Embed Size (px)
Citation preview

Pharmacogenomics: Pharmacogenomics: Clinical Application and Clinical Application and
Effects on Drug Effects on Drug
MetabolismMetabolism Rodney J. Hunter, Pharm.D.Rodney J. Hunter, Pharm.D.
Assistant ProfessorAssistant ProfessorTexas Southern University College of Pharmacy and Texas Southern University College of Pharmacy and
Health SciencesHealth SciencesSNPhA Regional Conference District III, IV, & VSNPhA Regional Conference District III, IV, & V
February 19February 19thth, 2011, 2011
Financial DisclosureFinancial Disclosure
I have no conflicts of interest in I have no conflicts of interest in regards to this program regards to this program
“Why genetic polymorphisms? Why pharmacogenomics and oncology? Why so much excitement in this field?”

ObjectivesObjectives
Describe pharmacogenomics and the clinical Describe pharmacogenomics and the clinical relevance of this field of study in relation to relevance of this field of study in relation to oncologyoncology
Outline the drug metabolism pathways Outline the drug metabolism pathways affected by pharmacogenomic abnormalities affected by pharmacogenomic abnormalities in the oncology patient populationin the oncology patient population
Identify the different drug classes and Identify the different drug classes and significant adverse drug effects associated significant adverse drug effects associated with pharmacogenomic changes in the with pharmacogenomic changes in the oncology patient populationoncology patient population
Human Genome ProjectHuman Genome Project
Begun in 1990 with an expected Begun in 1990 with an expected completion date of 2005, it was completion date of 2005, it was completed in 2003 due to advances in completed in 2003 due to advances in technologytechnology
Set out to map the 20,000-25,000 Set out to map the 20,000-25,000 human geneshuman genes
3 billion DNA bases3 billion DNA bases
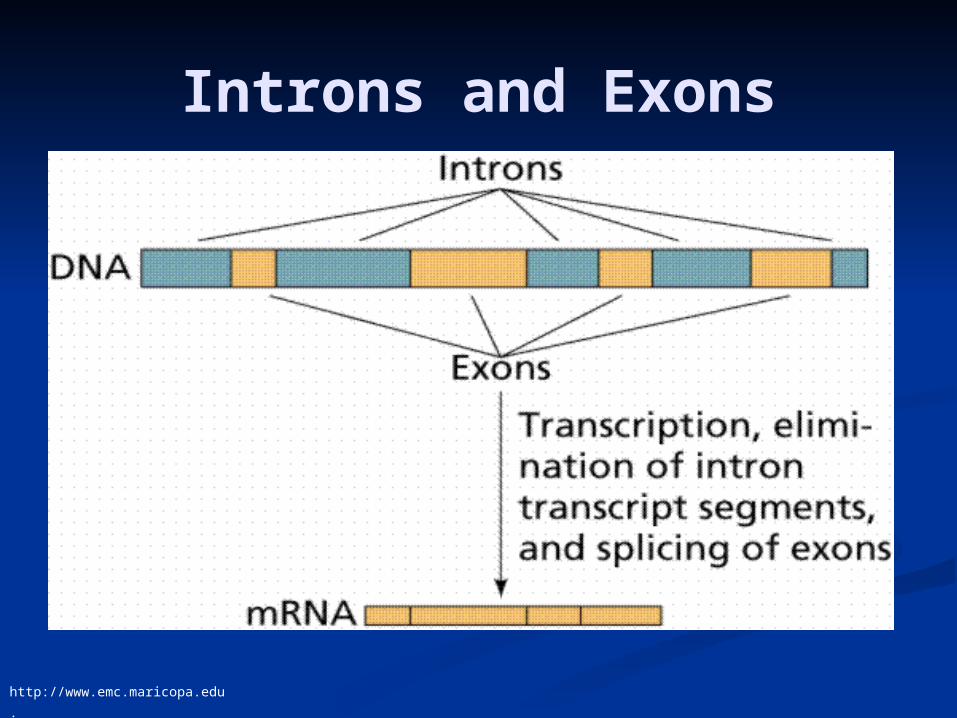
Introns and Exons
http://www.emc.maricopa.edu
.
Genetic PolymorphismsGenetic Polymorphisms
Single Nucleotide Polymorphism Single Nucleotide Polymorphism (SNPs)(SNPs) 1/1000 base pairs 1/1000 base pairs
Types of SNPsTypes of SNPs Insertion-DeletionInsertion-Deletion Tandem repeatsTandem repeats Frameshift mutationFrameshift mutation Defective splicingDefective splicing Aberrant splice siteAberrant splice site Premature stop codonPremature stop codon
Dipiro JT, Talbert RL, et al. Pharmacotherapy 7th ed. 2008;6:31-45.

Rationale for Rationale for PharmacogenomicsPharmacogenomics
Meta-analysis estimated ~2 Meta-analysis estimated ~2 million ADR/yr in the USmillion ADR/yr in the US
ADR accounting for 100,000 ADR accounting for 100,000 deathsdeaths
Cost in 2000 ~$177.4 billionCost in 2000 ~$177.4 billion
Lazarou, J et al JAMA. 1998;279:1200-05.

Goals of Goals of PharmacogenomicsPharmacogenomics
Prevent and predict adverse drug Prevent and predict adverse drug reactionsreactions
Optimize drug therapyOptimize drug therapy
Lead to novel approaches to drug Lead to novel approaches to drug discoverydiscovery

Goals of Goals of PharmacogenomicsPharmacogenomics
Evans WE and Johnson JA. Annu Rev Genomics Hum Genet. 2001;2:9-39.
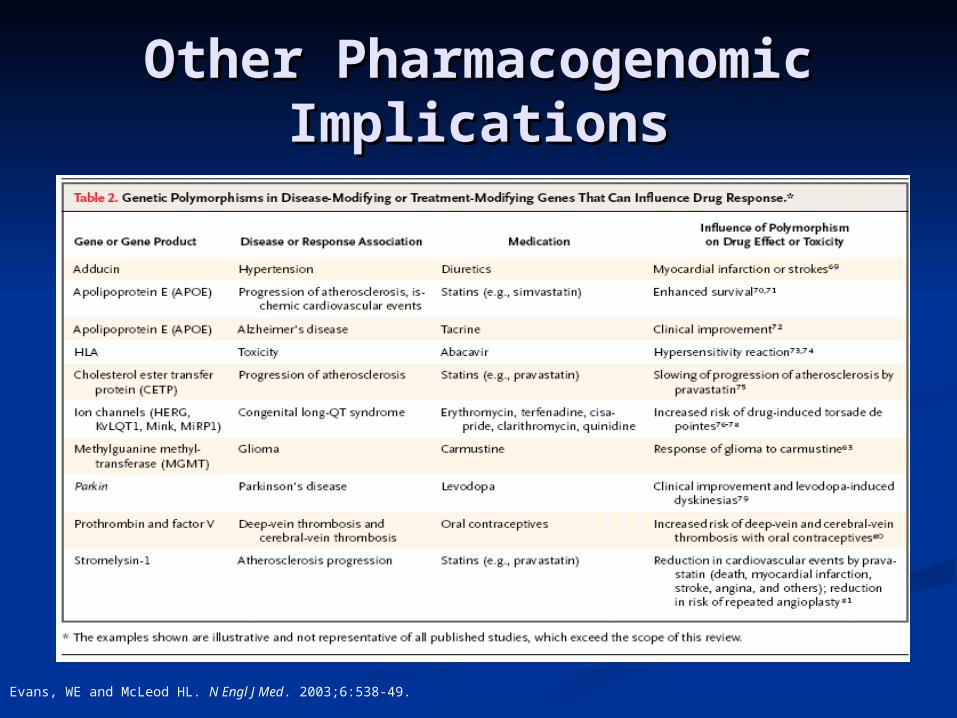
Other Pharmacogenomic Other Pharmacogenomic ImplicationsImplications
Evans, WE and McLeod HL. N Engl J Med. 2003;6:538-49.
Pharmacogenomics in Pharmacogenomics in OncologyOncology
Drug effectsDrug effects Drug metabolismDrug metabolism Drug TargetsDrug Targets Drug Transporters Drug Transporters
Somatic mutations in malignant tissueSomatic mutations in malignant tissue
Narrow therapeutic indexNarrow therapeutic index
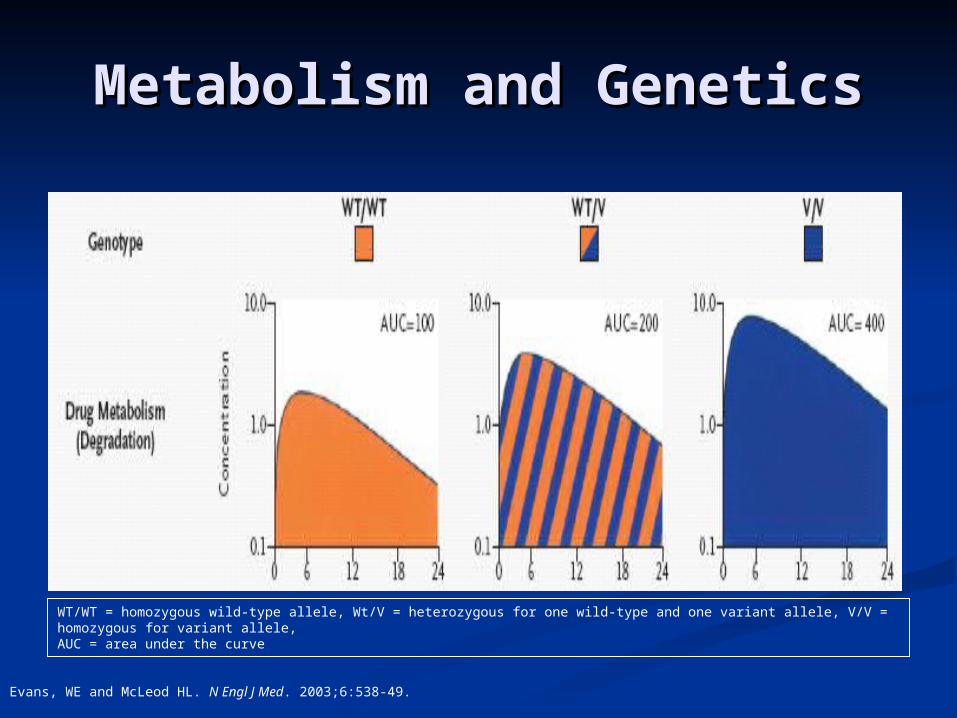
Metabolism and GeneticsMetabolism and Genetics
Evans, WE and McLeod HL. N Engl J Med. 2003;6:538-49.
WT/WT = homozygous wild-type allele, Wt/V = heterozygous for one wild-type and one variant allele, V/V = homozygous for variant allele, AUC = area under the curve
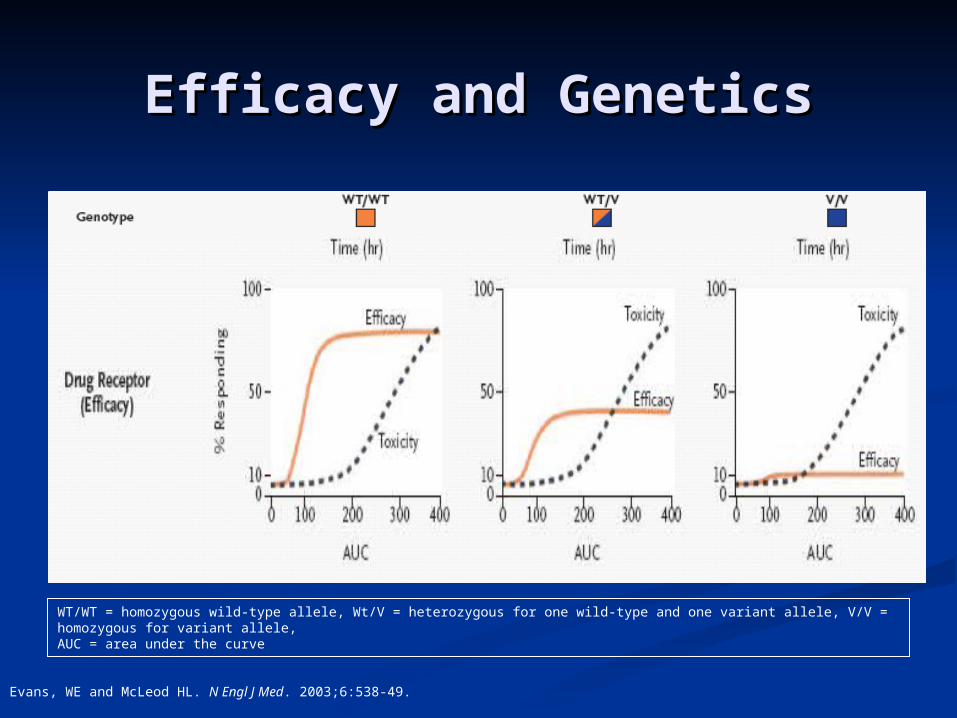
Efficacy and GeneticsEfficacy and Genetics
Evans, WE and McLeod HL. N Engl J Med. 2003;6:538-49.
WT/WT = homozygous wild-type allele, Wt/V = heterozygous for one wild-type and one variant allele, V/V = homozygous for variant allele, AUC = area under the curve
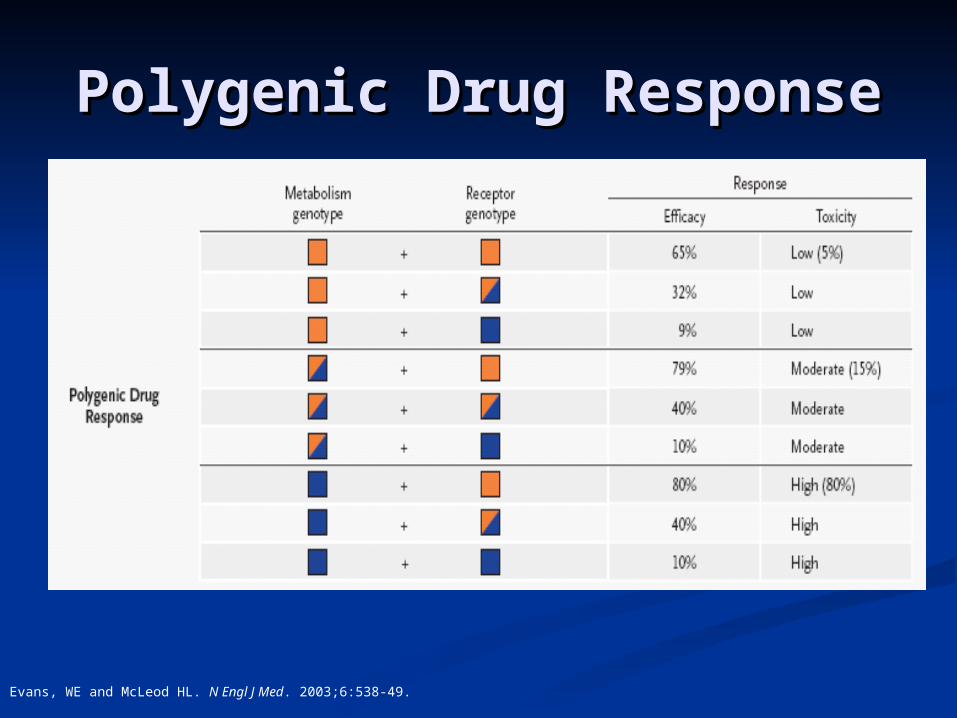
Polygenic Drug ResponsePolygenic Drug Response
Evans, WE and McLeod HL. N Engl J Med. 2003;6:538-49.
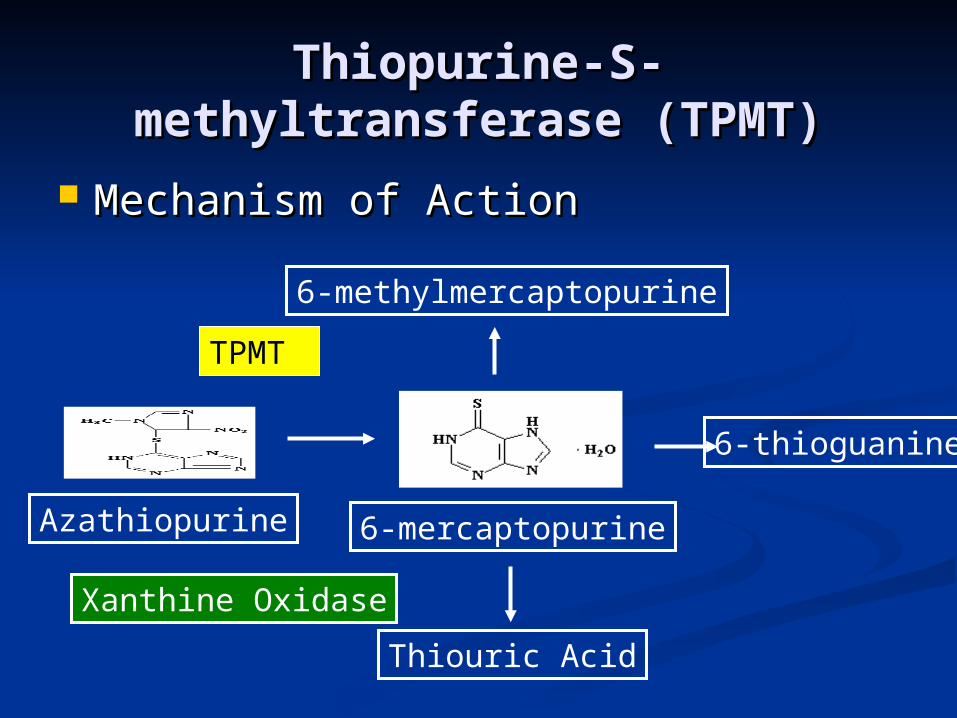
Thiopurine-S-Thiopurine-S-methyltransferase (TPMT)methyltransferase (TPMT)
Mechanism of ActionMechanism of Action
Azathiopurine 6-mercaptopurine
6-thioguanine
6-methylmercaptopurine
Thiouric Acid
TPMT
Xanthine Oxidase
Thiopurine-S-Thiopurine-S-methyltransferase (TPMT)methyltransferase (TPMT)
TPMT deficiencyTPMT deficiency Autosomal codominant genetic Autosomal codominant genetic
polymorphismpolymorphism High TPMT activity is most commonHigh TPMT activity is most common
TMPT*3A and TMPT*3CTMPT*3A and TMPT*3C
Heterozygous phenotypeHeterozygous phenotype Intermediate toleranceIntermediate tolerance
Evans WE, Hon YY, et al. J Clin Oncol. 2001;2293-301.

Patient populationPatient population Patient referred due to excessive Patient referred due to excessive
toxicity secondary to 6-MP or AZAtoxicity secondary to 6-MP or AZA Twenty-three patients evaluatedTwenty-three patients evaluated Hospitalizations, platelet transfusions, Hospitalizations, platelet transfusions,
and missed chemotherapy dosesand missed chemotherapy doses
Genetic TestingGenetic Testing TMPT genotype determined by PCRTMPT genotype determined by PCR
Thiopurine-S-Thiopurine-S-methyltransferase (TPMT)methyltransferase (TPMT)
Evans WE, Hon YY, et al. J Clin Oncol. 2001;2293-301.

Thiopurine-S-Thiopurine-S-methyltransferase (TPMT)methyltransferase (TPMT)
Evans WE, Hon YY, et al. J Clin Oncol. 2001;2293-301.
90%
SummarySummary A dosage reduction of A dosage reduction of 90%90% has benefited has benefited
patients with homozygous TPMT patients with homozygous TPMT deficiencydeficiency
Homozygous TPMT deficient patients Homozygous TPMT deficient patients have a high incidence of hematopoetic have a high incidence of hematopoetic toxicity induced by thiopurinestoxicity induced by thiopurines
Heterozygous patients can tolerate full Heterozygous patients can tolerate full doses in most casesdoses in most cases
Thiopurine-S-Thiopurine-S-methyltransferase (TPMT)methyltransferase (TPMT)

“JP has a homozygous TPMT deficiency, JP’s full dose of 6-MP is 500 mg/m2/week. What dose should JP receive?”

UGT1A1UGT1A1
Mechanism of ActionMechanism of Action
UGT1A1UGT1A1 UGT1A1*28UGT1A1*28
Extra TA dinucleotide promotor Extra TA dinucleotide promotor regionregion
Decreased expression of UGT1A1 Decreased expression of UGT1A1 proteinprotein
Increased risk of irinotecan toxicityIncreased risk of irinotecan toxicity Mainly in homozygous patientsMainly in homozygous patients
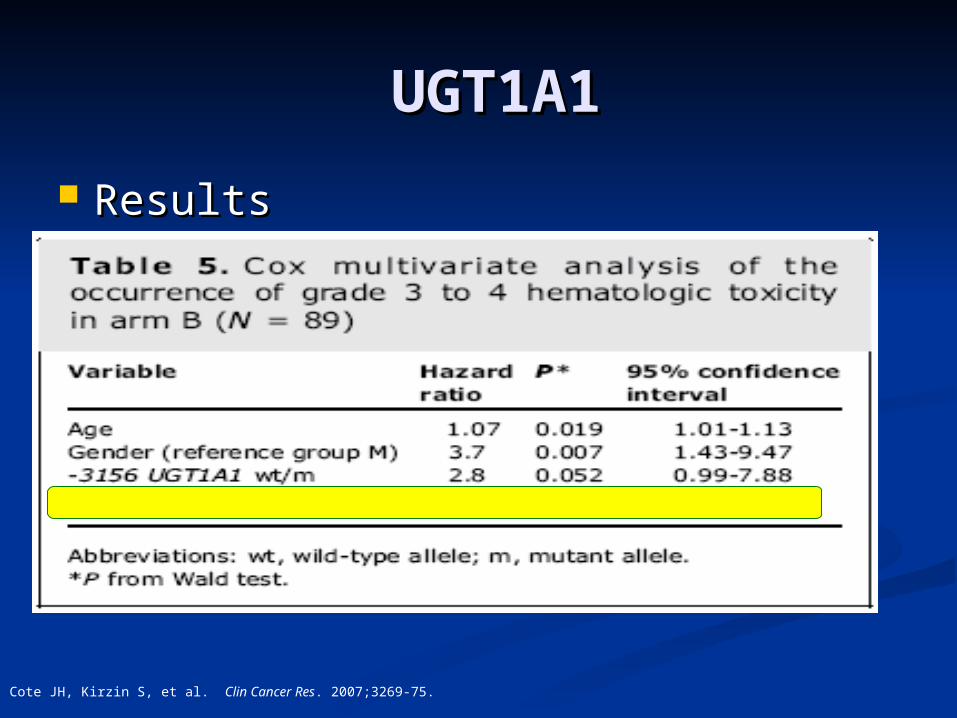
UGT1A1UGT1A1
Cote JH, Kirzin S, et al. Clin Cancer Res. 2007;3269-75.

Patient populationPatient population 400 patients with high-risk stage III colon 400 patients with high-risk stage III colon
cancercancer Patients randomizedPatients randomized
5-fluorouracil/Leucovorin (Arm A) or FOLFIRI 5-fluorouracil/Leucovorin (Arm A) or FOLFIRI (Arm B)(Arm B)
Genetic TestingGenetic Testing DNA from 184 patients was evaluatedDNA from 184 patients was evaluated
UGT1A1, ABCB1, and CYP3A5UGT1A1, ABCB1, and CYP3A5
UGT1A1UGT1A1
Cote JH, Kirzin S, et al. Clin Cancer Res. 2007;3269-75.
UGT1A1UGT1A1
Cote JH, Kirzin S, et al. Clin Cancer Res. 2007;3269-75.
Results Results

UGT1A1UGT1A1
SummarySummary Homozygous patients usually require at Homozygous patients usually require at
least one level dosing reductionleast one level dosing reduction
Heterozygous patients can tolerate normal Heterozygous patients can tolerate normal dosesdoses
Irinotecan screeningIrinotecan screening FDA-approved genotype test (Invader® FDA-approved genotype test (Invader®
Molecular Assay)Molecular Assay)
Cote JH, Kirzin S, et al. Clin Cancer Res. 2007;3269-75.

Dihydropyrimidine dehydrogenase Dihydropyrimidine dehydrogenase
(DPD)(DPD)
Watters JW, McLeod HL. Biochimica et Biophysica Acta 2003 1603; 99–111
Dihydropyrimidine dehydrogenase Dihydropyrimidine dehydrogenase
(DPD)(DPD) DPD deficiencyDPD deficiency
AG to C single nucleotide change on AG to C single nucleotide change on exon 14exon 14
Decreased activity of DPD responsible Decreased activity of DPD responsible for 5-FU breakdownfor 5-FU breakdown
Major SymptomsMajor Symptoms Diarrhea, neutropenia, and neurotoxicityDiarrhea, neutropenia, and neurotoxicity
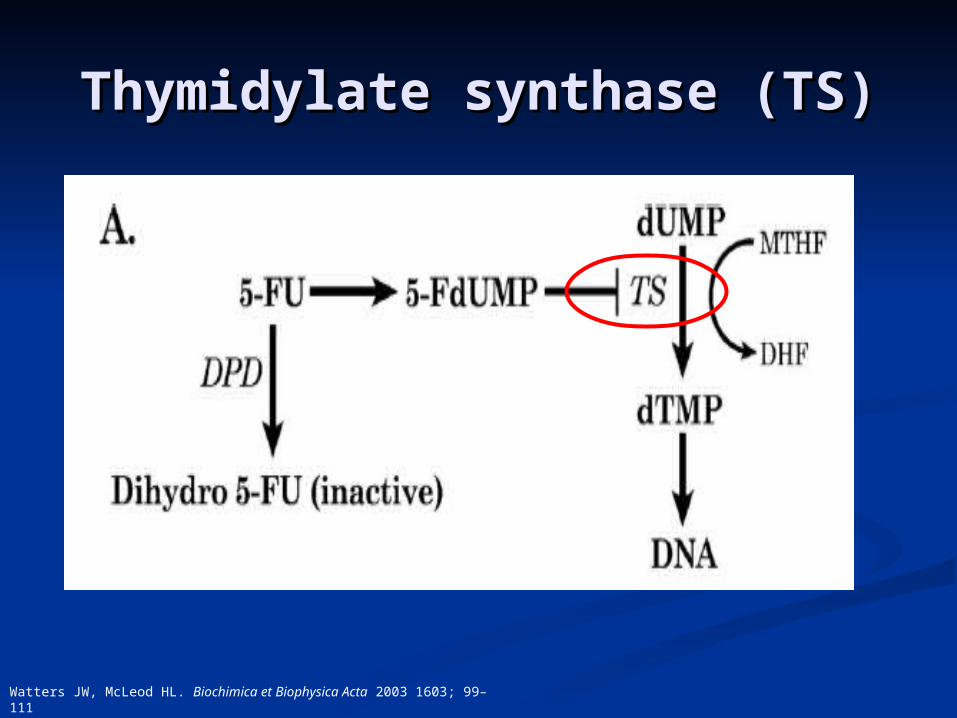
Thymidylate synthase (TS)Thymidylate synthase (TS)
Watters JW, McLeod HL. Biochimica et Biophysica Acta 2003 1603; 99–111
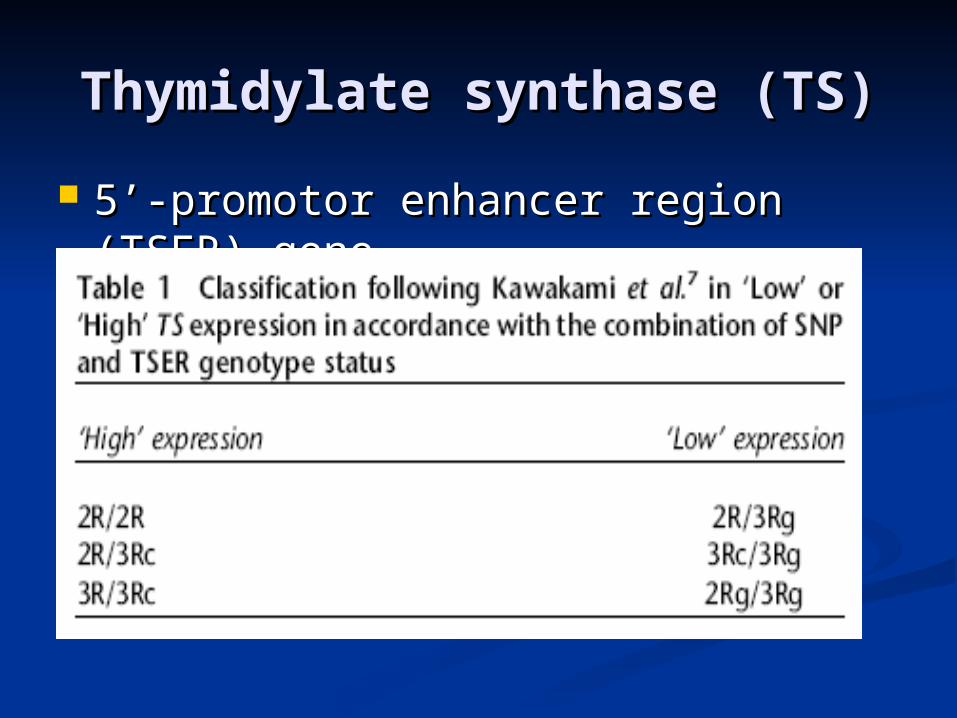
5’-promotor enhancer region (TSER) 5’-promotor enhancer region (TSER) genegene
Thymidylate synthase (TS)Thymidylate synthase (TS)
Methylenetetrahydrofolate Methylenetetrahydrofolate
Reductase (MTHFR)Reductase (MTHFR) Mechanism of action in relation to Mechanism of action in relation to
fluoropyrimidines and antifolatesfluoropyrimidines and antifolates
AntifolatesAntifolates MethotrexateMethotrexate and and pemetrexedpemetrexed
FluoropyrimidinesFluoropyrimidines 5-fluorouracil 5-fluorouracil

Methylenetetrahydrofolate Methylenetetrahydrofolate Reductase (MTHFR)Reductase (MTHFR)
C677T and A1298CC677T and A1298C Caucasian and Asian PopulationCaucasian and Asian Population Possible increase susceptibilityPossible increase susceptibility 5-FU increased activity5-FU increased activity Other implicationsOther implications
Further study mandatedFurther study mandated Folate status and geographic originFolate status and geographic origin
Dezemtje VO, Guchelaar HJ, et al. Annu Rev Clin Cancer Res 2009;15:15-21.

Thymidylate synthase (TS)Thymidylate synthase (TS)
Patient populationPatient population 76 patients initiated on 5-FU therapy76 patients initiated on 5-FU therapy TS, DPD, and MTHFR analyzedTS, DPD, and MTHFR analyzed
Patient Genetic CharacteristicsPatient Genetic Characteristics TS 2R/2R – TS 2R/2R – 18%18%; 2R/3R – ; 2R/3R – 50%50%; 3R/3R - ; 3R/3R -
30%30% MTHFR polymorphisms evenly spreadMTHFR polymorphisms evenly spread DPD deficiency in DPD deficiency in 1.6%1.6%
Capitain O et al. Pharmacogenomics J 2008;6:256-67.
5-FU, Genetics, and Outcome
Advanced colorectal cancer patients Receiving 5-FU (n = 76)
Efficacy TS 3R/3R genotype (log-rank test p =
0.0065)
Toxicity DPD (p = 0.031) MTHFR 1298 A > T (p = 0.0018)
Capitain O et al. Pharmacogenomics J 2008;6:256-67.
SummarySummary Patients with verified homozygous Patients with verified homozygous DPD DPD
deficiencydeficiency should be changed to another should be changed to another treatment regimentreatment regimen
Patients with DPD deficiency develop Patients with DPD deficiency develop significantly earlier than patients with normal significantly earlier than patients with normal DPD activityDPD activity
Increased TS activity linked to poor outcomes Increased TS activity linked to poor outcomes in patients treated with 5-FU and its derivativesin patients treated with 5-FU and its derivatives
5-Fluorouracil (5FU)5-Fluorouracil (5FU)
“Should RS, a patient with homozygous DPD deficiency be treated with 5-fluorouracil?
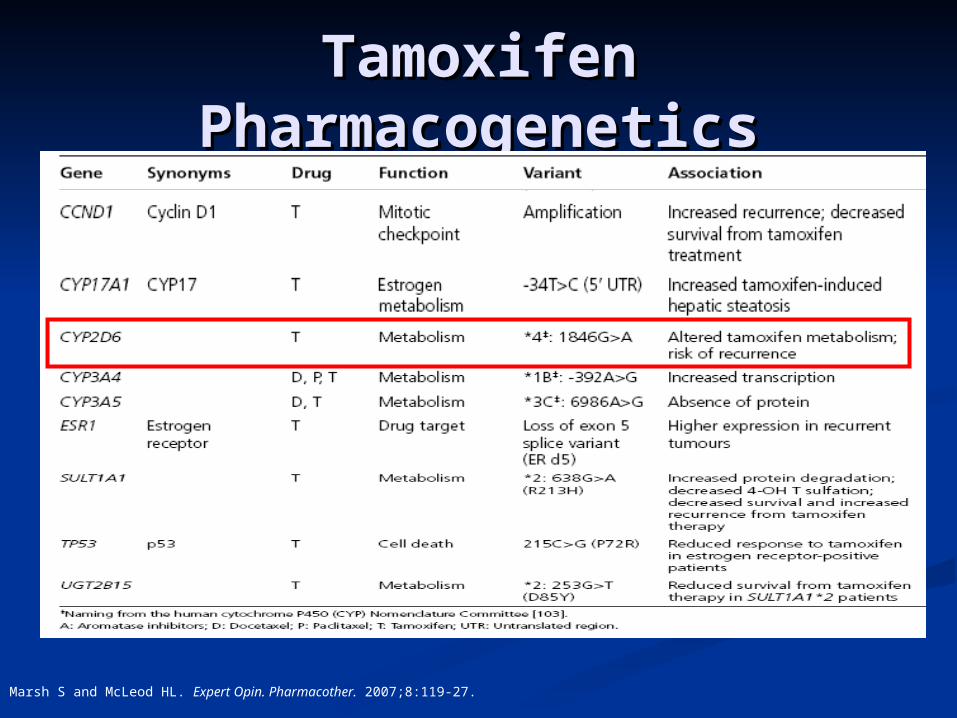
Tamoxifen Tamoxifen PharmacogeneticsPharmacogenetics
Marsh S and McLeod HL. Expert Opin. Pharmacother. 2007;8:119-27.
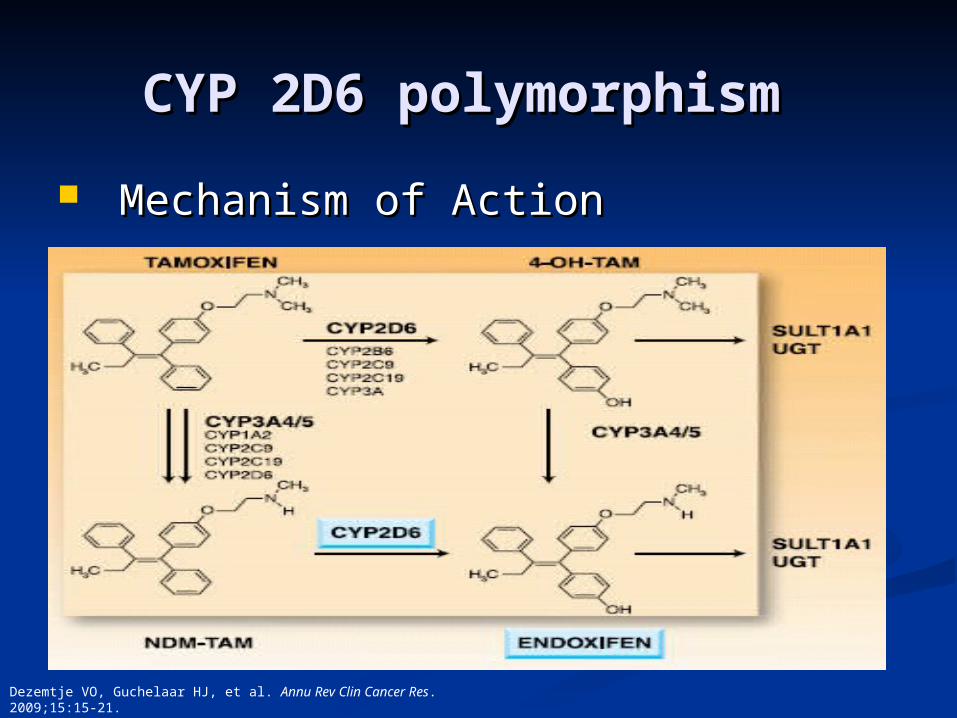
CYP 2D6 polymorphismCYP 2D6 polymorphism
Mechanism of ActionMechanism of Action
Dezemtje VO, Guchelaar HJ, et al. Annu Rev Clin Cancer Res. 2009;15:15-21.
CYP 2D6 polymorphismCYP 2D6 polymorphism
Patient enzyme activity identified by Patient enzyme activity identified by probeprobe
Patients separated in to four groupsPatients separated in to four groups Poor, intermediate, extensive, or ultra-Poor, intermediate, extensive, or ultra-
rapid metabolizersrapid metabolizers
Higher rates of recurrence in poor Higher rates of recurrence in poor metabolizersmetabolizers
Dezemtje VO, Guchelaar HJ, et al. Annu Rev Clin Cancer Res. 2009;15:15-21.
SummarySummary Majority of studies conducted failed to account Majority of studies conducted failed to account
for tumor grade and prognostic factorsfor tumor grade and prognostic factors
Only one of the major studies accounts for the Only one of the major studies accounts for the use of other CYP2D6 inhibitorsuse of other CYP2D6 inhibitors
Recent studies showing some “negative data” Recent studies showing some “negative data” publishedpublished
AmpliChip CYP450 test is an FDA approved testAmpliChip CYP450 test is an FDA approved test
CYP 2D6 polymorphismCYP 2D6 polymorphism

Food and Drug Food and Drug Administration Administration
Endocrinology and Metabolic Drugs FDA Endocrinology and Metabolic Drugs FDA Advisory Committee Advisory Committee
October 16October 16thth, 2006, 2006
Package insert updated for tamoxifenPackage insert updated for tamoxifen
““Increased risk of breast cancer recurrence Increased risk of breast cancer recurrence in postmenopausal estrogen receptor positive in postmenopausal estrogen receptor positive patients who are CYP2D6 poor metabolizers”patients who are CYP2D6 poor metabolizers”
Epidermal Growth Factor Epidermal Growth Factor Receptor (EGFR)Receptor (EGFR)
Small Molecule InhibitorsSmall Molecule Inhibitors Gefitinib and ErlotinibGefitinib and Erlotinib
Monoclonal AntibodiesMonoclonal Antibodies Cetuximab and Cetuximab and Panitumumab
EGFR prognostic or predictive EGFR prognostic or predictive
Epidermal Growth Factor Epidermal Growth Factor Receptor (EGFR)Receptor (EGFR)
Tyrosine Kinase Domain MutationsTyrosine Kinase Domain Mutations Cluster around the ATP-binding sitesCluster around the ATP-binding sites
Exons 18, 19, and 21Exons 18, 19, and 21
Most common mutationsMost common mutations L858RA (exon 21)L858RA (exon 21) E19delE19del
Yong WO et al. Br J Pharmacol. 2006;62:35-46.

Epidermal Growth Factor Epidermal Growth Factor Receptor (EGFR)Receptor (EGFR)
Major focuses of new research Major focuses of new research Somatic mutations tyrosine kinase Somatic mutations tyrosine kinase
domaindomain Erlotinib and GefitinibErlotinib and Gefitinib
Development of skin rashDevelopment of skin rash
Transcriptional activity and expression Transcriptional activity and expression of EGFRof EGFR
Yong WO et al. Br J Pharmacol. 2006;62:35-46.
Epidermal Growth Factor Epidermal Growth Factor Receptor (EGFR)Receptor (EGFR)
GefitinibGefitinib ISELISEL
Efficacy associated with nationalityEfficacy associated with nationality Japanese vs. CaucasianJapanese vs. Caucasian
High gene copy numberHigh gene copy number
ErlotinibErlotinib BR.21BR.21
Gene status had no significant Gene status had no significant contributions to activitycontributions to activity

Patient populationPatient population Prospective clinical study Prospective clinical study NSCLC, Head and neck CA, and NSCLC, Head and neck CA, and
Ovarian CAOvarian CA ErlotinibErlotinib
Pharmacokinetics, toxicity, and Pharmacokinetics, toxicity, and polymorphic changespolymorphic changes ABCG2 levelsABCG2 levels
Rudin CM et al. J Clin Oncol 2008;26:1119-27.
Epidermal Growth Factor Epidermal Growth Factor Receptor (EGFR)Receptor (EGFR)
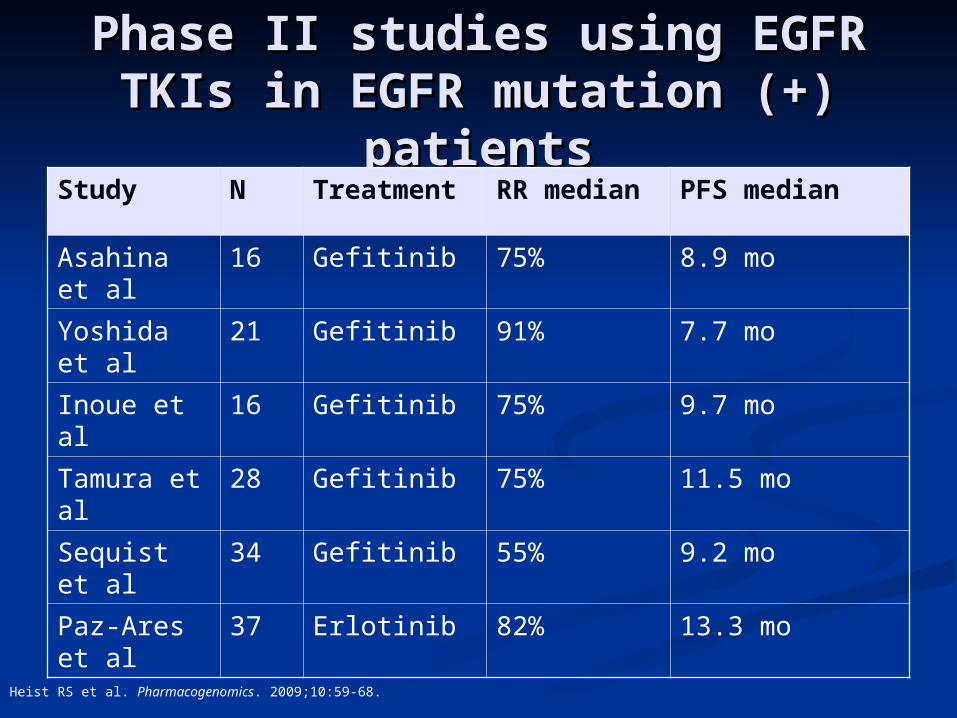
Phase II studies using EGFR Phase II studies using EGFR TKIs in EGFR mutation (+) TKIs in EGFR mutation (+)
patientspatientsStudy N Treatment RR median PFS median
Asahina et al
16 Gefitinib 75% 8.9 mo
Yoshida et al
21 Gefitinib 91% 7.7 mo
Inoue et al 16 Gefitinib 75% 9.7 mo
Tamura et al
28 Gefitinib 75% 11.5 mo
Sequist et al
34 Gefitinib 55% 9.2 mo
Paz-Ares et al
37 Erlotinib 82% 13.3 mo
Heist RS et al. Pharmacogenomics. 2009;10:59-68.
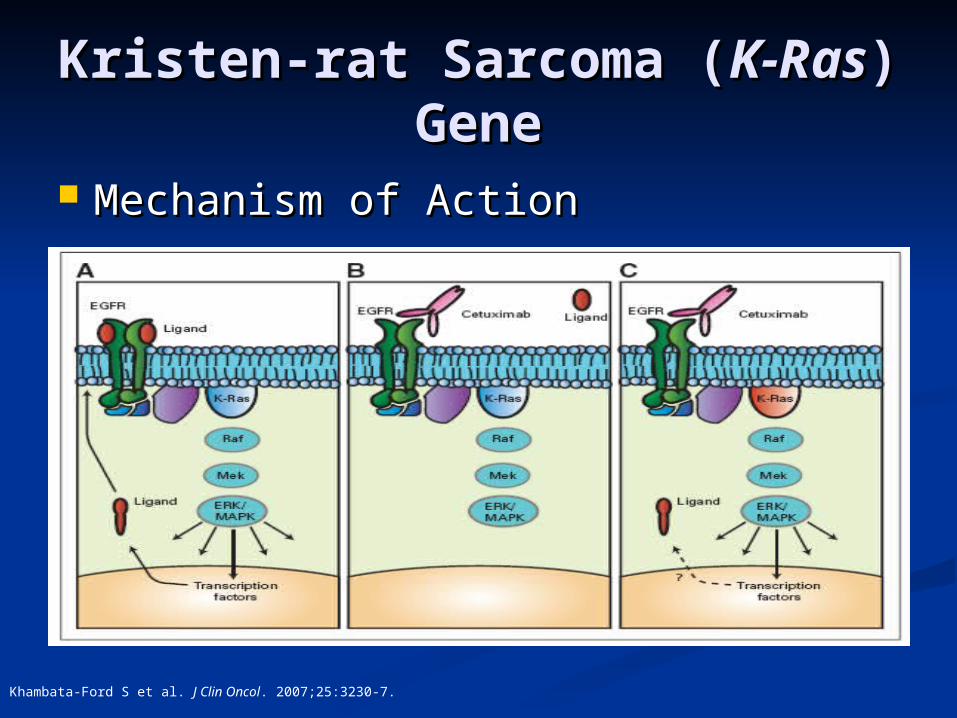
Kristen-rat Sarcoma (Kristen-rat Sarcoma (K-K-RasRas) Gene) Gene
Mechanism of Action Mechanism of Action
Khambata-Ford S et al. J Clin Oncol. 2007;25:3230-7.
K-RasK-Ras
K-RasK-Ras mutation mutation Codon 12 or 13 mutationsCodon 12 or 13 mutations
G-protein coupled receptor signalingG-protein coupled receptor signaling Cell proliferation and survivalCell proliferation and survival
Adenocarcinomas in North AmericaAdenocarcinomas in North America
Progression free survival and overall Progression free survival and overall survival implications?survival implications?

K-RasK-Ras Testing and Testing and Economic ImplicationsEconomic Implications
Annual incidence of 29,762 mCRC casesAnnual incidence of 29,762 mCRC cases Cetuximab Cost $4,032 loading dose, Cetuximab Cost $4,032 loading dose,
$2,880/weekly$2,880/weekly $753 million annually$753 million annually
K-RasK-Ras testing testing PCR-based = $452/patientPCR-based = $452/patient $13 million annually$13 million annually
Theoretical cost savings of $740 millionTheoretical cost savings of $740 million
Shankaran V et al. ASCO GI Cancer Symposium. 2009; abstract 298.
SummarySummary Standardized Standardized K-RasK-Ras mutation testing mutation testing
Substantial Cost savingsSubstantial Cost savings
Patients can benefit from Patients can benefit from preemptive testingpreemptive testing ASCO & NCCN endorsement for ASCO & NCCN endorsement for K-RasK-Ras testing testing
K-RasK-Ras Testing and Testing and Economic ImplicationsEconomic Implications
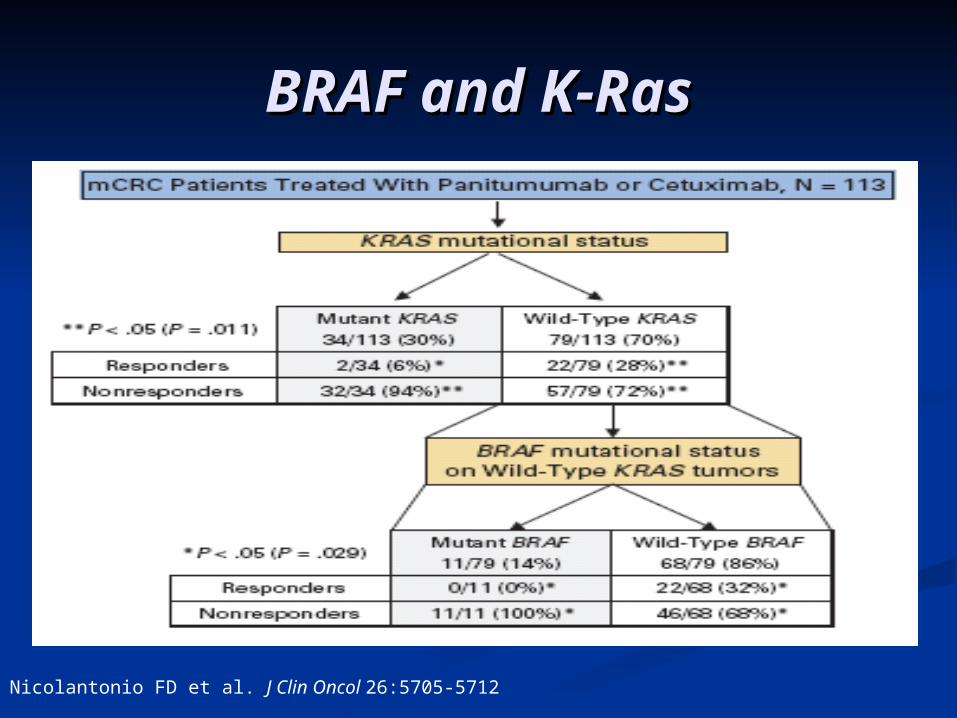
BRAF and K-RasBRAF and K-Ras
Nicolantonio FD et al. J Clin Oncol 26:5705-5712

Study Conclusions Demonstrated a 30% frequency of the K-
Ras mutation in the patients analyzed
The BRAF V600E is has negative implications on EGFR monoclonal antibody therapy, progression free survival, and overall survival
Sorafenib restored sensitivity to the EGFR monoclonal antibody therapies
BRAF BRAF and and K-RasK-Ras
“So what exactly do we want to take away from the information presented this morning?”

ConclusionsConclusions
Pharmacogenomic sampling Pharmacogenomic sampling continues to be focus of researchcontinues to be focus of research TPMT, UGT1A1, DPD, TS, TPMT, UGT1A1, DPD, TS, K-RasK-Ras, and , and
most recently most recently BRAF BRAF impact drug impact drug efficacy and toxicityefficacy and toxicity
Drug dosing guidelines based upon Drug dosing guidelines based upon pharmacogenetics will continue to pharmacogenetics will continue to emergeemerge

Pharmacogenomics: Pharmacogenomics: Clinical Application and Clinical Application and
Effects on Drug Effects on Drug
MetabolismMetabolism Rodney J. Hunter, Pharm.D.Rodney J. Hunter, Pharm.D.
Assistant ProfessorAssistant ProfessorTexas Southern University College of Pharmacy and Texas Southern University College of Pharmacy and
Health SciencesHealth SciencesSNPhA Regional Conference District III, IV, & VSNPhA Regional Conference District III, IV, & V
February 19February 19thth, 2011, 2011