Embed Size (px)
Citation preview
Pharmaceuticals and the DevelopingWorld
Michael Kremer
Pharmaceuticals have brought tremendous health bene ts to developingcountries but existing pharmaceuticals are often underused or misusedand pharmaceutical RampD on health problems speci c to poor countries is
woefully inadequateThe role of pharmaceuticals and medical technology in improving health in
developing countries stands in contrast to the historical experience of the devel-oped countries Historically health in currently developed countries improvedlargely due to higher incomes and consequent improvements in nutrition sanita-tion and water supplies Fogel (1986) nds that half of the decline in standardizedBritish death rates and 70 percent of the decline in standardized American deathrates between 1700 and 1980 occurred before 1911 in an era with few effectivemedicines However modern medical technologies allow tremendous improve-ments in health even at low income levels The outward shift of the technologicalfrontier is illustrated by Vietnam which has a life expectancy of 69 years despite aper capita income that according to of cial statistics is less than one-tenth that ofthe United States in 1900 which had a 47-year life expectancy1 To take anotherexample per capita GDP in low-income sub-Saharan African nations decreased13 percent from 1972 through 1992 but life expectancy increased by 10 percent
1 Data are from Balke and Gordon (1989) Johnston and Williamson (2002) Kurian (1994) and WorldBank (2001b) Even if GDP growth in the United States were underestimated by two percentage pointsannually 1900 US per capita GDP exceeds Vietnamrsquos current per capita GDP
y Michael Kremer is Professor of Economics Harvard University Cambridge MassachusettsSenior Fellow The Brookings Institution Washington DC and Research Fellow NationalBureau of Economic Research Cambridge Massachusetts His e-mail address ismkremerfasharvardedu
Journal of Economic PerspectivesmdashVolume 16 Number 4mdashFall 2002mdashPages 67ndash90
from 45 to 49 years and infant mortality fell 30 percent from 133 per thousandbirths to 93 per thousand births (World Bank 2001b) (Unfortunately since thenlife expectancy in sub-Saharan Africa has fallen due to the AIDS pandemic)Indeed analysis of worldwide health trends in the twentieth century has found thatmost improvements resulted from technological advances rather than from incomegrowth Using the cross-sectional relationship between income and life expectancyPreston (1975) estimated that income growth accounted for only 10 to 25 percentof the growth in world life expectancy between the 1930s and 1960s and suggestedthat the diffusion of technological advances was a major factor for the increase inlife expectancy at any given income level Jamison et al (2001) attribute 74 percentof the decline in infant mortality rates over the period from 1962 to 1987 totechnical progress 21 percent to greater education and only about 5 percent toincome growth
While other technological improvementsmdashsuch as the development of oralrehydration therapy against diarrhea and the use of radios in public health cam-paignsmdashmay have played a role in improving health the development and dissem-ination of pharmaceuticals has played a key role To take one example aboutthree-quarters of the worldrsquos children receive a standard package of cheap off-patent vaccines through the World Health Organizationrsquos (WHO) Expanded Pro-gram on Immunization and these vaccines are estimated to save 3 million lives peryear (Kim-Farley 1992) Though vaccination rates are uneven around the worldthe World Bank (2001b) estimates that 70 percent of infants in low-income coun-tries received the three-dose DTP (diphtheria tetanus and pertussis) vaccine overthe period from 1995 through 1999
Yet many people in developing countries who could bene t from pharmaceu-ticals do not receive them The failure of antiretroviral therapy to reach more thana tiny fraction of people with AIDS in developing countries has attracted wide-spread publicity but even medicines that are far cheaper and easier to deliver arenot reaching many of the people who need them More than a quarter of childrenworldwide and over half of children in some countries do not receive the vaccinesthat are part of WHOrsquos Expanded Program on Immunization although these costonly pennies per dose and require no diagnosis Three million lives are lostannually as a result (World Bank 2001a) Only a small fraction of children in poorcountries receive the newer hepatitis B and Haemophilus in uenzae b (Hib)vaccines which cost a dollar or two per dose One in four people worldwide sufferfrom intestinal worms although treatments only need to be taken once or twice peryear have virtually no side effects and cost less than a dollar per year Theseexamples suggest that while intellectual property rights undoubtedly prevent somefrom obtaining needed pharmaceuticals eliminating these rights would not helpthe majority of those without access to drugs
While developing countries have obtained substantial bene ts from pharma-ceuticals originally developed for rich country markets little research is conductedon diseases that primarily affect poor countries such as malaria or tuberculosisPecoul et al (1999) report that of the 1233 drugs licensed worldwide between 1975
68 Journal of Economic Perspectives
and 1997 only 13 were for tropical diseases Of these ve came from veterinaryresearch two were modi cations of existing medicines and two were produced forthe US military Only four were developed by commercial pharmaceutical rmsspeci cally for tropical diseases of humans According to WHO (1996) 50 percentof global health research and development in 1992 was undertaken by privateindustry but less than 5 percent of that was spent on diseases speci c to lessdeveloped countries Even for diseases that affect both rich and poor countriesresearch tends to focus on products that are best suited for use in rich countriesFor example much research is conducted on sophisticated AIDS drugs that areuseful in developed countries but are too expensive and dif cult to deliver to themajority of the population in the poorest countries Much less research is con-ducted on vaccines which are typically much more feasible to deliver than drugs indeveloping countries since they often require only a few doses to deliver and canbe delivered by personnel with limited medical training
The controversy over intellectual property rights for pharmaceuticals andaccess to antiretroviral therapies in developing countries has been the subject ofmuch public debate recently This article provides a broader context for the debateIt rst reviews characteristics of the developing country market for pharmaceuti-cals including small markets distinct disease environments and weak health careand regulatory systems It then outlines key market and government failuresExisting products are underused to the extent that patients do not take intoaccount positive externalities from reducing the spread of communicable diseaseand that monopolyoligopoly pricing of pharmaceuticals leads to prices greaterthan marginal cost overused to the extent that patients do not take into accountnegative externalities from encouraging the development of drug-resistant strainsand underused overused and misused due to asymmetric information betweenpatients and providers and inef cient government health care delivery RampD onnew pharmaceuticals is undersupplied because competitive markets do not rewardRampD expenditures and because governments face free-rider problems in supplyingthe global public good of RampD and have time-inconsistent preferences regardingrewarding rms for doing so
Drawing on this background the article then explores policy options forbroadening access to pharmaceuticals and encouraging RampD on products neededin developing countries In particular it explores differential pricing priorities forforeign assistance in health the prospects for addressing pharmaceutical misuse byimproving health care delivery systems drug regulation and the potential for richcountries or international organizations to encourage research and developmenton products needed by developing countries by committing to buy the productsonce they are developed and make them available to those who need them
Characteristics of the Pharmaceutical Market in Developing Countries
The market for pharmaceuticals in developing countries differs in several waysfrom that in the developed world
Michael Kremer 69
Small MarketsThe market for pharmaceuticals in the poorest countries is tiny Connecticut
spends more on health than the 38 low-income countries of sub-Saharan Africacombined (World Bank 2001b US Census 2000) In 1998 US public andprivate health spending constituted 13 percent of its almost $32000 per capitaincome for a total of more than $4000 per person In contrast low-incomesub-Saharan African nations spent only 6 percent of their average $300 per capitaGDP on health or around $18 per person (World Bank 2001b) though develop-ing countries spend a higher percentage of their health budgets on pharmaceuti-cals than do developed countries Drug developers often do not even bother to takeout patents in small poor countries (Attaran and Gillespie-White 2001)
Middle-income country markets are small but comprise a signi cant andgrowing source of revenue for pharmaceutical rms The Pharmaceutical Researchand Manufacturers of America (PhRMA) estimate that while only 1 percent of theirmarket is in Africa including middle-income countries such as South Africa7 percent is in Southeast Asia and China and 75 percent is in Latin America(PhRMA 2000) as shown in Table 1
Different Disease EnvironmentDeveloping countries face a signi cantly different disease environment than
developed countries due to both their poverty and their geography The burden ofdifferent diseases can be compared across countries using the concept of DisabilityAdjusted Life Years (Murray and Lopez 1996) DALYs take into account not onlythe lives lost through disease but also the number of years of disability causedWorld Health Organization (2001) estimates imply that infectious and parasiticdiseases account for one-third of the disease burden in low-income countries (infact for nearly half of Africarsquos disease burden) but only 3 percent of the burden inhigh-income countries as seen in Table 2 (WHO 2001) In contrast the disease
Table 1World Pharmaceutical MarketSales by Region 1998
Region Percentage of Market
United States 396Europe 261Japan 154Latin America 75Southeast Asia amp China 70Canada 19Africa 10Middle East 09Australasia 06
Source PhRMA (2000 adapted from Figure 7-2)
70 Journal of Economic Perspectives
burden in high-income countries mainly consists of noncommunicable conditionslike cancer and cardiovascular disease Table 3 lists speci c diseases for which morethan 99 percent of the burden falls in low- and middle-income countries whichinclude malaria schistosomiasis and leprosy (Lanjouw and Cockburn 2001)
Table 2Percentage of Disease Burden
Cause WorldLow-IncomeCountries
Middle-IncomeCountries
High-IncomeCountries
Infectious and parasitic diseases 231 333 139 30Tuberculosis 24 29 22 03HIVAIDS 61 97 26 07Malaria 27 45 10 00
Noncommunicable conditions 461 332 555 827Malignant neoplasms (cancers) 53 29 67 144Cardiovascular diseases 103 77 123 164
Sources World Health Report (2001) World Bank (2001b)
Table 3Diseases for Which 99 Percent or More of the Global Burden Fellon Low- and Middle-Income Countries in 1990
Disease
Disability AdjustedLife Years
(Thousands 2000)Deaths per Year
(2000)
Chagas disease 680 21299Dengue 433 12037Ancylostomiasis and necatoriasis (hookworm) 1829 5650Japanese encephalitis 426 3502Lymphatic lariasis 5549 404Malaria 40213 1079877Onchocerciasis (river blindness) 951 mdashSchistosomiasis 1713 11473Tetanus 9766 308662Trachoma 1181 14Trichuriasis 1640 2123Trypanosomiasis 1585 49668Leishmaniasis 1810 40913Measles 27549 776626Poliomyelitis 184 675Syphilis 5574 196533Diphtheria 114 3394Leprosy 141 2268Pertussis 12768 296099Diarrhoeal diseases 62227 2124032
Sources Global Burden from WHO (1996) quoted in Lanjouw and Cockburn (2001 Table 1) Figuresupdated from Lanjouw and Cockburn (2001) using WHO (2001)
Pharmaceuticals and the Developing World 71
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives

from 45 to 49 years and infant mortality fell 30 percent from 133 per thousandbirths to 93 per thousand births (World Bank 2001b) (Unfortunately since thenlife expectancy in sub-Saharan Africa has fallen due to the AIDS pandemic)Indeed analysis of worldwide health trends in the twentieth century has found thatmost improvements resulted from technological advances rather than from incomegrowth Using the cross-sectional relationship between income and life expectancyPreston (1975) estimated that income growth accounted for only 10 to 25 percentof the growth in world life expectancy between the 1930s and 1960s and suggestedthat the diffusion of technological advances was a major factor for the increase inlife expectancy at any given income level Jamison et al (2001) attribute 74 percentof the decline in infant mortality rates over the period from 1962 to 1987 totechnical progress 21 percent to greater education and only about 5 percent toincome growth
While other technological improvementsmdashsuch as the development of oralrehydration therapy against diarrhea and the use of radios in public health cam-paignsmdashmay have played a role in improving health the development and dissem-ination of pharmaceuticals has played a key role To take one example aboutthree-quarters of the worldrsquos children receive a standard package of cheap off-patent vaccines through the World Health Organizationrsquos (WHO) Expanded Pro-gram on Immunization and these vaccines are estimated to save 3 million lives peryear (Kim-Farley 1992) Though vaccination rates are uneven around the worldthe World Bank (2001b) estimates that 70 percent of infants in low-income coun-tries received the three-dose DTP (diphtheria tetanus and pertussis) vaccine overthe period from 1995 through 1999
Yet many people in developing countries who could bene t from pharmaceu-ticals do not receive them The failure of antiretroviral therapy to reach more thana tiny fraction of people with AIDS in developing countries has attracted wide-spread publicity but even medicines that are far cheaper and easier to deliver arenot reaching many of the people who need them More than a quarter of childrenworldwide and over half of children in some countries do not receive the vaccinesthat are part of WHOrsquos Expanded Program on Immunization although these costonly pennies per dose and require no diagnosis Three million lives are lostannually as a result (World Bank 2001a) Only a small fraction of children in poorcountries receive the newer hepatitis B and Haemophilus in uenzae b (Hib)vaccines which cost a dollar or two per dose One in four people worldwide sufferfrom intestinal worms although treatments only need to be taken once or twice peryear have virtually no side effects and cost less than a dollar per year Theseexamples suggest that while intellectual property rights undoubtedly prevent somefrom obtaining needed pharmaceuticals eliminating these rights would not helpthe majority of those without access to drugs
While developing countries have obtained substantial bene ts from pharma-ceuticals originally developed for rich country markets little research is conductedon diseases that primarily affect poor countries such as malaria or tuberculosisPecoul et al (1999) report that of the 1233 drugs licensed worldwide between 1975
68 Journal of Economic Perspectives
and 1997 only 13 were for tropical diseases Of these ve came from veterinaryresearch two were modi cations of existing medicines and two were produced forthe US military Only four were developed by commercial pharmaceutical rmsspeci cally for tropical diseases of humans According to WHO (1996) 50 percentof global health research and development in 1992 was undertaken by privateindustry but less than 5 percent of that was spent on diseases speci c to lessdeveloped countries Even for diseases that affect both rich and poor countriesresearch tends to focus on products that are best suited for use in rich countriesFor example much research is conducted on sophisticated AIDS drugs that areuseful in developed countries but are too expensive and dif cult to deliver to themajority of the population in the poorest countries Much less research is con-ducted on vaccines which are typically much more feasible to deliver than drugs indeveloping countries since they often require only a few doses to deliver and canbe delivered by personnel with limited medical training
The controversy over intellectual property rights for pharmaceuticals andaccess to antiretroviral therapies in developing countries has been the subject ofmuch public debate recently This article provides a broader context for the debateIt rst reviews characteristics of the developing country market for pharmaceuti-cals including small markets distinct disease environments and weak health careand regulatory systems It then outlines key market and government failuresExisting products are underused to the extent that patients do not take intoaccount positive externalities from reducing the spread of communicable diseaseand that monopolyoligopoly pricing of pharmaceuticals leads to prices greaterthan marginal cost overused to the extent that patients do not take into accountnegative externalities from encouraging the development of drug-resistant strainsand underused overused and misused due to asymmetric information betweenpatients and providers and inef cient government health care delivery RampD onnew pharmaceuticals is undersupplied because competitive markets do not rewardRampD expenditures and because governments face free-rider problems in supplyingthe global public good of RampD and have time-inconsistent preferences regardingrewarding rms for doing so
Drawing on this background the article then explores policy options forbroadening access to pharmaceuticals and encouraging RampD on products neededin developing countries In particular it explores differential pricing priorities forforeign assistance in health the prospects for addressing pharmaceutical misuse byimproving health care delivery systems drug regulation and the potential for richcountries or international organizations to encourage research and developmenton products needed by developing countries by committing to buy the productsonce they are developed and make them available to those who need them
Characteristics of the Pharmaceutical Market in Developing Countries
The market for pharmaceuticals in developing countries differs in several waysfrom that in the developed world
Michael Kremer 69
Small MarketsThe market for pharmaceuticals in the poorest countries is tiny Connecticut
spends more on health than the 38 low-income countries of sub-Saharan Africacombined (World Bank 2001b US Census 2000) In 1998 US public andprivate health spending constituted 13 percent of its almost $32000 per capitaincome for a total of more than $4000 per person In contrast low-incomesub-Saharan African nations spent only 6 percent of their average $300 per capitaGDP on health or around $18 per person (World Bank 2001b) though develop-ing countries spend a higher percentage of their health budgets on pharmaceuti-cals than do developed countries Drug developers often do not even bother to takeout patents in small poor countries (Attaran and Gillespie-White 2001)
Middle-income country markets are small but comprise a signi cant andgrowing source of revenue for pharmaceutical rms The Pharmaceutical Researchand Manufacturers of America (PhRMA) estimate that while only 1 percent of theirmarket is in Africa including middle-income countries such as South Africa7 percent is in Southeast Asia and China and 75 percent is in Latin America(PhRMA 2000) as shown in Table 1
Different Disease EnvironmentDeveloping countries face a signi cantly different disease environment than
developed countries due to both their poverty and their geography The burden ofdifferent diseases can be compared across countries using the concept of DisabilityAdjusted Life Years (Murray and Lopez 1996) DALYs take into account not onlythe lives lost through disease but also the number of years of disability causedWorld Health Organization (2001) estimates imply that infectious and parasiticdiseases account for one-third of the disease burden in low-income countries (infact for nearly half of Africarsquos disease burden) but only 3 percent of the burden inhigh-income countries as seen in Table 2 (WHO 2001) In contrast the disease
Table 1World Pharmaceutical MarketSales by Region 1998
Region Percentage of Market
United States 396Europe 261Japan 154Latin America 75Southeast Asia amp China 70Canada 19Africa 10Middle East 09Australasia 06
Source PhRMA (2000 adapted from Figure 7-2)
70 Journal of Economic Perspectives
burden in high-income countries mainly consists of noncommunicable conditionslike cancer and cardiovascular disease Table 3 lists speci c diseases for which morethan 99 percent of the burden falls in low- and middle-income countries whichinclude malaria schistosomiasis and leprosy (Lanjouw and Cockburn 2001)
Table 2Percentage of Disease Burden
Cause WorldLow-IncomeCountries
Middle-IncomeCountries
High-IncomeCountries
Infectious and parasitic diseases 231 333 139 30Tuberculosis 24 29 22 03HIVAIDS 61 97 26 07Malaria 27 45 10 00
Noncommunicable conditions 461 332 555 827Malignant neoplasms (cancers) 53 29 67 144Cardiovascular diseases 103 77 123 164
Sources World Health Report (2001) World Bank (2001b)
Table 3Diseases for Which 99 Percent or More of the Global Burden Fellon Low- and Middle-Income Countries in 1990
Disease
Disability AdjustedLife Years
(Thousands 2000)Deaths per Year
(2000)
Chagas disease 680 21299Dengue 433 12037Ancylostomiasis and necatoriasis (hookworm) 1829 5650Japanese encephalitis 426 3502Lymphatic lariasis 5549 404Malaria 40213 1079877Onchocerciasis (river blindness) 951 mdashSchistosomiasis 1713 11473Tetanus 9766 308662Trachoma 1181 14Trichuriasis 1640 2123Trypanosomiasis 1585 49668Leishmaniasis 1810 40913Measles 27549 776626Poliomyelitis 184 675Syphilis 5574 196533Diphtheria 114 3394Leprosy 141 2268Pertussis 12768 296099Diarrhoeal diseases 62227 2124032
Sources Global Burden from WHO (1996) quoted in Lanjouw and Cockburn (2001 Table 1) Figuresupdated from Lanjouw and Cockburn (2001) using WHO (2001)
Pharmaceuticals and the Developing World 71
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
and 1997 only 13 were for tropical diseases Of these ve came from veterinaryresearch two were modi cations of existing medicines and two were produced forthe US military Only four were developed by commercial pharmaceutical rmsspeci cally for tropical diseases of humans According to WHO (1996) 50 percentof global health research and development in 1992 was undertaken by privateindustry but less than 5 percent of that was spent on diseases speci c to lessdeveloped countries Even for diseases that affect both rich and poor countriesresearch tends to focus on products that are best suited for use in rich countriesFor example much research is conducted on sophisticated AIDS drugs that areuseful in developed countries but are too expensive and dif cult to deliver to themajority of the population in the poorest countries Much less research is con-ducted on vaccines which are typically much more feasible to deliver than drugs indeveloping countries since they often require only a few doses to deliver and canbe delivered by personnel with limited medical training
The controversy over intellectual property rights for pharmaceuticals andaccess to antiretroviral therapies in developing countries has been the subject ofmuch public debate recently This article provides a broader context for the debateIt rst reviews characteristics of the developing country market for pharmaceuti-cals including small markets distinct disease environments and weak health careand regulatory systems It then outlines key market and government failuresExisting products are underused to the extent that patients do not take intoaccount positive externalities from reducing the spread of communicable diseaseand that monopolyoligopoly pricing of pharmaceuticals leads to prices greaterthan marginal cost overused to the extent that patients do not take into accountnegative externalities from encouraging the development of drug-resistant strainsand underused overused and misused due to asymmetric information betweenpatients and providers and inef cient government health care delivery RampD onnew pharmaceuticals is undersupplied because competitive markets do not rewardRampD expenditures and because governments face free-rider problems in supplyingthe global public good of RampD and have time-inconsistent preferences regardingrewarding rms for doing so
Drawing on this background the article then explores policy options forbroadening access to pharmaceuticals and encouraging RampD on products neededin developing countries In particular it explores differential pricing priorities forforeign assistance in health the prospects for addressing pharmaceutical misuse byimproving health care delivery systems drug regulation and the potential for richcountries or international organizations to encourage research and developmenton products needed by developing countries by committing to buy the productsonce they are developed and make them available to those who need them
Characteristics of the Pharmaceutical Market in Developing Countries
The market for pharmaceuticals in developing countries differs in several waysfrom that in the developed world
Michael Kremer 69
Small MarketsThe market for pharmaceuticals in the poorest countries is tiny Connecticut
spends more on health than the 38 low-income countries of sub-Saharan Africacombined (World Bank 2001b US Census 2000) In 1998 US public andprivate health spending constituted 13 percent of its almost $32000 per capitaincome for a total of more than $4000 per person In contrast low-incomesub-Saharan African nations spent only 6 percent of their average $300 per capitaGDP on health or around $18 per person (World Bank 2001b) though develop-ing countries spend a higher percentage of their health budgets on pharmaceuti-cals than do developed countries Drug developers often do not even bother to takeout patents in small poor countries (Attaran and Gillespie-White 2001)
Middle-income country markets are small but comprise a signi cant andgrowing source of revenue for pharmaceutical rms The Pharmaceutical Researchand Manufacturers of America (PhRMA) estimate that while only 1 percent of theirmarket is in Africa including middle-income countries such as South Africa7 percent is in Southeast Asia and China and 75 percent is in Latin America(PhRMA 2000) as shown in Table 1
Different Disease EnvironmentDeveloping countries face a signi cantly different disease environment than
developed countries due to both their poverty and their geography The burden ofdifferent diseases can be compared across countries using the concept of DisabilityAdjusted Life Years (Murray and Lopez 1996) DALYs take into account not onlythe lives lost through disease but also the number of years of disability causedWorld Health Organization (2001) estimates imply that infectious and parasiticdiseases account for one-third of the disease burden in low-income countries (infact for nearly half of Africarsquos disease burden) but only 3 percent of the burden inhigh-income countries as seen in Table 2 (WHO 2001) In contrast the disease
Table 1World Pharmaceutical MarketSales by Region 1998
Region Percentage of Market
United States 396Europe 261Japan 154Latin America 75Southeast Asia amp China 70Canada 19Africa 10Middle East 09Australasia 06
Source PhRMA (2000 adapted from Figure 7-2)
70 Journal of Economic Perspectives
burden in high-income countries mainly consists of noncommunicable conditionslike cancer and cardiovascular disease Table 3 lists speci c diseases for which morethan 99 percent of the burden falls in low- and middle-income countries whichinclude malaria schistosomiasis and leprosy (Lanjouw and Cockburn 2001)
Table 2Percentage of Disease Burden
Cause WorldLow-IncomeCountries
Middle-IncomeCountries
High-IncomeCountries
Infectious and parasitic diseases 231 333 139 30Tuberculosis 24 29 22 03HIVAIDS 61 97 26 07Malaria 27 45 10 00
Noncommunicable conditions 461 332 555 827Malignant neoplasms (cancers) 53 29 67 144Cardiovascular diseases 103 77 123 164
Sources World Health Report (2001) World Bank (2001b)
Table 3Diseases for Which 99 Percent or More of the Global Burden Fellon Low- and Middle-Income Countries in 1990
Disease
Disability AdjustedLife Years
(Thousands 2000)Deaths per Year
(2000)
Chagas disease 680 21299Dengue 433 12037Ancylostomiasis and necatoriasis (hookworm) 1829 5650Japanese encephalitis 426 3502Lymphatic lariasis 5549 404Malaria 40213 1079877Onchocerciasis (river blindness) 951 mdashSchistosomiasis 1713 11473Tetanus 9766 308662Trachoma 1181 14Trichuriasis 1640 2123Trypanosomiasis 1585 49668Leishmaniasis 1810 40913Measles 27549 776626Poliomyelitis 184 675Syphilis 5574 196533Diphtheria 114 3394Leprosy 141 2268Pertussis 12768 296099Diarrhoeal diseases 62227 2124032
Sources Global Burden from WHO (1996) quoted in Lanjouw and Cockburn (2001 Table 1) Figuresupdated from Lanjouw and Cockburn (2001) using WHO (2001)
Pharmaceuticals and the Developing World 71
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
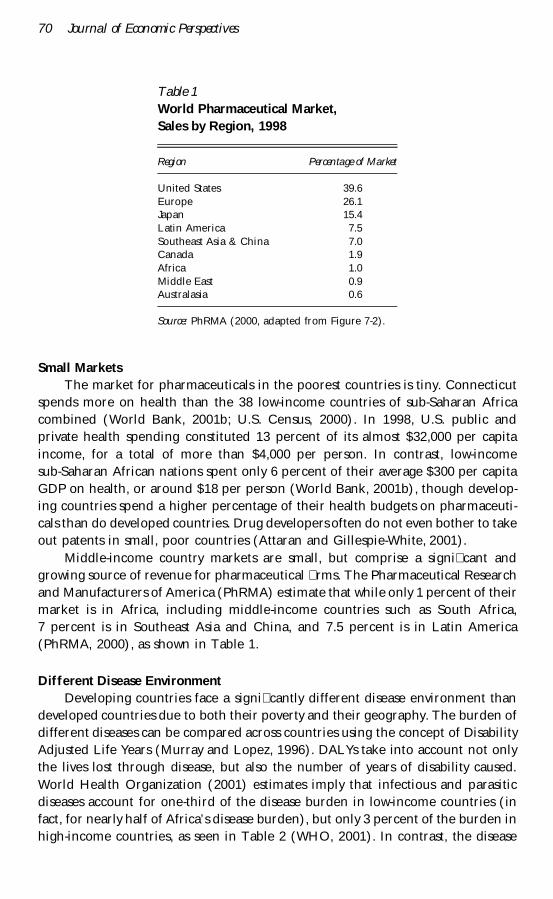
Small MarketsThe market for pharmaceuticals in the poorest countries is tiny Connecticut
spends more on health than the 38 low-income countries of sub-Saharan Africacombined (World Bank 2001b US Census 2000) In 1998 US public andprivate health spending constituted 13 percent of its almost $32000 per capitaincome for a total of more than $4000 per person In contrast low-incomesub-Saharan African nations spent only 6 percent of their average $300 per capitaGDP on health or around $18 per person (World Bank 2001b) though develop-ing countries spend a higher percentage of their health budgets on pharmaceuti-cals than do developed countries Drug developers often do not even bother to takeout patents in small poor countries (Attaran and Gillespie-White 2001)
Middle-income country markets are small but comprise a signi cant andgrowing source of revenue for pharmaceutical rms The Pharmaceutical Researchand Manufacturers of America (PhRMA) estimate that while only 1 percent of theirmarket is in Africa including middle-income countries such as South Africa7 percent is in Southeast Asia and China and 75 percent is in Latin America(PhRMA 2000) as shown in Table 1
Different Disease EnvironmentDeveloping countries face a signi cantly different disease environment than
developed countries due to both their poverty and their geography The burden ofdifferent diseases can be compared across countries using the concept of DisabilityAdjusted Life Years (Murray and Lopez 1996) DALYs take into account not onlythe lives lost through disease but also the number of years of disability causedWorld Health Organization (2001) estimates imply that infectious and parasiticdiseases account for one-third of the disease burden in low-income countries (infact for nearly half of Africarsquos disease burden) but only 3 percent of the burden inhigh-income countries as seen in Table 2 (WHO 2001) In contrast the disease
Table 1World Pharmaceutical MarketSales by Region 1998
Region Percentage of Market
United States 396Europe 261Japan 154Latin America 75Southeast Asia amp China 70Canada 19Africa 10Middle East 09Australasia 06
Source PhRMA (2000 adapted from Figure 7-2)
70 Journal of Economic Perspectives
burden in high-income countries mainly consists of noncommunicable conditionslike cancer and cardiovascular disease Table 3 lists speci c diseases for which morethan 99 percent of the burden falls in low- and middle-income countries whichinclude malaria schistosomiasis and leprosy (Lanjouw and Cockburn 2001)
Table 2Percentage of Disease Burden
Cause WorldLow-IncomeCountries
Middle-IncomeCountries
High-IncomeCountries
Infectious and parasitic diseases 231 333 139 30Tuberculosis 24 29 22 03HIVAIDS 61 97 26 07Malaria 27 45 10 00
Noncommunicable conditions 461 332 555 827Malignant neoplasms (cancers) 53 29 67 144Cardiovascular diseases 103 77 123 164
Sources World Health Report (2001) World Bank (2001b)
Table 3Diseases for Which 99 Percent or More of the Global Burden Fellon Low- and Middle-Income Countries in 1990
Disease
Disability AdjustedLife Years
(Thousands 2000)Deaths per Year
(2000)
Chagas disease 680 21299Dengue 433 12037Ancylostomiasis and necatoriasis (hookworm) 1829 5650Japanese encephalitis 426 3502Lymphatic lariasis 5549 404Malaria 40213 1079877Onchocerciasis (river blindness) 951 mdashSchistosomiasis 1713 11473Tetanus 9766 308662Trachoma 1181 14Trichuriasis 1640 2123Trypanosomiasis 1585 49668Leishmaniasis 1810 40913Measles 27549 776626Poliomyelitis 184 675Syphilis 5574 196533Diphtheria 114 3394Leprosy 141 2268Pertussis 12768 296099Diarrhoeal diseases 62227 2124032
Sources Global Burden from WHO (1996) quoted in Lanjouw and Cockburn (2001 Table 1) Figuresupdated from Lanjouw and Cockburn (2001) using WHO (2001)
Pharmaceuticals and the Developing World 71
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
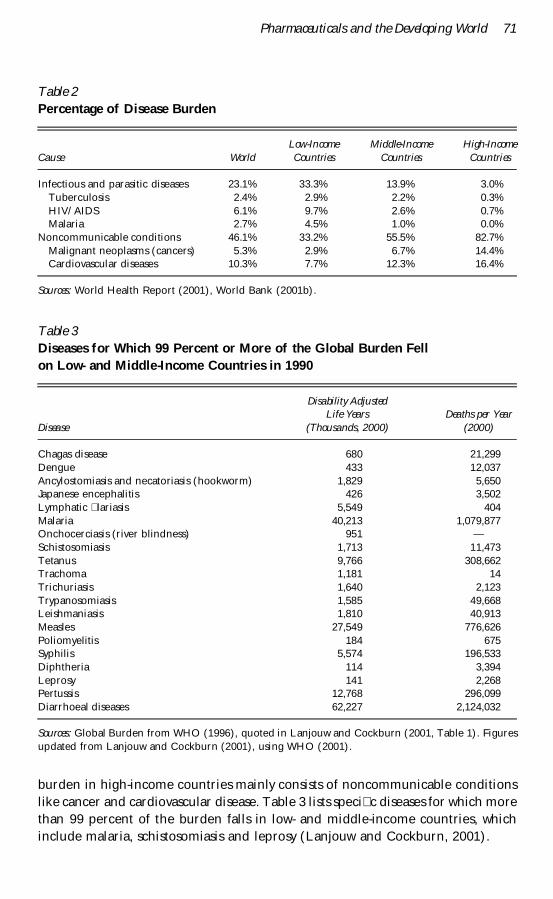
burden in high-income countries mainly consists of noncommunicable conditionslike cancer and cardiovascular disease Table 3 lists speci c diseases for which morethan 99 percent of the burden falls in low- and middle-income countries whichinclude malaria schistosomiasis and leprosy (Lanjouw and Cockburn 2001)
Table 2Percentage of Disease Burden
Cause WorldLow-IncomeCountries
Middle-IncomeCountries
High-IncomeCountries
Infectious and parasitic diseases 231 333 139 30Tuberculosis 24 29 22 03HIVAIDS 61 97 26 07Malaria 27 45 10 00
Noncommunicable conditions 461 332 555 827Malignant neoplasms (cancers) 53 29 67 144Cardiovascular diseases 103 77 123 164
Sources World Health Report (2001) World Bank (2001b)
Table 3Diseases for Which 99 Percent or More of the Global Burden Fellon Low- and Middle-Income Countries in 1990
Disease
Disability AdjustedLife Years
(Thousands 2000)Deaths per Year
(2000)
Chagas disease 680 21299Dengue 433 12037Ancylostomiasis and necatoriasis (hookworm) 1829 5650Japanese encephalitis 426 3502Lymphatic lariasis 5549 404Malaria 40213 1079877Onchocerciasis (river blindness) 951 mdashSchistosomiasis 1713 11473Tetanus 9766 308662Trachoma 1181 14Trichuriasis 1640 2123Trypanosomiasis 1585 49668Leishmaniasis 1810 40913Measles 27549 776626Poliomyelitis 184 675Syphilis 5574 196533Diphtheria 114 3394Leprosy 141 2268Pertussis 12768 296099Diarrhoeal diseases 62227 2124032
Sources Global Burden from WHO (1996) quoted in Lanjouw and Cockburn (2001 Table 1) Figuresupdated from Lanjouw and Cockburn (2001) using WHO (2001)
Pharmaceuticals and the Developing World 71
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
However many diseases affect both developed and developing countries Forinstance cancer and heart disease account for 15 percent of the total diseaseburden even in low- and middle-income countries (Lanjouw 2001) Moreover thedisease environment in developing countries is projected to become substantiallymore like that in developed countries over the next 20 years (WHO 2000)
Weak Health Care Systems and Misuse of PharmaceuticalsMisuse of pharmaceuticals is a signi cant problem in developed countries but
it is a much greater problem in many developing countries where health caresystems are often weak and quali ed medical personnel are scarce Whereas theUnited States has 27 trained physicians per thousand people and Europe has 39sub-Saharan Africa has only 01 physicians per thousand people (World Bank2001b) In some low-income countries medical personnel assigned to public clinicsoften do not show up particularly in rural areas Moreover clinics in developingcountries often lack drugs because salaries of health care workers take priority inbudget allocations and because drug procurement and distribution is inef cient orcorrupt2
Many patients therefore rely on the private health care system but privatepractitioners are often untrained (Das 2000) Medical personnel often prescribeinappropriate pharmaceuticals in part to demonstrate effort to the patient Forinstance in Africa injections are often given rather than pills as many patients seethese as more powerful In a detailed study of medication in India Phadke (1998)categorized more than 50 percent of all drugs prescribed as ldquounnecessaryrdquo orldquocontra-indicatedrdquo although some of these judgments are subjective
Moreover while self-prescription is not uncommon in the west it is extremelycommon in the poorest countries where rules requiring prescriptions for pharma-ceutical purchases are typically not enforced perhaps in part because of theshortage of trained physicians (Kamat and Nichter 1998) Many patients purchaseand consume only an incomplete course of medication especially when symptomssubside after a partial course (Nichter and Nichter 1996) Drug overuse and misusespeeds the development of drug-resistant forms of diseases because the mostresistant parasites are not eliminated and these resistant parasites are then trans-mitted to others For example chloroquine was once highly effective for preventingand treating malaria but strains of chloroquine-resistant malaria have emerged inmost parts of the world (NIH 2000) Strains of multidrug-resistant tuberculosishave also emerged over the last decade (NIH 2000) and the development ofresistance to the remaining tuberculosis drugs would pose a severe threat not onlyto developing countries but also to developed ones
Pharmaceutical RegulationDeveloping countries often simply follow the approval decisions of developed
countries rather than conducting their own risk-bene t calculations While this
2 See Di Tella and Schargrodsky (2001) on purchases by public hospitals in Argentina
72 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
practice may be appropriate in some cases it may also block the adoption ofneeded drugs and vaccines For example rotavirus kills three-quarters of a millionchildren each year in developing countries but it is a minor health nuisance in theUnited States causing more than three million cases of childhood diarrhea eachyear but few deaths (CVI 1999 Murphy et al 2001a) An oral rotavirus vaccinereceived regulatory approval in the United States and was introduced into the USmarket in 1998 A few months later it was withdrawn following evidence that it cancause intususception a form of intestinal obstruction Because children in devel-oping countries would have had much greater exposure to disease prior to inocu-lation it is not clear that the risk of intususception would be as signi cant indeveloping countries Moreover even if the risk of intususception were similar therisk-bene t calculation in countries with high rotavirus mortality would likelyoverwhelmingly favor vaccine use The investigators who recommended removingthe vaccine from the US market therefore advocated conducting a risk-bene tanalysis for the rotavirus vaccine in the developing world (Murphy et al 2001b)
Yet no such testing and analysis is taking place There is little hope for pro tfrom selling rotavirus vaccine in the poorest countries and neither the vaccinedeveloper nor health authorities in developing countries have much incentive totake on the risk of being attacked by activists for conducting trials of a vaccine thatis not deemed safe for use in more developed countries Top-level political lead-ership from the World Health Organization (WHO) or UNICEF potentially couldhave provided industry and national authorities with political cover against this riskperhaps making it feasible for the vaccine developer to give the rights to anonpro t organization that could conduct testing but this leadership was notforthcoming
While following drug approval decisions in the developed countries maysometimes prevent approval of useful drugs developing countries that depart fromthis practice can encounter other problems For instance the South Africangovernment has discouraged the widespread use of Nevirapine which preventsmother-to-child transmission of AIDS and is an extremely cost-effective interven-tion in part because President Mbeki gave credence to discredited scienti ctheories that HIV does not cause AIDS and that Nevirapine is toxic (The SouthAfrican government recently lost a lawsuit that may force the government to allowNevirapine to be distributed widely and as of this writing it appears that thegovernment has conceded and will eventually support the widespread use ofNevirapine) Kenya and South Africa also each backed several domestically devel-oped but ineffective AIDS drugs None of these quack remedies provided a cure forAIDS but they were promoted in part for nationalistic reasons
Industry FactorsSome of the characteristics of the pharmaceutical industry that differentiate it
from other industries are particularly relevant for developing countries First thepharmaceutical industry has high xed RampD costs and low marginal costs ofproduction Second the industry is exceptional in that patents rather than rst-
Michael Kremer 73
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
mover advantages or other sources of monopoly power provide the key protectionfor innovators Third pharmaceutical regulation and prescription requirements indeveloped countries facilitate price discrimination across countries by makingresale across national borders easier to block As a result price differentials be-tween countries are often large
The chief constraint on further price discrimination is the potential for apolitical backlash in higher-price markets Selling pharmaceuticals cheaply indeveloping countries reveals an upper bound on the marginal cost of productionand developed country politicians and activists may be able to use this informationto strengthen their appeals for lower prices For example when President Clintonannounced his childhood immunization initiative in 1993 he said ldquoI cannotbelieve that anyone seriously believes that America should manufacture vaccines forthe world sell them cheaper in foreign countries and immunize fewer kids as apercentage of the population than any nation in this hemisphere but Bolivia andHaitirdquo (Mitchell et al 1993) After a 1982 Congressional hearing in which USSenator Paula Hawkins asked a major vaccine manufacturer how it could justifycharging nearly three times as much to the US government for vaccines as toforeign countries US manufacturers stopped submitting bids to UNICEF tosupply vaccines (Mitchell et al 1993)
Limited Intellectual Property RightsMany developing countries have historically provided little or no intellectual
property rights protection for pharmaceuticals India for example offers patentson pharmaceutical processes but not on products and has developed a largeindustry that reverse engineers existing drugs Developed countries the UnitedStates in particular have pressed developing countries to strengthen protection ofintellectual property rights by linking the issue to trade negotiations The 1994Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) re-quired the least developed countries to join the rest of WTO member countries inproviding 20-year patent protection for pharmaceuticals by 2006 (WTO 2001a)
However it is unclear what impact TRIPS will ultimately have on intellectualproperty rights in developing countries Several provisions of the agreement pro-vide potential escape hatches For instance countries can impose compulsorylicensing in national emergencies the de nition of which is deliberately not set out(WTO 2001a) Countries are still free to impose price controls as well (though rms of course are not required to sell to countries with price controls) More-over the public storm over pricing of AIDS drugs led WTO negotiators to extendthe transition period for instituting patent protection for pharmaceuticals in theleast developed countries to 2016 (WTO 2001b) and it seems possible the dead-line could be extended further Finally enforcement of WTO provisions relies oncountries bringing suits but as a result of the public outcry the United Statesdropped its dispute with South Africa over the countryrsquos imports of pharmaceuticalproducts from countries with weaker patent laws and abandoned its dispute withBrazil over generic manufacturing of drugs that are still under patent It is not clear
74 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
whether the WTO will lead to effective intellectual property rights enforcement indeveloping countries
Market Failures Government Failures and Policy Implications
Clearly the pharmaceutical market in developing countries is rife with marketand government failures Pharmaceutical use is sometimes suboptimal due topricing above marginal cost and positive treatment externalities for infectiousdiseases sometimes too great due to the failure of consumers to take into accountexternalities from drug resistance and sometimes simply inappropriate due toinformation asymmetries between health care providers and their patients Drugprocurement is often inef cient and corrupt and inappropriate regulation canhinder access In addition health care workers are politically powerful relative topatients
However the most severe distortions in developing country pharmaceuticalmarkets probably involve dynamic issues Pharmaceutical rms are reluctant toinvest in RampD on the diseases that primarily affect developing countries not onlybecause the poverty of the potential users reduces their willingness to pay but alsobecause the potential revenue from product sales is far smaller than the sum ofcustomersrsquo potential willingness to pay due to the lack of intellectual propertyprotection and the tendency for governments to force prices down after rms havesunk their research and development costs The underprovision of RampD on prob-lems facing the poor even relative to their incomes implies that a redirection offoreign assistance from private goods such as food or even public goods such asroads to the international public good of RampD on health problems of the poorcould make the poor better-off
One reason why governments provide suboptimal RampD incentives is thatpharmaceutical research and development is a global public good so each countryhas an incentive to free ride on research nanced by the governments of othercountries or induced by their intellectual property rights protection This is ageneral problem faced by all countries not just developing ones Indeed themystery is not why developing countries have historically offered little protectionfor intellectual property rights but why small developed countries offer so muchA second reason for suboptimal RampD incentives is that the high xed costs of RampD andlow marginal costs of production for pharmaceuticals create a time-inconsistencyproblem for governments Once products have been developed governmentshave an incentive to set prices at or near marginal cost Products are then con-sumed at the ef cient level and surplus is transferred from (typically foreign)producers to consumers Governments are in a strong bargaining position becausethey are major pharmaceutical purchasers they regulate products and often pricesand they are arbiters of intellectual property rights However if pharmaceutical rms anticipate low prices they will be reluctant to invest In a repeated gamebetween nations and pharmaceutical producers this time-inconsistency problem
Pharmaceuticals and the Developing World 75
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
could potentially be overcome through reputation formation Indeed one reasonwhy developed countries are developed may be that these countries were able toestablish good reputational equilibria in a variety of areas including researchincentives Developed countries typically have more stable governments that aremore likely to invest in reputation formation for the long run
Whatever the underlying causes intellectual property rights for pharmaceuti-cals in developing countries are weak and hence the private returns for developingproducts to ght diseases of developing countries are likely to be a tiny fractionof the social returns to these products For example consider a hypotheticalfuture malaria vaccine A standard way to assess the cost-effectiveness of a healthintervention is the cost per Disability Adjusted Life Year saved A common cost-effectiveness threshold for health interventions in the poorest countries is $100 perDALY For comparison health interventions are considered cost-effective in theUnited States at up to 500 to 1000 times this amount $50000ndash$100000 per year oflife saved (Neumann et al 2000) At a threshold of $100 per DALY a malariavaccine would be cost-effective even at a price of $40 per immunized person(Glennerster and Kremer 2001) but based on the historical record of vaccineprices the developer of a malaria vaccine would be lucky to receive payments ofone-tenth or one-twentieth of that amount Of course a full comparison of thesocial and private values of a vaccine would also take into account the positive andnegative externalities that vaccine development would create for other researchers
The rest of this article considers a number of public policy issues regarding theavailability and use of pharmaceuticals in developing countries from the standpointof these market and government failures differential pricing foreign assistance forhealth misuse of pharmaceuticals drug regulation and procurement and ways ofencouraging RampD on products needed by developing countries
Differential PricingNoneconomists often resent price discrimination but it can improve both
access and RampD incentives Price discrimination allows those who value the productat more than the marginal cost of production to obtain it so the product reachesmore people than under a single worldwide monopoly price It also allows rms tocapture closer to the full social surplus of their products thus providing them witha greater incentive for product development
Since the chief constraint on further price discrimination is the fear ofundermining prices in developed and middle-income countries public acknowl-edgements by politicians in developed countries that different prices are appropri-ate for different countries could potentially make pharmaceutical rms morewilling to risk lowering prices in developing countries Rich country governmentscould also facilitate price discrimination by prohibiting imports of pharmaceuticalproducts from countries with weaker patent laws Individual rich countries can gainby taking advantage of lower-priced imports but the developed world as a whole isunlikely to bene t because if developed countries began importing drugs fromdeveloping countries on a wider scale pharmaceutical rms would simply charge
76 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
higher prices in developing countries and their incentives to conduct RampD wouldbe curbed by the smaller total market available to them with lower sales There istherefore a justi cation for international agreements to limit such imports sincethey create negative externalities for other countries Poor country governmentscan facilitate price discrimination by taking steps to prevent re-export of pharma-ceuticals to rich countries
However given that markets in the poorest countries are so small pro t-maximizing prices in poor countries are likely to be substantially above marginalcost if selling at a lower price in these countries has any appreciable effect on pricesin rich or even middle-income country markets Indeed prices in at least somemarkets will remain substantially above marginal cost even if governments adoptpolicies to encourage price discrimination further Hence many have called notjust for differential pricing in poor countries but also for using compulsorylicensing of patents andor the threat of compulsory licensing to lower pricescloser to marginal cost in poor countries One potential objection to compulsorylicensing is that it could reduce RampD incentives If restrictions on intellectualproperty rights were limited to the poorest countries the impact on researchincentives would be minimal for most diseases but for diseases that primarily affectpoor countries RampD incentives may be affected Indeed Lanjouw and Cockburn(2001) nd some evidence of a limited reallocation of funds toward malariaresearch with the introduction of intellectual property concerns into the GATT inthe 1990s and the consequent move toward strengthening intellectual propertyrights protection for pharmaceuticals in developing countries
Lanjouw (2001) proposes limiting the extension of patent protection in poorcountries for pharmaceuticals for global diseases while allowing patent protectionin these countries to increase as envisaged by the 1994 Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPs) on products for diseasesthat predominately affect the poor Under her proposal pharmaceutical develop-ers would effectively have to choose patent protection in either rich or poorcountries for a designated list of global diseases such as cancer Because developingcountries contribute little to the pro ts rms can realize from pharmaceuticals forglobal diseases patent applicants would choose protection in developed countriesDifferential patent protection would facilitate bene cial differential pricing If a rm sold a product for a global disease in a developing country at a high priceother rms could enter the market (This is essentially equivalent to allowingcompulsory licensing for global diseases)
Lanjouwrsquos (2001) proposal would be fairly close to returning to a pre-TRIPSpatent regime for global diseases but would preserve the limited existing incentivesto develop products primarily needed in developing countries such as a malariavaccine because it preserves intellectual property protections in those cases More-over the proposal is robust to errors in the list of global diseases For example ifall forms of cancer were designated as global diseases but a form of cancer speci cto Africa was later identi ed the developer of a drug against this form of cancercould choose patent protection in developing countries However since incentives
Michael Kremer 77
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
for RampD on diseases of developing countries are inadequate new ways of providingincentives for RampD on these products would still be needed
A potentially dif cult problem with limiting intellectual property rights in thepoorest countries is the political effects on prices in the middle- and high-incomecountries If sanctioning weak or no intellectual property rights in the poorestcountries weakened political support for intellectual property rights in richercountries or put pressure on prices there it could have a signi cant impact onresearch incentives for global diseases If India has limited intellectual propertyrights Brazil may not be inclined to provide intellectual property rights either andif antiretroviral drugs cost $500 per year in Brazil European governments maylower the prices they pay for the drugs and US AIDS activists may object to paying$10000 per year Moreover the existence of different intellectual property rightsrules in different countries may undermine attempts to cast intellectual propertyrights protection as a natural self-evident right rather than as an institutionjusti ed by its instrumental value Of course it is dif cult to predict the politicallinks between pricing in low- middle- and high-income countries but the fact thatpharmaceutical rms pressed for the TRIPS agreement suggests that they thinkthese links could be signi cant If this channel is indeed important weak intellec-tual property rights in poor countries could limit RampD incentives
It may therefore be worth considering an alternative approach in which rmssimply donate products to the poorest countries rather than charging the manu-facturing cost This could bolster rmsrsquo reputations rather than posing a publicrelations challenge in maintaining prices in developed countries In fact in the ght over pricing AIDS drugs antiretroviral producers sought to donate their AIDSdrugs in Africa but activists insisted on countries paying for the drugs at low pricesbelieving that rms would not continue the donations once the political heat wasoff
To give rms an incentive to continue donating their products developedcountry governments could provide enhanced tax deductions to pharmaceutical rms that make approved donations of drugs or vaccines for use in developingcountries The US government currently provides a tax deduction for donationsbut it is based on the productrsquos manufacturing cost which is often very low Anenhanced tax deduction or credit could be based on some fraction of a productrsquosUS price or on an estimate of the social bene t of the product perhaps measuredin dollars per Disability Adjusted Life Years saved Such a provision would have tobe limited to appropriate donations requested by approved organizations andshown to be reaching those who need them or else rms could pro t by donatingunneeded products with low production costs This approach would provide thebene ts of price discrimination without jeopardizing either research incentives orthe principle of intellectual property rights
Priorities for Foreign Assistance in HealthThe World Health Organizationrsquos Commission on Macroeconomics and
Health (CMH) chaired by economist Jeffrey Sachs has called for developed
78 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
countries to increase assistance for health in the developing world by $27 billionannually by 2007 and $38 billion annually by 2015 (CMH 2001) A signi cant shareof this would be for pharmaceuticals including antiretroviral treatments for AIDS
The Commission report argues that these investments in health will pay forthemselves six times over through higher productivity and increased earnings(CMH 2001) However evidence on the magnitude of the economic impact ofhealth gains is patchy Extravagant claims based on cross-country regressionsshould be taken with a grain of salt in light of the poor economic performance ofAfrica from the 1960s through the 1990s despite the substantial technology-drivenimprovements in health over the period and by the more recent stellar growthperformance of Uganda one of the countries earliest and hardest hit by AIDSmorbidity and mortality In my view a stronger case for health spending rests on itseffect on welfare rather than measured GDP Indeed the 13 percent decline inof cial GDP in the low-income countries of sub-Saharan Africa from 1972 to 1992while life expectancy increased by nearly 10 percent and infant mortality fell30 percent suggests that measured GDP can in some cases be a poor guide towelfare A version of GDP that was corrected to measure improvements in theproductivity of health services over this period would probably not have declinedover the period
Economists have advocated two main approaches for determining prioritiesfor the limited foreign assistance that is likely to be forthcoming for health from thedeveloped world Some argue that the interventions that save the greatest numberof lives at the least cost should be prioritized using cost per Disability Adjusted LifeYears saved as a guideline Others argue that outside assistance should concentrateon addressing market failures for example by funding public goods However thedebate between advocates of the cost-effectiveness and market failure approachesmay be overblown To the extent that analysts estimate DALYs correctly andconsumers value DALYs incurred by different diseases equally (rather than beingwilling to pay more to avoid deaths from airplane crashes than automobile acci-dents for example) the two approaches should yield broadly similar resultsIndeed they do point to similar health priorities For example the WHO Ex-panded Program on Immunization is extremely cost-effective at only around $20 to$40 per DALY saved in part because vaccination creates positive externalities bypreventing the spread of disease Treatments for some infectious diseases wouldlikely be another priority under both approaches For example school-based masstreatment of intestinal worm infections would cost as little as $7 per DALY savedand the externality bene ts of such treatments can account for over 70 percent ofthe reduction in disease burden (Miguel and Kremer 2002) Some AIDS interven-tions are also very cost-effective Nevirapine is extremely cost-effective in preventingmother-to-child transmission of AIDS at $5 to $20 per DALY saved (Marseille et al1999) and a targeted AIDS prevention program in Tanzania costs an estimated $10to $12 per DALY saved (World Bank 1999)
Given a xed budget helping extend the programs above to reach morepeople is likely to be a much higher priority than using antiretroviral drugs to treat
Pharmaceuticals and the Developing World 79
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
HIVAIDS The well-known call by 133 Harvard faculty members for antiretroviraltreatment in developing countries estimates that even given the recent dramaticreductions in prices by pharmaceutical rms purchasing and delivering antiretro-virals will cost $1100 per person per year (Adams et al 2001) This is in large partbecause the drugs are so dif cult to deliver safely and effectively Because the drugscause signi cant side effects and must be taken according to a rigid schedule if theyare to be effective and not lead to the spread of drug resistance they requiremonitoring by medical personnel Adherence to drug regimes is highly imperfecteven in rich countries with good medical care (Ammassari et al 2001 Brook et al2001 Nieuwkerk et al 2001) The statement by the 133 Harvard faculty memberstherefore advocates ldquodirectly observed therapyrdquo wherein a community healthworker visits each patient and observes him or her taking the antiretroviral medi-cation It is worth noting however that recent randomized controlled trials ndthat direct observation is no more effective than self-administered treatment fortuberculosis (Walley et al 2001) But even setting this issue aside many more livescould be saved with alternative interventions given the $1100 per patient per yearestimated cost of antiretroviral therapy For instance for every person treated for ayear with antiretroviral therapy 25 to 110 Disability Adjusted Life Years could besaved through targeted AIDS prevention efforts or vaccination against easily pre-ventable diseases
Advocates of antiretroviral drugs for HIVAIDS often argue that treatmentencourages prevention and slows transmission since people do not have incentivesto be tested unless treatment is available However the impact of antiretrovirals onthe spread of the AIDS epidemic is unclear Even if the availability of treatmentencourages testing knowledge of HIV status may not prevent the spread of thedisease since people who are infected may decide they have nothing left to loseMoreover while treatment with antiretroviral therapy may lower viral loads andreduce transmission it may also help HIV-infected people stay sexually activelonger contributing to the spread of the disease Finally the expectation oftreatment could reduce incentives to adopt safer behaviors While there is no cleartheoretical presumption about the effect of subsidizing antiretroviral therapies onthe rate of transmission of HIV in low-income countries there is at least someempirical evidence that the availability of treatment has led to a resurgence of riskybehavior in the United States (Lehman et al 2000) There is also anecdotalevidence that risky sexual behavior increased in Kenya following fraudulent an-nouncements of an AIDS cure (McGreal 1996)
Some advocates of antiretroviral treatment argue that public campaigns toextend antiretroviral treatment will generate enough new aid that both antiretro-virals and other interventions can be funded It is worth bearing in mind howeverthat even if 90 percent of funds for antiretroviral therapy were ldquonewrdquo foreign aidand only 10 percent were diverted from vaccination efforts more lives would be lostfrom reductions in vaccinations than would be gained through antiretroviraltherapy Calls for foreign assistance to provide antiretroviral therapy might thus
80 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
stipulate that any available funds should be used in the way that saves the most livesso that if only a small amount was provided it would be used to cover low-costinterventions such as vaccinations but that if a larger amount was made availableit could be used to cover antiretroviral therapy
Since individual countries can potentially correct market failures within theirborders it may make sense to focus foreign assistance on the provision of globalpublic goods Key global public goods include slowing the development of drugresistance creating knowledge on drug ef cacy and safety and most importantRampD on new pharmaceuticals Since the spread of a disease once it crosses nationalborders is determined primarily by conditions within the host nation cross-borderexternalities from improved disease control are likely to be small with the excep-tion of diseases near eradication such as smallpox in the 1970s and polio now
Addressing Misuse of PharmaceuticalsSince misuse of pharmaceuticals that facilitates the development of drug
resistance creates negative externalities for the rest of the world discouraging drugmisuse is a global public good However the impact of pharmaceutical prices onexternalities from drug resistance is ambiguous Higher prices could reduce thenumber of people taking drugs and thus reduce the spread of drug resistance buthigher prices could also lead those people who do take the drug to take incompletedoses promoting the spread of drug resistance The latter effect may be particularlylikely in developing countries where pharmaceuticals are often taken with weakmedical supervision Conceivably governments could require medicines to bepackaged for sale only in complete courses and could penalize stores sellingfractions of a course However shopkeepers in developing countries routinely sellindividual units from packages and monitoring this would be dif cult Anotherpossibility would be to subsidize combination therapies that are less likely to inducedrug resistance3
Improving the overall quality of medical care would also reduce the spread ofdrug resistance by helping to ensure that pharmaceuticals are used appropriatelyand that patients are encouraged to complete the course of treatment Brandingand franchising of medical practices and care facilities could potentially helpaddress the problems of asymmetric information between patients and providersMission hospitals in Africa have managed to develop reputations for providingquality care for example (Leonard 2002) Managing such branding efforts couldbe dif cult however and the effectiveness of such efforts is uncertain In somecountries the Internet might potentially play a role in facilitating the standardiza-tion of medical care Clinic workers with only moderate levels of training couldenter patient information and programs on the Internet could offer possible
3 For example Mead Over has suggested that subsidizing combination therapies for AIDS might reducethe risk of drug resistance developing since while this practice would encourage greater use of multidrugtherapy it might discourage the use of monotherapies that are more prone to drug resistance
Michael Kremer 81
diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives

diagnoses for them to consider as well as advice on when referrals are needed Sucha system could complement the services currently provided by health care workersand help to monitor whether local health care workers were showing up to work orwere likely to be routinely mistreating patients Efforts to experiment with suchapproaches deserve international support since they could potentially lead toinnovations in health care delivery that would be bene cial across much of thedeveloping world
RampD on Needed ProductsAs discussed earlier current incentives for the development of products
needed primarily by developing countries are inadequate Vaccines for malariatuberculosis and the strains of AIDS prevalent in Africa are a prime examplePrograms to encourage RampD can take two broad forms ldquoPushrdquo programs subsidizeresearch inputsmdashfor example through grants to researchers or RampD tax creditsldquoPullrdquo programs reward research outputs for example by committing in advance topurchase a speci ed amount of a desired product at a speci ed price Bothapproaches have important roles but current policy underutilizes pull programs
Push programs are subject to asymmetric information between researchers andprogram administrators and between these groups and politicians and the publicgiving rise to both moral hazard and adverse selection Moral hazard arises becausefunders cannot perfectly monitor the actions of grant recipients and grant recip-ients may have incentives to devote effort to pursuing general scienti c research orpreparing their next grant application rather than focusing on development of thedesired product In contrast under a pull program researchers will not receivepayment unless a useable product is delivered so researchers have incentives tofocus on developing the desired product
Adverse selection arises because researchers have more information than dofunders about the probability that their research will lead to successful productsResearch administrators and their ultimate employersmdash elected of cials and thegeneral publicmdashmay not be able to determine which research projects in responseto certain diseases are worth pursuing nor which diseases and products should betargeted Decision makers may therefore wind up nancing ideas with only aminute probability of success or worse failing to fund promising research becausethey do not have con dence that its backers are presenting objective informationon its prospects In contrast under a pull program in which developers arerewarded only if they successfully produce the desired product there is a strongincentive for rms considering research investments to assess the prospects forsuccess realistically
The moral hazard and adverse selection problems that plague push programsare illustrated by the US Agency for International Developmentrsquos (USAID) 1980sprogram to develop a malaria vaccine During the USAID program externalevaluators suggested that additional funding should not be provided to two of thethree research teams However as a result of information provided by the projectdirector USAID provided substantial new resources to all three teams and was
82 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
suf ciently con dent that vaccines would be developed that it even arranged topurchase monkeys for testing a vaccine Two of three researchers diverted grantfunds into their private accounts and were later indicted for theft and criminalconspiracy The project director received kickbacks from the contract to purchasemonkeys and eventually pleaded guilty to accepting an illegal gratuity ling falsetax returns and making false statements In 1984 before the indictments theagency claimed that there had been a ldquomajor breakthrough in the development of avaccine against the most deadly form of malaria in human beings The vac-cine should be ready for use around the world especially in developing countrieswithin ve yearsrdquo (Desowitz 1991) By the end of the project USAID had spent$60 million on its malaria vaccine effort with few results While the example isextreme it vividly illustrates the problems with push programs
As an alternative to direct government nancing of research some haveproposed RampD tax credits targeted to private research on drugs and vaccinesneeded by developing countries However such tax credits are subject to similarproblems Firms would have an incentive to relabel as much of their RampD aspossible as eligible for the targeted credit For example if there were an RampD taxcredit for a malaria vaccine researchers might focus on a vaccine that would likelyonly provide temporary protection and would be suitable for travelers and militarypersonnel spending only short times in developing countries but not for residentsof these areas To take another example modern vaccines typically include bothantigens speci c to a particular organism and adjuvants that potentially boost theeffectiveness of several different vaccines Firms would have every incentive to claimthat an adjuvant intended for an ineligible vaccine was actually for a malariavaccine so as to claim a tax credit Finally RampD tax credits will not improve accessto products once they are developed
In contrast under pull programs the public pays nothing unless a viableproduct is developed Pull programs give researchers incentives to self-selectprojects with a reasonable chance of yielding a viable product and to focus ondeveloping a marketable product Under pull programs governments do not needto ldquopick winnersrdquo among RampD proposalsmdashthey simply need to decide what successwould be worth to society and offer a corresponding reward Moreover appropri-ately designed pull programs can help ensure that if new products are developedthey will reach those who need them One kind of pull program is a purchasecommitment in which sponsors would commit to purchase a speci ed number ofdoses at a speci ed price if a vaccine meeting certain speci cations were developedPurchase commitment programs are discussed in Kremer (2001a b) World Bank(1999) and Batson and Ainsworth (2001) while shorter treatments of the idea inthe popular press appear in Kremer and Sachs (1999) and Sachs (1999)4 Anexample of a purchase commitment would be for developed countries or private
4 An alternative push program design that has been proposed is to reward developers with extensions ofpatents on other pharmaceuticals This would inef ciently and inequitably place the entire burden of nancing development on patients who need these other pharmaceuticals For example giving a patent
Pharmaceuticals and the Developing World 83
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
foundations to commit to purchase malaria vaccine at $5 per immunized personand to make it available to developing countries either free or for a modestcopayment
A key limitation of pull programs is that they require specifying the output inadvance A pull program could not have been used to encourage the developmentof the Post-It Notereg or the graphical user interface because these products couldnot have been adequately described before they were invented Similarly pullprograms may not work well to encourage basic research because it is typicallydif cult to specify the desired results of basic research in advance (Of course somebasic research outputs such as proving Fermatrsquos last theorem can be de ned inadvance) Simply rewarding the development of applied products is not a good wayto stimulate basic research since a program that tied rewards to the developmentof a speci c product would encourage researchers to keep their results private aslong as possible to have an advantage in the next stage of research Indeed a keyobjective of basic research is to provide information to other researchers ratherthan to develop products and grant-funded academics and scientists in govern-ment laboratories have career incentives to publish their results quickly In contrastto unanticipated inventions like the Post-It Notereg or to basic research it iscomparatively easier to de ne what is meant by a safe and ef cacious vaccineespecially as existing institutions such as the US Food and Drug Administration(FDA) are already charged with making these determinations
Nonetheless if donor governments international organizations or privatefoundations commit to purchase a future vaccine the eligibility rules they set willbe key Eligibility conditions for candidate products would likely include someminimal technical requirements These technical requirements could includeclearance by a regulatory agency such as the US FDA or a waiver of regulatoryapproval in developed countries for products that would pass a risk-bene t analysisfor use in developing but not developed countries Products that pass theserequirements might then be subject to a market test nations wishing to purchaseproducts might be required to provide a modest copayment tied to their per capitaincome so that countries would have an incentive to investigate carefully whethercandidate products are appropriate for their local conditions This provision wouldalso help to assure that limited donor funds are allocated well and would increaseincentives for developers by increasing the payment offered to the successfuldeveloper On the other hand it could reduce the con dence of potential vaccinedevelopers in the program A purchase commitment could also include a system ofbonus payments for products that exceed the minimum requirements Eligibilityconditions should also specify who will have authority to judge whether the eligi-
extension on Prozac for developing an HIV vaccine could prevent some people from getting neededtreatment for depression
84 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
bility conditions have been ful lled Ideally these adjudicators should be insulatedfrom political pressure through long terms of service
A well-written contract should also be credible to potential vaccine developersCourts have held that similar public commitments to reward contest winners or topurchase speci ed goods constitute legally binding contracts and that the decisionsof independent parties appointed in advance to adjudicate such programs arebinding For example in the 1960s the US government pledged to purchase ata minimum price domestically produced manganese After the world price of thecommodity fell the General Services Administration (GSA) the US agency incharge of administering the program attempted to renege but US courts forcedthe GSA to honor the commitment (Morantz and Sloane 2001)
The total market promised by a purchase commitment should be large enoughto induce substantial effort by vaccine developers but less than the social value ofthe vaccine The larger the market for a product the more rms will enter the eldthe more research leads each rm will pursue and the faster a product will bedeveloped Given the enormous burden of diseases such as malaria tuberculosisand HIVAIDS it is important to provide suf cient incentive for many researchersto enter the eld and to induce major pharmaceutical rms to pursue severalpotential leads simultaneously so that products can be developed quickly There islittle risk that payments made as a result of a purchase commitment could exceedthe cost of saving the equivalent number of lives using todayrsquos treatments
Prior work by the author and others suggests that an annual market of$250 million to $500 million is needed to motivate substantial research (Kettler1999 Kremer 2001b Mercer Management Consulting 1998) A commitment atthis level to purchase vaccines for malaria tuberculosis and HIVAIDS would beextremely cost effective costing nothing if a useable product was not developedand as little as $4 per year of life saved if a vaccine were developed
Purchase commitments could potentially be implemented by national govern-ments international organizations or private foundations A number of policymak-ers have indicated interest in this approach As US Treasury Secretary LawrenceSummers advocated a closely related tax credit for sales of vaccines where everydollar of qualifying vaccine sales to nonpro t and international organizationsserving developing countries would be matched by a dollar of tax credit effectivelydoubling the incentive to develop vaccines for neglected diseases This proposalwas part of the Clinton administrationrsquos FY 2001 budget but did not become lawSenators William Frist (R-TN) and John Kerry (D-MA) and Representatives NancyPelosi (D-CA) and Jennifer Dunn (R-WA) have proposed both the tax measure anda purchase commitment in the Vaccines for the New Millennium Act
The purchase commitment approach has also attracted interest from policy-makers internationally including the United Kingdomrsquos Chancellor of the Exche-quer the United Kingdom Cabinet Of ce the German foreign minister and theDutch development minister (Brown 2001 Elliott and Atkinson 2001 PIU 2001)The World Bank president James Wolfensohn has said that the institution plans to
Michael Kremer 85
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
create a $1 billion fund to help countries purchase speci ed vaccines if and whenthey are developed (ldquoDiscovering Medicines for the Poorrdquo 2000) However theWorld Bank has yet to act on this commitment The Gates Foundation with$22 billion in assets and a focus on childrenrsquos health in developing countries andvaccines in particular is also well-placed to forward a vaccine purchase commit-ment While continuing to fund its other priorities such a foundation could simplypledge that if a product were actually developed the foundation would purchaseand distribute it in developing countries
Drug Regulation and ProcurementThe case of rotavirus vaccine suggests that if developing countries simply rely
on regulatory institutions in developed countries decisions will not always beappropriate given the different bene t-cost ratios for particular pharmaceuticals indeveloping countries On the other hand the Kenyan and South African govern-mentsrsquo endorsement of ineffective but domestically developed AIDS ldquocuresrdquo sug-gests that if individual developing countries without adequate domestic institutionsmake regulatory decisions decisions may re ect politics and nationalism as muchas health concerns Since gathering information on drug safety and ef cacy is aninternational public good there may be a role for an international body to reviewdeveloped country pharmaceutical approval decisions for relevance to developingcountry conditions and where appropriate to sponsor additional trials or issuealternative certi cation The organization could make a recommendation on theappropriateness of the product for use in different circumstances and each coun-try could then decide whether to follow that recommendation However the WorldHealth Organization has historically eschewed such a role and it is not clear thatit is equipped to act as a regulatory body Like many other international organiza-tions the quality of WHOrsquos work sometimes suffers as member countries investresources in seeking funding contracts or leadership positions rather than intrying to improve the organization as a whole5
Milton Friedman (Friedman and Friedman 1980) has suggested replacingpharmaceutical regulation and prescription requirements with a system of manda-tory labeling and letting consumers make their own decisions on pharmaceuticaluse While proponents of strict drug regulation point to disasters of prematureapproval such as thalidomide opponents argue that the health burden of regula-tory delays in approving new drugs far exceeds the health costs of these well-publicized disasters It seems possible for example that the failure to proceed withthe rotavirus vaccine in developing countries will cost millions of lives
In my view the justi cation for pharmaceutical regulation needs to be recon-ceptualized Were the declared purpose of pharmaceutical regulationmdashto protectcurrent consumers from unsafe and ineffective drugsmdashthe main reason for regu-
5 For instance in 1993 Hiroshi Nakajima was re-elected to head WHO amid allegations that Japanbribed developing nations to vote for the Japanese Director General (Crossette 1998)
86 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
lation Friedmanrsquos (Friedman and Friedman 1980) proposal would be appealingI would argue however that the primary advantage of drug regulation is that itcreates incentives for rms to conduct the randomized trials that provide informa-tion on product effectiveness for future consumers The current regulatory systemin which products that have not undergone clinical trials cannot be sold legallygives pharmaceutical rms an incentive to conduct these trials and to do so in arigorous enough manner to pass muster with regulators If new pharmaceuticalswere available during trials it may be dif cult to preserve the integrity of thecomparison group necessary for conducting randomized trials Seen in this lightdrug regulation denies current consumers the option of taking unproven drugsbut it provides future consumers with information about the drugs
Since incentives from large rich country markets are suf cient to encouragetesting small poor countries may want to consider requiring labels that tell cus-tomers whether the product received regulatory approval but not prohibiting salesof products for which approval had not been granted On the other hand thetraditional justi cation for drug regulation may better apply in environments whereconsumers are often illiterate deceptive advertising is dif cult to regulate and tortlaw is weak In such environments replacing prohibition with labeling couldpotentially exacerbate misuse of pharmaceuticals The best case for replacing drugregulation with labeling requirements could therefore be made in small developedcountries such as Australia or New Zealand
Some have proposed posting information on all public pharmaceutical pur-chases on the Internet as a way to improve pharmaceutical procurement by devel-oping country governments and such a system has been tried in Brazil This systemhas been advocated as a way to provide information to ill-informed public purchas-ers and strengthen their bargaining power but posting prices could also facilitatecollusion among suppliers to keep prices high A better rationale for the system isthat publicly posting prices could help reduce corruption in drug procurementwhich is likely a bigger problem than collusion by sellers
Conclusions
Pharmaceuticals have brought tremendous health improvements to develop-ing countries The international community could greatly increase these bene ts byimplementing systems to provide better access to existing pharmaceuticals and tomanage their use as well as by investing in the global public good of RampD ondiseases that disproportionately affect the poor Developing countries could redi-rect their health budgets away from salaries and toward cost-effective public healthmeasures such as vaccination and school-based control of intestinal worms andcould explore institutional reforms for health care delivery Developed countriesand international organizations could encourage differential pricing allow morefavorable tax treatment of appropriate drug donations and encourage RampD and
Pharmaceuticals and the Developing World 87
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
facilitate access to new products by committing in advance to purchase productsneeded in developing countries if and when they are developed
y I am grateful to Jessica Leino for outstanding research assistance and to Ernst BerndtJishnu Das Brad De Long Varun Gauri Dean Jamison Lynn Johnson Jenny LanjouwMead Over Timothy Taylor Michael Waldman and David Webber for suggestions
References
Adams Gregor et al 2001 ldquoConsensus State-ment on Antiretroviral Treatment for AIDSin Poor Countriesrdquo Available at httpwwwhsphharvardeduorganizationshaioverviewnews_eventseventsconsensushtml
Ammassari Adriana et al 2001 ldquoSelf-Reported Symptoms and Medication Side Ef-fects In uence Adherence to Highly Active An-tiretroviral Therapy in Persons with HIVInfectionrdquo Journal of Acquired Immune DeciencySyndromes December 15 285 pp 445ndash49
Attaran Amir and Lee Gillespie-White 2001ldquoDo Patents for Antiretroviral Drugs ConstrainAccess to AIDS Treatment in Africardquo Journal ofthe American Medical Association October 17 28615 pp 1886ndash892
Balke Nathan S and Robert J Gordon 1989ldquoThe Estimation of Prewar Gross National Prod-uct Methodology and New Evidencerdquo Journal ofPolitical Economy February 97 pp 38ndash92
Batson Amie and Martha Ainsworth 2001ldquoPrivate Investment in AIDS Vaccine Develop-ment Obstacles and Solutionsrdquo Bulletin of theWorld Health Organization 798 pp 721ndash27
Brook MG et al 2001 ldquoAdherence to HighlyActive Antiretroviral Therapy in the Real WorldExperience of Twelve English HIV Unitsrdquo AIDSPatient Care STDS September 159 pp 491ndash94
Brown Gordon 2001 Speech given by GordonBrown Chancellor of the Exchequer at the In-ternational Conference Against Child PovertyLondon February 26 Available at httpwwwhm-treasurygovukdocs2001child_povesrtychxspeechhtm
CMH (Commission on Macroeconomics andHealth) 2001 ldquoMacroeconomics and HealthInvesting for Healthrdquo Available at httpwwwcidharvardeducidcmhCMHReportpdf
Costa Dora 2001 ldquoEstimating Real Incomein the United States from 1988 to 1994 Correct-ing CPI Bias Using Engel Curvesrdquo Journal ofPolitical Economy December 1096 pp 1288ndash310
Crossette Barbara 1998 ldquoAt WHO 2 Phy-sicians Lead the Race for Top Jobrdquo New YorkTimes January 11 Section 1 p 4
CVI (Childrenrsquos Vaccine Initiative) 1999 CVIForum No 16 Geneva
Das Jishnu 2000 ldquoDo Patients Learn AboutDoctor Quality Theory and an Application toIndialdquo Manuscript Harvard
Desowitz Robert S 1991 The Malaria CapersTales of Parasites and People New York W WNorton
Di Tella Rafael and Ernesto Schargrodsky2001 ldquoThe Role of Wages and Auditing during aCrackdown on Corruption in the City of BuenosAiresrdquo Manuscript Harvard
Elliott Larry and Mark Atkinson 2001 ldquoFundto Beat Third World Diseaserdquo Guardian Febru-ary 23 Available at httpwwwguardiancoukinternationalstory0360444183500html
ldquoDiscovering Medicines for the Poorrdquo 2000Financial Times February 2 p 7
Fogel Robert W 1986 ldquoNutrition and theDecline in Mortality Since 1700 Some Prelimi-nary Findingsrdquo in Long-Term Factors in AmericanEconomic Growth Stanley L Engerman and Rob-ert E Gallman eds Chicago University of Chi-cago Press pp 439ndash527
Friedman Milton and Rose Friedman 1980Free to Choose New York Harcourt Brace Jovan-ovich
Glennerster Rachel and Michael Kremer2001 ldquoA Vaccine Purchase Commitment Cost-Effectiveness Estimates and Pricing GuidelinesrdquoUnpublished Manuscript
88 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives
Jamison Dean T et al 2001 ldquoCross-CountryVariation in Mortality Decline 1962ndash87 TheRole of Country-Speci c Technical ProgressrdquoCMH Working Paper No WG14 April
Johnston Louis and Samuel H Williamson2002 ldquoThe Annual Real and Nominal GDP forthe United States 1789ndashPresentrdquo EconomicHistory Services April available at httpwwwehnethmitgdp
Kamat Vinay R and Mark Nichter 1998ldquoPharmacies Self-Medication and Pharmaceuti-cal Marketing in Bombay Indiardquo Social Scienceand Medicine 476 pp 779ndash94
Kettler Hannah E 1999 ldquoUpdating the Costof a New Chemical Entityrdquo London Of ce ofHealth Economics
Kim-Farley R and the Expanded Programmeon Immunization Team 1992 ldquoGlobal Immuni-zationrdquo Annual Review of Public Health 13 pp223ndash37
Kremer Michael 2001a ldquoCreating Marketsfor New Vaccines Part I Rationalerdquo in Innova-tion Policy and the Economy Adam B Jaffe JoshLerner and Scott Stern eds Cambride MITPress pp 35ndash72
Kremer Michael 2001b ldquoCreating Marketsfor New Vaccines Part II Design Issuesrdquo in In-novation Policy and the Economy Adam B JaffeJosh Lerner and Scott Stern eds CambrideMIT Press pp 73ndash118
Kremer Michael and Jeffrey Sachs 1999 ldquoACure for Indifferencerdquo Financial Times May 5available at httpwwwbrookeduviewsopedkremer19990505htm
Kurian George Thomas 1994 Datapedia of theUnited States 1790ndash2000 Lanham Md BernanPress
Lanjouw Jean O 2001 ldquoA Patent Policy Pro-posal for Global Diseasesrdquo Brookings PolicyBrief June
Lanjouw Jean O and Iain M Cockburn 2001ldquoNew Pills for Poor People Empirical Evidenceafter GATTrdquo World Development 292 pp 265ndash89
Lehman Stan et al 2000 ldquoAre At-Risk Popu-lations Less Concerned about HIV Infection inthe HAART Erardquo San Francisco CDC SeventhConference on Retroviruses and OpportunisticInfections January 30 ndashFebruary 2
Leonard Kenneth L 2002 ldquoWhen Both Statesand Markets Fail Asymmetric Information andthe Role of NGOs in African Health Carerdquo In-ternational Review of Law and Economics July 221pp 61ndash81
Marseille E et al 1999 ldquoCost-Effectiveness ofSingle-Dose Nevirapine Regimen for Mothersand Babies to Decrease Vertical HIV-1 Transmis-
sion in Sub-Saharan Africardquo Lancet September4 3549181 pp 803ndash09
McGreal Chris 1996 ldquoHorror Greets AIDSlsquoMiracle Curersquordquo Guardian May 25 p 11
Mercer Management Consulting 1998 ldquoHIVVaccine Industry Study October-December1998rdquo World Bank Task Force on Acceleratingthe Development of an HIVAIDS Vaccine forDeveloping Countries
Miguel Edward and Michael Kremer 2002ldquoWorms Education and Health Externalities inKenyardquo Manuscript Harvard
Mitchell Violaine S et al 1993 The ChildrenrsquosVaccine Initiative Achieving the Vision Washing-ton DC National Academy Press
Morantz Alison and Robert Sloane 2001ldquoVaccine Purchase Commitment Contract LegalStrategies for Ensuring Enforceabilityrdquo MimeoHarvard University
Murphy Trudy V et al 2001a ldquoIntussuscep-tion Among Infants Given an Oral RotavirusVaccinerdquo New England Journal of Medicine Febru-ary 22 3448 pp 564ndash72
Murphy Trudy V et al 2001b ldquoIntussuscep-tion and an Oral Rotavirus Vaccinerdquo New En-gland Journal of Medicine June 14 34424 pp1866ndash867
Murray Christopher J L and Alan D Lopez1996 The Global Burden of Disease a ComprehensiveAssessment of Mortality and Disability from DiseasesInjuries and Risk Factors in 1990 and Projected to2020 Global Burden of Disease and Injury SeriesVolume 1 Cambridge Mass Published by theHarvard School of Public Health on behalf ofthe World Health Organization and the WorldBank Distributed by Harvard University Press
Neumann Peter J et al 2000 ldquoAre Pharma-ceuticals Cost-Effective A Review of the Evi-dencerdquo Health Affairs MarchApril 192 pp92ndash109
Nichter Mark and Mimi Nichter 1996 Anthro-pology and International Health Asian Case StudiesAmsterdam Gordon and Breach
Nieuwkerk PT et al 2001 ldquoLimited PatientAdherence to Highly Active Antiretroviral Ther-apy for HIV-1 Infection in an Observational Co-hort Studyrdquo Archives of Internal Medicine Septem-ber 10 16116 pp 1962ndash968
NIH (National Institutes of Health) 2000 ldquoFactSheet Antimicrobial Resistancerdquo Available athttp wwwniaidnihgovfactsheetsantimicro
htm JunePecoul Bernard et al 1999 ldquoAccess to Essen-
tial Drugs in Poor Countries A Lost BattlerdquoJournal of the American Medical Association January27 2814 pp 361ndash67
Phadke Anant 1998 Drug Supply and Use To-
Michael Kremer 89
wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives

wards a Rational Policy in India New Delhi SagePublications
PhRMA 2000 PhRMA Industry Prole 2000Available at httpwwwphrmaorgpublica-tionspublicationspro le00
PIU (Performance and Innovation Unit Cab-inet Of ce) 2001 ldquoTackling the Diseases of Pov-erty Meeting the OkinawaMillenium Targetsfor HIVAIDS Tuberculosis and MalariardquoLondon May 8 Available at httpwwwcabinet-of cegovukinnovationhealthreportdefaulthtm
Preston Samuel H 1975 ldquoThe Changing Re-lation between Mortality and Level of EconomicDevelopmentrdquo Population Studies July 292 pp231ndash48
Sachs Jeffrey 1999 ldquoHelping the WorldrsquosPoorestrdquo Economist August 14 3528132 pp 17ndash20
United States Census2000 Available at httpwwwcensusgovdmdwww2khomehtm
Walley John D et al 2001 ldquoEffectiveness ofthe Direct Observation Component of DOTS for
Tuberculosis A Randomised Controlled Trial inPakistanrdquo Lancet March 3 357 pp 664ndash69
WHO (World Health Organization) 1996 In-vesting in Health Research and Development Reportof the Ad Hoc Committee on Health Research Relatingto Future Intervention Options Geneva WHO
WHO (World Health Organization) 2000World Heath Report 2000 Geneva WHO
WHO (World Health Organization) 2001World Heath Report 2001 Geneva WHO
World Bank 1999 Confronting AIDS Public Pri-orities in a Global Epidemic Washington DCOxford University Press
World Bank 2001a Immunization at a GlanceWashington DC World Bank November
World Bank 2001b World Development Indica-tors Washington DC Oxford University Press
WTO 2001a ldquoFact Sheet TRIPS and Pharma-ceutical Patentsrdquo April
WTO 2001b ldquoDeclaration on the TRIPSAgreement and Public Healthrdquo Available at httpwww-chilwto-ministerialorgenglishthewto_eminist_emin01_emin01_14nov_ehtm
90 Journal of Economic Perspectives





























