Embed Size (px)
Citation preview

Global | Healthcare
Pharmaceuticals September 12, 2013
PharmaceuticalsRespiratory Market 2025: Taking A DeepBreath And A Deep Dive
EQU
ITY R
ESEARC
H G
LOB
AL
Jeffrey Holford, PhD, ACA *Equity Analyst
(212) 336-7409 [email protected] McManus, PhD §
Equity Analyst44 (0) 20 7029 8274 [email protected]
Ian Hilliker §Equity Analyst
44 (0) 20 7029 8672 [email protected] Ramakanth, PhD, MBA *
Equity Associate(212) 336-7054 [email protected]
David Gu, PhD *Equity Associate
(212) 336-7459 [email protected]
* Jefferies LLC § Jefferies International Limited
Key TakeawayWe present a deep dive on the respiratory market through to 2025, duringwhich we will see multiple new competitors, treatment modalities andincreased pressure from value brands and generics. We see near to mid termupside for GSK from new product launches, but a devastating hit from US Advairgenerics if launched by 2017. AZN's franchise is likely to be hit by increasedcompetition and generics, whilst NOVN looks only able to build a modestbranded franchise.
Taking a deep breath and a deep dive on the respiratory market: We have builta new Global Respiratory Model out to 2025, which primarily focuses on the inhaledrespiratory market for COPD and asthma. Our work includes input from the results of ourproprietary survey of 52 US based pulmonologists, physician consultations and discussionswith key market players. This market is critical to a number of companies under our coverage,with GlaxoSmithKline being particularly exposed as the market leader, with 19% of Grouprevenues in Advair/ Seretide alone. Other branded players such as AstraZeneca and Novartis(and Sandoz) also remain committed to this market in the long term.
We expect sluggish growth despite multiple new launches and positivedemographics: We forecast that the Global inhaled respiratory maintenance market willshow volume growth of just 2% over the period 2012A-2025E as combination therapiesbecome more prevalent, reducing the number of individual prescriptions per patient,despite positive demographic changes in Emerging Markets. We forecast only 1% revenuegrowth over the same period, reaching a peak of c$22bn in 2016E before the expectedcombined impact of non-substitutable generics for key products in Europe from 2014E andAB-rated substitutable Advair generics in the US from 2017E. However, we do expect thatthe market will return to revenue growth thereafter, driven by premium pricing for triplecombination therapy products in particular.
LABA/ ICS market set for the most change: The LABA/ ICS market for asthma andCOPD is dominated by GlaxoSmithKline's Advair and AstraZeneca's Symbicort. Our surveypredicts that GlaxoSmithKline's Breo Ellipta will become the leading LABA/ ICS brand forCOPD as soon as five years after launch. Despite some near term upside from new productlaunches and aggressive price increases for Advair (and Symbicort in parallel) to force theswitch onto Breo Ellipta, we forecast that the LABA/ ICS class will come under intensepressure from the launch of value brands and non-substitutable generics in Europe andsubstitutable Advair generics in the US (from late 2016E). Further pressure will likely comefrom the launch of the LABA/ LAMA class in the near term and then from LABA/ LAMA/ ICStriple combination products in the longer term.
New LABA/ LAMA class offers some switching potential and pricing upside: Ourproprietary physician survey and interviews indicate that pulmonologists are enthusiasticabout new fixed dose LABA/ LAMA offerings, such as GlaxoSmithKline's Anoro Ellipta,expecting this class to be prescribed to c20% of COPD patients five years after launch. Muchof the market share for this class is expected be gained from the LAMA class (e.g. BoehringerIngelheim's Spiriva). GlaxoSmithKline appears very well positioned in this class with likelyfirst-to-market status in the US, once-daily dosing and a premium device.
Stock implications: Company notes published in parallel and taking the implicationsof this report into account show a positive impact (3%-8%) to our GlaxoSmithKline EPSestimates between 2014E-16E, whilst our 2017E EPS estimate falls by 14% when US Advairgenerics are brought into the equation. Our AstraZeneca EPS estimates fall by 3%-12% across2014E-17E based on our work in this report (see separate company note), whilst our Novartisestimates are not impacted and we have made no formal changes to estimates.
Jefferies does and seeks to do business with companies covered in its research reports. As a result, investors should be aware that Jefferies may have a conflictof interest that could affect the objectivity of this report. Investors should consider this report as only a single factor in making their investment decision.Please see analyst certifications, important disclosure information, and information regarding the status of non-US analysts on pages 40 to 43 of this report.
Executive Summary The $31bn Global respiratory market is likely to see a number of significant changes over
the next five to ten years as new players enter the market either with new branded or
generic products and existing players broaden their product offerings with new
combination products and devices. This market is critical to a number of companies under
our coverage, with GlaxoSmithKline (GSK LN, 1,629p, Hold) being particularly exposed as
the market leader, with 19% of Group revenues in Advair/ Seretide alone. Other branded
players such as AstraZeneca (AZN LN, 3,190p, Hold) and Novartis (NOVN VX, CHF71.35,
Buy) also remain committed to this market in the long term, whilst generics companies,
such as Mylan (MYL, $38.05, NC) and Novartis’ own Sandoz unit see significant potential
in virgin markets for generic products in the US and Europe.
Guided by a survey of 52 US based pulmonologists conducted in August 2013, we have
built out what we believe is the most contemporary and forward thinking Global
respiratory market models available to investors. The market is extremely complex and the
large number of moving pieces that we have had to consider have led us to make some
significant changes to our thinking on several key respiratory franchises as described in
detail in this report.
It is worth noting specifically at this point that we have mostly considered and evaluated
the Global inhaled maintenance respiratory market for COPD and asthma for the
purposes of this report (total value c$18bn in 2012A), which does exclude some product
classes. However, all of our company models reflect the entirety of their respiratory
franchises including other classes such as oral leukotriene D4 antagonists, corticosteroids,
antibody-based injectable therapeutics and short-acting beta-agonists.
The key implications for the respiratory market and individual companies considered
within this report are as follows:
We expect that the Global inhaled respiratory maintenance market will show
volume growth of just 2% over the period 2012A-2025E as combination
therapies become more prevalent, reducing the number of individual
prescriptions per patient. This driver is likely to be somewhat offset by price
increases for new combination products as well as positive demographics in
Emerging Market countries, where increased prevalence of smoking may act as a
strong volume driver over time. However, it remains unclear as to how well high
value branded products will fair in these markets,
We expect that the Global inhaled respiratory maintenance market will show
only 1% value growth over this period, reaching a peak of c$22bn in 2016E
before we anticipate the combined impact of non-substitutable generics for key
products in Europe from 2014E and AB-rated substitutable generics in the US
from 2017E. However, we do expect the market to begin to recover some value
growth thereafter, driven by premium pricing for triple combination therapy
products in particular,
We anticipate a strong shift towards fixed dose combination products such as
LABA/ LAMA and eventually LABA/ LAMA/ ICS (or MABA/ ICS) with patient
compliance, potential for increased efficacy and a better overall deal for payors
being strong drivers of this,
Healthcare
Pharmaceuticals
September 12, 2013
page 2 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
GlaxoSmithKline should see value growth in its respiratory franchise out to
2016E at least driven by strong US pricing behind Advair to help force switching
over to Breo Ellipta, as well as the launch of Anoro Ellipta. We expect that Anoro
Ellipta will gain significant share from the LAMA class in COPD, while putting
limited pressure on the LABA/ ICS and LABA alone classes. However, we see
significant destruction of value should substitutable generics launch in the US by
2017E, compounded by price referencing pressure from non-substitutable
generics in Europe from 2014E. As a result we have increased our key respiratory
combination franchise (Advair, Anoro Ellipta, Breo Ellipta) revenue estimates for
GlaxoSmithKline by 2%-17% from 2013E-16E, but have then reduced our 2017E
estimate by 25% due to the impact of US generics. From the Group context, this
and other updates (e.g. FX [negative impact of [1%-2%] and the setback on the
MAGE-A3 program) have led us to increase group revenue estimates by 0%-2%
from 2014E-16E and cut 2017E by 6%. From the perspective of Group EPS, we
have increased 2014E-16E EPS by 3%-8%, whilst lowering our 2017E EPS by
14%. We have cut our PT for GlaxoSmithKline to 1,750p from 1,800p and
reiterate our Hold rating (see separate company note also published today for
more details),
AstraZeneca should see slowing growth for its respiratory franchise from 2014E
as Symbicort volume is pressured by in-class competitors (Breo for COPD in the
US, value brands and potentially generics ex-US), and new class launches (LABA/
LAMA class). We expect AstraZeneca to increase the price of Symbicort in the US,
following expected Advair price increases by GlaxoSmithKline, which should
ensure franchise value growth through to 2016E. Volume pressure in the US and
ex-US, and price pressure ex-US will likely push the franchise into decline from
2016E, with the launch of Novartis’ LABA/ ICS QMF149 further adding to the
pressure on the franchise. We see significant pressure on Symbicort revenues
due should a substitutable generic of Advair launch in the US by 2017E,
compounded by price referencing pressure from non-substitutable LABA/ ICS
generics in Europe from 2014E. Whilst the launch of AstraZeneca’s LABA/ LAMA
PT003 will provide a new leg to the franchise, this will be a comparatively late
entrant to the class in 2016E. Revising our company model to reflect this and
other fine tuning, including updated FX, lowers our Group revenue
expectations by 0% to 7% and our CORE EPS numbers by 0% to 12% over the
forecast period. We have cut our PT for AstraZeneca to 2,850p from 3,200p and
reiterate our Hold rating (see separate company note also published today for
more details),
Novartis is a relative new market entrant in the inhaled respiratory market, with
its only significant marketed respiratory product to date being the injectable
anti-IgE mAb Xolair. We expect Novartis’ inhaled respiratory franchise to reach
‚blockbuster‛ status in 2017E. Our global therapy model and proprietary
pulmonologist survey suggests Novartis’ inhaled respiratory franchise (QVA149,
Arcapta, Seebri, QMF149) will struggle to meet current consensus expectations
which are looking for 2017E sales of $1.7bn. Regulatory delays in the US and an
inferior device (according to pulmonologists) will make it difficult for Novartis to
compete successfully in what has become a competitive market. At only 3% of
group sales in 2017E (including Xolair), we do not see the company’s
respiratory franchise as being a significant driver for investor sentiment in either
direction.
Healthcare
Pharmaceuticals
September 12, 2013
page 3 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
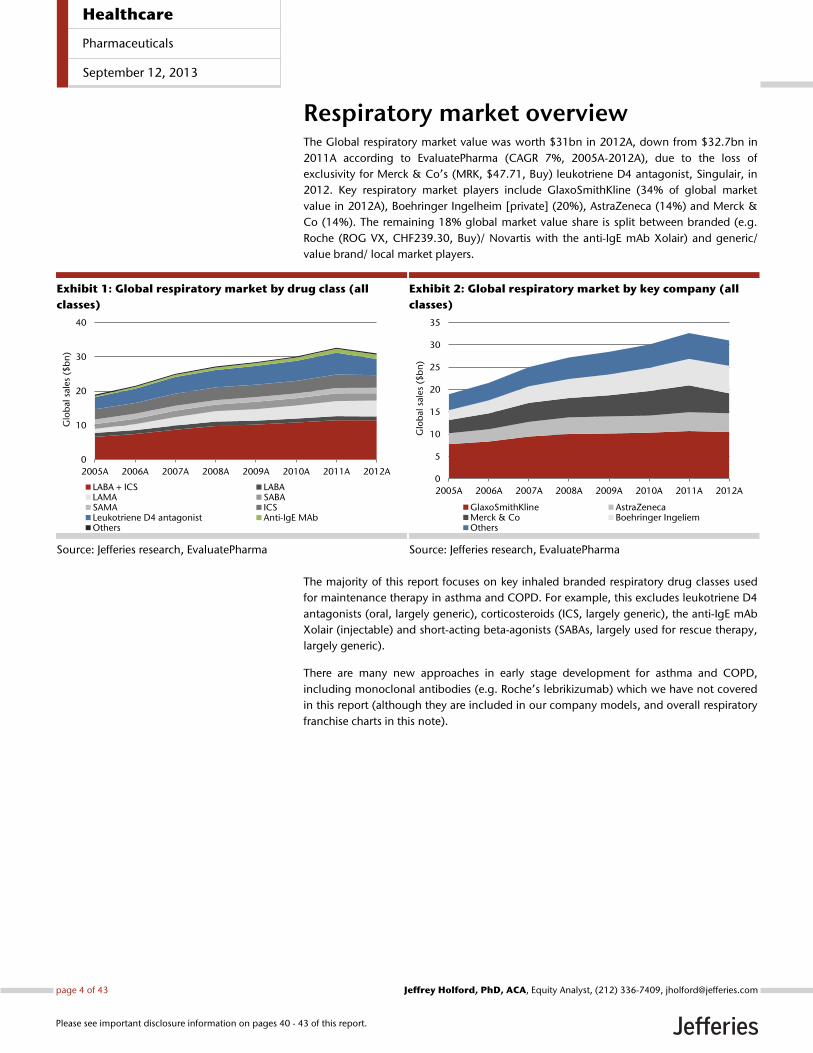
Respiratory market overview The Global respiratory market value was worth $31bn in 2012A, down from $32.7bn in
2011A according to EvaluatePharma (CAGR 7%, 2005A-2012A), due to the loss of
exclusivity for Merck & Co’s (MRK, $47.71, Buy) leukotriene D4 antagonist, Singulair, in
2012. Key respiratory market players include GlaxoSmithKline (34% of global market
value in 2012A), Boehringer Ingelheim [private] (20%), AstraZeneca (14%) and Merck &
Co (14%). The remaining 18% global market value share is split between branded (e.g.
Roche (ROG VX, CHF239.30, Buy)/ Novartis with the anti-IgE mAb Xolair) and generic/
value brand/ local market players.
Exhibit 1: Global respiratory market by drug class (all
classes)
Source: Jefferies research, EvaluatePharma
Exhibit 2: Global respiratory market by key company (all
classes)
Source: Jefferies research, EvaluatePharma
The majority of this report focuses on key inhaled branded respiratory drug classes used
for maintenance therapy in asthma and COPD. For example, this excludes leukotriene D4
antagonists (oral, largely generic), corticosteroids (ICS, largely generic), the anti-IgE mAb
Xolair (injectable) and short-acting beta-agonists (SABAs, largely used for rescue therapy,
largely generic).
There are many new approaches in early stage development for asthma and COPD,
including monoclonal antibodies (e.g. Roche’s lebrikizumab) which we have not covered
in this report (although they are included in our company models, and overall respiratory
franchise charts in this note).
0
10
20
30
40
2005A 2006A 2007A 2008A 2009A 2010A 2011A 2012A
Glo
bal
sale
s ($
bn
)
LABA + ICS LABALAMA SABASAMA ICSLeukotriene D4 antagonist Anti-IgE MAbOthers
0
5
10
15
20
25
30
35
2005A 2006A 2007A 2008A 2009A 2010A 2011A 2012A
Glo
bal
sale
s ($
bn
)
GlaxoSmithKline AstraZenecaMerck & Co Boehringer IngeliemOthers
Healthcare
Pharmaceuticals
September 12, 2013
page 4 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
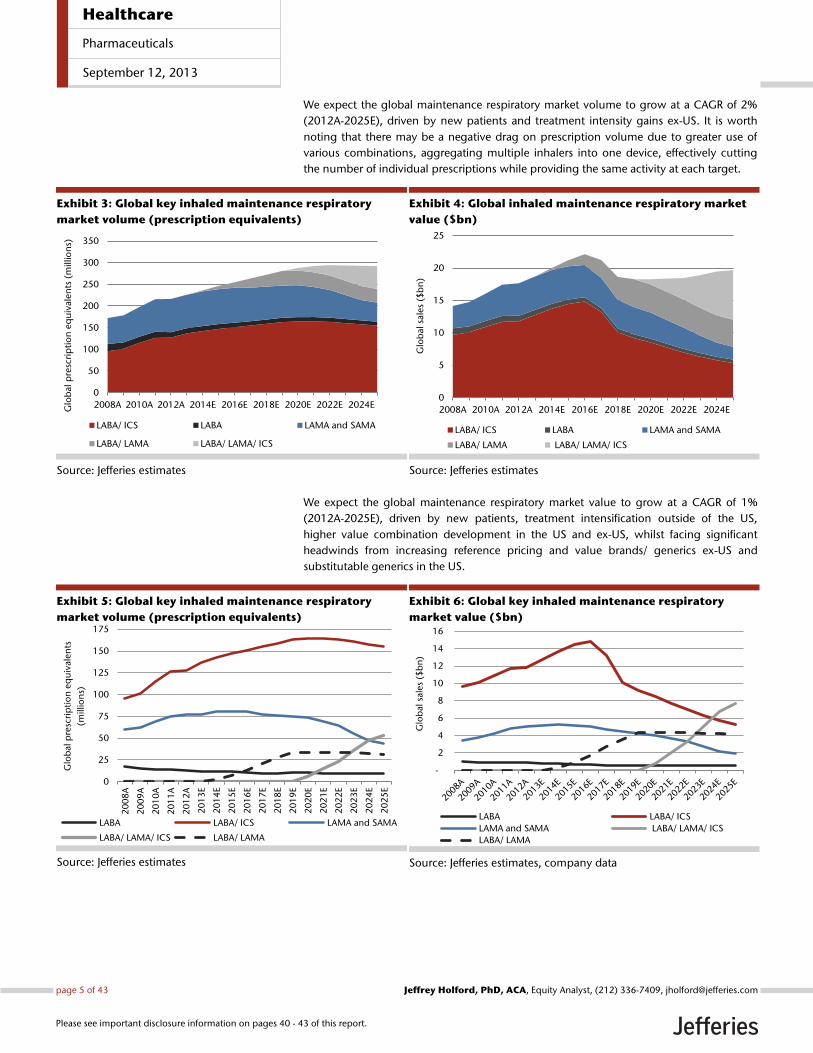
We expect the global maintenance respiratory market volume to grow at a CAGR of 2%
(2012A-2025E), driven by new patients and treatment intensity gains ex-US. It is worth
noting that there may be a negative drag on prescription volume due to greater use of
various combinations, aggregating multiple inhalers into one device, effectively cutting
the number of individual prescriptions while providing the same activity at each target.
Exhibit 3: Global key inhaled maintenance respiratory
market volume (prescription equivalents)
Source: Jefferies estimates
Exhibit 4: Global inhaled maintenance respiratory market
value ($bn)
Source: Jefferies estimates
We expect the global maintenance respiratory market value to grow at a CAGR of 1%
(2012A-2025E), driven by new patients, treatment intensification outside of the US,
higher value combination development in the US and ex-US, whilst facing significant
headwinds from increasing reference pricing and value brands/ generics ex-US and
substitutable generics in the US.
Exhibit 5: Global key inhaled maintenance respiratory
market volume (prescription equivalents)
Source: Jefferies estimates
Exhibit 6: Global key inhaled maintenance respiratory
market value ($bn)
Source: Jefferies estimates, company data
0
50
100
150
200
250
300
350
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024EGlo
bal
pre
scri
pti
on
eq
uiv
alen
ts (
mill
ion
s)
LABA/ ICS LABA LAMA and SAMA
LABA/ LAMA LABA/ LAMA/ ICS
0
5
10
15
20
25
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024EG
lob
al s
ale
s ($
bn
)LABA/ ICS LABA LAMA and SAMA
LABA/ LAMA LABA/ LAMA/ ICS
0
25
50
75
100
125
150
175
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Glo
bal
pre
scri
pti
on
eq
uiv
ale
nts
(mill
ion
s)
LABA LABA/ ICS LAMA and SAMA
LABA/ LAMA/ ICS LABA/ LAMA
-
2
4
6
8
10
12
14
16
Glo
bal
sale
s ($
bn
)
LABA LABA/ ICS
LAMA and SAMA LABA/ LAMA/ ICS
LABA/ LAMA
Healthcare
Pharmaceuticals
September 12, 2013
page 5 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
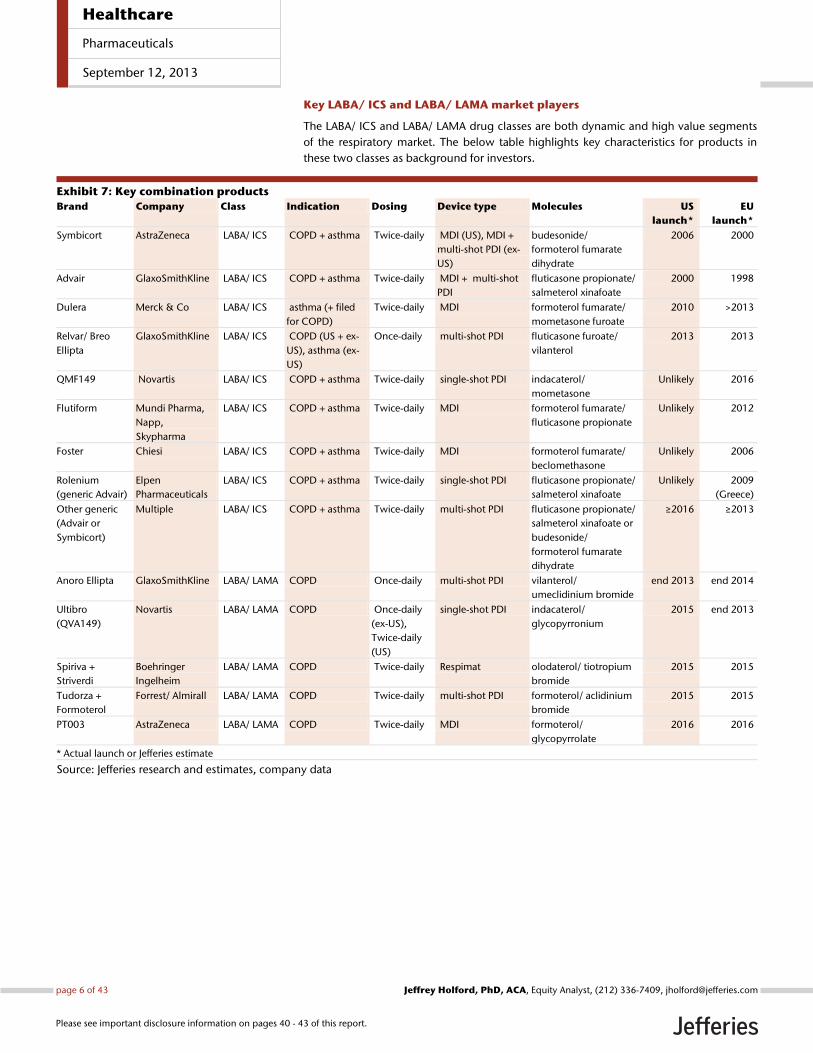
Key LABA/ ICS and LABA/ LAMA market players
The LABA/ ICS and LABA/ LAMA drug classes are both dynamic and high value segments
of the respiratory market. The below table highlights key characteristics for products in
these two classes as background for investors.
Exhibit 7: Key combination products
Brand Company Class Indication Dosing Device type Molecules US
launch*
EU
launch*
Symbicort AstraZeneca LABA/ ICS COPD + asthma Twice-daily MDI (US), MDI +
multi-shot PDI (ex-
US)
budesonide/
formoterol fumarate
dihydrate
2006 2000
Advair GlaxoSmithKline LABA/ ICS COPD + asthma Twice-daily MDI + multi-shot
PDI
fluticasone propionate/
salmeterol xinafoate
2000 1998
Dulera Merck & Co LABA/ ICS asthma (+ filed
for COPD)
Twice-daily MDI formoterol fumarate/
mometasone furoate
2010 >2013
Relvar/ Breo
Ellipta
GlaxoSmithKline LABA/ ICS COPD (US + ex-
US), asthma (ex-
US)
Once-daily multi-shot PDI fluticasone furoate/
vilanterol
2013 2013
QMF149 Novartis LABA/ ICS COPD + asthma Twice-daily single-shot PDI indacaterol/
mometasone
Unlikely 2016
Flutiform Mundi Pharma,
Napp,
Skypharma
LABA/ ICS COPD + asthma Twice-daily MDI formoterol fumarate/
fluticasone propionate
Unlikely 2012
Foster Chiesi LABA/ ICS COPD + asthma Twice-daily MDI formoterol fumarate/
beclomethasone
Unlikely 2006
Rolenium
(generic Advair)
Elpen
Pharmaceuticals
LABA/ ICS COPD + asthma Twice-daily single-shot PDI fluticasone propionate/
salmeterol xinafoate
Unlikely 2009
(Greece)
Other generic
(Advair or
Symbicort)
Multiple LABA/ ICS COPD + asthma Twice-daily multi-shot PDI fluticasone propionate/
salmeterol xinafoate or
budesonide/
formoterol fumarate
dihydrate
≥2016 ≥2013
Anoro Ellipta GlaxoSmithKline LABA/ LAMA COPD Once-daily multi-shot PDI vilanterol/
umeclidinium bromide
end 2013 end 2014
Ultibro
(QVA149)
Novartis LABA/ LAMA COPD Once-daily
(ex-US),
Twice-daily
(US)
single-shot PDI indacaterol/
glycopyrronium
2015 end 2013
Spiriva +
Striverdi
Boehringer
Ingelheim
LABA/ LAMA COPD Twice-daily Respimat olodaterol/ tiotropium
bromide
2015 2015
Tudorza +
Formoterol
Forrest/ Almirall LABA/ LAMA COPD Twice-daily multi-shot PDI formoterol/ aclidinium
bromide
2015 2015
PT003 AstraZeneca LABA/ LAMA COPD Twice-daily MDI formoterol/
glycopyrrolate
2016 2016
* Actual launch or Jefferies estimate
Source: Jefferies research and estimates, company data
Healthcare
Pharmaceuticals
September 12, 2013
page 6 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
US Pulmonologist Survey Design We conducted a quantitative survey of 52 US based pulmonologists in August 2013. The
aim of the study was to gain insight into the impact of the launch of new drug classes and
new brands in the COPD and asthma indications.
The surveyed pulmonologists treated on average 646 patients per month, and practiced
in a cross section of medical facilities. On average, our surveyed pulmonologists had
practiced this specialty for 14 years. We have presented the full results (expressed as the
numerical mean) of this survey in the appendix to this document. We also interviewed a
KOL consultant Pulmonologist following the survey. The following section outlines the
key findings from the survey.
Current treatment algorithm likely to change
At present, COPD patients are treated with LAMA, LABA, and ICS containing treatments in
various combinations as maintenance therapies, depending upon the severity of their
disease (see Appendix I for the percentage of patients treated with each individual option
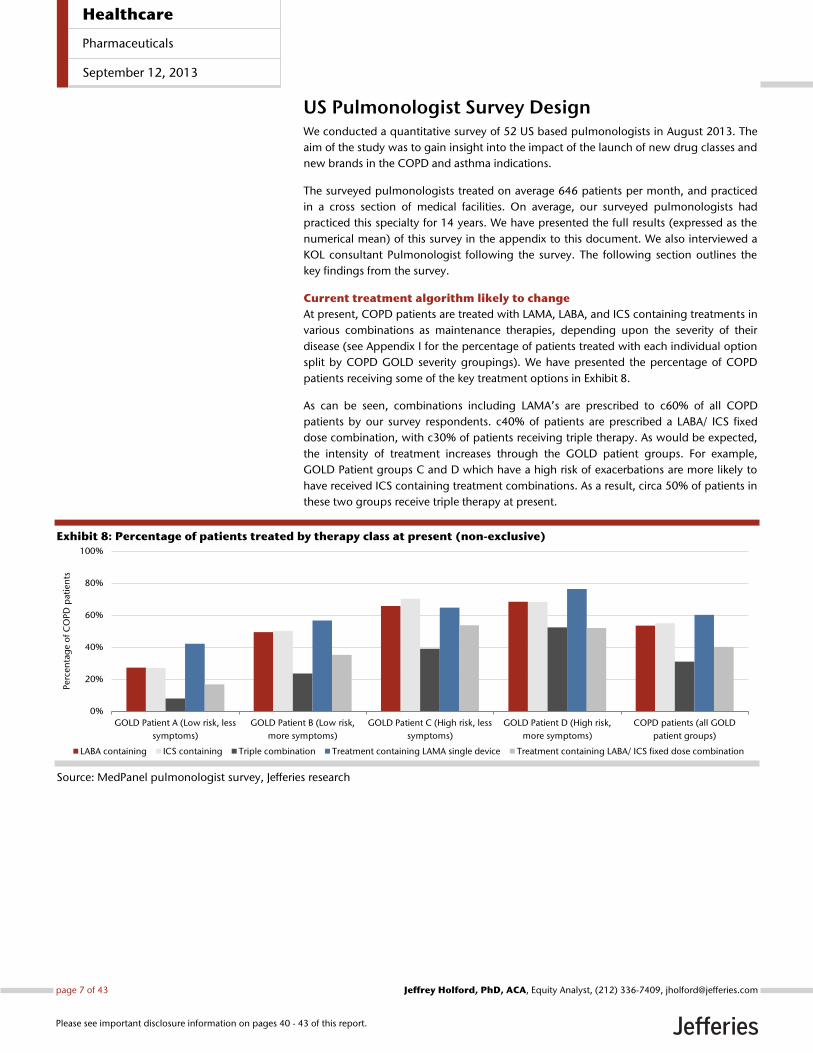
split by COPD GOLD severity groupings). We have presented the percentage of COPD
patients receiving some of the key treatment options in Exhibit 8.
As can be seen, combinations including LAMA’s are prescribed to c60% of all COPD
patients by our survey respondents. c40% of patients are prescribed a LABA/ ICS fixed
dose combination, with c30% of patients receiving triple therapy. As would be expected,
the intensity of treatment increases through the GOLD patient groups. For example,
GOLD Patient groups C and D which have a high risk of exacerbations are more likely to
have received ICS containing treatment combinations. As a result, circa 50% of patients in
these two groups receive triple therapy at present.
Exhibit 8: Percentage of patients treated by therapy class at present (non-exclusive)
Source: MedPanel pulmonologist survey, Jefferies research
0%
20%
40%
60%
80%
100%
GOLD Patient A (Low risk, less
symptoms)
GOLD Patient B (Low risk,
more symptoms)
GOLD Patient C (High risk, less
symptoms)
GOLD Patient D (High risk,
more symptoms)
COPD patients (all GOLD
patient groups)
Perc
en
tag
e o
f C
OP
D p
ati
en
ts
LABA containing ICS containing Triple combination Treatment containing LAMA single device Treatment containing LABA/ ICS fixed dose combination
Healthcare
Pharmaceuticals
September 12, 2013
page 7 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
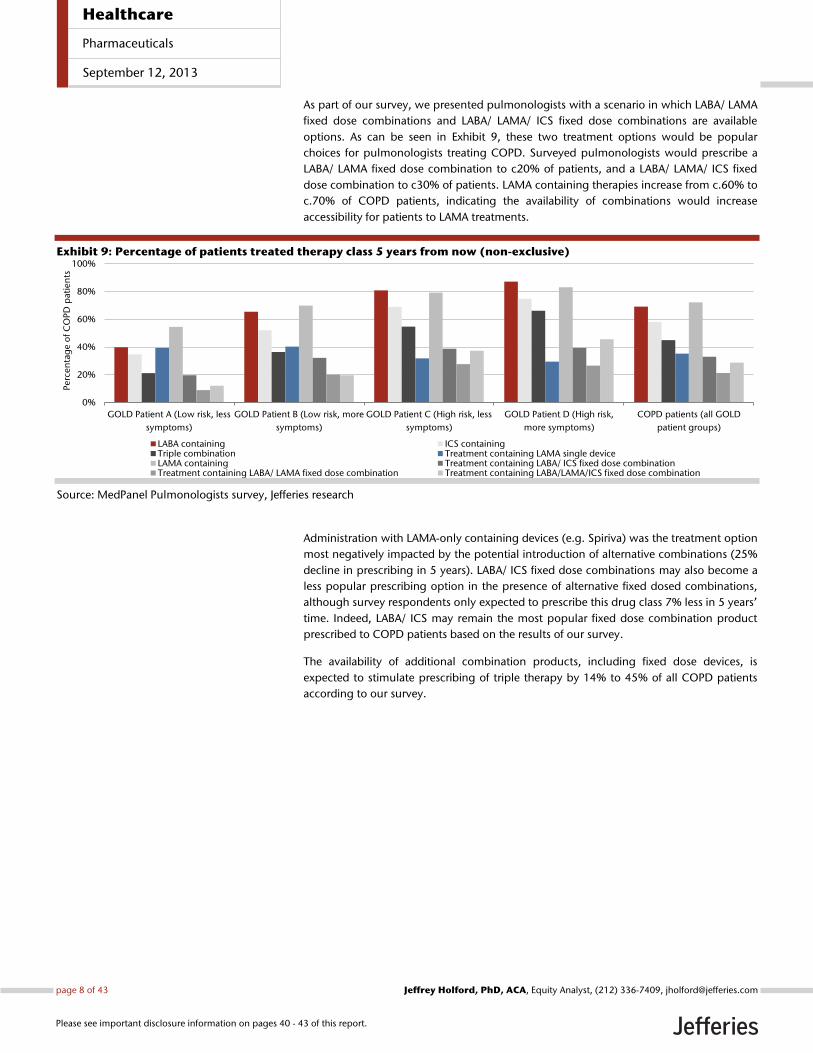
As part of our survey, we presented pulmonologists with a scenario in which LABA/ LAMA
fixed dose combinations and LABA/ LAMA/ ICS fixed dose combinations are available
options. As can be seen in Exhibit 9, these two treatment options would be popular
choices for pulmonologists treating COPD. Surveyed pulmonologists would prescribe a
LABA/ LAMA fixed dose combination to c20% of patients, and a LABA/ LAMA/ ICS fixed
dose combination to c30% of patients. LAMA containing therapies increase from c.60% to
c.70% of COPD patients, indicating the availability of combinations would increase
accessibility for patients to LAMA treatments.
Exhibit 9: Percentage of patients treated therapy class 5 years from now (non-exclusive)
Source: MedPanel Pulmonologists survey, Jefferies research
Administration with LAMA-only containing devices (e.g. Spiriva) was the treatment option
most negatively impacted by the potential introduction of alternative combinations (25%
decline in prescribing in 5 years). LABA/ ICS fixed dose combinations may also become a
less popular prescribing option in the presence of alternative fixed dosed combinations,
although survey respondents only expected to prescribe this drug class 7% less in 5 years’
time. Indeed, LABA/ ICS may remain the most popular fixed dose combination product
prescribed to COPD patients based on the results of our survey.
The availability of additional combination products, including fixed dose devices, is
expected to stimulate prescribing of triple therapy by 14% to 45% of all COPD patients
according to our survey.
0%
20%
40%
60%
80%
100%
GOLD Patient A (Low risk, less
symptoms)
GOLD Patient B (Low risk, more
symptoms)
GOLD Patient C (High risk, less
symptoms)
GOLD Patient D (High risk,
more symptoms)
COPD patients (all GOLD
patient groups)
Perc
en
tag
e o
f C
OP
D p
ati
en
ts
LABA containing ICS containingTriple combination Treatment containing LAMA single deviceLAMA containing Treatment containing LABA/ ICS fixed dose combinationTreatment containing LABA/ LAMA fixed dose combination Treatment containing LABA/LAMA/ICS fixed dose combination
Healthcare
Pharmaceuticals
September 12, 2013
page 8 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
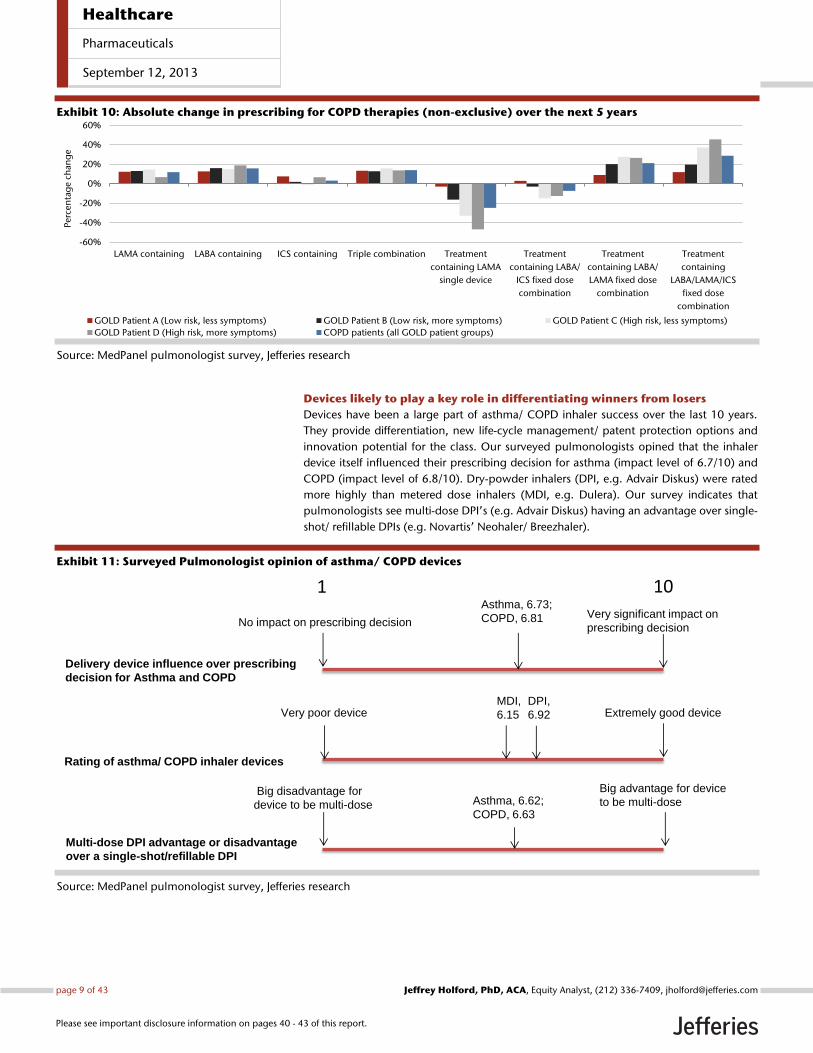
Exhibit 10: Absolute change in prescribing for COPD therapies (non-exclusive) over the next 5 years
Source: MedPanel pulmonologist survey, Jefferies research
Devices likely to play a key role in differentiating winners from losers
Devices have been a large part of asthma/ COPD inhaler success over the last 10 years.
They provide differentiation, new life-cycle management/ patent protection options and
innovation potential for the class. Our surveyed pulmonologists opined that the inhaler
device itself influenced their prescribing decision for asthma (impact level of 6.7/10) and
COPD (impact level of 6.8/10). Dry-powder inhalers (DPI, e.g. Advair Diskus) were rated
more highly than metered dose inhalers (MDI, e.g. Dulera). Our survey indicates that
pulmonologists see multi-dose DPI’s (e.g. Advair Diskus) having an advantage over single-
shot/ refillable DPIs (e.g. Novartis’ Neohaler/ Breezhaler).
Exhibit 11: Surveyed Pulmonologist opinion of asthma/ COPD devices
Source: MedPanel pulmonologist survey, Jefferies research
-60%
-40%
-20%
0%
20%
40%
60%
LAMA containing LABA containing ICS containing Triple combination Treatment
containing LAMA
single device
Treatment
containing LABA/
ICS fixed dose
combination
Treatment
containing LABA/
LAMA fixed dose
combination
Treatment
containing
LABA/LAMA/ICS
fixed dose
combination
Perc
en
tag
e c
han
ge
GOLD Patient A (Low risk, less symptoms) GOLD Patient B (Low risk, more symptoms) GOLD Patient C (High risk, less symptoms)
GOLD Patient D (High risk, more symptoms) COPD patients (all GOLD patient groups)
Delivery device influence over prescribing
decision for Asthma and COPD
Rating of asthma/ COPD inhaler devices
Multi-dose DPI advantage or disadvantage
over a single-shot/refillable DPI
No impact on prescribing decisionVery significant impact on
prescribing decision
1 10
Very poor device Extremely good device
Big disadvantage for
device to be multi-dose
Big advantage for device
to be multi-dose
Asthma, 6.73;
COPD, 6.81
MDI,
6.15
DPI,
6.92
Asthma, 6.62;
COPD, 6.63
Healthcare
Pharmaceuticals
September 12, 2013
page 9 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
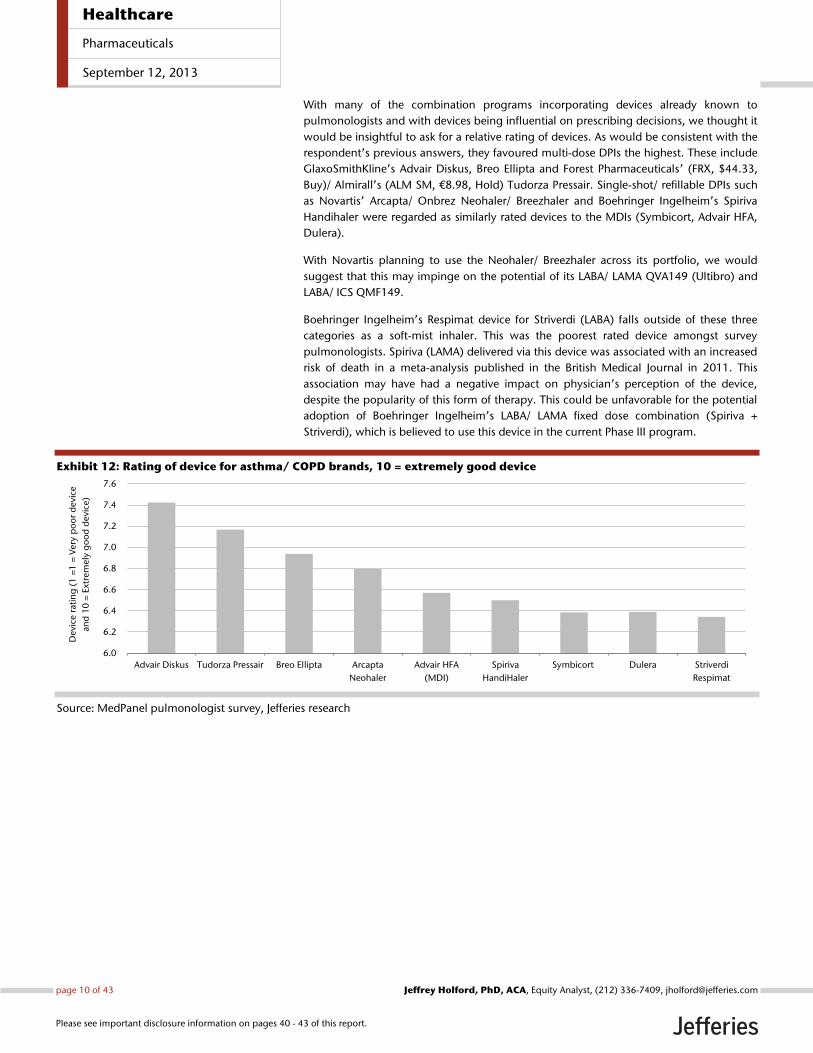
With many of the combination programs incorporating devices already known to
pulmonologists and with devices being influential on prescribing decisions, we thought it
would be insightful to ask for a relative rating of devices. As would be consistent with the
respondent’s previous answers, they favoured multi-dose DPIs the highest. These include
GlaxoSmithKline’s Advair Diskus, Breo Ellipta and Forest Pharmaceuticals’ (FRX, $44.33,
Buy)/ Almirall’s (ALM SM, €8.98, Hold) Tudorza Pressair. Single-shot/ refillable DPIs such
as Novartis’ Arcapta/ Onbrez Neohaler/ Breezhaler and Boehringer Ingelheim’s Spiriva
Handihaler were regarded as similarly rated devices to the MDIs (Symbicort, Advair HFA,
Dulera).
With Novartis planning to use the Neohaler/ Breezhaler across its portfolio, we would
suggest that this may impinge on the potential of its LABA/ LAMA QVA149 (Ultibro) and
LABA/ ICS QMF149.
Boehringer Ingelheim’s Respimat device for Striverdi (LABA) falls outside of these three
categories as a soft-mist inhaler. This was the poorest rated device amongst survey
pulmonologists. Spiriva (LAMA) delivered via this device was associated with an increased
risk of death in a meta-analysis published in the British Medical Journal in 2011. This
association may have had a negative impact on physician’s perception of the device,
despite the popularity of this form of therapy. This could be unfavorable for the potential
adoption of Boehringer Ingelheim’s LABA/ LAMA fixed dose combination (Spiriva +
Striverdi), which is believed to use this device in the current Phase III program.
Exhibit 12: Rating of device for asthma/ COPD brands, 10 = extremely good device
Source: MedPanel pulmonologist survey, Jefferies research
6.0
6.2
6.4
6.6
6.8
7.0
7.2
7.4
7.6
Advair Diskus Tudorza Pressair Breo Ellipta Arcapta
Neohaler
Advair HFA
(MDI)
Spiriva
HandiHaler
Symbicort Dulera Striverdi
Respimat
Devi
ce r
atin
g (
1 =
1 =
Very
po
or
devi
ce
and
10
= E
xtre
mely
go
od
devi
ce)
Healthcare
Pharmaceuticals
September 12, 2013
page 10 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
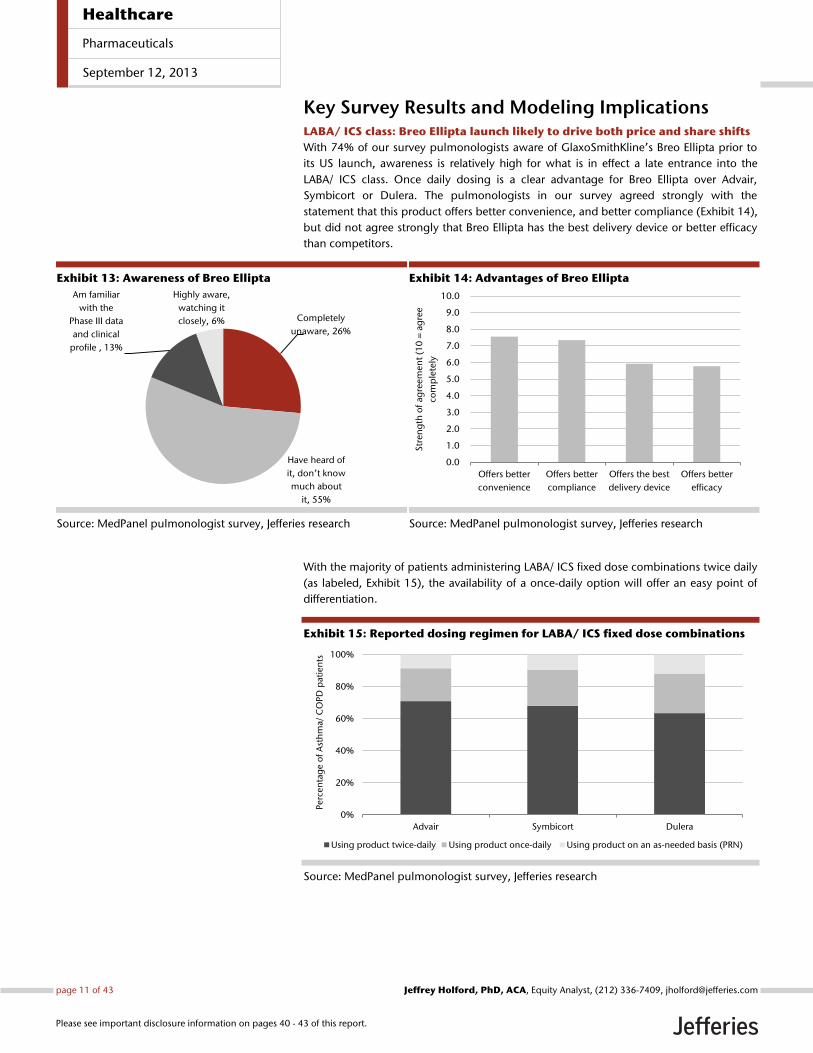
Key Survey Results and Modeling Implications LABA/ ICS class: Breo Ellipta launch likely to drive both price and share shifts
With 74% of our survey pulmonologists aware of GlaxoSmithKline’s Breo Ellipta prior to
its US launch, awareness is relatively high for what is in effect a late entrance into the
LABA/ ICS class. Once daily dosing is a clear advantage for Breo Ellipta over Advair,
Symbicort or Dulera. The pulmonologists in our survey agreed strongly with the
statement that this product offers better convenience, and better compliance (Exhibit 14),
but did not agree strongly that Breo Ellipta has the best delivery device or better efficacy
than competitors.
Exhibit 13: Awareness of Breo Ellipta
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 14: Advantages of Breo Ellipta
Source: MedPanel pulmonologist survey, Jefferies research
With the majority of patients administering LABA/ ICS fixed dose combinations twice daily
(as labeled, Exhibit 15), the availability of a once-daily option will offer an easy point of
differentiation.
Exhibit 15: Reported dosing regimen for LABA/ ICS fixed dose combinations
Source: MedPanel pulmonologist survey, Jefferies research
Completely
unaware, 26%
Have heard of
it, don’t know
much about
it, 55%
Am familiar
with the
Phase III data
and clinical
profile , 13%
Highly aware,
watching it
closely, 6%
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Offers better
convenience
Offers better
compliance
Offers the best
delivery device
Offers better
efficacy
Str
en
gth
of
agre
em
en
t (1
0 =
ag
ree
com
ple
tely
0%
20%
40%
60%
80%
100%
Advair Symbicort Dulera
Perc
en
tag
e o
f A
sth
ma/
CO
PD
pati
en
ts
Using product twice-daily Using product once-daily Using product on an as-needed basis (PRN)
Healthcare
Pharmaceuticals
September 12, 2013
page 11 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
Breo Ellipta will initially only be indicated for COPD in the US (an asthma filing could
occur, but we presume that this will not be successful for now), although it will likely be
available for both asthma and COPD outside of the US. Our survey indicates that 48% of
LABA/ ICS fixed dose combination prescribing is currently for COPD, with 51% for asthma
(1% for other). Feedback we have received from our consultant in this area would suggest
that we should expect some off-label prescribing of Breo Ellipta in asthma in the US.
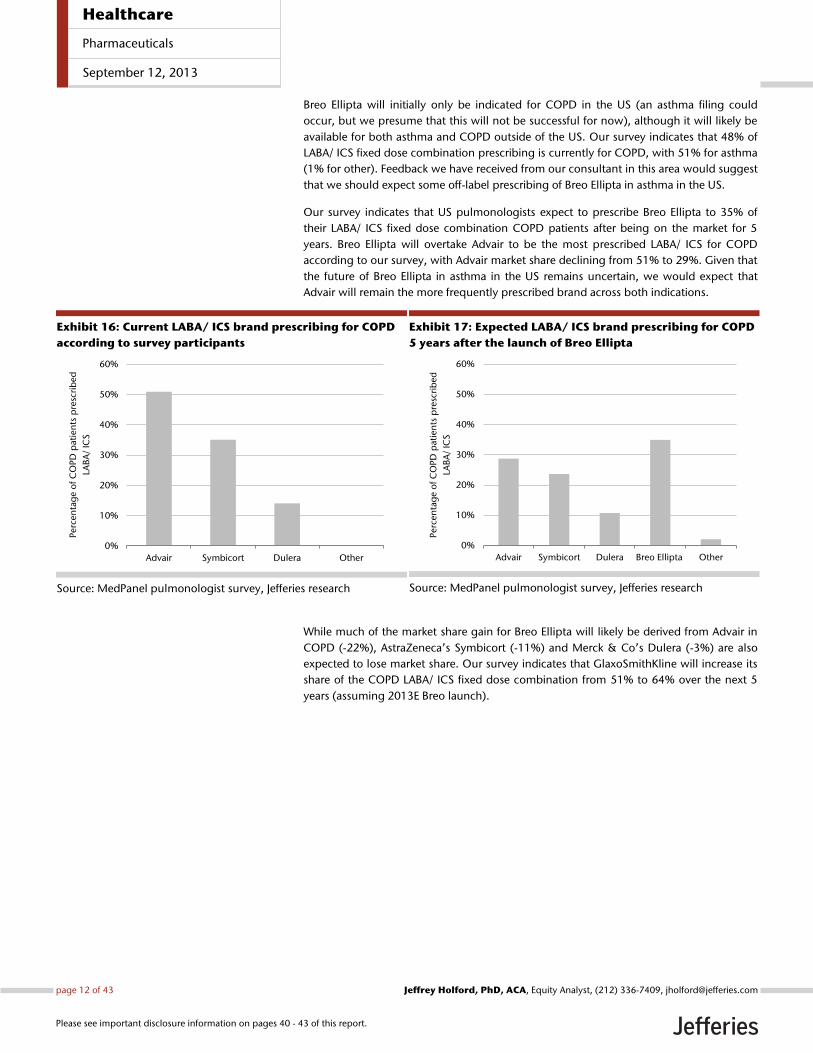
Our survey indicates that US pulmonologists expect to prescribe Breo Ellipta to 35% of
their LABA/ ICS fixed dose combination COPD patients after being on the market for 5
years. Breo Ellipta will overtake Advair to be the most prescribed LABA/ ICS for COPD
according to our survey, with Advair market share declining from 51% to 29%. Given that
the future of Breo Ellipta in asthma in the US remains uncertain, we would expect that
Advair will remain the more frequently prescribed brand across both indications.
Exhibit 16: Current LABA/ ICS brand prescribing for COPD
according to survey participants
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 17: Expected LABA/ ICS brand prescribing for COPD
5 years after the launch of Breo Ellipta
Source: MedPanel pulmonologist survey, Jefferies research
While much of the market share gain for Breo Ellipta will likely be derived from Advair in
COPD (-22%), AstraZeneca’s Symbicort (-11%) and Merck & Co’s Dulera (-3%) are also
expected to lose market share. Our survey indicates that GlaxoSmithKline will increase its
share of the COPD LABA/ ICS fixed dose combination from 51% to 64% over the next 5
years (assuming 2013E Breo launch).
0%
10%
20%
30%
40%
50%
60%
Advair Symbicort Dulera Other
Perc
en
tag
e o
f C
OP
D p
ati
en
ts p
resc
rib
ed
LAB
A/
ICS
0%
10%
20%
30%
40%
50%
60%
Advair Symbicort Dulera Breo Ellipta Other
Perc
en
tag
e o
f C
OP
D p
ati
en
ts p
resc
rib
ed
LAB
A/
ICS
Healthcare
Pharmaceuticals
September 12, 2013
page 12 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
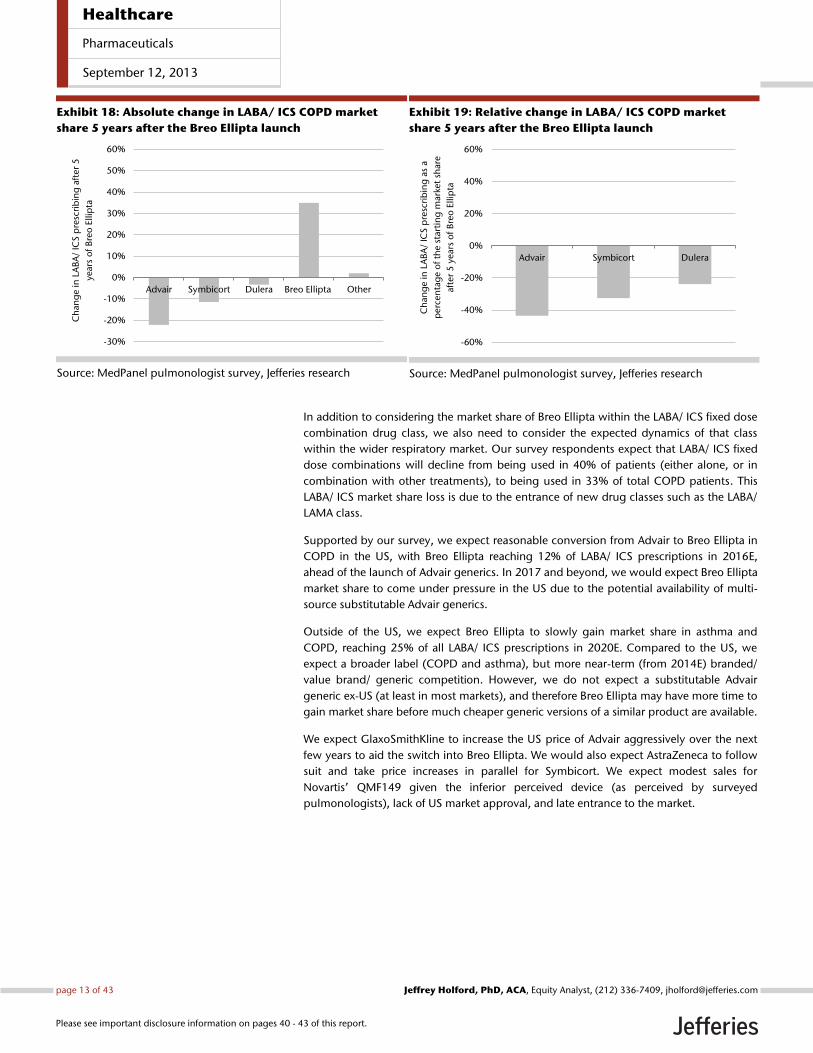
Exhibit 18: Absolute change in LABA/ ICS COPD market
share 5 years after the Breo Ellipta launch
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 19: Relative change in LABA/ ICS COPD market
share 5 years after the Breo Ellipta launch
Source: MedPanel pulmonologist survey, Jefferies research
In addition to considering the market share of Breo Ellipta within the LABA/ ICS fixed dose
combination drug class, we also need to consider the expected dynamics of that class
within the wider respiratory market. Our survey respondents expect that LABA/ ICS fixed
dose combinations will decline from being used in 40% of patients (either alone, or in
combination with other treatments), to being used in 33% of total COPD patients. This
LABA/ ICS market share loss is due to the entrance of new drug classes such as the LABA/
LAMA class.
Supported by our survey, we expect reasonable conversion from Advair to Breo Ellipta in
COPD in the US, with Breo Ellipta reaching 12% of LABA/ ICS prescriptions in 2016E,
ahead of the launch of Advair generics. In 2017 and beyond, we would expect Breo Ellipta
market share to come under pressure in the US due to the potential availability of multi-
source substitutable Advair generics.
Outside of the US, we expect Breo Ellipta to slowly gain market share in asthma and
COPD, reaching 25% of all LABA/ ICS prescriptions in 2020E. Compared to the US, we
expect a broader label (COPD and asthma), but more near-term (from 2014E) branded/
value brand/ generic competition. However, we do not expect a substitutable Advair
generic ex-US (at least in most markets), and therefore Breo Ellipta may have more time to
gain market share before much cheaper generic versions of a similar product are available.
We expect GlaxoSmithKline to increase the US price of Advair aggressively over the next
few years to aid the switch into Breo Ellipta. We would also expect AstraZeneca to follow
suit and take price increases in parallel for Symbicort. We expect modest sales for
Novartis’ QMF149 given the inferior perceived device (as perceived by surveyed
pulmonologists), lack of US market approval, and late entrance to the market.
-30%
-20%
-10%
0%
10%
20%
30%
40%
50%
60%
Advair Symbicort Dulera Breo Ellipta Other
Ch
ang
e in
LA
BA
/ IC
S p
resc
rib
ing
aft
er
5
year
s o
f B
reo
Ellip
ta
-60%
-40%
-20%
0%
20%
40%
60%
Advair Symbicort Dulera
Ch
an
ge in
LA
BA
/ IC
S p
resc
rib
ing
as
a
perc
en
tag
e o
f th
e s
tart
ing
mark
et
share
aft
er
5 y
ears
of
Bre
o E
llip
ta
Healthcare
Pharmaceuticals
September 12, 2013
page 13 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
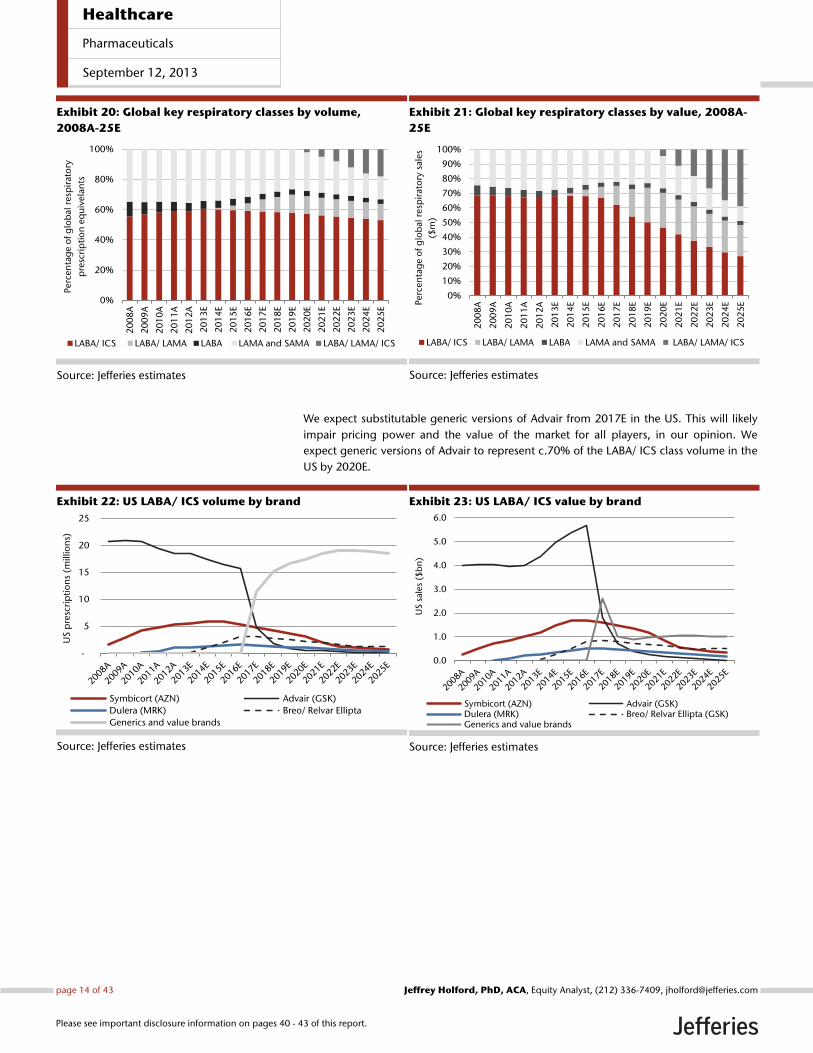
Exhibit 20: Global key respiratory classes by volume,
2008A-25E
Source: Jefferies estimates
Exhibit 21: Global key respiratory classes by value, 2008A-
25E
Source: Jefferies estimates
We expect substitutable generic versions of Advair from 2017E in the US. This will likely
impair pricing power and the value of the market for all players, in our opinion. We
expect generic versions of Advair to represent c.70% of the LABA/ ICS class volume in the
US by 2020E.
Exhibit 22: US LABA/ ICS volume by brand
Source: Jefferies estimates
Exhibit 23: US LABA/ ICS value by brand
Source: Jefferies estimates
0%
20%
40%
60%
80%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Perc
en
tag
e o
f g
lob
al r
esp
irat
ory
pre
scri
pti
on
eq
uiv
ela
nts
LABA/ ICS LABA/ LAMA LABA LAMA and SAMA LABA/ LAMA/ ICS
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
EPerc
en
tag
e o
f g
lob
al
resp
irato
ry s
ale
s
($m
)
LABA/ ICS LABA/ LAMA LABA LAMA and SAMA LABA/ LAMA/ ICS
-
5
10
15
20
25
US
pre
scri
pti
on
s (m
illio
ns)
Symbicort (AZN) Advair (GSK)
Dulera (MRK) Breo/ Relvar Ellipta
Generics and value brands
0.0
1.0
2.0
3.0
4.0
5.0
6.0
US
sale
s ($
bn
)
Symbicort (AZN) Advair (GSK)Dulera (MRK) Breo/ Relvar Ellipta (GSK)Generics and value brands
Healthcare
Pharmaceuticals
September 12, 2013
page 14 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
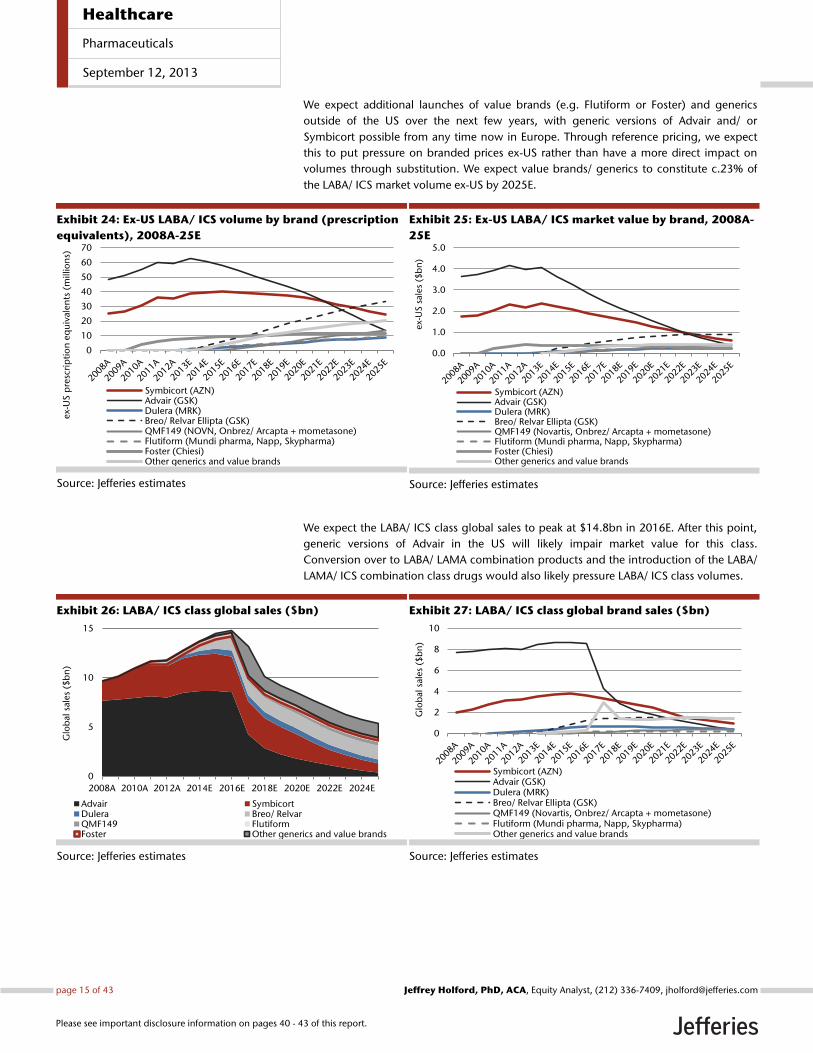
We expect additional launches of value brands (e.g. Flutiform or Foster) and generics
outside of the US over the next few years, with generic versions of Advair and/ or
Symbicort possible from any time now in Europe. Through reference pricing, we expect
this to put pressure on branded prices ex-US rather than have a more direct impact on
volumes through substitution. We expect value brands/ generics to constitute c.23% of
the LABA/ ICS market volume ex-US by 2025E.
Exhibit 24: Ex-US LABA/ ICS volume by brand (prescription
equivalents), 2008A-25E
Source: Jefferies estimates
Exhibit 25: Ex-US LABA/ ICS market value by brand, 2008A-
25E
Source: Jefferies estimates
We expect the LABA/ ICS class global sales to peak at $14.8bn in 2016E. After this point,
generic versions of Advair in the US will likely impair market value for this class.
Conversion over to LABA/ LAMA combination products and the introduction of the LABA/
LAMA/ ICS combination class drugs would also likely pressure LABA/ ICS class volumes.
Exhibit 26: LABA/ ICS class global sales ($bn)
Source: Jefferies estimates
Exhibit 27: LABA/ ICS class global brand sales ($bn)
Source: Jefferies estimates
0
10
20
30
40
50
60
70
ex-
US
pre
scri
pti
on
eq
uiv
alen
ts (
mill
ion
s)
Symbicort (AZN)Advair (GSK)Dulera (MRK)Breo/ Relvar Ellipta (GSK)QMF149 (NOVN, Onbrez/ Arcapta + mometasone)Flutiform (Mundi pharma, Napp, Skypharma)Foster (Chiesi)Other generics and value brands
0.0
1.0
2.0
3.0
4.0
5.0
ex-
US
sale
s ($
bn
)
Symbicort (AZN)Advair (GSK)Dulera (MRK)Breo/ Relvar Ellipta (GSK)QMF149 (Novartis, Onbrez/ Arcapta + mometasone)Flutiform (Mundi pharma, Napp, Skypharma)Foster (Chiesi)Other generics and value brands
0
5
10
15
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sal
es
($b
n)
Advair SymbicortDulera Breo/ RelvarQMF149 FlutiformFoster Other generics and value brands
0
2
4
6
8
10
Glo
bal
sale
s ($
bn
)
Symbicort (AZN)Advair (GSK)Dulera (MRK)Breo/ Relvar Ellipta (GSK)QMF149 (Novartis, Onbrez/ Arcapta + mometasone)Flutiform (Mundi pharma, Napp, Skypharma)Other generics and value brands
Healthcare
Pharmaceuticals
September 12, 2013
page 15 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.

LABA/ LAMA class: Enter Anoro Ellipta
The pulmonologists included in our survey expect to prescribe a LABA/ LAMA fixed dose
combination to c20% of COPD patients in five years’ time. This would either be as a
standalone product, or in combination with an ICS to produce an alternative form of
triple therapy. The majority of patients at low risk of exacerbation (GOLD patient groups A
and B) do not receive ICS treatment at present according to pulmonologists (c.60%).
Feedback from our consultant suggests that treatment with an ICS adds little or no benefit
in these patients, but offers the potential for side effects. Therefore in these patients, a
once-daily LABA/ LAMA could offer a safer, convenient, and effective alternative. Indeed,
this would be in line with the current GOLD recommendations.
At present our survey suggests that c27% and 50% of GOLD patient group A and B
patients, respectively, are receiving an ICS, the majority of which is through use of a
LABA/ ICS fixed dose inhaler. Our consultant suggests that in order to achieved LAMA and
LABA therapy, combining a LABA/ ICS and LAMA is sometimes conducted because of a
lack of good LABA single device options. He also mentioned that the recent launch of
Novartis’ Arcapta/ Onbrez Neohaler/ Breezhaler has meant that combination use with
Spiriva to achieve LABA/ LAMA therapy has become an alternative option in GOLD patient
group A and B patients which do not require ICS treatment. We therefore believe that the
availability a LABA/ LAMA fixed dose combination (starting with GlaxoSmithKline’s Anoro
Ellipta in the US, and Novartis’ QVA149 ex-US) will be welcomed by pulmonologists
because it offers a convenient route to dual therapy in a single modern device.
Triple combination could also be achieved with Anoro Ellipta and potentially a generic
ICS. This would offer potentially a much cheaper option than the most popular route to
achieving this outcome at present which is Advair/ Symbicort + Spiriva. In addition, triple
therapy could be achieved by combining Anoro Ellipta with GlaxoSmithKline’s new ICS
fluticasone furoate (although likely off-label, currently in Phase III for Asthma only), to
achieve triple therapy with once-daily dosing.
The potential to achieve cheaper and more convenient triple therapy, and the formation
of this new class, underpins our expectation for a price premium for Anoro Ellipta over
Advair/ Breo Ellipta (c40% premium to Advair in 2014).
GlaxoSmithKline may have to tread carefully when launching Anoro Ellipta. It would be
potentially damaging to market Anoro as a ‚safer‛ alternative to triple therapy when it
has so much at stake in the LABA/ ICS class. Nevertheless, our survey suggests that a clear
role for LABA/ LAMA monotherapy is present and formation of an alternative triple
therapy regime is also a possibility in the future for patients with different stages of COPD.
We would expect Anoro Ellipta to be the market leading LABA/ LAMA due to its once-daily
dosing, first-to-market status (in the US), and multi-dose DPI device. Novartis’ QVA149 is
likely to be administered twice daily in the US, as is Forest/ Almirall’s Tudorza +
Formoterol, AstraZeneca’s PT003, and Boehringer Ingelheim’s Spiriva + Striverdi.
We would expect aggressive marketing from Forest/ Almirall and Boehringer Ingelheim in
the LABA/ LAMA class. Unlike GlaxoSmithKline/ AstraZeneca, they will potentially be able
to describe ICS use in low exacerbation risk patients as inappropriate when detailing
LABA/ LAMA as a safer option to triple therapy in this patient group. Novartis would also
potentially be able to employ this strategy in the US where it is not expected to file
QMF149 for approval.
We expect the LABA/ LAMA class to peak at 12% of global prescriptions in 2019, and 24%
of global value in the same year. After this point the introduction of LABA/ LAMA/ ICS
class drugs would likely impinge on the LABA/ LAMA class.
Healthcare
Pharmaceuticals
September 12, 2013
page 16 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
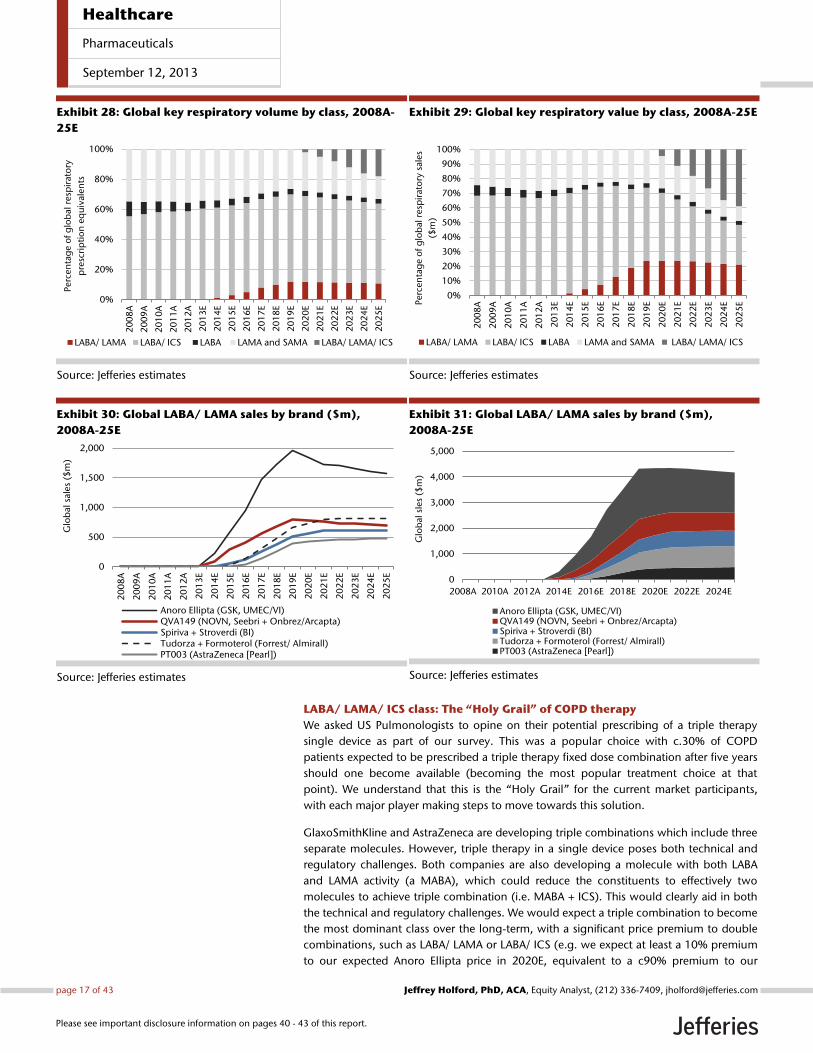
Exhibit 28: Global key respiratory volume by class, 2008A-
25E
Source: Jefferies estimates
Exhibit 29: Global key respiratory value by class, 2008A-25E
Source: Jefferies estimates
Exhibit 30: Global LABA/ LAMA sales by brand ($m),
2008A-25E
Source: Jefferies estimates
Exhibit 31: Global LABA/ LAMA sales by brand ($m),
2008A-25E
Source: Jefferies estimates
LABA/ LAMA/ ICS class: The “Holy Grail” of COPD therapy
We asked US Pulmonologists to opine on their potential prescribing of a triple therapy
single device as part of our survey. This was a popular choice with c.30% of COPD
patients expected to be prescribed a triple therapy fixed dose combination after five years
should one become available (becoming the most popular treatment choice at that
point). We understand that this is the ‚Holy Grail‛ for the current market participants,
with each major player making steps to move towards this solution.
GlaxoSmithKline and AstraZeneca are developing triple combinations which include three
separate molecules. However, triple therapy in a single device poses both technical and
regulatory challenges. Both companies are also developing a molecule with both LABA
and LAMA activity (a MABA), which could reduce the constituents to effectively two
molecules to achieve triple combination (i.e. MABA + ICS). This would clearly aid in both
the technical and regulatory challenges. We would expect a triple combination to become
the most dominant class over the long-term, with a significant price premium to double
combinations, such as LABA/ LAMA or LABA/ ICS (e.g. we expect at least a 10% premium
to our expected Anoro Ellipta price in 2020E, equivalent to a c90% premium to our
0%
20%
40%
60%
80%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Perc
en
tag
e o
f g
lob
al r
esp
irat
ory
pre
scri
pti
on
eq
uiv
alen
ts
LABA/ LAMA LABA/ ICS LABA LAMA and SAMA LABA/ LAMA/ ICS
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
EPerc
en
tag
e o
f g
lob
al r
esp
irat
ory
sale
s
($m
)
LABA/ LAMA LABA/ ICS LABA LAMA and SAMA LABA/ LAMA/ ICS
0
500
1,000
1,500
2,000
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Glo
bal
sale
s ($
m)
Anoro Ellipta (GSK, UMEC/VI)QVA149 (NOVN, Seebri + Onbrez/Arcapta)Spiriva + Stroverdi (BI)Tudorza + Formoterol (Forrest/ Almirall)PT003 (AstraZeneca [Pearl])
0
1,000
2,000
3,000
4,000
5,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sle
s ($
m)
Anoro Ellipta (GSK, UMEC/VI)QVA149 (NOVN, Seebri + Onbrez/Arcapta)Spiriva + Stroverdi (BI)Tudorza + Formoterol (Forrest/ Almirall)PT003 (AstraZeneca [Pearl])
Healthcare
Pharmaceuticals
September 12, 2013
page 17 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
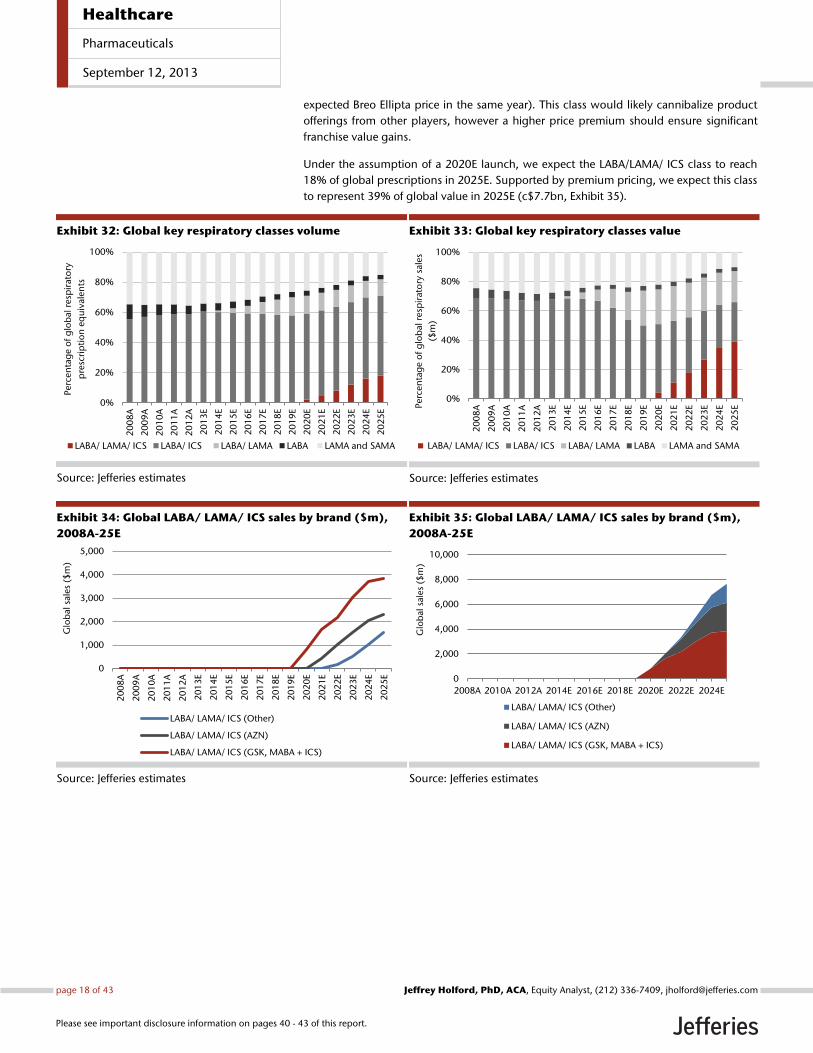
expected Breo Ellipta price in the same year). This class would likely cannibalize product
offerings from other players, however a higher price premium should ensure significant
franchise value gains.
Under the assumption of a 2020E launch, we expect the LABA/LAMA/ ICS class to reach
18% of global prescriptions in 2025E. Supported by premium pricing, we expect this class
to represent 39% of global value in 2025E (c$7.7bn, Exhibit 35).
Exhibit 32: Global key respiratory classes volume
Source: Jefferies estimates
Exhibit 33: Global key respiratory classes value
Source: Jefferies estimates
Exhibit 34: Global LABA/ LAMA/ ICS sales by brand ($m),
2008A-25E
Source: Jefferies estimates
Exhibit 35: Global LABA/ LAMA/ ICS sales by brand ($m),
2008A-25E
Source: Jefferies estimates
0%
20%
40%
60%
80%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Perc
en
tag
e o
f g
lob
al r
esp
irat
ory
pre
scri
pti
on
eq
uiv
alen
ts
LABA/ LAMA/ ICS LABA/ ICS LABA/ LAMA LABA LAMA and SAMA
0%
20%
40%
60%
80%
100%
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
EPerc
en
tag
e o
f g
lob
al r
esp
irat
ory
sale
s
($m
)
LABA/ LAMA/ ICS LABA/ ICS LABA/ LAMA LABA LAMA and SAMA
0
1,000
2,000
3,000
4,000
5,000
20
08
A
20
09
A
20
10
A
20
11
A
20
12
A
20
13
E
20
14
E
20
15
E
20
16
E
20
17
E
20
18
E
20
19
E
20
20
E
20
21
E
20
22
E
20
23
E
20
24
E
20
25
E
Glo
bal
sale
s ($
m)
LABA/ LAMA/ ICS (Other)
LABA/ LAMA/ ICS (AZN)
LABA/ LAMA/ ICS (GSK, MABA + ICS)
0
2,000
4,000
6,000
8,000
10,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sale
s ($
m)
LABA/ LAMA/ ICS (Other)
LABA/ LAMA/ ICS (AZN)
LABA/ LAMA/ ICS (GSK, MABA + ICS)
Healthcare
Pharmaceuticals
September 12, 2013
page 18 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
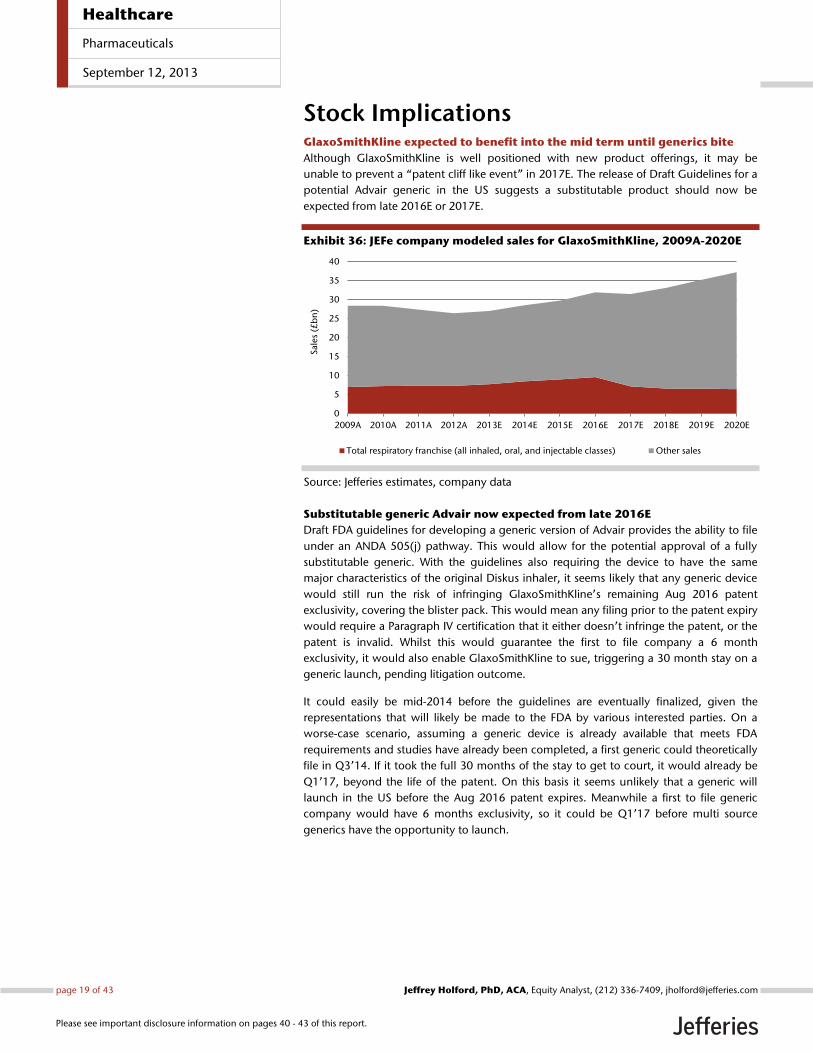
Stock Implications GlaxoSmithKline expected to benefit into the mid term until generics bite
Although GlaxoSmithKline is well positioned with new product offerings, it may be
unable to prevent a ‚patent cliff like event‛ in 2017E. The release of Draft Guidelines for a
potential Advair generic in the US suggests a substitutable product should now be
expected from late 2016E or 2017E.
Exhibit 36: JEFe company modeled sales for GlaxoSmithKline, 2009A-2020E
Source: Jefferies estimates, company data
Substitutable generic Advair now expected from late 2016E
Draft FDA guidelines for developing a generic version of Advair provides the ability to file
under an ANDA 505(j) pathway. This would allow for the potential approval of a fully
substitutable generic. With the guidelines also requiring the device to have the same
major characteristics of the original Diskus inhaler, it seems likely that any generic device
would still run the risk of infringing GlaxoSmithKline’s remaining Aug 2016 patent
exclusivity, covering the blister pack. This would mean any filing prior to the patent expiry
would require a Paragraph IV certification that it either doesn’t infringe the patent, or the
patent is invalid. Whilst this would guarantee the first to file company a 6 month
exclusivity, it would also enable GlaxoSmithKline to sue, triggering a 30 month stay on a
generic launch, pending litigation outcome.
It could easily be mid-2014 before the guidelines are eventually finalized, given the
representations that will likely be made to the FDA by various interested parties. On a
worse-case scenario, assuming a generic device is already available that meets FDA
requirements and studies have already been completed, a first generic could theoretically
file in Q3’14. If it took the full 30 months of the stay to get to court, it would already be
Q1’17, beyond the life of the patent. On this basis it seems unlikely that a generic will
launch in the US before the Aug 2016 patent expires. Meanwhile a first to file generic
company would have 6 months exclusivity, so it could be Q1’17 before multi source
generics have the opportunity to launch.
0
5
10
15
20
25
30
35
40
2009A 2010A 2011A 2012A 2013E 2014E 2015E 2016E 2017E 2018E 2019E 2020E
Sale
s (£
bn
)
Total respiratory franchise (all inhaled, oral, and injectable classes) Other sales
Healthcare
Pharmaceuticals
September 12, 2013
page 19 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.

A number of generic companies have been looking at developing inhaled generic DPI
products for some time now, including Novartis’ Sandoz and Mylan. Following disclosure
of the draft guidelines John Sheehan, the CFO of Mylan, was quoted at the Morgan
Stanley Global Healthcare Conference on 10th September 2013, saying:
“…the guidance…is exactly in line with what we had indicated our discussions with the FDA –
were, and so, fully anticipated from our side”. “Our device…..has been examined by the FDA.
Our program has been validated as a AB-rated program, generically substitutable program.
And so, we are definitely moving down the path for a generic form of Advair.”
This implies that as long as the final guidelines do not have any major changes in them,
Mylan would appear to be well advanced. Sheehan went on to say;
“….this is going to be a hard to formulate product, hard to manufacture that's where
Mylan's expertise has typically been and therefore we believe that this will be a market that
still have a small number of players and as a result that there will be significant value….”.
He later clarified that Mylan expected “the launch of a generic Advair in 2016”.
This further confirms the expectation that we could have a US generic shortly after the
remaining Advair patent expires. Even if the assertion that it is hard to formulate and
manufacture is correct, even a ‘small number of players’ will still have a devastating effect
on pricing as they fight for market share. Lovenox would serve as a good example to
prove the point here, in our view.
Positive Anoro AdCom vote and supportive class expectations from our survey
Following the near unanimous vote for approval by the FDA’s Advisory committee panel
on September 10th, Anoro Ellipta is very likely to offer first-to-market status in the US, will
likely be the only once-daily LABA/ LAMA on the US market and uses a best-in-class
device, in our opinion. Novartis will present competition ex-US, where QVA149 (Ultibro)
will be first-to-market and once-daily, although our surveyed pulmonologists appeared
less convinced regarding the Neohaler/ Breezhaler device it uses.
We expect GlaxoSmithKline to price Anoro Ellipta at a significant premium to Advair or
Breo Ellipta and our surveyed pulmonologists expect to prescribe a LABA/ LAMA fixed
dose combination to c20% of COPD patients in five years’ time. Much of the market share
for Anoro Ellipta will be gained from patients who would have been prescribed two
branded products (Advair + Spiriva for example), therefore a higher price should be
justified. Some market share for GlaxoSmithKline’s LABA/ ICSs’ Advair and Breo Ellipta
may be lost to Anoro Ellipta in COPD, but this should be a positive event given our
expected higher price point for Anoro Ellipta.
Breo Ellipta offers a chance to protect some of the franchise, but not enough
Breo Ellipta offers once-daily LABA/ ICS therapy for COPD patients in the US, and
potentially for both COPD and asthma patients ex-US. 74% of surveyed pulmonologists
were aware of Breo Ellipta prior to the product’s launch, and noted convenience and
compliance as key attributes. We expect GlaxoSmithKline to employ a price-driven
switching strategy from Advair, helping to protect the franchise from potential Advair
generics and value brands. We expect a key part of this strategy to include significant
price increases for Advair from the point of launch, encouraging switching and providing
a near term boost to overall franchise sales. GlaxoSmithKline is also well positioned to
reach the COPD ‚holy grail‛ of triple therapy in a single device. This could be through its
new LABA, LAMA, and ICS molecules or through development of MABA in combination
with an ICS.
Healthcare
Pharmaceuticals
September 12, 2013
page 20 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
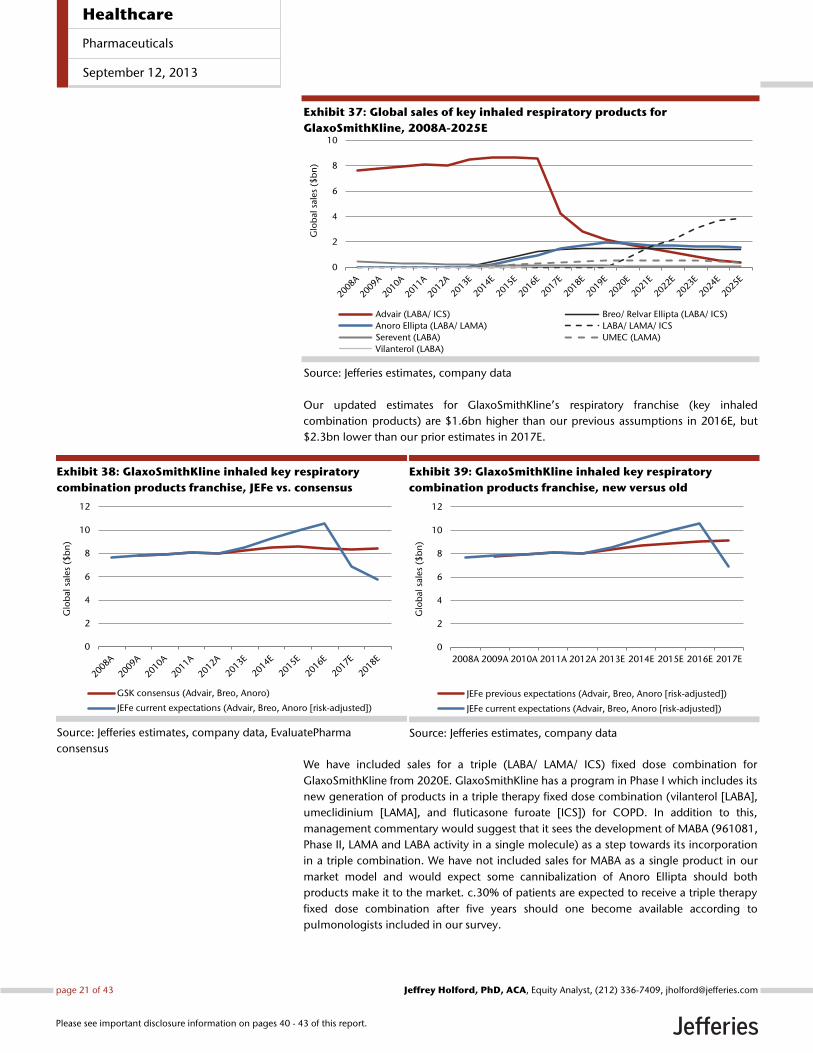
Exhibit 37: Global sales of key inhaled respiratory products for
GlaxoSmithKline, 2008A-2025E
Source: Jefferies estimates, company data
Our updated estimates for GlaxoSmithKline’s respiratory franchise (key inhaled
combination products) are $1.6bn higher than our previous assumptions in 2016E, but
$2.3bn lower than our prior estimates in 2017E.
Exhibit 38: GlaxoSmithKline inhaled key respiratory
combination products franchise, JEFe vs. consensus
Source: Jefferies estimates, company data, EvaluatePharma
consensus
Exhibit 39: GlaxoSmithKline inhaled key respiratory
combination products franchise, new versus old
Source: Jefferies estimates, company data
We have included sales for a triple (LABA/ LAMA/ ICS) fixed dose combination for
GlaxoSmithKline from 2020E. GlaxoSmithKline has a program in Phase I which includes its
new generation of products in a triple therapy fixed dose combination (vilanterol [LABA],
umeclidinium [LAMA], and fluticasone furoate [ICS]) for COPD. In addition to this,
management commentary would suggest that it sees the development of MABA (961081,
Phase II, LAMA and LABA activity in a single molecule) as a step towards its incorporation
in a triple combination. We have not included sales for MABA as a single product in our
market model and would expect some cannibalization of Anoro Ellipta should both
products make it to the market. c.30% of patients are expected to receive a triple therapy
fixed dose combination after five years should one become available according to
pulmonologists included in our survey.
0
2
4
6
8
10
Glo
bal
sale
s ($
bn
)Advair (LABA/ ICS) Breo/ Relvar Ellipta (LABA/ ICS)
Anoro Ellipta (LABA/ LAMA) LABA/ LAMA/ ICS
Serevent (LABA) UMEC (LAMA)
Vilanterol (LABA)
0
2
4
6
8
10
12
Glo
bal
sale
s ($
bn
)
GSK consensus (Advair, Breo, Anoro)
JEFe current expectations (Advair, Breo, Anoro [risk-adjusted])
0
2
4
6
8
10
12
2008A 2009A 2010A 2011A 2012A 2013E 2014E 2015E 2016E 2017E
Glo
bal
sale
s ($
bn
)
JEFe previous expectations (Advair, Breo, Anoro [risk-adjusted])
JEFe current expectations (Advair, Breo, Anoro [risk-adjusted])
Healthcare
Pharmaceuticals
September 12, 2013
page 21 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
GlaxoSmithKline is also investigating umeclidinium (LAMA) and fluticasone furoate (ICS)
in a fixed dose combination for asthma in Phase II. With a lack of LAMA data in asthma to
date, we have not included sales for LAMA or its combinations for asthma within our
market model and therefore it could present some upside to our estimates.
GlaxoSmithKline is also investigating fluticasone furoate (ICS) as a single product for
asthma. We have not specifically included sales for this product in our market model, with
the ICS class sales included as a single class line. This class generated $3bn in sales in
2012A according to IMS health. We would see fluticasone furoate as a useful once-daily
option, especially if combined with a once daily LABA/ LAMA such as Anoro Ellipta to
produce an alternative triple therapy regime.
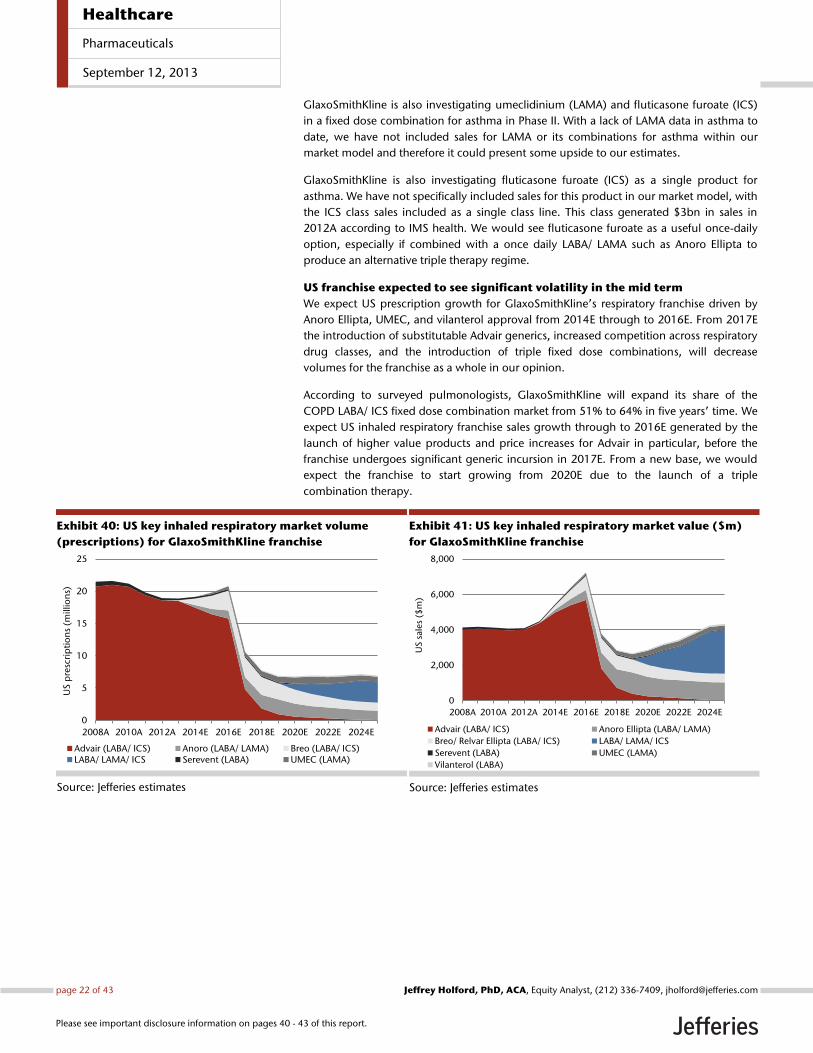
US franchise expected to see significant volatility in the mid term
We expect US prescription growth for GlaxoSmithKline’s respiratory franchise driven by
Anoro Ellipta, UMEC, and vilanterol approval from 2014E through to 2016E. From 2017E
the introduction of substitutable Advair generics, increased competition across respiratory
drug classes, and the introduction of triple fixed dose combinations, will decrease
volumes for the franchise as a whole in our opinion.
According to surveyed pulmonologists, GlaxoSmithKline will expand its share of the
COPD LABA/ ICS fixed dose combination market from 51% to 64% in five years’ time. We
expect US inhaled respiratory franchise sales growth through to 2016E generated by the
launch of higher value products and price increases for Advair in particular, before the
franchise undergoes significant generic incursion in 2017E. From a new base, we would
expect the franchise to start growing from 2020E due to the launch of a triple
combination therapy.
Exhibit 40: US key inhaled respiratory market volume
(prescriptions) for GlaxoSmithKline franchise
Source: Jefferies estimates
Exhibit 41: US key inhaled respiratory market value ($m)
for GlaxoSmithKline franchise
Source: Jefferies estimates
0
5
10
15
20
25
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
US
pre
scri
pti
on
s (m
illio
ns)
Advair (LABA/ ICS) Anoro (LABA/ LAMA) Breo (LABA/ ICS)LABA/ LAMA/ ICS Serevent (LABA) UMEC (LAMA)
0
2,000
4,000
6,000
8,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
US
sale
s ($
m)
Advair (LABA/ ICS) Anoro Ellipta (LABA/ LAMA)
Breo/ Relvar Ellipta (LABA/ ICS) LABA/ LAMA/ ICS
Serevent (LABA) UMEC (LAMA)
Vilanterol (LABA)
Healthcare
Pharmaceuticals
September 12, 2013
page 22 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
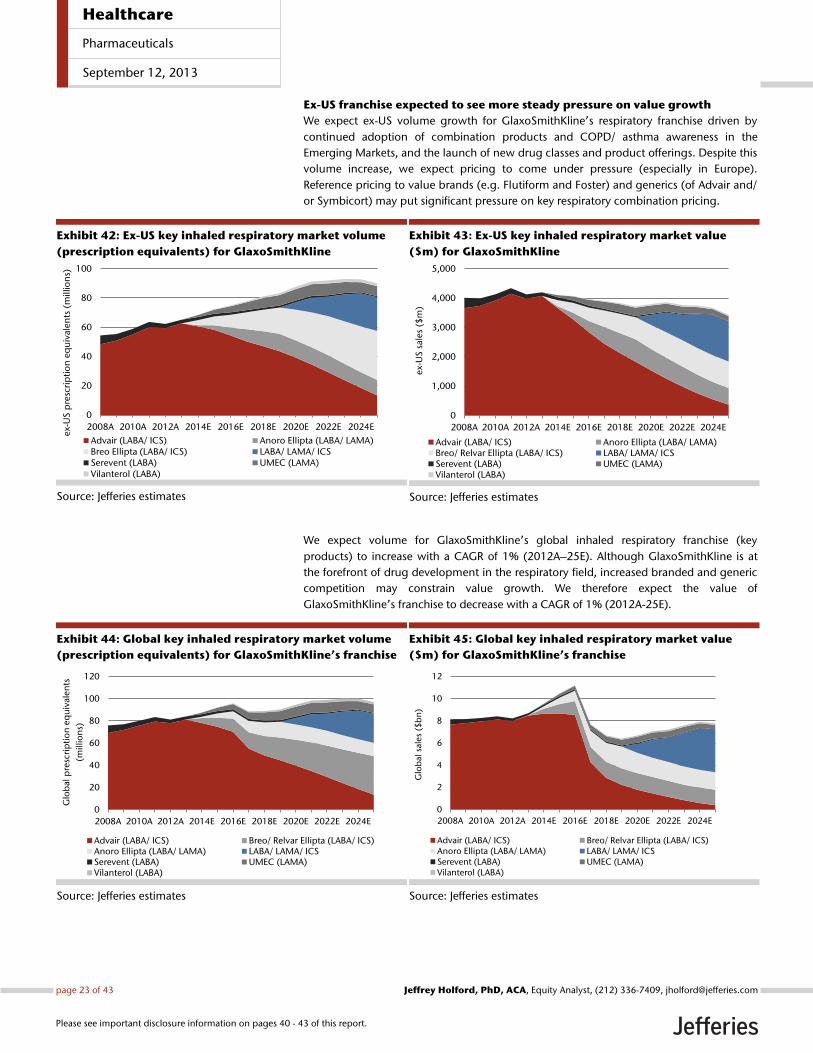
Ex-US franchise expected to see more steady pressure on value growth
We expect ex-US volume growth for GlaxoSmithKline’s respiratory franchise driven by
continued adoption of combination products and COPD/ asthma awareness in the
Emerging Markets, and the launch of new drug classes and product offerings. Despite this
volume increase, we expect pricing to come under pressure (especially in Europe).
Reference pricing to value brands (e.g. Flutiform and Foster) and generics (of Advair and/
or Symbicort) may put significant pressure on key respiratory combination pricing.
Exhibit 42: Ex-US key inhaled respiratory market volume
(prescription equivalents) for GlaxoSmithKline
Source: Jefferies estimates
Exhibit 43: Ex-US key inhaled respiratory market value
($m) for GlaxoSmithKline
Source: Jefferies estimates
We expect volume for GlaxoSmithKline’s global inhaled respiratory franchise (key
products) to increase with a CAGR of 1% (2012A–25E). Although GlaxoSmithKline is at
the forefront of drug development in the respiratory field, increased branded and generic
competition may constrain value growth. We therefore expect the value of
GlaxoSmithKline’s franchise to decrease with a CAGR of 1% (2012A-25E).
Exhibit 44: Global key inhaled respiratory market volume
(prescription equivalents) for GlaxoSmithKline’s franchise
Source: Jefferies estimates
Exhibit 45: Global key inhaled respiratory market value
($m) for GlaxoSmithKline’s franchise
Source: Jefferies estimates
0
20
40
60
80
100
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
ex-
US
pre
scri
pti
on
eq
uiv
alen
ts (
mill
ion
s)
Advair (LABA/ ICS) Anoro Ellipta (LABA/ LAMA)Breo Ellipta (LABA/ ICS) LABA/ LAMA/ ICSSerevent (LABA) UMEC (LAMA)Vilanterol (LABA)
0
1,000
2,000
3,000
4,000
5,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024Eex-
US
sale
s ($
m)
Advair (LABA/ ICS) Anoro Ellipta (LABA/ LAMA)Breo/ Relvar Ellipta (LABA/ ICS) LABA/ LAMA/ ICSSerevent (LABA) UMEC (LAMA)Vilanterol (LABA)
0
20
40
60
80
100
120
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
pre
scri
pti
on
eq
uiv
alen
ts
(mill
ion
s)
Advair (LABA/ ICS) Breo/ Relvar Ellipta (LABA/ ICS)Anoro Ellipta (LABA/ LAMA) LABA/ LAMA/ ICSSerevent (LABA) UMEC (LAMA)Vilanterol (LABA)
0
2
4
6
8
10
12
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sale
s ($
bn
)
Advair (LABA/ ICS) Breo/ Relvar Ellipta (LABA/ ICS)Anoro Ellipta (LABA/ LAMA) LABA/ LAMA/ ICSSerevent (LABA) UMEC (LAMA)Vilanterol (LABA)
Healthcare
Pharmaceuticals
September 12, 2013
page 23 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
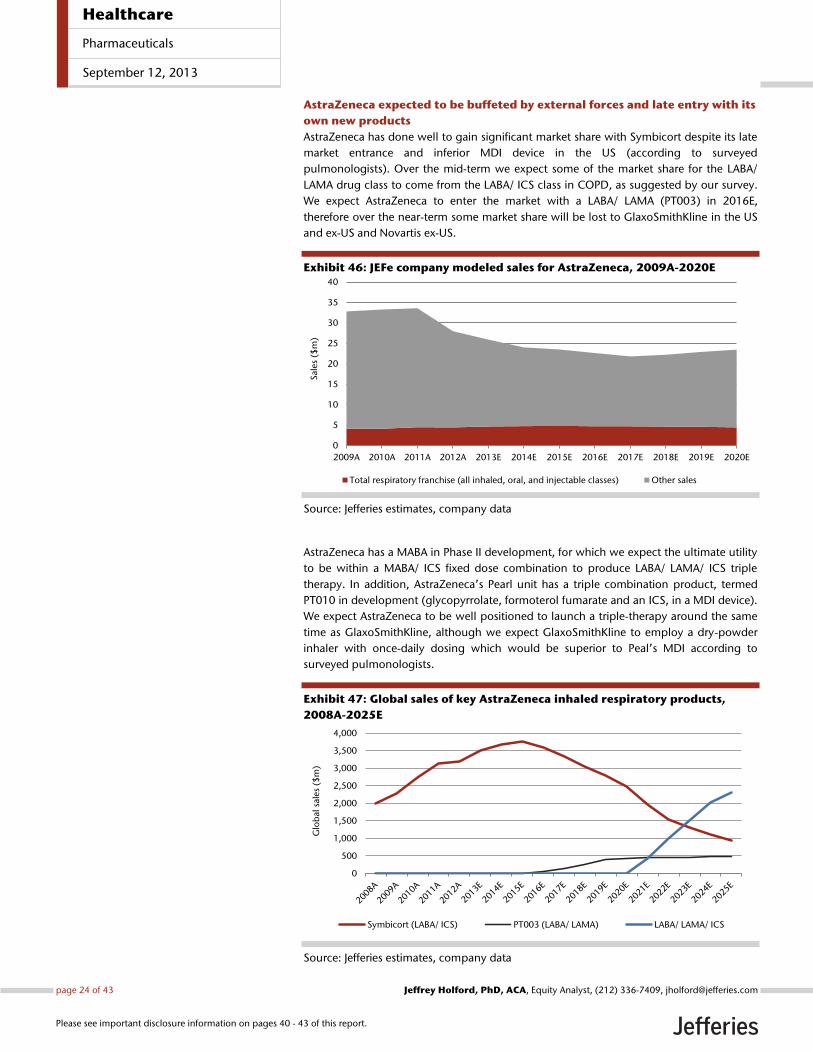
AstraZeneca expected to be buffeted by external forces and late entry with its
own new products
AstraZeneca has done well to gain significant market share with Symbicort despite its late
market entrance and inferior MDI device in the US (according to surveyed
pulmonologists). Over the mid-term we expect some of the market share for the LABA/
LAMA drug class to come from the LABA/ ICS class in COPD, as suggested by our survey.
We expect AstraZeneca to enter the market with a LABA/ LAMA (PT003) in 2016E,
therefore over the near-term some market share will be lost to GlaxoSmithKline in the US
and ex-US and Novartis ex-US.
Exhibit 46: JEFe company modeled sales for AstraZeneca, 2009A-2020E
Source: Jefferies estimates, company data
AstraZeneca has a MABA in Phase II development, for which we expect the ultimate utility
to be within a MABA/ ICS fixed dose combination to produce LABA/ LAMA/ ICS triple
therapy. In addition, AstraZeneca’s Pearl unit has a triple combination product, termed
PT010 in development (glycopyrrolate, formoterol fumarate and an ICS, in a MDI device).
We expect AstraZeneca to be well positioned to launch a triple-therapy around the same
time as GlaxoSmithKline, although we expect GlaxoSmithKline to employ a dry-powder
inhaler with once-daily dosing which would be superior to Peal’s MDI according to
surveyed pulmonologists.
Exhibit 47: Global sales of key AstraZeneca inhaled respiratory products,
2008A-2025E
Source: Jefferies estimates, company data
0
5
10
15
20
25
30
35
40
2009A 2010A 2011A 2012A 2013E 2014E 2015E 2016E 2017E 2018E 2019E 2020E
Sale
s ($
m)
Total respiratory franchise (all inhaled, oral, and injectable classes) Other sales
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
Glo
bal
sale
s ($
m)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
Healthcare
Pharmaceuticals
September 12, 2013
page 24 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
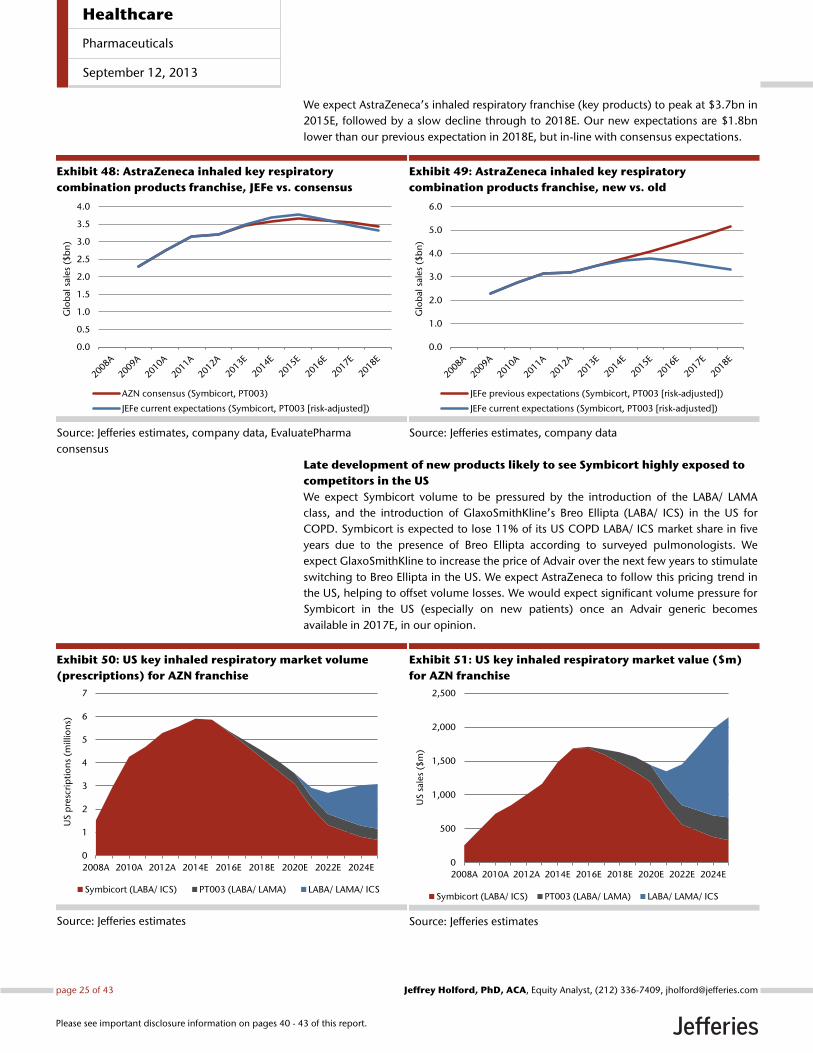
We expect AstraZeneca’s inhaled respiratory franchise (key products) to peak at $3.7bn in
2015E, followed by a slow decline through to 2018E. Our new expectations are $1.8bn
lower than our previous expectation in 2018E, but in-line with consensus expectations.
Exhibit 48: AstraZeneca inhaled key respiratory
combination products franchise, JEFe vs. consensus
Source: Jefferies estimates, company data, EvaluatePharma
consensus
Exhibit 49: AstraZeneca inhaled key respiratory
combination products franchise, new vs. old
Source: Jefferies estimates, company data
Late development of new products likely to see Symbicort highly exposed to
competitors in the US
We expect Symbicort volume to be pressured by the introduction of the LABA/ LAMA
class, and the introduction of GlaxoSmithKline’s Breo Ellipta (LABA/ ICS) in the US for
COPD. Symbicort is expected to lose 11% of its US COPD LABA/ ICS market share in five
years due to the presence of Breo Ellipta according to surveyed pulmonologists. We
expect GlaxoSmithKline to increase the price of Advair over the next few years to stimulate
switching to Breo Ellipta in the US. We expect AstraZeneca to follow this pricing trend in
the US, helping to offset volume losses. We would expect significant volume pressure for
Symbicort in the US (especially on new patients) once an Advair generic becomes
available in 2017E, in our opinion.
Exhibit 50: US key inhaled respiratory market volume
(prescriptions) for AZN franchise
Source: Jefferies estimates
Exhibit 51: US key inhaled respiratory market value ($m)
for AZN franchise
Source: Jefferies estimates
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Glo
bal
sale
s ($
bn
)
AZN consensus (Symbicort, PT003)
JEFe current expectations (Symbicort, PT003 [risk-adjusted])
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Glo
bal
sale
s ($
bn
)
JEFe previous expectations (Symbicort, PT003 [risk-adjusted])
JEFe current expectations (Symbicort, PT003 [risk-adjusted])
0
1
2
3
4
5
6
7
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
US
pre
scri
pti
on
s (m
illio
ns)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
0
500
1,000
1,500
2,000
2,500
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
US
sale
s ($
m)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
Healthcare
Pharmaceuticals
September 12, 2013
page 25 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
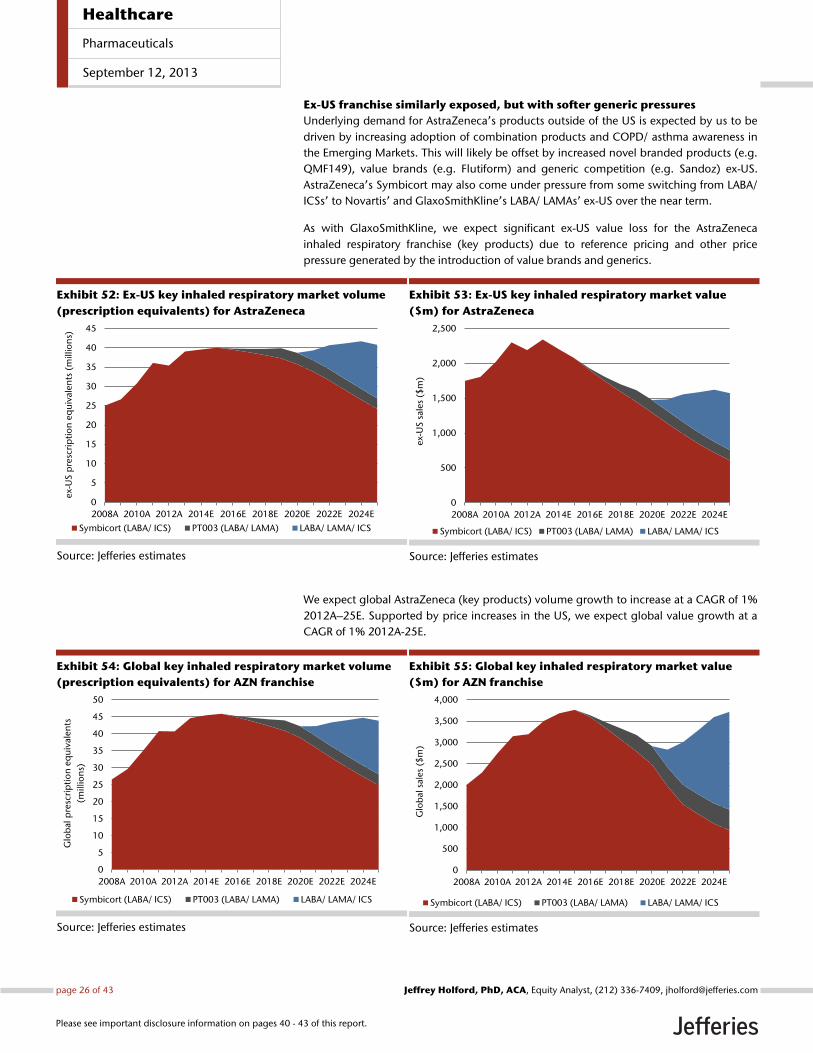
Ex-US franchise similarly exposed, but with softer generic pressures
Underlying demand for AstraZeneca’s products outside of the US is expected by us to be
driven by increasing adoption of combination products and COPD/ asthma awareness in
the Emerging Markets. This will likely be offset by increased novel branded products (e.g.
QMF149), value brands (e.g. Flutiform) and generic competition (e.g. Sandoz) ex-US.
AstraZeneca’s Symbicort may also come under pressure from some switching from LABA/
ICSs’ to Novartis’ and GlaxoSmithKline’s LABA/ LAMAs’ ex-US over the near term.
As with GlaxoSmithKline, we expect significant ex-US value loss for the AstraZeneca
inhaled respiratory franchise (key products) due to reference pricing and other price
pressure generated by the introduction of value brands and generics.
Exhibit 52: Ex-US key inhaled respiratory market volume
(prescription equivalents) for AstraZeneca
Source: Jefferies estimates
Exhibit 53: Ex-US key inhaled respiratory market value
($m) for AstraZeneca
Source: Jefferies estimates
We expect global AstraZeneca (key products) volume growth to increase at a CAGR of 1%
2012A–25E. Supported by price increases in the US, we expect global value growth at a
CAGR of 1% 2012A-25E.
Exhibit 54: Global key inhaled respiratory market volume
(prescription equivalents) for AZN franchise
Source: Jefferies estimates
Exhibit 55: Global key inhaled respiratory market value
($m) for AZN franchise
Source: Jefferies estimates
0
5
10
15
20
25
30
35
40
45
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
ex-
US
pre
scri
pti
on
eq
uiv
alen
ts (
mill
ion
s)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
0
500
1,000
1,500
2,000
2,500
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
ex-
US
sal
es
($m
)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
0
5
10
15
20
25
30
35
40
45
50
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
pre
scri
pti
on
eq
uiv
alen
ts
(mill
ion
s)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sale
s ($
m)
Symbicort (LABA/ ICS) PT003 (LABA/ LAMA) LABA/ LAMA/ ICS
Healthcare
Pharmaceuticals
September 12, 2013
page 26 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.

Branded respiratory products unlikely to be a major success in the long term
for Novartis
Novartis is a relatively new entrant in the inhaled respiratory disease area. Surveyed
pulmonologists were not overly impressed with Novartis’ Neohaler/ Breezhaler device,
which is being employed across its product portfolio. This may be a missed opportunity in
our opinion, as are the regulatory challenges that the company has faced in the US. We
do not expect a significant revenue opportunity for Arcapta/ Onbrez (LABA) or Seebri
(LAMA). Both products offer little advantage over existing therapies, will be facing
competition from GlaxoSmithKline with vilanterol and UMEC, respectively, and are
entering a market at the point when further combinations will erode single product sales
(LABA/ LAMA class development).
Exhibit 56: JEFe company modeled sales for Novartis, 2009A-2020E
Source: Jefferies estimates, company data
We have not explicitly forecast revenues for Novartis’ Sandoz business unit to benefit from
launching generic versions of key respiratory products (e.g. Advair or/ and Symbicort) in
our market model, although this opportunity is included within our revenue estimates for
Sandoz and Novartis as a whole. It is worth pointing out that we expect generic versions
of LABA/ ICS’s to generate c$1.4bn globally in 2020E (and a one-off peak of $3bn globally
in 2017E, driven by a higher price point for first-to-file status in the US for one generic
player). It would seem likely that Sandoz would be a significant participant in this market,
in our view.
As a viable alternative to multi-blockbuster Spiriva, Seebri is a welcomed addition to the
pulmonologist’s armory, but the opportunity to capitalize on this ahead of fixed dose
combinations and the launch of GlaxoSmithKline’s UMEC was lost in the US when further
dose finding studies were required. QVA149 received a positive CHMP recommendation
in July 2013, and therefore will likely be a first-to-market LABA/ LAMA in Europe. It is also
dosed once-daily in Europe. In the US, further dose finding studies were required, we
expect QVA149 to be ultimately approved as a twice-daily product in the US, with launch
not until 2015. QMF149 (LABA/ ICS) offers further potential ex-US, but is unlikely to be
filed in the US.
0
10
20
30
40
50
60
70
80
2010A 2011A 2012A 2013E 2014E 2015E 2016E 2017E 2018E 2019E 2020E
Sale
s ($
bn
)
Total respiratory franchise (all inhaled, oral, and injectable classes) Other sales
Healthcare
Pharmaceuticals
September 12, 2013
page 27 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
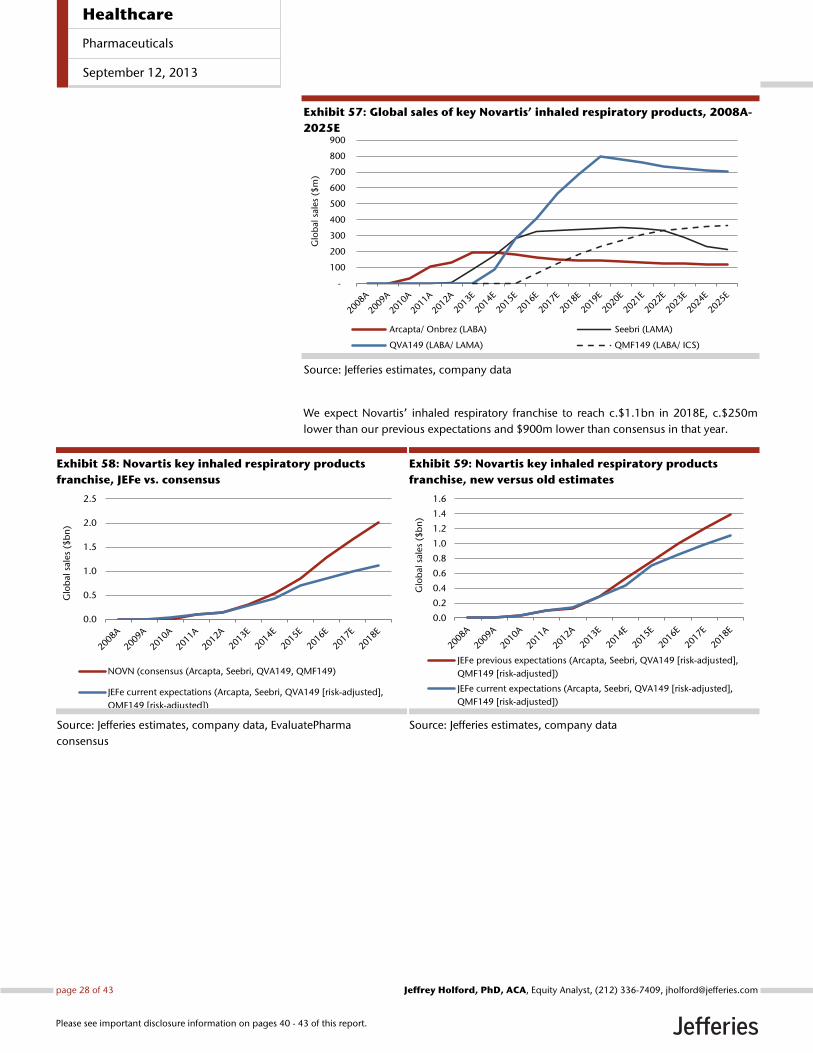
Exhibit 57: Global sales of key Novartis’ inhaled respiratory products, 2008A-
2025E
Source: Jefferies estimates, company data
We expect Novartis’ inhaled respiratory franchise to reach c.$1.1bn in 2018E, c.$250m
lower than our previous expectations and $900m lower than consensus in that year.
Exhibit 58: Novartis key inhaled respiratory products
franchise, JEFe vs. consensus
Source: Jefferies estimates, company data, EvaluatePharma
consensus
Exhibit 59: Novartis key inhaled respiratory products
franchise, new versus old estimates
Source: Jefferies estimates, company data
-
100
200
300
400
500
600
700
800
900
Glo
bal
sale
s ($
m)
Arcapta/ Onbrez (LABA) Seebri (LAMA)
QVA149 (LABA/ LAMA) QMF149 (LABA/ ICS)
0.0
0.5
1.0
1.5
2.0
2.5
Glo
bal
sale
s ($
bn
)
NOVN (consensus (Arcapta, Seebri, QVA149, QMF149)
JEFe current expectations (Arcapta, Seebri, QVA149 [risk-adjusted],
QMF149 [risk-adjusted])
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
Glo
bal
sale
s ($
bn
)
JEFe previous expectations (Arcapta, Seebri, QVA149 [risk-adjusted],
QMF149 [risk-adjusted])
JEFe current expectations (Arcapta, Seebri, QVA149 [risk-adjusted],
QMF149 [risk-adjusted])
Healthcare
Pharmaceuticals
September 12, 2013
page 28 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
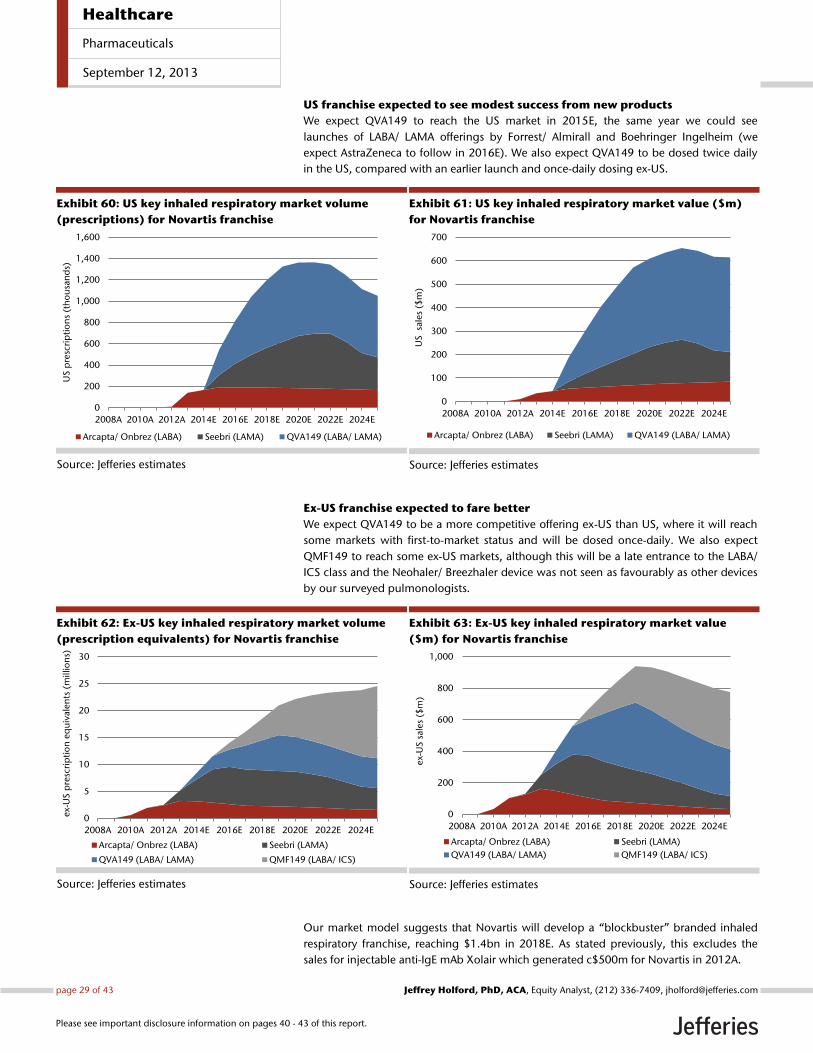
US franchise expected to see modest success from new products
We expect QVA149 to reach the US market in 2015E, the same year we could see
launches of LABA/ LAMA offerings by Forrest/ Almirall and Boehringer Ingelheim (we
expect AstraZeneca to follow in 2016E). We also expect QVA149 to be dosed twice daily
in the US, compared with an earlier launch and once-daily dosing ex-US.
Exhibit 60: US key inhaled respiratory market volume
(prescriptions) for Novartis franchise
Source: Jefferies estimates
Exhibit 61: US key inhaled respiratory market value ($m)
for Novartis franchise
Source: Jefferies estimates
Ex-US franchise expected to fare better
We expect QVA149 to be a more competitive offering ex-US than US, where it will reach
some markets with first-to-market status and will be dosed once-daily. We also expect
QMF149 to reach some ex-US markets, although this will be a late entrance to the LABA/
ICS class and the Neohaler/ Breezhaler device was not seen as favourably as other devices
by our surveyed pulmonologists.
Exhibit 62: Ex-US key inhaled respiratory market volume
(prescription equivalents) for Novartis franchise
Source: Jefferies estimates
Exhibit 63: Ex-US key inhaled respiratory market value
($m) for Novartis franchise
Source: Jefferies estimates
Our market model suggests that Novartis will develop a ‚blockbuster‛ branded inhaled
respiratory franchise, reaching $1.4bn in 2018E. As stated previously, this excludes the
sales for injectable anti-IgE mAb Xolair which generated c$500m for Novartis in 2012A.
0
200
400
600
800
1,000
1,200
1,400
1,600
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
US
pre
scri
pti
on
s (t
ho
usa
nd
s)
Arcapta/ Onbrez (LABA) Seebri (LAMA) QVA149 (LABA/ LAMA)
0
100
200
300
400
500
600
700
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024EU
S
sale
s ($
m)
Arcapta/ Onbrez (LABA) Seebri (LAMA) QVA149 (LABA/ LAMA)
0
5
10
15
20
25
30
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
ex-
US
pre
scri
pti
on
eq
uiv
alen
ts (
mill
ion
s)
Arcapta/ Onbrez (LABA) Seebri (LAMA)
QVA149 (LABA/ LAMA) QMF149 (LABA/ ICS)
0
200
400
600
800
1,000
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
ex-
US
sale
s ($
m)
Arcapta/ Onbrez (LABA) Seebri (LAMA)
QVA149 (LABA/ LAMA) QMF149 (LABA/ ICS)
Healthcare
Pharmaceuticals
September 12, 2013
page 29 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
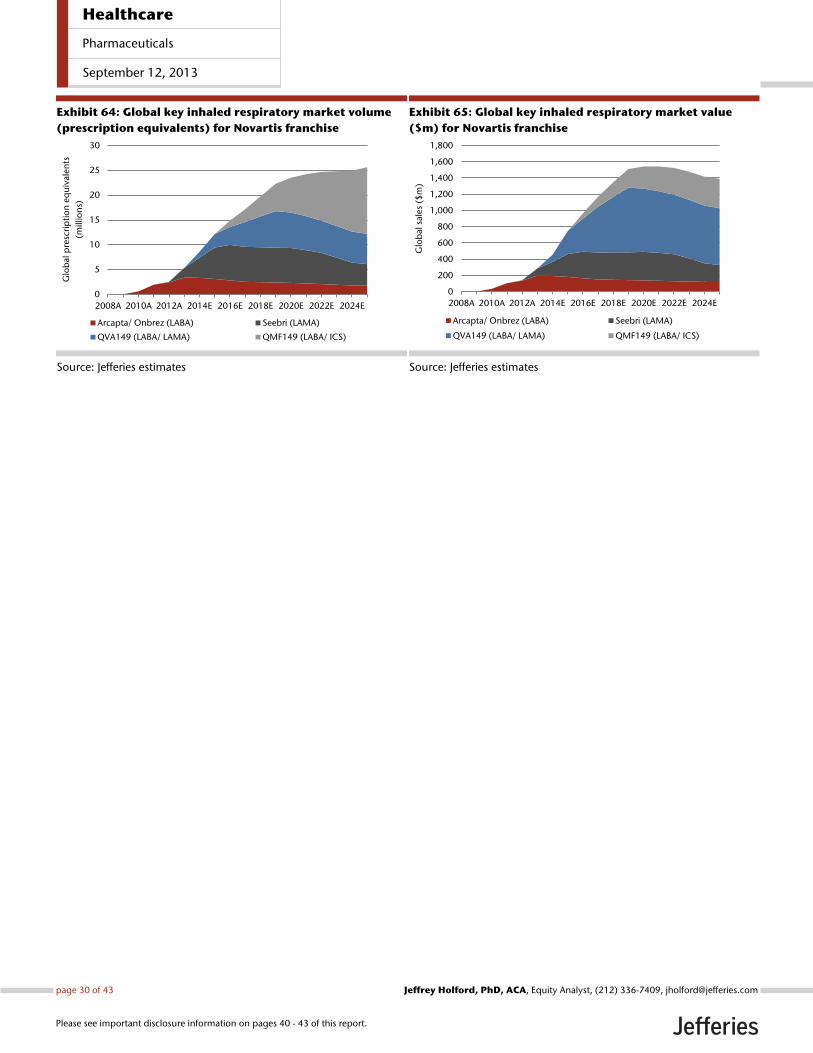
Exhibit 64: Global key inhaled respiratory market volume
(prescription equivalents) for Novartis franchise
Source: Jefferies estimates
Exhibit 65: Global key inhaled respiratory market value
($m) for Novartis franchise
Source: Jefferies estimates
0
5
10
15
20
25
30
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
pre
scri
pti
on
eq
uiv
alen
ts
(mill
ion
s)
Arcapta/ Onbrez (LABA) Seebri (LAMA)
QVA149 (LABA/ LAMA) QMF149 (LABA/ ICS)
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2008A 2010A 2012A 2014E 2016E 2018E 2020E 2022E 2024E
Glo
bal
sal
es
($m
)
Arcapta/ Onbrez (LABA) Seebri (LAMA)
QVA149 (LABA/ LAMA) QMF149 (LABA/ ICS)
Healthcare
Pharmaceuticals
September 12, 2013
page 30 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
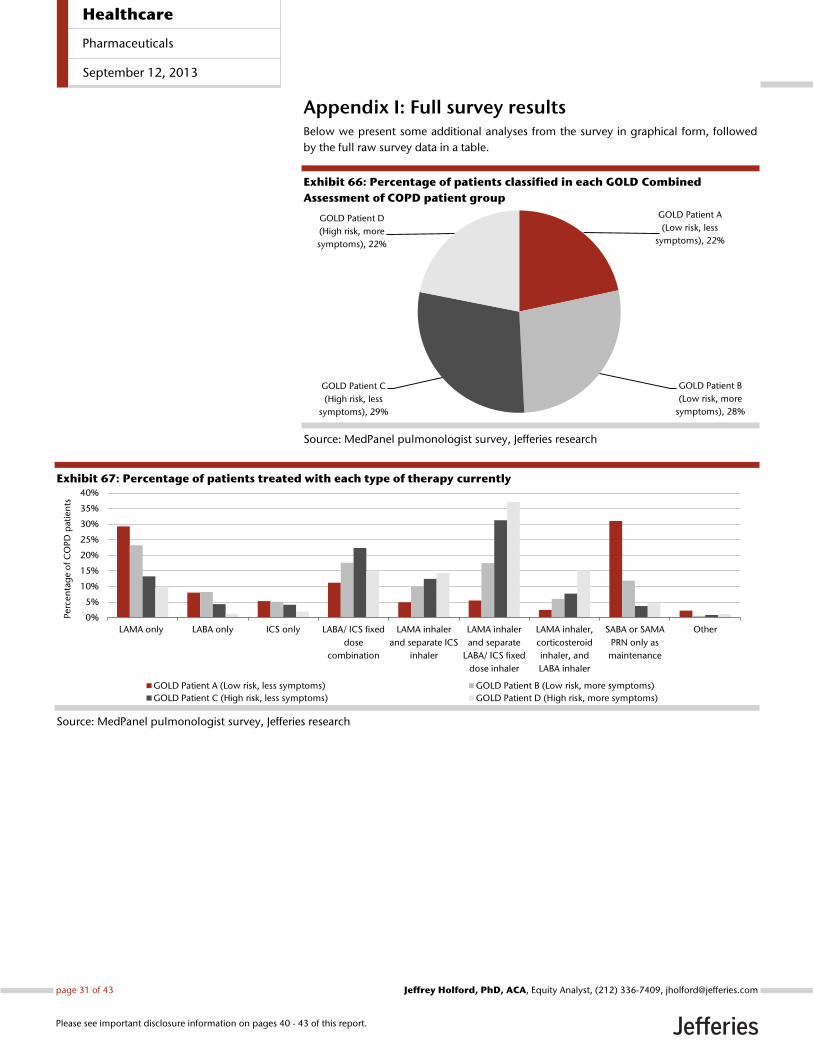
Appendix I: Full survey results Below we present some additional analyses from the survey in graphical form, followed
by the full raw survey data in a table.
Exhibit 66: Percentage of patients classified in each GOLD Combined
Assessment of COPD patient group
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 67: Percentage of patients treated with each type of therapy currently
Source: MedPanel pulmonologist survey, Jefferies research
GOLD Patient A
(Low risk, less
symptoms), 22%
GOLD Patient B
(Low risk, more
symptoms), 28%
GOLD Patient C
(High risk, less
symptoms), 29%
GOLD Patient D
(High risk, more
symptoms), 22%
0%
5%
10%
15%
20%
25%
30%
35%
40%
LAMA only LABA only ICS only LABA/ ICS fixed
dose
combination
LAMA inhaler
and separate ICS
inhaler
LAMA inhaler
and separate
LABA/ ICS fixed
dose inhaler
LAMA inhaler,
corticosteroid
inhaler, and
LABA inhaler
SABA or SAMA
PRN only as
maintenance
Other
Perc
en
tag
e o
f C
OP
D p
ati
en
ts
GOLD Patient A (Low risk, less symptoms) GOLD Patient B (Low risk, more symptoms)
GOLD Patient C (High risk, less symptoms) GOLD Patient D (High risk, more symptoms)
Healthcare
Pharmaceuticals
September 12, 2013
page 31 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
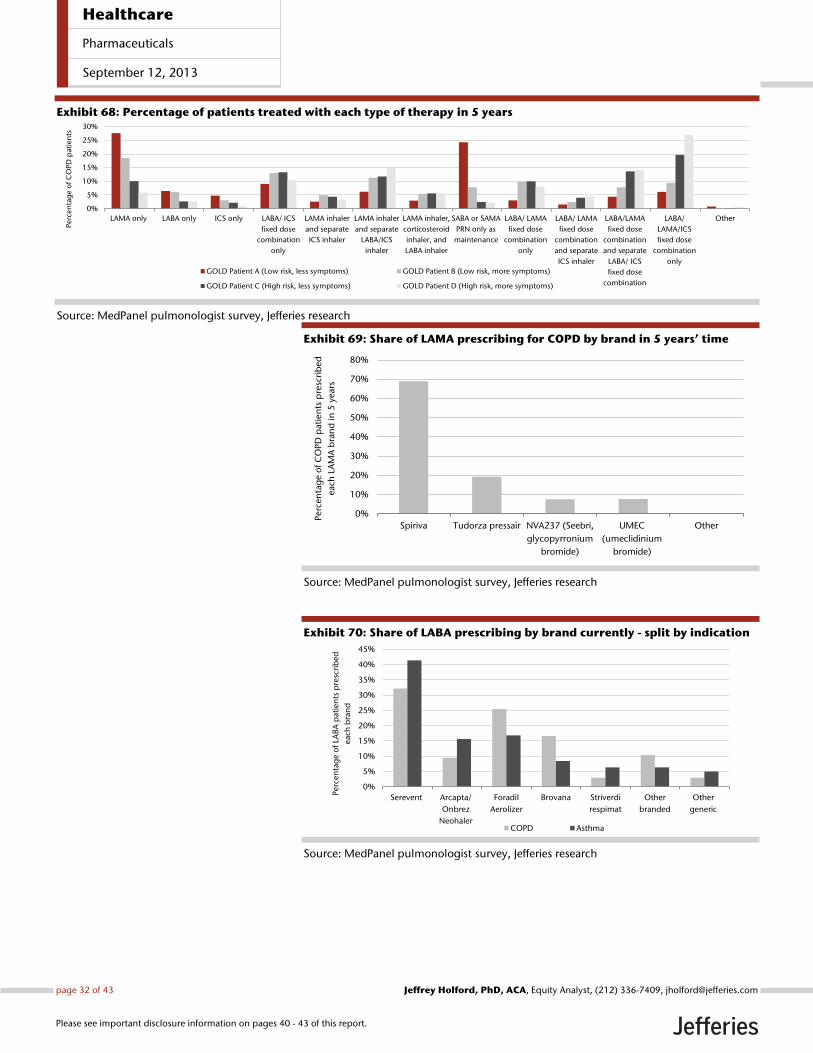
Exhibit 68: Percentage of patients treated with each type of therapy in 5 years
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 69: Share of LAMA prescribing for COPD by brand in 5 years’ time
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 70: Share of LABA prescribing by brand currently - split by indication
Source: MedPanel pulmonologist survey, Jefferies research
0%
5%
10%
15%
20%
25%
30%
LAMA only LABA only ICS only LABA/ ICS
fixed dose
combination
only
LAMA inhaler
and separate
ICS inhaler
LAMA inhaler
and separate
LABA/ICS
inhaler
LAMA inhaler,
corticosteroid
inhaler, and
LABA inhaler
SABA or SAMA
PRN only as
maintenance
LABA/ LAMA
fixed dose
combination
only
LABA/ LAMA
fixed dose
combination
and separate
ICS inhaler
LABA/LAMA
fixed dose
combination
and separate
LABA/ ICS
fixed dose
combination
LABA/
LAMA/ICS
fixed dose
combination
only
Other
Perc
en
tag
e o
f C
OP
D p
ati
en
ts
GOLD Patient A (Low risk, less symptoms) GOLD Patient B (Low risk, more symptoms)
GOLD Patient C (High risk, less symptoms) GOLD Patient D (High risk, more symptoms)
0%
10%
20%
30%
40%
50%
60%
70%
80%
Spiriva Tudorza pressair NVA237 (Seebri,
glycopyrronium
bromide)
UMEC
(umeclidinium
bromide)
Other
Perc
en
tag
e o
f C
OP
D p
ati
en
ts p
resc
rib
ed
eac
h L
AM
A b
ran
d in
5 y
ear
s
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Serevent Arcapta/
Onbrez
Neohaler
Foradil
Aerolizer
Brovana Striverdi
respimat
Other
branded
Other
generic
Perc
en
tag
e o
f LA
BA
pati
en
ts p
resc
rib
ed
eac
h b
ran
d
COPD Asthma
Healthcare
Pharmaceuticals
September 12, 2013
page 32 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
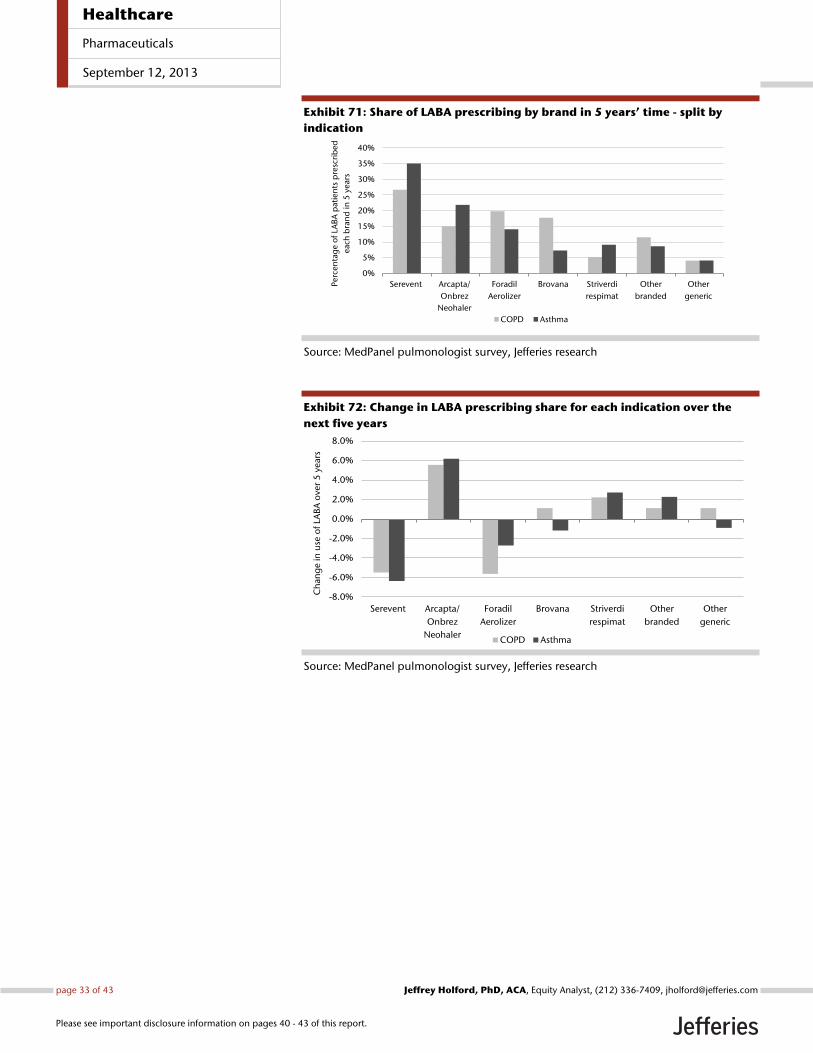
Exhibit 71: Share of LABA prescribing by brand in 5 years’ time - split by
indication
Source: MedPanel pulmonologist survey, Jefferies research
Exhibit 72: Change in LABA prescribing share for each indication over the
next five years
Source: MedPanel pulmonologist survey, Jefferies research
0%
5%
10%
15%
20%
25%
30%
35%
40%
Serevent Arcapta/
Onbrez
Neohaler
Foradil
Aerolizer
Brovana Striverdi
respimat
Other
branded
Other
generic
Perc
en
tag
e o
f LA
BA
pati
en
ts p
resc
rib
ed
eac
h b
ran
d in
5 y
ear
s
COPD Asthma
-8.0%
-6.0%
-4.0%
-2.0%
0.0%
2.0%
4.0%
6.0%
8.0%
Serevent Arcapta/
Onbrez
Neohaler
Foradil
Aerolizer
Brovana Striverdi
respimat
Other
branded
Other
generic
Ch
ang
e in
use
of
LAB
A o
ver
5 y
ear
s
COPD Asthma
Healthcare
Pharmaceuticals
September 12, 2013
page 33 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
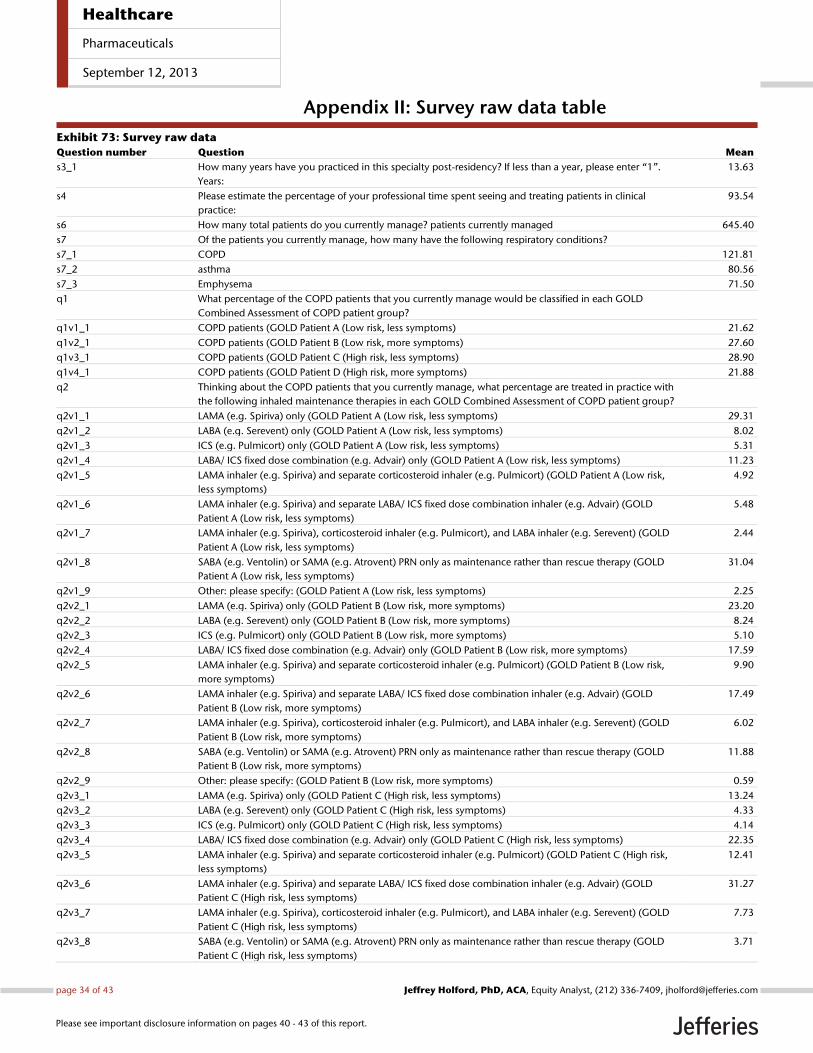
Appendix II: Survey raw data table
Exhibit 73: Survey raw data
Question number Question Mean
s3_1 How many years have you practiced in this specialty post-residency? If less than a year, please enter ‚1‛.
Years:
13.63
s4 Please estimate the percentage of your professional time spent seeing and treating patients in clinical
practice:
93.54
s6 How many total patients do you currently manage? patients currently managed 645.40
s7 Of the patients you currently manage, how many have the following respiratory conditions?
s7_1 COPD 121.81
s7_2 asthma 80.56
s7_3 Emphysema 71.50
q1 What percentage of the COPD patients that you currently manage would be classified in each GOLD
Combined Assessment of COPD patient group?
q1v1_1 COPD patients (GOLD Patient A (Low risk, less symptoms) 21.62
q1v2_1 COPD patients (GOLD Patient B (Low risk, more symptoms) 27.60
q1v3_1 COPD patients (GOLD Patient C (High risk, less symptoms) 28.90
q1v4_1 COPD patients (GOLD Patient D (High risk, more symptoms) 21.88
q2 Thinking about the COPD patients that you currently manage, what percentage are treated in practice with
the following inhaled maintenance therapies in each GOLD Combined Assessment of COPD patient group?
q2v1_1 LAMA (e.g. Spiriva) only (GOLD Patient A (Low risk, less symptoms) 29.31
q2v1_2 LABA (e.g. Serevent) only (GOLD Patient A (Low risk, less symptoms) 8.02
q2v1_3 ICS (e.g. Pulmicort) only (GOLD Patient A (Low risk, less symptoms) 5.31
q2v1_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient A (Low risk, less symptoms) 11.23
q2v1_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient A (Low risk,
less symptoms)
4.92
q2v1_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ ICS fixed dose combination inhaler (e.g. Advair) (GOLD
Patient A (Low risk, less symptoms)
5.48
q2v1_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient A (Low risk, less symptoms)
2.44
q2v1_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient A (Low risk, less symptoms)
31.04
q2v1_9 Other: please specify: (GOLD Patient A (Low risk, less symptoms) 2.25
q2v2_1 LAMA (e.g. Spiriva) only (GOLD Patient B (Low risk, more symptoms) 23.20
q2v2_2 LABA (e.g. Serevent) only (GOLD Patient B (Low risk, more symptoms) 8.24
q2v2_3 ICS (e.g. Pulmicort) only (GOLD Patient B (Low risk, more symptoms) 5.10
q2v2_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient B (Low risk, more symptoms) 17.59
q2v2_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient B (Low risk,
more symptoms)
9.90
q2v2_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ ICS fixed dose combination inhaler (e.g. Advair) (GOLD
Patient B (Low risk, more symptoms)
17.49
q2v2_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient B (Low risk, more symptoms)
6.02
q2v2_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient B (Low risk, more symptoms)
11.88
q2v2_9 Other: please specify: (GOLD Patient B (Low risk, more symptoms) 0.59
q2v3_1 LAMA (e.g. Spiriva) only (GOLD Patient C (High risk, less symptoms) 13.24
q2v3_2 LABA (e.g. Serevent) only (GOLD Patient C (High risk, less symptoms) 4.33
q2v3_3 ICS (e.g. Pulmicort) only (GOLD Patient C (High risk, less symptoms) 4.14
q2v3_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient C (High risk, less symptoms) 22.35
q2v3_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient C (High risk,
less symptoms)
12.41
q2v3_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ ICS fixed dose combination inhaler (e.g. Advair) (GOLD
Patient C (High risk, less symptoms)
31.27
q2v3_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient C (High risk, less symptoms)
7.73
q2v3_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient C (High risk, less symptoms)
3.71
Healthcare
Pharmaceuticals
September 12, 2013
page 34 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
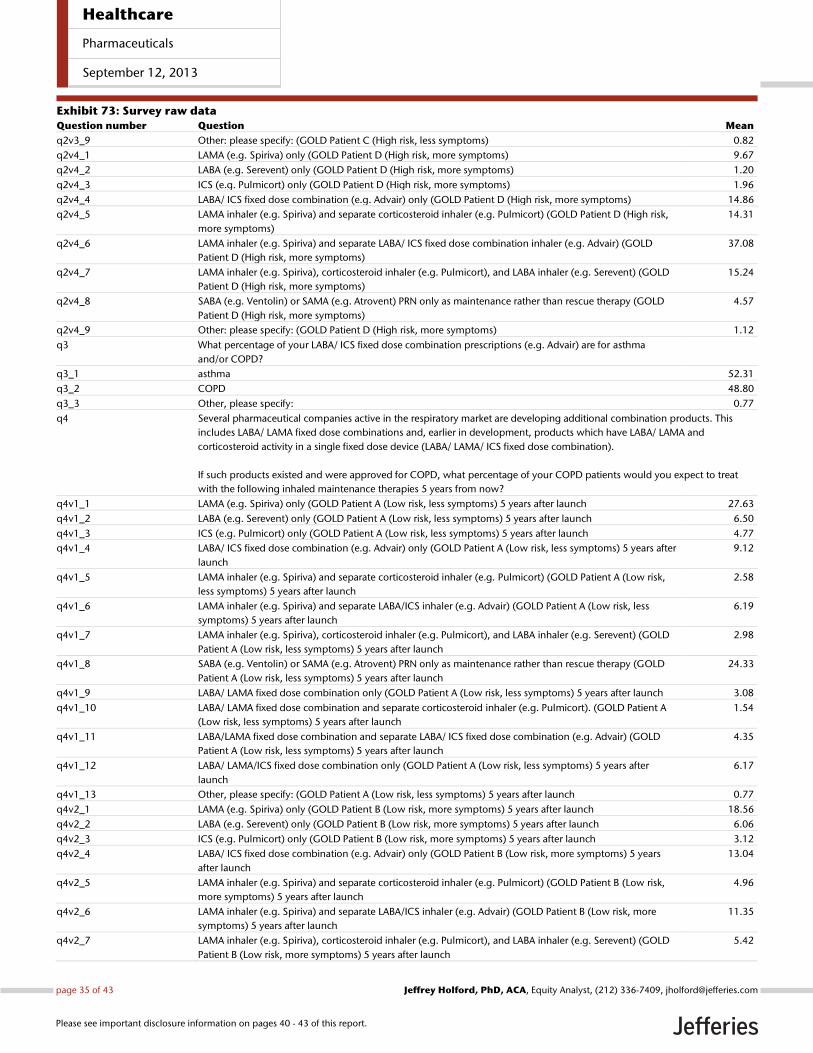
Exhibit 73: Survey raw data
Question number Question Mean
q2v3_9 Other: please specify: (GOLD Patient C (High risk, less symptoms) 0.82
q2v4_1 LAMA (e.g. Spiriva) only (GOLD Patient D (High risk, more symptoms) 9.67
q2v4_2 LABA (e.g. Serevent) only (GOLD Patient D (High risk, more symptoms) 1.20
q2v4_3 ICS (e.g. Pulmicort) only (GOLD Patient D (High risk, more symptoms) 1.96
q2v4_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient D (High risk, more symptoms) 14.86
q2v4_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient D (High risk,
more symptoms)
14.31
q2v4_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ ICS fixed dose combination inhaler (e.g. Advair) (GOLD
Patient D (High risk, more symptoms)
37.08
q2v4_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient D (High risk, more symptoms)
15.24
q2v4_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient D (High risk, more symptoms)
4.57
q2v4_9 Other: please specify: (GOLD Patient D (High risk, more symptoms) 1.12
q3 What percentage of your LABA/ ICS fixed dose combination prescriptions (e.g. Advair) are for asthma
and/or COPD?
q3_1 asthma 52.31
q3_2 COPD 48.80
q3_3 Other, please specify: 0.77
q4 Several pharmaceutical companies active in the respiratory market are developing additional combination products. This
includes LABA/ LAMA fixed dose combinations and, earlier in development, products which have LABA/ LAMA and
corticosteroid activity in a single fixed dose device (LABA/ LAMA/ ICS fixed dose combination).
If such products existed and were approved for COPD, what percentage of your COPD patients would you expect to treat
with the following inhaled maintenance therapies 5 years from now?
q4v1_1 LAMA (e.g. Spiriva) only (GOLD Patient A (Low risk, less symptoms) 5 years after launch 27.63
q4v1_2 LABA (e.g. Serevent) only (GOLD Patient A (Low risk, less symptoms) 5 years after launch 6.50
q4v1_3 ICS (e.g. Pulmicort) only (GOLD Patient A (Low risk, less symptoms) 5 years after launch 4.77
q4v1_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient A (Low risk, less symptoms) 5 years after
launch
9.12
q4v1_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient A (Low risk,
less symptoms) 5 years after launch
2.58
q4v1_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (GOLD Patient A (Low risk, less
symptoms) 5 years after launch
6.19
q4v1_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient A (Low risk, less symptoms) 5 years after launch
2.98
q4v1_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient A (Low risk, less symptoms) 5 years after launch
24.33
q4v1_9 LABA/ LAMA fixed dose combination only (GOLD Patient A (Low risk, less symptoms) 5 years after launch 3.08
q4v1_10 LABA/ LAMA fixed dose combination and separate corticosteroid inhaler (e.g. Pulmicort). (GOLD Patient A
(Low risk, less symptoms) 5 years after launch
1.54
q4v1_11 LABA/LAMA fixed dose combination and separate LABA/ ICS fixed dose combination (e.g. Advair) (GOLD
Patient A (Low risk, less symptoms) 5 years after launch
4.35
q4v1_12 LABA/ LAMA/ICS fixed dose combination only (GOLD Patient A (Low risk, less symptoms) 5 years after
launch
6.17
q4v1_13 Other, please specify: (GOLD Patient A (Low risk, less symptoms) 5 years after launch 0.77
q4v2_1 LAMA (e.g. Spiriva) only (GOLD Patient B (Low risk, more symptoms) 5 years after launch 18.56
q4v2_2 LABA (e.g. Serevent) only (GOLD Patient B (Low risk, more symptoms) 5 years after launch 6.06
q4v2_3 ICS (e.g. Pulmicort) only (GOLD Patient B (Low risk, more symptoms) 5 years after launch 3.12
q4v2_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient B (Low risk, more symptoms) 5 years
after launch
13.04
q4v2_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient B (Low risk,
more symptoms) 5 years after launch
4.96
q4v2_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (GOLD Patient B (Low risk, more
symptoms) 5 years after launch
11.35
q4v2_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient B (Low risk, more symptoms) 5 years after launch
5.42
Healthcare
Pharmaceuticals
September 12, 2013
page 35 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
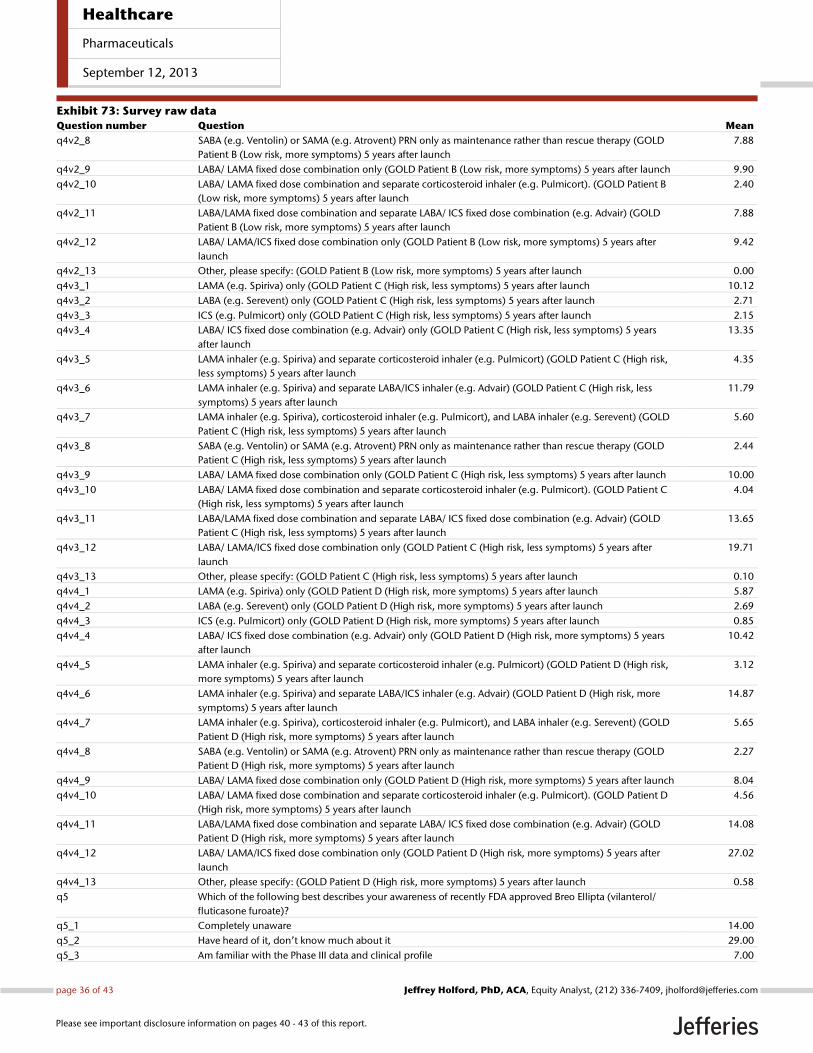
Exhibit 73: Survey raw data
Question number Question Mean
q4v2_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient B (Low risk, more symptoms) 5 years after launch
7.88
q4v2_9 LABA/ LAMA fixed dose combination only (GOLD Patient B (Low risk, more symptoms) 5 years after launch 9.90
q4v2_10 LABA/ LAMA fixed dose combination and separate corticosteroid inhaler (e.g. Pulmicort). (GOLD Patient B
(Low risk, more symptoms) 5 years after launch
2.40
q4v2_11 LABA/LAMA fixed dose combination and separate LABA/ ICS fixed dose combination (e.g. Advair) (GOLD
Patient B (Low risk, more symptoms) 5 years after launch
7.88
q4v2_12 LABA/ LAMA/ICS fixed dose combination only (GOLD Patient B (Low risk, more symptoms) 5 years after
launch
9.42
q4v2_13 Other, please specify: (GOLD Patient B (Low risk, more symptoms) 5 years after launch 0.00
q4v3_1 LAMA (e.g. Spiriva) only (GOLD Patient C (High risk, less symptoms) 5 years after launch 10.12
q4v3_2 LABA (e.g. Serevent) only (GOLD Patient C (High risk, less symptoms) 5 years after launch 2.71
q4v3_3 ICS (e.g. Pulmicort) only (GOLD Patient C (High risk, less symptoms) 5 years after launch 2.15
q4v3_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient C (High risk, less symptoms) 5 years
after launch
13.35
q4v3_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient C (High risk,
less symptoms) 5 years after launch
4.35
q4v3_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (GOLD Patient C (High risk, less
symptoms) 5 years after launch
11.79
q4v3_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient C (High risk, less symptoms) 5 years after launch
5.60
q4v3_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient C (High risk, less symptoms) 5 years after launch
2.44
q4v3_9 LABA/ LAMA fixed dose combination only (GOLD Patient C (High risk, less symptoms) 5 years after launch 10.00
q4v3_10 LABA/ LAMA fixed dose combination and separate corticosteroid inhaler (e.g. Pulmicort). (GOLD Patient C
(High risk, less symptoms) 5 years after launch
4.04
q4v3_11 LABA/LAMA fixed dose combination and separate LABA/ ICS fixed dose combination (e.g. Advair) (GOLD
Patient C (High risk, less symptoms) 5 years after launch
13.65
q4v3_12 LABA/ LAMA/ICS fixed dose combination only (GOLD Patient C (High risk, less symptoms) 5 years after
launch
19.71
q4v3_13 Other, please specify: (GOLD Patient C (High risk, less symptoms) 5 years after launch 0.10
q4v4_1 LAMA (e.g. Spiriva) only (GOLD Patient D (High risk, more symptoms) 5 years after launch 5.87
q4v4_2 LABA (e.g. Serevent) only (GOLD Patient D (High risk, more symptoms) 5 years after launch 2.69
q4v4_3 ICS (e.g. Pulmicort) only (GOLD Patient D (High risk, more symptoms) 5 years after launch 0.85
q4v4_4 LABA/ ICS fixed dose combination (e.g. Advair) only (GOLD Patient D (High risk, more symptoms) 5 years
after launch
10.42
q4v4_5 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (GOLD Patient D (High risk,
more symptoms) 5 years after launch
3.12
q4v4_6 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (GOLD Patient D (High risk, more
symptoms) 5 years after launch
14.87
q4v4_7 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (GOLD
Patient D (High risk, more symptoms) 5 years after launch
5.65
q4v4_8 SABA (e.g. Ventolin) or SAMA (e.g. Atrovent) PRN only as maintenance rather than rescue therapy (GOLD
Patient D (High risk, more symptoms) 5 years after launch
2.27
q4v4_9 LABA/ LAMA fixed dose combination only (GOLD Patient D (High risk, more symptoms) 5 years after launch 8.04
q4v4_10 LABA/ LAMA fixed dose combination and separate corticosteroid inhaler (e.g. Pulmicort). (GOLD Patient D
(High risk, more symptoms) 5 years after launch
4.56
q4v4_11 LABA/LAMA fixed dose combination and separate LABA/ ICS fixed dose combination (e.g. Advair) (GOLD
Patient D (High risk, more symptoms) 5 years after launch
14.08
q4v4_12 LABA/ LAMA/ICS fixed dose combination only (GOLD Patient D (High risk, more symptoms) 5 years after
launch
27.02
q4v4_13 Other, please specify: (GOLD Patient D (High risk, more symptoms) 5 years after launch 0.58
q5 Which of the following best describes your awareness of recently FDA approved Breo Ellipta (vilanterol/
fluticasone furoate)?
q5_1 Completely unaware 14.00
q5_2 Have heard of it, don’t know much about it 29.00
q5_3 Am familiar with the Phase III data and clinical profile 7.00
Healthcare
Pharmaceuticals
September 12, 2013
page 36 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
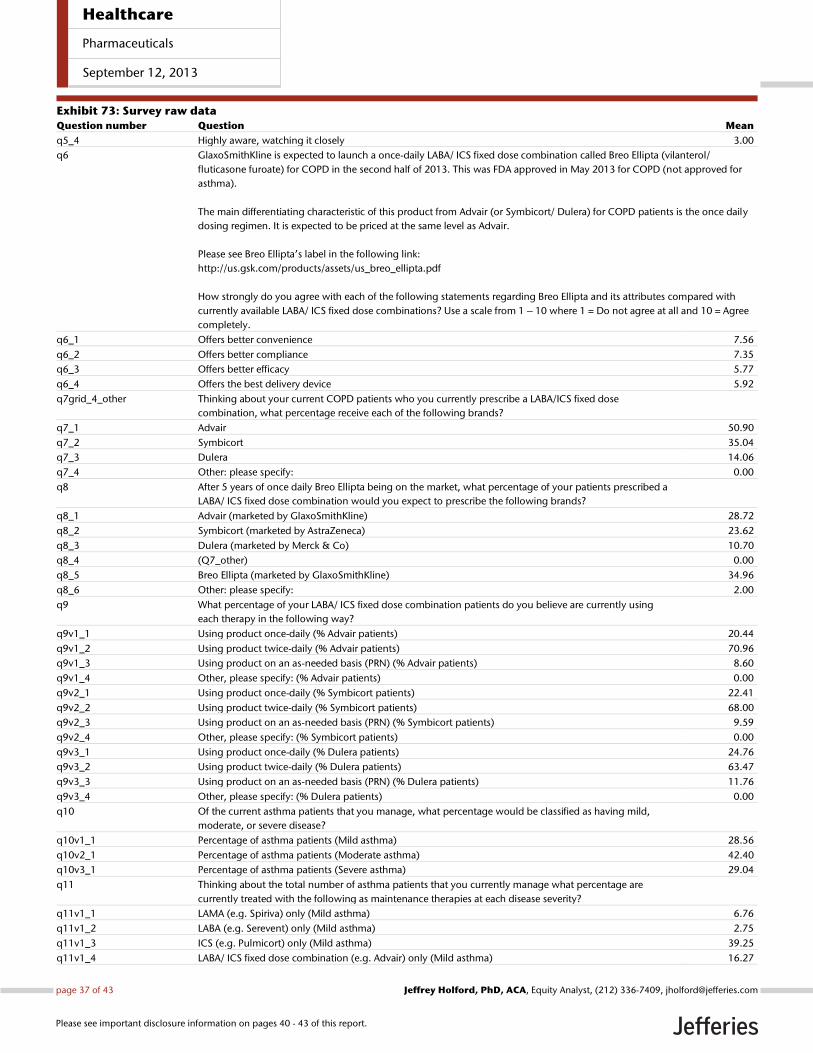
Exhibit 73: Survey raw data
Question number Question Mean
q5_4 Highly aware, watching it closely 3.00
q6 GlaxoSmithKline is expected to launch a once-daily LABA/ ICS fixed dose combination called Breo Ellipta (vilanterol/
fluticasone furoate) for COPD in the second half of 2013. This was FDA approved in May 2013 for COPD (not approved for
asthma).
The main differentiating characteristic of this product from Advair (or Symbicort/ Dulera) for COPD patients is the once daily
dosing regimen. It is expected to be priced at the same level as Advair.
Please see Breo Ellipta’s label in the following link:
http://us.gsk.com/products/assets/us_breo_ellipta.pdf
How strongly do you agree with each of the following statements regarding Breo Ellipta and its attributes compared with
currently available LABA/ ICS fixed dose combinations? Use a scale from 1 – 10 where 1 = Do not agree at all and 10 = Agree
completely.
q6_1 Offers better convenience 7.56
q6_2 Offers better compliance 7.35
q6_3 Offers better efficacy 5.77
q6_4 Offers the best delivery device 5.92
q7grid_4_other Thinking about your current COPD patients who you currently prescribe a LABA/ICS fixed dose
combination, what percentage receive each of the following brands?
q7_1 Advair 50.90
q7_2 Symbicort 35.04
q7_3 Dulera 14.06
q7_4 Other: please specify: 0.00
q8 After 5 years of once daily Breo Ellipta being on the market, what percentage of your patients prescribed a
LABA/ ICS fixed dose combination would you expect to prescribe the following brands?
q8_1 Advair (marketed by GlaxoSmithKline) 28.72
q8_2 Symbicort (marketed by AstraZeneca) 23.62
q8_3 Dulera (marketed by Merck & Co) 10.70
q8_4 (Q7_other) 0.00
q8_5 Breo Ellipta (marketed by GlaxoSmithKline) 34.96
q8_6 Other: please specify: 2.00
q9 What percentage of your LABA/ ICS fixed dose combination patients do you believe are currently using
each therapy in the following way?
q9v1_1 Using product once-daily (% Advair patients) 20.44
q9v1_2 Using product twice-daily (% Advair patients) 70.96
q9v1_3 Using product on an as-needed basis (PRN) (% Advair patients) 8.60
q9v1_4 Other, please specify: (% Advair patients) 0.00
q9v2_1 Using product once-daily (% Symbicort patients) 22.41
q9v2_2 Using product twice-daily (% Symbicort patients) 68.00
q9v2_3 Using product on an as-needed basis (PRN) (% Symbicort patients) 9.59
q9v2_4 Other, please specify: (% Symbicort patients) 0.00
q9v3_1 Using product once-daily (% Dulera patients) 24.76
q9v3_2 Using product twice-daily (% Dulera patients) 63.47
q9v3_3 Using product on an as-needed basis (PRN) (% Dulera patients) 11.76
q9v3_4 Other, please specify: (% Dulera patients) 0.00
q10 Of the current asthma patients that you manage, what percentage would be classified as having mild,
moderate, or severe disease?
q10v1_1 Percentage of asthma patients (Mild asthma) 28.56
q10v2_1 Percentage of asthma patients (Moderate asthma) 42.40
q10v3_1 Percentage of asthma patients (Severe asthma) 29.04
q11 Thinking about the total number of asthma patients that you currently manage what percentage are
currently treated with the following as maintenance therapies at each disease severity?
q11v1_1 LAMA (e.g. Spiriva) only (Mild asthma) 6.76
q11v1_2 LABA (e.g. Serevent) only (Mild asthma) 2.75
q11v1_3 ICS (e.g. Pulmicort) only (Mild asthma) 39.25
q11v1_4 LABA/ ICS fixed dose combination (e.g. Advair) only (Mild asthma) 16.27
Healthcare
Pharmaceuticals
September 12, 2013
page 37 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
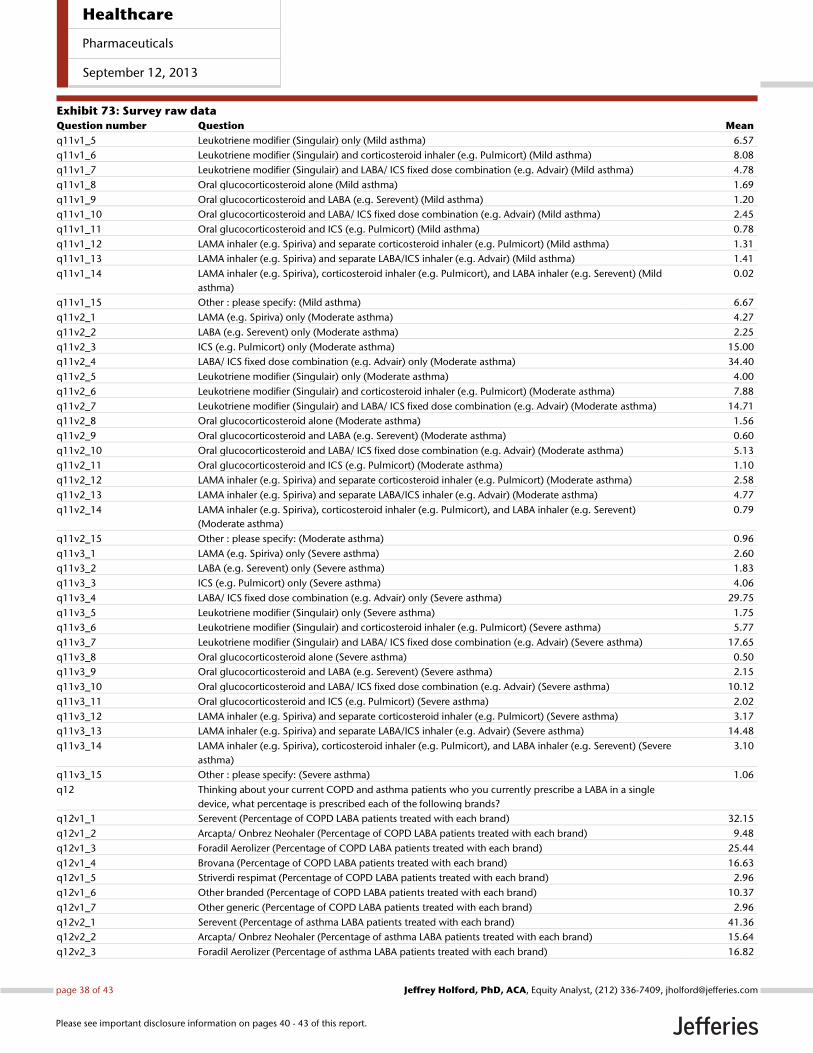
Exhibit 73: Survey raw data
Question number Question Mean
q11v1_5 Leukotriene modifier (Singulair) only (Mild asthma) 6.57
q11v1_6 Leukotriene modifier (Singulair) and corticosteroid inhaler (e.g. Pulmicort) (Mild asthma) 8.08
q11v1_7 Leukotriene modifier (Singulair) and LABA/ ICS fixed dose combination (e.g. Advair) (Mild asthma) 4.78
q11v1_8 Oral glucocorticosteroid alone (Mild asthma) 1.69
q11v1_9 Oral glucocorticosteroid and LABA (e.g. Serevent) (Mild asthma) 1.20
q11v1_10 Oral glucocorticosteroid and LABA/ ICS fixed dose combination (e.g. Advair) (Mild asthma) 2.45
q11v1_11 Oral glucocorticosteroid and ICS (e.g. Pulmicort) (Mild asthma) 0.78
q11v1_12 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (Mild asthma) 1.31
q11v1_13 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (Mild asthma) 1.41
q11v1_14 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (Mild
asthma)
0.02
q11v1_15 Other : please specify: (Mild asthma) 6.67
q11v2_1 LAMA (e.g. Spiriva) only (Moderate asthma) 4.27
q11v2_2 LABA (e.g. Serevent) only (Moderate asthma) 2.25
q11v2_3 ICS (e.g. Pulmicort) only (Moderate asthma) 15.00
q11v2_4 LABA/ ICS fixed dose combination (e.g. Advair) only (Moderate asthma) 34.40
q11v2_5 Leukotriene modifier (Singulair) only (Moderate asthma) 4.00
q11v2_6 Leukotriene modifier (Singulair) and corticosteroid inhaler (e.g. Pulmicort) (Moderate asthma) 7.88
q11v2_7 Leukotriene modifier (Singulair) and LABA/ ICS fixed dose combination (e.g. Advair) (Moderate asthma) 14.71
q11v2_8 Oral glucocorticosteroid alone (Moderate asthma) 1.56
q11v2_9 Oral glucocorticosteroid and LABA (e.g. Serevent) (Moderate asthma) 0.60
q11v2_10 Oral glucocorticosteroid and LABA/ ICS fixed dose combination (e.g. Advair) (Moderate asthma) 5.13
q11v2_11 Oral glucocorticosteroid and ICS (e.g. Pulmicort) (Moderate asthma) 1.10
q11v2_12 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (Moderate asthma) 2.58
q11v2_13 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (Moderate asthma) 4.77
q11v2_14 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent)
(Moderate asthma)
0.79
q11v2_15 Other : please specify: (Moderate asthma) 0.96
q11v3_1 LAMA (e.g. Spiriva) only (Severe asthma) 2.60
q11v3_2 LABA (e.g. Serevent) only (Severe asthma) 1.83
q11v3_3 ICS (e.g. Pulmicort) only (Severe asthma) 4.06
q11v3_4 LABA/ ICS fixed dose combination (e.g. Advair) only (Severe asthma) 29.75
q11v3_5 Leukotriene modifier (Singulair) only (Severe asthma) 1.75
q11v3_6 Leukotriene modifier (Singulair) and corticosteroid inhaler (e.g. Pulmicort) (Severe asthma) 5.77
q11v3_7 Leukotriene modifier (Singulair) and LABA/ ICS fixed dose combination (e.g. Advair) (Severe asthma) 17.65
q11v3_8 Oral glucocorticosteroid alone (Severe asthma) 0.50
q11v3_9 Oral glucocorticosteroid and LABA (e.g. Serevent) (Severe asthma) 2.15
q11v3_10 Oral glucocorticosteroid and LABA/ ICS fixed dose combination (e.g. Advair) (Severe asthma) 10.12
q11v3_11 Oral glucocorticosteroid and ICS (e.g. Pulmicort) (Severe asthma) 2.02
q11v3_12 LAMA inhaler (e.g. Spiriva) and separate corticosteroid inhaler (e.g. Pulmicort) (Severe asthma) 3.17
q11v3_13 LAMA inhaler (e.g. Spiriva) and separate LABA/ICS inhaler (e.g. Advair) (Severe asthma) 14.48
q11v3_14 LAMA inhaler (e.g. Spiriva), corticosteroid inhaler (e.g. Pulmicort), and LABA inhaler (e.g. Serevent) (Severe
asthma)
3.10
q11v3_15 Other : please specify: (Severe asthma) 1.06
q12 Thinking about your current COPD and asthma patients who you currently prescribe a LABA in a single
device, what percentage is prescribed each of the following brands?
q12v1_1 Serevent (Percentage of COPD LABA patients treated with each brand) 32.15
q12v1_2 Arcapta/ Onbrez Neohaler (Percentage of COPD LABA patients treated with each brand) 9.48
q12v1_3 Foradil Aerolizer (Percentage of COPD LABA patients treated with each brand) 25.44
q12v1_4 Brovana (Percentage of COPD LABA patients treated with each brand) 16.63
q12v1_5 Striverdi respimat (Percentage of COPD LABA patients treated with each brand) 2.96
q12v1_6 Other branded (Percentage of COPD LABA patients treated with each brand) 10.37
q12v1_7 Other generic (Percentage of COPD LABA patients treated with each brand) 2.96
q12v2_1 Serevent (Percentage of asthma LABA patients treated with each brand) 41.36
q12v2_2 Arcapta/ Onbrez Neohaler (Percentage of asthma LABA patients treated with each brand) 15.64
q12v2_3 Foradil Aerolizer (Percentage of asthma LABA patients treated with each brand) 16.82
Healthcare
Pharmaceuticals
September 12, 2013
page 38 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
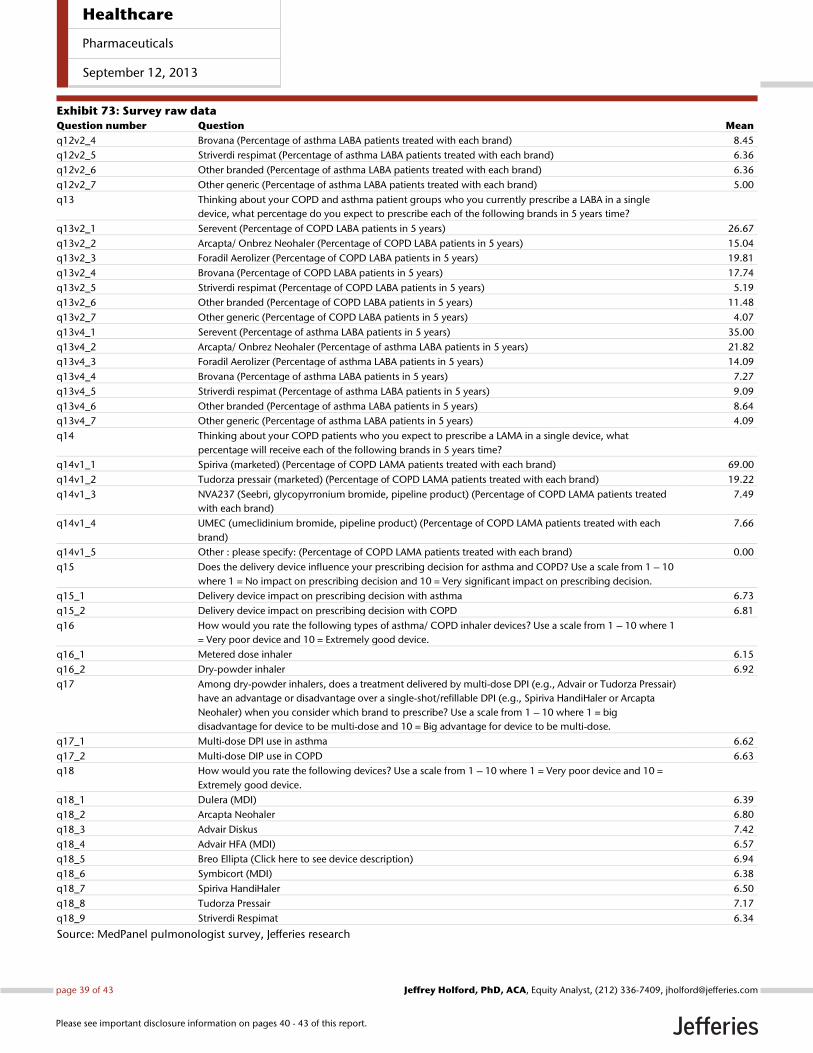
Exhibit 73: Survey raw data
Question number Question Mean
q12v2_4 Brovana (Percentage of asthma LABA patients treated with each brand) 8.45
q12v2_5 Striverdi respimat (Percentage of asthma LABA patients treated with each brand) 6.36
q12v2_6 Other branded (Percentage of asthma LABA patients treated with each brand) 6.36
q12v2_7 Other generic (Percentage of asthma LABA patients treated with each brand) 5.00
q13 Thinking about your COPD and asthma patient groups who you currently prescribe a LABA in a single
device, what percentage do you expect to prescribe each of the following brands in 5 years time?
q13v2_1 Serevent (Percentage of COPD LABA patients in 5 years) 26.67
q13v2_2 Arcapta/ Onbrez Neohaler (Percentage of COPD LABA patients in 5 years) 15.04
q13v2_3 Foradil Aerolizer (Percentage of COPD LABA patients in 5 years) 19.81
q13v2_4 Brovana (Percentage of COPD LABA patients in 5 years) 17.74
q13v2_5 Striverdi respimat (Percentage of COPD LABA patients in 5 years) 5.19
q13v2_6 Other branded (Percentage of COPD LABA patients in 5 years) 11.48
q13v2_7 Other generic (Percentage of COPD LABA patients in 5 years) 4.07
q13v4_1 Serevent (Percentage of asthma LABA patients in 5 years) 35.00
q13v4_2 Arcapta/ Onbrez Neohaler (Percentage of asthma LABA patients in 5 years) 21.82
q13v4_3 Foradil Aerolizer (Percentage of asthma LABA patients in 5 years) 14.09
q13v4_4 Brovana (Percentage of asthma LABA patients in 5 years) 7.27
q13v4_5 Striverdi respimat (Percentage of asthma LABA patients in 5 years) 9.09
q13v4_6 Other branded (Percentage of asthma LABA patients in 5 years) 8.64
q13v4_7 Other generic (Percentage of asthma LABA patients in 5 years) 4.09
q14 Thinking about your COPD patients who you expect to prescribe a LAMA in a single device, what
percentage will receive each of the following brands in 5 years time?
q14v1_1 Spiriva (marketed) (Percentage of COPD LAMA patients treated with each brand) 69.00
q14v1_2 Tudorza pressair (marketed) (Percentage of COPD LAMA patients treated with each brand) 19.22
q14v1_3 NVA237 (Seebri, glycopyrronium bromide, pipeline product) (Percentage of COPD LAMA patients treated
with each brand)
7.49
q14v1_4 UMEC (umeclidinium bromide, pipeline product) (Percentage of COPD LAMA patients treated with each
brand)
7.66
q14v1_5 Other : please specify: (Percentage of COPD LAMA patients treated with each brand) 0.00
q15 Does the delivery device influence your prescribing decision for asthma and COPD? Use a scale from 1 – 10
where 1 = No impact on prescribing decision and 10 = Very significant impact on prescribing decision.
q15_1 Delivery device impact on prescribing decision with asthma 6.73
q15_2 Delivery device impact on prescribing decision with COPD 6.81
q16 How would you rate the following types of asthma/ COPD inhaler devices? Use a scale from 1 – 10 where 1
= Very poor device and 10 = Extremely good device.
q16_1 Metered dose inhaler 6.15
q16_2 Dry-powder inhaler 6.92
q17 Among dry-powder inhalers, does a treatment delivered by multi-dose DPI (e.g., Advair or Tudorza Pressair)
have an advantage or disadvantage over a single-shot/refillable DPI (e.g., Spiriva HandiHaler or Arcapta
Neohaler) when you consider which brand to prescribe? Use a scale from 1 – 10 where 1 = big
disadvantage for device to be multi-dose and 10 = Big advantage for device to be multi-dose.
q17_1 Multi-dose DPI use in asthma 6.62
q17_2 Multi-dose DIP use in COPD 6.63
q18 How would you rate the following devices? Use a scale from 1 – 10 where 1 = Very poor device and 10 =
Extremely good device.
q18_1 Dulera (MDI) 6.39
q18_2 Arcapta Neohaler 6.80
q18_3 Advair Diskus 7.42
q18_4 Advair HFA (MDI) 6.57
q18_5 Breo Ellipta (Click here to see device description) 6.94
q18_6 Symbicort (MDI) 6.38
q18_7 Spiriva HandiHaler 6.50
q18_8 Tudorza Pressair 7.17
q18_9 Striverdi Respimat 6.34
Source: MedPanel pulmonologist survey, Jefferies research
Healthcare
Pharmaceuticals
September 12, 2013
page 39 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
Analyst CertificationI, Jeffrey Holford, PhD, ACA, certify that all of the views expressed in this research report accurately reflect my personal views about the subjectsecurity(ies) and subject company(ies). I also certify that no part of my compensation was, is, or will be, directly or indirectly, related to the specificrecommendations or views expressed in this research report.I, Terence McManus, PhD, certify that all of the views expressed in this research report accurately reflect my personal views about the subjectsecurity(ies) and subject company(ies). I also certify that no part of my compensation was, is, or will be, directly or indirectly, related to the specificrecommendations or views expressed in this research report.I, Ian Hilliker, certify that all of the views expressed in this research report accurately reflect my personal views about the subject security(ies) andsubject company(ies). I also certify that no part of my compensation was, is, or will be, directly or indirectly, related to the specific recommendationsor views expressed in this research report.I, Swayampakula Ramakanth, PhD, MBA, certify that all of the views expressed in this research report accurately reflect my personal views about thesubject security(ies) and subject company(ies). I also certify that no part of my compensation was, is, or will be, directly or indirectly, related to thespecific recommendations or views expressed in this research report.I, David Gu, PhD, certify that all of the views expressed in this research report accurately reflect my personal views about the subject security(ies) andsubject company(ies). I also certify that no part of my compensation was, is, or will be, directly or indirectly, related to the specific recommendationsor views expressed in this research report.Registration of non-US analysts: Terence McManus, PhD is employed by Jefferies International Limited, a non-US affiliate of Jefferies LLC and isnot registered/qualified as a research analyst with FINRA. This analyst(s) may not be an associated person of Jefferies LLC, a FINRA member firm, andtherefore may not be subject to the NASD Rule 2711 and Incorporated NYSE Rule 472 restrictions on communications with a subject company, publicappearances and trading securities held by a research analyst.
Registration of non-US analysts: Ian Hilliker is employed by Jefferies International Limited, a non-US affiliate of Jefferies LLC and is not registered/qualified as a research analyst with FINRA. This analyst(s) may not be an associated person of Jefferies LLC, a FINRA member firm, and therefore maynot be subject to the NASD Rule 2711 and Incorporated NYSE Rule 472 restrictions on communications with a subject company, public appearancesand trading securities held by a research analyst.
As is the case with all Jefferies employees, the analyst(s) responsible for the coverage of the financial instruments discussed in this report receivescompensation based in part on the overall performance of the firm, including investment banking income. We seek to update our research asappropriate, but various regulations may prevent us from doing so. Aside from certain industry reports published on a periodic basis, the large majorityof reports are published at irregular intervals as appropriate in the analyst's judgement.
Company Specific DisclosuresFor Important Disclosure information on companies recommended in this report, please visit our website at https://javatar.bluematrix.com/sellside/Disclosures.action or call 212.284.2300.
Meanings of Jefferies RatingsBuy - Describes stocks that we expect to provide a total return (price appreciation plus yield) of 15% or more within a 12-month period.Hold - Describes stocks that we expect to provide a total return (price appreciation plus yield) of plus 15% or minus 10% within a 12-month period.Underperform - Describes stocks that we expect to provide a total negative return (price appreciation plus yield) of 10% or more within a 12-monthperiod.The expected total return (price appreciation plus yield) for Buy rated stocks with an average stock price consistently below $10 is 20% or more withina 12-month period as these companies are typically more volatile than the overall stock market. For Hold rated stocks with an average stock priceconsistently below $10, the expected total return (price appreciation plus yield) is plus or minus 20% within a 12-month period. For Underperformrated stocks with an average stock price consistently below $10, the expected total return (price appreciation plus yield) is minus 20% within a 12-month period.NR - The investment rating and price target have been temporarily suspended. Such suspensions are in compliance with applicable regulations and/or Jefferies policies.CS - Coverage Suspended. Jefferies has suspended coverage of this company.NC - Not covered. Jefferies does not cover this company.Restricted - Describes issuers where, in conjunction with Jefferies engagement in certain transactions, company policy or applicable securitiesregulations prohibit certain types of communications, including investment recommendations.Monitor - Describes stocks whose company fundamentals and financials are being monitored, and for which no financial projections or opinions onthe investment merits of the company are provided.
Valuation MethodologyJefferies' methodology for assigning ratings may include the following: market capitalization, maturity, growth/value, volatility and expected totalreturn over the next 12 months. The price targets are based on several methodologies, which may include, but are not restricted to, analyses of marketrisk, growth rate, revenue stream, discounted cash flow (DCF), EBITDA, EPS, cash flow (CF), free cash flow (FCF), EV/EBITDA, P/E, PE/growth, P/CF,P/FCF, premium (discount)/average group EV/EBITDA, premium (discount)/average group P/E, sum of the parts, net asset value, dividend returns,and return on equity (ROE) over the next 12 months.
Conviction List Methodology
Healthcare
Pharmaceuticals
September 12, 2013
page 40 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
1. The aim of the conviction list is to publicise the best individual stock ideas from Jefferies Global Research2. Only stocks with a Buy or Underperform rating are allowed to be included in the recommended list.3. Stocks are screened for minimum market capitalisation and adequate daily turnover. Furthermore, a valuation, correlation and style screen
is used to ensure a well-diversified portfolio.4. Stocks are sorted to a maximum of 30 stocks with the maximum country exposure at around 50%. Limits are also imposed on a sector basis.5. Once a month, analysts are invited to recommend their best ideas. Analysts’ stock selection can be based on one or more of the following:
non-Consensus investment view, difference in earnings relative to Consensus, valuation methodology, target upside/downside % relativeto the current stock price. These are then assessed against existing holdings to ensure consistency. Stocks that have either reached theirtarget price, been downgraded over the course of the month or where a more suitable candidate has been found are removed.
6. All stocks are inserted at the last closing price and removed at the last closing price. There are no changes to the conviction list duringthe month.
7. Performance is calculated in US dollars on an equally weighted basis and is compared to MSCI World AC US$.8. The conviction list is published once a month whilst global equity markets are closed.9. Transaction fees are not included.
10. All corporate actions are taken into account.
Risk which may impede the achievement of our Price TargetThis report was prepared for general circulation and does not provide investment recommendations specific to individual investors. As such, thefinancial instruments discussed in this report may not be suitable for all investors and investors must make their own investment decisions basedupon their specific investment objectives and financial situation utilizing their own financial advisors as they deem necessary. Past performance ofthe financial instruments recommended in this report should not be taken as an indication or guarantee of future results. The price, value of, andincome from, any of the financial instruments mentioned in this report can rise as well as fall and may be affected by changes in economic, financialand political factors. If a financial instrument is denominated in a currency other than the investor's home currency, a change in exchange rates mayadversely affect the price of, value of, or income derived from the financial instrument described in this report. In addition, investors in securities suchas ADRs, whose values are affected by the currency of the underlying security, effectively assume currency risk.
Other Companies Mentioned in This Report• Almirall (ALM SM: €8.69, HOLD)• AstraZeneca PLC (AZN LN: p3,195.00, HOLD)• Forest Laboratories, Inc. (FRX: $44.33, BUY)• GlaxoSmithKline Plc (GSK LN: p1,619.00, HOLD)• Merck & Co. (MRK: $48.14, BUY)• Novartis AG (NOVN VX: CHF71.10, BUY)• Roche (ROG VX: CHF237.90, BUY)
Distribution of RatingsIB Serv./Past 12 Mos.
Rating Count Percent Count Percent
BUY 814 47.55% 179 21.99%HOLD 756 44.16% 119 15.74%UNDERPERFORM 142 8.29% 1 0.70%
Other Important Disclosures
Jefferies Equity Research refers to research reports produced by analysts employed by one of the following Jefferies Group LLC (“Jefferies”) groupcompanies:
United States: Jefferies LLC which is an SEC registered firm and a member of FINRA.
United Kingdom: Jefferies International Limited, which is authorized and regulated by the Financial Conduct Authority; registered in England andWales No. 1978621; registered office: Vintners Place, 68 Upper Thames Street, London EC4V 3BJ; telephone +44 (0)20 7029 8000; facsimile +44 (0)207029 8010.
Hong Kong: Jefferies Hong Kong Limited, which is licensed by the Securities and Futures Commission of Hong Kong with CE number ATS546; locatedat Suite 2201, 22nd Floor, Cheung Kong Center, 2 Queen’s Road Central, Hong Kong.
Singapore: Jefferies Singapore Limited, which is licensed by the Monetary Authority of Singapore; located at 80 Raffles Place #15-20, UOB Plaza 2,Singapore 048624, telephone: +65 6551 3950.
Healthcare
Pharmaceuticals
September 12, 2013
page 41 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
Japan: Jefferies (Japan) Limited, Tokyo Branch, which is a securities company registered by the Financial Services Agency of Japan and is a memberof the Japan Securities Dealers Association; located at Hibiya Marine Bldg, 3F, 1-5-1 Yuraku-cho, Chiyoda-ku, Tokyo 100-0006; telephone +813 52516100; facsimile +813 5251 6101.
India: Jefferies India Private Limited, which is licensed by the Securities and Exchange Board of India as a Merchant Banker (INM000011443) and aStock Broker with Bombay Stock Exchange Limited (INB011491033) and National Stock Exchange of India Limited (INB231491037) in the Capital MarketSegment; located at 42/43, 2 North Avenue, Maker Maxity, Bandra-Kurla Complex, Bandra (East) Mumbai 400 051, India; Tel +91 22 4356 6000.
This material has been prepared by Jefferies employing appropriate expertise, and in the belief that it is fair and not misleading. The information setforth herein was obtained from sources believed to be reliable, but has not been independently verified by Jefferies. Therefore, except for any obligationunder applicable rules we do not guarantee its accuracy. Additional and supporting information is available upon request. Unless prohibited by theprovisions of Regulation S of the U.S. Securities Act of 1933, this material is distributed in the United States ("US"), by Jefferies LLC, a US-registeredbroker-dealer, which accepts responsibility for its contents in accordance with the provisions of Rule 15a-6, under the US Securities Exchange Act of1934. Transactions by or on behalf of any US person may only be effected through Jefferies LLC. In the United Kingdom and European EconomicArea this report is issued and/or approved for distribution by Jefferies International Limited and is intended for use only by persons who have, or havebeen assessed as having, suitable professional experience and expertise, or by persons to whom it can be otherwise lawfully distributed. JefferiesInternational Limited has adopted a conflicts management policy in connection with the preparation and publication of research, the details of whichare available upon request in writing to the Compliance Officer. Jefferies International Limited may allow its analysts to undertake private consultancywork. Jefferies International Limited’s conflicts management policy sets out the arrangements Jefferies International Limited employs to manage anypotential conflicts of interest that may arise as a result of such consultancy work. For Canadian investors, this material is intended for use only byprofessional or institutional investors. None of the investments or investment services mentioned or described herein is available to other personsor to anyone in Canada who is not a "Designated Institution" as defined by the Securities Act (Ontario). In Singapore, Jefferies Singapore Limited isregulated by the Monetary Authority of Singapore. For investors in the Republic of Singapore, this material is provided by Jefferies Singapore Limitedpursuant to Regulation 32C of the Financial Advisers Regulations. The material contained in this document is intended solely for accredited, expert orinstitutional investors, as defined under the Securities and Futures Act (Cap. 289 of Singapore). If there are any matters arising from, or in connectionwith this material, please contact Jefferies Singapore Limited, located at 80 Raffles Place #15-20, UOB Plaza 2, Singapore 048624, telephone: +656551 3950. In Japan this material is issued and distributed by Jefferies (Japan) Limited to institutional investors only. In Hong Kong, this report isissued and approved by Jefferies Hong Kong Limited and is intended for use only by professional investors as defined in the Hong Kong Securities andFutures Ordinance and its subsidiary legislation. In the Republic of China (Taiwan), this report should not be distributed. The research in relation tothis report is conducted outside the PRC. This report does not constitute an offer to sell or the solicitation of an offer to buy any securities in the PRC.PRC investors shall have the relevant qualifications to invest in such securities and shall be responsible for obtaining all relevant approvals, licenses,verifications and/or registrations from the relevant governmental authorities themselves. In India this report is made available by Jefferies India PrivateLimited. In Australia this information is issued solely by Jefferies International Limited and is directed solely at wholesale clients within the meaning ofthe Corporations Act 2001 of Australia (the "Act") in connection with their consideration of any investment or investment service that is the subject ofthis document. Any offer or issue that is the subject of this document does not require, and this document is not, a disclosure document or productdisclosure statement within the meaning of the Act. Jefferies International Limited is authorised and regulated by the Financial Conduct Authorityunder the laws of the United Kingdom, which differ from Australian laws. Jefferies International Limited has obtained relief under Australian Securitiesand Investments Commission Class Order 03/1099, which conditionally exempts it from holding an Australian financial services licence under theAct in respect of the provision of certain financial services to wholesale clients. Recipients of this document in any other jurisdictions should informthemselves about and observe any applicable legal requirements in relation to the receipt of this document.
This report is not an offer or solicitation of an offer to buy or sell any security or derivative instrument, or to make any investment. Any opinion orestimate constitutes the preparer's best judgment as of the date of preparation, and is subject to change without notice. Jefferies assumes no obligationto maintain or update this report based on subsequent information and events. Jefferies, its associates or affiliates, and its respective officers, directors,and employees may have long or short positions in, or may buy or sell any of the securities, derivative instruments or other investments mentioned ordescribed herein, either as agent or as principal for their own account. Upon request Jefferies may provide specialized research products or servicesto certain customers focusing on the prospects for individual covered stocks as compared to other covered stocks over varying time horizons orunder differing market conditions. While the views expressed in these situations may not always be directionally consistent with the long-term viewsexpressed in the analyst's published research, the analyst has a reasonable basis and any inconsistencies can be reasonably explained. This materialdoes not constitute a personal recommendation or take into account the particular investment objectives, financial situations, or needs of individualclients. Clients should consider whether any advice or recommendation in this report is suitable for their particular circumstances and, if appropriate,seek professional advice, including tax advice. The price and value of the investments referred to herein and the income from them may fluctuate. Pastperformance is not a guide to future performance, future returns are not guaranteed, and a loss of original capital may occur. Fluctuations in exchangerates could have adverse effects on the value or price of, or income derived from, certain investments. This report has been prepared independently ofany issuer of securities mentioned herein and not in connection with any proposed offering of securities or as agent of any issuer of securities. Noneof Jefferies, any of its affiliates or its research analysts has any authority whatsoever to make any representations or warranty on behalf of the issuer(s).Jefferies policy prohibits research personnel from disclosing a recommendation, investment rating, or investment thesis for review by an issuer priorto the publication of a research report containing such rating, recommendation or investment thesis. Any comments or statements made herein arethose of the author(s) and may differ from the views of Jefferies.
This report may contain information obtained from third parties, including ratings from credit ratings agencies such as Standard & Poor’s. Reproductionand distribution of third party content in any form is prohibited except with the prior written permission of the related third party. Third party contentproviders do not guarantee the accuracy, completeness, timeliness or availability of any information, including ratings, and are not responsible forany errors or omissions (negligent or otherwise), regardless of the cause, or for the results obtained from the use of such content. Third party contentproviders give no express or implied warranties, including, but not limited to, any warranties of merchantability or fitness for a particular purpose or
Healthcare
Pharmaceuticals
September 12, 2013
page 42 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.

use. Third party content providers shall not be liable for any direct, indirect, incidental, exemplary, compensatory, punitive, special or consequentialdamages, costs, expenses, legal fees, or losses (including lost income or profits and opportunity costs) in connection with any use of their content,including ratings. Credit ratings are statements of opinions and are not statements of fact or recommendations to purchase, hold or sell securities. Theydo not address the suitability of securities or the suitability of securities for investment purposes, and should not be relied on as investment advice.
Jefferies research reports are disseminated and available primarily electronically, and, in some cases, in printed form. Electronic research issimultaneously available to all clients. This report or any portion hereof may not be reprinted, sold or redistributed without the written consent ofJefferies. Neither Jefferies nor any officer nor employee of Jefferies accepts any liability whatsoever for any direct, indirect or consequential damagesor losses arising from any use of this report or its contents.
For Important Disclosure information, please visit our website at https://javatar.bluematrix.com/sellside/Disclosures.action or call 1.888.JEFFERIES
© 2013 Jefferies Group LLC
Healthcare
Pharmaceuticals
September 12, 2013
page 43 of 43 , Equity Analyst, (212) 336-7409, [email protected] Holford, PhD, ACA
Please see important disclosure information on pages 40 - 43 of this report.
![The effect of exacerbation history on outcomes in the ... · treatment with LAMA/LABA versus ICS/LABA [14], or with ICS/LAMA/LABA single-inhaler triple therapy versus ICS/LABA or](https://img.pdfslide.us/doc/110x75/5f2bc7ab0568d57da721eaf0/the-effect-of-exacerbation-history-on-outcomes-in-the-treatment-with-lamalaba.jpg)
















![€¦ · Web viewBACKGROUND. T. riple fixed-dose combinations (inhaled . glucocorticoid [ICS]/ long-acting mus. carinic antagonist [LAMA]/ long-acting β. 2-agonist [LABA]) for](https://img.pdfslide.us/doc/110x75/60b248cbf19f060b930e921f/web-view-background-t-riple-fixed-dose-combinations-inhaled-glucocorticoid.jpg)










