Embed Size (px)
Citation preview

CliniCal pharmaCology & TherapeuTiCs 1
articlesnature publishing group
Glucagon-like peptide 1 (GLP-1) is an incretin hormone secreted by intestinal L cells. GLP-1 circulates as the 7–36 and the 7–36 amide, with the amide providing the majority of the biologi-cal activity.1,2 GLP-1 stimulates insulin release and decreases gastric motility. GLP-1 receptor (GLP-1R) agonists are used in the treatment of type 2 diabetes.3 GLP-1Rs are also present in the heart and the central nervous system and may exert some of their gastrointestinal (GI) effects through central vagal nerve circuits.4,5 The current clinically available formulations are sub-cutaneous (s.c.) injections. New approaches to the administra-tion of GLP-1R agonists have focused on extending the duration of agonist exposure by developing once-daily to once-weekly formulations, thereby achieving chronic continuous exposure. Chronic exposure to GLP-1 and GLP-1 analogs have been shown to desensitize the GLP-1R. Chronic central nervous sys-tem exposure has been shown to reverse the beneficial effects of GLP-1 agonists in animal models.6,7 No reported clinical con-sequences of chronic exposure have been noted to date with a GLP-1 analog administered twice a day for 30 weeks.8,9 Chronic administration of an extended-exposure formulation of a GLP-1
agonist has been associated with the development of medullary thyroid tumors in animals.10
Formulations that deliver GLP-1 in a normal physiologic pattern would rapidly reach peak levels soon after a meal and produce rapid rises in insulin concentrations. Patients with type 2 diabetes often have an impaired first-phase insulin response. Bolus administration of GLP-1 produces an increase in insulin concentrations in response to the intravenous administration of glucose. The insulin response to a bolus of GLP-1 was not as high as for a 3-h infusion of GLP-1 that reached the same peak concentration levels.11 When patients with type 2 diabetes were given 16- or 24-h infusions of GLP-1, the overall insulin levels were lower than those produced by the shorter infusions. This suggests that chronic administration may downregulate GLP-1R response.12
Technosphere inhalation particles are microspheres of 2–2.5 microns in median diameter; they are composed of fumaryl diketopiperazine (FDKP) and are capable of carrying small pep-tides deep into the lungs. The particles dissolve rapidly at physi-ological pH. This drug delivery platform allows the efficient
1MannKind Corporation, Paramus, New Jersey, USA; 2Pharmaceutical Research Associates International (PRA), Zuidlaren, The Netherlands. Correspondence: MT Marino ([email protected])
Received 28 February 2010; accepted 12 April 2010; advance online publication 30 June 2010. doi:10.1038/clpt.2010.85
Pharmacokinetics and Pharmacodynamics of Inhaled GLP-1 (MKC253): Proof-of-Concept Studies in Healthy Normal Volunteers and in Patients With Type 2 DiabetesMT Marino1, D Costello1, R Baughman1, A Boss1, J Cassidy1, C Damico1, S van Marle2, A van Vliet2 and PC Richardson1
mKC253 is glucagon-like peptide 1 (glp-1, 7–36 amide) adsorbed onto Technosphere microparticles for oral inhalation. The pharmacokinetics of inhaled glp-1 and the pharmacokinetic–pharmacodynamic (pK–pD) relationship between inhaled glp-1 and insulin were analyzed in two trials, one in healthy normal volunteers and the other in patients with type 2 diabetes. inhaled glp-1 was absorbed quickly, with peak concentrations occurring within 5 min, and levels returned to baseline within 30 min. inhaled glp-1 appeared to produce plasma levels of glp-1 comparable to those of parenteral administration and sufficient to induce insulin secretion resulting in attenuation of postmeal glucose excursions in subjects with type 2 diabetes. an Emax (maximum effect) model described the relationship between glp-1 concentration and insulin release. The variability in the Emax may be due to differences in baseline glucose levels, differences resulting from genetic polymorphisms in glp-1 receptors (glp-1rs), or the stage of diabetes of the patient.

2 www.nature.com/cpt
articles
transport of small-molecular-weight peptides to the surface of the respiratory epithelium, where they are absorbed into the cir-culation. The inhalation is facilitated by a palm-sized device, the proprietary MedTone Inhaler, a breath-powered, unit-dose, dry-powder inhaler that does not require propulsion synchroniza-tion by the user. The investigational medicinal product, MKC253 (GLP-1/Technosphere) Inhalation Powder is composed of specific doses of synthetic GLP-1 (7–36 amide), a human incretin hor-mone, as the active agent and FDKP as a carrier to deliver GLP-1 to the deep lung through inhalation.13 FDKP is a pH-sensitive molecule that, under mildly acidic conditions, can self-assemble into small particles. GLP-1 is adsorbed onto these particles. The half-life of FDKP in blood, when administered to humans by inhalation, is ~3 h, and it is excreted unchanged in the urine.
The aim of these studies was to determine the pharmaco-kinetics of GLP-1 administered via the pulmonary route and to evaluate its effects on levels of insulin, C-peptide, blood glucose, and glucagon in healthy normal subjects and in subjects with type 2 diabetes. The effect on gastric emptying in subjects with type 2 diabetes was also evaluated.
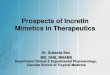
ResultsPharmacokineticsGLP-1 as delivered by MKC253 was rapidly absorbed and pro-duced peak concentrations in the plasma within 5 min. GLP-1 concentrations returned to baseline values within 30 min both in healthy volunteers and in subjects with type 2 diabetes (Figure 1). In healthy subjects, when GLP-1 was administered
Time (min)
50100150200250
102030405060
0.5
1.0
1.5
2.0
3.5
4.0
4.55.0
5.5
10
15
20
25
0.05 mg
0 60 120
0.45 mg
0 60 120
0.75 mg
0 60 120
1.05 mg
0 60 120
1.5 mg
0 60 120
GLP-1
INSULIN
C-PEPTIDE
GLUCOSE
GLUCAGON
pmol
/lµU
/ml
ng/m
lm
mol
/lpm
ol/l
Figure 1 Study 1: GLP-1, insulin, C-peptide, glucose, and glucagon levels by dose group. The doses of 0.05, 0.45, 0.75, 1.05, and 1.5 mg are shown from left to right. All data and mean lines are shown. GLP-1, glucagon-like peptide 1.
table 1 summary of pharmacokinetic parameters in healthy volunteers (study 1) and in subjects with type 2 diabetes (study 2)
study 1 study 2
Clearance Volume Ka Clearance Volume Ka
Mean 305 l/min 1,580 l 2.62/min 188 l/min 1,650 l 1.26/min
SE 46.2 l/min 368 l 1.06/min 25.5 l/min 230 l 0.383/min
CV% 63% 92% 120% 56% 52% 89%
Error model Log normal CV Constant CV variance Additive variance
CV 24% 50% 7.97
CV, coefficient of variance.

CliniCal pharmaCology & TherapeuTiCs 3
articles
as an inhalation, the changes in GLP-1 concentration in plasma over time were found to have the best fit with a two- compartment model with first-order absorption. In patients with type 2 diabetes, the best fit was with a one-compartment model with first-order absorption and first-order elimination (where Ke = clearance/volume). A summary of the pharmaco-kinetic parameters is given in Table 1.
Although the estimated population mean values for clearance and volume of distribution appear to be high, it must be noted that they are not corrected for bioavailability. Previously pub-lished studies using GLP-1 administered by intravenous bolus in healthy subjects and in subjects with type 2 diabetes have esti-mated clearance and volume of distribution to be between 4–9 l/min and 9–26 l, respectively.14 Using the value for volume of distribution previously published in conjunction with our values for inhaled GLP-1, the estimate of bioavailability for MKC253 is between 0.5 and 1.6%. This low value may be secondary to both the inhaled fraction of drug entering the lungs and the dipeptidyl peptidase-4 activity in the lungs and pulmonary vasculature.15 The Ka values of 2.62 min−1 in healthy subjects and 1.26 min−1 in subjects with type 2 diabetes reflect rapid absorption, with the absorptive process being relatively complete within 2–3 min. This finding is also consistent with the pharmacokinetic profiles seen in these studies. Some of the variability in the pharmaco-kinetic parameters may be explained on the basis of intersubject
variability in inhalation technique as well as drug administration on different dosing days with the same subject.
Pharmacodynamics of insulinIn the fasting state, both healthy volunteers and subjects with type 2 diabetes had a rise in GLP-1 levels after inhalation, followed quickly by a rise in insulin and C-peptide levels that peaked within 10–15 min. There was a small delay between the time point of peak GLP-1 level and that of peak insulin level. In subjects with type 2 diabetes, the peak concentration of GLP-1-stimulated insulin was similar in subjects who had fasted and those who had not. This demonstrates that GLP-1 at suffi-cient concentrations can stimulate insulin secretion in the fasting state. In subjects who were in the fasting state, whether they were healthy volunteers or patients with type 2 diabetes, insulin levels returned to baseline within 30–40 min, whereas in subjects with type 2 diabetes who had eaten a meal, the expected prolongation of meal-stimulated insulin was seen for several hours.
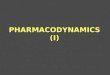
Figures 1 and 2 show the plasma concentrations of GLP-1 and insulin for each dose group in studies 1 and 2, respectively.
A pharmacokinetic–pharmacodynamic (PK–PD) Emax (maxi-mum effect) model was used for each of the studies. In study 1, the rapid equilibration between the plasma GLP-1 and tissue concen-trations allowed for a direct model without a delay between the GLP-1 and insulin. In study 2, an effect compartment improved
Placebo fasted
800
600
400
200
250
200
150
100
50
pmol
/lµU
/ml
mm
ol/l
20
15
10
5
0 60 120 180 240 0 60 120 180 240 0 60 120 180 240 0 60 120 180 240 0 60 120 180 240 0 60 120 180 240
Glucose
InsulinG
LP-1
1.5 mg GLP-1 fasted 1.5 mg GLP-1/placebo fed 1.5 mg GLP-1 × 2 fedPlacebo fed Exenatide fed
Time (min)
Figure 2 Study 2: GLP-1, insulin, and glucose levels by treatment group. The treatment groups are (from left to right) placebo and fasted, 1.5 mg GLP-1 and fasted, placebo and fed, and 1.5 mg GLP-1 given once followed by placebo and fed, 1.5 mg GLP-1 given twice and fed, and 10 µg exenatide and fed. All data and mean lines are shown. GLP-1, glucagon-like peptide 1.

4 www.nature.com/cpt
articles
the model, as a result of the slight delay between the plasma GLP-1 concentrations and the release of insulin. The effect compartment concentration reflects the time required for GLP-1 to interact with the GLP-1R and induce the secretion of insulin and for the insu-lin to appear in the bloodstream. Compartment concentration represents the hypothetical concentration of GLP-1 at the level of the GLP-1R. Figures 1 and 2 show the plasma concentrations of GLP-1 and insulin and the short time delay between the appear-ance of GLP-1 and the appearance of insulin in plasma. The rela-tionship between plasma concentrations of GLP-1 and insulin is shown in Figure 3 for study 1. In study 2, Emax was fitted as a function of baseline glucose, with higher baseline glucose con-centrations associated with a higher Emax, as shown in Figure 4. The PK–PD modeling parameters are shown in Table 2 for GLP-1-induced insulin secretion. Both EC50 (concentration required to produce half the maximal effect) and Emax, depending on the baseline glucose value (maximal output of insulin), were lower in healthy volunteers than in subjects with type 2 diabetes.
Pharmacodynamics of glucose(MKC253) GLP-1 was administered, along with a meal challenge, to patients with type 2 diabetes. The meal consisted of Boost Plus and a 13C-labeled muffin. Changes in glucose excursions as well as GLP-1 and insulin concentrations were tracked. The effect of GLP-1-stimulated insulin secretion is seen in Figure 2. One inhalation of GLP-1 reduced early glucose excursion, and two inhalations separated by 30 min produced a larger reduction in glucose excursion. Inhalation of GLP-1 in the absence of a meal did not produce clinically significant hypoglycemia.
Pharmacodynamics of glucagonIn the study in healthy volunteers, glucagon levels were meas-ured in all the subjects. GLP-1 at the higher doses minimally suppressed glucagon secretion, as shown in Figure 1.
Pharmacodynamics of gastric emptyingIn the study in subjects with type 2 diabetes, gastric emptying was determined by measuring the absorption of 13C octanoate from the meal. Inhaled GLP-1 did not have any significant effect on gastric emptying, as shown in Figure 5.
Patient characteristicsAll 26 subjects in study 1 were healthy, normal subjects without a diagnosis of diabetes.
All 20 subjects (19 Caucasian men and 1 Caucasian woman) in study 2 had a diagnosis of type 2 diabetes. The average age of the cohort was 60 years (range 40–69). The average duration of diabetes was 7.2 years (range 1–23), average body mass index was 27.2 (range 23.2–31.4), average level of hemoglobin A1cwas 7.11% (range 5.7–8.4), and average baseline glucose value was
0 20 40 60
GLP-1 plasma concentration (pmol/l)
50
40
30
20
10
0Bas
elin
e co
rrec
ted
insu
lin p
lasm
a co
ncen
trat
ion
(µU
/ml)
Figure 3 Study 1: insulin response curve in relation to GLP-1 concentration. All data and population predicted mean lines are shown. GLP-1, glucagon-like peptide 1.
table 2 summary of pharmacokinetic–pharmacodynamic modeling parameters in healthy volunteers (study 1) and in subjects with type 2 diabetes (study 2)
Emax (µu/ml insulin) eC50 (glp-1 pmol/l) hill coefficient (γ )
Study 1
Mean 41.7 19.5 2.42
SE 6.47 5.08 0.56
Intersubject variability (% CV) ND 26 27
Error model Constant CV variance Additive variance
Mean 23% 0.13
Emax (µu/ml insulin) eC50 (glp-1 pmol/l) Keo (/min)
Study 2
Mean ± SE by baseline glucose <8 mmol>8–10 mmol>10–12 mmol>12 mmol
34.5 ± 1.948.6 ± 5.369.1 ± 13.1136 ± 36
92.3 ± 32.2 0.041 ± 0.009
Intersubject variability (% CV) 98 26 62
Error model Constant CV variance Additive variance
Mean 5% 22.0
CV, coefficient of variance; Emax, maximum effect; EC50, concentration required to produce half the maximal effect; GLP-1, glucagon-like peptide.

CliniCal pharmaCology & TherapeuTiCs 5
articles
8.76 mmol (range 6.1–14.2). The average serum creatinine level was 94.1 μmol/l (range 64–111). None of the subjects had retinopathy.
safety and adverse eventsTwenty-six healthy normal subjects completed study 1. Seventeen subjects reported adverse events, all of which were considered mild and limited to the time period around dosing. Twelve subjects reported cough, which was mild and limited to the time period around dosing. The cough was not dose related because the subjects in whom it occurred were from different dose groups. None of the subjects reported nausea or vomiting, and none had clinically significant hypoglycemia. None of the subjects withdrew from the study.
Twenty subjects with type 2 diabetes completed study 2. Nineteen subjects reported adverse events, all of which were considered mild except for 2 moderate events. The 2 events were in one subject who was given exenatide and experienced nausea and vomiting; another subject had an intravenous catheter site infection, which was not considered to be related to study drug administration. Fifteen subjects reported cough, which was mild and limited to the time period around dosing. Cough consti-tuted 85% of the adverse events. One subject who was given MKC253 had nausea, and three subjects given exenatide had nausea, with one subject having nausea and vomiting. None of the subjects had clinically significant hypoglycemia. One sub-ject discontinued the study because of infection at the site of an intravenous catheter.
0 100 200 300 0 100 200 300 0 100 200 300 0 100 200 300
GLP-1 plasma concentration (ng/ml)
150
100
50
0
Insu
lin p
lasm
a co
ncen
trat
ion
(µU
/ml)
<8 mmol/l >8–10 mmol/l >10–12 mmol/l >12 mmol/l
Figure 4 Study 2: insulin response curves in relation to GLP-1 concentration, categorized by baseline glucose concentration. All data and population predicted mean lines are shown. GLP-1, glucagon-like peptide 1.
0 60 120 180 240 0 60 120 180 240 0 60 120 180 240
Time (min)
60
70
80
90
100
% R
emai
ning
in th
e st
omac
h
Placebo 1.5 mg GLP-1 2 Doses 1.5 mg GLP-1
Figure 5 Study 2: gastric-emptying effect of GLP-1 treatment. All data and mean lines are shown. GLP-1, glucagon-like peptide 1.

6 www.nature.com/cpt
articles
DiscussionGLP-1, as MKC253, when administered via the pulmonary route, is rapidly absorbed and stimulates insulin secretion sufficient to reduce meal-induced glucose excursions in subjects with type 2 diabetes. Inhaled GLP-1 stimulates C-peptide secretion to levels comparable to those of insulin secretion but minimally suppresses glucagon secretion. The rapid pulmonary absorption produces peak levels of GLP-1 within several minutes, but it is then degraded rapidly, with levels returning to baseline values with 30 min. The absorption rate constant, volume of distribu-tion, and clearance of GLP-1 were similar in healthy volunteers and in subjects with type 2 diabetes, as has been reported else-where.14 It should be noted, however, that the values of absorp-tion rate constant and clearance were slightly lower in subjects with diabetes. GLP-1 is metabolized by dipeptidyl peptidase-4 and cleared by the kidney16; in subjects with mild renal dysfunc-tion, its clearance is lower.17 Pulmonary function also is lower in patients with type 2 diabetes,18,19 and this may explain the slightly lower absorption rate constant in these patients. The good fit provided by the two-compartment model in healthy normal subjects is probably attributable to the slightly faster tissue uptake and distribution of GLP-1, the known decrease in dipeptidyl peptidase-4 activity, and the slower absorption rate in subjects with type 2 diabetes.20 For similar doses of GLP-1, the plasma concentrations attained after the inhalation route of administration were much higher than those reported after oral administration.21,22 The inhalation device used in our trial was a prototype and was not optimized for delivery of GLP-1. The more prolonged concentration-vs.-time profiles of insulin and C-peptide simply reflect their longer half-lives.
There is a difference between healthy subjects and those with type 2 diabetes with respect to the effects GLP-1 on insulin secre-tion. Both EC50 and Emax were lower in healthy volunteers than in subjects with type 2 diabetes. These differences may be due to inherent differences in insulin secretion response to GLP-1 stim-ulation, differences in genetic polymorphisms of GLP-1Rs,23 and the fact that subjects with type 2 diabetes have higher baseline glucose values.24,25 For instance, the insulin response in subjects with type 2 diabetes who had baseline glucose values <8 mmol/l were similar to those in healthy subjects but required higher GLP-1 concentrations to stimulate insulin secretion.
The administration of GLP-1 as an inhalant in patients with type 2 diabetes produced a rapid and transient secretion of insu-lin that seemed to mimic the first-phase response seen in normal subjects given a square-wave glucose infusion. This rapid appear-ance of insulin was able to blunt the early glucose excursion seen after a meal in subjects with type 2 diabetes. GLP-1-stimulated insulin secretion was also dependent on baseline glucose values, with higher baseline glucose values being associated with higher peak concentrations of insulin for the same concentrations of GLP-1. This finding confirms that GLP-1 insulin secretion is glucose dependent. The delivery of GLP-1 rapidly produces a pulse-like insulin secretion. This pulse-like secretion has been shown to improve glucose-lowering effects as compared with more prolonged insulin infusions at steady rates.26,27 This effect is similar to that of the metiglinides.28
The administration of GLP-1 by inhalation was also notable for a lack of GI side effects. The absence of an effect on gastric motility was a surprising finding. The reported plasma concen-trations of GLP-1 after intravenous administration are similar to those found in the subjects in our study after the administra-tion of inhaled GLP-129 However, whereas these concentrations were associated with profound GI adverse effects after intrave-nous GLP-1, similar concentrations in our studies using inhaled GLP-1 did not produce any GI adverse effects. The reason for this is unknown, but it may implicate pulmonary GLP-1Rs.30
Studies 1 and 2 demonstrate the feasibility of delivering GLP-1 via the pulmonary route. The administration of GLP-1 as an inhalant stimulated insulin secretion to a sufficient extent to blunt postprandial glucose excursions in subjects with type 2 diabetes, without producing the adverse GI effects that are seen with s.c. or intravenous administration of GLP-1 or its analogs. The prospect of utilizing inhaled GLP-1 as a therapeutic agent for the treatment of diabetes is quite attractive for two reasons. First, the use and exposure are intermittent and may therefore obviate some of the adverse events that have been associated with long-acting GLP-1 analogs. Second, the administration of GLP-1 rapidly and briefly produces a response that closely mimics that seen in healthy subjects, and reproduces the “first-phase” pattern of insulin secretion that seems to be absent in patients with type 2 diabetes without producing a prolonged stimulation of the β-cell or a prolonged “hyperinsulinemia.”
MethoDsStudy 1, carried out in healthy subjects, was a phase I, single-dose trial that incorporated an open-label, ascending-dose structure to determine the safety and tolerability of MKC253. The study was consistent with 21 CFR 312, Good Clinical Practice: Consolidated Guidance (ICH E6), and the Guidance on General Considerations for Clinical Trials (ICH E8). The trial consisted of three periods: (i) a screening visit to determine the subject’s eligibility; to obtain informed consent; to measure baseline levels of C-peptide, fasting blood glucose (FBG), and insulin; and to carry out pulmonary function tests; (ii) a treatment visit during which a single dose of MKC253 inhalation powder was administered; and (iii) a follow-up visit that was planned to occur 8–14 days after treatment. The trial objectives were to evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of MKC253 in each dose cohort. Dose escala-tion was carried out only after all the safety and tolerability data for the prior dose had been reviewed by the principal investigator and the spon-sor. A half-hour lag time was implemented between dose administration to successive subjects in each group so as to monitor adverse reactions and thereby protect the safety of the subjects. The dosing was planned to be halted if three or more subjects within a cohort experienced severe nausea and/or vomiting, or when the maximum dose was reached, or at the discretion of the principal investigator. The response to MKC253 inhalation powder was assessed for five doses: 0.05, 0.45, 0.75, 1.05, and 1.5 mg GLP-1. The lowest two dose levels were evaluated in two cohorts of four subjects each, and the three higher dose levels were evaluated in three cohorts of six subjects each. Each subject received only one dose. Blood samples were drawn at protocol-specified time points for meas-urement of GLP-1 (active and total), FDKP, glucagon, glucose, insulin, and C-peptide between the time point immediately before the adminis-tration of the dose and at 120 min after the dose. The dosing was carried out with the subjects in the fasting condition. At 125 min after the dose, they were given a snack of orange juice and fruit, and at 240 min after the dose, they were given a full meal.
Plasma samples for measuring the concentrations of active and total GLP-1 and glucagon were stored frozen at −70 °C at the clinical site until

CliniCal pharmaCology & TherapeuTiCs 7
articles
shipment for bioanalytical analysis to Pharmaceutical Research Associates International (PRA), Early Development Services, Bioanalytical Labora-tory (Assen, The Netherlands) or PRA International, Early Develop ment Services, Clinical Laboratory (Zuidlaren, The Netherlands), for assess-ment of glucose, insulin, and C-peptide levels.
Study 2, carried out in subjects with type 2 diabetes, was a phase I, single-dose, placebo- and active comparator–controlled, repeat- administration trial incorporating a partial double-blind, randomized treatment design that was consistent with 21 CFR 312, Good Clini-cal Practice: Consolidated Guidance (ICH E6), and the Guidance on General Considerations for Clinical Trials (ICH E8) to determine the safety and tolerability of MKC253. The Clinical Trials Registry identifier for this study is NCT00642538. The placebo was Technosphere inhalation powder without GLP-1 (referred to as T inhalation powder). The clinical trial included four periods. The first was a screening visit to determine the subject’s eligibility; to obtain informed consent; to measure base-line levels of C-peptide, FBG and insulin; and to carry out pulmonary function tests (between 5 and 2 weeks before dosing). Second, after the screening visit and 2 weeks before dosing, a washout period started for all subjects during which all antidiabetic treatment was stopped and the FBG levels of the subjects were monitored on a daily basis. Subjects in whom the FBG level exceeded 13.5 mmol/l on two occasions during the washout period were to resume their original treatment and were to be excluded from the trial. The third period was the treatment period. Sub-jects stayed in the clinic from day 1 (~17 h before the first dosing) to day 10 (at least 24 h after the last dose had been administered). Five differ-ent treatments were administered on days 1, 3, 5, 7, and 9. Subjects in whom the FBG value exceeded 14.9 mmol/l during the treatment period were to be removed from participation in the trial and were to resume their original treatment. The fourth period consisted of a follow-up visit 8–14 days after each subject’s last treatment. Each of the subjects received five different treatments. All the subjects received treatment 1 as the first treatment, followed by treatments 2–5 in a randomly assigned sequence. Treatment 1 was administered in an open-label fashion, and treatments 2–5 were administered in a double-blind fashion. The treatments are listed below:
1. Treatment 1: 1.5 mg GLP-1 as MKC253 inhalation powder (in 15 subjects) or T inhalation powder (in 5 subjects), with con-tinued fasting after dosing
2. Treatment 2: 1.5 mg GLP-1 as MKC253 inhalation powder imme-diately before and 30 min after the meal (total 3.0 mg GLP-1) pre-ceded by an s.c. saline injection 15 min before the meal
3. Treatment 3: 1.5 mg GLP-1 as MKC253 inhalation powder imme-diately before the meal and T inhalation powder 30 min after the meal, preceded by an s.c. saline injection 15 min before the meal
4. Treatment 4: T inhalation powder immediately before and 30 min after the meal, preceded by an s.c. saline injection 15 min before the meal (placebo comparison)
5. Treatment 5: T inhalation powder immediately before and 30 min after the meal, preceded by a 10-µg exenatide injection administered s.c. 15 min before the meal (active comparison)
Blood samples were collected in order to measure plasma levels of GLP-1, insulin, glucagon, C-peptide, and glucose, both prior to admin-istration of MKC253 and for up to 240 min after administration. Plasma samples for measuring concentrations of active and total GLP-1 and glu-cagon were stored frozen at −70 °C at the clinical site until shipment for bioanalytical analysis to PRA International, Early Development Services, Bioanalytical Laboratory, or PRA International, Early Development Services, Clinical Laboratory, for measurement of glucose, insulin, and C-peptide levels.
In order to evaluate gastric emptying, a muffin containing 13C octanoate (Na–13C–octanoate, 100 mg) was administered as part of the standard meal after treatments 2–5. The ingredients to prepare this muf-fin were provided to PRA International by Metabolic Solutions (Nashua, NH). The standardized meal consisted of 240 ml of Boost high-protein drink and one muffin containing 13C octanoate. The total caloric value
of the meal was 575 kcal, and the meal contained a total of 24 g protein, 97 g carbohydrates, and 13 g lipids. Breath-test samples were obtained for 13C assessment in expired air to measure gastric emptying. The samples were collected by asking the subjects to blow into exetainers (10-ml plain tubes) through drinking straws. Gastric emptying was measured indirectly by monitoring the appearance of 13CO2 in the exhaled breath subsequent to ingestion and metabolism of 13C octanoate. The stand-ardized meal was eaten in 10 min or less, and samples were collected every 15 min for 4 h thereafter. The samples were analyzed at Metabolic Solutions.
All pharmacokinetics and PK–PD modeling was carried out using NONMEM version VI 2.0 on a on an HP xw4550 workstation, and the data were graphed in R version 2.10.1 using the ggplot2 and lattice packages. Both models included parameters for intersubject variability as well as residual variance.
conFlict oF inteRestEach of the authors is a full-time employee of either MannKind Corporation or PRA.
© 2010 American Society for Clinical Pharmacology and Therapeutics
1. Orskov, C., Wettergren, A. & Holst, J.J. Biological effects and metabolic rates of glucagonlike peptide-1 7-36 amide and glucagonlike peptide-1 7-37 in healthy subjects are indistinguishable. Diabetes 42, 658–661 (1993).
2. Drucker, D.J. Minireview: the glucagon-like peptides. Endocrinology 142, 521–527 (2001).
3. Gallwitz, B. The evolving place of incretin based therapies in type 2 diabetes. Pediatr. Nephrol. (2010); e-pub ahead of print 4 February 2010.
4. Bullock, B.P., Heller, R.S. & Habener, J.F. Tissue distribution of messenger ribonucleic acid encoding the rat glucagon-like peptide-1 receptor. Endocrinology 137, 2968–2978 (1996).
5. Alvarez, E. et al. The expression of glp 1 receptor mrna and protein allows the effect of glp 1 on glucose metabolism in the human hypothalamus and brainstem. J. Neurochem. 92, 798–806 (2005).
6. Davis, H.R. Jr et al. Effect of chronic central administration of glucagon-like peptide-1 (7-36) amide on food consumption and body weight in normal and obese rats. Obes. Res. 6, 147–156 (1998).
7. Meeran, K. et al. Repeated intracerebroventricular administration of glucagon-like peptide-1-(7-36) amide or exendin-(9-39) alters body weight in the rat. Endocrinology 140, 244–250 (1999).
8. Baggio, L.L., Kim, J.G. & Drucker, D.J. Chronic exposure to glp 1r agonists promotes homologous glp 1 receptor desensitization in vitro but does not attenuate glp 1r dependent glucose homeostasis in vivo. Diabetes 53 (suppl 3), S205–S214 (2004).
9. Buse, J.B. et al. Effects of exenatide (exendin 4) on glycemic control over 30 weeks in sulfonylurea treated patients with type 2 diabetes. Diabetes Care 27, 2628–2635 (2004).
10. Parks, M. & Rosebraugh, C. Weighing risks and benefits of liraglutide–the FDA’s review of a new antidiabetic therapy. N. Engl. J. Med. 362, 774–777 (2010).
11. Quddusi, S., Vahl, T.P., Hanson, K., Prigeon, R.L. & D’Alessio, D.A. Differential effects of acute and extended infusions of glucagons like peptide 1 on first and second phase insulin secretion in diabetic and nondiabetic humans. Diabetes Care 26, 791–798 (2003).
12. Larsen, J., Hylleberg, B., Ng, K. & Damsbo, P. Glucagon-like peptide-1 infusion must be maintained for 24 h/day to obtain acceptable glycemia in type 2 diabetic patients who are poorly controlled on sulphonylurea treatment. Diabetes Care 24, 1416–1421 (2001).
13. Leone-Bay, A. et al. Evaluation of novel particles as an inhalation system for GLP-1. Diabetes. Obes. Metab. 11, 1050–1059 (2009).
14. Vilsbøll, T., Agersø, T., Krarup, T. & Holst, J.J. Similar elimination rates of glucagon-like peptide-1 in obese type 2 diabetic patients and healthy subjects. J. Clin. Endocrinol. Metab. 88, 220–224 (2003).
15. Abbott, C.A., Baker, E., Sutherland, G.R. & McCaughan, G.W. Genomic organization, exact localization, and tissue expression of the human CD26 (dipeptidyl peptidase IV) gene. Immunogenetics 40, 331–338 (1994).
16. Ruiz-Grande, C., Pintado, J., Alarcón, C., Castilla, C., Valverde, I. & López-Novoa, J.M. Renal catabolism of human glucagon-like peptides 1 and 2. Can. J. Physiol. Pharmacol. 68, 1568–1573 (1990).
17. Lugari, R. et al. Urinary excretion of glucagon like peptide 1 (glp 1) 7 36 amide in human type 2 (non insulin dependent) diabetes mellitus. Horm. Metab. Res. 33, 568–571 (2001).

8 www.nature.com/cpt
articles
18. Kaminsky, D.A. Spirometry and diabetes: implications of reduced lung function. Diabetes Care 27, 837–838 (2004).
19. Goldman, M.D. Lung dysfunction in diabetes. Diabetes Care 26, 1915–1918 (2003).
20. McKillop, A.M., Duffy, N.A., Lindsay, J.R., O’Harte, F.P., Bell, P.M. & Flatt, P.R. Decreased dipeptidyl peptidase iv activity and glucagons like peptide 1(736)amide degradation in type 2 diabetic subjects. Diabetes Res. Clin. Pract. 79, 79–85 (2008).
21. Beglinger, C. et al. Pharmacokinetics and pharmacodynamic effects of oral GLP-1 and PYY3-36: a proof-of-concept study in healthy subjects. Clin. Pharmacol. Ther. 84, 468–474 (2008).
22. Steinert, R.E. et al. Orally administered glucagon-like peptide-1 affects glucose homeostasis following an oral glucose tolerance test in healthy male subjects. Clin. Pharmacol. Ther. 86, 644–650 (2009).
23. Villareal, D.T. et al. Tcf7l2 variant rs7903146 affects the risk of type 2 diabetes by modulating incretin action. Diabetes 59, 479–485 (2010).
24. Kjems, L.L., Holst, J.J., Vølund, A. & Madsbad, S. The influence of glp 1 on glucose stimulated insulin secretion: effects on beta cell sensitivity in type 2 and nondiabetic subjects. Diabetes 52, 380–386 (2003).
25. Vilsbøll, T., Krarup, T., Madsbad, S. & Holst, J.J. Both glp 1 and gip are insulinotropic at basal and postprandial glucose levels and contribute nearly equally to the incretin effect of a meal in healthy subjects. Regul. Pept. 114, 115–121 (2003).
26. Paolisso, G. et al. Pulsatile insulin delivery has greater metabolic effects than continuous hormone administration in man: importance of pulse frequency. J. Clin. Endocrinol. Metab. 72, 607–615 (1991).
27. Paolisso, G. et al. Pulsatile insulin delivery is more efficient than continuous infusion in modulating islet cell function in normal subjects and patients with type 1 diabetes. J. Clin. Endocrinol. Metab. 66, 1220–1226 (1988).
28. Hollander, P.A. et al. Importance of early insulin secretion: comparison of nateglinide and glyburide in previously diet treated patients with type 2 diabetes. Diabetes Care 24, 983–988 (2001).
29. Little, T.J. et al. Effects of intravenous glucagons like peptide 1 on gastric emptying and intragastric distribution in healthy subjects: relationships with postprandial glycemic and insulinemic responses. J. Clin. Endocrinol. Metab. 91, 1916–1923 (2006).
30. Korner, M., Stockli, M., Waser, B., & Reubi, J.C. Glp 1 receptor expression in human tumors and human normal tissues: potential for in vivo targeting. J. Nucl. Med. 48, 736–743 (2007).