Embed Size (px)
Citation preview
Pharmaceutical benefit management under health insurance – common issues in emerging economiesPharmaceutical benefit management under health
insurance – common issues in emerging economies
Zagreb, January 19, 2010
Andreas Seiter
World Bank
Navigating between two extremes
Political death if drug coverage becomes too
skimpy
Bankruptcy if drug coverage is
too generous
Sustainable path
Common Features
Insurance funds cover majority or all of population Insurance “drug benefit” = coverage for drugs is major enabling
factor for drug market Coverage based on positive list (formulary) Two challenges for suppliers:
• Getting on the list
• Once on the list, sell as much as possible
Two intervention points for insurance funds to control costs• Decide what is covered, at which price, under which conditions
• Control/manage consumption
Sleeping giants?
Bureaucratic tradition, but have to endure increasingly tough negotiations with stakeholders
Politicized governance: mixed signals are common due to high sensitivity of coverage decisions
Status and credibility gap to providers (doctors) Technical challenges: many drugs and formulations, difficulty to get
reliable data on clinical benefit and pricing Millions of transactions to be monitored
What happened in “Old Europe”?
Insurance funds were ahead of the curve – total coverage in the 60s and 70s was affordable (young population, rapid growth)
Systems, tools and skills could emerge over time Financial room to maneuver is significantly greater Significant power shift to insurance funds over time
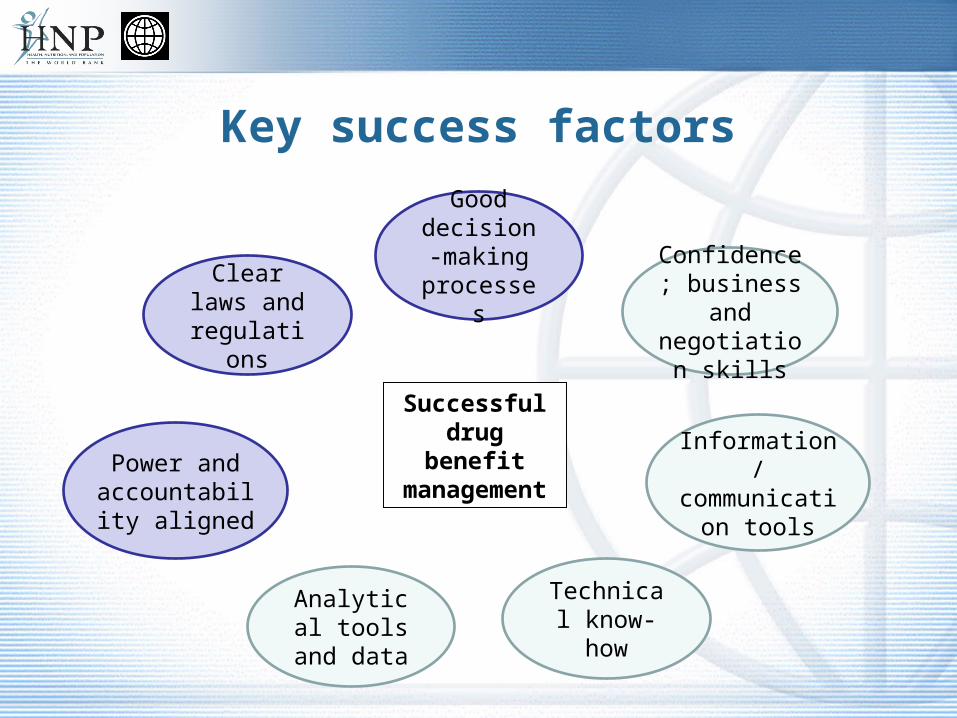
Key success factors
Clear laws and
regulations
Power and accountability
aligned
Confidence; business and negotiation
skills
Analytical tools and
data
Good decision-making
processes
Technical know-how
Information / communicatio
n tools
Successful drug benefit management
Reimbursement decisions
Principles:
• Only cost-effective choices should be reimbursed
• Reimbursement should be sufficient to ensure access without discriminating against low-income groups or chronically ill patients
Cost control from an insurer and patient perspective
Cost = price x volume Insurance funds often look at reimbursement rates as proxy for price, but
this is not fair to patients Two types of co-payments:
• Statutory as fixed amount or percentage of a theoretical reimbursement price
• Difference between reimbursed price and full market price of selected product
When products are being clustered for reimbursement purposes, choices made by doctors, pharmacists, patients can lead to significant variations of out-of-pocket payments
Tolerance for co-payment varies based on patient experience
Brand loyalty is a hurdle
More relevant in markets with traditionally high co-payments Usually “brokered” by doctor or pharmacist in response to incentives Patients are rarely loyal* to a specific drug (even chronic patients go
through frequent changes in their medication), but easily scared by remarks made by experts on quality, strength
*except in cases where there is a “stand-alone treatment” like in certain cancers, immunological diseases, transplantation etc. – here switching to a generic or alternative, cheaper treatment may require appropriate consultation to ensure patient compliance
Neutralizing incentives that work against policy
Generic prescribing should be the rule Pharmacist’s income based on flat dispensing fee rather than
percentage of sales Prescribing targets and monitoring for physicians; feedback, ranking,
academic detailing, incentives, fines Measures to stimulate price competition within clusters, for example
“preferred brand” status with lower co-payment
Variations of clustering
Same molecule (example all simvastatin products) - with adjustments for strength and formulation
Same chemical class as long as effects and tolerability are similar (example all statins) – with adjustment for different per-mg activity
Equivalent clinical efficacy and tolerability without chemical class limit
How manufacturers fight clustering
Same molecule: special formulations, packaging variations, shift to other, more expensive drugs in the same class (example esomeprazole instead of omeprazole)
Same class: shift to other classes (example from ACE inhibitors to ARBs), clinical differentiation in head-to-head trials or large scale trials to establish long term outcomes
Across classes: ?
Questions to be answered
Scientific criteria for clustering beyond “same molecule” category? Adequate decision making process? Expected budget impact – is it worth the fight? Is know-how from other countries transferrable? Should patented drugs get a special status / be exempt from clustering? Are there good alternatives that are easier to implement? What is the “maintenance” process, for example if a manufacturer
launches a variation of a clustered product? Which other measures are necessary to achieve the desired impact
without exposing patients to higher co-payments?