Embed Size (px)
Citation preview

Journal of Controlled Release, 11 (1990) 343-356 343 Elsevier Science Publishers B.V., Amsterdam - - Printed in The Netherlands
P H A R M A C O K I N E T I C A N D P H A R M A C O D Y N A M I C ASPECTS OF POLYPEPTIDE DELIVERY*
Norman A. Mazer** Thera Tech, Inc. and DepaFtment of Pharmaceutics, University of Utah, Sa/t Lake City, UT (U.S.A.)
Key words: polypeptides; pharmacokinetics; pharmacodynamics; input function; modelling
The rational design and development of drug delivery systems for polypeptide compounds re- quires a quantitative understanding of the pharmacokinetics (PK) and pharmacodynamics (PD) of the compound in the intended therapeutic indication. In particular it is necessary to define the characteristics of the input function, i.e. the rate and time course o/systemic drug input, that will maximize the therapeutic effect, minimize unwanted side effects and prevent tachyphylaxis from occurring. This paper reviews the general concepts of input/unction, PK and PD, and illustrates these concepts using two examples from the literature: (1) Sandoz compound SMS 201-995 and (2) gonadotropin-releasing hormone (GnRH). For SMS 201-995, a continuous (zero-order) input function is shown to be optimal for suppressing growth hormone secretion in the treatment of acromegaly. For GnRH, a pulsatile input function is optimal for stimulating pituitary gonadotro- pin secretion, whereas continuous input leads to a paradoxical suppression of gonadotropin se- cretion. These examples further illustrate the types of novel experimental approaches, using pro- grammable infusion pumps, that are needed for investigating the relationship between PK and PD, and for defining the optimal input function experimentally. In addition, we show how math- ematical models may be used to describe the interrelationships between input function, PK and PD. For SMS 201-995, a model based on the "effect compartment" concept offers a self-consistent description of the linkage between PK and PD and provides insight into the superiority of con- tinuous input in the treatment of acromegaly. For GnRH, the complex relationship between input function and gonadotropin secretion is modelled on the basis of heuristic concepts that relate the time-averaged occupancy of the GnRH-receptors (by GnRH) to the expression of GnRH-receptors by the pituitary (i.e. down and up regulation). Together these examples illustrate the diversity of input functions that will be needed in polypeptide delivery and the novel experimental and the- oretical approaches required for defining them.
*Paper presented at the Fourth International Symposium on Recent Advances in Drug Delivery Systems, Salt Lake City, UT, U.S.A., February 21-24, 1989. **Correspondence should be sent to the author c/o: TheraTech, Inc., 410 Chipeta Way, Suite 219, Salt Lake City, UT 84108 (U.S.A.)
INTRODUCTION
The selection of appropriate technologies and routes of administration for the delivery of any drug should be based on a quantitative under- standing of the pharmacokinetics and phar- macodynamics of the particular compound.
0168-3659/90/$03.50 © 1990 Elsevier Science Publishers B.V.

344
This is especially true for natural polypeptides and their synthetic analogues, whose physio- logical and pharmacological activities can in- volve complex feedback interactions with tar- get organ receptors.
To design polypeptide drug delivery systems on a rational base, it is first necessary to define the input function i (t) that will provide the op- timal rate and time course of systemic drug in- put (e.g. zero order, first order, pulsatile, etc. ) with respect to: 1. maximizing therapeutic efficacy, 2. minimizing undesirable side effects, and 3. preventing, if possible, the development of
tolerance (tachyphylaxis) to the desired ef- fects of the compound.
This paper introduces the general concept of input function and its linkage to pharmacoki- netics (PK) and pharmacodynamics (PD). Novel experimental and theoretical approaches for investigating the interrelationships be- tween i (t), PK and PD are then illustrated with recent literature data from two well-studied polypeptides. The first example, Sandoz com- pound SMS 201-995, is a synthetic analogue of somatostatin used in the treatment of acrome- galy and certain GI hormone-secreting tumors [ 1 ]. Experimental PD data and mathematical models (developed by the author) show that a continuous (zero-order) input of SMS 201-995 is optimal for the suppression of growth hor- mone levels in acromegalic patients. The sec- ond example, GnRH {also known as LHRH), is the native hypothalamic gonadotropin re- leasing hormone. The elegant experimental studies carried out by Knobil and co-workers in the rhesus monkey [ 2 ] demonstrate that a pul- satile GnRH input function is necessary to stimulate the physiological secretion of LH and FSH by the pituitary, whereas continuous GnRH input leads to a paradoxical suppression of LH and FSH levels. A novel phenomenolog- ical model for understanding the complex in- teraction between the GnRH input function and the PD response, on the basis of receptor mod- ulation (down-regulation), is also presented.
INTERRELATIONSHIPS BETWEEN INPUT FUNCTION, PHARMACOKINETICS AND PHARMACODYNAMICS
Figure 1 schematizes the interrelationships between the drug input function [i(t) ] (i.e. the rate and time course of systemic drug input), the pharmacokinetics (i.e. the time course of plasma levels of parent compound and metab- olites), and the pharmacodynamics (i.e. the time course of drug/receptor interactions and cell modulation which ultimately produce the desired pharmacological effects and side effects of the drug). In this context, i(t) "drives" the PK response Cp (t), which in turn drives the di- rect PD response E(t) and side effects. For polypeptide compounds in particular, the phar- macodynamic responses of the target organs can be influenced at various levels (e.g. receptors, intracellular responses and at more distal sites) by external feedback from other organs, hot-
DRUG i(t)t . . . . ] . . . . . . . INPUT [ '~ I FUfJcNPIUNT i(t) | i% ~,
, t
K [NETICS (PK) / / ~ y ~ t
- - SIDE EFFECTS
DRUG/ I RECEPTOR
I NTERACTION
SELF ,'T--i" CELL ~ ME:D~jEL~NA~N FEEDBACK ~'__-~ MODU LATION PHARMACO- DYNAMICS
(PD)
i 1 down
EFFECTE(I) E ( l ) ~
- - t
Fig. 1. Schematic diagram illustrating the linkage between the drug input function (i.e. the rate and time course of drug input into the systemic circulation), pharmacokinet- its and pharmacodynamics of polypeptide compounds [see text for explanation of i(t), Cp(t) and E(t) ].

345
INPUT FUNCTIONS ] =_ I EFFEOTSJ ZERO ORDER:
F,RSTOROER: PEUT,C I . VENT
+(t) I ;_ [ " " * k71 I~-~ Ti ---~ t t
MI EFFECT(S)
t
+1 I-,- ~-Ti -"4 t At
Fig. 2. The optimal input function for a given polypeptide drug (left side of figure) may be zero-order, first-order, pulsatile, mixed or some other wave form. It must achieve three pharmacodynamic criteria (right side of figure): (1) maximize the therapeutic effect, (2) minimize unwanted side effects and (3) prevent tolerance development to the desired therapeutic effect of the compound.
mones or neurons that positively or negatively modulate the system. In addition, self-feedback within the target organs themselves can also modulate the time course of the PD responses. For the zero-order input function depicted in Fig. 1, Cp(t) should increase to a steady-state plateau (Cp+s). In simple cases (e.g. SMS 201- 995) E(t) will likewise reach a plateau, but in more complex systems (e.g. GnRH), E(t) may decrease with time even in the face of a con- stant drug plasma level. This represents the so called "down"-regulation phenomenon which is presumably related to the self or external feedback effects.
As depicted in Fig. 2, the optimal input func- tion (e.g. zero order, first order, pulsatile, mixed or other) should produce effects which satisfy the three criteria given above (e.g. maximize therapeutic efficacy, minimize side effects and prevent down-regulation). A priori, it is diffi- cult to know which type of input function will be best suited for a particular polypeptide and
therapeutic indication. To answer this impor- tant question innovative experimental ap- proaches and theoretical models, as presented below, are needed to investigate the interrela- tionships between i (t), PK and PD.
I LLUSTRATIVE E X A M PLES
a. S M S 2 0 1 - 9 9 5 : Continuous input is best for the t reatment of acromegaly, as shown by an "effect compartment" model
SMS 201-995, a synthetic octapeptide ana- logue of somatostatin, suppresses the pituitary secretion of growth hormone (GH) in normal and pathological states (e.g. acromegaly) and is also used clinically to suppress GI hormone secretion from endocrine pancreatic tumors and carcinoids [3 ].

346
1. Pharmacokinetics of SMS 2 0 1 - 9 9 5 The pharmacokinetics of SMS 201-995, ad-
ministered by IV and subcutaneous (SC) injec- tion, has been studied as a function of dose in healthy subjects by Kutz et al. [4]. The IV data are consistent with a dose-independent, two- compartment model [4]. Although the phar- macokinetics after SC injection qualitatively exhibits a single exponential decay (i.e. one- compartment behavior ) it can be shown that the SC data are nevertheless consistent with the same two-compartment parameters of the IV administration [4] driven by dose-indepen- dent first-order SC input function. From our analysis, the absorption half-life tl/2abs is esti- mated to be 0.37 h, which is intermediate be- tween t1/2~ (0.167 h) and tz/2p (1.34 h). The bioavailability of the SC route is approximately 100% [4 ]. A graphical illustration of our phar- macokinetic model, simulations of the IV and
SC plasma levels, and derived pharmacokinetic parameters are given in Fig. 3.
2. Pharmacodynamics of SMS 2 0 1 - 9 9 5 The pharmacodynamics of SMS 201-995 (i.e.
reduction in plasma GH levels) has been stud- ied in acromegalic patients after single SC doses of 50, 100 and 200 #g by Wass et al. [5]. From these mean data (n = 4), we have computed a measure of the PD effect, E( t ) , as:
E(t ) = 100× GH( t) - B a s a l level% (1) Basal level
where GH(t) is the GH plasma level at time t, and Basal level reflects the average GH level at time 0 (see Fig. 4A). In view of the short half- life o fGH ( ~22 min. [6] ), the E(t) values de- fined in this way will closely parallel the time dependence of GH secretion by the acromegalic tumor. Although SMS 201-995 plasma levels
SC INPUT k12 = 1.7311 hr~ l,f~_
F = 100% ) " f ^ ~
kab s = 1.85 hr -I k21 1.5125 hr-
t]abs = 0.37 hr
.4124 hr -I
Simulations: 100 meg / kabs = 1.85 hr-I 100
Derived Parameters
(_J
Cpe.~x - 4 .4 n ~ ' s l
t O "
O.'lO .o Lo 2.0 3.o 4.0 s.o s.o "/2 e.Q
tlme(hr)
C£ = 9.71 E/hr
a = 4.14 hr -I
t2ia = 0.167 hr
B = 0.516 hr -I
t]B = 1.34 hr
Fig. 3. Pharmacokinetic model of SMS 201-995 in healthy volunteers derived from experimental data of Kutz et al. [4 ]. IV bolus input is consistent with a two-compartment model. The microconstants k12, k21 and k~0 are estimated from the mean macroconstant parameters given in Ref. [4 ]. Subcutaneous (SC) input has been modelled as a first-order absorption process with 100% bioavailability. The SC rate constant kab~ (1.85 h-1 ) was deduced by fitting the mean Cpmax (4.4 ng/ml) and tmax (26 min) observed experimentally for a 100 #g dose (see simulated plasma levels for SC and IV input). Derived mean pharmacokinetic parameters for SMS 201-995 are also given.

0
LL
IL l
-2O
-40
- 6 0
- 8 0
- 100 .0
5O
100
200
I I I I I I 2.0 4.0 6.0 8.0 ]o.o 12.0 14.0 t/me(hr}
LLI
o
- 2 0 •
- 4 0 -
- 6 0 •
- 8 0 •
- lOO .o
i
I I I 2 .0 4.n 6 .0
Cp(ng/ml}
I 8 .0 10J]
Fig. 4. (A) Time course of pharmacodynamic effect (growth hormone suppression) of SMS 201-995 administered sub- cutaneously to acromegalic patients (n--4) at doses of 50, 100 and 200 pg (from study of Wass et al. [5] ). (B) Hys- teresis loops are obtained by plotting the pharmacodyn- amic effect data from panel A versus the simulated SMS 201-995 plasma levels (Cp) obtained from the pharmaco- kinetic model of Fig. 3. The simulated pharmacokinetic profiles at each SC dose are shown in the upper left panel of Fig. 6.
were not measured in this study, limited PK data obtained in acromegalic patients [7 ] are similar to the modelled results of healthy sub- jects. For this reason, we have interpreted the E(t) data of Wass et al. using simulated PK
347
profiles (shown in Fig. 6) for the three SC doses administered. When the E(t) values at each dose are plotted versus the simulated Cp (t) val- ues, three hysteresis loops are obtained (Fig. 4B ). This result clearly shows that E (t) is not instantaneously related to Cp (t). What then is the P K / P D relationship?
3. An ef fect c o m p a r t m e n t model for S i S 2 0 1 - 9 9 5
The dose-dependent hysteresis behavior ex- hibited in Fig. 4B is often seen in pharmaco- dynamic analysis [8] and suggests that a time delay or equilibration process exists between the instantaneous plasma level and the effect it produces. To account for such behavior, Shei- ner et al. introduced the phenomenological "ef- fect compartment" model [9]. As schematized in Fig. 5, the local concentration in the effect c o m p a r t m e n t C e ( t) is driven by the plasma drug level Cp (t), according to the equation:
dCe = k leCp( t ) -keo Ce(t) (2) dt
By convention kle is set equal to ke0 (the elim- ination rate constant of the effect compart- ment) so that under conditions when Cp(t) is constant, Ce(t) will approach the same value exponentially with an equilibration half-life
(kle) I _ _
C e ( t )
keo
CENTRAL COMPARTMENT
EFFECT COMPARTMENT , ~ E m o x
E ~ - • - 4 l , E ( t )
Ceso Ce
Fig. 5. Schematic illustration of the effect compartment model introduced by Sheiner et al. [9]. Four parameters (keo, Em~, Ce~o and n) determine linkage between phar- macokinetics Cp (t) and pharmacodynamics E (t). See text for explanation.

348
10.0
8 . 0
E 6.0"
~ 4 . 0 - L.)
\
( D
2 . 0 -
.0 .0
10.0
PK SIMULATION
I I 2.0 4.a 6:0 8:0
~ime(hr}
I I 10.0 12.0 1,4.0
8.0"
6 . 0
4 , 0 -
2.0-
.O .0
EFFECT CONCENTRATIONS
Dose (meg)
200 100
: I I I t 2.0 4.0 e.o s.o m.o 12.o 14.o
time(hr}
I , I
0 ! I | PD FIT
-20 711 5~
-6o " O
-s0.t \ "--2 ~ o=~...~.---~,~
.0 2.0 4.0 6.0 8.0 10.0 12.0 14.0
~lme(hr}
t 0 , , , ,
-20
-40
-60 •
-SO •
-100
E vs C e
I I I I .50 1.00 1.50 2.00 2.50
Ce (nQ/ml)
Fig. 6. Effect compartment model of growth hormone suppression by S M S 201-995 in acromegalic patients. Upper right panel shows pharmacodynamic data of Fig. 4A fit by theoretical curves using only three free parameters (keo=0.217 h -1, Ceso = 0.241 ng/ml and n -- 1.19; Emax was fixed a priori at - 100% ). Upper left panel illustrates pharmacokinetic simulations in central compartment Cp ( t ). Lower left panel shows inferred time dependence of the local concentration Ce (t) in the effect compartment. Lower right panel shows the inferred relationship between E and Ce. Experimental effect data at all three doses are plotted versus the computed Ce values to show self-consistency. Arrows indicate the intermediate steps linking pharmacokinetics Cp ( t ) and pharmacodynamics E (t) .
given by ln2/keo. The effect of E (t) is assumed to be instantaneously related to Ce(t) (rather than Cp (t)) in accordance with the non-linear Hill equation [8, 9]:
c~ E=EmaxC25o +C2 (3)
where Ema x is the maximum possible effect, Ceso represents the Ce value at which the half-max- imal effect is observed and n is the sigmoidicity parameter which determines the curvature of the E vs. C~ relationship. The time dependence of C~(t) and E(t) has been omitted from eqn. (3) to reflect the time-invariant nature of the
relationship. Together eqns. (2) and (3) imply that four parameters (keo, Em~x, Ceso and n) de- termine the linkage between Cp (t) and E(t).
In applying the effect compartment model to the data of Wass et al., we have fixed the value of E . . . . a priori, to be -100% (i.e. complete suppression of GH secretion) and performed a simultaneous three-parameter fit (keo, C~5o and n) to the E(t) data obtained at all three doses. The simultaneous curve fitting was accom- plished using the MINSQ non-linear regression program. As seen in Fig. 6, a good fit to the E (t) data was obtained at each dose using a single set of parameters: keo-- 0.217 _+ 0.02 h -1,

Emax= - 100% (fixed), Ce5o=0.241 +_ 0.018 ng/ ml and n = 1.19 +0.10. Also shown in Fig. 6 are the Cp(t) simulations (obtained from the PK model of Fig. 3), the derived Ce (t) profiles, and the inferred relationship between E and Ce, in which the experimental E (t) values at each dose have also been plotted. These self-consistent results demonstrate the utility of the effect compartment model for representing the PK/
349
PD interrelationship of SMS 201-995 and GH secretion in acromegaly.
4. Continuous VSl intermittent subcutaneous administration: the optimal input function for S M S 2 0 1 - 9 9 5
In a truly innovative study, Christensen et al. [7] compared the pharmacokinetics and phar- macodynamics (GH suppression) of SMS 201-
Simulation I:
L60~
,2o / c p
.80
0
~ime(hr)
o
-20
-40
-60
-8O •
-130 .0
T.I.D. /
C.S.I.
42 6~ J.0 EI~ 2/.0 2 ,2 ~ime(hr]
Simulation 2:
L60
I.,9.0-
~ .80 -
.40 -
= i 4.0 82 I22 15.0 20.0 2~..0
~im~Chr]
0"
-80
-=.o ,S & ~.o ,~ Ao ~,.o time,rhr)
Fig. 7. Pharmacokinetic (PK) and pharmacodynamic (PD) simulations of the study of Christensen et al. of acromegalic patients [ 7 ], comparing continuous subcutaneous infusion (C.S.I.) of SMS 201-995 vs. three SC injections per day (T.I.D.), both regimens at a daily dose of 100 pg/day. In all simulations, PK parameters were those deduced from healthy subjects (see Fig. 3). In Simulation 1, PD parameters (keo = 0.217 h - 1, Emax = - 100%, Ces0-- 0.241 ng/ml and n- - 1.19) are those derived from the analysis of the study of Wass et al. [5]. Left panel illustrates Cp(t) and Ce(t) profiles for T.I.D. regimen (solid curves), and for C.S.I. (dashed line). Right panel illustrates E(t) for both regimens. In Simulation 2, PD parameters are the same as in Simulation 1 except for keo which is increased to 0.5 h - 1. Note the increased fluctuation of Ca (t) and E (t) for T.I.D. regimen.

Ce(ng/ml}
Effect vs. Ce:
o
-20 ~ n = 4
n=l . 1 9 n=1 .19
o t~o L 0 2 O0 2 0
Simulation 3A:
% L~ -EO
-80
Simulation 3B:
-100 2 413 A2 8 2 t2O 160 O0
T.I.D.
~ime(hr]
o
-20
-40
~ ~ 0 -
- 8 0
- 100 .O
350
time(hr]
Fig. 8. Influence of sigmoidicity parameter, n, on PD simulations of the study of Christensen et al. [7]. Upper panel shows dependence of E vs. Ce for n = 1.19 (Simulations 1, 2) and 4 (Simulations 3A, 3B) at constant values o f E m ~ = - 100% and Ceso = 0.241 ng/ml. Both curves are marked at Ce value corresponding to the C.S.I. regimen. In PD Simulations 3A and 3B, parameters are the same as in Simulations 1 and 2, respectively, with the exception that n equals 4. Note the considerable fluctuation of E (t) with the T.I.D. regimen compared to C.S.I.
995 administered to acromegalic patients via two regimens, first using a portable pump to de- liver a continuous subcutaneous infusion (C.S.I.) and second in three daily SC injections (T.I.D.). Both regimens provided the same daily dose of SMS 201-995, i.e. 100 #g/day. The pharmacodynamic results showed [7] a more constant and complete lowering of the GH lev- els with C.S.I. than with the T.I.D. regimen. In some subjects, GH levels returned to near basal levels prior to each SC injection.
We have tried to simulate the experiment of Christensen et al. using the previously defined
PK and PD models. The PK parameters de- rived from Kutz's study (see Fig. 3) were uti- lized in all simulations. In Simulation 1 [Fig. 7 (upper panel) ], the PD parameters are identi- cal to those deduced from the data of Wass et al. For the T.I.D. regimen, Cp (t) and Ce (t) show marked fluctuation about the constant plasma level of ~ 0.43 ng/ml obtained with the C.S.I. regimen. Correspondingly, E(t) fluctuates be- tween - 5 0 and - 7 3 % for the T.I.D. regimen and remains constant at - 6 7 % for the C.S.I. regimen. This behavior is similar to that shown by some of Christensen's patients but the fluc-

Input
PK
PD
2000
l
1ooo
5O
45
40
I 3s ~ 30
~ 25
~ 20
15
io
5
I ~g/rnin [ ] 1040
120
110
100 ~
9O N
80
I0 ZO 30 40 SO 60 70 80 90 I00 liO 120 MINUTES
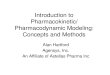
Fig. 9. Steady-state pharmacokinetics (PK) and pharma- codynamics (PD) of the gonadotropin-releasing hormone (GnRH) measured in a rhesus monkey given a pulsatile IV input of GnRH at a rate of 1 pg /min for 6 min every hour. The PD effect corresponds to the pulsatile secretion of LH and FSH by the pituitary which results in a sawtooth plasma level profile of both gonadotropins. Reprinted from E. Knobil [2] with the kind permission of Academic Press, Inc., and the author.
tuations are not as extreme as others [7]. To allow for the intersubject differences between the two studies, we examined other perturba- tions of the PD parameters. In Simulation 2 [Fig 7 (lower panel) ], the equilibration param- eter ke0 was increased to 0.5 h-1. This greatly increased the amplitude of the Ce(t) and E(t) fluctuations for the T.I.D. regimen without af- fecting the C.S.I. results. Finally in Simula-
351
tions 3A and 3B (Fig. 8), the sigmoidicity pa- rameter, n, was increased from 1.19 (the value derived from the study by Wass et al.) to 4, and keo was varied from 0.217 to 0.5 h -1. As seen in Fig. 8 (upper panel), increasing n leads to a steeper dependence of E on Ce, without chang- ing Ceso. The effect on E(t) [Fig. 8 (lower panel) ] is a deeper suppression with C.S.I. and a greater fluctuation with the T.I.D. regimen. For simulation 3B (keo = 0.5 h - 1 ), E (t) nearly returns to zero prior to each dose of the T.I.D. regimen. Collectively, these simulations dem- onstrate the range of responses seen among Christensen's patients [7] and show that such behavior is consistent with an effect compart- ment model.
Furthermore, both experiment and theory il- lustrate that continuous infusion of SMS 201- 995 can maintain the local effect concentration at the necessary level (i.e. about twice Ceso ~ 0.4 ng/ml) in the most efficient manner. In this regard, recent long-term studies by Ducasse et al. [10] have shown that continuous infusion of SMS 201-995 for up to one year has resulted in sustained GH suppression and the actual shrinkage of a pituitary tumor in an acrome- galic patient. This indicates that no down-reg- ulation had occurred during the prolonged zero- order input of SMS 201-995.
b. GnRH: Dependence of LH, FSH secretion on the GnRH input function
GnRH (LHRH) is a decapeptide hormone secreted by the hypothalamus to physiologi- cally stimulate LH and FSH secretion by the pituitary. In a series of landmark studies, Kno- bil and co-workers systematically investigated [2] the pharmacokinetics of GnRH and phar- macodynamics of LH and FSH secretion in re- sponse to various input regimens of GnRH, ad- ministered by a programmable intravenous infusion pump to rhesus monkeys with no en- dogenous GnRH production. In these animals, GnRH production had been abolished by pro- ducing a radiofrequency lesion in the medial basal hypothalamus; in addition, some of the

352
A 3 5
zo
I Pulse/~ur S Pulses/hour
15
1039 I ~lse / hour
I0 5 0 5 iO 15 20 25 30 35 ~YS
,~ ~=
B I
25
20
15
lO
5
I ~cJ / ra in 0.1 ~¢J / ra in
999
200 l
L51~ "='-
I00 ~ N
50 ~
15 13 II 9 7 5 3 I 0 1 3 5 7 9 It DAYS
C
I
:c
999 Pulsahle COnhnuOus Puhlatill
IO 15 20 25 30 ]S DAYS
,s0 l
v
Fig. 10. Influence of the GnRH input function on the pharmacodynamics of LH and FSH secretion in a rhesus monkey. (A) GnRH pulse frequency is varied from 1 pulse/h to 5 pulses/h and back again (at constant pulse amplitude 1 ttg/min and duration 6 min). Note fall in LH and FSH levels at high frequency. (B) GnRH pulse amplitude is decreased from 1 #g/min to 0.1 ttg/min (at constant pulse frequency 1/h and duration 6 rain). (C) A pulsatile input function (1 pulse/h) is changed to continuous input and back again (at constant input rate of 1 ~g/min). Each panel represents the results of an individual monkey. Panels A and B reprinted from E. Knobil [2] with the kind permission of Academic Press, Inc., and the author. Panel C reprinted from P.E. Belchetz et al., Science, vol. 202, pp. 631-633 (1978), with permission of publisher and author (copyright 1979 by the AAAS).

monkeys had been ovariectomized. Although these studies were undertaken to investigate the physiological mechanisms involved in the neu- roendocrine control of the menstrual cycle, they nevertheless illustrate one of the most system- atic studies of the interrelationships between i(t), PK and PD carried out thus far with a polypeptide hormone.
1. Pulsatile input functions While continuous infusion of GnRH pro-
duces transient increases in LH and FSH (last- ing a few hours), a sustained physiological in- crease in the gonadotropin levels occurs only when GnRH is administered at a rate of about 1 #g /min in short (6 min) pulses given every hour [2]. As seen in Fig. 9, the steady-state PK profile from such an input function consists of GnRH spikes which decay rapidly to zero prior to each pulse. In contrast, the steady-state PD profiles of LH and FSH have saw-tooth pat- terns reflecting the GnRH spike-driven secre- tion of each gonadotropin. The fact that the de- gree of plasma level fluctuation of LH and FSH is much smaller than for GnRH is apparently due to the longer half-lives of LH and FSH.
When the frequency of GnRH pulses was in- creased from I per hour to 5 per hour, LH and FSH levels decreased over 10 to 20 days to non- detectable levels, and slowly increased to the previous levels when the pulse frequency was returned to I per hour (Fig. 10A). Conversely, when the pulse frequency was decreased to 1 per 3 hours (data not shown) the FSH level de- creased 50%, but the LH level increased by about 2-fold [2]. Such effects were also reversible.
At constant pulse frequency (1 per hour) variations in pulse amplitude also affect the PD response. As seen in Fig. 10B, decreasing the amplitude from 1 #g /min to 0.1/~g/min led to a suppression of gonadotropin levels within 5 days. Increasing the amplitude to 10 #g /min (data not shown) had no effect on LH but pro- duced a 50% decrease in FSH after 10 days [2 ].
Most interestingly, Knobil showed that when
353
GnRH was administered in 6-min pulses to a pre-pubertal monkey at a frequency of 1 per hour and amplitude of 1 #g/rain (for 6 min), spontaneous ovulation and menstrual cycles occurred during 100 days, and ceased upon ter- minating the pulsatile GnRH infusion [2 ]. On the basis of these studies it was concluded that hypothalamic control of the menstrual cycle consists of a "metronome-like" release of GnRH at a frequency of about 1 per hour, and a well- defined pulse amplitude. In certain human fer- tility disorders (in both male and female), pul- satile administration of LHRH, using SC or IV infusions, has also been shown to stimulate normal gonadotropin release and establish nor- mal reproductive function [11].
2. Continuous input functions In contrast to pulsatile input, continuous in-
put of GnRH causes only a transient secretion of LH and FSH, and after a period of 10-20 days results in complete (reversible) suppression of gonadotropin secretion (Fig. 10C). This occurs at an input rate of I #g /min as well as at lower input rates, and is now recognized as the para- doxical gonadotropin inhibition seen with con- tinuous GnRH input [12] and also with high affinity GnRH agonist analogues [13]. Clini- cally, these suppressive effects are useful in the t reatment of precocious puberty, prostate and breast cancer, endometriosis and other endo- crine disorders where the effects resulting from gonadotropin stimulation are unwanted [ 13 ].
3. Toward a quantitative model of GnRH action
The observation that high frequency or con- tinuous GnRH input leads to the eventual suppression of LH and FSH secretion in the monkey and other species has been regarded in qualitative terms as a down-regulation phe- nomenon wherein the pituitary gland "de- fends" itself against excessive stimulation by GnRH [2,14].
Biochemically, down-regulation may result from a reduction in the number (concentra-

354
A
EFFECT ~ ~ / LH, FSH
SECRETION
.. . . . . . Ce(GnRH ) ......... ~.~
GnRH Receptors down
r up
0 j TFR0
C k - - - - - - ~ ~------ Nrnox ~ low TFRO
[><.._ NR(t)
[- . . . . . . . . ~ N rni n --high TFRO
t t In2/k R
Fig. 11. Heuristic concepts used to model the action of GnRH on gonadotropin secretion. (A) Relationship be- tween effect (LH and FSI-I secretion) and the instanta- neous concentration of GnRH, Ce (t), in the pituitary effect compartment. Different curves reflects down- and up-reg- ulation of GnRI-I receptors, as indicated by vertical arrows. (B) Postulated relationship between the production rate of GnRH receptors and the time-averaged fractional GnRH receptor occupancy (TFRO). (C) Time dependence of the number of GnRH receptors, NR (t), as the production rate changes from Pmax to Pmin (and vice versa) due to varia- tions in TFRO. The equilibration half-life for such transi- tions is given by ln2/kR, where kR is the clearance rate of GnRH receptors (see text for details).
tion) of pituitary GnRH receptors, and/or re- ductions in the concentration of effector mole- cules which mediate the cellular effects (e.g. LH and FSH secretion) of GnRH interaction with its receptor [ 14 ]. Although there is experimen- tal evidence to support both types of biochem- ical mechanisms in the GnRH system [ 14,15 ], we will assume for simplicity that down-regu- lation and its restoration (up-regulation) re- sults from a modulation in the number of GnRH
receptors expressed by the pituitary gland in re- sponse to different patterns of GnRH input. In principle, the same feedback mechanisms pro- posed in our model could be applied equally well to the modulation of effector molecules.
As illustrated in Fig. l lA, the relationship between effect (LH/FSH secretion) and the local concentration (Ce) of GnRH at the pitui- tary (the presumed effect compartment) is de- scribed in our model by a family of sigmoidal curves, where the Emax levels parallel the num- ber of GnRH receptors. On a time scale of min- utes to hours, a single E vs. Ce curve determines the secretory response to variations in the local GnRH concentration. However, on a time scale of 5 to 10 days, during which time down- or up- regulation occurs in the monkey [ 2 ], the E vs. Ce curves shift over time, thus accounting for the long-term response to a given GnRH input function.
To account phenomenologically for the prin- cipal features of GnRH action, we postulate that the key feedback variable controlling the recep- tor number is the time-averaged fractional re- ceptor occupancy (TFRO), which is defined in terms of the following equilibrium:
K R + GnRH ~ R" GnRH (4)
where R is an unoccupied GnRH receptor and K is the equilibrium binding constant. TFRO is related to the concentration of R, GnRH and R" GnRH by:
( [R-GnRH] ) (5) TFRO= [R] + [R.GnRH] t i m e avg.
Using the law of mass action and assuming that the local concentration of GnRH, Ce(t), ap- proximates the unbound GnRH concentration, TFRO can be expressed as:
[ gCe(t) TFRO ~ L 1 ~-~ ~ee ~t) )time avg" (6)
This result shows that TFRO will range be- tween zero (when Ce(t) is much smaller than

K - 1 ) and one (when Ce (t) is much greater than K -1). Furthermore, through the time depen- dence of Ce(t), TFRO will be sensitive to both the amplitude and frequency of the GnRH in- put function. Interestingly, TFRO will be in- dependent of the absolute number of GnRH re- ceptors, so long as there are at least some receptors present to determine the fractional occupancy.
As a feedback variable, we postulate that TFRO will modulate the instantaneous pro- duction rate PR of GnRH receptors in accord- ance with the sigmoidal relationship depicted qualitatively in Fig. l lB . At low TFRO, PR will approach the maximal production rate, Pmax, whereas at high TFRO, PR will fall to the min- imum production rate Pmin. By modulating PR the number of GnRH receptors expressed by the pituitary, NR (t), will vary according to the fol- lowing receptor population kinetic equation:
dNR~ = PR -- kR NR ( t ) (7)
where kR is a first-order rate constant reflecting the clearance of GnRH receptors by the pitui- tary. The consequences of equation [ 7 ] are de- picted in Fig. 11C, which shows the time depen- dence of Na (t) as PR changes from/)max to Pmin and vice versa. As TFRO varies between 0 and 1 (as a consequence of changing the GnRH in- put function) NR(t) will establish a new level (Nr~ax or N~n) with an equilibration half-life given by ln2/kR. The steady-state values of Nm~ and Nmnin are simply given by Pm~/kR and PmiJ kR, respectively. In the case of the rhesus mon- key, the equilibration half-life is on the order of 5-10 days as seen from the kinetics of LH and FSH secretion associated with varying the fre- quency of pulsatile input (Fig. 10A) and the transitions between pulsatile and continuous input (Fig. 10C).
Collectively, the heuristic concepts repre- sented in Figs. l lA, B, C provide the starting point for a quantitative, mechanistic under- standing of the complex linkage between the GnRH input function and its pharmacodyn-
355
amic effects. Although Smith's earlier mathe- matical model of LH secretion is noteworthy [16], it preceded the publications of Knobil's group and did not consider the down-regulation phenomenon per se. In future work, we intend to present a complete quantitative model of the GnRH system based on the above concepts that will fully account for such pharmacologically important phenomena.
CONCLUSIONS
The two examples provided by SMS 201-995 and GnRH show that the optimal input func- tion needed in polypeptide delivery is specific to each drug and may even depend on the ther- apeutic indication itself. For SMS 201-995 a continuous (zero-order) input function has been shown to be the most efficacious way to deliver SMS 201-995 in the t reatment of acro- megaly. Furthermore, the continuous infusion of SMS 201-995 for periods up to one year has not been observed to produce down-regulation [10]. Conversely, in the case of GnRH, a pul- satile input function of a defined frequency and amplitude is necessary to stimulate the pitui- tary secretion of LH and FSH in man [11 ] and other species [2], whereas the continuous in- put of GnRH leads to a paradoxical suppression of gonadotropin secretion [2,12]. Both actions of GnRH, as determined by the input function, are of use clinically [ 13 ].
The cited studies also illustrate the type of novel experimental approaches that are needed for investigating the relationship between the pharmacokinetics and pharmacodynamics of polypeptides and for experimentally defining the optimal input function. In general, such work requires the use of programmable infu- sion pumps that deliver drug intravenously or subcutaneously at various rates and wave forms.
Finally, we have shown how mathematical models such as the effect compartment model [8,9] and novel extensions which account for receptor occupancy and modulation can be used

356
to e lucidate t he i n t e r r e l a t i onsh ip s b e t w e e n the i npu t func t ion a n d the t i m e course of t he p h a r - m a c o k i n e t i c a n d p h a r m a c o d y n a m i c responses . Such models no t on ly p rov ide ins igh t in to the p h a r m a c o l o g y of the drug b u t can also be useful as s imu la t ion tools for def in ing the o p t i m a l in- p u t funct ion .
As the ava i lab le n u m b e r o f p o l y p e p t i d e drugs increases in t he future , s imi la r i nnova t i ve ap- p roaches , as i l lus t ra ted here, will be needed to e x p e r i m e n t a l l y a n d theore t i ca l ly def ine the op- t ima l i npu t func t ion requ i red for each com- pound . B y these effor ts , t he se lec t ion a n d de- v e l o p m e n t of a p p r o p r i a t e de l ivery s y s t e m s for po lypep t ides (i.e. rou tes of a d m i n i s t r a t i o n a n d p h a r m a c e u t i c a l t echno log ies ) can be p l aced on a r a t i ona l a n d q u a n t i t a t i v e basis .
ACKNOWLEDGEMENTS
T h e a u t h o r wishes to t h a n k the confe rence organizers for t he o p p o r t u n i t y to p r e s e n t th i s paper , and gra te fu l ly acknowledges t he s u p p o r t o f p a s t a n d p r e s e n t col leagues in the develop- m e n t of th is work. T h i s p a p e r is ded ica ted to P ro fe s so r E r n s t K n o b i l a n d his col leagues.
REFERENCES
1 J. Pless, W. Bauer, U. Briner, W. Doepfner, P. Mar- bach, R. Maurer, T.J. Petcher, J.-C. Reubi and J. Von- derscher, Chemistry and pharmacology of SMS 201- 995, a long-acting octapeptide analogue of somatos- tatin, Scand. J. Gastroenterol., 21, suppl. 119 (1986) 54-64.
2 E. Knobil, The neuroendocrine control of the men- strual cycle, Recent Prog. Horm. Res. 36 (1980) 53- 88.
3 S.W.J. Lamberts, A guide to the clinical use of the so- matostatin analogue SMS 201-995 (Sandostatin), Acta Endocrinol., (Copenh.), Suppl. 286 (1987) 54- 66.
4 K. Kutz, E. Nuesch and J. Rosenthaler, Pharmacoki- netics of SMS 201-995 in healthy subjects, Scand. J. Gastroenterol., 21, Suppl. 119 (1986) 65-72.
5 J.A.H. Wass, N. Lytras and G.M. Besser, Somatosta- tin octapeptide (SMS 201-995) in the medical treat- ment of acromegaly, Scand. J. Gastroenterol., 21, suppl. 119 (1986) 136-140.
6 W.H. Daughaday, The adenohypophysis, in: R.H. Williams (Ed.), Textbook of Endocrinology 5th edn., W.B. Saunders, Philadelphia, PA, 1974, Chap. 2, pp. 31-77.
7 S.E. Christensen, J. Weeke, H. Orskov, N. Moller, A. Flyvbjerg, A.G. Harris, E. Lund and J. Jorgensen, Continuous subcutaneous pump infusion of somatos- tatin analogue SMS 201-995 versus subcutaneous in- jection schedule in acromegalic patients, Clin. Endo- crinol., 27 (1987) 297-306.
8 N.H.G. Holford and L.B. Sheiner, Understanding the dose-effect relationship: Clinical application of phar- macokinetic-pharmacodynamic models, Clin. Phar- macokin., 6 (1981) 429-453.
9 L.B. Sheiner, D.R. Stanski, S. Vozeh, R.D. Miller and J. Ham, Simultaneous modeling of pharmacokinetics and pharmacodynamics: Application to d-tubocurar- ine, Clin. Pharmacol. Ther., 25 (1979) 358-371.
10 M.C.R. Ducasse, J.P. Tauber, A. Tourre, A. Bonafe, Th. Babin, M.T. Tauber, A.G. Harris and F. Bayard, Shrinking of a growth hormone-producing pituitary tumor by continuous subcutaneous infusion of the so- matostatin analog SMS 201-995, J. Clin. Endocrinol. Metab., 65 (1987) 1042-1046.
11 N. Santoro, M. Filicori and W.F. Crowley, Jr., Hypo- gonadotropic disorders in men and women: diagnosis and therapy with pulsatile gonadotropin-releasing hormone, Endocrinol. Rev., 7 (1986) 11-23.
12 D. Rabin and L.W. McNeil, Pituitary and gonadal de- sensitization after continuous luteinizing hormone- releasing hormone infusion in normal females, J. Clin. Endocrinol. Metab., 51 (180) 873-876.
13 B.H. Vickery, Comparison of the potential for thera- peutic utilities with gonadotropin-releasing hormone agonists and antagonists, Endocrinol. Rev., 7 (1986) 115-124.
14 R.N. Clayton, Pharmacological regulation of pituitary LHRH receptors, in: B.H. Vickery et al. (Eds.), LHRH and Its Analogs: Contraceptive and Therapeutic Ap- plications, MTP Press Ltd., Lancaster, PA, 1982, Chap. 2, pp. 35-46.
15 P.M. Conn, W.R. Huckle, W.V. Andrews and C.A. McArdle, The molecular mechanism of action of go- nadotropin releasing hormone (GnRH) in the pitui- tary, Recent Prog. Horm. Res., 43 (1987) 29-68.
16 W.R. Smith, Hypothalamic regulation of pituitary se- cretion of luteinizing hormone. II. Feedback control of gonadotropin secretion, Bull. Math. Biol., 42 (1980) 55-78.