Embed Size (px)
Citation preview
Pharmacoltinetic-pharmacodynamic relationships of controlled-release oxycodone
Plasma concentrations of oxycodone, oxymorphone, and noroxycodone were determined after adminis- tration of 20 mg oral controlled-release oxycodone tablets to four subject groups: young (aged 21 to 45 years) men, elderly (aged 65 to 79 years) men, young women, and elderly women. Area under the oxycodone and noroxycodone concentration-time curve (AUC) values were comparable among the four groups. Compared with oxycodone, the oxymorphone AUC values were small, with significant differences between subject groups. AUC values were also calculated for the pharmacodynamic variable “drug effect,” scored on a 100 mm visual analog scale. The two groups with the highest oxycodone AUC values (young and elderly women) had the lowest oxymorphone AUC values and the greatest drug effect AUC values. The two groups with the lowest oxycodone AUC values (young and elderly men) had the highest oxymorphone AUC values and the lowest drug effect AUC values. These results support oxycodone, and not oxymorphone, as being primarily responsible for pharmacodynamic and analgesic effects. ( CLIN PHAR-
MACOL THER 1996;59:52-61.)
Robert F. Kaiko, PhD, David I’. Benziger, PhD, Ronald D. Fitzmartin, PhD, Brian E. Burke, PhD, Robert F. Reder, MD, and Paul D. Goldenheim, MD Nomalk, Corm.
Oxycodone is a strong opioid analgesic that has been available for clinical use since 1915.1’2 In the United States, oxycodone is most widely used in fixed combinations with acetaminophen or acetylsal- icylic acid for the management of moderate to mod- erately severe pain. Recently, single-agent oxy- codone has been recognized as an alternative to oral morphine for the management of postoperative3 and cancer-related4’s pain, and controlled-release oxycodone and other opioids have been reported to provide relief for some patients whose postherpetic neuralgia did not respond to tricyclic antidepres- sants or nonsteroidal antiinflammatory drugs.6
Metabolism of oxycodone in animals and humans proceeds by way of N-demethylation (noroxy- codone), O-demethylation (oxymorphone), 6-keto reduction (6-oxycodol), and conjugation with glucu- ronic acid.7-13 The unconjugated oxycodone metab-
From the Purdue Frederick Company. Sponsored by The Purdue Frederick Company, Norwalk, Conn. Received for publication April 26, 1995; accepted Aug. 16, 1995. Reprint requests: Robert F. Kaiko, PhD, The Purdue Frederick
Company, 100 Connecticut Ave., Norwalk, CT 06850-3590. Copyright 0 1996 by Mosby-Year Book, Inc. 0009-9236/96/$5.00 + 0 1311168641
52
olites that have been identified in humans and con- sidered to possibly contribute to opioid effects after oxycodone administration include noroxycodone and oxymorphone. Of these metabolites, only oxy- morphone has been shown to have clinically signif- icant opioid agonist activity in humans, with a rela- tive potency estimated to be approximately 14 times that of oxycodone when both drugs are administered parenterally.14 In contrast, the opioid activity of nor- oxycodone has not been established in humans. However, the decreased antinociceptive activity of noroxycodone, compared with oxycodone, has been demonstrated in animal studies.15 Given the results of animal studies and the diminished analgesic ac- tivity of normorphine compared with that of mor- phine,16 it is unlikely that noroxycodone produced during the metabolism of oxycodone would have significant opioid agonist activity.
The high analgesic potency of oxymorphone com- pared with oxycodone and the results of opioid- receptor binding studies have led some investigators to suggest that oxymorphone could be responsible, at least in part, for the analgesic activity of oxy- codone.5a17 Recently, Otton et al.” suggested that the P450-dependent conversion of oxycodone to
CLINICAL PHAKMACOLOGY &THERAPEUTICS VOLUME 59, NUMBER 1 Ibib et al. 53
oxymorphone may be responsible for the analgesic effects of oxycodone, as is proposed for the conver- sion of hydrocodone and codeine to hydromor- phone and morphine, respectively. The extent of such metabolite-mediated analgesia could vary be- cause of genetic differences in P450 activity, al- though such variation would have little or no impact in the clinical setting because oxycodone doses are usually titrated to effect. In fact, the pharmacologic activity of oxymorphone produced by metabolism of oxycodone is uncertain; results of animal studies have not been consistent with the hypothesis that oxymorphone is the principal pharmacologically ac- tive agent after oxycodone administration” and, in human studies, oxymorphone plasma concentrations have been reported to remain below the measurable limit.11’20 Thus assessment of the pharmacokinetic- pharmacodynamic relationships of oxymorphone produced during the metabolism of oxycodone has been difficult.
This study was undertaken to compare the phar- macokinetics of oxycodone and its metabolites oxy- morphone and noroxycodone in young and elderly male and female volunteers after administration of one 20 mg controlled-release oxycodone tablet. In addition, correlations between pharmacodynamic effects and the pharmacokinetic profiles of oxy- codone and oxymorphone were estimated.
METHODS Study design and subject selection. The 28 healthy
volunteers enrolled in this open-label, analytically blinded, single-dose parallel-group study comprised four groups of seven subjects each: young men, young women, elderly men, and elderly women (Ta- ble I). All subjects gave written informed consent before participating in the study, and the study was approved by the ethics committee of GFI Pharma- ceutical Services, Inc. (Evansville, Ind). Volunteers with known hypersensitivity to opioids or with a history of nausea, emesis, drug abuse, or any condi- tion known to interfere with blood sampling or drug disposition were excluded from the study. Female volunteers of childbearing potential were excluded. All subjects were free of significant abnormal find- ings during baseline physical examination, clinical laboratory testing, and assessment of vital signs.
Drug administration and blood sample analysis. Subjects received a single 20 mg dose of oral controlled-release oxycodone hydrochloride (Oxy- Contin tablets, Purdue Pharma LP, Norwalk, Conn.) while fasting. Blood samples were collected in tubes
Table I. Characteristics of subjects enrolled in the study
Men Women
Characteristic Young Elderly Young Elderly (n = 7) (n = 7) (n = 7) (12 = 7)
Age (yr) Mean Range
Height (cm) Mean Range
Weight (kg) Mean Range
28 73 37 70 21-39 68-79 24-45 65-78
179 175 166 159 168-183 168-185 155-178 X0-165
72 81 66 68 62-84 69-92 54-85 47-78
containing the anticoagulant ethylenediaminetetra- acetic acid at 0, r/2, 1, lY2, 2,2X, 3, 3X, 4,5, 6, 8, 10, 12, 18, 24, 30, 36, and 48 hours after dosing. Plasma was obtained by centrifugation and frozen until an- alyzed by a validated gas chromatographicimass spectrometric (GUMS) procedure. Plasma samples were spiked with d,-oxycodone and d,-noroxycodone as internal standards and 1 ml of pH 6 phosphate buffer was added. The sample was applied to a pre- conditioned mixed-mode resin solid-phase extraction column. After rinsing, the analytes were eluted with methylene chlorideiisopropanol(4: 1, vol/vol) contain- ing 2% ammonium hydroxide. The eluent was evapo- rated to dryness and derivatized with acetic anhydridel pyridine (1:l). Aliquots (2 ~1) were analyzed with use of an HP5890 GUHP5890 MS (Hewlett-Packard Co., Palo Alto, Calif.), equipped with 15 m X 0.32 mm, 0.25 km film DB17-50% phenyl methyl silicone column (J&W Scientific, Folsom, Calif.). The column was op- erated with a helium inlet pressure of 100 kPa and septum purge of 5 ml/min. After an initial hold of 1 minute at 180” C, the temperature was increased to 280” C at 20” C/min. The MS was operated in the negative chemical ionization mode with methane as the reagent gas. The peak area ratios of the M+ ions (m/z) were used to construct standard curves: oxycodone (357)/d,-oxycodone (360); oxymorphone (385)/d,-oxycodone (357); and noroxycodone (343)/d,- noroxycodone (346). The standard curves were linear over the range from 0.2 to 100 rig/ml for all analytes. The interday variability (coefficients of variability) based on quality control samples with nominal concen- trations of 0.5,5,20, and 50 @ml ranged from 6.8% to 9.5% for oxycodone, from 7.6% to 9.2% for oxymor- phone, and from 3.0% to 12.1% for noroxycodone.
54 I(a&o et al. CLINCAL PHARMACOLOGY &THERAPEUTICS
JANUARY 1996
Pharmacodynamic assessment. A drug effect ques- tionnaire that included 10 of the 22 items used by Preston et al.‘l was completed by each subject and an observer at baseline and immediately before each blood sample was drawn, except for the 1% and 30-hour samples. The subjects rated each of the following items on a 100 mm visual analog scale (VAS) anchored on one end by “not at all” and the other end by “an awful lot”: (1) Do you feel any effects of the drug? (2) Does your skin feel itchy? (3) Do you feel relaxed? (4) Do you feel sleepy? (5) Do you feel drunk? (6) Do you feel nervous? (7) Do you feel full of energy? (8) Do you feel the need to talk? (9) Do you feel sick to your stomach? and (10) Do you feel dizzy? In addition, the subjects used a VAS to rate their mood from “worst mood” to “best mood” and their level of sedation from “asleep” to “awake.” The following items were rated by the observer using a VAS anchored on one end by “not at all” and the other end by “extremely”: (1) Is the subject showing any drug effects? (2) Is the subject scratching? (3) Is the subject relaxed? (4) Is the subject drunk? (5) Is the subject nervous? (6) Is the subject talking? (7) Is the subject vomiting? (8) Is the subject confused? (9) Is the subject restless? and (10) Is the subject perspiring? In addition, both respiratory rate and pupil size were measured. Re- sponses to questionnaires were obtained indepen- dently from subjects and observer, and precautions were taken to prevent subjects from disclosing their ratings to other subjects.
Statistical and pharmacokinetic analysis. Time- concentration and time-effect curves were generated from the data with use of arithmetic means of plasma concentrations and drug effect scores at each sample time. Plasma concentrations of oxycodone and metabolites that were less than 0.2 rig/ml were reported as zero (0). For each analyte, the peak plasma concentration (C,,,) was defined as the highest observed concentration and the time to C,,, (t,=) was defined as the postdose time at which C,,, was observed. The area under the analyte con- centration-time curves (ng * hriml) and drug effect- time curves (mm * hr) from 0 to 48 hours (AUC) were calculated by use of the trapezoidal method. SAS (SAS Institute, Cary, N.C.) and in-house sta- tistical programs (C++) were used for pharmaco- kinetic and pharmacodynamic analyses. Scores from pharmacodynamic assessments for all subjects were included in calculations of pharmacodynamic AUC values. A one-way ANOVA was used to test group differences for AUC and C,, at the 01 = 0.05 level
of significance. A weighted Pearson correlation of the pharmacodynamic variables and plasma concen- trations was performed with use of the sum of squares regression for each subject. Subjects whose plasma oxymorphone concentrations remained be- low the measurable limit (less than 0.2 rig/ml) were not included in correlation analysis for oxymor- phone. Chi square analysis was used to detect dif- ferences in the incidence of adverse experiences between subject groups.
RESULTS Pharmacokinetics
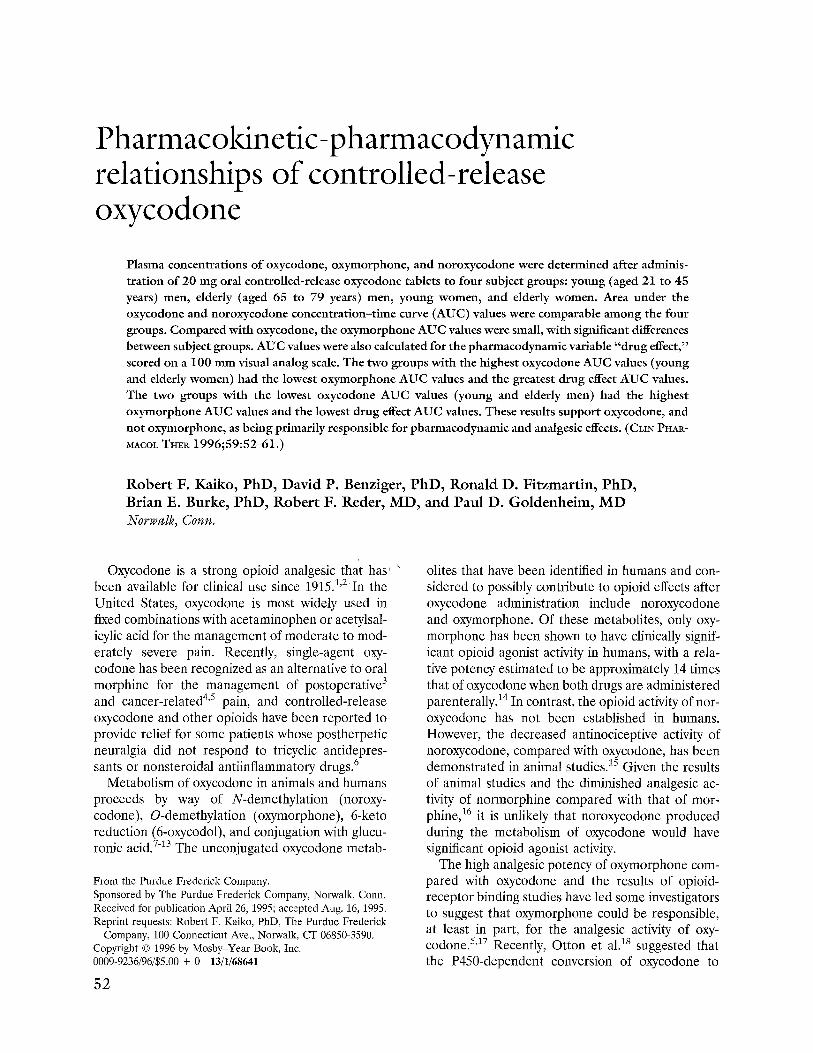
All subjects. The mean plasma oxycodone con- centrations for all subjects were higher than the mean oxymorphone or noroxycodone concentra- tions at each sample time through 12 hours after dosing (Fig. 1). For 10 subjects (six elderly women, three young women, and one elderly man), all postdose plasma samples (n = 18 per subject) had plasma oxymorphone concentrations below the measurable limit (co.2 rig/ml). The remaining subjects had at least one plasma sample with an oxymorphone level greater than 0.2 rig/ml. The mean ? SD AUC was 236 2 102 ng * hr/ml for oxycodone, 233 t 102 ng * hr/ml for noroxy- codone, and 12.3 t 12 ng * hr/ml for oxymor- phone. C,,, values of 23.2 ? 8.6 rig/ml for oxy- codone, 15.2 i 4.5 ngiml for noroxycodone, and 0.82 t 0.85 rig/ml for oxymorphone occurred at 3.2, 4.3, and 4.5 hours after dosing, respectively.
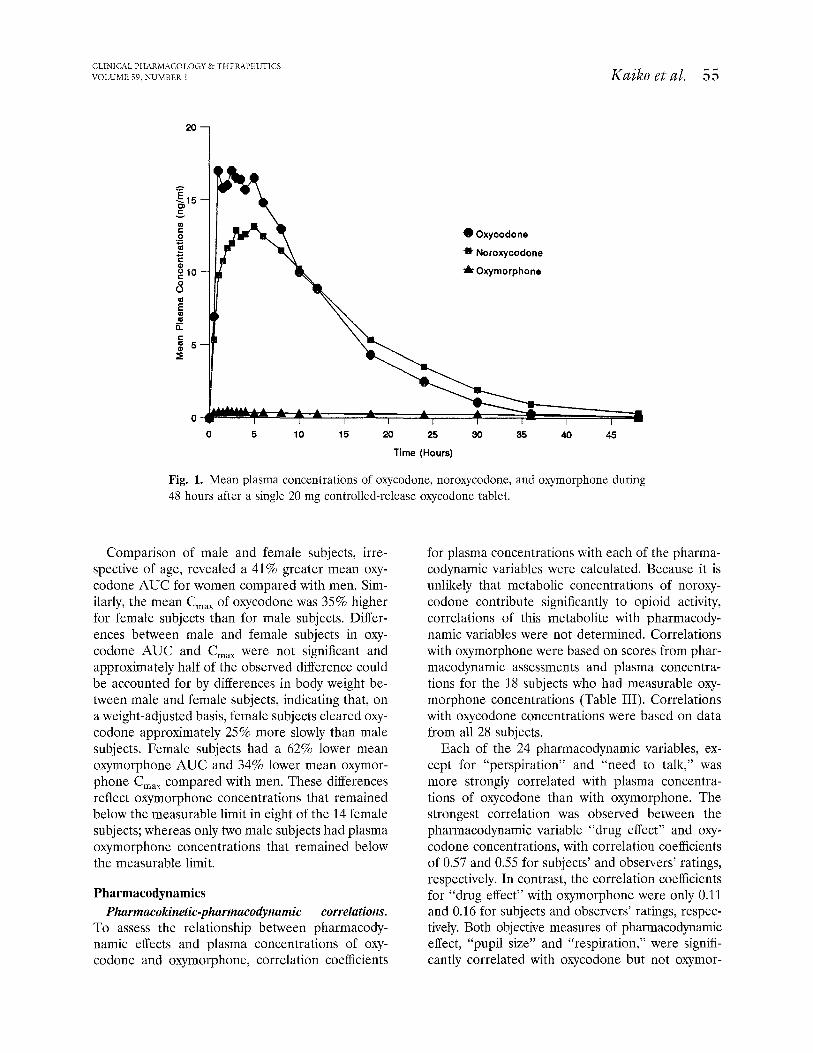
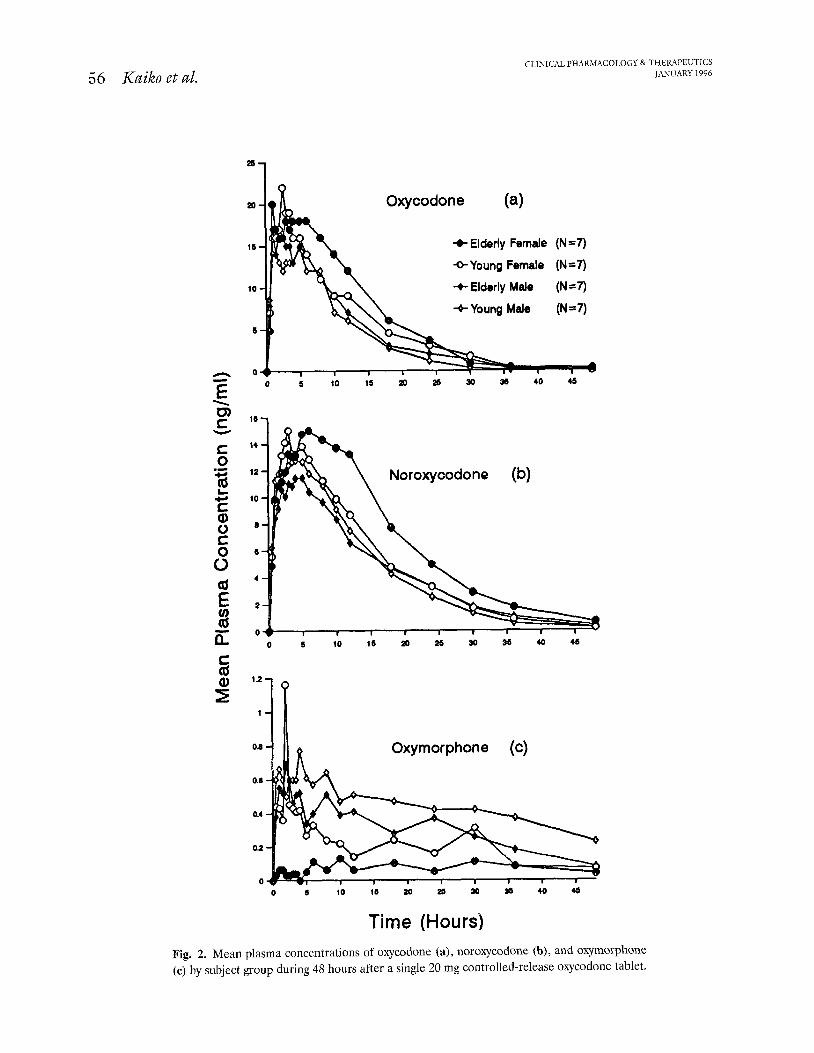
Comparisons by subject group. The mean concen- tration-time curves for oxycodone, noroxycodone, and oxymorphone were compared for the four sub- ject groups (Fig. 2). Based on AUC values for oxy- codone, absorption of the drug was greatest in eld- erly women, followed by young women, elderly men, and young men (Table II). In contrast, the greatest oxymorphone AUC occurred in young men, fol- lowed by elderly men and young women. Elderly women had the lowest oxymorphone AUC, with measurable oxymorphone concentrations in only one of the seven subjects in this group. The rank order of noroxycodone AUC values was similar to that of oxycodone. Differences between the four groups in oxycodone AUC values (p = 0.161) and noroxycodone AUC values (‘JJ = 0.203) were not significant, whereas the oxymorphone AUC was sig- nificantly greater in young men compared with young and elderly women and significantly greater in elderly men compared with elderly women (p = 0.018).
CLINICAL PHARMACOLOGY & THERAI’ELJTICS VOLUME 59, NUMBER 1 IGxiko et al. 55
d Oxycodone
* Noroxycodone
p Oxymorphone
20 25
Time (Hours)
Fig. 1. Mean plasma concentrations of oxycodone, noroxycodone, and oxymorphone during 48 hours after a single 20 mg controlled-release oxycodone tablet.
Comparison of male and female subjects, irre- spective of age, revealed a 41% greater mean oxy- codone AUC for women compared with men. Sim- ilarly, the mean C,, of oxycodone was 35% higher for female subjects than for male subjects. Differ- ences between male and female subjects in oxy- codone AUC and C,,, were not significant and approximately half of the observed difference could be accounted for by differences in body weight be- tween male and female subjects, indicating that, on a weight-adjusted basis, female subjects cleared oxy- codone approximately 25% more slowly than male subjects. Female subjects had a 62% lower mean oxymorphone AUC and 34% lower mean oxymor- phone C,,, compared with men. These differences reflect oxymorphone concentrations that remained below the measurable limit in eight of the 14 female subjects; whereas only two male subjects had plasma oxymorphone concentrations that remained below the measurable limit.
Pharmacodynamics Pharmacokinetic-pharmacodynamic correlations.
To assess the relationship between pharmacody- namic effects and plasma concentrations of oxy- codone and oxymorphone, correlation coefficients
for plasma concentrations with each of the pharma- codynamic variables were calculated. Because it is unlikely that metabolic concentrations of noroxy- codone contribute significantly to opioid activity, correlations of this metabolite with pharmacody- namic variables were not determined. Correlations with oxymorphone were based on scores from phar- macodynamic assessments and plasma concentra- tions for the 18 subjects who had measurable oxy- morphone concentrations (Table III). Correlations with oxycodone concentrations were based on data from all 28 subjects.
Each of the 24 pharmacodynamic variables, ex- cept for “perspiration” and “need to talk,” was more strongly correlated with plasma concentra- tions of oxycodone than with oxymorphone. The strongest correlation was observed between the pharmacodynamic variable “drug effect” and oxy- codone concentrations, with correlation coefficients of 0.57 and 0.55 for subjects’ and observers’ ratings, respectively. In contrast, the correlation coefficients for “drug effect” with oxymorphone were only 0.11 and 0.16 for subjects and observers’ ratings, respec- tively. Both objective measures of pharmacodynamic effect, “pupil size” and “respiration,” were signifi- cantly correlated with oxycodone but not oxymor-
56 Kuiko et al. CLINICAL PHARMACOLOGY & THEMI’EUTICS
JANUARY 1996
Oxycodone (a)
+ Elderly Female (N=7)
*Young Female (N=7)
t Elderly Male (N=7)
14
12
10
5
5
4
2
o--- I 0 5 IO 15 30 35 40 45
-I II 6 Oxymorphone (c)
10 15 20 zs 30 35 40 45
Time (Hours) Fig. 2. Mean plasma concentrations of oxycodone (a), noroxycodone (b), and oxymorphone (c) by subject group during 48 hours after a single 20 mg controlled-release oxycodone tablet.
CLINICAL PHARMACOLOGY &THERAPEUTICS VOLUME 59, NUMBER I Kaiko et al. 57
Table II. Mean AUC for oxycodone, noroxycodone, oxymorphone, and subject-rated drug effect
AUC ? SD
Subject group Oxycodone Norogxodone
(p = 0.161)” (p = 0.203)” Oqrnouphone (p = o.ols)t
Drug effect (p = O.Oll)$
Young men 178 ir 73.5 202.9 k 55.1 21.3 t: 6.0 18.0 +- 19.8 Elderly men 218 i- 105 199.7 t 84.7 14.3 rt 12.1 37.9 -t 39.7 Young women 250 + 61.9 227.6 +- 90.9 9.9 ir 11.4 110 t 81.7 Elderly women 297 i- 134 302.7 k 143 3.7 +- 9.70 109 Ifi 74
AUC, Area under the concentration-time curve (ng . hriml) or drug effect-time curve (mm . hr). *No significant difference between groups. tYoung men significantly greater than young or elderly women; elderly men significantly greater than elderly women. $Young and elderly women significantly greater than young or elderly men. BOxymorphone below measurable concentration (50.2 ngiml) in six of seven subjects.
phone plasma concentrations, with the strongest correlation (Y = -0.53) between oxycodone and pupil size. Correlations between oxycodone and pharmacodynamic variables were statistically signif- icant (p 5 0.05) for all variables except “need to talk,” which was also not significantly correlated with oxymorphone concentration. Perspiration was the only pharmacodynamic variable that was signif- icantly correlated with oxymorphone plasma con- centrations.
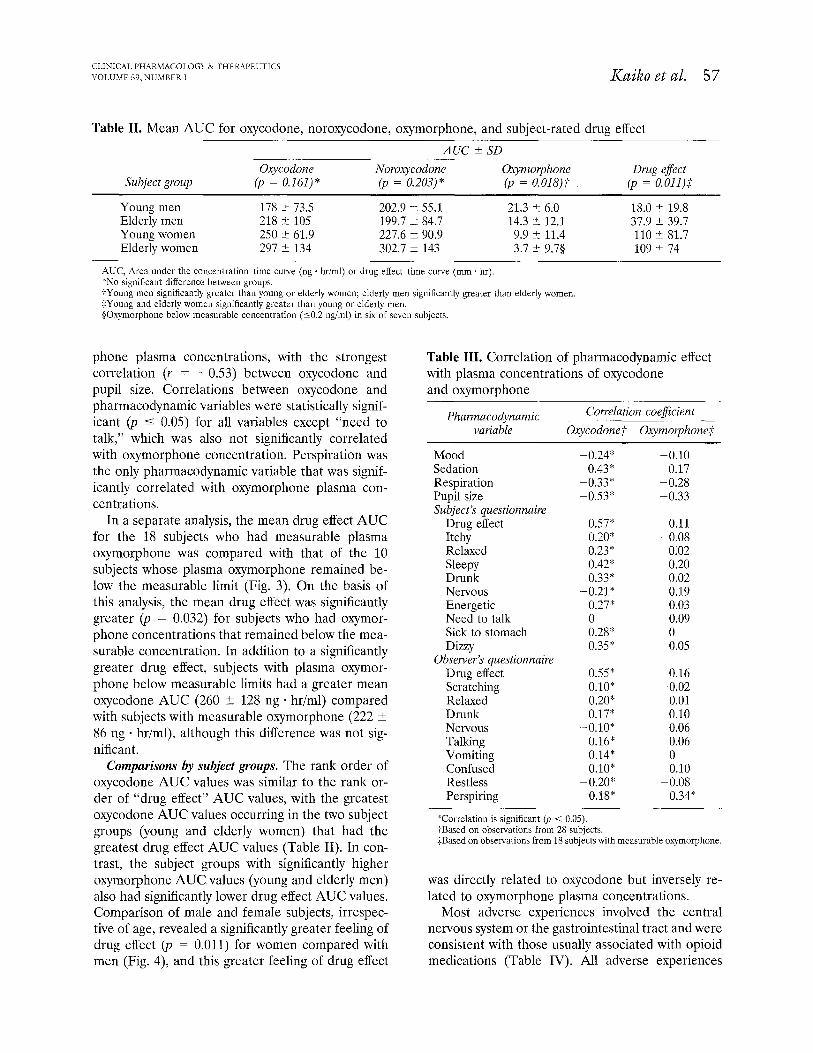
In a separate analysis, the mean drug effect AUC for the 18 subjects who had measurable plasma oxymorphone was compared with that of the 10 subjects whose plasma oxymorphone remained be- low the measurable limit (Fig. 3). On the basis of this analysis, the mean drug effect was significantly greater (p = 0.032) for subjects who had oxymor- phone concentrations that remained below the mea- surable concentration. In addition to a significantly greater drug effect, subjects with plasma oxymor- phone below measurable limits had a greater mean oxycodone AUC (260 t 128 ng ’ hriml) compared with subjects with measurable oxymorphone (222 ? 86 ng * hr/ml), although this difference was not sig- nificant.
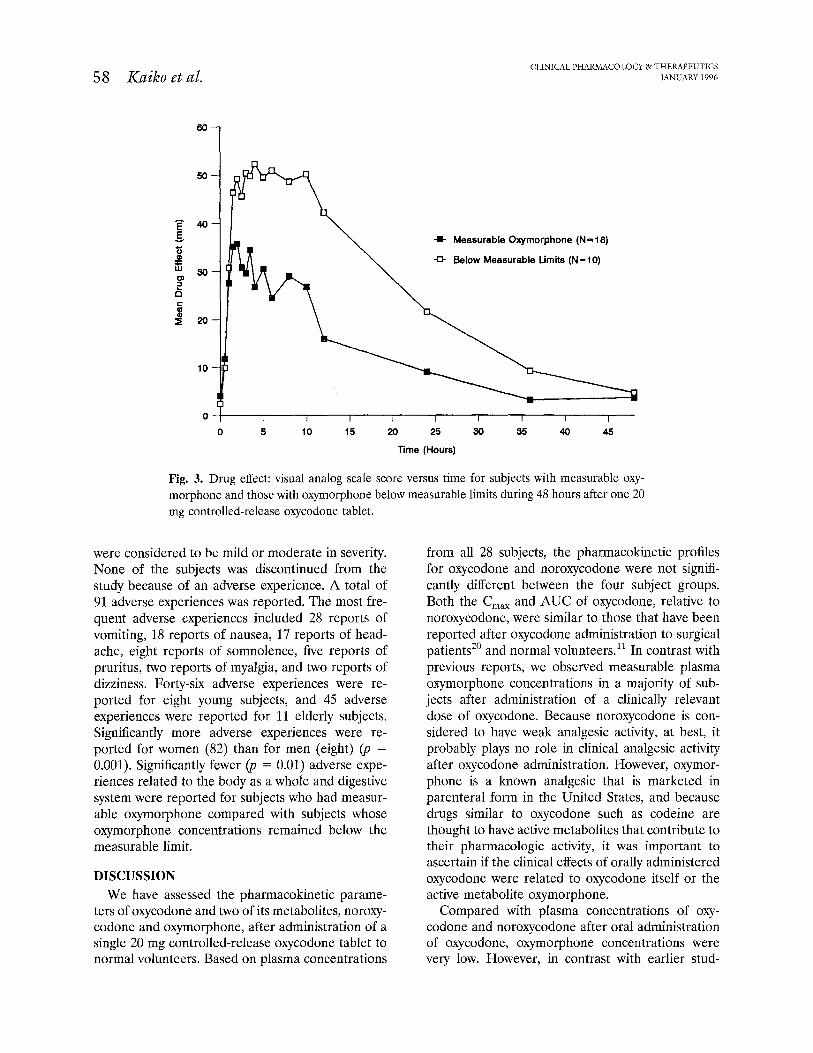
Comparisons by subject groups. The rank order of oxycodone AUC values was similar to the rank or- der of “drug effect” AUC values, with the greatest oxycodone AUC values occurring in the two subject groups (young and elderly women) that had the greatest drug effect AUC values (Table II). In con- trast, the subject groups with significantly higher oxymorphone AUC values (young and elderly men) also had significantly lower drug effect AUC values. Comparison of male and female subjects, irrespec- tive of age, revealed a significantly greater feeling of drug effect (p = 0.011) for women compared with men (Fig. 4) and this greater feeling of drug effect
Table III. Correlation of pharmacodynamic effect with plasma concentrations of oxycodone and oxymorphone
Pharmacodynamic variable
Cowelation coeficient
Oxycodonet 0xymolphone;t
Mood Sedation Respiration Pupil size Subject’s questionnaire
Drug effect Itchy Relaxed Sleepy Drunk Nervous Energetic Need to talk Sick to stomach Dizzy
Observer’s questionnaire Drug effect Scratching Relaxed Drunk Nervous Talking Vomiting Confused Restless Perspiring
-0.24” 0.43*
-0.33* -0.53”
0.57* 0.20* 0.23* 0.42” 0.33*
-0.21* 0.27* 0 0.28” 0.35*
0.55* 0.16 0.10* -0.02 0.20* 0.01 0.17* 0.10
-0.10* 0.06 0.16” 0.06 0.14” 0 0.10* 0.10
-0.20” -0.08 0.1s* 0.34*
-0.10 0.17
-0.28 -0.33
0.11 -0.08
0.02 0.20 0.02 0.19 0.03 0.09 0 0.05
*Correlation is significant (p < 0.05). tBased on observations from 28 subjects. $Based on observations from 18 subjects with measurable oxymorphone.
was directly related to oxycodone but inversely re- lated to oxymorphone plasma concentrations.
Most adverse experiences involved the central nervous system or the gastrointestinal tract and were consistent with those usually associated with opioid medications (Table IV). All adverse experiences
58 Ku&o et al. CLINICAL P HARMACOLOGY Pr THERAPEUTICS
JANUARY 1996
I I I I I I I I I 0 5 10 15 20 25 30 35 40 45
Time (Hours)
Fig. 3. Drug effect: visual analog scale score versus time for subjects with measurable oxy- morphone and those with oxymorphone below measurable limits during 48 hours after one 20 mg controlled-release oxycodone tablet.
were considered to be mild or moderate in severity. None of the subjects was discontinued from the study because of an adverse experience. A total of 91 adverse experiences was reported. The most fre- quent adverse experiences included 28 reports of vomiting, 18 reports of nausea, 17 reports of head- ache, eight reports of somnolence, five reports of pruritus, two reports of myalgia, and two reports of dizziness. Forty-six adverse experiences were re- ported for eight young subjects, and 45 adverse experiences were reported for 11 elderly subjects. Significantly more adverse experiences were re- ported for women (82) than for men (eight) (p = 0.001). Significantly fewer (p = 0.01) adverse expe- riences related to the body as a whole and digestive system were reported for subjects who had measur- able oxymorphone compared with subjects whose oxymorphone concentrations remained below the measurable limit.
DISCUSSION We have assessed the pharmacokinetic parame-
ters of oxycodone and two of its metabolites, noroxy- codone and oxymorphone, after administration of a single 20 mg controlled-release oxycodone tablet to normal volunteers. Based on plasma concentrations
from all 28 subjects, the pharmacokinetic profiles for oxycodone and noroxycodone were not signifi- cantly different between the four subject groups. Both the C,, and AUC of oxycodone, relative to noroxycodone, were similar to those that have been reported after oxycodone administration to surgical patients2’ and normal volunteers.‘i In contrast with previous reports, we observed measurable plasma oxymorphone concentrations in a majority of sub- jects after administration of a clinically relevant dose of oxycodone. Because noroxycodone is con- sidered to have weak analgesic activity, at best, it probably plays no role in clinical analgesic activity after oxycodone administration. However, oxymor- phone is a known analgesic that is marketed in parenteral form in the United States, and because drugs similar to oxycodone such as codeine are thought to have active metabolites that contribute to their pharmacologic activity, it was important to ascertain if the clinical effects of orally administered oxycodone were related to oxycodone itself or the active metabolite oxymorphone.
Compared with plasma concentrations of oxy- codone and noroxycodone after oral administration of oxycodone, oxymorphone concentrations were very low. However, in contrast with earlier stud-
CLINICAL PHWCOLOGY e; THEWEUTICS VOLUME 59, NUMBER 1 Km%0 et al. 59
*Elderly Female (N=7)
OYoung Female (N=7)
+ Elderly Male (N=7)
+Young Male (N=7)
0 5 10 15 20 25 30 35 40 45
Time (Hours)
Fig. 4. Drug effect: visual analog scale score versus postdose time by subject group during 48 hours after one 20 mg controlled-release oxycodone tablet.
Table IV. Adverse effects reported after one 20 mg controlled-release oxycodone tablet
Adverse effect
Measurable oxymorphonef
No. of No. of adverse events subjects
Oxymorphone below measurable limit
No. of No. of adverse events subjects
Body as a whole 7 5 12* 6 Digestive 13 5 35* 9 Muscular 1 1 2 1 Nervous 8 5 6 5 Skin 3 3 2 2 Special senses 0 0 2 2
TOTAL 32 9 59 10
*Significantly different (p < 0.05). tOxymorphone plasma concentration ~0.2 ngiml
ies 11,20 in which plasma oxymorphone remained be- low the assay detection limit in all subjects (CO.5 r&ml), only 10 of 28 subjects in this study had oxymorphone plasma concentrations that remained below the measurable limit (<0.2 rig/ml). Differ- ences between this and earlier studies in oxymor- phone plasma concentrations may be attributed to differences in the sensitivity of the oxymorphone assays, differences in the dosage and route of drug
administration, and age- and sex-related differences in oxycodone metabolism.
The two objective pharmacodynamic variables- pupil size and respiration-were significantly corre- lated with oxycodone but not oxymorphone, with the strongest correlation occurring between pupil size and oxycodone plasma concentration. However, it is interesting to note that respiratory rate did not change significantly during the study and that the

60 Kuiko et al. CLINICAL PHARMACOLOGY &THERAPEUTICS
JAMJARY 1996
mean change in respiratory rate was an increase relative to baseline. These results indicate that oxy- codone concentrations observed during the study were not high enough to alter respiration. Pupil size, on the other hand, decreased in a manner that was consistent with known opioid effects.
Among the subjective pharmacodynamic vari- ables, the strongest correlation was found between oxycodone plasma concentrations and the subjects’ assessment of drug effect. The magnitude of “drug effect” AUC was greatest for young and elderly female subjects, the subject groups that had the highest oxycodone and the lowest oxymorphone AUC. In addition, the rank order of the drug effect AUC values corresponded with the rank order of oxycodone AUC values and was opposite the rank order of the oxymorphone AUC values. The corre- lations of observer-rated drug effect with oxycodone and oxymorphone plasma concentrations were con- sistent with those based on subject ratings. Although a positive correlation between two variables does not in itself prove that changes in one variable are predictive of changes in the second variable, the rank orders for oxycodone and oxymorphone AUC values, compared with the rank order for drug effect (the most highly correlated pharmacodynamic vari- able), argue strongly for oxycodone and not for oxymorphone as the principal pharmacologically ac- tive agent after oxycodone administration.
Further evidence that suggests a negligible con- tribution of oxymorphone to pharmacologic effects after oral oxycodone administration can be found in the observation that the 10 subjects with no measur- able oxymorphone and higher mean oxycodone con- centrations had a significantly higher incidence and number of reports of typical opioid adverse experi- ences compared with the 18 subjects who had mea- surable oxymorphone and lower oxycodone plasma concentrations. Given that the number of adverse experiences can be expected to increase as plasma concentrations of an active opioid are increased, these results suggest that plasma concentrations of oxymorphone were either not high enough to pro- duce detectable concentration-dependent increases in adverse experiences or that any such increases were masked by the effects of oxycodone. This ex- planation is consistent with the pharmacodynamic analyses that indicated oxycodone was primarily re- sponsible for changes in pharmacodynamic variables observed during this study.
The results of pharmacokinetic-pharmacodynamic analyses in this study are consistent with results ob-
tained with use of animal models” in that both sup- port oxycodone as a pharmacologically active opioid and neither supports the contention that oxycodone requires conversion to oxymorphone for pharmaco- logic activity after oxycodone administration. In the present study, the low plasma oxymorphone concen- trations compared with oxycodone, the statistically significant and stronger correlations of pharma- codynamic variables with oxycodone compared with oxymorphone, and the lack of a detectable concentration-effect relationship between oxy- morphone and the incidence of typical opioid ad- verse experiences all support oxycodone itself as the principal active agent. Additional support for the activity of oxycodone can be found in a comparison of the pharmacokinetic and pharmacodynamic as- sessments of the four subject groups, with agree- ment in the rank orders of oxycodone AUC values and drug effect AUC values compared with the lack of correspondence between the rank orders of AUC values for oxymorphone and drug effect.
In summary, pharmacokinetic-pharmacodynamic correlations indicate that oxycodone, not oxymor- phone? is the principal pharmacologically active agent after oral oxycodone administration. The pharmacokinetics of oxycodone and its relatively inactive N-demethylated metabolite noroxycodone were not significantly different between young men, young women, elderly men, and elderly women. Dif- ferences between the four subject groups in the pharmacokinetic profile of oxymorphone suggest differential metabolism of oxycodone to oxymor- phone based on gender and perhaps age. However, the apparent differences in oxycodone metabolism are likely to be of little clinical significance because plasma concentrations of oxymorphone remained very low, if measurable at all, after oxycodone ad- ministration, and pharmacodynamic effects were sig- nificantly correlated with oxycodone, not oxymor- phone. As with other drugs of this class, oxycodone therapy should be individualized. Therapy with oxy- codone should begin with a conservative initial dose based on the patient’s previous opioid exposure, disease state, and medical status and be followed with titration to analgesic effect.
References 1. Falk E. Eukodal, ein neues narkotikum. Muenchener
Med Wochenschr 1917;64:381-4. 2. Falk E. Eukodal, ein neue narkotikum. Ther Monatsh
1919;33:180-6. 3. Kalso E, P6yhiS R, Onnela P, et al. Intravenous mor-

CLINICALPHARMACOLOGY&THER‘U'EUTICS VOLUME59,NUMBERl I(aitk0 et al. 61
phine and oxycodone for pain after abdominal sur- gery. Acta Anaesthesiol Stand 1991;35:642-6.
4. Glare PA, Walsh TD. Dose-ranging study of oxy- codone for chronic pain in advanced cancer. J Clin Oncol 1993;11:973-8.
5. Kalso E, Vainio A. Morphine and oxycodone hydro- chloride in the management of cancer pain. CLIN PHARMACOL THER 1990;47:639-46.
6. Pappagallo M, Raja SN, Haythornwaite JA, Clark M, Campbell JA. Oral opioids in the management of post-herpetic neuralgia: a prospective survey. Analge- sia 1994;1:51-5.
7. Cone EJ, Darwin WD, Buchwald WF, et al. Compar- ative metabolism and excretion of oxycodone in man and laboratory animals [Abstract]. Fed Proc 1984;43: 655.
8. Ishida T, Oguri K, Yoshimura H. Isolation and iden- tification of urinary metabolites of oxycodone in rab- bits. Drug Metab Dispos 1979;7:162-5.
9. Ishida T, Oguri K, Yoshimura H. A novel metabolite of oxycodone in the urine of rabbits. J Pharm Dyn 1982;5:134-6.
10. Ishida T, Oguri K, Yoshimura H. Determination of oxycodone metabolites in urines and feces of several mammalian species. J Pharm Dyn 1982;5:521-5.
11. Poyhia R, Seppala T, Olkkola KT, et al. The pharma- cokinetics and metabolism of oxycodone after intra- muscular and oral administration to healthy subjects. Br J Clin Pharmacol 1992;33:617-21.
12. Baselt RC, Stewart CB. Determination of oxycodone and a major metabolite in urine by electron-capture GLC. Drug Intel1 Clin Pharm 1978;2:107-9.
13. Weinstein SH, Gaylord JC. Determination of oxy- codone in plasma and identification of a major me- tabolite. J Pharm Sci 1979;68:527-8.
14. Beaver WT, Wallenstein SL, Rogers A, Houde RW. Analgesic studies of codeine and oxycodone in pa- tients with cancer; II: comparison of intramuscular oxycodone with intramuscular morphine and codeine. J Pharmacol Exp Ther 1978;207:101-8.
15. Leow IQ, Smith MT. The antinociceptive potencies of oxycodone, noroxycodone, and morphine after in- tracerebroventricular administration to rats. Life Sci 1994;54:1229-36.
16. Lasagna L, Kornfeld TJ. Analgesic potency of nor- morphine in patients with postoperative pain. J Phar- macol Exp Ther 1958;124:260-3.
17. Chen ZR, Irvine RJ, Somogyi AA, Bochner F. Mu receptor binding of some commonly used opioids and their metabolites. Life Sci 1991;48:2165-71.
18. Otton SV, Wu D, Joffe RT, Cheung SW, Sellers EM. Inhibition by fluoxetine of cytochrome P450 2D6 ac- tivity. CLIN PHARMACOL THER 1993;53:401-9.
19. Clear-y J, Mikus G, Somogyi A, Bochner F. The influ- ence of pharmacogenetics on opioid analgesia with codeine and oxycodone in Sprague-Dawleyidark Ag- outi rat model. J Pharmacol Exp Ther 1994;271:1528- 34.
20. Poyhia R, Olkkola KT, Seppala T, Kalso E. The phar- macokinetics of oxycodone after intravenous injection in adults. Br J Clin Pharmacol 1991;32:516-8.
21. Preston Kl, Jasinski DR, Testa M. Abuse potential and pharmacological comparison of tramadol and morphine. Drug Alcohol Depend 1991;27:7-17.





























