Embed Size (px)
Citation preview

Clinical Therapeutics/Volume 31, Number 10, 2009
2206 Volume 31 Number 10
Accepted for publication September 3, 2009.
Express Track online publication October 16, 2009.doi:10.1016/j.clinthera.2009.10.0080149-2918/$ - see front matter
© 2009 Excerpta Medica Inc. All rights reserved.
ABSTRACTBackground: Fampridine (4-aminopyridine) is a po-
tassium channel–blocking agent that has been reported to have therapeutic potential for improving walking and mobility in patients with multiple sclerosis (MS). A sustained-release (SR) formulation of fampridinewas developed to improve the agent’s pharmacokinetic profile by extending its t1/2 relative to that of immediate-release fampridine.
Objectives: The primary study objective was to ex-amine the pharmacokinetics of fampridine SR tabletsafter single escalating doses in patients with MS.Tolerability was evaluated as a secondary end point.
Methods: This multicenter, Phase I-II, open-labeltrial evaluated the dose proportionality and tolerabil-ity of 4 single doses of fampridine SR (5, 10, 15, and 20 mg) in patients with MS. There was a 4-day wash-out between doses. Blood samples were collected im-mediately before drug administration, hourly for the first 8 hours after administration, and at 10, 12, 14, 18, and 24 hours after administration. The pharma-cokinetic parameters evaluated included Cmax, Tmax, AUC, elimination rate constant, apparent elimination t1/2, and apparent CL/F. Twelve-lead ECGs were ob-tained at baseline (0.5 hour before dosing) and at 1, 4,12, and 24 hours after drug administration to evaluatepotential effects on the QTc interval. All adverse events, abnormal laboratory values, and ECG abnor-malities were recorded and evaluated for clinical rele-vance. Adverse-event data were monitored for 24 hoursafter the last dose, and patients were instructed to re-port any adverse events for 14 days after the conclu-sion of the study.
Results: Twenty-four white patients were enrolled (58% female; mean [SD] age, 45.4 [7.3] years; weight range, 47.8–87.1 kg), and 23 completed the study.Mean plasma concentrations and AUC values were dose proportional. Tmax occurred at 3.36 to 3.92 hours after dosing; the apparent elimination t1/2 was
5.47 hours. Both sex and weight affected the pharma-cokinetic parameters of fampridine SR. Eleven treament-related adverse events were reported in 10 patients,with dizziness being the most common (7 incidents re-ported by 6 patients [1 at 10 mg, 3 at 15 mg, and 3 at 20 mg]). Other adverse events included amblyo-pia, asthenia, headache, and ataxia. All treatment- related adverse events were mild to moderate in severity,with the exception of 1 case of dizziness (20 mg) thatwas considered severe. No serious adverse events were reported, and no clinically significant changes in cor-rected QT intervals were observed. No patients with-drew due to treatment-related adverse events.
Conclusion: In these patients with MS, fampridineSR (5–20 mg) had a potentially advantageous phar-macokinetic profile relative to that associated withimmediate-release fampridine and was generally welltolerated. (Clin Ther. 2009;31:2206–2214) © 2009 Excerpta Medica Inc.
Key words: pharmacokinetics, fampridine SR,4-aminopyridine, multiple sclerosis.
INTRODUCTIONBased on the role of potassium channels in action-potential conduction failure in demyelinated nerve fi-bers, potassium channel blockade may be a potentiallyuseful therapeutic strategy for enhancing neurologicfunction in individuals with multiple sclerosis (MS).1
Fampridine (4-aminopyridine) is a potassium channel–blocking agent that enhances conduction in focallydemyelinated axons, improves synaptic transmission,and potentiates muscle contraction.2–5 Fampridine is
Pharmacokinetics and Tolerability of Single Escalating Dosesof Fampridine Sustained-Release Tablets in Patients With Multiple Sclerosis: A Phase I-II, Open-Label Trial
Timothy Vollmer, MD1; and Herbert R. Henney III, PharmD2
1University of Colorado, Denver, Colorado; and 2Acorda Therapeutics, Hawthorne, New York

October 2009 2207
T. Vollmer and H.R. Henney III
The differences included a 32% decrease in AUCtmaxamong tetraplegic patients relative to paraplegic pa-tients that was ascribed to a slower rate of initial ab-sorption, although total bioavailability over the 12-hourassessment period did not differ between the 2 sub-groups.9 Different target populations may sometimes exhibit characteristic patterns of drug disposition that are inconsistent with those in healthy volunteers, andpharmacokinetic characteristics may predict variabili-ty in efficacy. A linear relationship with dose was ob-served in a clinical trial evaluating mean fampridineplasma concentrations in patients with MS receivingfampridine SR 10 to 40 mg BID for 8 weeks; however,the measured concentrations of fampridine represent-ed only an approximation of steady-state concentra-tions between Cmax and Cmin, as there was no pre-scribed interval between dosing and sample collectionand other pharmacokinetic parameters were not assessed.14
The primary objective of the present study was toexamine the pharmacokinetics of single escalatingdoses of fampridine SR in patients with MS. A second-ary objective was to evaluate tolerability in this pa-tient population over the dose range from 5 to 20 mg. The entire study was conducted as part of a New Drug Application.
PATIENTS AND METHODSPatients
Male and female patients with clinically definiteMS (Poser criteria26) were enrolled from October 21,1997, through January 21, 1998. Eligible patientswere between the ages of 18 and 65 years, had beentaking stable doses of concomitant medications for2 weeks before initial dosing with fampridine SR, andhad no clinically significant abnormality based on the medical history, physical examination, and laboratory evaluations. Key exclusion criteria were participation in another clinical trial within 30 days before fampri-dine dosing; history of alcohol or drug abuse; blooddonation within the previous 30 days; known sensi-tivity to 4-aminopyridine or similar compounds; pre-vious gastrointestinal surgery that might interferewith drug absorption; impaired liver function or useof known inducers or inhibitors of hepatic enzymes within 30 days before dosing; presence or history of a psychiatric disorder that in the opinion of the investi-gator, would interfere with the conduct of the proto-col or jeopardize the validity of informed consent;
an investigational drug, and a New Drug Application iscurrently under review by the US Food and Drug Admin-istration (FDA). It has been evaluated in the treatment of spinal cord injury,6–11 and the results of MS trials havesuggested that fampridine may be associated with im-provements in leg strength, gait, and mobility.12–14
Fampridine has a relatively narrow therapeutic in-dex, with immediate-release (IR) formulations associ-ated with a Tmax of ~1 hour.15–17 The incidence of adverse events with fampridine appears to be dependenton plasma concentrations. In a randomized, double- blind, placebo-controlled crossover study in patientswith MS, Bever et al18 found that 36 adverse events occurred at a mean (SE) plasma concentration of 83 (6) ng/mL, compared with 9 adverse events at amean plasma concentration of 46 (4) ng/mL, a 4-foldhigher incidence. There have been several reports of fampridine-associated toxicity due to overdose or use in an unregulated setting.19–22 Furthermore, a regimenof ≥4 daily doses would be required to sustain themean (SD) therapeutic plasma concentration of 0.243 (0.113) μM that has been suggested for the proposed therapeutic dose of 20 mg/d.14
The IR formulation of 4-aminopyridine has beenemployed in clinical trials and is prepared extempora-neously by compounding pharmacies for unregulatedcommercial use. Although compounded drugs, includ-ing fampridine, may be used in the clinical setting, a2006 FDA assessment of compounded drugs reportedthat 33% of 36 sampled products failed ≥1 of the standard quality tests performed, with potencies rang-ing from 67.5% to 268.4% of amounts stated in theproduct labeling.23 In a recent report of 4 cases of fampridine toxicity, all cases involved excessive fam-pridine in the compounded product, with doses rang-ing from 90.1 to 125.6 mg for a 10-mg tablet.24
Fampridine sustained-release (SR) coated matrixtablets have been developed to overcome some of thepharmacokinetic limitations and safety concerns as-sociated with IR formulations of 4-aminopyridine. Specifically, the SR formulation was developed to ex-tend the elimination t1/2 and reduce the Cmax to sus-tain plasma concentrations of fampridine over a long- er period relative to IR formulations while reducing the risk of concentration-dependent adverse effects.
The pharmacokinetic characteristics of fampridine SR have been evaluated in patients with spinal cordinjury, with minor differences in absorption character-istics among subgroups with spinal cord injury.9,15,25

2208 Volume 31 Number 10
Clinical Therapeutics
Blood Sampling and Analytic ProceduresBlood samples (5 mL) for analysis of fampridine
concentrations were collected in 7-mL heparinizedtubes during each of the 4 dosing periods. Samples were collected immediately before drug administra-tion; hourly for the first 8 hours after drug adminis-tration; and at 10, 12, 14, 18, and 24 hours after drugadministration. The samples were centrifuged at 1500gfor 15 minutes at 2°C within 1 hour of collection. Theresulting plasma was removed and stored at –20°Cuntil assayed.
Plasma samples were assayed by the Drug Studies Unit, Analytical Division, University of California, SanFrancisco, using validated liquid-chromatographytechniques, including a PE/Sciex API III system (Perkin-Elmer/Sciex, Foster City, California) equipped with a silica column, 90% CH3CN, 0.1% trifluoroacetic acid,and a 5-mM ammonium acetate mobile phase. Mass-spectrometric detection was performed with sampleinlet by heated nebulizer, positive ionization by atmospheric-pressure chemical ionization, and massscanning by multiple-reaction monitoring analysis.
Sample preparation was performed by extractionof 0.2 mL plasma with 1.0 mL ethyl acetate beforeseparation by liquid chromatography with tandemmass spectrometry (LC-MS/MS). Standard curve andquality control samples were generated by spikinginterference-free human plasma samples with knownamounts of fampridine and internal standards (IS). Thepeak area ratios of fampridine to IS were calculated for each sample from the measured peak areas ob-tained by LC-MS/MS. Spiked concentrations and peak area ratios of fampridine to IS for the standard curvesamples were fit by 1/y weighted least squares linear regression to the equation for the best straight line,and drug concentrations in the assay samples werecalculated by the equation from the fampridine to ISpeak area ratios obtained by LC-MS/MS. Calibrationstandards at 8 concentrations (2–200 ng/mL) and qual-ity control samples (5, 40, and 150 ng/mL) within thecalibration range were routinely analyzed with studysamples.
Quality control samples were generated by spikingblank human plasma with fampridine to monitor assayperformance. Interday precision (%CV) ranged from5.18% to 9.37%, and interday accuracy (relative error[RE]), calculated as [([mean-nominal concentration]/nominal concentration) 100], ranged from –4.67%to +7.25%. The intraday precision ranged from 2.49%
personal or familial history of epilepsy or cardiac ar-rhythmias, as the known excitatory effect of potassi-um channel blockade would potentially place these patients at undue risk; and serious local or systemicinfection within 30 days before dosing. Women who were lactating, pregnant, or of childbearing potentialand not using approved methods of birth control and patients who were substantially underweight or over-weight in the opinion of the investigator, who tested positive for HIV, or who had evidence of malignancy were also excluded.
Study Design and ProceduresThis Phase I-II, open-label trial was conducted at
2 sites in the United States, the University of Rochester Medical Center in Rochester, New York, and the YaleUniversity School of Medicine in New Haven, Con-necticut. It was conducted in compliance with na-tional regulations for good clinical practices and in accordance with the Declaration of Helsinki (3rd revi-sion). The protocol was approved by local ethics com-mittees (Western Institutional Review Board, Olym-pia, Washington, and Human Investigation Committee,Yale University School of Medicine), and written in-formed consent was obtained from all patients before study participation.
The study evaluated the dose proportionality andtolerability of 4 doses of oral fampridine SR tablets: 5, 10, 15, and 20 mg. Patients received an initial dose of fampridine SR 5 mg, with a 4-day washout betweenescalating doses. This dosing regimen was designed tominimize any possible pharmacokinetic effects fromthe previous dose and to enable an evaluation of thesafety profile before advancing to the next dose. Tab-lets were administered to patients in the fasted state.
Patients were monitored for 24 hours after eachdose of fampridine SR and were advanced to the nextdose only after consideration of the safety profile and pharmacokinetic parameters of the previous dose. Pa-tients with peak plasma 4-aminopyridine concentra-tions >90 ng/mL, regardless of reported tolerability,were not allowed to progress to the next dose. This threshold was based on the findings of studies andcase reports of plasma fampridine concentrations inpatients with reported seizures, which suggested thata plasma fampridine concentration of ~100 ng/mLmay be considered a likely threshold for increased seizure risk in the absence of other significant riskfactors.14,20,21,27–30

October 2009 2209
T. Vollmer and H.R. Henney III
the interpretation of the ECGs, the QT interval wascorrected using the Bazett formula (QTc = QT/RR0.5), as recommended in International Conference on Har-monisation guidance E14.32 All safety data, including laboratory values and ECGs, were evaluated by theon-site physician, including determination of the clini-cal relevance of any laboratory values outside normalranges or ECG changes from baseline.
Statistical AnalysisNo formal sample-size calculation was performed.
Primary pharmacokinetic variables were analyzed us-ing inferential statistics, with a primary focus on AUCand Cmax, normalized to the 5-mg dose to facilitate comparison.33 Safety data were presented using de-scriptive statistics.
All data manipulations, tabulations, comparisons,and regressions were performed using the GLM pro-cedure in SAS version 6.08 (SAS Institute Inc., Cary,North Carolina). Statistical significance was tested against the null hypothesis with a critical P value setat 0.05.
RESULTSPatient Disposition
The study enrolled 24 patients, 23 of whom re-ceived all 4 doses. One patient was unwilling to attendthe final hospital visit and therefore received only3 doses; this patient was discontinued from the study. Several minor protocol deviations were recorded,mainly omissions of data that were deemed to have noimpact on the integrity of the study. The patients weremainly female (58%) and all were white; the mean (SD)age of the population was 45.4 (7.3) years (Table I).
Pharmacokinetic ProfileThe pharmacokinetic parameters of fampridine af-
ter oral administration of single escalating doses of fampridine SR (5–20 mg) are summarized in Table II.The mean Tmax ranged from 3.36 to 3.92 hours. Theoverall apparent elimination t1/2 was 5.47 hours (range, 5.05–5.76 hours).
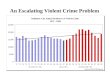
When normalized to a 5-mg dose, the Cmaxhad good consistency across the dose range (12.31–13.13 ng/mL) (Table II). This was also the case for the other pharmacokinetic parameters, in-cluding normalized AUC and AUC0–∞, apparent ke, and apparent CL/F. The results of multiple compari-sons of the dose-normalized data suggested no signifi-
to 8.28%, and the intraday RE ranged from –5.50%to –6.00%. The lower limit of quantification for theassay was equivalent to the low point of the standard curve, or nominally 1.00 ng/mL. The intraday mean, %CV, and RE values were 1.83 ng/mL, 11.7%, and–7.00%, respectively; the corresponding interday val-ues were 1.88 ng/mL, 10.6%, and –6.00%.
Pharmacokinetic AnalysisPharmacokinetic parameters were evaluated after
each dose, and noncompartmental analysis was per-formed.31 The plasma pharmacokinetic parametersevaluated were Cmax, Tmax, apparent elimination rateconstant (ke), AUC, AUC0–∞, t1/2, and CL/F. The appar-ent ke was estimated as the negative slope, calculated by least squares regression, of the last 3 observed natural log concentration–time points. AUC was cal-culated to the Cmax using the linear trapezoidal rule and to the last observed concentration using the log-linear trapezoidal rule. The AUC0–∞ was calculated by dividing the concentration at the last measured time point by the apparent ke, and this value was then added to the AUC to obtain the AUC0–∞. The elimina-tion t1/2 was calculated as 0.693 (constant value, ln 2) divided by the apparent ke for each patient. The mean parameter was then calculated from each patient’s derived data. The CL/F (clearance divided by bioavail-ability) was estimated as the fampridine dose divided by the AUC0–∞. Pharmacokinetic parameter estimateswere compared among dose levels and between sexes.Linear regressions of the pharmacokinetic parameters versus body weight, age, and sex were performed.
TolerabilityTolerability was monitored during the 24-hour pe-
riod after administration of each dose of fampridineSR. In addition, patients were instructed to report anyadverse events for 14 days after the conclusion of thestudy. All adverse events were reported, regardless of causality. The investigator evaluated the relationshipbetween adverse events and study treatment. Labora-tory tests, vital signs, and physical examinations wereperformed and evaluated for changes between the pre-treatment and posttreatment periods. A 12-lead ECGwas obtained at baseline (0.5 hour before dosing) andat 1, 4, 12, and 24 hours after administration of each dose. Evaluation of ECGs to identify potential effects on the QT interval was included as a specific safetyobjective, as recommended by the FDA.32 As part of

2210 Volume 31 Number 10
Clinical Therapeutics
cant differences among dose levels for any pharmacoki-netic parameter. The figure illustrates the mg/kg-correctedconcentration–time profiles in each dose group.
There were significant differences in normalized mean pharmacokinetic values between men and women.The mean normalized Cmax was 9.9 ng/mL for men and 14.6 ng/mL for women (P = 0.001). There also were differences between men and women in both mean normalized AUC (99 and 147 ng · h/mL, respec-tively; P = 0.001) and normalized AUC0–∞ (113 and 163 ng · h/mL; P = 0.001). However, neither the me-dian Tmax nor mean apparent ke differed between menand women.
Because sex may be confounded by body weight and age, multiple linear regression was performed for each pharmacokinetic parameter versus body weight,age, and sex. The apparent CL/F was significantly in-fluenced by body weight (~5%–10% higher for each10-kg increase in weight), age (~5%–10% lower per increasing decade), and sex (~23% lower in womenthan men) (all, P ≤ 0.05). The effects of weight and sex on apparent CL/F were reflected in changes in theAUC, AUC0–∞, and Cmax, and the effects of age were reflected in changes in the AUC0–∞. The apparent ke
Table I. Demographic characteristics (N = 24).
Variable Value
Sex, no. (%)Female 14 (58)Male 10 (42)
White race, no. (%) 24 (100)
Age, yMean (SD) 45.4 (7.3)Range 29–56
Age at onset of MS, yMean (SD) 29.6 (8.3)Range 19–50
Weight, kgMean (SD) 71.9 (11.3)Range 47.8–87.1
Height, cmMean (SD) 170.7 (8.1)Range 149.9–182.9
MS = multiple sclerosis.
Table II. Fampridine pharmacokinetic parameters.
Pharmacokinetic Overall,Parameter 5 mg 10 mg 15 mg 20 mg Mean (95% CI)
TmaxTT , h 3.88 (0.20) 3.92 (0.25) 3.36 (0.25) 3.57 (0.25) 3.75 (3.52–3.98)
Cmax, ng/mL 13.13 (0.64) 25.23 (1.39) 37.00 (1.99) 49.23 (3.16) NA
AUC, ng · h/mL 122.1 (9.4) 252.2 (15.6) 394.4 (22.2) 511.3 (27.7) NA
AUC0–∞, ng · h/mL 146.4 (10.0) 283.2 (18.0) 428.9 (25.6) 546.7 (31.4) NA
Apparent ke, h–1 0.143 (0.012) 0.143 (0.011) 0.138 (0.008) 0.148 (0.008) 0.14 (0.13–0.15)
Apparent t1/2, h 5.76 (0.53) 5.55 (0.44) 5.50 (0.38) 5.05 (0.32) 5.47 (5.05–5.89)
Apparent CL/F, mL/min 619.8 (36.2) 641.4 (39.1) 632.4 (39.0) 653.9 (37.1) 636.7 (600.0–674.0)
Normalized values*Cmax, ng/mL 13.13 (0.64) 12.61 (0.69) 12.34 (0.66) 12.31 (0.79) 12.60 (11.90–13.30)AUC, ng · h/mL 122.1 (9.4) 126.1 (7.8) 131.5 (7.4) 127.8 (6.9) 126.9 (119.0–135.0)AUC0–∞, ng · h/mL 146.4 (10.0) 141.6 (6.9) 143.0 (8.5) 136.7 (7.9) 142.0 (133.0–151.0)
NA = not applicable; ke = terminal rate constant.*Normalized to a 5-mg dose.
Value by Fampridine Dose, Mean (SE)

October 2009 2211
T. Vollmer and H.R. Henney III
from baseline in laboratory values, vital signs, findingson physical or neurologic examinations, or ECG pa-rameters. No clinically significant changes in QTc in-tervals were observed (Table IV).
DISCUSSIONThe pharmacokinetics of orally administered fampri-dine IR have been characterized previously.15,17,34
The Tmax of fampridine IR has been reported to occur ~1 hour after dosing, and its elimination t1/2 has beenreported as ~3.5 hours.15–17 Fampridine is eliminatedthrough the kidneys, with ≥90% of the drug excreted unchanged in the urine and most of this excretion (85%) occurring by 14 hours after dosing.16 Thesepharmacokinetic properties suggest that ≥4 daily dosesof the IR formulation would be needed to maintain a therapeutic effect.
Fampridine SR was developed to provide sustained plasma concentrations of fampridine over a longer period of time than with IR formulations. The phar-macokinetics of fampridine SR in patients with MS inthe present study were consistent with values previ-ously reported in healthy volunteers35 and patients
was significantly influenced by age (P ≤ 0.05), as evi-denced by a longer apparent elimination t1/2 in older patients. When the pharmacokinetic parameters werecorrected for weight, the results were not substantiallydifferent (Table III). Because an SR formulation wasused, calculation of the apparent ke may have been affected by the delay in absorption.
TolerabilityA total of 11 treatment-related adverse events were
reported in 10 patients. Dizziness was the most com-mon adverse event, with 7 incidents reported by 6 pa-tients (1 at 10 mg, 3 at 15 mg, and 3 at 20 mg). Other adverse events included amblyopia (1 patient at 20 mg),asthenia (1 patient at 10 mg), headache (1 patient at10 mg), and ataxia (1 patient at 20 mg). All treatment-related adverse events were mild to moderate in severi-ty, with the exception of 1 case of dizziness at the20-mg dose, which was severe and resolved withoutintervention within 4.5 hours. No patients withdrewfrom the study because of treatment-related adverseevents. No deaths or other serious adverse events werereported. There were no clinically significant changes
0.01
Plas
ma
Con
cent
ratio
n([
ng/m
L]/[
mg/
kg])
85 6 74321 181412100 24
Time (h)
5 mg10 mg15 mg20 mg
1.0
0.1
x
x
xx
xx
xxxxxx
x
x
x
Figure. Mean weight-normalized fampridine plasma concentrations.

2212 Volume 31 Number 10
Clinical Therapeutics
teers and patients with spinal cord injury,15 suggesting a lower likelihood for occurrence of the adverse eventsthat have been associated with higher plasma concen-trations. Fampridine pharmacokinetics were linear across doses, and no dose-dependent pharmacokineticeffects were observed. Linear regression of oral clear-ance versus body weight and age found significant relationships between increased clearance, higherweight, and lower age. Clearance also appeared to belower in women than in men. Although many factors may play a role in these differences, the most notablemay be sex-related differences in the apparent Vd, which was not assessed in this study.
In the present study, fampridine SR was rapidly andcompletely absorbed after oral administration. How-ever, the terminal elimination t1/2 was greater than the3.14 hours reported by Blight and Henney34 for an
with spinal cord injury.9,25,36 Both the Tmax of 3.75 hours xand the apparent elimination t1/2 of 5.47 hours were numerically longer than values reported for the IR formulation.15–17 The mean Tmax was delayed~2.8 hours compared with previously published data.34
Compared with the previously reported t1/2 of ~3.5 hoursafter oral administration of the IR formulation,15 the value in the present study would appear to have been influenced by delayed absorption of the SR formulation. The increases in these pharmacokinetic parameters may support twice-daily dosing of fampridine SR. Reduced dosing compared with the IR formulation may have abenefit in terms of patient compliance, as it has been suggested that the number of daily doses prescribed is generally inversely related to medication compliance.37
Cmax values in the present study were approximately half those reported for fampridine IR in healthy volun-
Table III. Mean (SD) fampridine pharmacokinetic parameters, normalized by dose and weight.
NormalizedPharmacokinetic Parameter 5 mg 10 mg 15 mg 20 mg
Cmax, (ng/mL)/(mg/kg) 184.71 (6.63) 177.63 (8.03) 174.17 (8.70) 171.32 (8.80)
AUC, (ng · h/mL)/(mg/kg) 1715.0 (107.2) 1776.1 (91.7) 1873.3 (105.3) 1792.0 (79.5)
AUC0–∞, (ng · h/mL)/(mg/kg) 2065.3 (114.7) 1993.7 (106.3) 2035.7 (119.7) 1916.5 (93.9)
Fampridine Dose
Table IV. Mean (SEM) QTc intervals (Bazett’s correction).
Fampridine Dose Baseline* 1 Hour 4 Hours 12 Hours 24 Hours
5 mg n = 24 n = 22 n = 24 n = 23 n = 22430 (4.4) 398 (5.0) 400 (5.5) 401 (5.3) 403 (3.7)
10 mg n = 24 n = 24 n = 24 n = 24 n = 24399 (4.2) 398 (4.7) 397 (4.7) 386 (13.8) 402 (5.0)
15 mg n = 24 n = 24 n = 24 n = 24 n = 24403 (4.9) 400 (6.4) 408 (6.8) 402 (4.2) 406 (5.4)
20 mg n = 22 n = 23 n = 23 n = 23 n = 21397 (5.0) 397 (5.2) 405 (4.9) 391 (10.6) 402 (4.9)
*The baseline QTc interval was measured 0.5 hour before administration of fampridine sustained release.
QTc Interval, msec

October 2009 2213
T. Vollmer and H.R. Henney III
E. Jay Bienen, PhD, an independent scientific con-sultant based in New York City, provided editorial support, which was funded by Acorda Therapeutics.
REFERENCES1. Judge SI, Bever CT Jr. Potassium channel blockers in
multiple sclerosis: Neuronal Kv channels and effects of symptomatic treatment. Pharmacol Ther. 2006;111:224–259.
2. Lundh H, Thesleff S. The mode of action of 4-aminopyridineand guanidine on transmitter release from motor nerveterminals. Eur J Pharmacol. 1977;42:411–412.
3. Targ EF, Kocsis JD. 4-Aminopyridine leads to restorationof conduction in demyelinated rat sciatic nerve. Brain Res.1985;328:358–361.
4. Kirsch GE, Drewe JA. Gating-dependent mechanism of 4-aminopyridine block in two related potassium chan-nels. J Gen Physiol. 1993;102:797–816.
5. Shi R, Blight AR. Differential effects of low and high concen-trations of 4-aminopyridine on axonal conduction in normaland injured spinal cord. Neuroscience. 1997;77:553–562.
6. Hansebout RR, Blight AR, Fawcett S, Reddy K. 4-Aminopyridine in chronic spinal cord injury: A controlled,double-blind, crossover study in eight patients. J Neuro-trauma. 1993;10:1–18.
7. Potter PJ, Hayes KC, Hsieh JT, et al. Sustained improve-ments in neurological function in spinal cord injured pa-tients treated with oral 4-aminopyridine: Three cases.Spinal Cord. 1998;36:147–155.
8. Segal JL, Pathak MS, Hernandez JP, et al. Safety and effi-cacy of 4-aminopyridine in humans with spinal cord inju-ry: A long-term, controlled trial. Pharmacotherapy. 1999;19:713–723.
9. Segal JL, Hayes KC, Brunnemann SR, et al. Absorptioncharacteristics of sustained-release 4-aminopyridine (fam-pridine SR) in patients with chronic spinal cord injury.J Clin Pharmacol. 2000;40:402–409.
10. van der Bruggen MA, Huisman HB, Beckerman H, et al.Randomized trial of 4-aminopyridine in patients withchronic incomplete spinal cord injury. J Neurol. 2001;248:665–671.
11. Cardenas DD, Ditunno J, Graziani V, et al. Phase 2 trial of sustained-release fampridine in chronic spinal cord injury.Spinal Cord. 2007;45:158–168.
12. Polman CH, Bertelsmann FW, van Loenen AC, Koetsier JC. 4-Aminopyridine in the treatment of patients withmultiple sclerosis. Long-term efficacy and safety. ArchNeurol. 1994;51:292–296.
13. Schwid SR, Petrie MD, McDermott MP, et al. Quantitativeassessment of sustained-release 4-aminopyridine for symptomatic treatment of multiple sclerosis. Neurology.1997;48:817–821.
oral solution of fampridine, which is believed to repre-sent the true elimination t1/2 of fampridine. The formu-lation tested in the present study releases ~50% of drugin solution over 4 hours in a sustained manner (data on file, Acorda Therapeutics, June 13, 2007). The longer terminal elimination t1/2 supports an effect on elimina-tion as a result of the delay in absorption of fampridine from the SR formulation, an effect sometimes referredto as flip-flop pharmacokinetics. To evaluate the poten-tial effect of flip-flop pharmacokinetics, noncompart-mental first-order pharmacokinetics were used to de-termine the apparent pharmacokinetic parameters of fampridine SR. In an attempt to determine whetherdelayed absorption would affect estimation of the ke, the following equation was applied to the data: Tmax*Cmax = AUC*e–1.38 The results of the 2 sides of the calculation revealed approximately equal values; thus, it was assumed that delayed absorption had an effect on elimination, and the values for t1/2, ke, andCL/F were reported as apparent values throughout.
Fampridine SR (5–20 mg) was well tolerated in these patients with MS. Although the study provided limitedcardiac safety information, particularly with regard to the potential for QTc-interval prolongation, no clinically significant changes in QTc intervals were observed. Fur-rrthermore, no relationship was observed between QTc-interval prolongation and plasma levels of fampridine.
The generalizability of the study data is limited bythe relatively small sample size and the administrationof single doses of fampridine SR in the fasted state. In addition, all participants were white. However, be-tween 75% and 90% of people with MS are white and of European background.39 Nonetheless, the im-pact of pharmacogenomic differences between ethnic groups cannot be ruled out.
CONCLUSIONSIn these patients with MS, fampridine SR 5 to 20 mg exhibited a pharmacokinetic profile that may support potential advantages relative to IR formulations. Fam-pridine SR was generally well tolerated.
ACKNOWLEDGMENTSThis study was supported by Acorda Therapeutics. Dr.Vollmer has been a consultant for Acorda Therapeu-tics, and Dr. Henney is an employee of the company.The authors have indicated that they have no otherconflicts of interest regarding the content of this article.

2214 Volume 31 Number 10
Clinical Therapeutics
32. International Conference on Harmon-isation. Guidance for Industry. E14Clinical evaluation of QT/QTc intervalprolongation and proarrhythmic po-tential for non-antiarrhythmic drugs.http://www.fda.gov/downloads/RegulatoryInformation/Guidances/ucm129357.pdf. Accessed June 9,2008.
33. Glantz SA. Primer of Biostatistics. New York, NY: McGraw-Hill; 1981.
34. Blight AR, Henney HR III. Pharma-cokinetics of 14C-radioactivity after oral intake of a single dose of 14C-labeled fampridine (4-aminopyridine)in healthy volunteers. Clin Ther. 2009;31:328-335.
35. Smith W, Swan S, Marbury T, Henney HR III. Single-dose pharmacokineticsof 4-aminopyridine slow release inhealthy volunteers and renally im-paired adults. J Clin Pharmacol. In press.
36. Hayes KC, Potter PJ, HanseboutRR, et al. Pharmacokinetic studiesof single and multiple oral doses of fampridine-SR (sustained-release4-aminopyridine) in patients withchronic spinal cord injury. Clin Neu-ropharmacol. 2003;26:185–192.
37. Claxton AJ, Cramer J, Pierce C. Asystematic review of the associa-tions between dose regimens andmedication compliance. Clin Ther.2001;23:1296–1310.
38. Boxenbaum H, Pharmacokineticstricks and traps: Flip-flop models.J Pharm Pharm Sci. 1998;1:90–91.
39. Burks JS, Johnson KP, eds. MultipleSclerosis: Diagnosis, Medical Manage-ment, and Rehabilitation. New York,NY: Demos; 2000.
sclerosis. Neurology. 2008;71:1833–1834.
25. Hayes KC, Potter PJ, Hsieh JT, et al.Pharmacokinetics and safety of multiple oral doses of sustained-release 4-aminopyridine (Fampridine-SR) in subjects with chronic, incom-plete spinal cord injury. Arch PhysMed Rehabil. 2004;85:29–34.
26. Poser CM, Paty DW, Scheinberg L,et al. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann Neurol. 1983;13:227–231.
27. Goodman AD, Brown TR, CohenJA, et al, for the Fampridine MS-F202Study Group. Dose comparison trialof sustained-release fampridine inmultiple sclerosis. Neurology. 2008;71:1134–1141.
28. Goodman AD, Brown TR, KruppLB, et al, for the FampridineMS-F203 Investigators. Sustained-release oral fampridine in multiplesclerosis: A randomised, double-blind, controlled trial. Lancet. 2009;373:732–738.
29. Smeets JW, Kunst MW. Severepoisoning by 4-aminopyridine ina body builder [in Dutch]. Ned Tijdschr Geneeskd. 1995;139:2667–2669.
30. Ball AP, Hopkinson RB, Farrell ID,et al. Human botulism caused by Clostridium botulinum type E: The Bir-mingham outbreak. Q J Med. 1979;48:473–491.
31. Ritschell WA. Handbook of Basic Pharmacokinetics—Including Clinical Applications. 4th ed. Hamilton, Ill:Drug Intelligence Publications; 1992.
14. Goodman AD, Cohen JA, Cross A,et al. Fampridine-SR in multiple scle-rosis: A randomized, double-blind,placebo-controlled, dose-rangingstudy. Mult Scler. 2007;13:357–368.
15. Hayes KC, Katz MA, Devane JG, et al.Pharmacokinetics of an immediate-release oral formulation of Fampri-dine (4-aminopyridine) in normalsubjects and patients with spinalcord injury. J Clin Pharmacol. 2003;43:379–385.
16. Evenhuis J, Agoston S, Salt PJ, et al.Pharmacokinetics of 4-aminopyridinein human volunteers. A preliminary study using a new GLC method for its estimation. Br J Anaesth. 1981;53:567–570.
17. Uges DR, Sohn YJ, Greijdanus B,et al. 4-Aminopyridine kinetics. ClinPharmacol Ther. 1982;31:587–593.
18. Bever CT Jr, Young D, AndersonPA, et al. The effects of 4-aminopyridine in multiple sclerosispatients: Results of a randomized,placebo-controlled, double-blind,concentration-controlled, crossover trial. Neurology. 1994;44:1054–1059.
19. Spyker DA, Lynch C, ShabanowitzJ, Sinn JA. Poisoning with 4-aminopyridine: Report of three cas-es. Clin Toxicol. 1980;16:487–497.
20. Stork CM, Hoffman RS. Characteri-zation of 4-aminopyridine in over-dose. J Toxicol Clin Toxicol. 1994;32:583–587.
21. Pickett TA, Enns R. Atypical presen-tation of 4-aminopyridine overdose.Ann Emerg Med. 1996;27:382–385.
22. Johnson NC, Morgan MW. An un-usual case of 4-aminopyridine toxic-ity. J Emerg Med. 2006;30:175–177.
23. US Food and Drug Administration,Center for Drug Evaluation andResearch. Report: 2006 limitedFDA survey of compounded drugproducts. http://www.fda.gov/cder/pharmcomp/survey_2006.htm. Ac-cessed June 9, 2008.
24. Burton JM, Bell CM, Walker SE,O’Connor PW. 4-Aminopyridinetoxicity with unintentional over-dose in four patients with multiple
Address correspondence to: Herbert R. Henney III, PharmD, Acorda Therapeutics, 15 Skyline Drive, Hawthorne, NY 10532. E-mail: [email protected]