Embed Size (px)
Citation preview

100.0
g lo.o|
g
Pharmacokinetic and pharmacodynamic principles
T H O M A S K. H E N T H O R N M I C H A E L J. A V R A M
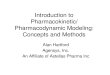
Mathematical characterization of the multiexponential plasma (or blood) drug concentrat ion versus t ime relationship during and after administering a dose (Figure 1) allows description of what the body does to the drug, which is referred to as pharmacokinetics. Pharmacokinet ic variables commonly repor ted are total apparent volume of distribution, total elimination clearance, and elimination half-life.
2
0 120 240 360 480 600 720
Time (min)
Figure 1. Blood thiopentone concentration versus time relationship following rapid intra- venous administration of the drug, illustrating the rapid decline in drug concentration during the early, distributional phases and the much slower decline during the terminal, elimination phases. From Fragen and Avram (3990), with permission, based on data from Henthorn et al (1989a).
The total apparent volume of distribution is an independent variable which relates the amount of drug in the body to the plasma or blood drug concentration:
Volume = Amoun t of drug/Drug concentration
Bailli#re' s Clinical Anaesthesiology-- 489 Vol. 5, No. 3, December 1991 Copyright �9 1991, by BaillEre Tindall ISBN 0-7020--1526-1 All rights of reproduction in any form reserved

490 "r. K . H E N T H O R N A N D M. J . A V R A M
A frequently reported total volume of distribution is the volume of distri- bution at steady state, Va~, the total apparent volume a drug would have if it were in equilibrium with all tissues. Another reported, usually larger, total volume of distribution is Va~ or VaAuC, which, together with elimination clearance, determines the elimination half-life.
The total elimination clearance, ClE, is the independent variable which relates the rate of irreversible drug removal from the body to the plasma or blood drug concentration:
Elimination clearance = Rate of elimination/Drug concentration
The total elimination clearance is the sum of the elimination clearances of all organs, principally the liver and the kidneys.
The elimination half-life, tl/2~, is the time required for the amount of drug in the body to decrease by one half. It is a dependent variable:
t1/2f3 = loge(2)" Vd[3/ CIE -= 0.693 Vd~/ CIE
While these pharmacokinetic variables can be useful for drugs with a rapid onset of effect, such as the intravenously administered anaesthetic agents (see below), they do not provide a complete description of the pharmaco- kinetics of these drugs. The total volume of distribution is not realized until after extensive drug distribution and redistribution have occurred (Figure 1); for this reason, predicted early drug concentrations on the basis of dose and total volume of distribution will be extremely low. Although elimination clearance begins when drug first reaches the clearing organs, the relatively slow decline in drug concentrations due to elimination clearance becomes a significant determinant of the plasma (or blood) drug concentration versus time relationship only after the rapid decline in drug concentrations characterizing the distribution and redistribution phases is over (Figure 1). Because the effect of a standard dose of an intravenously administered drug terminates during distribution or redistribution, the elimination half-life provides no information on the time to termination of drug effect. Thus, knowledge of the early pharmacokinetics of intravenously administered anaesthetics is essential to understanding the kinetic basis of the time course of drug effect intensity.
After rapid intravenous administration, a drug mixes quickly within the central blood pool. From there it is distributed by blood flow and molecular diffusion throughout the various tissues of the body, according to their rate of perfusion, their affinity for the drug, and the relative concentration of the drug in the blood and the tissues (Figure 2). This is called distribution clearance, and it is an independent variable which relates the rate of drug movement between tissues to tissue drug concentrations (Avram et al, 1986):
Distribution clearance = Rate of transfer/Drug concentration
Highly perfused, small volume tissues with a high affinity for lipophilic drugs (including the brain and the viscera) equilibrate very rapidly with the high, but briskly falling, early arterial blood drug concentrations, leading to the onset of effect of drugs acting on these tissues. Blood drug concentrations

PHARMACOKINETICS AND PHARMACODYNAMICS 491
1 ! %%% ~ Lean
Viscera / ~. , ; X /
/ \ / \ . , / " j J
20
1 1 1 1 1 2 4 8 16 32 128 ,~ 16 8 4 2
Time (min) Figure 2. Percentage of a dose of intravenously administered thiopentone in the central blood pool, viscera, lean tissue and fat after rapid intravenous administration and in the absence of elimination clearance. From Price et al (1960), with permission.
and the concentrations in the tissues with high blood flow rates then decrease less rapidly as the drug redistributes to the large reservoir of less well- perfused and lower-affinity lean tissues, such as muscle, terminating their effect on highly perfused tissues. The poorly perfused adipose tissue takes up drug very slowly despite its high affinity for lipophilic drugs; the amount of drug distribution to adipose tissue is not significant until long after the effects of a single-dose wane.
Arterial-venous drug concentration differences
Studies that attempt to establish the pharmacokinetic basis for differences in patient reactivity to various drugs used in the practice of anaesthesia have generally been based on venous blood drug concentrations and have, until recently, ignored the processes affecting early drug distribution. The commonly held assumption that blood drug concentrations are uniform throughout the vascular system in the minutes to hours after rapid intra- venous drug administration is incorrect (Chiou, 1989). For example, arterial to venous concentration differences have been reported for thiopentone (Figure 3) (Barratt et al, 1984; Stanski et al, 1984). During the distribution phases, arterial blood drug concentrations exceed venous blood drug concentrations, while the opposite may be true during the elimination phase. Venous blood drug concentrations reflect the drug concentrations in tissues draining into the venous system being sampled, while arterial blood drug concentrations reflect drug concentrations being delivered to tissues

492 T. K. H E N T H O R N A N D M. J. AVRAM
c- O
C 03
0
50
40
30
20
10
0 0
t ~_. i~!iE!~ ra" �9 ..... Jugular
_ir I I ~ I ~ I m I n I �9 �9 I
2 4 6 8 10 12 Time (min)
Figure 3. Mean (from eight patients) plasma thiopentone concentration versus time relation- ship for samples obtained from arterial, peripheral venous, central venous and jugular venous sampling sites, illustrating the lack of intravascular mixing of thiopentone in the minutes after its rapid intravenous administration. From Barratt et al (1984), with permission.
for distribution, to clearing organs for elimination, and to effector organs. Thus, pharmacokinetic studies should be based on arterial blood drug concentrations whenever possible, especially if the drug is being admini- stered acutely and has a rapid onset of effect.
Pulmonary drug uptake
First-pass pulmonary uptake of an intravenously administered drug may attenuate its peak plasma concentration, diminishing its central nervous system effects if it has a rapid onset of effect, and increasing its initial volume of distribution. On the other hand, anything that interferes with the first- pass pulmonary uptake of such a drug will produce higher initial drug concentrations, resulting in a more profound effect, and a decreased central volume.
Drugs that are lipophilic basic amines have significant first-pass pulmonary uptake, possibly because they have a higher affinity for lipophilic lung tissue than for the a~-acid glycoprotein to which they are bound in plasma. Lipophilic neutral amines and acidic drugs may have little pulmonary uptake because they have higher affinities for the plasma albumin to which they are bound than they have for the lung tissue. Consistent with their hypotheses are the observations of Roerig et al (1989b) that the basic amine verapamil had a 48 % first-pass pulmonary uptake, while that of the non-basic amine diazepam

PHARMACOKINETICS AND PHARMACODYNAMICS 493
was 30%, and the acidic drug thiopentone had a 14% first-pass pulmonary uptake. These same investigators (Roerig et al, 1989a) also found that the 83% first-pass pulmonary uptake of the lipophilic basic amine fentanyl was reduced by approximately one third in subjects treated chronically with propranolol, a drug with similar physicochemical properties (Figure 4).
O o
O o
z IJJ u .
(.9 O "5 C
. O
I J-
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0 ' ' 10
o ICG 1.0 _~" 1.8 . . �9 Fentanyl ~ 'ER = 1.6
~o 1.4 O.8
~ 1.2
o 0 0.4-}. .8 =o ~
0.2 v ~ 0.4
o ~. 0.2
0 0 20 30 40 50 60
o I C G �9 ny l
10 20 30 40 50
Time (s) Time (s)
1.0
0.8 m
o 0.6 g-
0.4~ m
0.2
0 60
Figure 4. Fraction of the dose of a non-extracted indicator (indocyanine green, ICG) and fentanyl (FEN) per millilitre of arterial blood versus time relationship after rapid intravenous administration to a patient taking no propranolol (left panel) and to a patient taking 120 mg propranolol per day for a month (right panel), illustrating the decreased first-pass pulmonary uptake of fentanyl by propranolol. From Roerig et al (1989a), with permission.
Early drug distribution
There have been two recent attempts to develop a pharmacokinetic description of the processes involved in the distribution of intravenously administered anaesthetic agents during the time they are exerting their maximum effect.
Stanski and Maitre (1990) described the disposition of thiopentone using arterial blood concentration data collected at 0.5-1.0-rain intervals during a 3-12-rain infusion of the drug at 75-100 mg/min. They collapsed a multi- compartment model to a simple one-compartment model, the volume of which was approximately that of the central volume of a three-compartment model. Drug is removed from the single compartment by both distribution and elimination clearances, but all such processes are treated as though they are elimination clearance, i.e. distribution is treated as a one-way process despite the fact that distribution clearance is bidirectional.
A multicompartmental model of thiopentone disposition that appears to

494 T. K. HENTHORN AND M . J . AVRAM
reflect physiological factors affecting early drug distribution has been developed by Henthorn and colleagues (1989a) (Figure 5). They simul- taneously modelled the disposition of concomitantly administered thio- pentone and indocyanine green, a marker of intravascular space, on the basis
I CG TP
Figure 5. The compartmental pharmacokinetic model used to describe the simultaneous disposition of thiopentone (TP; solid lines) and indocyanine green (ICG; dashed lines), including late intravascular mixing. From Henthorn et al (1989a), with permission.
of frequent arterial blood samples (Figure 6). This allowed them to characterize central and peripheral blood pools, and to describe thiopentone distribution by mixing within the blood pools and by cardiac output to the other tissues of the body.
Both Stanski and Maitre (1990) and Avram et al (1990) have used their models to study the possible pharmacokinetic basis of the decreased thiopentone dose requirement in the elderly (Christensen and Andreasen, 1978; Dundee et al, 1982; Homer and Stanski, 1985). Neither study was able to reproduce the observation of a decreased central volume with increasing age reported by Homer and Stanski (1985) as the pharmacokinetic basis of the altered dose requirement. Despite using different approaches to the study of early drug distribution, both groups found the clearance of thiopentone from its initial distribution volume decreases with advancing age. Stanski and Maitre (1990) concluded that the reduced clearance in the elderly accounts for the reduced dose requirements. However, Avram et al (1990) suggested that, while it is appealing to make dosing adjustments in the elderly on the basis of this pharmacokinetic change, it does not provide sufficient rationale for suggesting that the thiopentone induction dose

PHARMACOKINETICS AND PHARMACODYNAMICS 495
E
c " O
o C : 0 o
0 0
50.0
10.0
5.0
t.0
0.5 o
B 50.0
1.0
.% .80 720
i I I I i I I J
4 8 12 16 Time (min)
Figure 6. Blood thiopentone concentration (A) and indocyanine green concentration (�9 versus time relationship illustrating an additional (fourth) exponential phase revealed by the frequent early arterial blood sampling and corresponding to the period of late intravascular mixing in the moments after rapid intravenous administration of the drug. From Avram et al (1990), with permission.
should be based on age alone. This is consistent with the results of a later study of patient characteristics associated with thiopentone induction dose requirements, in which Sanghvi et al (1991) found that age, cardiac output and lean body mass are co-determinants of dose requirements.
PHARMACOKINETIC-PHARMACODYNAMIC MODELS
Responses to a dose of drug can vary widely among patients. Such variability may result from differences in what the drug does to the patient (pharmaco- dynamics) or in what the body does with the drug (pharmacokinetics). It is important to determine the relative importance of variability in both drug disposition and effect in order to understand variations in dose-response relationships. Because interindividual differences in the dose-response relation- ship can be due to either pharmacokinetic or pharmacodynamic factors, a study that examines both of these factors by simultaneously measuring drug concentrations and drug effect and analyses these data with a combined approach is the most efficient.
Pharmacokinetics are best studied in circumstances that maximize the changes in concentration over time (i.e. following rapid intravenous admini- stration), whereas pharmacodynamics are best studied by correlating steady-state concentrations (i.e. during continuous intravenous infusion) with measured effect. As these study designs are mutually exclusive, pharmacokinetics and pharmacodynamics have been studied in separate investigations in the past.

496 T . K . H E N T H O R N A N D M. J. AVRAM
Up to 3.3 elimination half-lives must elapse before plasma concentrations reach even 90% of their eventual steady-state level when administered by a constant infusion. Sufficient steady-state concentration--effect data are difficult to obtain because such time requirements often preclude studying more than a single plasma concentration in a typical surgical patient. Physiological changes that routinely occur during clinical anaesthesia compound the problem of obtaining reliable steady-state data.
In an effort to solve these problems, two major advances in clinical pharmacokinetics have been made which allow for meaningful analysis of concentration-response data in non-steady-state conditions (e.g. following a rapid intravenous injection or during short infusions). One improvement is the development of combined pharmacokinetic-pharmacodynamic models with a separate 'effect compartment' designed to define drug concentration- response relations kinetically. These investigations are best done following a rapid intravenous injection, as a well-grounded mathematical description of drug disposition facilitates this sort of analysis. The other advance is the introduction of computer-controlled infusion pumps which continuously adjust the drug infusion rate to compensate for tissue distribution (see discussion of the Kriiger-Theimer infusion method below). This allows a desired plasma concentration to be attained immediately and held constant. By waiting a short time for effect site concentrations to equilibrate with the plasma, an effect measurement can be made.
Pharmacokinetic-pharmacodynamic models are based upon the classical dose-response relationship. Data obtained in dose-response studies are classified as quantal or graded depending on the nature of the effect measured. Quantal (all-or-none) responses describe the presence or absence of a drug-induced state, such as sleep or analgesia. The variable frequency of a positive all-or-none response to doses of a given drug may be normally distributed or skewed. By plotting the logarithm of dose against the number of subjects responding, a skewed distribution becomes log- normal. This normal or log-normal distribution, if plotted as cumulative response (i.e. percentage responding to a given dose), has the classic sigmoid shape. The median effective dose (EDs0) provides information on the position of the curve along the dose axis, but provides none about the shape of the curve. In anaesthesia, minimum alveolar concentration (MAC) is the most familiar example of an EDs0 of such a quantal, dose-response relationship.
Graded responses to a drug (e.g. percentage paralysis resulting from a neuromuscular blocker) are manifest on a continuous scale from no effect to maximum effect. Graded response is considered to be a function of receptor occupancy. Plotting effect as a function of log-dose yields a classical sigmoid curve that is linear from 20% to 80% of maximum effect.
Quantal and graded dose-response relationships may be expressed mathematically by the equation:
D r E - (1)
D r + D(50) ~
where E is the intensity of pharmacological effect (or cumulative percentage

PHARMACOKINETICS AND PHARMACODYNAMICS 497
of quantal response), D is the dose related to that effect, D(50) is a constant giving the dose producing a 50% effect, and ~ is a parameter defining sigmoidicity. When graded responses are considered, a variation of equation (1) is used:
E,~ax" D r E - (2)
D'~ + D(50) "v
where gmax is the maximum effect. The measured effect should optimally be a direct measure of the pharmacological effect of the drug being studied, and the observed maximum effect must be the maximal possible one. In experi- ments in which the dose or concentration is varied over such a small range that the observed effects fall only within the linear range (i.e. between 20% and 80% of the maximum effect), insufficient data are present to determine the variables in equation (2). In this case, a linear or proportional model may �9 be more appropriate.
Clinical anaesthesia is replete with conditions that can be characterized as being non-steady state, making it necessary to understand the temporal relation or time lag between plasma concentrations and pharmacological effect. Pharmacokinetic analysis of blood or plasma drug concentration history defines several phases or compartments. Drug concentrations in the peripheral compartments lag behind and are driven by drug concentrations in the plasma.
Levy (1966) first proposed that drug concentrations in one of the peripheral compartments might have the same temporal course as that of the observed effect. Usually, when concentration is plotted as the independent variable against effect, clockwise or counter-clockwise hysteresis is encountered. In the case of counter-clockwise hysteresis, concentrations rise before effects are observed and concentrations fall before the effect dissipates. This is the usual pattern seen for the plasma compartment.
Exactly the opposite relationships are observed in deep tissue compartments in which clockwise hysteresis is seen. If no or minimal hysteresis is seen, the pharmacokinetic compartment and the effect compartment share the same time course and, perhaps, the same tissue site. However, since with most drugs the actual mass of drug-specific tissue for a given effect is quite small compared with the vast quantity of tissues that are non-specific, the contribution of the effector site to the total disposition of systemically administered drug is very small. Thus, if a strong temporal correlation exists between the pharmacological effect and concentration in a kinetic compartment, it is probably serendipitous.
An alternative approach proposed by Segre (1968) and adopted by Sheiner et al (1979) is shown schematically in Figure 7. This models effect as a function of the drug concentration in a biophase compartment. The pharmacokinetics of the biophase are related to the central compartment by a first-order process (i.e. the drug reaches the biophase along a single concentration gradient). This effect compartment is assumed not to alter the pharmacokinetic properties of the drug, and is linked to the measured effect by equation (2), with biophase concentrations substituted for dose. The plasma concentra-

498 T. K. HENTHORN AND M . J . AVRAM
kl e I
kl2
k2]
keo
1.0
E
0 Ae
Figure 7. Multicompartmental system used to model the distribution and elimination of a drug (o-tubocurarine) and its effects (twitch-height suppression). D-tubocurarine injected into the central compartment distributes to one (in this example) or more tissue compartments, as determined by the transfer rate constants, while also being cleared from the body. The square marked 'effect' represents the biophase of D-tubocurarine effect. The rate constants kt0 and k~o determine the rate of onset and offset of the effect. The sigmoidal plasma concentration-effect relation (at steady state) can be calculated from these variables and equation (1). From Stanski et al (1979), with permission.
tions and the observed effects can thus be tracked separately, as demon- strated in Figure 8.
This approach allows calculation of steady-state plasma concentration- response relations in an individual for multiple points following a single dose, plus estimation of the Cpss(50) (the concentration at steady state that would produce 50% of the maximum effect). The rate constant of the effect compartment, often expressed as k~o, characterizes the time course of drug equilibration with the site of action.
An additional consideration when using the combined pharmacokinetic- pharmacodynamic model following a single dose is the ability to measure the effect in a short time relative to changes in plasma drug concentration. For example, determining the slope of a PaCO2 versus minute ventilation curve would be inappropriate when plasma drug levels are changing rapidly, but measuring twitch suppression following a bolus of pancuronium would be ideal.
Data analysis for the combined pharmacokinetic-pharmacodynamic model has followed this general scheme: first, pharmacokinetic data are fit to an appropriate exponential decay curve which can be expressed in terms of a compartmental model. These terms are fixed and serve as an input function for the effect model, A biophase compartment is added to the

PHARMACOKINETICS AND PHARMACODYNAMICS 499
c 1.0 .0_
E I1) o 0.8 8 E
~_ 0.6
O
~6 0.4
.o_
0 . 2 "5 II) ~=
UJ
D-tubocurarine infusion rate (;ag kg ~ min ~)
_ 1 6 . 8 _1_ 1 . 2 . j - ] - i
o - o ~ Q = Plasma concentration
\ o = Effect (paralysis)
" o
l / - . . ._ . . oo
o
! ~ u l . . . . i . . . . 1 . . . . a l ' k l I L [ ! I i I I I I I
) 10 2030405060 80 100 120 140 160 180 200 220
Time (min)
Figure 8. Kinetic analysis of plasma D-tubocurarine concentrations (0 ) and twitch-height suppression (�9 in a patient, The solid lines are least-squares fits of the observed values indicated by the data-points. From Stanski et al (1979), with permission.
model with first-order rate constants which can adjust during least-squares, non-linear regression analysis. This is used to derive effect site concentra- tions that optimally remove hysteresis between these drug concentrations and the observed effects. The biophase can then be linked to an appropriate effect model, e.g. the Hill equation (equation 2).
Remarkable progress has been made in recent years in characterizing the time course of drug effect and directly relating this to the drug's plasma pharmacokinetics. Sheiner (1989) has suggested that such combined pharmacokinetic-pharmacodynamic studies can often lead to mechanistic insights. Stanski et al (1979) have used combined pharmacokinetic- pharmacodynamic models to demonstrate that a pharmacodynamic, rather than a pharmacokinetic, interaction increases sensitivity to D-tubocurare under halothane anaesthesia. Fisher et al (1982), using similar models, have shown that dosing adjustments for single injections of D-tubocurare are unnecessary in infants because of offsetting differences in distribution volume and Cpss(50) when compared with older children and adults. Homer and Stanski (1985) and Arden et al (1986) have used the combined technique to study the increased reactivity of the elderly to thiopentone and etomidate, respectively. They concluded that the elderly are more sensitive to these drugs because of age-related kinetic, rather than dynamic, changes.
Additionally, advances may be expected in the area of pharmaco- dynamics. Btihrer et al (1987) have utilized improved electroencephalo- graphic (EEG) techniques to delineate more accurately the cerebral effects

500 T. K. HENTHORN AND M. J. AVRAM
of thiopentone including the biphasic response. It is anticipated that with improvements in both pharmacokinetic study design/analysis and measure- ment of cerebral effect, a clearer image will emerge of the important factors determining interdrug and interindividual differences in the response to anaesthetic drugs.
Simulations performed with combined pharmacokinetic-pharmacodynamic models have been used by Sharer and Varvel (1991) to examine differences in anaesthesia recovery times. Continuous, computer-controlled infusions of variable duration were used to compare fentanyl, alfentanil and sufentanil. The authors were able to use these models to explain the clinical observation that alfentanil appears to have a very rapid onset and offset when given as a single bolus dose but has a longer duration of effect after short infusions lasting only 15 min. Additionally, they elegantly demon- strated the reasons for the poor correlation between the (often-cited) pharmacokinetic parameters of distribution and elimination half-lives and duration of effect after terminating continuous infusions of variable length.
Their analysis led to the conclusion that for infusions of up to 6 hours' duration, patients given sufentanil would recover faster than patients given alfentanil, despite the fact that alfentanil has an elimination half-life of less than half that of sufentanil. Shafer and Varvel's paper is important because it demonstrates the need to consider the full complexities of the multi- compartmental pharmacokinetics of lipid-soluble, centrally acting drugs linked to a kinetic biophase in order to use these drugs rationally in the clinical anaesthesia setting. At the same time, it lucidly explains how to interpret the results of pharmacokinetic analyses and how these analyses should be applied to answer clinical questions.
The crux of pharmacodynamics is, of course, measurement of drug effect. Perhaps the most difficult challenge facing investigators studying CNS drug effect is finding an objective quantifiable pharmacodynamic measure. Green- blatt et al (1989) used a combined pharmacokinetic-pharmacodynamic study design, originally with thiopentone. The effects of midazolam and diazepam were studied using processed EEG as a measure of CNS drug effect.
They found that [~ frequency (13-30 Hz) power increased with increasing plasma levels of both benzodiazepines, provided the subject remained conscious. B-frequency power was maximal at the end of infusion for diazepam but was not maximal until 5-10 min later for midazolam. Despite the obvious disparity in the kinetics of effect, all data were fit to a v e n o u s
concentration-versus-effect model, with no effect compartment (biophase) or other attempt made to remove the bias introduced by the hysteresis.
Bfihrer et al (1991a) have also recently examined the effects of these benzodiazepines using processed EEG. However, they argued that the usual methods of processing the EEG, based on Fourier transformation, assume the waveforms have an underlying sine wave-like periodicity. They utilized an aperiodic analysis that breaks the complex waveforms into sequential trough-peak-trough units or waves, and calculates their number and the sum of their amplitudes per unit time ('voltage'). With this method, they not only avoided making assumptions concerning the nature of CNS signals, but also improved the ability to discern changes in CNS effects.

PHARMACOKINETICS AND PHARMACODYNAMICS 501
Biihrer et al (1991b) went on to use aperiodic processing of EEG to examine the differences between diazepam and midazolam using a combined pharmacokinetic-pharmacodynamic model with arter ia l drug concentrations. Despite study design differences in plasma drug sampling site, methods of measuring CNS effect and kinetic modelling techniques, both Greenblatt et al (1989) and Btihrer et al, (1991b) found similar potency ratios comparing diazepam and midazolam ECs0s (7.7 and 6.3, respectively) and a greater delay between plasma concentration and measured EEG effect (hysteresis) for midazolam.
These observed differences in hysteresis between midazolam and diazepam may explain some of the difficulty that has been experienced in safely achieving conscious sedation with midazolam. Those who routinely administered intravenous diazepam became accustomed to observing its peak sedative effect almost immediately. Because the effect of midazolam lags further behind plasma concentrations than that of diazepam, inter- vening midazolam doses titrated on a diazepam schedule (every minute or so) would result in a phenomenon called 'dose-stacking', in which the cumulative effect of a cluster (or stack) of doses is not observed until some time after administration of the final dose.
However, there are important differences in the results reported in these two studies. Biihrer et al (1991b) predicted effective steady-state plasma drug concentrations four times higher than those estimated by Greenblatt et al. The former are much more in line with those reported by Persson et al (1988) and Fragen and Avram (1989) to be required clinically. These differences may be explained on the basis that EEG parameters selected in these two studies were measuring different effects. Also the characteristic benzodiazepine EEG effect (the increased [3 activity) in the study by Greenblatt et al (1989) was lost with loss of consciousness. No such limitation was seen by Biihrer et al (1991b).
The differences between these studies reveal some of the difficulties of 'measuring' CNS effect. EEG effects may not measure or even be related to the clinical drug effects of interest. EEG measures cortical activity; most responses during anaesthesia are actuated subcortically. EEG changes may be secondary to the fundamental pharmacological effect and thus may not be related linearly or temporally. Despite these difficulties, there appears to be sufficient evidence to say that EEG measures are appropriate for making comparisons among similar CNS active drugs (e.g. among opiates or benzodiazepines), or for determining the basis of interindividual differences in dose-response with a particular drug.
Logistic plasma concentration v e r s u s response relationships have been used to examine data obtained from adjustable continuous infusions of alfentanil. Ausems et al (1986) were able to determine the Cp(50) (plasma concentration at which there is a 50:50 likelihood of clinical response to painful stimulus) for various surgical stimuli. Lemmens et al (1989) used this technique to examine whether there is a pharmacodynamic difference between similar surgical patients who differ only in their alcohol con- sumption. Two groups of healthy adult female patients (one group con- sumed 20-40g alcohol per day) were studied to determine alfentanil

502 T. K. H E N T H O R N A N D M. J. AVRAM
plasma concentration requirements for analgesia during breast cancer surgery. The study also compared alfentanil levels when spontaneous ventilation resumed. All members of the alcohol-consuming group had a higher Cpss(50), as determined by a probabilistic model of no response, than the abstaining group; on average, the Cpss(50) was more than double, 522 + 104 versus 208 + 26 ng/ml. The mean alfentanil plasma concentration at resumption of spontaneous ventilation was more than twice as high, 372 + 114 versus 176 + 39, in the alcohol-consuming group.
DRUG INFUSIONS
A continuous drug infusion at a constant rate, I, for a sufficient duration will achieve a steady-state plasma or blood drug concentration, Css, that is a function of both the infusion rate and the elimination clearance of the drug:
Css = I/CIE
That is, steady state is achieved when there is no net drug distribution and the rate of drug administration is equal to its rate of removal from the body. Until steady state is achieved, the drug is not only being cleared from the body but is also being distributed throughout it, in effect diluting the drug and producing plasma drug concentrations lower than those achieved at steady state. A continuous, constant rate infusion will take more than three half-lives of the drug being infused to achieve 90% of the eventual steady- state concentration. For the anaesthetist, who needs to achieve effective concentrations rapidly, this approach to drug infusions is unsuitable.
The easiest way to both achieve effective plasma or blood drug concentra- tions rapidly, and to maintain them continually throughout the period of drug distribution and after, is to use the combined bolus and infusion method of Mitenko and Ogilvie (1972). This drug-infusion technique uses a loading dose, or bolus, which would provide effective plasma or blood drug concentrations if the drug instantaneously equilibrated throughout its entire volume of distribution:
Loading dose = Css" VD~
The loading dose is administered simultaneously with the commencement of a maintenance infusion, the rate of which is matched to the elimination clearance . . . . .
�9 Maintenance infusion rate (I) = Css. ClE
While the combined bolus and infusion method of Mitenko and Ogilvie produces and maintains effective plasma or blood drug concentrations from soon after beginning drug administration, it produces very high initial drug concentrations which persist until drug distribution is well under way (Figure 8). Thus, this technique is useful only for drugs, such as muscle relaxants, which have high clinical margins of safety when used by anaesthetists.
An infusion regimen for drugs with low clinical margins of safety must

PHARMACOKINETICS AND PHARMACODYNAMICS 503
quickly produce and continually maintain effective plasma or blood drug concentrations without the overshoot of drug concentrations characteristic of the Mitenko and Ogilvie infusion method. Such an approach was proposed in 1968 by Kriiger-Thiemer. The loading dose or bolus is designed to provide effective plasma or blood drug concentrations upon mixing within an initial, rapidly equilibrating, volume of distribution or central volume, Vc:
Loading dose = C,,- Vc
The maintenance infusion rate is matched to the multiexponential character- ization of the plasma or blood drug concentration versus time relationship, decreasing exponentially, until at the end of the drug distribution phase, it is matched to the elimination clearance:
Maintenance infusion rate (I) = C~ ( CIE + C/I e-k21t)
where CII is the distributive or intercompartmental clearance, k2~ is the rate constant from the peripheral compartment to Vr and t is elapsed time since commencing the infusion. McMurray and associates (1986) have admini- stered methohexitone as part of a methohexitone-N20/fentanyl anaesthetic regimen using this technique, implemented with readily available equip- ment (Figure 9).
The above approaches to drug infusions are open-loop regimens, i.e. they are fixed techniques which make no formal allowance for individualization to a patient's needs. When they are based on conservative estimates of pharmacokinetics and effective plasma or blood concentrations, they should
E O
"E o
O o
E "E O
> t~
E.
1.00
0.50
0.10
0.05
0.01 0
. . . .O
~ . ~ . ~ : : ...... ..oO.....o ......
, I I I , I I I , I 1.0 2.0 3.0 4.0 5.0
Time (h)
- - 100
8O
60
40
20
0
6.0
"10
t~
tg~
o
o
Figure 9. Plasma drug concentration versus time relationship and the corresponding percentage paralysis during and after an infusion of vecuronium using the bolus and infusion scheme of Mitenko and Ogilvie (1972). From Avram and Henthorn (1988), with permission, based on data from Shanks et al (1987).

504 T . K . H E N T H O R N A N D M . J . A V R A M
prove satisfactory in most patients. However, infusions may be optimized by adjusting them on the basis of a patient's response or lack of response to stimuli, closing the loop. If a suitable measure of drug effect is available, the patient, the anaesthetist or a computer can adjust the infusion rate to that just maintaining the desired effect. Unfortunately, unequivocal measures of the effects of many of the drugs used in the practice of anaesthesia are not available.
Two drug effects that are easily measured are neuromuscular blockade and arterial blood pressure, and closed-loop infusions to control both have been described. MacLeod and associates (1989) described a closed-loop infusion of atracurium to provide automatic control of neuromuscular blockade which was both close to the target and stable (Figure 10) despite a threefold range in dosage requirements. Successful postoperative feedback control of arterial blood pressure was provided by an infusion of glyceryl trinitrate up to a maximum rate of 50 mg/h, at which point an infusion of sodium nitroprusside was added automatically in a technique described by Colvin and Kenney (1989). This method has the advantage of avoiding the use of the potentially toxic sodium nitroprusside in patients who do not need it.
A 8 8 ~ o ~ 9 9
1 . . . . . . . . . . . . . . . . . . . . . ' . . . . . . . . . . . .
5 0 . . . . . . . . . . . . . . . . . . . . . . . . . . .
oj II~.,,,, ,...,,,,t._,-,,,,nlIMIHMHUUHIMImulHmu(mm_eWIBH!Igll HI IHIf f i l I I I~
1 :t 7 I: s,,0,o 0or,e0 , . - - - - - - - - Control ler in operation
~5 120 q,
100",' ~, . . . . . . . .
5 0 ,
0 7 Stable period
J~-----Controller in operation
Figure 10. Neuromuscular blockade produced by atracurium during a feedback-controlled infusion of the drug in two patients. From MacLeod et al (1989), with permission

PHARMACOKINETICS AND PHARMACODYNAMICS 505
The primary means of terminating the effect of a standard dose of a drug administered by rapid intravenous injection is by redistribution. When drugs are administered by continuous infusion, the tissues of the body approach equilibrium with plasma or blood drug concentrations, making the contribution of redistribution to the termination of drug effect upon dis- continuing the infusion less important, and that of elimination clearance more important. Therefore, drugs with high elimination clearances are best suited to administration by infusion.
Continuous intravenous infusions of several drugs can be used to produce hypnosis, analgesia and muscle relaxation in a totally intravenous anaesthetic technique. Alternatively, infusions of individual drugs can be used selectively as adjuvants to nitrous oxide or the potent volatile anaesthetics, or to provide sedation for regional anaesthetic techniques. Commercially available drug infusion pumps make implementation of some of the general approaches to drug infusions described above very easy. In addition, a pocket calculator programme described by Maitre and Sharer (1990) estimates plasma or blood drug concentrations at any time during and after an intravenous drug infusion, helping anaesthetists to understand drug administration by infusions in the same way as they understand the administration of potent volatile anaesthetics.
A textbook discussing the use of drug infusions in anaesthesia has recently been published, and is recommended to those interested in a more thorough treatment of this subject (Fragen, 1991).
PHARMACOGENETICS AND PHARMACOKINETIC VARIABILITY
Much has been learned in the past decade about the genetic variability of hepatic oxidative metabolism. Magoub et al (1977) and Eichelbaum et al (1979) reported that the 4-hydroxylation of debrisoquine and the y-oxidation of sparteine had distinctly polymorphic metabolism, indicating that the responsible P-450 isozymes were under monogenic control. It has since been shown that the same isozyme is responsible for the oxidative metabolism of both of these drugs and that 5-10% of caucasians are homozygous for the recessive gene, expressing the defective or absent isozyme.
A growing list of drugs has been shown to rely on this cytochrome P-450 isozyme, the P450IID6 (P450dbl), for oxidative metabolism (primarily hydroxylations, o-dealkylations, and o-dealkylations) and elimination clearance. Wedlund et al (1984) first reported that the 4-hydroxylation of s-mephenytoin represented a second polymorphism of drug oxidation. While these investigators found the defective isozyme (P450IIC9) to be present in fewer than 5% of caucasians, Jurima et al (1985) reported that perhaps 25% of certain oriental groups may be poor metabolizers.
Because interindividual variability in response to drugs is so common, variability due to genetic inheritance should not be viewed as a particular problem. It should be possible to predict the optimal dose from the patient's phenotype. Unfortunately, sparteine-debrisoquine phenotyping is not yet a routine clinical test. Br0sen and Gram (1989) have pointed out that

506 T. K. H E N T H O R N A N D M. J. AVRAM
polymorphic drug oxidation attains clinical significance when a drug is significantly dependent on P450IID6, resulting in clinically important pharmacokinetic variability which leads to a variability in response that can not be easily detected (because the effect is not easily titratable), before the materialization of an unfavourable clinical response (due to a narrow therapeutic index).
In general, three classes of drugs are heavily represented among those having P450IID6-dependent metabolism: tricyclic antidepressants, anti- arrhythmics and ~-blockers. [3-blockers, such as metoprolol, have relatively large therapeutic indices and are easily titrated to clinical response. The polymorphic metabolism of metoprolol has not posed much of a problem. Antidepressants and antiarrhythmics are difficult to titrate to effect, and have significant toxicity at levels just above those that are therapeutic. These drugs usually require plasma level monitoring.
Although intravenous anaesthetic drugs are generally considered safe within the controlled context of the operating room, they are difficult to titrate. Persisting somnolence and respiratory depression after surgery are no longer advantageous. If these effects become prolonged because poor elimination clearance results in elevated plasma concentrations of a particu- lar agent, they would have to be considered clinically significant adverse responses.
Drug-drug interaction related to selective inhibition of the P450IID6 isozyme is also a potential problem. When potent competitive in vitro inhibitors such as quinidine (Steiner et al, 1988) or propafenone (Wagner et al, 1987) are given with a polymorphically oxidized drug, the pharmaco- kinetics become similar to those observed in patients of the poor metabolizer phenotype. Such interactions can result in fivefold increases in plasma concentrations of the polymorphically oxidized drug.
Alfentanil
Prolonged clinical effect of alfentanil following continuous infusion for anaesthesia has been a disconcerting feature in some patients. Shafer et al (1986) observed late respiratory depression related to reduced elimination clearance of alfentanil; a similar series was recently reported by Krane et al (1990). McDonnell et al (1984) first suggested that polymorphic metabolism of alfentanil might be the cause of these unwanted clinical effects.
Simple in vitro techniques such as the one proposed by von Bahr et al (1985) have been used to screen drugs for interaction with the P450IID6 isozyme. Test drugs are investigated for their ability competitively to inhibit a known exclusive pathway of P450IID6. Henthorn et al (1989b) tested a series of narcotic analgesics in vitro for their ability competitively to inhibit P450IID6. They found that alfentanil was a weak inhibitor (Ki = 176 p~M), suggesting that its elimination clearance may depend on P450IID6 for elimination clearance. Fentanyl was a relatively strong inhibitor (Ki = 21 IXM), also suggesting a possible P450IID6 influence. Dextropro- poxyphene was so potent an inhibitor (Ki = 2.5 p,M) as to indicate that it may inhibit this isozyme in vivo under clinical conditions.

P H A R M A C O K I N E T I C S A N D P H A R M A C O D Y N A M I C S 507
Henthorn et al (1989c) later reported the pharmacokinetics of alfentanil in seven healthy volunteers of known debrisoquine oxidation phenotype (four extensive metabolizers and three poor metabolizers) and found no correlation between phenotype and elimination clearance. This, along with a previous report of in vivo alfentanil metabolism by Meuldermans et al (1988), in which one poor metabolizer was studied, provides further, possibly final, evidence that P450IID6 is not important for the metabolism of alfentanil.
This apparently contradictory in vivo observation is explained by a Lavrijsen et al's (1988) more complete in vitro description of alfentanil's interaction with P450IID6. They found that debrisoquine did not com- petitively inhibit the formation of the major alfentanil metabolites, noralfentanil and N-phenylpropanamide. Furthermore, the Km for alfentanil metabolism was 22.8 tXM, much smaller than the Ki of 176 DxM mentioned above, indicating the relative lack of importance of P450IID6 to alfentanil metabolism.
Other factors, then, must account for the marked interindividual variability in alfentanil pharmacokinetics. The study by Henthorn et al (1989c) also showed that hepatic blood flow is not likely to be a major factor, inasmuch as they found no correlation between the clearance of indocyanine green and that of alfentanit. An important source of pharmacokinetic variability was reported by Bartkowski et al (1989). They showed that marked decreases in alfentanil elimination clearance can result from conco- mitant treatment with erythromycin. Clinicians should be alert to this inter- action.
Benzodiazepines Benzodiazepines also have variable pharmacokinetics that have resulted in significant prolongation of effect. Greenblatt et al (1980) extensively studied factors accounting for the variability in diazepam disposition. With the advent of midazolam, Dundee et al (1986) raised similar concerns. Both of these drugs are metabolized by hepatic P-450 enzymes via hydroxylation (midazolam and diazepam) and N-demethylation (diazepam). Therefore, P-450 polymorphism may account for some of the observed variability in clearance.
Klotz et al (1986), utilizing a phenotyped panel of healthy subjects, studied the possible importance of P450IID6 to midazolam clearance and found no relationship. Later, as reported by Kassai et al (1989), this group measured the elimination half-life of midazolam in 168 surgical patients. While they did report three patients with significantly prolonged half-lives of 7.5-10.2 h, they concluded, based on the t~/2 frequency distribution, that these patients did not constitute a separate group. Although none of the subjects in this study had their metabolic phenotypes determined, it was concluded that neither P450IID6 nor s-mephenytoin 4-hydroxylase (P450IIC9) was significantly involved in the metabolism of midazolam.
Bertilsson et al (1989) studied the possible contribution of P450IID6 and s-mephenytoin 4-hydroxylase to the elimination clearance of diazepam.

5 0 8 T. K. HENTHORN AND M. J. AVRAM
They used a phenotyped panel that included three poor metabolizers of debrisoquine and three other subjects who were poor metabolizers of s-mephenytoin. They found that approximately one half of the diazepam dose is metabolized by N-demethylation to desmethyldiazepam and that another one half is metabolized by other means, probably 3-hydroxylation to temazepam. Like diazepam, desmethyldiazepam is also 3-hydroxylated to oxazepam.
The results indicated that P450IID6 was not involved in any of these pathways. However, the clearance of both diazepam and desmethyldiazepam was approximately halved in those subjects with poor s-mephenytoin oxidation phenotypes. The close relationship between total diazepam clearance and the clearance of desmethyldiazepam indicates that the demethylation and hydroxylation of these two compounds are performed by the same isozyme. These findings may have more importance for oriental patients, because up to 25% may be poor metabolizers of s-mephenytoin.
SUMMARY
New drugs continue to be introduced into anaesthetic practice. Often innovation involves a modification of pharmacokinetic properties rather than pharmacologic activity. Besides selecting drugs based on its pharmaco- kinetic profile, the anaesthetist is increasingly faced with giving repetitive doses or continuous infusions of drugs to maintain the anaesthetic state. Accordingly, an understanding of pharmacokinetic and pharmacodynamic principles as well as factors which may cause patients or drugs to vary from one to another is essential.
A description of the basic pharmacokinetic variables volume, elimination clearance, and half-life and their uses provides a foundation for introducing concepts of multicompartmental kinetics to clinical anaesthesia. Distri- bution clearance is defined as the ratio of drug transfer rate and drug concentration. Recent studies examining possible age-dependent changes in thiopentone distribution clearance are reviewed. During the onset of intravenous anaesthetic drug effect, pharmacokinetics are complicated by intravascular mixing and the interaction of drug with lung tissue. These processes influence early arterial drug concentrations and arterial-venous concentration differences.
Combined pharmacokinetic-pharmacodynamic models were developed to characterize the time course of drug action and its relationship to plasma concentrations. More recent studies have used these models to detail differences between drugs and understand better the differences in dose response relationship among patients or groups of patients. However, the use of these models often requires a reliable continuous measure of drug effect on the central nervous system. Approaches to the use of computer- processed electroencephalograms have shown some promise in this regard, but still have sufficient limitations to make them impractical in the clinical setting and unusable in many investigational situations.

PHARMACOKINETICS AND PHARMACODYNAMICS 509
Many anaesthet ic drugs are metabol ized by oxidative metabol ic pathways actuated by specific pro te ins (e.g. P-450 enzymes) . Several of these prote ins are subject to c o m m o n genetic variabil i ty that lead to marked variabil i ty in the per formance of the oxidative pathway. While studies have suggested that a lfentani l and midazo lam are not subject to this variabil i ty in elimi- na t ion , o ther drugs (e.g. d iazepam) may be affected and require fur ther studies.
Pharmacokine t i c and pha rmacodynamic in format ion have come together to permi t the in t roduc t ion of con t inuous adminis t ra t ion of anaesthet ic drugs. The bases for des igning and implemen t ing these techniques should be unders tood by anaesthet is ts , so that the advantages of newer drugs can be realized.
R E F E R E N C E S
Arden JR, Holley FO & Stanski DR (1986) Increased sensitivity to etomidate in the elderly: initial distribution versus altered brain response. Anesthesiology 65: 19-27.
Ausems ME, Hug CC, Stanski DR & Burro AG (1986) Plasma concentrations of alfentanil required to supplement nitrous oxide anesthesia for general surgery. Anesthesiology 65: 362-372.
Avram MJ & Henthorn TK (1988) What's new in pharmacokinetics and pharmacodynamics? Anesthesiology Clinics of North America 6: 251-280.
Avram MJ, Henthorn TK, Shanks CA & Krejcie TC (1986) The initial rate of change in distribution volume is the sum of intercompartmental clearances. JournalofPharmaceutical Sciences 75: 919-920.
Avram MJ, Krejcie TC & Henthorn TK (1990) The relationship of age to the pharmacokinetics of early drug distribution: the concurrent disposition of thiopental and indocyanine green. Anesthesiology 72" 403-411.
Barratt RL, Graham GG & Torda TA (1984) Kinetics of thiopentone in relation to the site of sampling. British Journal of Anaesthesia 56: 1385-1391.
Bartkowski RR, Goldberg ME, Larijani GE & Boerner T (1989) Inhibition of alfentanil metabolism by erythromycin. Clinical Pharmacology and Therapeutics 46: 99-102.
Bertilsson L, Henthorn TK, Sanz E et al (1989) Importance of genetic factors in the regulation of diazepam metabolism: relationship to s-mephenytoin, but not debrisoquin, hydroxy- lation phenotype. Clinical Pharmacology and Therapeutics 45- 348-355.
BrOsen K & Gram LF (1989) Clinical significance of the sparteine/debrisoquine oxidation polymorphism. European Journal of Clinical Pharmacology 36: 537-547.
Bfihrer M, Maitre PO, Ebling WF et al (1987) Defining thiopental's steady state plasma concentration-EEG effect relationship. Anesthesiology 67: A658.
Biihrer M, Maitre PO, Hung O & Stanski DR (1990a) Electroencephalographic effects of benzodiazepines. I. Choosing an electroencephalographic parameter to measure the effect of midazolam on the central nervous system. Clinical Pharmacology and Therapeutics 48: 544-554.
Bfihrer M, Maitre PO, Crevoisier C & Stanski DR (1990b) Electroencephalographic effects of benzodiazepines. I. Pharmacodynamic modeling of the electroencephalographic effects of midazolam and diazepam. Clinical Pharmacology and Therapeutics 48: 555-567.
Chiou WL (1989) The phenomenon and rationale of marked dependence of drug concentration on blood sampling site: implications in pharmacokinetics, pharmacodynamics, toxicology and therapeutics (parts I and II). Clinical Pharmacokinetics 17:175-199 & 275-290.
Christensen JH & Andreasen F (1978) Individual variation in response to thiopental. Acta Anaesthesiologica Scandinavica 22: 303-313.
Colvin JR & Kenney GNC (1989) Automatic control of arterial pressure after cardiac surgery: evaluation of a microcomputer-based control system using glyceral trinitrate and sodium nitroprusside. Anaesthesia 44: 3%41.

510 T. K. HENTHORN AND M. J. AVRAM
Dundee JW, Hassard TH, McGowan WAW & Henshaw J (1982) The 'induction' dose of thiopentone: a method of study and preliminary illustrative results. Anaesthesia 37: 1176-1184.
Dundee JW, Collier PS, Carlisle RJT & Harper KW (1986) Prolonged midazolam elimination half-life. British Journal of Clinical Pharmacology 21: 425-429.
Eichelbaum M, Spannbrucker N, Steincke B & Dengler HJ (1979) Defective N-oxidation of sparteine in man: a new pharmacogenetic defect. European Journal of Clinical Pharma- cology 16: 183-187.
Fisher DM, O~Keeffe C, Stanski DR et al (1982) Pharmacokinetics and pharmacodynamics of •-tubocurarine in infants, children, and adults. Anesthesiology 57: 203-208.
Fragen RJ (ed.) (1991) Drug Infusions in Anesthesiology. New York: Raven Press. Fragen RJ & Avram MJ (1989) Non-opioid intravenous anesthetics. In Barash PG, Cullen BF
& Stoelting RK (eds) Clinical Anesthesia, pp 227-254. Philadelphia: Lippincott. Fragen RJ & Avram MJ (1990) Barbiturates. In Miller RD (ed.) Anesthesia, 3rd edn, pp 225-
242. New York: Churchill Livingstone. Greenblatt D J, Allen MD, Harmatz JS & Shader RI (1980) Diazepam disposition determi-
nants. Clinical Pharmacology and Therapeutics 27: 301-312. Greenblatt DJ, Ehrenberg BL, Gunderman J e t al (1989) Pharmacokinetic and electro-
encephalographic study of intravenous diazepam, midazolam, and placebo. Clinical Pharmacology and Therapeutics 45: 356-365.
Henthorn TK, Avram MJ & Krejcie TC (1989a) Intravascular mixing and drug distribution: the concurrent disposition of thiopental and indocyanine green. Clinical Pharmacology and Therapeutics 45: 56-65.
Henthorn TK, Spina E, Dumont E &von Bahr C (1989b) In vitro inhibition of a polymorphic human liver p-450 isozyme by narcotic analgesics. Anesthesiology 70: 339-342.
Henthorn TK, Avram MJ & Krejcie TC (1989c) Alfentanil clearance is independent of the polymorphic debrisoquin hydroxylase. Anesthesiology 71: 635-639.
Homer TD & Stanski DR (1985) The effect of increasing age on thiopental disposition and anesthetic requirement. Anesthesiology 62: 714-724.
Jurima M, Inaba T, Kadar D & Kalow W (1985) Genetic polymorphism of mephenytoin p(4')-hydroxylation: difference between orientals and caucasians. British Journal of Clinical Pharmacology 19: 483-487.
Kassai A, Toth G, Eichelbaum M & Klotz U (1989) No evidence of a genetic polymorphism in the oxidative metabolism of midazolam. Clinical Pharmacokineties 15: 319-325.
Klotz U, Mikus G, Zekorn C & Eichelbaum M (1986) Pharmacokinetics of midazolam in relation to polymorphic sparteine oxidation. British Journal of Clinical Pharmacology 22: 618-619.
Krane BD, Kreutz JM, Johnson DL & Mazuzan JE (1990) Alfentanil and delayed respiratory depression: case studies and review. Anesthesia and Analgesia 70: 557-561.
Kriiger-Thiemer E (1968) Continuous intravenous infusion and multicompartmental accumu- lation. European Journal of Pharmacology 4: 317-324.
Lavrijsen KLM, van Houdt JMG, van Dijck DMJ et al (1988) Is the metabolism of alfentanil subject to debrisoquine polymorphism? A study using human liver microsomes. Anesthesiology 69: 535-540.
Lemmens HJM, Bovill JG, Hennis PJ et al (1989) Alcohol consumption alters the pharmaco- dynamics of alfentanil. Anesthesiology 71: 669-674.
Levy G (1966) Kinetics of pharmacologic effects. Clinical Pharmacology and Therapeutics 7: 362-372.
McDonnell TE, Bartkowski RR & Kahn C (1984) Evidence for polymorphic oxidation of alfentanil in man. Anesthesiology 61: A284.
MacLeod AD, Asbury AJ, Gray WM & Linken DA (1989) Automatic control of neuro- muscular blockade with atracurium. British Journal of Anaesthesia 63: 31-35.
McMurray TJ, Robinson FP, Dundee JW, Riddell JG & McLean E (1986) A method for producing constant plasma concentrations of drugs: application to methohexitone. British Journal of Anaesthesia 58: 1085-1090.
Magoub A, Idle JR, Dring LG et al (1977) Polymorphic hydroxylation of debrisoquine in man. Lancet ii: 584-586.
Maitre PO & Sharer SL (1990) A simple pocket calculator approach to predict anesthetic drug concentrations from pharmacokinetic data. Anesthesiology 73: 225-229.

PHARMACOKINETICS AND PHARMACODYNAMICS 511
Meuldermans W, van Peer A, Hendrickx J e t al (1988) Alfentanil pharmacokinetics and metabolism in humans. Anesthesiology 69: 527-534.
Mitenko PA & Ogilvie RI (1972) Rapidly achieved plasma concentration plateaus, with observations on theophylline kinetics. Clinical Pharmacology and Therapeutics 13: 329- 335.
Persson MP, Nilsson A & Hartvig P (1988) Relation of sedation and amnesia to plasma concentrations of midazolam in surgical patients. Clinical Pharmacology and Therapeutics 43: 324-331.
Price HL, Kovnat PJ, Safer JN, Conner EH & Price ML (1960) The uptake of thiopental by body tissues and its relationship to the duration of narcosis. Clinical Pharmacology and Therapeutics 1: 16-22.
Roerig DL, Kotrly KJ, Ahlf SB, Dawson CA & Kampine JP (1989a) Effect of propranolol on the first pass uptake of fentanyl in the human and rat lung. Anesthesiology 71: 62-68.
Roerig DL, Kotrly K J, Dawson CA et al (1989b) First-pass uptake of verapamil, diazepam, and thiopental in the human lung. Anesthesia and Analgesia 69: 461-466.
Sanghvi R, Henthorn TK, Krejcie TC et al (1991) Patient characteristics associated with the thiopental doses at clinical and EEG induction endpoints. Clinical Pharmacology and Therapeutics 49: 164.
Segre G (1968) Kinetics of interaction between drugs and biological systems, ll Farmaco Edizione Scientifica 23: 907-918.
Sharer A, Sung M-L & White PF (1986) Pharmacokinetics and pharmacodynamics of alfentanil infusions during general anesthesia. Anesthesia and Analgesia 65: 1021-1028.
Sharer SL & Varvel JR (1991) Pharmacokinetics, pharmacodynamics, and rational opioid selection. Anesthesiology 74: 53-63.
Shanks CA, Avram MJ, Fragen RJ & O'Hara DA (1987) Pharmacokinetics and pharmaco- dynamics of vecuronium administered by bolus and infusion during halothane or balanced anesthesia. Clinical Pharmacology and Therapeutics 42: 459-464.
Sheiner LB (1989) Clinical pharmacology and the choice between theory and empiricism. Clinical Pharmacology and Therapeutics 46: 605-615.
Sheiner LB, Stanski DR, Vozeh Set al (1979) Simultaneous modeling of pharmacokinetics and pharmacodynamics: application to D-tubocurarine. Clinical Pharmacology and Thera- peutics 25: 358-371.
Stanski DR & Maitre PO (1990) Population pharmacokinetics and pharmacodynamics of thiopentah the effect of age revisited. Anesthesiology 72: 412-422.
Stanski DR, Ham J, Miller RD & Sheiner LB (1979) Pharmacokinetics and pharmacodynamics of dTc during nitrous oxide-narcotic and halothane anesthesia in man. Anesthesiology 51: 235-241.
Stanski DR, Hudson RJ, Homer TD, Saidman LJ & Meathe E (1984) Pharmacodynamic modeling of thiopental anesthesia. Journal of Pharmacokinetics and Biopharmaceutics 12: 223-240.
Steiner E, Dumont E, Spina E & Dahlqvist R (1988) Inhibition of desipramine 2-hydroxylation by quinidine and quinine in rapid and slow hydroxylators. Clinical Pharmacology and Therapeutics 43: 577-581.
von Bahr C, Spina E, Birgersson C et al (1985) Inhibition of desmethylimipramine 2- hydroxytation by drugs in human liver microsomes. Biochemical Pharmacology 14: 2501- 2505.
Wagner F, Kalusche D, Trenk D et al (1987) Drug interaction between propafenone and metoprolol. British Journal of Clinical Pharmacology 24: 213-220.
Wedlund PJ, Aslanian WS, McAllister CB et al (1984) Mephenytoin hydroxylation deficiency in caucasians: frequency of a new oxidative drug metabolism polymorphism. Clinical Pharmacology and Therapeutics 36: 773-780.