hafterinfusion
CVV
HDclearanceof
pipe
racillinwas
37%
(med
ian,
with
arang
eof
13to
100%
)andtheCVV
HDclearanceof
tazobactam
was
38%
(med
ian,
with
arang
eof
32to
92%)of
CLtotal
Vdwas
0.31
±0.07
and0.24
±0.09
forpipe
racilin
andtazobactam
,respectively
t1/2
was
4.3±1.2and5.6±1.3for
pipe
racilin
andtazobactam
,respectively
Simulations
of4gof
pipe
racillinand
0.5gof
tazobactam
administered
every12
hand2gof
pipe
racillin
and0.25
gof
tazobactam
administeredevery8hresultedin
times
aboveMIC
of>50%
for
pipe
racillinwith
suscep
tible(M
ICof
pipe
racillin16
mg/liter;tim
eabove
MIC,48to
100%
)andinterm
ediate
suscep
tible(M
IC32
mg/liter;tim
eaboveMIC,17to
100%
)pathog
ens
insevenof
eigh
tpatients
Arelevant
contrib
utionof
CVV
HDto
theoverallelim
inationof
both
drug
shasto
betakeninto
accoun
tTheestim
ated
Vdvalues
aregreater
than
thoseof
healthysubjectsand
t1/2
ofbo
thdrug
swerefourfold
greaterthan
thoseof
healthy
subjectsandtw
ofoldgreaterthan
thosewith
acreatin
ineclearance<
20mL/min/1.73m
2
Patientswith
residu
alrenalfun
ction
andpatientsthat
receiveCRR
Twith
high
erdialysateflow
ratesor
high
eradditio
nalh
emofiltrate
flow
rates
might
have
high
erCLof
pipe
racillin-
tazobactam
,resultin
gin
high
erdo
sage
need
s
Veiga and Paiva Critical Care (2018) 22:233 Page 6 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
Robe
rtset
al.
[70]
Toassess
thevariabilityof
antib
iotic
trou
ghconcen
trations,the
influen
ceof
effluen
tflow
rateson
such
concen
trations,and
theincide
nceof
subo
ptim
alantib
iotic
dosage
Merop
enem
and
pipe
racilin-tazob
actam
Prospe
ctive,ob
servational,
multicen
terstud
y,cond
uctedwith
inthemulticen
terRENALstud
y.It
assessed
theeffect
ofpo
st-dilutio
nal
high
erintensity
(40mL/kg/h
effluen
trate)or
lower
intensity
(25mL/kg/h
effluen
trate)CRR
T.Patientswere
rand
omized
toreceiveeither
high
eror
lower
intensity
effluen
tflow
rate
24adultICUpatientswith
AKI
onCVV
H.17patientswereon
merop
enem
and7patientson
pipe
racilin-tazob
actam
Antibiotic
dosing
was
atthe
discretio
nof
thetreatin
gph
ysician:
merop
enem
0.5gevery12
hto
1g
every8h;pipe
racilin
4gevery12
hto
4gevery6h
Bloo
dsamples
wereob
tained
onmorethan
oneoccasion
ondifferent
days
andbe
fore
administrationof
theantib
iotic
tode
term
inethe
trou
ghconcen
tration
Therewas
markedvariabilityin
trou
ghconcen
trations
forall
antib
iotics:6.7-fold
formerop
enem
;3.8-fold
forpipe
racillin;
10.5-fo
ldfor
tazobactam
Whe
ninvestigatingtrou
ghconcen
trationvariabilityaccordingto
effluen
tflow
rate,n
ostatistically
sign
ificant
differences
werefoun
dusingun
ivariate
analysis
Merop
enem
trou
ghconcen
trations
were10.1±8.7and15.0±6.4for
low
andhigh
effluen
tflow
rates,
respectively
Pipe
racilin
trou
ghconcen
trations
were83.6±63.8and204.0±105.0
forlow
andhigh
effluen
tflow
rates,
respectively
100%
T>MIC
was
achieved
with
merop
enem
(forMIC
2mg/L)
and
pipe
racilin-tazob
actam
(forMIC
16mg/L)
76%
T>MIC
was
achieved
for
merop
enem
(forMIC
8mg/L)
86%
T>MIC
was
achieved
for
pipe
racilin-tazob
actam
(forMIC
64mg/L)
Itappe
arsthat
CRR
Teffluen
tflow
ratescann
otbe
used
inde
pend
ently
togu
idedo
seadjustmen
tTrou
ghconcen
trations
failedto
achievethehigh
ertherapeutic
target
in24%
ofpatientsreceiving
merop
enem
and14%
ofpatients
receivingpipe
racillin,
which
isof
concern
Dose-adjustingto
achieveatarget
concen
trationthat
exceed
sthe
approp
riate
MIC
butisless
than
potentially
toxicconcen
trations
seem
sde
sirablebu
tcann
otbe
reliablyachieved
with
empirical
dosing
Banyaiet
al.[71]
Tostud
ythePK
ofcefpiro
mein
critically
illpatientswith
acute
kidn
eyfailure
treatedby
CVV
Hand
tode
velopan
optim
aldo
sing
regimen
inpatientswith
CVV
H
Cefpirome
Prospe
ctive,ob
servationalstudy
8adultICUanuricpatientswith
acutekidn
eyfailure
onCVV
HAllpatientsreceived
ado
sage
of2g
cefpiro
meover
ape
riodof
30min,
every8hafterstartin
gthe
hemofiltratio
nBloo
dsamples
werecollected
from
thearterialand
veno
uslineof
the
extracorpo
realcircuitim
med
iatelyat
baselineandat
60,120,180,240,
300,360,and420min
afterthestart
ofthefirstinfusion
.Add
ition
albloo
dsamples
werecollected
immed
iately
before
theen
dand30
min
afterthe
endof
each
infusion
,upto
atotal
stud
ype
riodof
48h
Ultrafiltratio
nsamples
werecollected
from
theou
tletof
theultrafiltrate
compartmen
tof
thehe
mofilter
atcorrespo
ndingtim
es
Cmax14.8±3.2μg
/mL(10.8to
19.7)
Cmin3.1±0.8μg
/mL
Posthe
mofiltratio
nto
pre-
hemofiltratio
nratio
of0.23
±0.10
Totald
rugremovalof
78.0%±8.8%
Elim
inationt1/2
was
2.36
±0.59
h(1.6to
3.2h).The
calculated
Vdwas
118±36
LTotalb
odyclearanceand
hemofiltratio
nclearancewere589.1
±164.5mL/min
and43.3±7.8mL/
min,respe
ctively
Thecalculated
AUCwas
60.4±
16.0mg/L·h
Highe
stlevelsof
cefpiro
mewere
sign
ificantlylower
comparedwith
values
observed
inhe
althy
volunteersandin
patientson
hemod
ialysis
Plasmacefpiro
meconcen
trations
remaine
dabove4μg/mLfor62%
andabove8μg/mLfor25%
ofthe
dosing
interval,respe
ctively
Inpatientsinfected
with
aninterm
ediate
suscep
tible
Pseudo
mon
asaerugino
sa(M
IC90
~8mg/L),n
osufficien
tantim
icrobial
efficacycanbe
expe
cted
Com
parablelow
trou
ghlevelsof
3.1±0.8μg/mLsugg
estado
sage
recommen
datio
nof
2gcefpiro
me
every8h
Veiga and Paiva Critical Care (2018) 22:233 Page 7 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
Eyleret
al.[72]
Tode
term
inethePK
ofertape
nem
incritically
illadultsreceivingCVV
HD
orCVV
HDF
Ertape
nem
Prospe
ctive,op
en-labe
l,first-dosePK
stud
y8adultICUpatientswith
suspected
orconfirm
edGram-neg
ative
infections
receivingCVV
HD
(4patients)or
CVV
HDF(4
patients)
1gertape
nem
was
administeredas
ahalf-ho
urintraven
ousinfusion
Bloo
dsamples
werecollected
from
theCVV
HDcircuitat
thesampling
port,justbe
fore
thehe
mod
ialysis
filterat
timezero
(baseline),30min
(end
ofinfusion
),and1,2,4,8,12,
18,and
24hafterthestartof
the
ertape
nem
infusion
.Atthesame
timepo
ints,effluent
was
also
collected
from
theeffluen
tpo
rtof
theCVV
HD/F
circuit
CLS,unb
ound
48mL/min
VC,unb
ound
32l
VP,unb
ound
21l
CLdial,un
boun
d36
mL/min
PTA(40%
T>MIC)andfractionof
the
dosage
intervalspen
tabovetheMIC
fordifferent
regimen
swere
ForMIC
of0.5mg/L
500mgq1
2h,1.0and0.999
500mgq2
4h,1.0and0.999
750mgq2
4h,1.0and0.999
1000
mgq2
4h,1.0and0.999
ForMIC
of1mg/L
500mgq1
2h,1.0and0.999
500mgq2
4h,0.99and0.916
750mgq2
4h,1.0and0.999
1000
mgq2
4h,1.0and0.999
ForMIC
of2mg/L
500mgq1
2h,1.0and0.992
500mgq2
4h,0.962
and0.563
750mgq2
4h,0.999
and0.750
1000
mgq2
4h,0.999
and0.917
Theun
boun
dfraction(20to
40%)
was
markedlyincreasedcompared
tothoserepo
rted
forhe
althy
volunteers(5
to15%)
Attheeffluen
trates,ertape
nem
was
clearedto
asubstantiald
egree
Duringthestud
ysamplingpe
riod,
thedo
seof
1gevery24
hprod
uced
unbo
undertape
nem
concen
trations
that
remaine
dabove2μ
g/mLforan
averageof
90%
ofthedo
sing
interval,achieving
thePD
targetsin
alleight
patients
Mon
teCarlo
simulations
revealed
that
99.9%
ofsimulated
subjects
wou
ldachieveun
boun
dertape
nem
concen
trations
above2μ
g/mLforat
least40%
oftheinterval,w
ithconcen
trations
remaining
above
2μg/mLforamed
ianof
92%
(rang
e,33
to100%
)of
thedo
sing
interval
Particularlyin
patientswhe
reorganism
swith
high
MICsare
suspected,
itmay
bene
cessaryto
usedo
ses>500mgq2
4h.
Con
centratio
nsremaine
dabove
2μg/mLforan
interquartile
rang
eof
only50
to67%
ofthedo
sing
interval
Vossen
etal.
[73]
TocharacterizethePK
profile
of1000
mgdo
ripen
emq8
hforcritically
illpatientsreceivingCRR
T
Doripen
emProspe
ctive,op
en-labe
l,ob
servationalstudy
13adultICUpatientsun
derCRR
T(5
onCVV
H,5
onCVV
HD,3
onCVV
HDF)
Allpatientsreceived
1000
mgevery
8hat
a30-m
ininfusion
Bloo
danddialysatesamples
were
draw
nfro
mthearterial(inpu
t),
veno
us(outpu
t),and
effluen
tdialysatepo
rtsof
thedialysis
machine
before
thefirst
administrationof
dorip
enem
andat
0.5,1,2,3.5,7,8,9,16,17,24,24.5,
25,26,27.5,31,32,33,40,41,and
48hfollowingthestartof
thefirst
infusion
Allpatients:AUC0–8(m
g·h/L)
78.58
±10.32;Clto
t(L/h)8.07
±1.77;
Clpre-postfilter(m
L/min)36.06±
14.27;Sc
0.150±0.053;ClSc(m
L/min)5.20
±1.95;Vdtotal59.26
±26.47;t1/2
(h)5.39
±2.84
Patientson
CVV
H(n
=3):A
UC0–8
(mg·h/L)
87.15±8.13;C
ltot(L/h)
6.53
±1.00;C
lpre-postfilter(m
L/min)
63.82±5.83;Sc0.129±0.033;ClSc
(mL/min)6.45
±1.81;Vdtotal
51.05±10.18;t1/2
(h)5.72
±1.96
Patientson
CVV
HD(n
=5):A
UC0–8
(mg·h/liter)77.59±12.31;Clto
t(L/h)
7.48
±1.43;C
lpre-postfilter(m
L/min)
34.03±7.22;Sc0.164±0.067;ClSc
(mL/min)5.63
±2.30;Vdtotal71.01
±34.98;t1/2
(h)6.80
±3.37
Patientson
CVV
HDF(n
=5):A
UC0–8
(mg·h/L)
76.15±4.50;C
ltot(L/h)
9.29
±1.28;C
lpre-postfilter(m
L/min)
26.99±5.34;Sc0.145±0.035;ClSc
(mL/min)4.68
±1.43;Vdtotal50.80
Themeanhe
mofilter
clearancerates
observed
slightlyexceed
edthose
repo
rted
intheliterature
Thesievingcoefficientsob
served
differeddram
aticallyfro
mthose
repo
rted
previously
Theprefilter/postfilter
clearance
values
foun
din
ourtrialare
with
intherang
eof
values
repo
rted
previouslyforim
ipen
emand
merop
enem
Therewas
anun
characteristicallylow
clearanceforCVV
HDFpatients,
which
may
beattributed
tothe
larger
mem
branesize
andhigh
ermem
branekU
Fem
ployed
forthe
CVV
HFandCVV
HDgrou
ps.The
usual
expe
ctationforbe
ta-lactam
antim
icrobialswou
ldbe
quite
the
oppo
site:C
VVHDFclearancevalues
shou
ldbe
high
erthan
CVV
HDor
CVV
Hclearancevalues.H
owever,this
istrue
onlyifthesameflow
rates
Veiga and Paiva Critical Care (2018) 22:233 Page 8 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
±6.34;t1/2(h)3.87
±0.80
Thesimulations
cond
uctedshow
that
theprop
osed
dose
levelo
f1000
mgevery8hissupe
riorto
lower
dosesforreaching
thede
sired
plasmado
ripen
emconcen
trationof
8mg/L.Alth
ough
meantrou
ghconcen
trations
inalld
osing
regimen
sexceed
ed4mg/Ldu
ring
steady
state,theindividu
alou
tcom
eswerehigh
lyvariable
Atado
seof
500mgevery8h,
only
39.5%
ofthesimulated
patients
show
edtrou
ghconcen
trations
that
wereconstantlyabovethelower
threshold(4
mg/L)
durin
gsteady
state.Atado
seof
1000
mgevery
8h,
plasmaconcen
trations
stillfell
below
8mg/L,bu
tno
tlower
than
4mg/L,for60.5%
ofthesimulated
patients
andmem
branematerialsarechosen
.Ifthe1-gq8
hregimen
isused
,39.5%
ofthepatientswillreacha
trou
ghlevelo
f8mg/Lat
theen
dof
each
dosing
interval.Toattain
sufficien
tdrug
expo
sure
durin
gthe
firstdo
singintervaltheadministratio
nof
aninitial“loadingdo
se”of
20.4mg/
kgof
body
weigh
tissugg
ested
Thebroadtherapeutic
inde
xof
beta-lactam
sfavorshigh
erdo
sing
,providingsafety
marginformore-
effectiveRR
Tmod
alities
Carlieret
al.[74]
Tode
scrib
ethePK
ofcefepimein
septicshockpatientsrequ
iring
CRR
Tandto
investigatewhe
ther
PK/PD
targetsareachieved
with
curren
tdo
sing
strategies
aswellasto
investigatethepo
tentialadvantage
sof
alternativedo
sing
regimen
s
Cefep
ime
Prospe
ctive,ob
servationalstudy
13adultICUpatientswith
septic
shockandon
CRR
T(CVV
HFor
CVV
HDF)
Patientsreceived
2gq8
hor
q12h
.Thedo
sewas
administeredas
a30-m
inintraven
ousinfusion
Bloo
dsamples
weredraw
non
the
dayof
inclusionandthen
every
second
daydu
ringCRR
Ttreatm
ent
whe
neverpo
ssible.O
neach
samplingday,bloo
dsamples
were
draw
nim
med
iatelybe
fore
antib
iotic
administration(0
h)andthen
at1,2,
and5handat
6or
12h(dep
ending
ontheantib
iotic
regimen
)afterthe
startof
theinfusion
CL(L/h)4.5
Vd(L)40.6
PTAat
different
UFR
consideringa
MIC
of16
mg/L
UFR
1000
mL/h
1gq1
2h100%
T>MIC
64%
and
60%T>MIC
95%
2gq1
2h100%
T>MIC
89%
and
60%T>MIC
99%
1gq8
h100%
T>MIC
95%
and
60%T>MIC
100%
2gq8
h100%
T>MIC
99%
and
60%T>MIC
100%
1gq6
h100%
T>MIC
100%
and
60%T>MIC
100%
UFR
1500
mL/h
1gq1
2h100%
T>MIC
31%
and
60%T>MIC
80%
2gq1
2h100%
T>MIC
82%
and
60%T>MIC
98%
1gq8
h100%
T>MIC
87%
and
60%T>MIC
99%
2gq8
h100%
T>MIC
96%
and
60%T>MIC
100%
1gq6
h100%
T>MIC
97%
and
60%T>MIC
100%
UFR
2000
mL/h
1gq1
2h100%
T>MIC
9%and
Antibiotic
clearancewas
prop
ortio
nal
toUFR,w
ithim
portantvariability
betw
eenpatientsbo
thforclearance
andVd
Ado
seof
2gq8
hor
1gq6
hleads
toop
timaltarget
attainmen
t(100%
T>MIC)whilstminim
izingthe
prob
ability
ofreaching
toxictrou
ghconcen
trations
forpatientstreated
with
ahigh
UFR
(1500–2000
mL/
min).How
ever,the
optim
aldo
sefor
patientstreatedwith
lower
UFRs
(≤1000
mL/h)
whe
naimingforthe
high
target
was
1gq8
h
Veiga and Paiva Critical Care (2018) 22:233 Page 9 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
60%T>MIC
51%
2gq1
2h100%
T>MIC
73%
and
60%T>MIC
95%
1gq8
h100%
T>MIC
79%
and
60%T>MIC
95%
2gq8
h100%
T>MIC
92%
and
60%T>MIC
100%
1gq6
h100%
T>MIC
93%
and
60%T>MIC
100%
Seyler
etal.[75]
Toevaluate
whe
ther
the
recommen
deddo
sesof
broad-
spectrum
beta
-lactam
sresultin
approp
riate
serum
concen
trations
inICUpatientswith
severe
sepsisand
septicshockreceivingCRR
T
Merop
enem
Pipe
racilin-tazob
actam
Cefep
ime
Ceftazidime
Prospe
ctive,op
en-labe
lstudy
53adultICUpatientswith
severe
sepsisor
septicshockon
CRR
T(CVV
H,n
=19
orCVV
HDF,n=34)
Merop
enem
1gq1
2h(n
=17)
Pipe
racilin-tazob
actam
4.5gq6
h(n
=16)Cefep
ime2gq1
2h(n
=8)
Ceftazidime2gq1
2h(n
=12)
Each
antib
iotic
dose
was
administeredas
a30-m
ininfusion
Serum
concen
trations
ofthese
antib
ioticswerede
term
ined
from
samples
takenbe
fore
(t=0)
and1,2,
5,and6or
12h(dep
ending
onthe
bea-lactam
regimen
)afterthe
administrationof
each
antib
iotic
Seriesof
measuremen
tswere
separatedinto
thosetakendu
ring
theearly
phase(<
48hfro
mthefirst
dose)of
therapyandthosetaken
later(>
48h)
Merop
enem
Vd(l/kg)0.45
(0.20to
3.03)
Cmax
(μg/mL)
26(15to
67)
Cmin
(μg/mL)
6(2
to11)
AUC(m
g/h/mL)
134(61to
291)
CL(m
L/min/kg)
1.15
(0.54to
3.37)
t1/2
(h)4.39
(2.61to
30.5)
Pipe
racilin-tazob
actam
Vd(l/kg)0.44
(0.22to
1.72)
Cmax
(μg/mL)
138(36to
262)
Cmin
(μg/mL)
60(4
to155)
AUC(m
g/h/mL)
527(62to
1378)
CL(m
L/min/kg)
1.15
(0.27to
6.26)
t1/2
(h)4.16
(1.05to
15.3)
Cefep
ime
Vd(l/kg)0.55
(0.33to
0.94)
Cmax
(μg/mL)
43(28to
83)
Cmin
(μg/mL)
11(3
to22)
AUC(m
g/h/mL)
379(148
to483)
CL(m
L/min/kg)
1.04
(0.43to
2.97)
t1/2
(h)6.17
(3.30to
22.9)
Ceftazidime
Vd(l/kg)0.37
(0.22to
0.84)
Cmax
(μg/mL)
78(54to
118)
Cmin
(μg/mL)
24(5
to46)
AUC(m
g/h/mL)
536(258
to906)
CL(m
L/min/kg)
0.52
(0.13to
1.61)
t1/2
(h)7.74
(2.52to
33.5)
PK/PDtarget
attainmen
t(fo
urtim
esMIC
attainmen
tforPseudo
mon
asspp.)
Merop
enem
Day
<48
h(n
=7)
71%
Day
>48
h(n
=15)87%
Pipe
racilin-tazob
actam
Day
<48
h(n=12)66%
Day
>48
h(n
=9)
78%
Cefep
ime
Day
<48
h(n=7)
0%Day
>48
h(n
=4)
0%
Therecommen
deddo
sesforbroad-
spectrum
beta-lactam
sarege
nerally
insufficien
tto
maintaintherapeutic
serum
concen
trations
greaterthan
four
times
theMIC
ofP.aerugino
saApp
lyingresults
toothe
rMICs,the
observed
concen
trations
forall
antib
ioticswereadeq
uate
in90%
ofpatientson
lyforMICslower
than
the
clinicalbreakpoint
ofPseudo
mon
asspp.,w
hich
correspo
ndto
MICsof
sensitive
Enteroba
cteriaceae
Inthefirst48
hof
treatm
ent,29%,
34%,100%,and
62%
ofou
rpatients
treatedwith
merop
enem
,piperacillin-
tazoba
ctam
,cefepimeand
ceftazidim
e,respectiv
ely,
never
reachedthePK
target.A
fter4
8hof
treatm
ent,thedrug
concentrations
obtained
werehigh
er(significantly
different
onlyform
erop
enem
),bu
tthey
remainedinsufficientinmany
patients
Attheon
setof
sepsisin
patients
receivingCRR
T,similarbe
ta-lactam
dosesto
thoseused
intheabsence
ofrenalfailure
shou
ldbe
given
durin
gthefirst48
hof
therapy
Doseredu
ctionshou
ldbe
considered
thereafter
toavoiddrug
accumulation.
Con
side
ringthelarge
PKvariability,therapeutic
drug
mon
itorin
gof
beta-lactam
sshou
ldbe
perfo
rmed
toop
timizeantib
iotic
efficacy
Veiga and Paiva Critical Care (2018) 22:233 Page 10 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
Ceftazidime
Day
<48
h(n=8)
38%
Day
>48
h(n=7)
71%
Robe
rts
etal.
[76]
Toevaluate
variabilityin
CLandVd
andto
assess
theeffect
ofCRR
Tprescriptio
non
extracorpo
realand
system
icantib
iotic
CLandVd
inpatientstreatedwith
CRR
Tof
different
intensities
Merop
enem
Pipe
racillin-tazobactam
Nestedcoho
rtprospe
ctive
multicen
terob
servationalP
Kstud
ywith
inarand
omized
controlledtrial
ofCRR
Tintensity
Patientswererand
omlyassign
edto
receivepo
st-dilutionalhem
odiafiltration
aseither
ahigh
er(40mL/kg
body
weigh
t/heffluentflowrate)o
rlow
er(25mL/kg
body
weigh
t/heffluent
flowrate)intensityrate
Samplingoccurred
each
day(1)
immed
iatelybe
fore
antib
iotic
dosing
,(2)aftercompletionof
their
intraven
ousinfusion
,and
(3)at
4h
aftercompletionof
infusion
Itoccurred
at65
timepo
intsfor
merop
enem
and29
timepo
intsfor
pipe
racillin-tazobactam
in24
patients
Meanhe
mod
iafiltrationclearanceof
merop
enem
,piperacillin,and
tazobactam
didno
tdiffersignificantly
betw
eenhigh
ervs
lower
CRRT
intensity:23(16–29)vs21
(15–28),
P=0.4802;22(21–31)vs24
(17–31),
P=0.9091;37(34–49)vs56
(41–66),
P=0.0642,respectively
System
icclearanceandVd
were
Merop
enem
38mL/min
(23–95)and
17.5L
Pipe
racillin59
mL/min
(37–115)
and
18.7L
Tazobactam
113mL/min
(45–248)
and49.3L
Theprescribed
intensity
ofCRR
Tdid
notadeq
uatelypredictextracorpo
real
clearanceor
Sd,CLs,Vd,or
half-life
System
icCLandelim
inationhalf-life
didno
tdifferaccordingto
CRR
Tdo
se,and
sotheCRR
Tprescriptio
nmay
notbe
useful
forgu
iding
antib
iotic
prescribing.
Inmanycases,
extracorpo
realCLaccoun
tedfor
morethan
30%
oftheob
served
system
icCLforthat
antib
iotic,w
hich
isasugg
estedthresholdfor
adjustmen
tof
thedo
sing
regimen
Drugmon
itorin
gmay
bethemost
practicalmetho
dforen
surin
gthat
antib
iotic
therapeutic
targetsare
achieved
incritically
illpatients
receivingCRR
T
Ohchi
etal.[77]
ToinvestigatePK
characteristicsof
dorip
enem
inpatientsreceiving
high
-flow
vsconven
tionalflow
intensity
CVV
HDF
Doripen
emProspe
ctive,ob
servationalstudy
Adu
ltICU
Twopatientswith
AKI
onhigh
-flow
CVV
HDF.Patientson
conven
tional
CVV
HDFwerede
scrib
edin
aprevious
stud
yDoripen
emadministrated
as250mg
sing
ledo
seinfusion
over
1h
Bloo
dsamples
werecollected
at1
(justpriorto
theen
dof
antib
iotic
infusion
),2,3,4,7,and12
hafter
initiatingtheinfusion
Highflow
CVV
HDFparameters:bloo
dflow
100mL/min;d
ialysate
flow
rate
1500
mL/h;
filtrationflow
rate
900mL/h
Con
ventionalC
VVHDF
AUC74.15±15.5mg.h/L
Cls58
±12.7mL/min
Cld
ialysis13.5±1.6mL/min
t1/2
7.9±3.7h
High-flow
CVV
HDF
AUC35.2mg.h/L
Cls118mL/min
Cld
ialysis41.9mL/min
t1/2
2.9h
Extracorpo
realclearanceincreasesin
prop
ortio
nwith
theintensity
dialysis
rate
Thedaily
dose
thus
mustbe
increased
to1.0–1.5g,thesamedo
sage
used
whencreatinineclearanceis>50
mL/
min
Arzuaga
etal.[78]
Tostud
ythePK
ofpipe
racillinand
tazobactam
durin
gCRR
Tin
ICU
patientswith
vario
usde
greesof
renalimpairm
ent.
Pipe
racilin-tazob
actam
Prospe
ctive,ob
servationalstudy
14adultICUpatientson
CVV
HDF,
grou
pedaccordingto
severity(CLC
R10
mL/min,10<CLC
R<50
mL/min,
andCLC
R>50
mL/min)
Pipe
racilin
4gandtazobactam
0.5g
wereadministrated
every6or
8h,
by20-m
inintraven
ousinfusion
Prefilter
bloo
dandultrafiltrate
samples
werecollected
at0,0.3,0.5,
0.75,1,3,6,and
8h(in
case
ofadministrationevery8h)
afterthe
CLC
R<10
mL/min
(n=4)
CLC
R:8.67
±2.31
mL/min
UFflow:27.1±7.8mL/min
Sc:PIP
0.42
±0.25;TZ0.76
±0.26
Cmax:PIP
365.6±232.3;TZ
38.4±
13.4mg/L
t1/2:PIP
7.8±4.2;TZ
7.9±3.0h
Cls:PIP
50.0±53.0;TZ50.4±
38.3mL/min
Hem
ofiltratio
nCl:PIP11.45±6.51;
TZ20.9±12.6mL/min
AUC:PIP
76143±49,748;TZ23218±
Thecontrib
utionof
thehemofiltratio
nclearanceto
thetotalclearance
increasedwith
thedegree
ofrenal
insufficiency.Correctdo
sesof
these
drug
sshou
ldtake
into
accoun
tthis
observationto
avoidclinicalfailures
dueto
unde
rdosing
Forb
othdrug
s,sig
nificantdifferences
weredo
cumentedinthemajority
ofthePK
parameterswhenpatientswith
CLCR
>50
mL/minwerecomparedto
patientswith
CLCR
≤10
mL/min
Veiga and Paiva Critical Care (2018) 22:233 Page 11 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
administrationof
theantib
iotic.Tim
e0was
considered
justbe
fore
the
beginn
ingof
the20-min
infusion
27,943
mg.h/L
Vd:PIP
21.0±11.7;TZ18.9±7.1l
10<CLC
R>50
mL/min
(n=5)
CLC
R25.20±7.73
mL/min
UFflow:30.3±4.3mL/min
Sc:PIP
0.38
±0.37;TZ0.73
±0.32
Cmax:PIP
244.5±122.1;TZ
31.5±
5.1mg/L
t1/2:PIP
4.2±2.3;TZ
4.1±0.9h
Cls:PIP
90.6±29.9;TZ68.2±
26.2mL/min
Hem
ofiltratio
nCl:PIP12.2±13.2;TZ
21.9±9.6mL/min
AUC:PIP
45445±25,525;TZ23218±
27,943
mg.h/L
Vd:PIP
26.8±19.8;TZ21.6±3.0l.
CLC
R>50
mL/min
(n=5)
CLC
R:82.40±20.03mL/min
UFflow:20.0±7.5mL/min
Sc:PIP
0.23
±0.07;TZ0.86
±0.30
Cmax:PIP
160.6±93.2;TZ15.7±
6.6mg/L
t1/2:PIP
2.6±0.8
TZ5.0±3.9h
Cls:PIP
265.2±152.2;TZ
180.1±
73.9mL/min
Hem
ofiltratio
nCl:PIP4.8±3.3;TZ
19.6±15.3mL/min
AUC:PIP
17,328
±11,134;TZ2098
±1030
mg.h/L
Vd:PIP
44.9±20.4;TZ60.3±34.6l
t>MIC90
obtained
were100%
forall
thepathog
ensin
patientswith
creatin
ineclearance<10
mL/min.In
patientswith
acreatin
ineclearance
betw
een10
and50
mL/min,t>
MIC90
was
100%
forpathog
enswith
MIC90
≤32,b
uton
ly50%
for
microorganism
swith
anMIC90
of64.
How
ever,inpatientswith
creatin
ine
clearance>50
mL/min,aspiperacillin
elim
inationwas
faster,t>MIC90
was
only55.5%and16.6%forp
atho
gens
with
MIC90
values
of32
and
64,respectively
Theob
served
sievingcoefficient
ofpipe
racillinandtazobactam
plus
the
effluen
tam
ount
gave
arelevant
extracorpo
realclearanceon
lyin
the
severe
renalimpairm
entgrou
p,with
morethan
25%
oftotalclearance
for
both
drug
sTo
increase
thet>
MIC90
inde
x,pipe
racillin-tazobactam
combinatio
nevery4hcouldbe
abe
tter
dosage
regimen
inpatientspresen
tingCLC
R>50
mL/min
Islaet
al.[79]
Tode
scrib
ethePK
ofmerop
enem
incritically
illpatientswith
different
degreesof
renalimpairm
ent
unde
rgoing
CVV
HFor
CVV
HD
Merop
enem
Prospe
ctive,ob
servationalstudy
20adultICUpatientson
CVV
HFor
CVV
HDF
Group
edinto
3catego
riesaccording
totherenalfun
ction:
7with
severe
failure,C
lCrless
than
10mL/min
Nosign
ificant
differences
depe
nding
onrenalimpairm
entwerefoun
din
theSc.N
odifferences
werefoun
din
theSc
obtained
byCVV
HFandthe
Saob
tained
byCVV
HD;b
oth
mem
branes
show
edasimilar
Differen
cesin
merop
enem
PKin
critically
illpatientsun
dergoing
CRR
Twith
different
degreesof
renal
impairm
enthave
been
observed
,andthey
shou
ldbe
takeninto
accoun
twhe
ndo
sing
critically
ill
Veiga and Paiva Critical Care (2018) 22:233 Page 12 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
(group
I);7with
mod
eratefailure,
ClCr10
to50
mL/min
(group
II);and
6with
ClCrgreaterthan
50mL/min
(group
III)
Bloo
dflow
rate
110–220mL/min;
dialysateflow
rate
500or
1000
mL/
min;ultrafiltrate
800–2500
mL/h
Patientsreceived
500,1000,or
2000
mgof
merop
enem
intraven
ouslyevery6or
8hand
infusedover
20min
Bloo
dwas
obtained
from
aprefilter
device
immed
iatelybe
fore
dosing
,at
theen
dof
theinfusion
,and
at20,
30,and
45min
and1,3,and6h
afterthebe
ginn
ingof
theinfusion
.Ano
ther
samplewas
collected
8h
afterthebe
ginn
ingof
theinfusion
inpatientsto
who
mmerop
enem
was
administeredevery8h
Simultane
ously,dialysate-ultrafiltrate
samples
weretakendirectlyfro
mthe
dialysate-ultrafiltrate
device
perm
eabilityto
merop
enem
Totalclearance
was
sign
ificantly
high
erin
grou
pIIIthan
intheothe
rtw
ogrou
ps.Thisfinding
couldbe
attributableto
thelower
t1/2
(1.51±0.52
hin
grou
pIIIversus
2.73
±0.68
hand3.72
±0.82
hin
grou
psIIandI,respectively)
andto
thehigh
Vdob
served
inthose
patients(1.31±0.90
L/kg
ingrou
pIII,
0.37
±0.10
L/kg
ingrou
pII,and
0.57
±0.29
L/kg
ingrou
pI)
Thecontrib
utionof
CRR
Tto
total
clearancediminishe
din
theextent
that
CLC
Rincreased.
Alth
ough
there
wereno
statisticallysign
ificant
differences
betw
eengrou
psIand
II,Cl CRRTwas
sign
ificantlylower
ingrou
pIII
Ingrou
pIp
atients,trou
ghplasma
concen
trations
wereabove4μg
/mL,
with
theexceptionof
theon
lypatient
who
received
500mg/8h.
Ingrou
pII,plasmaconcen
trations
were
above2μg
/mLdu
ringtheen
tire
dose
interval,excep
tin
thepatient
towho
m1000
mg/8hwas
administered
Inspite
ofthehigh
erdo
sesthe
patientsof
grou
pIIIreceived
,4of
6patientsshow
edconcen
trations
below
0.5μg
/mL
patients
Inthosepatientswith
norenal
impairm
enttheriskof
unde
rdosing
andclinicalfailure
isim
portant,and
theadministrationof
merop
enem
2000
mgevery8hdidno
treach
plasmalevelsto
ensure
adeq
uate
T>MIC
values
againstmanybacteria
Ulldem
olins
etal.[80]
Tode
scrib
ethePKsof
merop
enem
incritically
illpatientswith
septic
shockandCRR
T,to
iden
tifythe
sourcesof
PKvariabilityin
these
patients,andto
perfo
rmdifferent
dosing
simulations
toassess
their
prob
ability
oftarget
attainmen
tby
MIC,inorde
rto
provideem
pirical
dosing
recommen
datio
nsbasedon
clinicalcharacteristics
Merop
enem
Prospe
ctive,ob
servational,
multicen
trestud
y30
adultICUpatientswith
septic
shockandCRR
T,either
CVV
HF(n
=4)
orCVV
HDF(n
=26)
Patientswereprescribed
merop
enem
at500mgq1
2hover
30min
(n=1);500
mgq8
hover
30min
(n=2)
oras
a3-hinfusion
(n=3);500
mgq6
has
a3-hinfusion
(n=1);1000mg
q12h
over
30min
(n=6)
asa3-h
infusion
(n=1)
oras
a4-hinfusion
(n=1);1000mgq8
hover
30min
(n=8)
asa3-hinfusion
(n=5)
oras
a4h-infusion
(n=1);or2000
mg
q8hover
30min
(n=1)
Bloo
dsamples
werecollected
at24
hof
CRR
Tandmerop
enem
Thestud
ymod
elfailedto
iden
tify
CRR
Tintensity
tobe
asign
ificant
mod
ifier
ofmerop
enem
CL,which
may
lead
tothehypo
thesisthat
even
thelowestCRR
Tintensities
stud
iedmay
been
ough
tomaxim
ize
merop
enem
clearanceandthat
high
erintensities
may
addlittle
tototalm
erop
enem
CL
Therewereno
differences
betw
een
CRR
Ttechniqu
es,likelybe
causeof
theun
derrep
resentationof
CVV
HF
(4ou
tof
30patients)in
thestud
ypo
pulatio
nFortheattainmen
tof
aPD
target
of100%
oftheT>MIC,fixed
doses
wou
ldbe
requ
ired,
depe
ndingon
theMIC
ofthebacteria,b
utthe
infusion
timewou
ldde
pend
on
Popu
latio
nPK
mod
elsuccessfully
iden
tifiedresidu
aldiuresisto
bea
mod
ifier
oftotalm
erop
enem
CL
CRR
Tintensity
didno
tsign
ificantly
mod
ifymerop
enem
CL,forwhich
dose
adjustmen
tsbasedon
intensity
seem
tobe
unne
cessary
Given
acertainMIC,sim
ulations
show
edthat
merop
enem
dose
titratio
nconsideringresidu
aldiuresis
was
advantageous
forthe
attainment
of100%
oftheT>MIC
asaPD
target.
Ifclassic
PDtargets(40%
oftheT>
MIC)w
eretargeted,a
standard
dose
of500mgq8has
a30-m
inbo
lus
wou
ldbe
sufficient,regardlessof
urineou
tput
Veiga and Paiva Critical Care (2018) 22:233 Page 13 of 34

Table
1PK/PDstud
iesof
beta-lactam
sin
patientsun
dergoing
CRRT(Con
tinued)
Stud
yEndp
oints
Antibiotic
Designandtype
ofCRR
TResults
Con
clusions
therapy.Forbo
lussampling,
6samples
werecollected
at10
min
pre-do
se;at0,15,and
60min
and
betw
een3and6haftertheen
dof
theinfusion
;and
justbe
fore
thene
xtdo
se.For
extend
edinfusio
nsampling,
samples
werecollected
at10
min
pre-do
se;0,60,and120minafterthe
endof
theinfusio
n;andjustbefore
thenextdo
seCRR
Tsettings:the
med
ianintensity
onthedayof
thestud
ywas
34.7mL/kg/h
(rang
e,18.7to
60.1mL/kg/h),andthemed
ian
bloo
dflow
was
200mL/min
(rang
e,130to
250mL/min)
residu
aldiuresis:o
ligo-anuricpatients
wou
ldbe
nefit
from
a30-m
inbo
lus,
whilea3-hextend
edinfusion
wou
ldbe
moreapprop
riate
forthose
patientswith
preserveddiuresis
Fortheattainmen
tof
theclassicPD
target
forcarbapen
ems(40%
ofthe
T>MIC),astandard
dose
of500mg
q8has
abo
lusover
30min
wou
ldbe
sufficien
tforallcases
Fortheattainmen
tof
amore
aggressive
target,suchas
aCmin/
MIC
ratio
of5,do
sesof
1000
mg
q8has
a3-hinfusion
orhigh
erwou
ldbe
requ
ired
Boum
anet
al.
[81]
Tocompare
theob
served
Cl CVVHF
(calculatedfro
mmeasureddata)and
thepred
ictedCl CVVHF(calculated
from
theF U
P)
Tode
term
inewhe
ther
dose
adjustmen
taccordingto
the
pred
ictedCVV
Hremovalprovides
anestim
ateas
reliableas
that
according
totheob
served
CVV
Hremoval
Amoxicillin
Ceftazidime
Flucloxacillin
Prospe
ctive,ob
servationalstudy
45adultICUoligoanu
ricpatientson
CVV
HF
Duringthesamplingpe
riodasing
leantim
icrobialdrug
was
administered
to31
patients,tw
odrug
sto
9patients,andacombinatio
nof
3to
5Dosages
were:am
oxicilin1000
mg
q6h;
ceftazidim
e1000
mgq6
-12h;
flucloxacillin
2000
mgq4
-6h
Bloo
dflow
rate
was
150mL/min
and
warmed
substitutionfluidswere
administeredin
pred
ilutio
nat
aflow
rate
of2000
mL/h.
Ifane
gativefluid
balancewas
requ
ired,theultrafiltration
flow
was
increasedan
dthe
substitutionflo
wwas
constant
Bloo
dsamples
werecollected
from
theafferent
(pre-hem
ofilter)and
efferent
(post-he
mofilter)lineof
the
extracorpo
realcircuitandfro
mthe
ultrafiltrate
line.Samples
were
collected
at2,4,and6hforagen
tsgivenevery6h;at
2,4,and8hfor
agen
tsgivenevery8h;andat
2,6,
and10
hforagen
tsgivenevery12
or24
h
Allthestud
iedagen
tswereeasily
filtered(SC>0.7)
with
theexception
offlucloxacillin
Therewas
ahigh
interin
dividu
alvariabilityin
theSC
values
ofthe
stud
ieddrug
s,in
particular
for
ceftazidim
eandto
alesser
degree
foram
oxycillin
andflucloxacillin
Thecorrelationbe
tweenob
served
andpred
ictedclearancewas
sign
ificant
(P=0.003)
onlywhe
nall
drug
swerecombine
d,no
tforthe
individu
alantim
icrobialdrug
s.Despite
theno
nsignificant
correlation,
thedifferencebe
tween
pred
ictedandob
served
clearance
foralld
rugs
was
small,with
the
exceptionof
ceftazidim
e
Therewas
nosign
ificant
correlation
betw
eenpred
ictedandob
served
CVV
Hdrug
removal.H
owever,for
clinicalpractice,do
seadjustmen
taccordingto
thepred
ictedCVV
Hremovalprovides
amorereliable
estim
atethan
that
accordingto
the
observed
CVV
Hremoval
Alth
ough
thereisinterpatient
variabilitybe
tweentheob
served
and
pred
ictedCl CVVHFvalues
forsome
antib
iotics,its
effect
ondo
sing
strategies
isno
tne
cessarily
clinically
relevant:flucloxacillin
hasan
impo
rtantno
n-renalelim
ination
route,andthereforetheFrCVVHF
valuewas
extrem
elylow
andno
taffected
bythewideinterin
dividu
alvariatio
nin
observed
Cl CVVHF.Also,
widetherapeutic
rang
e,such
aswith
ceftazidim
e,makes
itsafe
tousethe
pred
ictedClCVVHFford
oseadjustment
AKI
acutekidn
eyinjury,A
UCarea
unde
rthecurve,
ClCr
creatin
ineclearance,
CLssystem
icclearance,
Cldialysisextracorpo
real
clearance,
Cmax
maxim
alconcen
tration,
Cmin
minim
alconcen
tration,
CRRT
continuo
usrena
lrep
lacemen
ttherap
y,CV
VHFcontinuo
usveno
us-ven
oushe
mofiltratio
n,CV
VHDcontinuo
usveno
us-ven
ousha
emod
ialysis,CV
VHDFcontinuo
usveno
-ven
ous
hemod
iafiltration,
Fupun
boun
dfractio
nof
adrug
,MIC
minim
alinhibitory
concen
tration,
PTAprob
ability
oftarget
attainmen
t,Ssaturatio
ncoefficient,Scsievingcoefficient,t1/2ha
lf-life,
T>MIC
timeab
oveMIC,U
FRultrafiltratio
nrate,V
dvo
lume
ofdistrib
ution
Veiga and Paiva Critical Care (2018) 22:233 Page 14 of 34

Table
2PK/PDstud
iesof
beta-lactam
sin
patientswith
sustaine
dlow-efficien
cydialysisor
extend
eddaily
dialysis
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Kielstein
etal.[82]
Toevaluate
PKof
merop
enem
incritically
illpatientswith
renal
failure
unde
rgoing
EDD
Merop
enem
Prospe
ctiveclinicalstud
yAdu
ltICUpatientswith
anuricacute
renalfailure
beingtreatedwith
EDD
andreceivingmerop
enem
(n=10)
Merop
enem
administeredas
1gdo
se,
asan
intraven
ousinfusion
over
ape
riodof
30mins,6hbe
fore
EDD
was
started
Bloo
dsamples
weredraw
nbe
fore
administrationof
thedrug
;at0.5,
1,2,4,and6hafterits
administration;
before
EDD;d
uringED
D,attim
epo
ints2,4,and6h;at
theen
dof
EDD;and
at0.5,1,3,and8hafter
EDD.A
ddition
albloo
dsamples
were
draw
npre-
andpo
st-dialyzerin
orde
rto
calculatethedialyzer
clearance
Theaverage(m
ean±SD
)dialysistim
edu
ringthestud
ywas
480±6min,
andmeanbloo
dandcoun
tercurrent
dialysateflow
was
160±3mL/min
T1/2offwas
8.7h[4.7–30]
T1/2on
was
3.7h[2.1–4.7]
Vdwas
0.72
L/kg
[0.35–2.78]
CLoff5.01
L/h[2.44–11.15]
CLdialw
as2.3L/h[0.7–3.7]
(estim
ated
from
thedrug
amou
ntrecoveredin
thedialysate)
and5.1L/h[4.3–5.7](estim
ated
from
drug
concen
trations
before
andafter
applicationof
thedialysismem
brane)
Merop
enem
issign
ificantlyelim
inated
byED
D.C
omparedwith
PKresults
intheliteratureforinterm
itten
tdialysis
andCRRT,do
sing
regimen
scann
otbe
used
forcritically
illsepticpatients
with
renalfailure
beingtreated
with
EDD
EDDelim
inates
merop
enem
atleast
toan
extent
similarto
CVVH.Thu
s,ph
ysicians
runtheriskof
unde
rdosing.
Ado
seof
0.5to
1.0gmerop
enem
every8hisrecommen
ded.
Theexact
dose
shou
ldbe
tailoredaccordingto
weigh
tandseverityof
illne
ssas
well
asto
thecurren
tMIC
againstthe
incrim
inated
bacteria.W
hene
ver
possible,the
rape
uticdrug
mon
itorin
gshou
ldbe
perfo
rmed
Lorenzen
etal.[83]
Theaimsof
thisstud
ywereto
evaluate
thePK
ofam
picillin/sulbactam
incritically
illpatientswith
AKI
unde
rgoing
extend
eddialysisandto
establishado
sing
recommen
datio
nfor
thistreatm
entmetho
d
Ampicilin-sulbactam
Prospe
ctive,op
en-labe
l,ob
servationalstudy
12adultICUpatientswith
anuricAKI
PKafterasing
ledo
seof
ampicillin/
sulbactam
(2g/1g)
over
ape
riodof
30min
was
obtained
in12
patients.
Multip
le-dosePK
after4days
oftw
ice-
daily
ampicillin/sulbactam
(2g/1g)
was
obtained
inthreepatients.The
averagedialysistim
ewas
442±77
min
andmeanbloo
dandcoun
ter
curren
tdialysateflow
was
162±6
mL/min,resultin
gin
ameanurea
redu
ctionratio
of50.1%
±2.7%
.ED
was
started3haftertheen
dof
the
ampicillin/sulbactam
infusion
Cmax
280.9±174.9mg/L
Tmax
0.5h
AUClast847.5±499.5mg.h/L
t1/2
2.8±0.8
Vd(L)13.1±11.1
CLtot
61.1±55.2mL/min
CLdial80.1±7.7mL/min
Ampicillin/sulbactam
iselim
inated
byED
Current
dosing
recommen
datio
nsfro
mpatientsun
dergoing
IHD(3
gevery24
h)wou
ldcauseasign
ificant
unde
rdosingof
thedrug
inpatients
treatedwith
EDAmpicillin/sulbactam
concen
trations
exceed
edMIC90
values
ofEnterobacteriaceae,suchas
Escherichia
colior
Klebsiella
pneumon
iae(M
IC90
<2.0mg/L)
orEnterococcus
faecalis
(MIC90
=2.0mg/L),o
nlyfor8h
(app
roximately30%
ofthedo
sing
intervalforpatientson
interm
itten
the
mod
ialysis)afterstartof
infusion
.Ado
sage
of3gevery12
hin
patients
unde
rgoing
EDdo
esno
tlead
toa
sign
ificant
accumulationof
thedrug
Burkhardt
etal.[84]
Toevaluate
PKof
ertape
nem,w
ithon
ce-dailydo
sing
,incritically
illpatients
with
anuricacuterenalfailure
unde
rgo-
ingED
D
Ertape
nem
Prospe
ctive,op
en-labe
lstudy
6adultICUpatientsun
dergoing
EDD
treatedwith
1gertape
nem
asa
sing
leintraven
ousdo
seBloo
dsamples
werecollected
before
ertape
nem
infusion
and0.5,1,2,4,6,
8haftertheen
dof
theinfusion
and
also
2,4,6,and8hafterthestartof
EDD.A
ddition
albloo
dsamples
were
draw
npre-
andpo
st-dialysisin
orde
rto
calculatethedialyzer
clearance.
Tostud
ypo
st-EDDPK,sam
ples
were
draw
n0.5,1,3,and8hafterthe
endof
EDD
Cmax
81.3±12.1mg/L
AUC0-inf687.4±212.0mg.h/L
T1/2off18.9±5.4h
T1/2on
6.7±0.4h
Vd(L)15.9±3.2
CLoff19.3±11.4mL/min
CLdial49.5±10.9mL/min
T>MIC
was
100%
(MIC90
≤1mg/L)
and85%
(MIC90
≤2mg/L)
1gertape
nem
perdayto
critically
illpatientswith
ARF
intheICUthat
unde
rgoED
Disne
cessaryto
ensure
optim
alfre
econcen
trations
ofertape
nem.A
redu
ctionof
thedo
seisno
tsupp
ortedby
ourdata.Further
dosing
recommen
datio
nsforpatients
with
renalfailure
intheICUtreated
with
such
effectivemod
esof
renal
replacem
enttherapyshou
ldbe
develope
dto
avoidexcess
mortality
dueto
unde
r-do
sing
oflife-saving
med
ication
Veiga and Paiva Critical Care (2018) 22:233 Page 15 of 34

Table
2PK/PDstud
iesof
beta-lactam
sin
patientswith
sustaine
dlow-efficien
cydialysisor
extend
eddaily
dialysis(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Tamme
etal.[85]
Tode
scrib
ethePK
ofpipe
racillinand
tazobactam
durin
gextend
edhigh
volumehe
mod
iafiltrationto
define
optim
aldo
sing
Pipe
racilin-
tazobactam
Prospe
ctive,ob
servationalstudy
10adultICUpatientswith
sepsis
andAKIrequ
iring
CRR
TAsing
ledo
seof
4000
mgof
pipe
racillinand500mgtazobactam
was
administeredas
a30-m
inintraven
ousinfusion
1hafterthe
startof
HVH
DF
Bloo
dsamples
of4mLwerecollected
before
andim
med
iatelyaftertheen
dof
pipe
racillin/tazobactam
infusion
and60,90,120,150,180,
240,300,360,420,and480min
afterthestartof
drug
administration
Theplasmaconcen
tration–
time
profilesof
pipe
racillinandespe
cially
tazobactam
demon
stratedhigh
interin
dividu
alvariability
Forpipe
racilin
CL(rang
e)6.9L/h(6.1–7.9)
Vdcentralcom
partmen
t(rang
e)9.0L(7.4–11.0)
Vdpe
riphe
ralcom
partmen
t(rang
e)11.2L(8.9–14.2)
Fortazobactam
CL(rang
e)5.1L/h(4.1–6.3)
Vdcentralcom
partmen
t(rang
e)8.6L(6.9–10.7)
Vdpe
riphe
ralcom
partmen
t(rang
e)8.9L(6.6–12.0)
Using
Mon
teCarlo
simulation,
the
prob
ability
of100%
fT>MIC
target
attainmen
tforpipe
racillin/tazobactam
4.5gdo
sedevery6and8has
4-h
infusion
were88.6%
and61.0%,
respectively,forMIC
16mg/l
App
licationof
extend
edHVH
DFforthe
treatm
entof
AKI
insepticshock
patientsresults
inconsiderable
clearanceof
pipe
racillinand
tazobactam
Pipe
racillin/tazobactam
dosesof
4.5g,
administeredevery8has
0.5-hinfusion
durin
gHVH
DF,en
suredmorethan
80%
prob
ability
ofattainingthe50%
fT>MIC
target
for
interm
ediatelysuscep
tiblebacteria(M
IC16
mg/l)
Whileaimingfor100%
fT>MIC
of16
mg/l,increasing
dosesto
4.5gevery6handprolon
ging
the
infusion
timeto
4hwou
ldbe
necessary
AKI
acutekidn
eyinjury,A
RFacuterena
lfailure,C
Ldiald
ialysisclearance,CLoffdrug
clearancewith
outdialysis,EDDextend
edda
ilydialysis,ICU
intensivecare
unit,
SDstan
dard
deviation,
SLED
sustaine
dlow-efficiencydialysis,T1/2o
ffha
lf-lifebe
fore/after
EDD,T1/2o
nha
lf-lifedu
ringED
D,V
dvo
lumeof
distrib
ution
Veiga and Paiva Critical Care (2018) 22:233 Page 16 of 34

Table
3PK/PDstud
iesof
beta-lactam
sin
patientswith
extracorpo
realmem
braneoxygen
ation
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Don
adello
etal.[100]
Toinvestigatewhe
ther
ECMOcouldalterthe
pharmacokineticsof
merop
enem
andpipe
racillin/
tazobactam
inICUpatients
Merop
enem
Pipe
racilin/
tazobactam
Retrospe
ctive,case-con
trol
stud
yin
67ICUpatients
Antibioticsdaily
dosing
was
done
accordingto
renald
osing
Beta-lactam
plasmaconcen
trations
weremeasuredT2
andjustbe
fore
administrationof
thesubseq
uent
dose
T0TD
Mresults
inEC
MOpatients
(VVor
VA)werematched
(1:1)to
TDM
results
ofno
n-EC
MOpatients
(total41
TDM
matches)accordingto
thefollowingcriteria:d
rugregimen
;renalfun
ction(sam
eClCror,ifon
CRR
T,sameCRR
Tintensity
with
anacceptable
differenceof
10%);totalb
odyweigh
t;SO
FAscoreat
thetim
eof
treatm
ent
initiation;
age
Forbo
thantib
iotics,therewerenu
merical
differences
butwith
nostatisticalsign
ificance
inV d,t1/2andCLbe
tweenEC
MOpatients
andcontrols
Theprop
ortio
nsof
insufficien
t(13/41
vs12/41),
adeq
uate
(15/41
vs19/41),and
excessive
(13/41
vs10/41)
drug
concen
trations
were
similarin
ECMOandcontrolp
atients
PKparametersandTD
Mresults
were
notsign
ificantlyalteredin
ECMOpatients
comparedwith
controlICUpatients
Alm
ost30%
oftheoverallTDM
results
were
associated
with
insufficien
tantib
iotic
concen
trations
toop
timallytreatP.aerugino
sa
Shekar
etal.[101]
Tode
scrib
esing
le-dosemerop
ene
mPK
durin
gEC
MOusing
critically
illpatientswith
sepsis
andno
treceivingEC
MO
ascontrols
Merop
enem
Ope
n-labe
l,de
scrip
tive,
matched
-coh
ortPK
stud
yAdu
ltICUpatientson
ECMO(noRR
Tn=6;on
RRTn=5)
andcontrols
(norenald
ysfunctio
nn=5;on
RRTn=5)
Merop
enem
dosesin
ECMO:
1g8/8h(n
=8);1.5g8/8h(n
=2)
and2gbo
lus;and1g8/8h(n
=1)
Con
trols:1.5gbo
lusand1g8/8h
(norenald
ysfunctio
n);1
g8/8h
Con
trolsvs
ECMO
Cmax:65.4(58.7–74.4)vs
55.3(37.8–60.4)mg/L
Cmin:4.2(0.0–5.7)vs
7.2(4.0–17.2)
mg/L
Vd:0.45±0.17
vs0.41
±0.13
L/kg,P
=0.21
Clearance:7.9±5.9vs
11.7±6.5L/h,P=0.18
ECMOpatients,trou
ghconcen
trations
>2mg/L
wereachieved
inallp
atients.Throug
hconcen
trations
>8mg/L(targe
tingless
suscep
tiblemicroorganism
s)wereachieved
inon
ly8ou
tof
11patients,5of
them
being
onRR
T
Standard
merop
enem
dosing
(1gIV
8-ho
urly)as
aninterm
itten
tbo
lusinfusion
inEC
MOpatients
islikelyto
resultin
drug
concen
trations
sufficien
tto
treathigh
lysuscep
tibleGram-neg
ative
pathog
ens
How
ever,w
hentreatin
gless
suscep
tibleP.
aerugino
sa(M
IC90
8mg/L)
andAcinetobacter
species(M
IC90
16mg/L)
high
ermerop
enem
dosesmay
have
tobe
considered
Welsch
etal.[102]
Torepo
rtthecasesof
two
patientson
VVEC
MOfor
refractoryARD
Sfollowinglung
transplantationandtreated
empiricallywith
imipen
em
Imipen
emCaserepo
rtIm
ipen
em1gevery6h
Serum
andmini-BALsamples
(native
andtransplant
lung
)collected
atsteady
stateafter2days
oftherapyim
med
i-atelybe
fore
thefifth
drug
dose
Enteroba
ctercloa
caewas
isolated
from
therespiratory
sampleof
patient
1and
Klebsiella
pneumon
iaewas
isolated
from
therespiratory
sampleof
patient
2MIC
ofthetw
oisolated
strainswere
0.125and0.25
mg/L,respectively
BALconcen
trations
were
unde
tectable(<
0.5mg/L)
Serum
T>MIC
ofbo
thmicroorganism
swas
100%
Con
side
ringmoreresistantmicroorganism
s,such
asP.aerugino
sawith
MIC
>2mg/L,theprob
ability
ofachievingafractionaltim
eaboveMIC
>50%
or100%
was
also
high
Therewas
greatvariabilityin
theresidu
alserum
concen
trationof
imipen
embe
tweenthetw
opatients
Anelevated
dosing
regimen
(4g/24
h)ismore
likelyto
optim
izedrug
expo
sure,and
therapeutic
drug
mon
itorin
gisrecommen
ded
ARD
Sacuterespira
tory
distress
synd
rome,
BALbron
chial-a
lveo
larlavage
,CLclearance,ClCr
creatin
ineclearance,
CRRT
continuo
usrena
lrep
lacemen
ttherap
y,EC
MOextracorpo
real
mem
bran
eoxyg
enation,
ICUintensivecare
unit,
MIC
minim
alinhibitory
concen
tration,
RRTrena
lrep
lacemen
ttherap
y,SO
FAsequ
entia
lorgan
failure
assessmen
t,T>MIC
percen
tage
oftim
eab
oveminim
alinhibitory
concen
tration,
T00hafterthestartof
infusion
,T22hafterthestartof
infusion
,TDM
therap
eutic
drug
mon
itorin
g,V d
volumeof
distrib
ution,
veno
us-arterial,VV
veno
us-ven
ous
Veiga and Paiva Critical Care (2018) 22:233 Page 17 of 34

However results are conflicting concerning decreasedmortality and bacteriological and clinical cure rates [144].A sub-analysis from the DALI study compared intermit-tent bolus vs prolonged infusions of beta-lactams in pa-tients with respiratory infection and concluded thatpatients receiving beta-lactams via prolonged infusiondemonstrated significantly better 30-day survival [145].Falagas et al. [114] conducted a meta-analysis of 14
studies comparing continuous and short-term infusionof carbapenems and piperacilin-tazobactam, involving1229 patients. Mortality was lower among patients re-ceiving extended or continuous infusion of carbapenemsor piperacillin/tazobactam compared to those receivingshort-term infusion (risk ratio (RR) 0.59, 95% confidenceinterval (CI) 0.41–0.83). Patients with pneumonia whoreceived extended or continuous infusion had lowermortality than those receiving short-term infusion (RR0.50, 95% CI 0.26–0.96) [114].An interesting retrospective study by Huang et al. [120]
reviewed 68 neurosurgical patients with post-operativeintracranial infections treated with 4 g/day cefepime over24 h as a continuous infusion (CI; n = 34) or 2 g every 12 has intermittent infusion (II; n = 34). CI controlled the intra-cranial infection more rapidly and effectively than II (6.6 ±1.9 days vs 7.8 ± 2.6 days; P = 0.036). PD targets were moreachievable with CI: for plasma cefepime concentrations,the percentage fT >MIC in the CI group was higher thanin the II group (for MICs of 8 μg/mL, 100% vs 75%, re-spectively). For cerebral spinal fluid (CSF) cefepime con-centrations, the percentage fT >MIC in the CI group washigher than in the II group (for MICs of 4 μg/mL and8 μg/mL, 83.3% and 75% vs 25% and 0%, respectively)[120].De Waele et al. [27] reviewed 343 patients from 68 ICUs
across ten countries and concluded that use of intermit-tent infusion was the most significant factor associatedwith target non-attainment, for both 50% and 100% fT >MIC. Other risk factors for target non-attainment wereClCr, recent surgery, and timing from initial antibiotictherapy and sampling. However, the type of infusion wassuch a significant covariate in the model that it eliminatedthe effects of other variables [27].
Site of infectionUsually drug concentrations in blood are used to deter-mine PD parameters, such as percentage of time druglevels exceed the MIC and peak drug AUC/MIC level,due to the relative accessibility of this body fluid. Be-cause infection usually occurs at extravascular sites, theuse of drug concentrations in blood is only satisfactory ifblood levels are an adequate surrogate for levels at thesite of infection [13]. In septic shock, blood misdistribu-tion in the microcirculation might decrease antibioticconcentration at the infection site [1].
Boyadjiev et al. [146] studied ertapenem penetrationinto muscle in mechanically ventilated patients and con-cluded that average muscle free-ertapenem concentra-tions were above the MIC values of targeted pathogensexcept in a few patients. Karjagin et al. [147] evaluatedthe PK/PD relations of meropenem in plasma and peri-toneal fluid by microdialysis and showed that area underthe concentration–time curve was lower in peritonealfluid than in plasma, concluding that in patients with se-vere peritonitis associated with septic shock, a dosingregimen of 1 g infused over 20 min every 8 h is sufficientagainst susceptible bacteria, but not always against inter-mediately susceptible bacteria. Also, beta-lactam PK isvariable between plasma and subcutaneous interstitialfluid in septic patients [148]. Thus, prediction of micro-biological outcome based on concentrations in plasmaresults in overestimation of antimicrobial activity at thesite of infection.Special anatomic barriers (e.g., brain, eye, and pros-
tate) can result in drug levels being much lower thanfree drug levels in plasma [13]. The combination of tightjunctions and active transport systems that form theblood–brain barrier creates a substantial impediment tothe penetration of most antibiotics into the CSF. How-ever, the presence of inflammation within the meningessignificantly alters the permeability of the blood–brainbarrier, increasing CSF exposure for the majority of anti-biotics [20]. For meningitis, CSF levels are appropriatefor determination of PD parameters.Very few studies have investigated PK/PD issues in the
CSF (Table 4). Five case reports, one randomized clinicaltrial in a paediatric population, and three prospectiveobservational studies found good probability of target at-tainment for susceptible strains but standard dosing maynot be optimal for less susceptible strains. Prolongedand/or continuous infusion is of benefit in the attemptto achieve PD targets. No data regarding intermittentversus continuous CSF ventricular drainage were foundand conceptually these two types of drainage may alterthe beta-lactam PK profile.There is very sparse data on possible surrogate central
nervous system penetration factors for beta-lactams, sono conclusions can be made. We recommend to usehigher than standard dosing, preferably with continuousor prolonged infusions, especially when treating less sus-ceptible bacterial strains. Toxicity did not increase at in-creased doses. Finally, none of these studies addressedclinical outcome.Though there are PK models of plasma concentrations
of beta-lactams specifically for the critically ill popula-tion with pneumonia, it is suggested that epithelial liningfluid (ELF) concentrations are important determinantsof efficacy of treatment of bacterial pneumonia.ELF-to-serum penetration ratios may vary widely among
Veiga and Paiva Critical Care (2018) 22:233 Page 18 of 34

Table
4PK/PDstud
iesof
beta-lactam
sin
cerebralspinalfluid
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Goldw
ater
etal.[149]
Toevaluate
antib
iotic
CSF
pene
trationand
antim
icrobialefficacy
Ceftriaxone
Cefotaxim
e
Rand
omised
,ope
n,comparativetrial
120paed
iatricpatientswith
men
ingitis,33with
repe
ated
lumbarpu
ncture
atdifferent
times
CRO
100mg/kg
once
daily;
CTX
50mg/kg
every6h
All33
repe
ated
lumbarpu
nctures
weresterile
ThelowestCSF
levelrecorde
d(0.45μg
/mLforCTX)was
45tim
estheMIC
(0.01μg
/mL).The
high
est
levels(24–35
μg/m
LforCRO
)were
upto
8750
times
theMIC
ofthe
patient’scausativeorganism
Antibiotic
levelsachieved
inCSF
weretherapeutic,b
eing
wellabo
vetheMIC
forallo
rganisms
encoun
tered
CSF
cellcoun
thadno
apparent
influen
ceon
antib
iotic
levels
Lonsdale
etal.[150]
Toillustrateissues
inthe
managem
entof
CSF
antib
iotic
concen
trations
Merop
enem
Caserepo
rtNeurosurgicalpatient
with
externalventricular
drain-relatedventriculitis
Ade
quateplasmathroug
hconcen
trations
achievableafterincreasing
dosing
to2g,
four
times
daily
CSF
concen
trations
ofmerop
enem
weresimilarto
thoseseen
inplasma
Therewerevariatio
nsin
CSF
drug
pene
tration
Achieving
CSF
therapeutic
antib
acterialcon
centratio
nsin
neurosurgicalcriticallyillpatientsis
difficult
Standard
antib
acterialp
rescrip
tion
ispo
tentially
flawed
inthissetting,
sugg
estin
gthene
edfortherapeutic
drug
mon
itorin
g
Abd
ul-Aziz
etal.[151]
Torepo
rtthedifficulty
inachieving
andmaintaining
target
antib
iotic
expo
sure
incritically
illpatients
with
deep
-seede
dinfections
Flucloxacillin
Caserepo
rtCriticalcare
patient
with
CNSinfection
Trou
ghplasmaconcen
trations
were
below
theMIC;C
SFconcen
trations
wereun
detectable(interm
itten
tdo
ses2g6/6h)
With
continuo
usinfusion
and
increasing
thedo
seto
20gdaily,
theplasmaandCSF
levelsbe
camede
tectable,albeit
lower
than
thepred
efined
targets
Antibiotic
pharmacokineticsmay
besign
ificantlyalteredin
critically
illpatients
App
lyingcontinuo
usinfusion
and
mon
itorin
gplasmaandCSF
levels
isof
sign
ificanceto
optim
ize
antib
iotic
delivery
Cieset
al.
[152]
Tode
scrib
etheph
armacokinetics
ofcontinuo
us-in
fusion
ofmerop
enem
Merop
enem
Caserepo
rt.
Paed
iatricpatient
with
ventriculitis
Serum
levelswere12
μg/m
Lat
2hand“und
etectable”
at4h,
with
CSF
levelsof
1and0.5μg
/mLat
2and4h,
respectively(M
IC<0.25)
Oncontinuo
usinfusion
,serum
,andCSF
levelswereno
tedto
be13
and0.5μg
/mL,respectively
Thecontinuo
us-in
fusion
dosing
regimen
allowed
for100%
prob
ability
oftarget
attainmen
tin
theserum
andCSF
andasuccessful
clinicalou
tcom
e
Dahyot-
Fizelier
etal.[153]
Tode
scrib
ebraindistrib
ution
ofcefotaximeby
microdialysis
inpatientswith
acutebraininjury
Cefotaxim
eObservatio
nal,
prospe
ctivestud
y5ICUpatientswith
acutebraininjury,treated
forlung
infection
Cefotaxim
e2g8/8h
MeanAUC b
rain/AUCplasm
aratio
was
26.1±12.1%
Unb
ound
cefotaximebrain
concen
trations
weremuchlower
than
correspo
ndingplasma
concen
trations
Simulated
brainconcen
trationat
two
dosage
regimen
s(usedfortreatm
ent
ofmen
ingitis)show
edT>MIC
high
erthan
90%
ofthedo
sing
intervalforbo
thdo
sing
regimen
s(4
gevery6hor
8h)
for
suscep
tiblestrainsandon
lyfor4gevery
6hforresistanton
es
Thereislim
itedbraindistrib
ution
ofcefotaxime
Highe
rcefotaximedo
sage
(4g6/6h)
isrequ
iredto
treatmen
ingitis
with
resistantbacterialstrains
Veiga and Paiva Critical Care (2018) 22:233 Page 19 of 34

Table
4PK/PDstud
iesof
beta-lactam
sin
cerebralspinalfluid
(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Morita
etal.[154]
Toassess
theefficacy,safety,
andconcen
trationof
merop
enem
incerebrospinalfluid
Merop
enem
Observatio
nal,
prospe
ctivestud
y5adultICUpatients
with
men
ingitis
Merop
enem
2g8/h
(durationof
infusion
was
variablefro
m0.5to
2h)
CSF
andbloo
dwereob
tained
pre-treatm
entandon
days
3,7,
14,and
21
Con
centratio
nsin
cerebrospinalfluid
rang
edfro
m0.27
to6.40
μg/m
Lup
to8.47
handwereover
1μg
/mL3h
afterstartin
gmerop
enem
infusion
TheCSF/plasm
aconcen
trationratio
rang
edfro
m0.008to
0.013,0.011to
0.953,and0.633to
1.821,respectively,
with
in2h,2–6h,andafter6hfro
mthestartof
drug
infusion
Therelatio
nshipof
CSF
concen
tration
toCSF
cellcoun
ts,C
SF/plasm
aglucoseratio
,and
CSF
protein
concen
tration,respectively,was
statisticallycorrelated
with
CSF
cell
coun
tsandCSF
proteinconcen
tration,
andinverselycorrelated
with
CSF/
plasmaglucoseratio
Con
centratio
nof
merop
enem
inCSF
exceed
edtheminim
alinhibitory
concen
trationforthepathog
ens
involved
(pen
icillin
sensitive
S.pn
eumon
iaeandS.salivarius;methicillin-
sensitive
Staphaureus)
Noserio
usadverseeven
tandno
discon
tinuatio
nof
treatm
entoccurred
Themerop
enem
concen
trationin
the
CSF
canbe
expe
cted
tobe
high
becauseof
thepresen
ceof
inflammation
Tsum
ura
etal.[155]
Toexam
inePK
andPD
ofmerop
enem
incerebrospinal
fluid
Merop
enem
Observatio
nal,prospe
ctivestud
y6ne
urosurgicalp
atients
Merop
enem
(0.5gevery8h)
was
administereddu
ring0.5h.
LumbarCSF
andveno
usbloo
dsamples
wereob
tained
at0.5–16
hafterthestartof
thefirstinfusion
Pene
trationinto
theCSF
with
the
AUCratio
was
0.10
±0.03
(mean±SD
)Ado
sage
of0.5gq8
hachieved
a>90%
PTA(50%
oftheT>MIC),and1gq8
hwas
need
edfora>90%
PTA(100%
oft
heT>MIC)forsuscep
tibleisolates
ForP.aerugino
sa,2
gq8
hachieved
alower
PTA
Less
suscep
tiblebacterialC
NSinfections
may
notbe
optim
ized
with
standard
merop
enem
dosage
Nicasio
etal.[156]
Tode
scrib
etheuseandcerebral
spinalfluid
pene
trationof
aprolon
gedinfusion
merop
enem
regimen
inapatient
with
Serra
tiamarcescensmen
ingitis
Merop
enem
Caserepo
rtAdu
ltpatient
with
men
ingitis
and
epiduralabscess
Merop
enem
2gq8
h,3-hinfusion
Theprolon
ged(3
h)infusion
regimen
of2g8hresultedin
concen
trations
inbo
thserum
andCSF
abovethe
MIC
of0.047μg
/mL,for100%
ofthe
dosing
interval
CSF
pene
trationwas
6.4%
Theuseof
ahigh
-doseprolon
gedinfu-
sion
ofmerop
enem
resultedin
ad-
equate
expo
sure
atthesite
ofinfection
andasuccessful
clinicalrespon
seAtfollow-up,
thepatient
hadcompleted
a4-weekcourse
with
outrelapseor
ad-
verseeven
ts
Frasca
etal.[157]
Tode
scrib
ePK–PDprofile
ofcefotaximein
theCSF
Cefotaxim
eCaserepo
rtAdu
ltICUpatient
with
TBI
Cefotaxim
e4gq8
h,30-m
ininfusion
Microdialysiswas
perfo
rmed
onday4,
afterthe12th
dose
Unb
ound
plasmaCmax
was
118.8μg
/mL
CSF
Cmax
was
11.4μg
/mL
T>MIC
inthebrainwere,respectively,
78%
(6.2h)
and46%
(3.7h)
forMIC
values
of2and4μg
/mL
ECFbrainconcen
trations
indicate
that
anadeq
uate
expo
sure
tocefotaximeis
achieved
inpreven
tionandtreatm
ent
ofmostCNSinfections
with
the
standard
dosage
regimen
Wanget
al.[158]
Toexplorewhe
ther
thereisincreased
CSF
pene
trationof
cefope
razone
/sulbactam
whe
nthee
bloo
d–brain
barrierisim
pairedfollowingcraniotomy;
andwhe
ther
extend
edinfusion
time
affectsdrug
concen
trations
Cefop
erazon
e/sulbactam
Observatio
nal,prospe
ctivestud
yDosingwas
3.0gin
a3-hinfusion
every6h,aftercraniotomy
Veno
usbloo
dandCSF
werecollected
before
thestartof
drug
administration
andat
hour
1,2,3,4,6,12,15,16,
and18
afteradministration
8ne
urosurgicaladu
ltpatients
enrolled
CSF
pene
tration:
Peak
concen
trations
(CSF/serum
):8.6%
±7.2%
forcefope
razone
and
13.5%±11.9%
forsulbactam
Trou
ghconcen
trations
(CSF/serum
):13.4%±5.3%
forcefope
razone
and
106.5%
±87.5%
forsulbactam
Ratio
oftheAUCof
CSF
andserum:
14.5%
forcefope
razone
and22.6%
for
Ifcefope
razone
/sulbactam
sing
leinfusion
timeisextend
edto
3h,the
serum
drug
concen
trationachieved
the
PK/PDstandard
of>50%T>MIC
(MIC
90
64mg/L)
Itisvery
difficultto
achievethisPK/PD
standard
intheCSF,and
ahigh
erdo
semight
bene
eded
totreatintracranial
infections
Veiga and Paiva Critical Care (2018) 22:233 Page 20 of 34

Table
4PK/PDstud
iesof
beta-lactam
sin
cerebralspinalfluid
(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
sulbactam
Cefop
erazon
eserum
concen
trations
achieved
>50%T>MIC
forPseudomon
asandAcinetobacter(M
IC90
64mg/L)
and
100%
T>MIC
formoresuscep
tiblebacteria
CSF
cefope
razone
T>MIC%
was
almost100%
(Escherichia
coliMIC50)a
ndT>MIC%
was
morethan
50%
(Acinetobacterbaum
annii
MIC50)
Sulbactam
serum
concen
trations
achieved
>50%T>MIC
forAcinetobacter(M
IC90
16mg/L)
CSF
sulbactam
concen
trations
didno
treachthelevelo
fMIC
50of
8mg/L
forAcinetobacter
Destructio
nof
thebloo
d–brainbarrier
aftercraniotomycanincrease
theCSF
concen
trationto
acertainextent
AUCarea
unde
rthecurve,
CNScentraln
ervo
ussystem
,CRO
ceftria
xone
,CSF
cerebral
spinal
fluid,C
TXcefotaxime,
ICUintensivecare
unit,
MIC
minim
alinhibitory
concen
tration,
MIC50
minim
alinhibitory
concen
tration
for50
%of
isolates,P
TAprob
ability
oftarget
attainmen
t,SD
stan
dard
deviation,
T>MIC
percen
tage
oftim
eab
oveminim
alinhibitory
concen
tration,
TBItraum
abraininjury
Veiga and Paiva Critical Care (2018) 22:233 Page 21 of 34

beta-lactams [13, 20, 159]. The impact of infection ontheir penetration into ELF in humans is unknown [159],though some reports state that ELF penetration in-creases in acute lung injury [160].Only a few studies have investigated beta-lactam PK/PD
issues in critically ill patients with pneumonia (Table 5)and in only seven of them were ELF drug concentrationsmeasured. A standard dosage of beta-lactams derivedfrom healthy patients’ PK profiles may be insufficient fortreatment of critically ill patients with pneumonia, espe-cially when caused by multidrug-resistant pathogens. Con-tinuous or prolonged infusions and higher than standarddoses improve the PD profiles of these antibiotics. This isvery important to achieve an adequate PD profile whentreating less susceptible bacterial strains. Therapy drugmonitoring would be extremely helpful in this setting.
New beta-lactam drugs and beta-lactamasecombinationsOf great concern is the worldwide increase in the number ofinfections caused by Gram-negative multidrug-resistant bac-teria. Treatment choices for these infections have been lim-ited, especially for infections caused by bacteria that producecarbapenemases and/or extended-spectrum beta-lactamases.Ceftolozane–tazobactam and ceftazidime–avibac-
tam are 2 beta-lactams/beta-lactamase combinations withanti-Gram-negative bacteria activity that were recently ap-proved for the treatment of complicated intra-abdominalinfections, complicated urinary tract infections, and noso-comial pneumonia.Ceftolozane is an oxyimino-aminothiazolyl cephalo-
sporin with a pyrazole substituent at the 3-position sidechain instead of the lighter pyridium present in ceftazi-dime. This heavier side chain provides improved sterichindrance to prevent hydrolysis mediated throughAmpC beta-lactamases.Ceftolozane–tazobactam combines a novel cephalo-
sporin with an established beta-lactam beta-lactamaseinhibitor, whereas ceftazidime–avibactam couples awell-known cephalosporin with a novel non-beta-lactambeta-lactamase inhibitor.Both tazobactam and avibactam target the active site
of serine beta-lactamases. Tazobactam, a beta-lactamsulfone, binds irreversibly to the active site ofbeta-lactamases and avibactam is a diazabicyclooctanenon-beta-lactam that binds covalently and reversibly tobeta-lactamases. This reversibility is a unique featurethat allows avibactam to undergo recyclization to inacti-vate another beta-lactamase. The crucial advantage ofavibactam is its ability to inhibit extended spectrumbeta lactamases, AmpC beta-lactamases (as expressed inPseudomonas aeruginosa and Enterobacteriaceae), andclass A carbapenemases of the Klebsiella pneumoniaecarbapenemase (KPC and OXA-48) family.
The pharmacokinetic and safety profiles of this anti-biotic have been established in healthy adults and sub-jects with various degrees of renal function [170, 171].The currently approved dosages for adult patients withan estimated ClCr > 50 mL/minute are ceftolozane 1 gwith tazobactam 500 mg every 8 h and ceftazidime 2 gwith avibactam 500 mg every 8 h for complicated urin-ary tract infections and intra-abdominal infections [172]and ceftolozane 2 g with tazobactam 1 g every 8 h fornosocomial pneumonia [173].However, data guiding its use in critically ill patients
are currently sparse, being entirely derived from studieswith very few patients and/or case reports.Veillete et al. [174] presented PK data for ceftazidime–
avibactam from two patients with bloodstream infectionscaused by carbapenemase (KPC)-producing K. pneumo-niae; the patients had renal impairment and one of themwas obese. In both patients half-lives were prolongedand Vd larger than predicted. They conclude that rec-ommended doses and intervals may not be sufficient forobese patients with renal failure, especially for those in-fected with KPC-producing organisms [174].Oliver et al. [175] evaluated the adequacy of
extended-infusion ceftolozane–tazobactam to achievetarget PK and PD goals in a critically ill patient withPseudomonas aeruginosa pneumonia and septic shockon CVVH. A dosage of 1.5 g every 8 h (3-h infusion)was given. All estimated plasma-free drug concentra-tions achieved the PD goals and remained well abovethe isolated organism’s MIC of 1.5 μg/mL and above thesusceptibility breakpoint of 4 μg/mL throughout thedosing interval, although the authors could not com-ment on drug concentrations at the site of infection.The authors conclude that, given the lowest estimatedfree-drug concentration was fivefold greater than thesusceptibility breakpoint, the estimated half-life of 28 hand the low extraction ratio observed, a lower total dailydose might be utilized and an extended infusion timemay not be necessary for patients on CVVH [175].Bremmer et al. [176] performed a PK analysis of
intravenous ceftolozane–tazobactam 3 g every 8 h in acritically ill patient with P. aeruginosa pneumonia onCVVHDF. They concluded that, compared with a patientwith normal renal function, this patient had decreased cef-tolozane clearance. A ceftolozane–tazobactam dosage of1.5 g every 8 h should adequately achieve a desired drugconcentration above the minimum inhibitory concentra-tion of 8 μg/mL for the treatment of pneumonia [176].Stokem et al. reported the successful treatment with
ceftolozane–tazobactam 3 g every 12 h for a pulmonaryexacerbation in a 35-year-old female post-lung trans-plant, with cystic fibrosis, malnutrition, chronic kidneydisease, and multi-drug resistant P. aeruginosa infection.Optimal time above MIC (estimated 100% time above
Veiga and Paiva Critical Care (2018) 22:233 Page 22 of 34

Table
5PK/PDstud
iesof
beta-lactam
sin
bron
chial-alveo
larlavage
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Kikuchi
etal.[52]
Com
pare
thePK/PDparameters
ofbiapen
emin
bron
chialELF
givenas
0.5-hand3-hinfusion
s
Biapen
emProspe
ctive,no
n-blinde
d,crossoverstud
y6he
althyadultvolunteers
Thepe
rcen
tage
(mean±SD
)of
T>MIC
inbron
chialELF
rang
edfro
mzero
(MIC
4μg
/mL)
to34.6%
±5.2%
(MIC
0.25
μg/m
L)afterthe0.5-hinfusion
and
from
5.1%
±5.6%
(MIC
4μg
/mL)
to52.2%±17.0%
(MIC
0.25
μg/m
L)after
the3-hinfusion
A3-hinfusion
ofbiapen
emtend
edto
prod
uceahigh
erT>MIC
inbron
chialELF,
aswellasin
plasma,than
a0.5-hinfusion
Theseresults
supp
orttheuseof
prolon
ged
infusion
sforsuccessful
treatm
entof
lower
respiratory
tractinfections
basedon
PK/PD
parametersin
bron
chialELF
Rodvold
etal.
[159]
Tode
finetheexpo
sure
targets
inlung
associated
with
good
microbiolog
icalactivity
ina
murinemod
elTo
determ
inedrug
pene
tration
into
ELFin
humans
Ceftobiprol
Prospe
ctive,ob
servationalstudy
Pre-clinical,m
urinemod
elClinicalstud
ywith
24he
althy
volunteers
500mgevery8h,2-h
infusion
regimen
Murinemod
el:for
cellkills
of1and2
log 1
0CFU
/g,totaldrug
mustbe
presen
tin
ELFat
aconcen
trationin
excess
ofthe
MIC
of12.9%
and24%
ofa24-h
interval,
respectively.ELFpe
netrationwas
69%
(med
ian)
MeanELFpe
netrationin
human
volunteerswas
25.5%
(med
ian,
15.3%;
interquartile
rang
e,7.9%
to30.4%)
Target
attainmen
tfalls
below
90%
for
acellkillof
2log 1
0CFU
/gat
aMIC
of1.0mg/Landfora1log 1
0CFU
/gcell
killat
aMIC
of2.0mg/L
Ceftobiprolepe
netrated
into
ELFvery
differentlyin
humanscomparedto
mice
Forserio
uslyillpatients,particularlyin
theICU,
high
erdo
sesor
long
erinfusion
times
(toprolon
gthetim
e>MIC),or
both,w
illbe
requ
iredto
comfortablyen
sure
a90%
target
attainmen
tfor
serio
uslyillpatientswith
MRSApn
eumon
ia
Con
teet
al.
Determinetheplasmaand
intrapulmon
aryELFandAC
pharmacokineticparametersof
intraven
ouslyadministered
merop
enem
Merop
enem
Prospe
ctive,ob
servational
Four
doses(8/8
h)of
0.5g,
1.0g
or2.0gwereadministered
intraven
ouslyto
20,20,and8
healthyadultsubjects,respe
ctively
Cmax,A
UC,T
1/2:
0.5ggrou
p:serum
25.8±5.8μg
/mL,
28.57μ
gh/mL,0.77
h;ELF5.3±2.5μg
/mL,
12.27μg
h/mL,1.51
h;AC1.0±0.5μ
g/mL,
4.30
μgh/mL,2.61
h1ggrou
p:serum
53.5±19.7μg
/mL,
55.49μ
gh/mL,1.31
h;ELF7.7±3.1μ
g/m
L,15.34μg
h/mL,0.95
h;AC5.0±3.4μg
/mL,
14.07μg
h/mL,2.17
h2ggrou
p:serum
131.7±18.2μg
/mL,
156.7μg
h/mL,0.89
hT≥MIC
(MIC90
values
of0.12–4μg
/mL):
0.5ggrou
p:serum
28–78%
,ELF
18–100%,
AC0–100%
1gGroup
:serum
45–100%,ELF
25–88%
,AC24–100%
Theprolon
gedT>MIC90
andhigh
intrapulmon
arydrug
concen
trations
following
every8hadministrationof
0.5–2.0gdo
sesof
merop
enem
arefavorableforthetreatm
entof
common
respiratory
pathog
ens.
Boselli
etal.
[161]
Determinethesteady-state
serum
andalveolar
concen
trations
ofpipe
racillin/tazobactam
administeredin
continuo
usinfusion
(12/1.5g/dayor
16/2
g/day)
atvario
usde
greesof
renal
failure
(terminalrenalfailure
exclud
ed)
Pipe
racilin/
tazobactam
Prospe
ctive,op
en-labe
l,comparative,sing
lecenter
40ICUpatientswith
ventilator-associated
pneumon
iaSamples
collected
after2days
oftreatm
ent
Med
ian(interquartile)serum
andalveolar
pipe
racilin
concen
trations
No/mild
renalfailure
(creatinineclearance
≥50
mL/min)
Serum
25.3mg/L(23.1–32.6)andalveolar
12.7mg/L(6.7–18.0)
for12/1.5g/day
Serum
38.9mg/L(32.9–59.6)andalveolar
19.1mg/L(14.0–21.5)for16/2
g/day
Mod
erate/advanced
renalfailure
(creatinineclearance<50
mL/min)
Serum
102.4mg/L(97.4–112.6)
and
alveolar
44.1mg/L(33.4–48.3)for12/2
g/day
Serum
135.3mg/L(119.5–146.2)andalveolar
54.9mg/L(45.2–110.3)
for16/2
g/day
Alveo
larpe
netrationwas
40–50%
for
pipe
racillinand65–85%
fortazobactam
Therewas
apo
sitivelinearrelatio
nship
betw
eenELFandserum
concen
trationin
both
patientsreceiving12/1.5g/day
Theadministrationof
daily
continuo
usinfusion
sof
P/T12/1.5gor
even
16/2
gmight
provideinsufficien
talveolar
concen
trationto
eradicatehigh
-riskpathog
ens
with
high
MICssuch
asmulti-drug
resistantP.aerugino
sain
patientswith
noor
mild
renalinsufficiency
Alinearrelatio
nshipbe
tweenalveolar
andserum
pipe
racillinconcen
trationwas
observed
inthisstud
y,with
ELFpipe
racillinconcen
trationbe
ing40–50%
ofcorrespo
ndingserum
values
Veiga and Paiva Critical Care (2018) 22:233 Page 23 of 34

Table
5PK/PDstud
iesof
beta-lactam
sin
bron
chial-alveo
larlavage
(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
(r=0.8437,P
<0.0001)and16/2
g/day
(r=0.7935,P
<0.0001)
T>MIC
was
100%
(assum
ingMIC
>16
mg/L)
inbo
thserum
andELFin
allp
atientswith
mod
erate/advanced
renalfailure;inpatients
with
no/m
ildrenalfailure
thisthresholdwas
notreache
din
6patientswith
12/0.5gdo
sing
and4patientswith
16/2
gdo
sing
Cou
sson
etal.
[162]
Com
pare
continuo
usvs
interm
itten
tadministrationof
drug
Determineaverageconcen
tration
inELF
Determinethefractionof
time,
durin
gthefirst48
hof
treatm
ent,
whe
reserum
concen
trations
remaine
dabovethe20
mg/Lplasmathreshold
Ceftazidime
Sing
le-cen
ter,controlled,
rand
omized
trialintw
oparallelg
roup
scomparin
gtw
omod
esof
administration:
grou
pA,
loadingdo
se20
mg/kg
+60
mg/kg/day;
grou
pB,20
mg/kg
over
30min
every8h
34adultICUpatientswith
ventilator-
associated
pneumon
iadu
eto
Gram-neg
ativebacilli.
ThemeanMIC
ofceftazidim
efor
P.aerugino
sawas
estim
ated
at2mg/L.
Thetarget
thresholdvaluefor
ceftazidim
ein
theELFwas
thus
fixed
at8mg/L,with
acorrespo
nding
serum
thresholdof
20mg/L
PlasmaT>20
mgwas
100%
ingrou
pAversus
46%
ingrou
pB(P<0.003)
IntheELF,themed
ianconcen
trationwas
12mg/Lin
grou
pAversus
6mg/Lin
grou
pB(P<0.08)
Athresholdof
8mg/Lin
theep
itheliallining
fluid
was
achieved
twiceas
oftenin
grou
pAas
ingrou
pB
Con
tinuo
usinfusion
presen
tsadvantages
interm
sof
PDandpred
ictableefficacyin
patientspresen
ting
ventilator-associated
pneumon
ia
Burkhardt
etal.
[163]
Determinein
vivo
pene
trationinto
LT,ELF,and
ACafter1gof
ertape
nem
(infusion
perio
d30
min)for
perio
perativeprop
hylaxis
Ertape
nem
Sing
le-cen
ter,prospe
ctive,
observational
of15
patientsun
dergoing
thoracotom
yBA
Lpe
rform
edat
1,3,and
5hafterertape
nem
infusion
Plasmaconcen
trationcollected
upto
24hafterinfusion
LTcollected
attim
eof
lung
extractio
n
Meanconcen
trations
inplasma,ELF,andAC
were:at
1.0h,
63.1,4.06,0.004mg/L;at
3.0h,
39.7,2.59,0.003mg/L;at
5.0h,27.2,2.83,0.007mg/L
Mean(rang
e)concen
trationin
LTwas
7.60
(2.5–19.4)
mg/kg
tissue,1.5to
4.5hafterinfusion
andLT
plasmaconcen
trationratio
was
23.6±12.3%
Meanlevelo
fELFpe
netrationwas
7.48%±8.17%,
andthehigh
estde
gree
ofpe
netrationwas
recorded
at5hafterinfusion
(mean±SD
,9.40%±10.7%)
A1-gdo
se,oncedaily,resultsin
drug
plasma
concen
trations
high
erthan
MICsof
mostcommun
ity-acquired
respiratory
pathog
ensdu
ringtheen
tiredo
sing
interval
Meanconcen
trations
inELFexceed
edMIC90
values
ofhigh
lyor
mod
eratelype
nicillin-sensitive
Pneumococci
andof
H.
influenzaewith
in1to
5hafterstartof
infusion
and
werepartlybe
low
theMIC90
ofpe
nicillin-resistant
Pneumococci
Theseresults,com
bine
dwith
therepo
rted
MIC
90
ofmostCAPbacteria,sup
portthepreviouslyob
served
clinicalefficacyof
ertape
nem
inthetreatm
entof
commun
ity-acquiredpn
eumon
ia
Boselliet
al.[164]
Determinethesteady-state
serum
andELFconcen
trations
ofun
boun
dertape
nem
administeredon
cedaily
tocritically
illpatientswith
early-onset
ventilator-associated
pneumon
ia
Ertape
nem
Prospe
ctive,op
en-labe
lstudy
inan
intensivecare
unit
15patientswith
VAPreceived
1-h
intraven
ousinfusion
sof
1gertape
nem
once
daily
Samples
obtained
atsteady-state,
after2days
oftherapy
ELFob
tained
bymini-BAL
Med
ian(interquartile
rang
e)Cmax,C
12,and
Cmin
concen
trations
(mg/l)1,12,and
24haftertheen
dof
infusion
were:30.3(27.1–37.8),4.8(3.9–6.4),and
0.8(0.5–1.2)
inserum
and9.4(8.0–10.7),2.0(1.1–2.5),
and0.3(0.2–0.4)in
ELF,respectively
Med
ianfre
epe
rcen
tage
pene
trationin
ELF
approxim
ately30–40%
Con
centratio
nsexceed
ingtheMIC90
values
ofmostof
thecausativepathog
ens(0.25–2mg/lfor
S.pn
eumon
iae,
0.06–0.125
mg/lfor
Haemophilusinfluenzae,0.25–0.5mg/l
foroxacillin-susceptible
S.aureus,and
0.03–0.125
mg/l
forEnterobacteriaceae
andanaerobe
s0.5–1mg/lw
asen
coun
teredin
early-onset
VAPdu
ring50–100%
time
1gintraven
ousertape
nem
once
daily
shou
ldbe
effectiveforearly-onset
VAPICUpatientswith
noknow
nriskfactorsfor
multid
rug-resistantpathog
ens
Veiga and Paiva Critical Care (2018) 22:233 Page 24 of 34

Table
5PK/PDstud
iesof
beta-lactam
sin
bron
chial-alveo
larlavage
(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Boselliet
al.[165]
Tode
term
inethesteady-state
plasma
andELFconcen
trations
ofceftazidim
eadministeredin
continuo
usinfusion
tocritically
illpatients
with
severe
nosocomialp
neum
onia
Ceftazidime
Prospe
ctive,op
en-labe
lstudy.
15adultpatientswith
severe
nosocomial
bacterialp
neum
oniaon
mechanical
ventilatio
nAdm
inistrationof
30min
infusion
of2g
ceftazidim
efollowed
bycontinuo
usinfusion
4gover
24h
Bloo
dandmini-BALsamples
collected
bythethird
dayof
antib
iotic
therapy
(8:00am
,12:00
pm,and
6:00
pm)
Themean±SD
steady-state
plasmaand
ELFconcen
trations
incontinuo
usinfusion
were39.6±15.2g/mLand8.2±4.8g/mL,
respectively,show
ingamean±SD
percen
tage
pene
trationof
ceftazidim
einto
ELFof
20.6±8.9%
Theadministrationof
theapplieddo
sein
critically
illpatientswith
severe
nosocomialp
neum
oniaprovides
concen
trations
inexcess
oftheMIC
ofmanysuscep
tible
organism
sover
thecourse
oftherapyin
both
serum
andELF.How
ever,for
somepathog
enssuch
asP.aerugino
sa,h
ighe
rdo
sesof
ceftazidim
eshou
ldbe
administered,
oranothe
ragen
tshou
ldbe
used
incombinatio
n
Felto
net
al.[166]
Toassess
plasmaandintra-pu
lmon
ary
PKof
pipe
racillin/tazobactam
incritic-
allyillpatients
Quantify
pulm
onarype
netration
Iden
tifyfactorsthat
may
influen
cepu
lmon
arype
netration
Pipe
racilin/
tazobactam
Prospe
ctive,op
enlabe
l,sing
learm
stud
y18
ICUadultpatientswith
pneumon
iaAdm
inistrationof
4/0.5ginfusion
every
8hdaily
Samples
collected
atsteady-state
(mean
of8.8do
ses(rang
e2–16).
Non
-directed
bron
chiallavagewas
perfo
rmed
forELFsampling
Med
ianpipe
racilin
andtazobactam
pulm
onarype
netrationratio
was
49.3%
and121.2%
respectively.
ELFprotein/plasmaproteinratio
,asa
surrog
atemeasure
oflung
perm
eability,
was
foun
dto
have
astatisticallyne
gative
correlationbe
tweenpipe
racilin
pulm
onary
pene
trationratio
andpu
lmon
arype
rmeability.
Therewas
nostatisticallysign
ificant
correlationfortazobactam
14–18%
ofpatientswillhave
subo
ptim
aldrug
expo
sure
(ELF
50%T>MIC)whe
ninfected
with
a“susceptible”(M
IC<16
mg/L)
organism
Pipe
racilin
andtazobactam
plasmaconcen
trations
dono
tpreciselypred
ictELFconcen
trations
ofbo
thdrug
s
Current
pipe
racilin-tazob
actam
regimen
sisinadeq
uate
foreffectivetreatm
entandsupp
ressionof
emerge
nce
ofantim
icrobialresistance
inan
unacceptablyhigh
prop
ortio
nof
critically
illpatients,espe
ciallythosewith
pneumon
iaresulting
from
infectionwith
aless
suscep
tible
organism
Boselliet
al.[167]
Tode
term
inethesteady-state
plasma
andELFconcen
trations
ofcefepime
administeredin
continuo
usinfusion
incritically
illpatientswith
severe
bacterialp
neum
onia
Cefep
ime
Prospe
ctive,op
en-labe
lstudy
20ICUadultpatientswith
severe
nosocomialb
acterialp
neum
onia
Allsubjectsreceived
a30-m
inintraven
-ou
sinfusion
ofcefepime2gfollowed
byacontinuo
usinfusion
of4gover
24h
Samples
werecollected
after48
hof
therapy.Bloo
dandminiB
ALsamples
werecollected
at8:00
am,12:00
pm,and
6:00
pm
Mean±SD
steady-state
plasmaandELF
concen
trations
were13.5±3.3g/mLand
14.1±2.8g/mL,respectively,with
amean
percen
tage
pene
trationinto
epith
eliallining
fluid
ofabou
t100%
Adm
inistrationof
cefepimein
continuo
usinfusion
incritically
illpatientswith
severe
nosocomialp
neum
onia
appe
arsto
optim
izetheph
armacod
ynam
icprofile
ofthis
beta-lactam
byconstantlyprovidingconcen
trations
inexcess
ofMIC
ofmostof
thesuscep
tibleorganism
sover
the
course
oftherapyin
both
serum
andELF
Forsomepathog
enssuch
asAcinetobacterspp.
and
P.aerugino
sahigh
erdo
sesshou
ldbe
administered
Boselliet
al.[168]
Tode
term
inethesteady-state
plasma
andep
ithelialliningfluid
concen
tra-
tions
ofpipe
racillin/tazobactam
admin-
isteredto
critically
illpatientswith
severe
bacterialp
neum
onia
Pipe
racilin/
tazobactam
Prospe
ctive,op
enlabe
lstudy
10ICUadultpatientswith
severe
nosocomialp
neum
onia
30-m
inintraven
ousinfusion
4/0.5gevery
8h
Samples
wereob
tained
atsteady-state,
after2days
oftreatm
ent.Bloo
dsamples
werecollected
atthree
pred
etermined
timepo
intsat
7:00
am(troug
h),8:00am
(peak),and
12:00pm
(interm
ediate)
MiniB
ALwas
perfo
rmed
simultane
ously
tobloo
dsamplingat
12:00pm
Mean±SD
steady-state
plasmatrou
gh,p
eak,
andinterm
ediate
concen
trations
were
8.5±4.6μg
/mL,55.9±21.6μg
/mL,and
24.0±13.8μg
/mLforpipe
racillin,
and
2.1±1.0μg
/mL,4.8±2.1μg
/mL,and
2.4±1.2μg
/mLfortazobactam
Mean±SD
steady-state
interm
ediate
ELFconcen
trations
were13.6±9.4μg
/mL
forpipe
racillinand2.1±1.1μg
/mLfor
tazobactam
,respe
ctively
Meanpe
rcen
tage
pene
tration
ofpipe
racillinand
tazobactam
into
ELFwas
56.8%
and
91.3%,respe
ctively
Treatm
entof
severe
nosocomialp
neum
oniawith
aregimen
ofP/T4/0.5gevery8hmight
provide
insufficien
tconcen
trations
into
lung
tissueto
exceed
theMIC
ofmanycausativepathog
ens
Veiga and Paiva Critical Care (2018) 22:233 Page 25 of 34

Table
5PK/PDstud
iesof
beta-lactam
sin
bron
chial-alveo
larlavage
(Con
tinued)
Stud
yEndp
oints
Antibiotic
Design
Results
Con
clusions
Lodise
etal.[169]
Tode
scrib
ethePD
profile
ofcefdito
renin
plasmaandELF
Cefditoren
Ope
n,no
ncon
trolled,
dual-cen
ter,ph
aseIstudy
24adultpatientswith
sche
duled
bron
choscopy
Sing
leoraldo
se400mgcefdito
ren
Threesamplingtim
ewindo
ws(1–2
h,2–
3h,
or3–4hpo
st-adm
inistration)
Plasma/ELFconcen
trations
(mg/L)/pen
etratio
nratio
s1–2h:
1.78
±1.27/0.39±0.21/38.1±50.1%
2–3h:
1.33
±0.95/0.34±0.25/23.2±18.1%
3–4h:
1.03
±0.51/0.30±0.18/31.8±19.2%
AUC
ELF/AUC
plasm
ape
netrationratio
(mean±SD
)was
0.33
±0.48
PTAin
plasmafT>MIC
of60
to70%
was
<90%
forMICsof
>0.03
mg/L
PTAin
ELFT>MIC
of60%
and70%
were
90.26%
and86.65%
,respe
ctively,at
aMIC
of0.0125
mg/Landweresign
ificantlyless
forhigh
erMICs
Cefditorenpe
netrates
reason
ablywellintotheELF,
asde
fined
bythemeanAUCELF/AUCplasm
a
pene
trationratio
Theoverallp
robabilityof
target
attainmen
t(T>MIC
>50%)in
plasmaandELF,ho
wever,
was
subo
ptim
al(<
90%)
ACalveolar
cells,A
UCarea
unde
rthecurve,
BALbron
choa
lveo
larlavage
,CAPcommun
ity-acq
uiredpn
eumon
ia,C
maxmaxim
alconcen
tration,
C 12concen
trationat
12h,
Cmintrou
ghconcen
tration,
CFUcolony
form
ing
unit,
ELFep
ithelialliningflu
id,ICU
intensivecare
unit,
LTlung
tissue,
MIC
minim
alinhibitory
concen
tration,
MIC90
minim
alinhibitory
concen
trationfor90
%of
isolates,M
RSAmethicillin-resistan
tStap
hylococcus
aureus,
P/Tpipe
racillin/tazoba
ctam
,PTA
prob
ability
oftarget
attainmen
t,SD
stan
dard
deviation,
T 1/2ha
lf-life,
T>MIC
percen
tage
oftim
eab
oveminim
alinhibitory
concen
tration,
VAPventilator-associated
pneu
mon
ia
Veiga and Paiva Critical Care (2018) 22:233 Page 26 of 34

MIC of ceftolozane achieved against both isolates was 2and 0.5 μg/mL) was likely attained at the dose and fre-quency provided in this case [177].
ToxicityBeta-lactams are generally considered to have a high safetywindow with relatively few adverse effects, even whenhigh doses are used [15]. Neurotoxicity is the most re-ported serious adverse effect of beta-lactams. Benzylpeni-cillin, cefepime, ceftazidime, and imipenem are consideredto be the high-risk beta-lactams for neurotoxicity. Renalimpairment, excess doses and/or concentrations, age, anda prior history of neurological disorders are known to bepredisposing factors [2, 178–184].Other adverse effects are found in a few case reports:
acute renal failure [185] and electrolyte disorders [186];severe intravascular haemolysis [187, 188]; extremethrombocytosis [189]; severe thrombocytopenia [190–193]; leukopenia [194]; delayed-type hypersensitivity[195]; anaphylactic shock [196]; and severe cutaneous re-actions [197].
Therapeutic dose monitoringSeveral studies reported high PK variability ofbeta-lactams in sepsis/septic shock, both in different pa-tients and in the same patient over time. In critically illpatients, hydrophilic and moderately lipophilic antimi-crobials, being at higher risk of daily PK variations,should be more closely monitored and their dosagesshould be streamlined according to the underlying dis-eases in order to prevent under- or overexposure [2, 11].Therapeutic drug monitoring (TDM) has been insti-
tuted for aminoglycosides and glycopeptides to reduce therate of toxicity. However, because of the safety profile ofbeta-lactams, TDM was thought unnecessary for thesedrugs. In line with PK changes in critically ill patients, in-sufficient PD target attainment with beta-lactams has beenreported in these patients, especially those with hypoalbu-minemia, altered renal function, and low susceptibilitybacterial strain infections [2, 35, 42, 198]. The challengesin achieving ‘optimal’ drug concentrations in the criticallyill suggest beta-lactam TDM as a useful strategy tooptimize drug exposure [199].The TDM approach could be particularly useful in
a certain group of critically ill patients in whomachieving target concentrations is more difficult, suchas those with highly resistant bacterial strains, obesepatients, immunocompromised patients, those under-going renal-replacement therapies, and patients withaugmented renal clearance [2, 198, 200, 201].Though there are PK models to estimate antibiotic
concentrations over a range of creatinine clearance(CrCl) and on renal replacement therapy [67, 202–205],the use of CrCl as a tool to optimize beta-lactam dosing
may not be reliable; although CrCl was significantly corre-lated with concentrations and clearance of broad-spectrumbeta-lactams, changes in CrCl and RRT parameters do notreliably predict variations in drug PK/PD. In this setting,routine TDM should be considered to adapt beta-lactamdoses [206].Daily TDM of beta-lactams with dose adaptation in
critically ill patients improves PD target attainment[207, 208]. Case reports have shown that TDM improvedclinical outcome [209], but the clinical efficacy of usingdrug levels to achieve adequate concentrations had neverbeen properly evaluated [1, 35, 210, 211] and there are re-ports concerning cost-effectiveness [111].Facing poor implementation in beta-lactam TDM,
Delattre et al. [212] proposed a predictive PK perform-ance between an aminoglycoside and a beta-lactam. Dueto physicochemical and PK similarities between amino-glycosides and beta-lactams, optimization of thebeta-lactam dosage could be reached without anybeta-lactam measurements, using TDM-related data ofan aminoglycoside. The study aimed to characterize thePK of four beta-lactams (piperacillin, ceftazidime, cefe-pime, and meropenem) at the first dose in 88 criticallyill septic patients co-medicated with amikacin, and toconfirm the predictive performance of amikacin data onthese PK, on a larger patient cohort, using a nonlinearmixed-effects modeling approach. There was a signifi-cant relationship between the exposure to amikacin andto beta-lactams. The population model presented wasable to guide dosage adjustments for piperacillin, ceftazi-dime, cefepime, and meropenem during the early phaseof severe sepsis in critically ill patients, using renal bio-markers or TDM-related aminoglycoside data [212].
ConclusionsThe duration of infusion of beta-lactams has beenshown to influence their fT >MIC and an improved PDprofile of beta-lactams may be obtained by longer expos-ure with more frequent dosing, extended infusions, orcontinuous infusions. This is particularly relevant in thecritically ill patient, as Vd and ClCr are often increased,namely in the early phase of systemic hyperinflammatorystates, promoting the risk of antibiotic underdosing.The use of extracorporeal support techniques, either
for renal replacement or ECMO, may further contributeto this problem and consequently concentrations belowthose expected are often found for beta-lactams. Giventhe heterogeneity of extracorporeal support therapymodes, it is difficult to suggest a specific dosage, but werecommend not to reduce dosage since no drug accu-mulation was found in the available literature and to usecontinuous or prolonged infusions to achieve the ad-equate PD profiles necessary to successfully treat infec-tions caused by less susceptible strains.
Veiga and Paiva Critical Care (2018) 22:233 Page 27 of 34

More studies are needed to define optimal dosing ofnew beta-lactams and new beta-lactam/beta-lactamasecombinations, which are increasingly important to ef-fectively treat multidrug-resistant bacterial strains,namely in patients on extracorporeal support therapyand with difficult-to-treat sites of infection.Although, it is not currently a clinical routine in most
hospitals and its clinical efficacy has not yet been prop-erly evaluated, a beta-lactam TDM approach with dailydose adaptation, allowing personalized antibiotic dosing,should be particularly useful in critically ill patients inwhom achieving target concentrations is more difficult,such as obese patients, the immunocompromised, pa-tients with augmented renal clearance, those undergoingextracorporeal support therapy, or those infected withhighly resistant bacterial strains. Studies comparingTDM- versus non-TDM-based beta-lactam regimensshould be promoted.However, infection usually occurs at extravascular sites
and prediction of outcome based on antibiotic plasmaconcentrations may result in overestimation of antimicro-bial activity at the site of infection. Very few studies haveinvestigated PK/PD issues concerning special anatomicbarriers like the brain and lung, but most suggest thatstandard ICU dosing for beta-lactams may be insufficientfor low susceptibility/high MIC pathogens in these sites.Therefore, although no studies have assessed clinical out-come, we recommend using higher than standard dosing,preferably with continuous or prolonged infusions, whentreating severe infections caused by less susceptible bac-terial strains at these sites, as PD profiles may improveand toxicity does not seems to increase.
AbbreviationsAKI: Aacute kidney injury; AUC: Aarea under the curve; C: Concentration;CFU: Colony-forming units; CI: Continuous infusion; Cl: Clearance;ClCr: Creatinine clearance; CNS: Central nervous system; CRRT: Continuousrenal replacement therapy; CSF: Cerebral spinal fluid; CVVHD: Continuousvenous-venous hemodialysis; CVVHDF: Continuous venous-venous hemodia-filtration; CVVHF: Continuous venous-venous hemofiltration;ECMO: Extracorporeal membrane oxygenation; EDD: Extended daily dialysis;ELF: Epithelial lining fluid; ICU: Intensive care unit; II: Intermittent infusion;KPC: Carbapenemase producing Klebsiella; MBC: Minimal bactericidalconcentration; MIC: Minimum inhibitory concentration; PAE: Post-antibioticeffect; PD: Pharmacodynamics; PK: Pharmacokinetics; PTA: Probability oftarget attainment; RRT: Renal replacement therapy; SLED: Sustained low-efficiency dialysis; TDM: Therapeutic drug monitoring; VAP: Ventilatorassociated pneumonia; Vd: Volume of distribution
Availability of data and materialsAll data generated or analyzed during this study are included in thispublished article (see bibliography).
Authors’ contributionsRV and JAP made substantial contributions to conception and design,acquisition of data, and analysis and interpretation of data; were involved indrafting the manuscript or revising it critically for important intellectualcontent; gave final approval of the version to be published; agreed to beaccountable for all aspects of the work in ensuring that questions related tothe accuracy or integrity of any part of the work are appropriatelyinvestigated and resolved.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Centro Hospitalar São João, EPE – Intensive Care Department, Porto,Portugal. 2Faculty of Medicine – University of Porto, Porto, Portugal. 3GrupoInfeção e Sepsis, Porto, Portugal.
Received: 23 April 2018 Accepted: 8 August 2018
References1. Gonçalves-Pereira J, Póvoa P. Antibiotics in critically ill patients: a systematic
review of the pharmacokinetics of b-lactams. Crit Care. 2011;15(5):R206.2. Sinnollareddy MJ, Roberts MS, Lipman J, Roberts JA. Beta-lactam
pharmacokinetics and pharmacodynamics in critically ill patients andstrategies for dose optimization: A structured review. Clin Exp PharmacolPhysiol. 2012;39:489–96.
3. Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Horton JM, Studnek JR,Kline JA, Jones AE, On behalf of the Emergency Medicine Shock ResearchNetwork. Association between timing of antibiotic administration andmortality from septic shock in patients treated with a quantitativeresuscitation protocol. Crit Care Med. 2011;39:2066–71.
4. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R,Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. Duration ofhypotension before initiation of effective antimicrobial therapy is the criticaldeterminant of survival in human septic shock. Crit Care Med. 2006;34:1589–96.
5. Roberts JA, Paul SK, Akova M, Bassetti M, De Waele JJ, Dimopoulos G,Kaukonen KM, Koulenti D, Martin C, Montravers P, Rello J, Rhodes A, Starr T,Wallis SC, Lipman J, for the DALI Study. DALI: defining antibiotic levels inintensive care unit patients: are current β-lactam antibiotic doses sufficient forcritically ill patients? Clin Infect Dis. 2014; https://doi.org/10.1093/cid/ciu027.
6. Zilberberg MD, Shorr AF, Micek ST, Vazquez-Guillamet C, Kollef MH. Multi-drug resistance, inappropriate initial antibiotic therapy and mortality inGram-negative severe sepsis and septic shock: a retrospective cohort study.Crit Care. 2014;18:596.
7. Bloos F, Ruddel H, Thomas-Ruddel D, Schwarzkopf D, Pausch C, Harbarth S,Schreiber T, Grundling M, Marshall J, Simon P, Levy MM, Weiss M, WeylandA, Gerlach H, Schurholz T, Engel C, Matthaus-Kramer C, Scheer C, Bach F,Riessen R, Poidinger B, Dey K, Weiler N, Meier-Helmann A, Haberle HH,Wobker G, Kaisers UX, Reinhart K. Effect of a multifaceted educationalintervention for anti-infectious measures on sepsis mortality: a clusterrandomized trial. Intensive Care Med. 2017;43:1602–12.
8. Ryoo SM, Kim WY, Sohn CH, Seo DW, Koh JW, Oh BJ, Lim KS. Prognosticvalue of timing of antibiotic administration in patients with septic shocktreated with early quantitative resuscitation in emergency departments. AmJ Med Sci. 2015;349:328–33.
9. Vilella AL, Seifert CF. Timing and appropriateness of initial antibiotic therapyin newly presenting septic patients. Am J Emerg Med. 2014;32:7–13.
10. Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A,Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, AngusDC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, CoopersmithC, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, HollenbergSM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR,Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, MorenoRP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM,Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, SimpsonSQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL,Wiersinga WJ, Zimmerman JL, Dellinger RP. Surviving Sepsis Campaign:
Veiga and Paiva Critical Care (2018) 22:233 Page 28 of 34

International guidelines for management of sepsis and septic shock: 2016.Intensive Care Med. 2017;43:304–77.
11. Bloos F, Rüdde H, Thomas-Rüddel D, Schwarzkopf D, Pausch C, Harbarth S,Schreiber T, Gründling M, Marshall J, Simon P, Levy MM, Weiss M, WeylandA, Gerlach H, Schürholz T, Engel C, Matth C, Scheer C, Bach F, Riessen R,Poidinger B, Dey K, Weiler N, Meier-Hellmann A, Häberle HH, Wöbker G,Kaisers UX, Reinhart K for the MEDUSA study group. Effect of a multifacetededucational intervention for anti-infectious measures on sepsis mortality: acluster randomized trial. Intensive Care Med. 2017;43:1602–12.
12. Pea F, Viale P, FurlanutM. Antimicrobial therapy in critically ill patients. Areview of pathophysiological conditions responsible for altered dispositionand pharmacokinetic variability. Clin Pharmacokinet. 2005;44:1009–34.
13. Levison ME. Pharmacodynamics of antimicrobial drugs. Infect Dis Clin NAm. 2004;18:451–65.
14. Roberts JA, Lipman J. Pharmacokinetic issues for antibiotics in the criticallyill patient. Crit Care Med. 2009;37:840–51.
15. McKinnon PS, Paladino JA, Schentag JJ. Evaluation of area under the inhibitorycurve (AUIC) and time above the minimum inhibitory concentration (T>MIC)as predictors of outcome for cefepime and ceftazidime in serious bacterialinfections. Int J Antimicrob Agents. 2008;31:345–51.
16. Roos JF, Lipman J, Kirkpatrick CMJ. Population pharmacokinetics andpharmacodynamics of cefpirome in critically ill patients against Gram-negative bacteria. Intensive Care Med. 2007;33:781–8.
17. Sime BK, Roberts MS, Warner MS, Hahn U, Robertson TA, Yeend S, Phay A,Lehman S, Lipman J, Peake SL, Roberts JA. Altered pharmacokinetics ofpiperacillin in febrile neutropenic patients with haematological malignancy.Antimicrob Agents Chemother. 2014;5:3533–7.
18. Taccone FS, Cotton F, Vincent JL, Jacobs F. Optimal meropenemconcentrations to treat multidrug-resistant Pseudomonas aeruginosa septicshock. Antimicrob Agents Chemother. 2012;56:2129–31.
19. Ashley WS, Allen N, Rafferty KD, Fish DN, Toschlog E, Newell M, Waibel B.Pharmacokinetic analysis of piperacillin administered with tazobactam incritically ill, Morbidly Obese Surgical Patients. Pharmacotherapy. 2014;34:28–35.
20. Onufrak NJ, Forrest A, Gonzalez D. Pharmacokinetic and pharmacodynamicprinciples of anti-infective dosing. Clin Ther. 2016;8:1930–47.
21. Syamhanin A, Li JX, Wallis SC, Rudd M, Jarrett P, Paterson DL, Lipman J, UdyAA, Roberts JA. Pharmacokinetics of meropenem and piperacillin in critically illpatients with indwelling surgical drains. Int J Antimicrob Agents. 2013;42:90–3.
22. Brink AJ, Richards JA, Schillack V, Kiem S, Schentag J. Pharmacokinetics ofonce-daily dosing of ertapenem in critically ill patients with severe sepsis.Int J Antimicrob Agents. 2009;33:432–6.
23. Roberts JA, Udy AA, Jarret P, Wallis SC, Hope WW, Sharma R, Kirkpatrick CMJ,Kruger PS, Roberts MS, Lipman J. Plasma and target-site subcutaneous tissuepopulation pharmacokinetics and dosing simulations of cefazolin in post-trauma critically ill patients. J Antimicrob Chemother. 2015;70:1495–502.
24. Jeon S, Han S, Lee J, Hong T, Paek J, Woo H, Yima DS. Populationpharmacokinetic analysis of piperacillin in burn patients. Antimicrob AgentsChemother. 2014;58:3744–51.
25. Carlier M, Noe M, Roberts JA, Stove V, Verstraete AG, Lipman J, De Waele JJ.Population pharmacokinetics and dosing simulations of cefuroxime incritically ill patients: non-standard dosing approaches are required toachieve therapeutic exposures. J Antimicrob Chemother. 2014;69:2797–803.
26. Coufignall C, Pajot O, Laouénan C, Burdet C, Foucrier A, Wolff M, Armand-Lefevre L, Mentré F, Massias L. Population pharmacokinetics of imipenem incritically ill patients with suspected ventilator-associated pneumonia andevaluation of dosage regimens. Br J Clin Pharmacol. 2014;78:1022–34.
27. De Waele JJ, Lipman J, Akova M, Bassetti M, Dimopoulos G, Kaukonen M,Koulenti D, Martin C, Montravers P, Rello J, Rhodes A, Udy AA, Starr T, WallisSC, Roberts JA. Risk factors for target non-attainment during empiricaltreatment with b-lactam antibiotics in critically ill patients. Intensive CareMed. 2014;40:1340–51.
28. Meyer B, Traunmueller F, Bojic A, Locker G, Schmid R, Winkler S,Thalhammer F. Single-dose pharmacokinetics of cefodizime in critically illelderly patients. Int J Antimicrob Agents. 2006;27:335–8.
29. Blot SI, Pea F, Lipman J. The effect of pathophysiology on pharmacokineticsin the critically ill patient - Concepts appraised by the example ofantimicrobial agents. Adv Drug Deliv Rev. 2014;77:3–11.
30. Joynt JM, Lipman J, Gomersall CD, Young RJ, Wong ELY, Gin T. Thepharmacokinetics of once-daily dosing of ceftriaxone in critically ill patients.J Antimicrob Chemother. 2001;47:421–9.
31. Dalley AJ, Lipman J, Deans R, Vankatesh B, Rudd M, Roberts MS, Cross SE. Tissueaccumulation of cephalothin in burns: a comparative study by microdialysis ofsubcutaneous interstitial fluid cephalothin concentrations in burn patients andhealthy volunteers. Antimicrob Agents Chemother. 2009;53:210–5.
32. Dalley AJ, Deans R, Lipman J, Venkatesh B, Rudd M, Roberts MS, Cross SE.Unbound cephalothin pharmacokinetics in adult burn patients are relatedto the elapsed time after injury. Antimicrob Agents Chemother. 2009;53:5303–5.
33. Gonçalves-Pereira J, Silva NE, Mateus A, Pinho C, Póvoa P. Assessment ofpharmacokinetic changes of meropenem during therapy in septic criticallyill patients. BMC Pharmacol Toxicol. 2014;15:21.
34. Conil JM, Georges B, Ravat F, Ruiz S, Seguin T, Metsu D, Fourcade O, SaivinS. Ceftazidime dosage recommendations in burn patients: from apopulation pharmacokinetic approach to clinical practice via Monte Carlosimulations. Clin Ther. 2013;35:1603–12.
35. Isla A, Rodriguez-Gascón A, Trocóniz IF, Bueno L, Solinís MA, Maynar J,Sanchéz-Izquierdo JÁ, Pedraz JL. Population pharmacokinetics ofmeropenem in critically ill patients undergoing continuous renalreplacement therapy. Clin Pharmacokinet. 2008;47:173–80.
36. Udy AA, Roberts JA, Lipman J. Clinical implications of antibiotic pharmacokineticprinciples in the critically ill. Intensive Care Med. 2013;39:2070–82.
37. Carlier M, Carrette S, Stove V, Verstraete AG. Does consistent piperacillindosing result in consistent therapeutic concentrations in critically illpatients? A longitudinal study over an entire antibiotic course. Int JAntimicrob Agents. 2014;43:470–3.
38. Burkhardt O. Ertapenem in critically ill patients with early-onset ventilator-associated pneumonia: pharmacokinetics with special consideration of free-drug concentration. J Antimicrob Chemother. 2007;59:277–84.
39. Ulldemolins M, Kumar V, Majcher-Peszynska J, Drewelow B, Derendorf H,Welte T. Flucloxacillin dosing in critically ill patients with hypoalbuminemia:special emphasis on unbound pharmacokinetics. J Antimicrob Chemother.2010;65:1771–8.
40. Taccone FS, Laterre PF, Dugernier T, Spapen H, Delattre I, Wittebole X, DeBacker D, Layeux B, Wallemacq P, Vincent JL, Jacobs F. Insufficient β-lactamconcentrations in the early phase of severe sepsis and septic shock. CritCare. 2010;14:R126.
41. Hanes SD, Wood C, Herring V, Croce MA, Fabian TC, Pritchard E, BoucherBA. Intermittent and continuous ceftazidime infusion for critically ill traumapatients. Am J Surg. 2000;179:436–40.
42. Garot D, Respaud R, Lanotte P, Simon N, Mercier E, Ehrmann S, Perrotin D,Dequin PF, Le Guellec C. Population pharmacokinetics of ceftriaxone incritically ill septic patients: a reappraisal. British J Clin Pharm. 2011;72:758–67.
43. Conil JM, Georges B, Mimoz O, Dieye E, Ruiz S, Cougot P, Samii K, Houin G,Saivin S. Influence of renal function on trough serum concentrations ofpiperacillin in intensive care unit patients. Intensive Care Med. 2006;32:2063–6.
44. Kees MG, Minichmayr I, Moritz S, Beck S, Wicha SG, Kees F, Kloft C, Steinke T.Population pharmacokinetics of meropenem during continuous infusion insurgical ICU patients. J Clin Pharmacol. 2016;56:307–15.
45. Ramon-Lopez A, Allen JM, Thompson AH, Dheansa BS, James SE, HanlanGW, Davies JG. Dosing regimen of meropenem for adults with severe burns:a population pharmacokinetic study with Monte Carlo simulations. JAntimicrob Chemother. 2015;70:882–90.
46. Blot S, Lipman J, Roberts DM, Roberts JA. The influence of acute kidneyinjury on antimicrobial dosing in critically ill patients: are dose reductionsalways necessary? Diagn Microbiol Infect Dis. 2014;79:77–84.
47. Roberts JA, Pea F, Lipman J. Clin Pharmacokinet. 2013;52:1–8.48. Udy AA. Are standard doses of piperacillin sufficient for critically ill patients
with augmented creatinine clearance? Crit Care. 2015:19–28.49. Udy AA, Lipman J, Jarret P, Klein K, Wallis SC, Patel K, Kirkpatrick CMJ, Kruger
PS, Paterson DL, Roberts MS, Roberts JA. Augmented renal clearance in theintensive care unit: an illustrative case series. Int J Antimicrob Agents. 2010;35:606–8.
50. Huttner A, Von Dach E, Renzoni A, Huttner B, Affaticati M, Pagani L, Daali Y,Pugin J, Karmime A, Fathi M, Lew D, Harbarth S. Augmented renalclearance, low Beta-lactam concentrations and clinical outcomes in thecritically ill: An observational prospective cohort study. Int J AntimicrobAgents. 2015;45:385–39.
51. Carlier M, Carrette S, Roberts JA, Stove V, Verstraete A, Hoste E, Depuydt P,Decruyenaere J, Lipman J, Wallis SC, De Waele JJ. Meropenem andpiperacillin/tazobactam prescribing in critically ill patients: does augmented
Veiga and Paiva Critical Care (2018) 22:233 Page 29 of 34

renal clearance affect pharmacokinetic/pharmacodynamic target attainmentwhen extended infusions are used? Crit Care. 2013;17:R84.
52. Kikuchi E, Kikuchi J, Nasuhara Y, Oizumi S, Ishizaka A, Nishimura M.Comparison of the pharmacodynamics of biapenem in bronchial epitheliallining fluid in healthy volunteers given half-hour and three-hourintravenous infusions. Antimicrob Agents Chemother. 2009;53:2799–803.
53. Mimoz O, Soreda S, Padoin C, Tod M, Petitjean O, Benhamou D. Ceftriaxonepharmacokinetics during iatrogenic hydroxyethyl starch-inducedhypoalbuminemia. Anesthesiology. 2000;93:735–43.
54. Udy AA, Varghese JM, Altukroni M, Briscoe S, McWhinney BC, Ungerer JP,Lipman J, Roberts JA. Subtherapeutic initial b-lactam concentrations inselect critically ill patients. Association between augmented renal clearanceand low trough drug concentrations. Chest. 2012;142:30–9.
55. Wong G, Briscoe S, Adnan S, McWhinney B, Ungerer J, Lipman J, Roberts JA.Protein binding of beta-lactam antibiotics in critically ill patients: can wesuccessfully predict unbound concentrations? Antimicrob AgentsChemother. 2013;57:6165–70.
56. Schleibinger M, Steinbach C, Topper C, Kratzer A, Liebchen U, Kees F,Salzberger B, Kees MG. Protein binding characteristics and pharmacokinetics ofceftriaxone in intensive care unit patients. Br J Clin Pharmacol. 2015;80:525–33.
57. Matuszkiewicz-Rowińska J. Dosing of antibiotics in critically ill patients: arewe left to wander in the dark? Polskie Archiwum Medycyny Wewnetrzney.2012;122:630–40.
58. Fissell WH. Antimicrobial dosing in acute renal replacement. Adv ChronicKidn Dis. 2013; https://doi.org/10.1053/j.ackd.2012.10.004.
59. Eyler RF, Mueller BA. Antimicrobial dosing in critically ill patients with acutekidney injury. Nat Rev Nephrol. 2011;7:226–35.
60. Lewis SJ, Mueller BA. Antibiotic dosing in critically ill patients receivingCRRT: underdosing is overprevalent. Semin Dial. 2014;27:441–5.
61. Harris LE, Reavesa AB, Kraussa AG, Grinerb J, Hudson JQ. Evaluation ofantibiotic prescribing patterns in patients receiving sustained low-efficiencydialysis: opportunities for pharmacists. Int J Pharm Pract. 2013;21:55–61.
62. Morabito S, Guzzo I, Vitaliano E, Muzi L, Solazzo A, Pistolesi V, Pierucci A.Farmacocinetica degli Antibiotici nelle Terapie Sostitutive Renali Continue(CRRT). Gionale Italiano di Nefrologia. 2012;29:425–44.
63. Morabito S, Guzzo I, Vitaliano E, Muzi L, Solazzo A, Pistolesi V, Pierucci A.Principi di farmacocinetica e aggiustamento posologico dei farmaci nelleterapie sostitutive renali continue (CRRT). Giornale Italiano di Nefrologia.2006;36:S127–38.
64. Choi G, Gomersall CD, Tian Q, Joynt GM, Freebairn R, Lipman J. Principles ofantibacterial dosing in continuous renal replacement therapy. Crit CareMed. 2009;37:2268–82.
65. Hites M, Dell’Anna AM, Scolletta S, Taccone FS. The challenges of multipleorgan dysfunction syndrome and extra-corporeal circuits for drug deliveryin critically ill patients. Adv Drug Deliv Rev. 2014;77:12–21.
66. Jamal J-A, Udy AA, Lipman J, Roberts JA. The impact of variation in renalreplacement therapy settings on piperacillin, meropenem, and vancomycindrug clearance in the critically ill: an analysis of published literature anddosing regimens. Crit Care Med. 2014;42:1640–50.
67. Fish DN, Teitelbaum I, Abraham E. Pharmacokinetics andpharmacodynamics of imipenem during continuous renal replacementtherapy in critically ill patients. Antimicrob Agents Chemother. 2005;49:2421–8.
68. Malone RS, Fish DN, Abraham E, Teitelbaum I. Pharmacokinetics of cefepimeduring continuous renal replacement therapy in critically ill patients.Antimicrob Agents Chemother. 2001;45:3148–55.
69. Mueller SC, Majcher-Peszynska J, Hickstein H, Francke A, Pertschy A, SchulzA, Mundkowski R, Drewelow B. Pharmacokinetics of piperacillin-tazobactamin anuric intensive care patients during continuous venovenoushemodialysis. Antimicrob Agents Chemother. 2002;46:1557–60.
70. Roberts DM, Roberts JA, Roberts MS, Liu X, Nair P, Cole L, Lipman J, BellomoR, on behalf of the RENAL Replacement Therapy Study Investigators.Variability of antibiotic concentrations in critically ill patients receivingcontinuous renal replacement therapy: A multicentre pharmacokineticstudy. Crit Care Med. 2012;40:1523–8.
71. Banyai M, Thalhammer F, El Menyawi I, Heinz G, Traunmüller F, SiostrzonekP. Pharmacokinetics of cefpirome during continuous venovenoushemofiltration: Rationale for an 8-hour dosing interval. Clin PharmacolTherapeut. 2000;67:368–72.
72. Eyler RF, Vilay AM, Nader AM, Heung M, Pleva M, Sowinski KM, DePestel DD,Sörgel F, Kinzig M, Mueller BA. Pharmacokinetics of ertapenem in critically ill
patients receiving continuous venovenous hemodialysis orhemodiafiltration. Antimicrob Agents Chemother. 2014;58:1320–6.
73. Vossen MG, Wenisch JM, Maier-Salamon A, Fritsch A, Saria K, Zuba C, Jilch S,Lemmerer R, Unger M, Jaehde U, Jäger W, Thalhammer F. Doripenemtreatment during continuous renal replacement therapy. Antimicrob AgentsChemother. 2016;60:1687–94.
74. Carlier M, Taccone FS, Beumier M, Seylerd L, Cottone F, Jacobs F, RobertsJA. Population pharmacokinetics and dosing simulations of cefepime inseptic shock patients receiving continuous renal replacement therapy. Int JAntimicrob Agents. 2015;46:413–9.
75. Seyler L, Cotton F, Taccone FS, De Backer D, Macours P, Vincent J-L,Jacobs F. Recommended b-lactam regimens are inadequate in septicpatients treated with continuous renal replacement therapy. Crit Care.2011;15:R137.
76. Roberts DM, Liu X, Roberts JA, Nair P, Cole L, Roberts MS, Lipman L,Bellomo R, on behalf of the RENAL Replacement Therapy StudyInvestigators. A multicenter study on the effect of continuoushemodiafiltration intensity on antibiotic pharmacokinetics. Crit Care. 2015;19:84.
77. Ohchi T, Hidaka S, Goto K, Shitomi R, Nishida T, Abe T, Yamamoto S, YasudaN, Hagiwara S, Noguchi T. Effect of hemopurification rate on doripenempharmacokinetics in critically ill patients receiving high-flow continuoushemodiafiltration. Yakugaku Zasshi. 2011;131:1395–9.
78. Arzuaga A, Maynar J, Gascón AR, Isla A, Corral E, Fonseca F, Sánchez-Izquierdo JA, Rello J, Canut A, Pedraz JL. Influence of renal function on thepharmacokinetics of piperacillin/tazobactam in intensive care unit patientsduring continuous venovenous hemofiltration. J Clin Pharmacol. 2005;45:168–76.
79. Isla A, Maynar J, Sánchez-Izquierdo JA, Gascón AR, Arzuaga A, Corral E,Pedraz JL. Meropenem and continuous renal replacement therapy: in vitropermeability of 2 continuous renal replacement therapy membranes andinfluence of patient renal function on the pharmacokinetics in critically illpatients. J Clin Pharmacol. 2005;45:1294–304.
80. Ulldemolins A, Soy D, Llaurado-Serra M, Vaquer S, Castro P, Rodríguez AH,Pontes C,J, Calvo G, Torres A, Martín-Loeches I. Meropenem populationpharmacokinetics in critically ill patients with septic shock and continuousrenal replacement therapy: influence of residual diuresis on doserequirements. Antimicrob Agents Chemother. 2015;59:5520–8.
81. Bouman CSC, van Kan HJM, Koopmans RP, Korevaar JC, Schultz MJ, VroomMB. Discrepancies between observed and predicted continuousvenovenous hemofiltration removal of antimicrobial agents in critically illpatients and the effects on dosing. Intensive Care Med. 2006;32:2013–9.
82. Kielstein JT, Czock D, Schöpke T, Hafer C, Bode-Böger SM, Kuse E, Keller F,Fliser D. Pharmacokinetics and total elimination of meropenem andvancomycin in intensive care unit patients undergoing extended dailydialysis. Crit Care Med. 2006;34:51–6.
83. Lorenzen JM, Broll M, Kaever V, Burhenne H, Hafer C, Clajus C, Knitsch W,Burkhardt O, Kielstein JT. Pharmacokinetics of ampicillin/sulbactam incritically ill patients with acute kidney injury undergoing extended dialysis.Clin J Am Soc Nephrol. 2012;7:385–90.
84. Burkhardt O, Hafer C, Langhoff A, Kaever V, Kumar V, Welte T, Haller H, FliserD, Kielstein JT. Pharmacokinetics of ertapenem in critically ill patients withacute renal failure undergoing extended daily dialysis. Nephrol DialTransplant. 2009;24:267–71.
85. Tamme K, Oselin K, Kipper K, Tasa T, Metsvaht T, Karjagin J, Herodes K, KernH, Starkopf J. Pharmacokinetics and pharmacodynamics of piperacillin/tazobactam during high volume haemodiafiltration in patients with septicshock. Acta Anaesthesiol Scand. 2016;60:230–40.
86. Bourquin V, Ponte B, Saudan P, Martin P-Y. Adaptation posologique desmédicaments couramment utilise’s en réanimation lors d’épurationextrarénale continue. Néphrol Thérapeut. 2009;5:533–41.
87. Trotman RL, Williamson JC, Shoemaker DM, Salzer WL. Antibiotic dosing incritically ill adult patients receiving continuous renal replacement therapy.Clin Infect Dis. 2005;41:1159–66.
88. Brett H, Matzke GR, Dager WE. Antimicrobial dosing concepts andrecommendations for critically ill adult patients receiving continuous renalreplacement therapy or intermittent hemodialysis. Pharmacotherapy. 2009;29:562–77.
89. De Waele JJ, Carlier M. Beta-lactam antibiotic dosing during continuousrenal replacement therapy: how can we optimize therapy? Crit Care. 2014;18:158.
Veiga and Paiva Critical Care (2018) 22:233 Page 30 of 34

90. Kielstein JT, Burkhardt O. Dosing of antibiotics in critically ill patients undergoingrenal replacement therapy. Curr Pharm Biotechnol. 2011;12:2015–9.
91. Churchwell MD, Mueller BA. Drug dosing during continuous renalreplacement therapy. Semin Dial. 2009;22:185–8.
92. Vossen MF, Thalhammer F. Effects of renal replacement therapy onantimicrobial therapy. Curr Clin Pharmacol. 2013;8:39–45.
93. Goldstein SL, Nolin TD. Lack of drug dosing guidelines for critically illpatients receiving continuous renal replacement therapy. Clin PharmacolTherapeut. 2014;96:159–61.
94. Scoville BA, Mueller BA. Medication dosing in critically ill patients with acutekidney injury treated with renal replacement therapy. Am J Kidney Dis.2013;61:490–500.
95. Mueller BA, Pasko DA, Sowinski KM. Higher renal replacement therapy dosedelivery influences on drug therapy. Artif Organs. 2003;27:808–14.
96. Ulldemolins M, Vaquer S, Llauradó-Serra M, Pontes C, Calvo G, Soy D,Martín-Loeches I. Beta-lactam dosing in critically ill patients with septicshock and continuous renal replacement therapy. Crit Care. 2014;18:227.
97. Shekar, Fraser JF, Smith MT, Roberts JA. Pharmacokinetic changes inpatients receiving extracorporeal membrane oxygenation. doi: https://doi.org/10.1016/j.jcrc.2012.02.013.
98. Shekar K, Roberts JA, Mcdonald CI, Fisquet S, Barnett AG, Mullany DV,Ghassabian S, Wallis SC, Fung YL, Smith MT, Fraser JF. Sequestration ofdrugs in the circuit may lead to therapeutic failure during extracorporealmembrane oxygenation. Crit Care. 2012;16:R194.
99. Dzierba AL, Abrams D, Brodie D. Medicating patients during extracorporealmembrane oxygenation: the evidence is building. Crit Care. 2017;21:66.
100. Donadello K, Antonucci E, Cristallini S, Roberts JA, Beumier M, Scolletta S,Jacobs F, Rondelet B, de Backer D, Vincent J-L, Taccone FS. β-Lactampharmacokinetics during extracorporeal membrane oxygenation therapy: Acase–control study. Int J Antimicrob Agents. 2015; 45: 278–282.
101. Shekar K, Fraser JF, Taccone FS, Welch S, Wallis SC, Mullany DV, Lipman J,Roberts JA, and on behalf of the ASAP ECMO Study Investigators. Thecombined effects of extracorporeal membrane oxygenation and renalreplacement therapy on meropenem pharmacokinetics: a matched cohortstudy. Crit Care. 2014;18:565.
102. Welsch C, Augustin P, Allyn J, Massias L, Montravers P, Allou N. Alveolar andserum concentrations of imipenem in two lung transplant recipients supportedwith extracorporeal membrane oxygenation. Transpl Infect Dis. 2015;17:103–5.
103. Perrott J, Mabasa VH, Ensom MHH. Comparing outcomes ofmeropenem administration strategies based on pharmacokinetic andpharmacodynamic principles: a qualitative systematic review. AnnPharmacother. 2010;44:557–64.
104. Mah GT, Mabasa VH, Chow I, Ensom MHH. Evaluating outcomes associatedwith alternative dosing strategies for piperacillin/tazobactam: a qualitativesystematic review. Ann Pharmacother. 2012;46:265–75.
105. Burgess SV, Mabasa VH, Chow I, Ensom MHH. Evaluating outcomes ofalternative dosing strategies for cefepime: a qualitative systematic review.Ann Pharmacother. 2015; https://doi.org/10.1177/1060028014564179.
106. Bauer KA, West JE, O’Brien JM, Goff DA. Extended-infusion cefepime reducesmortality in patients with Pseudomonas aeruginosa Infections. AntimicrobAgents Chemother. 2013;57:2907–12.
107. Roberts JA, Boots R, Rickard CM, Thomas P, Quinn J, Roberts DM, Richards B,Lipman J. Is continuous infusion ceftriaxone better than once-a-day dosingin intensive care? A randomized controlled pilot study. J AntimicrobChemother. 2007;59:285–91.
108. Lorente L, Lorenzo L, Martín MM, Jiménez A, Mora ML. Meropenem bycontinuous versus intermittent infusion in ventilator-associated pneumoniadue to Gram-negative bacilli. Ann Pharmacother. 2006;40:219–23.
109. Roberts JA, Kirkpatrick CMJ, Roberts MS, Robertson TA, Dalley AJ, Lipman J.Meropenem dosing in critically ill patients with sepsis and without renaldysfunction: intermittent bolus versus continuous administration? MonteCarlo dosing simulations and subcutaneous tissue distribution. J AntimicrobChemother. 2009;64:142–50.
110. Rafati MR, Rouini MR, Mojtahedzadeh M, Najafi A, Tavakoli H, Gholami K,Fazeli MR. Clinical efficacy of continuous infusion of piperacillin comparedwith intermittent dosing in septic critically ill patients. Int J AntimicrobAgents. 2006;28:122–7.
111. Duszynskaa W, Taccone FS, Switala M, Hurkacz M, Kowalska-Krochmal B,Kübler A. Continuous infusion of piperacillin/tazobactam in ventilator-associated pneumonia: a pilot study on efficacy and costs. Int J AntimicrobAgents. 2012;39:153–8.
112. Roberts JA, Kirkpatrick CMJ, Roberts MS, Dalley AJ, Lipman J. First-dose andsteady-state population pharmacokinetics and pharmacodynamics ofpiperacillin by continuous or intermittent dosing in critically ill patients withsepsis. J Antimicrob Agents. 2010;35:156–63.
113. Chytra I, Stepan M, Benes J, Pelnar P, Zidkova A, Bergerova T, Pradl R, KasalE. Clinical and microbiological efficacy of continuous versus intermittentapplication of meropenem in critically ill patients: a randomized open-labelcontrolled trial. Crit Care. 2012;16:R113.
114. Falagas ME, Tansarli GS, Ikawa K, Vardakas KZ. Clinical outcomes withextended or continuous versus short-term intravenous infusion ofcarbapenems and piperacillin/tazobactam: a systematic review and meta-analysis. Clin Infect Dis. 2013;56:272–82.
115. Lorente L, Jimenez A, Palmero S, Jimenez JJ, Iribarren JL, Santana M, MartinMM, Mora ML. Comparison of clinical cure rates in adults with ventilator-associated pneumonia treated with intravenous ceftazidime administeredby continuous or intermittent infusion: a retrospective, nonrandomized,open-label, historical chart review. Clin Ther. 2007;29:2433–9.
116. Dulhunty JM, Roberts JA, Davis JS, Webb SAR, Bellomo R, Gomersall C,Shirwadkar C, Eastwood GM, Myburgh J, Paterson DL, Lipman J. Continuousinfusion of beta-lactam antibiotics in severe sepsis: a multicenter double-blind, Randomized Controlled Trial. Clin Infect Dis. 2013;56:236–44.
117. Gonçalves-Pereira J, Oliveira BS, Janeiro S, Estilita J, Monteiro C, Salgueiro A, VieiraA, Gouveia J, Paulino C, Bento L, Póvoa P. Continuous infusion of piperacillin/tazobactam in septic critically ill patients—a multicenter propensity matchedanalysis. PLoS One. 2012;7:e4984. https://doi.org/10.1371/journal.pone.0049845.
118. Abdul-Aziz MH, Staatz CE, Kirkpatrick CMJ, Lipman J, Roberts JA. Continuousinfusion vs. bolus dosing: implications for beta-lactam antibiotics. MinervaAnestesiol. 2012;78:94–10.
119. Nicolau DP, McNabb J, Lacy MK, Quintiliani R, Nightingale CH. Continuousversus intermittent administration of ceftazidime in intensive care unitpatients with nosocomial pneumonia. Int J Antimicrob Agents. 2001;17:497–504.
120. Huang H, Hang S, Zhu P, Xi X. Continuous versus intermittent infusion ofcefepime in neurosurgical patients with post-operative intracranialinfections. Int J Antimicrob Agents. 2014;43:68–72.
121. van Zanten ARH, Oudijk M, Nohlmans-Paulssen MKE, van der Meer YG,Girbes ARJ, Polderman KH. Continuous vs. intermittent cefotaximeadministration in patients with chronic obstructive pulmonary disease andrespiratory tract infections: pharmacokinetics/pharmacodynamics, bacterialsusceptibility and clinical efficacy. Br J Clin Pharmacol. 2006;63:100–9.
122. Lee GC, Liou H, Yee R, Quan CF, Neldner K. Outcomes of extended-infusionpiperacillin-tazobactam: a retrospective analysis of critically ill patients. ClinTher. 2012;34:2297–300.
123. Jaruratanasirikul S, Limapichat T, Jullangkoon M, Aeinlang N, Ingviya N,Wongpoowarak W. Pharmacodynamics of meropenem in critically illpatients with febrile neutropenia and bacteraemia. Int J Antimicrob Agents.2011;38:231–6.
124. Angus BJ, Smith MD, Suputtamongkol Y, Mattie H, Walsh AL, WuthiekanunV, Chaowagul W, White NJ. Pharmacokinetic-pharmacodynamic evaluationof ceftazidime continuous infusion vs intermittent bolus injection insepticaemic melioidosis. Br J Clin Pharmacol. 2000;49:184–91.
125. Roos JF, Bulitta J, Lipman J, Kirkpatrick CMJ. Pharmacokinetic-pharmacodynamic rationale for cefepime dosing regimens in intensive careunits. J Antimicrob Chemother. 2006;58:987–93.
126. Breilh D, Fleureau C, Gordien J-B, Joanes-Boyau O, Texier-Maugein J,Rapaport S, Boselli E, Janvier G, Saux M-C. Pharmacokinetics of freeertapenem in critically ill septic patients: intermittent versus continuousinfusion. Minerva Anestesiol. 2011;77:1058–62.
127. Roberts JA, Roberts MS, Robertson TA, Daley AJ, Lipman J. Piperacillinpenetration into tissue of critically ill patients with sepsis—Bolus versuscontinuous administration? Crit Care Med. 2009;37:926–33.
128. Lodise TP, Lomaestro B, Drusano GL. Piperacillin-tazobactam forPseudomonas aeruginosa infection: clinical implications of an extended-infusion dosing strategy. Clin Infect Dis. 2007;44:357–63.
129. Sakka SG, Glauner AK, Bulitta JB, Kinzig-Schippers M, Pfister W, Drusano GL,Sorgel F. Population pharmacokinetics and pharmacodynamics ofcontinuous versus short-term infusion of imipenem-cilastatin in critically illpatients in a randomized, controlled trial. Antimicrob Agents Chemother.2007;51:3304–10.
130. Nicasio AM, Ariano RE, Zelenitski SA, Kim A, Crandon JL, Kuti JL, Nicolau DP.Population pharmacokinetics of high-dose, prolonged-infusion cefepime in
Veiga and Paiva Critical Care (2018) 22:233 Page 31 of 34

adult critically ill patients with ventilator-associated pneumonia. AntimicrobAgents Chemother. 2009;53:1476–81.
131. Arnold HM, Hollands JM, Skrupky LP, Smith JR, Juang PH, Hampton NB,McCormick S, Reichley RM, Hoban A, Hoffman J, Micek ST, Kollef MH.Prolonged infusion antibiotics for suspected Gram-negative infections in theICU: a before-after study. Ann Pharmacother. 2013;47:170–80.
132. Yusuf E, Spapen H, Piérard D. Prolonged vs. intermittent infusion ofpiperacillin/tazobactam in critically ill patients: A narrative and systematicreview. J Crit Care. 2014;29:1089–95.
133. Cheatham SC, Fleming MR, Healy DP, Kyoung E, Shea KM, Humphrey ML,Kays MB. Steady-state pharmacokinetics and pharmacodynamics ofmeropenem in morbidly obese patients hospitalized in an intensive careunit. J Clin Pharmacol. 2013;54:324–30.
134. Laterre P-F, Wittebole X, Van de Velde S, Muller AE, Mouton JW, Carryn S,Tulkens PM, Dugernir T. Temocillin (6 g daily) in critically ill patients:continuous infusion versus three times daily administration. J AntimicrobChemother. 2015;70:891–8.
135. Langgartner J, Lehn N, Gluck T, Herzig H, Kees F. Comparison of thepharmacokinetics of piperacillin and sulbactam during intermittent andcontinuous intravenous infusion. Chemotherapy. 2007;53:370–7.
136. Langgartner J, VasoldA, Glück T, Reng M, Kees F. Pharmacokinetics ofmeropenem during intermittent and continuous intravenous application inpatients treated by continuous renal replacement therapy. Int Care Med.2008; 34:1091–96.
137. Langgartner J, Vasold A, Glück T, Reng M, Kees F. Pharmacokinetics ofmeropenem during intermittent and continuous intravenous application inpatients treated by continuous renal replacement therapy. Intens Care Med.2008;34:1091–6.
138. Jamal J-A, Mat-Nor MB, Mohamad-Nor F-S, Udy AA, Wallis SC, Lipman J,Roberts JA. Pharmacokinetics of meropenem in critically ill patientsreceiving continuous venovenous haemofiltration: A randomised controlledtrial of continuous infusion versus intermittent bolus administration. Int JAntimicrob Agents. 2015;45:41–5.
139. Asín-Prieto E, Rodriguez-Gasco A, Tracóniz I, Soraluce A, Maynar J, Sánchez-Izquierdo JA, Isla A. Population pharmacokinetics of piperacillin andtazobactam in critically ill patients undergoing continuous renalreplacement therapy: application to pharmacokinetic/pharmacodynamicanalysis. J Antimicrob Chemother. 2014;69:180–9.
140. Obrink-Hansen K, Juul RV, Storgaard M, Thomsen MK, Hardlei TF, Brock B,Kreilgaard M, Gjedsted J. Population pharmacokinetics of piperacillin in theearly phase of septic shock: does standard dosing result in therapeuticplasma concentrations? Antimicrob Agents Chemother. 2015;59:7018–26.
141. D’Agostino C, Rhodes NJ, Skoglund E, Roberts JA. Microbiologic clearancefollowing transition from standard infusion piperacillin-tazobactam toextended-infusion for persistent Gram- negative bacteremia and possibleendocarditis: A case report and review of the literature. J Infect Chemother.2015;21:742–6.
142. Lips M, Siller M, Strojil J, Urbánek K, Balík M, Suchánková H.Pharmacokinetics of imipenem in critically ill patients during empiricaltreatment of nosocomial pneumonia: A comparison of 0.5-h and 3-hinfusions. Int J Antimicrob Agents. 2014;44:358–62.
143. De Waele J, Carlier M, Hoste E, Depuydt P, Decruyenaere J, Wallis SC,Lipman J, Roberts JA. Extended versus bolus infusion of meropenem andpiperacillin: a pharmacokinetic analysis. Minerva Anestesiol. 2014;80:1302–9.
144. Dulhunty JM, Roberts JA, Davis JS, SAR W, Bellomo R, Gomersall C,Shirwadkar C, Eastwood GM, Myburgh J, Paterson DL, Starr T, Paul SK,Lipman J, for the BLING II Investigators for the ANZICS Clinical Trials Group.A multicenter randomized trial of continuous versus intermittent b-lactaminfusion in severe sepsis. Am J Respir Crit Med. 2015;192:1298–305.
145. Abdul-Aziz MH, Lipman J, Akova M, Bassetti M, De Waele JJ, Dimopoulos G,Dulhunty J, Kaukonen K-M, Koulenti D, Martin C, Montravers P, Rello J,Rhodes A, Starr T, Wallis SC, Roberts JA, on behalf of the DALI Study Group.Is prolonged infusion of piperacillin/tazobactam and meropenem incritically ill patients associated with improved pharmacokinetic/pharmacodynamic and patient outcomes? An observation from theDefining Antibiotic Levels in Intensive care unit patients (DALI) cohort. JAntimicrob Chemother. 2016;71:196–207.
146. Boyadjiev I, Boulamery A, Simon N, Martin C, Bruguerolle B, Leone M.Penetration of ertapenem into muscle measured by in vivo microdialysis inmechanically ventilated patients. Antimicrob Agents Chemother. 2011;55:3573–5.
147. Karjagin J, Lefeuvre S, Oselins K, Kipper K, Marchand S, Tikkerberi A, StarkopfJ, Coue W, Sawchuk RJ. Pharmacokinetics of meropenem determined bymicrodialysis in the peritoneal fluid of patients with severe peritonitisassociated with septic shock. Clin Pharmacol Ther. 2008;83:452–9.
148. Zeitlinger MA, Erovic BM, Sauermann R, Georgopoulos A, Muller M,Joukhadar C. Plasma concentrations might lead to overestimation of targetsite activity of piperacillin in patients with sepsis. J Antimicrob Chemother.2005;56:703–8.
149. Goldwater PN. Cefotaxime and ceftriaxone cerebrospinal fluid levels duringtreatment of bacterial meningitis in children. Int J Antimicrob Agents. 2005;26:408–11.
150. Do L, Udy AA, Roberts JA, Lipman J. Antibacterial therapeutic drugmonitoring in cerebrospinal fluid: difficulty in achieving adequate drugconcentrations. J Neurosurg. 2013;118:297–301.
151. Abdul-Aziz MH, McDonald C, McWhinney B, Ungerer JPJ, Lipman J, RobertsJA. Low flucloxacillin concentrations in a patient with central nervoussystem infection: the need for plasma and cerebrospinal fluid drugmonitoring in the ICU. Ann Pharmacother. 2014;48:1380–4.
152. Cies JJ, Moore WS, Calaman S, Brown M, Narayan P, Parker J, Chopra A.Pharmacokinetics of continuous-infusion meropenem for the treatment ofSerratia marcescens ventriculitis in a pediatric patient. Pharmacotherapy.2015;35:e32–6.
153. Dahyot-Fizelier C, Frasca D, Grégoire N, Adier C, Mimoz O, Debaene B,Couet W, Marchand S. Microdialysis study of cefotaxime cerebraldistribution in patients with acute brain injury. Antimicrob AgentsChemother. 2013;6:2738–42.
154. Morita A, Kamei S, Minami M, Yoshida K, Kawabata S, Kuroda H, Suzuki Y,Araki N, Iwasaki Y, Kobayashi R, Hayashi N, Hirayama T, Ochiai J, Ueda M,Yamagishi Y, Niwa J, Shindo K, Fukushima Y, Takita T, Sato T, Sato S, MikamoH, Iwata S. Open-label study to evaluate the pharmacodynamics, clinicalefficacy, and safety of meropenem for adult bacterial meningitis in Japan. JInfect Chemother. 2014;20:535–40.
155. Tsumura R, Ikawa K, Morikawa N, Ikeda K, Shibukawa M, Iida K, Kurisu K. Thepharmacokinetics and pharmacodynamics of meropenem in thecerebrospinal fluid of neurosurgical patients. J Chemother. 2008;20:615–21.
156. Nicasio AM, Quintiliani R Jr, DeRyke CA, Kuti JL, Nicolau DP. Treatment ofSerratia marcescens meningitis with prolonged infusion of meropenem.Ann Pharmacother. 2007;41:1077–81.
157. Frasca D, Dahyot-Fizelier C, Couet W, Debaene B, Mimoz O, Marchand S.Brain microdialysis distribution study of cefotaxime in a patient withtraumatic brain injury. Br J Anesthesiol. 2012;109:830–1.
158. Wang Q, Wu Y, Chen B, Zhou J. Drug concentrations in the serum andcerebrospinal fluid of patients treated with cefoperazone/sulbactam aftercraniotomy. BMC Anesthesiol. 2015;15:33.
159. Rodvold KA, Nicolau DP, Lodise TP, Khashab M, Noel GJ, Kahn JB, GotfriedM, Murray SA, Nicholson S, Laohavaleeson S, Tessier PR, Drusano GL.Identifying exposure targets for treatment of staphylococcal pneumoniawith ceftobiprole. Antimicrob Agents Chemother. 2009;53:3294–301.
160. Bayat S, Louchahi K, Verdière B, Anglade D, Rahoui A, Sorin P-M, Tod M,Petitjean O, Fraisse F, Grimbert FA. Comparison of 99mTc-DTPA and urea formeasuring cefepime concentrations in epithelial lining fluid. Eur Respir J.2004;24:150–6.
161. Boselli E, Breilh B, Rimmelé T, Guillaume C, Xuereb F, Saux M-C, Bouvet L,Chassard D, Allaouchiche B. Alveolar concentrations of piperacillin/tazobactam administered in continuous infusion to patients with ventilator-associated pneumonia. Crit Care Med. 2008;36:1500–6.
162. Cousson J, Floch T, Guillard T, Vernet V, Raclot P, Wolak-Thierry A, Jolly D.Lung concentrations of ceftazidime administered by continuous versusintermittent infusion in patients with ventilator-associated pneumonia.Antimicrob Agents Chemother. 2015;59:1905–9.
163. Burkhardt O, Majcher-Peszynska J, Borner K, Mundkowski R, Drewelow B,Derendorf H, Welte T. Penetration of ertapenem into different pulmonarycompartments of patients undergoing lung surgery. J Clin Pharmacol. 2005;45:659–65.
164. Boselli E, Breilh D, Saux M-C, Gordien J-B, Allaouchiche B. Pharmacokineticsand lung concentrations of ertapenem in patients with ventilator-associatedpneumonia. Intensive Care Med. 2006;32:2059–62.
165. Boselli E, Breilh D, Rimmel T, Poupelin J-C, Saux M-C, Chassard D,Allaouchiche A. Plasma and lung concentrations of ceftazidimeadministered in continuous infusion to critically ill patients with severenosocomial pneumonia. Intensive Care Med. 2004;30:989–91.
Veiga and Paiva Critical Care (2018) 22:233 Page 32 of 34

166. Felton TW, McCalman K, Malagon I, Isalska B, Whalley S, Goodwin J, BentleyAM, Hope WW. Pulmonary penetration of piperacillin and tazobactam incritically ill patients. Clin Pharmacol Ther. 2014;96:438–48.
167. Boselli, et al. Steady-state plasma and intrapulmonary concentrations ofcefepime administered in continuous infusion in critically ill patients withsevere nosocomial pneumonia. Crit Care Med. 2003;31(8):2102–6.
168. Boselli E, Breilh D, Cannesson M, Xuereb F, Rimmel T, Chassard D, Saux M-C,Allaouchiche B. Steady-state plasma and intrapulmonary concentrations ofpiperacillin/tazobactam 4 g/0.5 g administered to critically ill patients withsevere nosocomial pneumonia. Intens Care Med. 2004;30:976–9.
169. Lodise TP, Kinzig-Schippers M, Drusano GL, Loos U, Vogel F, Bulitta J, HinderM, Sorgel F. Use of population pharmacokinetic modeling and Monte Carlosimulation to describe the pharmacodynamic profile of cefditoren in plasmaand epithelial lining fluid. Antimicrob Agents Chemother. 2008;52:1945–51.
170. Xiao AJ, Caro L, Popejoy MW, Huntigton JA, Kullar R. PK/PD targetattainment with ceftolozane/tazobactam using Monte Carlo simulation inpatients with various degrees of renal function, including augmented renalclearance and end-stage renal disease. Infect Dis Ther. 2017;6:137–48.
171. Chandorkar G, Xiao AJ, Mouksassi M-S, Hershberger E, Krishna G. Populationpharmacokinetics of ceftolozane/tazobactam in healthy volunteers, subjectswith varying degrees of renal function and patients with bacterialinfections. J Clin Pharmacol. 2015;55:230–9.
172. Van Duin B, Bonomo RA. Ceftazidime/avibactam and ceftolozane/tazobactam: second-generation β-lactam/β-lactamase inhibitorcombinations. Clin Infect Dis. 2016;63:234–41.
173. Xiao AJ, Miller BW, Huntington JA, Nicolau DP. Ceftolozane/tazobactampharmacokinetic/pharmacodynamic-derived dose justification for phase 3studies in patients with nosocomial pneumonia. J Clin Pharmacol. 2016;56:56–66.
174. Veillette JJ, Truong J, Forland SC. Pharmacokinetics of ceftazidime-Avibactam in two patients with KPC-Producing Klebsiella pneumoniaeBacteremia and renal Impairment. Pharmacotherapy. doi:org/https://doi.org/10.1002/phar.1840.
175. Oliver WD, Heil EL, Gonzales JP, Mehrotra S, Robinett K, Saleeb P, NicolauDP. Ceftolozane-tazobactam pharmacokinetics in a critically ill patient oncontinuous venovenous hemofiltration. Antimicrob Agents Chemother.2016;60:1899–901.
176. Bremmer DN, Nicolau DP, Burcham P, Chunduri A, Shidham G, Bauer KA.Ceftolozane/tazobactam pharmacokinetics in a critically ill adult receivingcontinuous renal replacement therapy. Pharmacotherapy. Doi.org/https://doi.org/10.1002/phar.1744.
177. Stokem K, Zuckerman JB, Nicolau DP, Wungwattana M, Sears EH. Use ofceftolozane-tazobactam in a cystic fibrosis patient with multidrugresistantpseudomonas infection and renal insufficiency. Respir Med Case Rep. 2018;23:8–9.
178. Fugate JE, Kalimullah EA, Hocker SE, Clark SL, Wijdicks EFM, Rabinstein AA.Cefepime neurotoxicity in the intensive care unit: a cause of severe,underappreciated encephalopathy. Crit Care. 2013;17:R264.
179. Shaheen T, Volles D, Calland F, Sifri CD, Mytinger J, Hagspiel K, Sawyer R,Bonati H. Cefepime-associated status epilepticus in an ICU patient withrenal failure. J Chemother. 2009;21:65–7.
180. Alvarez SD, Aragon MCFG, Moreno A, Alonso FP, Cook HJ, Cárdenas G, Soto-Hernández JL. Clinical and electroencephalographic assessment of cefepimeduring treatment of nosocomial infections in neurological patients. CentNerv Syst Agents Med Chem. 2011;11:1–5.
181. Finkelsztejn A, Cabral L, Bragatti JÁ, da Silva AV, Schuh AFS. Imipenem-associated encephalopathy. Arquivo Neuropsiquiatria. 2010;68:137–9.
182. Smith NL, Freebairn RC, Park MAJ, Wallis SC, Roberts JA, Lipman J.Therapeutic drug monitoring when using cefepime in continuous renalreplacement therapy: seizures associated with cefepime. Crit Care Resusc.2012;14:312–5.
183. Collins RD, Tverdek FP, Bruno JJ, Coyle EA. Probable nonconvulsive statusepilepticus with the use of high-dose continuous infusion ceftazidime. JPharm Pract. 2016;29:564–8.
184. Beumier M, Casu GS, Hites M, Wolff F, Cotton F, Vincent J-L, Jacobs F,Taccone FS. Elevated β-lactam concentrations associated with neurologicaldeterioration in ICU septic patients. Minerva Anestesiol. 2015;81:497–506.
185. Fritz G, Barner C, Schindler R, Boemke W, Falke K. Amoxicillin-induced acuterenal failure. Nephrol Dial Transp. 2003;18:1660–2.
186. Polderman KH, Girbes ARJ. Piperacillin-induced magnesium and potassiumloss in intensive care unit patients. Intensive Care Med. 2002;28:520–2.
187. Lambden SP, Akeru J, Barrett NA. Acute intravascular hemolysis associatedwith intravenous administration of meropenem in a sixty-year-old man. CanJ Clin Pharmacol. 2010;17:e64–6.
188. Marik PE, Parekh P. Life-threatening piperacillin-induced immune haemolysisin a patient with cystic fibrosis. BMJ Case Rep. 2013; https://doi.org/10.1136/bcr-2012-007801.
189. Yang C-J, Hwang J-J, Hung J-Y, Chong I-W, Huang M-S. Extremethrombocytosis under the treatment by amoxicillin/clavulanate. PharmWorld Sci. 2006;28:326–8.
190. Lim PP, Chong CP, Abdul AN. Cefepime-associated thrombocytopenia in acritically ill patient. Int J Clin Pharmacol. 2011;33:902–4.
191. Macwilliam JL, Mistry R, Floyd MS Jr, Baird AD. Piperacillin/tazobactaminduced thrombocytopaeniaa delayed response. BMJ Case Rep. 2012;https://doi.org/10.1136/bcr.03.2012.5981.
192. Rousan TA, Aldoss IT, Cowley BD Jr, Curtis BR, Bougie DW, Aster RH, George JN.Recurrent acute thrombocytopenia in the hospitalized patient: Sepsis, DIC, HIT,or antibiotic-induced thrombocytopenia. Am J Hematol. 2010;85:71–4.
193. Nguyen VD, Tourigny JF, Roy R, Brouillette D. Rapid-onsetthrombocytopenia following piperacillin-tazobactam reexposure.Pharmacotherapy. 2015;35:e326–30.
194. Whitman CB, Joseph JM, Sjoholm LO. Cephalosporin-induced leukopeniafollowing rechallenge with cefoxitin. Ann Pharmacother. 2008;42:1327–32.
195. Lambourne J, Kitchen J, Hughes C, Merry C. Piperacillin/tazobactam-inducedparesthesiae. Ann Pharmacother. 2006;40:977–9.
196. Nag DS, Samaddar DP, Kant S, Mahanty PR. Perianesthetic refractoryanaphylactic shock with cefuroxime in a patient with history of penicillinallergy on multiple antihypertensive medications. Rev Brasil Anestesiol. 2017;67:217–20.
197. Lin Y-F, Yang C-H, Sindy H, Lin J-Y, Hui C-YR, Tsai Y-C, Wu TS, Huang CT, KaoK-C Hu H-C, Chiu C-H, Hung S-I, Chung W-H. Severe cutaneous adversereactions related to systemic antibiotics. Clin Infect Dis. 2014;58:1377–85.
198. Hayashi, et al. Beta-Lactam therapeutic drug monitoring in the critically ill:optimising drug exposure in patients with fluctuating renal function andhypoalbuminaemia. Int J Antimicrob Agents. 2013;41:162–6.
199. Hites M, Taccone FS, Wolff F, Cotton F, Beumier M, De Backer D, Roisin S,Lorent S, Surin R, Seyler L, Vincent J-L, Jacobs F. Case-control study of drugmonitoring of beta-lactams in obese critically ill patients. Antimicrob AgentsChemother. 2013;57:708–15.
200. Blondiaux N, Wallet F, Favory R, Onimus T, Nseir S, Courcol RJ, Durocher A,Roussel-Delvallez M. Daily serum piperacillin monitoring is advisable incritically ill patients. 2010; https://doi.org/10.1016/j.ijantimicag.2010.01.018.
201. Pea F, Cojutti P, Sbrojavacca R, Cadeo B, Cristini F, Bulfoni A, Furlanut M.TDM-guided therapy with daptomycin and meropenem in a morbidlyobese, Critically Ill Patient. Ann Pharmacother. 2011;45:e37.
202. Crandon JL, Ariano RE, Zelenitsky SA, Nicasio AM, Kuti JL, Nicolau DP.Optimization of meropenem dosage in the critically ill population based onrenal function. Intensive Care Med. 2011;37:632–8.
203. Robatel C, Decosterd LA, Biollaz J, Eckert P, Schaller MD, Buclin T.Pharmacokinetics and dosage adaptation of meropenem during continuousvenovenous hemodiafiltration in critically ill patients. J Clin Pharmacol. 2003;43:1329–40.
204. Kawano S, Matsumoto K, Hara R, Kuroda Y, Ikawa K, Morikawa N, Horino T,Hori S, Kizu J. Pharmacokinetics and dosing estimation of meropenem inJapanese patients receiving continuous veno-venous hemodialysis. J InfectChemother. 2015;21:476–8.
205. Bugge JF. Pharmacokinetics and drug dosing adjustments duringcontinuous venovenous hemofiltration or hemodiafiltration in critically illpatients. Acta Anaesthesiol Scand. 2001;45:929–34.
206. Casu GS, Hites M, Jacobs F, Cotton F, Wolff F, Beumier M, De Backer D,Vincent J-L, Taccone FS. Can changes in renal function predict variations inbeta-lactam concentrations in septic patients? Int J Antimicrob Agents.2013;42:422–8.
207. De Waele JJ, Carrette S, Carlier M, Stove V, Boelens J, Claeys G, Leroux-RoelsI, Hoste E, Depuydt P, Decruyenaere J, Verstraete AG. Therapeutic drugmonitoring-based dose optimisation of piperacillin and meropenem: arandomised controlled trial. Intensive Care Med. 2014;40:380–7.
208. Sime FB, Roberts MS, Tiong IS, Gardner JH, Lehman S, Peake SL, Hahn U,Warner MS, Roberts JA. Can therapeutic drug monitoring optimize exposureto piperacillin in febrile neutropenic patients with haematologicalmalignancies? A randomized controlled trial. J Antimicrob Chemother. 2015;70:2369–75.
Veiga and Paiva Critical Care (2018) 22:233 Page 33 of 34

209. Neuner EA, Ahrens CL, Groszek JJ, Isada C, Vogelbaum MA, Fissell WH,Bhimraj A. Use of therapeutic drug monitoring to treat Elizabethkingiameningoseptica meningitis and bacteraemia in an adult. J AntimicrobChemother. 2012; https://doi.org/10.1093/jac/dks053.
210. Roberts JA, Ulldemolins M, Roberts MS, McWhinney B, Ungerer J, PatersonDL, Lipman J. Therapeutic drug monitoring of Beta-lactams in critically illpatients: proof of concept. Int J Antimicrob Agents. https://doi.org/10.1016/j.ijantimicag.2010.06.008.
211. Roberts JA, Norris R, Paterson DL, Martin JH. Therapeutic drug monitoring ofantimicrobials. Br J Clin Pharmacol. 2011;73:27–36.
212. Delattre IK, Musuamba FT, Jacqmin P, Taccone FS, Laterre P-F, Verbeeck RK,Jacobs F, Wallemacq P. Population pharmacokinetics of four β-lactams incritically ill septic patients co-medicated with amikacin. Clin Biochem. 2012;45:780–6.
Veiga and Paiva Critical Care (2018) 22:233 Page 34 of 34