Embed Size (px)
Citation preview
IBM Business Consulting Services
ibm.com/bcs
An IBM Institute for Business Value executive brief
Pharma 2010: The threshold of innovation
The IBM Institute for Business Value develops fact-based strategic insights for senior
business executives around critical industry-specific and cross-industry issues. This executive
brief is based on an in-depth study created by the IBM Institute for Business Value. This
research is a part of an ongoing commitment by IBM Business Consulting Services to provide
analysis and viewpoints that help companies realize business value. You may contact the
authors or send an e-mail to [email protected] for more information.
Pharma 2010: The threshold of innovation IBM Business Consulting Services3
Pharma 2010: The threshold of innovation – an updateIt has been almost two years since we originally published the 2010 story told in
Pharma 2010: The threshold of innovation. It has received wide coverage in the
media; we have presented at numerous industry conferences in North America,
Europe and Asia; and we have taken the story to major pharmaceutical companies
around the globe, many of whom have asked us to come back repeatedly to
present the story to other groups within their organizations. The story has met with
overwhelming support, and the general response has confi rmed our assessment
of industry conditions. We have entered lively discussions about many of our “ways
forward” approaches, but they are invariably centered on when a particular trend
will occur, not whether it will occur. Our defi nition of the problem statement is now
well accepted by the industry, to the point where several CEOs have waived off the
fi rst part of the presentation, proclaiming, “We buy the problem now, now design
solutions that meet our needs.”
Since publishing Pharma 2010, the passage of time has added facts and
experiences, which have substantiated our original premises, namely, that the
industry still does not generate enough innovation, will miss its growth targets and
needs a new model for meeting emerging realities.
We have seen additional consolidation with Pfi zer’s acquisition of Pharmacia and
Sanofi ’s acquisition of Aventis, and analysts have adjusted their forecasts, coming
closer to our own compounded annual growth forecast of 5.2 percent. There is,
today, little question that the industry has entered an era of much lower returns.
Further, the premise of the “threshold of innovation” – that pressure from managed
care providers will make it increasingly diffi cult to bring products to market if they
do not add signifi cant value through improved effi cacy, safety, delivery or cost
– has been borne out with products like AstraZeneca’s Crestor, that has, to date,
experienced disappointing sales. And yet another blockbuster, Merck’s Vioxx, has
been withdrawn due to safety concerns identifi ed almost fi ve years after marketing
approval was fi rst granted.
The focus on cost reduction is intense today, and we expect this trend to continue
as the industry manages the near-term trough and attempts to build a future based
on product innovation and cost effective, streamlined operations. To enhance cost
containment strategies and improve responses to market conditions, companies
are broadening their outsourcing of key enterprisewide processes, such as HR,
Pharma 2010: The threshold of innovation IBM Business Consulting Services4
fi nance, procurement and customer care. This adds fuel to a burgeoning trend which
is prompting companies industrywide to search for a new business model, one
that looks strikingly similar to the Targeted Treatment Solutions model described in
Pharma 2010. New business models, based on business transformation outsourcing
for example, represent one way the industry can refocus its resources.
What have we learned during the past two years? First, business models already
exist that this industry can borrow from others to drive down costs and increase
innovation. Second, although it has been diffi cult for large fi rms to make the kinds of
changes called for, interest in doing so has simply grown over time. That is why we
are republishing Pharma 2010.
The report is essentially the same as published two years ago; however, we have
updated information where appropriate. Since the new data reinforced the paper’s
original concepts, we have not revised its key points. Since 2002, we have also
examined facets of the story in more detail, publishing additional studies related to the
use of information technology, supply chain transformation and a wide mix of other
industry-specifi c issues. These papers can be accessed at http://www.ibm.com/bcs/
pharma2010.
We want to thank all of the industry executives and analysts who worked with us and
endorsed our assessment. We are continuing to identify ways that fi rms can meet
the twin challenges of cost control and profi table growth, and we will publish those
ideas as they mature. But in the meantime, thank you for making Pharma 2010 an
industry “best seller!”
– The 2010 Team
Pharma 2010: The threshold of innovation IBM Business Consulting Services1
On target: The future of medicinesIn 2010, the pharmaceutical industry (Pharma) will not only make white powders; it will sell a variety of products and therapeutic healthcare packages that include diagnostic tests, drugs and monitoring devices and mechanisms, as well as a wide range of services to support patients. Companies that learn how to make “targeted treatment solutions”, as we call them, will deliver bigger shareholder returns than they have ever delivered before. This is what our vision of the future looks like.
Discovery and developmentDrug discovery and development will be underpinned by an understanding of how different diseases function both at a molecular level and as part of a biological system. The molecular sciences will enable the industry to defi ne diseases much more accurately – and to create a collection of treatments and services for patients with specifi c disease subtypes, rather than making one-size-fi ts-all drugs for patients with similar symptoms but essentially different diseases.
Many of these new medicines will be based on biology rather than chemistry, because biologics are typically less toxic than chemical entities and behave more predictably. They will be made using biological methods of discovery and research, which are easier and faster than traditional methods. And they will be available in a variety of formulations that patients fi nd convenient, rather than having to be delivered by injection.
Modeling, simulation and high-performance computing will play a vital role in the way such medicines are discovered and developed. They will enable the industry to model how drugs act in whole body systems, organs and at a sub-cellular level; to design accurate trials; and to conduct adaptive trials, where information acquired during a particular trial is used to modify the course of the same trial without compromising its statistical validity.
Promising new drugs will fi rst be tested in man during late-stage discovery, to prove their safety and effi cacy. They will be tested still further in Phase II trials and submitted to the regulators for conditional approval. They will then be launched on the market and subjected to additional “in-life testing,” using a variety of remote monitoring devices that exploit advances in bandwidth, networking, mobile telecoms, radio frequency technologies and miniaturization – thereby obviating the need to expose patients to placebos or dosing levels that are pharma-cologically ineffective.
Contents
1 On target: The future of medicines
4 Introduction
6 Drivers of change
6 Chapter 1: Tough times
14 Chapter 2: The old ways don’t work
19 The road to the future
19 Chapter 3: The rise of the targeted treatment solution
29 Recommendations
29 Chapter 4: A disease-driven approach to drug discovery
33 Chapter 5: The transformation of drug development
42 Chapter 6: The potential for global blockbusters
48 Chapter 7: Targeted marketing for targeted treatments
56 Summary and implications
56 Chapter 8: A new business model
59 About the authors
59 About IBM Business Consulting Services
60 References

Pharma 2010: The threshold of innovation IBM Business Consulting Services2
Collectively, these changes will blur the boundaries between discovery, development and the marketplace – creating a fully integrated model. They will also massively reduce the time and cost of making new drugs. In 2010, the discovery and development process will take half as long as it does now, and costs per drug will fall to a quarter of the current average.
Regulation Pharma companies will initiate contact with the regulatory authorities regarding the devel-opment of a particular treatment while it is still in the early stages of discovery. They will submit clinical data to the regulators on an ongoing automated basis via rolling dossiers. And they will work much more closely in partnership with the regulators throughout the entire discovery and development process.
The very basis on which the regulators grant permission to sell a drug will also change. The traditional one-off endorsement will be replaced by continuous evaluation. The right to market a drug will be granted and re-confi rmed subject to regular reviews of its safety and effi cacy – reviews that are even more stringent than the checks involved in adverse-event reporting.
In 2010, Pharma will engage much more fully with healthcare payers, physicians and patients as well. In this way, it will get better feedback – both clinical and commercial – at a much earlier point in the development process. It will also be able to promote accurate diagnosis and treatments, and support medical practitioners.
Sales and marketing Many of the new medicines that are made will cover secondary rather than primary care, so they will be marketed differently – using smaller sales teams, trained to converse with specialists. But all new medicines will be promoted on the basis of the specifi c disease states they address, rather than whether or not they work better than competing products. They will be supported by objective evidence and priced according to the medical results they deliver, not the price of rival drugs that are already on the market. And a substantial part of their value will lie in the services that come with them.
These services will form the backbone of a comprehensive support network that helps individual patients to identify when they really need to see a doctor; to manage the particular disease states from which they suffer; and to understand why they should keep taking the medicines they have been prescribed. In conjunction with targeted treatments and remote monitoring, better persistence will improve the healthcare patients receive. It will also boost the industry’s revenues.

Pharma 2010: The threshold of innovation IBM Business Consulting Services3
The future of Pharma Our research shows that these changes will be driven by the shifting balance of power between Pharma and its customers. Governments, healthcare insurers and patients are increasingly dictating the sort of new drugs they want and the prices they are willing to pay. In short, it is the healthcare payers – not the drug makers – that are now defi ning the threshold of innovation. They are also squeezing every ounce of value out of products that are already available, so they are raising the threshold of innovation ever higher.
But a much better grasp of the biological sciences and a massive increase in computing power will equip the industry with the tools to rise to this challenge. In 2010, we believe Pharma will be able to develop products and therapeutic packages that demonstrably surpass the drugs that are already on the market – the hurdle governments and healthcare insurers will set in deciding when to pay premium prices.
Pharma 2010: The threshold of innovation IBM Business Consulting Services4
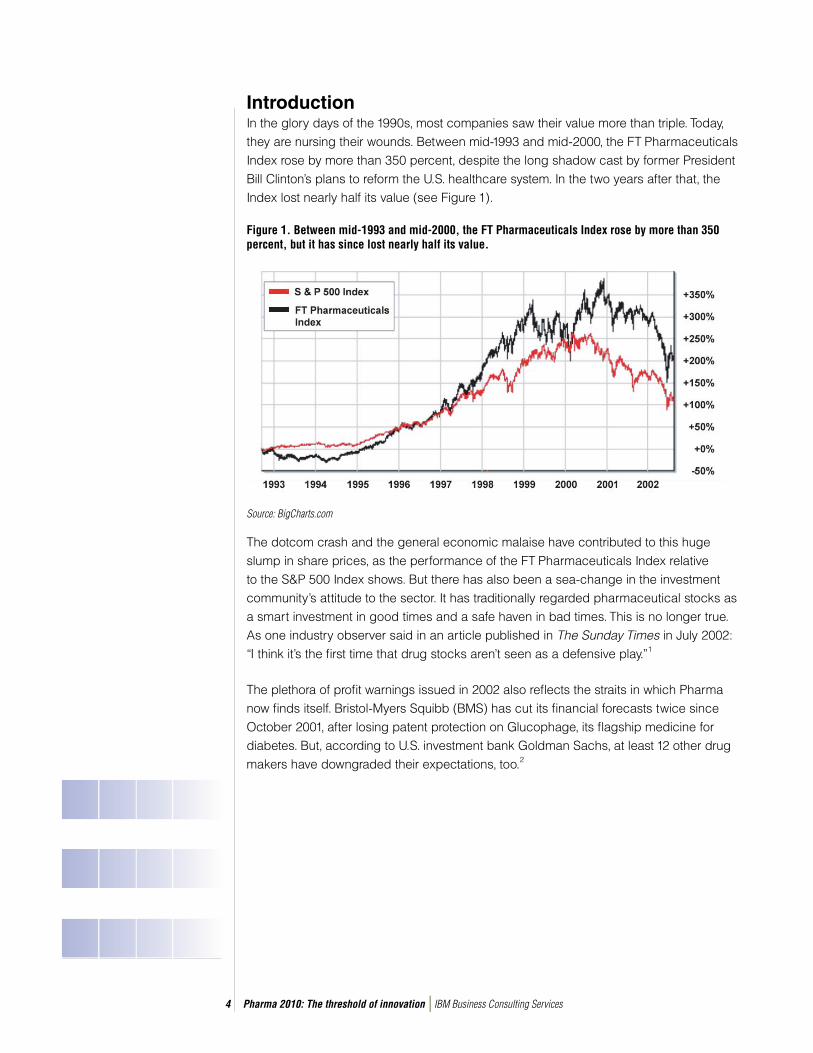
IntroductionIn the glory days of the 1990s, most companies saw their value more than triple. Today, they are nursing their wounds. Between mid-1993 and mid-2000, the FT Pharmaceuticals Index rose by more than 350 percent, despite the long shadow cast by former President Bill Clinton’s plans to reform the U.S. healthcare system. In the two years after that, the Index lost nearly half its value (see Figure 1).
Figure 1. Between mid-1993 and mid-2000, the FT Pharmaceuticals Index rose by more than 350 percent, but it has since lost nearly half its value.
The dotcom crash and the general economic malaise have contributed to this huge slump in share prices, as the performance of the FT Pharmaceuticals Index relative to the S&P 500 Index shows. But there has also been a sea-change in the investment community’s attitude to the sector. It has traditionally regarded pharmaceutical stocks as a smart investment in good times and a safe haven in bad times. This is no longer true. As one industry observer said in an article published in The Sunday Times in July 2002: “I think it’s the fi rst time that drug stocks aren’t seen as a defensive play.”1
The plethora of profi t warnings issued in 2002 also refl ects the straits in which Pharma now fi nds itself. Bristol-Myers Squibb (BMS) has cut its fi nancial forecasts twice since October 2001, after losing patent protection on Glucophage, its fl agship medicine for diabetes. But, according to U.S. investment bank Goldman Sachs, at least 12 other drug makers have downgraded their expectations, too.2
Source: BigCharts.com

Pharma 2010: The threshold of innovation IBM Business Consulting Services5
The shifting balance of power A potent mix of problems, including lack of productivity in the laboratory, patent expiries and intense therapeutic competition, has made it increasingly diffi cult for Pharma to make good new medicines. The situation has been compounded by a gradual shift in the balance of power. Where once the industry could command a good return on investment, governments and healthcare insurers are now beginning to stipulate the sort of improve-ments they want and the prices they are willing to pay. They are not just defi ning the threshold of innovation; they are using much more quantitative measures of innovation than they did previously, and squeezing every ounce of value out of drugs that are already on the market, so they are raising the threshold of innovation ever higher.
Pharma has also incurred growing criticism for concentrating primarily on the chronic degenerative illnesses of the developed world and failing to address the needs of the billions of people living in less developed countries, although some companies have done more on this front than is widely recognized. Pfi zer has, for example, launched an initiative to deal with trachoma, while Aventis has focused on African trypanosomiasis and Novartis on leprosy. Similarly, GlaxoSmithKline (GSK) is trying to tackle malaria.3 It is also cutting prices yet again.4
A totally different perspective Yet, bleak though the current outlook is, we believe there are grounds for great optimism. A better grasp of the molecular sciences and a better electronic infrastructure will give Pharma some of the tools it needs to meet these challenges. Those tools will ultimately enable the industry both to surmount the rising threshold of innovation in the developed world and to reduce the cost of pharmaceutical discovery and development so signifi -cantly that it can serve some of the world’s poorer markets, profi tably.
But if Pharma is to realize the full potential of these scientifi c and technological advances, it will need to alter its perspective. Rather than focusing on the search for new one-size-fi ts-all drugs, it will need to focus on defi ning diseases much more precisely – and that will, in turn, enable it to develop treatments for specifi c disease states. Looking through the opposite end of the telescope to the one on which the industry has relied for so many decades will entail massive changes in the way it makes and markets new medicines. It will also require that companies forge much closer links with the regulators, healthcare payers, doctors and patients, to ensure that they make the sort of drugs people really want.

Pharma 2010: The threshold of innovation IBM Business Consulting Services6
We shall discuss all these changes in much greater detail in the rest of this paper, which follows up on the work we published in the “Pharma 2005” series. We shall also discuss the fi nancial implications they carry. We have modeled the impact of various scenarios on the industry’s shareholder value.5 Our model shows that, regardless of what happens over the next eight years – the landmark we have set – Pharma cannot stand still.
Companies that fail to respond to the market conditions which are now emerging – and those that are currently most successful may well be those that most resist making the requisite changes – will see their value continue to plummet. But even those that are most successful in using traditional techniques to maximize revenues from traditional products will not be able to generate suffi cient growth. At best, they will do little more than double their current value by 2010 – a performance that falls far short of the increase in shareholder value the industry provided in the 1990s.
It is only by entering totally new terrain that Pharma companies can hope to produce the truly innovative medicines for which people will readily pay, but if they succeed, the rewards will be huge. We estimate that, even if the market for “targeted treatment solutions” (as we have called them) is slow to get started, companies that learn how to make such medicines could triple their shareholder value by 2010. If the market for such medicines takes off more rapidly, they could enjoy almost twice the growth the industry enjoyed in its heyday – a prize well worth the effort required.
Drivers of changeThe shortage of good new drugs in the pipeline; the imminent expiry of the patents on numerous blockbusters; intense competition; a more demanding market that has begun to specify the sort of innovations it wants, and what it is willing to pay for them – all these challenges are making life very much harder for Pharma than it was a few years ago. The industry has responded with several strategies that have previously proved successful. It has shopped around for new leads in the biotechnology sector, exploited its consid-erable marketing clout, and consolidated rapidly. Yet the evidence suggests that none of these tried and tested techniques will be suffi cient to close the fi nancial gap.
Chapter 1: Tough timesOver the years Pharma has developed a very successful model for making new medicines. The world’s leading companies have collectively validated about 500 targets – the biological mechanisms (usually receptors or enzymes in human cells) through which drugs work.6 They have created large compound libraries, containing as many as two million molecules apiece. They have evolved a phased development process that includes large-scale trials to establish the safety and effi cacy of their products, and they have patented those products to protect their huge investment.
Pharma 2010: The threshold of innovation IBM Business Consulting Services7
They have become equally profi cient at marketing and selling new medicines. They have acquired the expertise to launch new drugs rapidly across a wide range of territories; built big sales forces to promote those drugs; and secured premium prices to generate the revenues they need for further research and development (R&D). They have also tapped the potential of direct-to-consumer (DTC) advertising; managed the lifecycle of their products to maximize returns on investment; and in-licensed new products to sustain their therapeutic franchise.
The results of this approach speak for themselves. During the past two decades, sales of new drugs and new formulations of older drugs have consistently outstripped the fall in income from products that have come off patent. And that has enabled Pharma to reward investors very handsomely: between 1993 and 1998, some of the industry leaders provided total shareholder returns of more than 40 percent a year. But for a variety of reasons the current model has recently come under growing pressure.
The dearth of good new drugsOne of the main reasons why Pharma has failed to meet shareholders’ expectations is lack of R&D productivity. In 1998, the biggest drug makers each announced that they aimed to produce three new chemical entities (NCEs) a year; indeed, some companies now claim they need to produce three or more billion-dollar blockbusters a year, just to maintain their sales growth. Yet they are far from fulfi lling this promise.
Goldman Sachs estimates that, in 2001, the industry leaders spent about US$35bn, roughly double the sum they spent in 1997 and three times the sum they spent in 1992.7 And in 2003 the 15 major pharmaceutical companies spent US$48bn on R&D.8 Even so, the output of new drugs has declined. In 2003, 30 new active substances (NASs) were launched on to the world market – the lowest number for 25 years – and this downward trend seems set to continue.9 (The number of NME fi lings has also dropped substantially, so longer approval times may have contributed to the fall in productivity, but they are certainly not the sole explanation.)
This is only one sign of how diffi cult it has become to create good new drugs using tradi-tional sciences and technologies. The incidence of post-marketing product withdrawals and late-stage failures in the pipeline is further evidence of the challenges the industry is facing. Between 1997 and 2001, 12 drugs with combined peak sales potential of more than US$11bn were removed from the market. Late-stage failures cost even more; in the three years to 2001, the industry leaders terminated 28 products, with potential peak sales of more than US$20bn, in Phases II or III.

Pharma 2010: The threshold of innovation IBM Business Consulting Services8
The ticking bomb of patent expiriesMeanwhile, Pharma’s existing revenues are exposed as never before. Between 2002 and 2007, the U.S. patents on 35 drugs with global sales of more than US$73bn will expire (see Figure 2).10
Figure 2. Patent expiries will make a huge hole in future revenues.
Experience shows that when a drug comes off patent, sales drop very sharply. Take one recent case: the dramatic erosion in sales of Prozac, Lilly’s well-known antidepressant, which came off patent in the U.S. in August 2001. As soon as the fi rst generic version hit the market, Merck-Medco started switching its mail order patients to the new product. Within a week, it had converted 80 percent of them. Express Scripts did the same and, by December 2001, almost 90 percent of its mail order patients were taking the generic alternative. As a result, sales of Prozac fell by 22 percent, in 2001.11
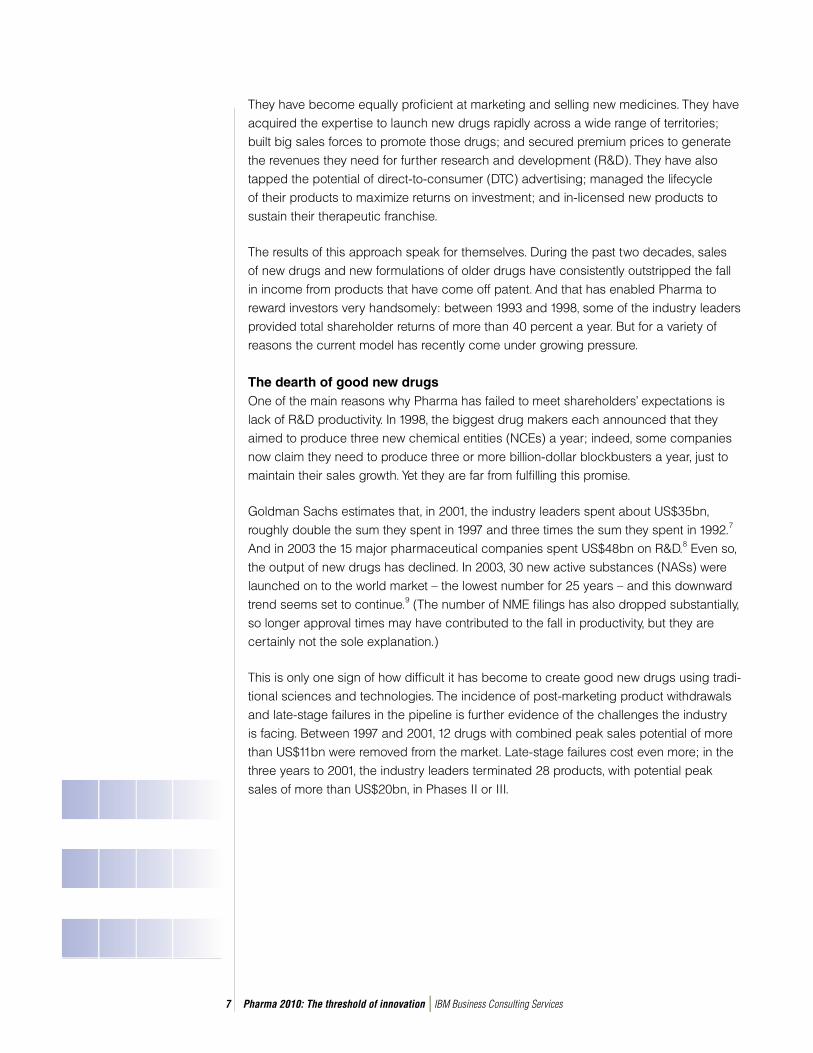
Pharma will fi nd it hard to replace much of this revenue. In a report published in 2002, Datamonitor estimated that there were four potential blockbusters in the industry’s pipeline in 2002, and another 14 such drugs in the pipeline between 2003 and the end of 2008 – excluding products that have already been launched in different indications or in any part of the world (see Figure 3).12 But none of these new medicines is expected
Source: Datamonitor, 2002.
Blockbuster U.S. Patent expires, 2002 - 2007
Pharma 2010: The threshold of innovation IBM Business Consulting Services9
to make as much money as the current stars in the industry’s fi rmament. Crestor, the dyslipidemia drug in AstraZeneca’s late-stage pipeline, is widely regarded as the most promising product on the horizon. Yet Datamonitor forecasts peak sales of about US$3.8bn – little more than half the US$6.7bn Merck’s blockbuster statin Zocor earned in 2001.
Figure 3. Only 14 potential blockbusters are likely to be launched between 2003 and 2006 and the next few years look even bleaker.
The might of managed careThe economic environment in which Pharma operates is also changing quite dramati-cally. The industry has put an increasing amount of its energies into developing block-buster drugs and marketing them very aggressively. In 1992, there were only four blockbusters on the market. By 2001, there were some 50 such drugs (most of them for treating chronic conditions). The blockbuster’s share of the total market has correspond-ingly expanded. In 1991, it represented about 6 percent of overall sales. By 2001, it repre-sented more than 45 percent.13
The industry has simultaneously focused to a much greater extent on the U.S., which has less rigid pricing restrictions than other countries. In 2001, the U.S. generated 48 percent of global sales, signifi cantly more than the 24 percent that was generated in Europe. The rate of growth was also bigger, at 17 percent, than it was anywhere else in the developed world.14 Both these changes have made Pharma increasingly dependent on blockbuster sales in the U.S. Today, the U.S. accounts for 67 percent of global blockbuster sales.
Source: Datamonitor, The Next Generation of Blockbusters, 2002.
Pharma 2010: The threshold of innovation IBM Business Consulting Services10
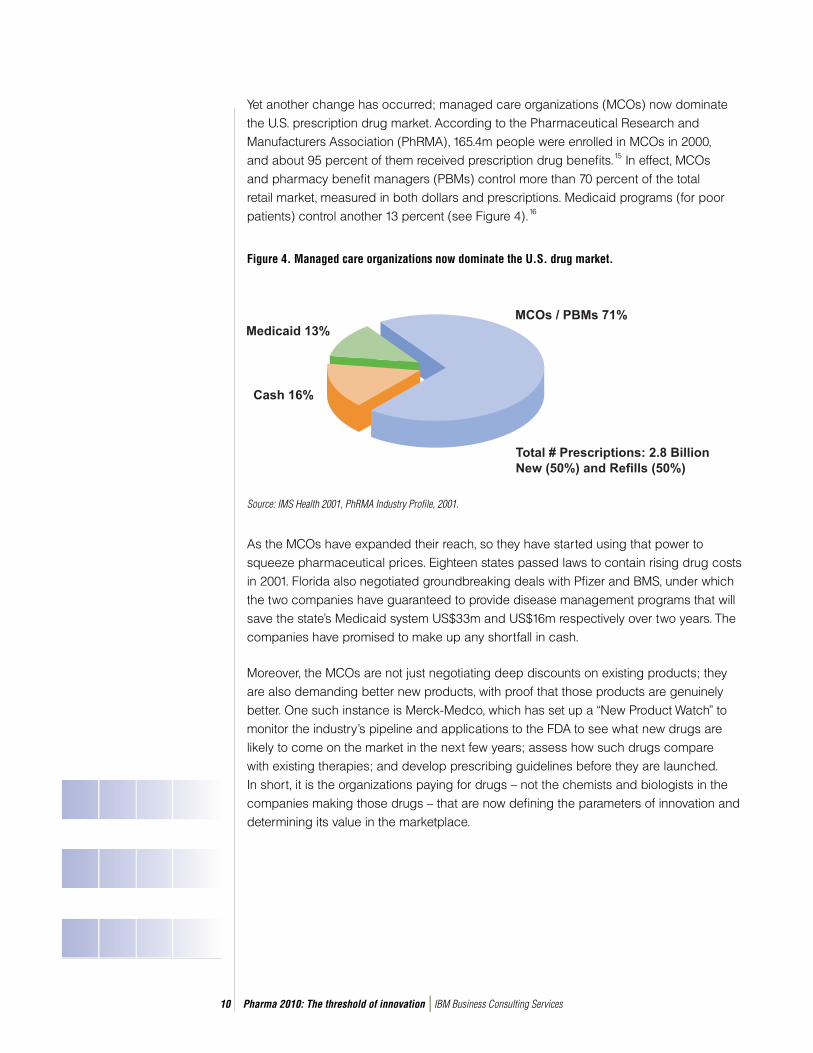
Yet another change has occurred; managed care organizations (MCOs) now dominate the U.S. prescription drug market. According to the Pharmaceutical Research and Manufacturers Association (PhRMA), 165.4m people were enrolled in MCOs in 2000, and about 95 percent of them received prescription drug benefi ts.15 In effect, MCOs and pharmacy benefi t managers (PBMs) control more than 70 percent of the total retail market, measured in both dollars and prescriptions. Medicaid programs (for poor patients) control another 13 percent (see Figure 4).16
Figure 4. Managed care organizations now dominate the U.S. drug market.
As the MCOs have expanded their reach, so they have started using that power to squeeze pharmaceutical prices. Eighteen states passed laws to contain rising drug costs in 2001. Florida also negotiated groundbreaking deals with Pfi zer and BMS, under which the two companies have guaranteed to provide disease management programs that will save the state’s Medicaid system US$33m and US$16m respectively over two years. The companies have promised to make up any shortfall in cash.
Moreover, the MCOs are not just negotiating deep discounts on existing products; they are also demanding better new products, with proof that those products are genuinely better. One such instance is Merck-Medco, which has set up a “New Product Watch” to monitor the industry’s pipeline and applications to the FDA to see what new drugs are likely to come on the market in the next few years; assess how such drugs compare with existing therapies; and develop prescribing guidelines before they are launched. In short, it is the organizations paying for drugs – not the chemists and biologists in the companies making those drugs – that are now defi ning the parameters of innovation and determining its value in the marketplace.
Source: IMS Health 2001, PhRMA Industry Profile, 2001.
Pharma 2010: The threshold of innovation IBM Business Consulting Services11
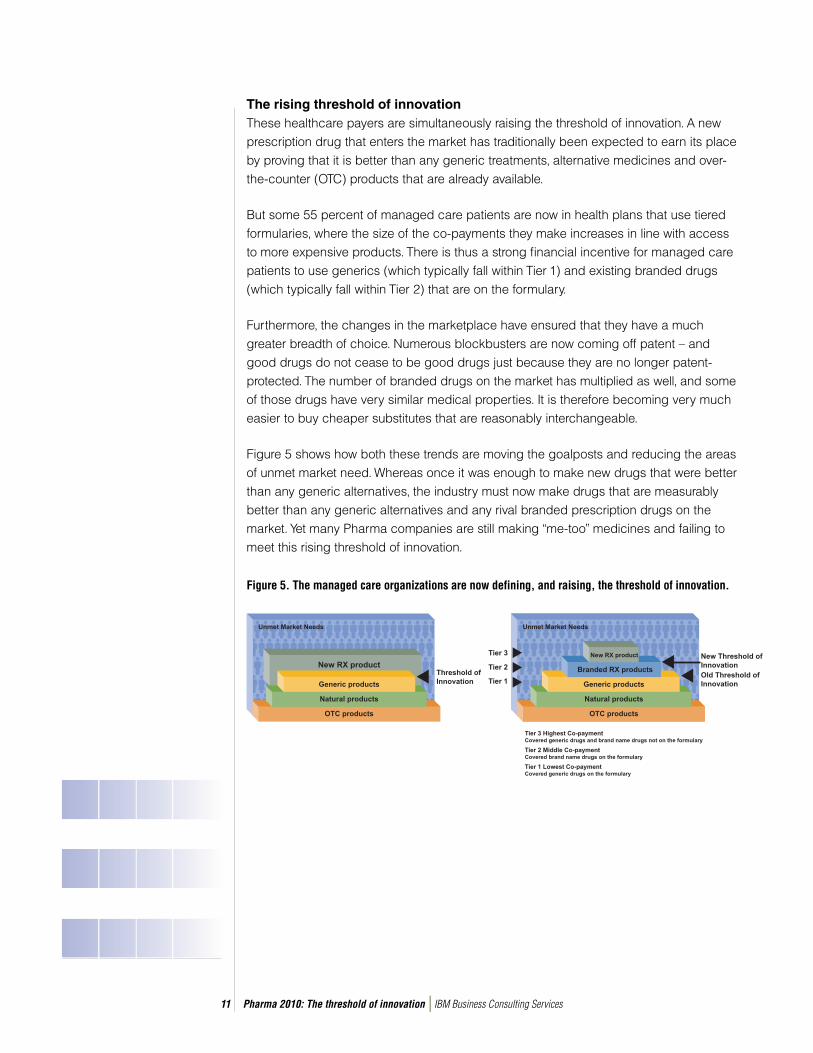
The rising threshold of innovation These healthcare payers are simultaneously raising the threshold of innovation. A new prescription drug that enters the market has traditionally been expected to earn its place by proving that it is better than any generic treatments, alternative medicines and over-the-counter (OTC) products that are already available.
But some 55 percent of managed care patients are now in health plans that use tiered formularies, where the size of the co-payments they make increases in line with access to more expensive products. There is thus a strong fi nancial incentive for managed care patients to use generics (which typically fall within Tier 1) and existing branded drugs (which typically fall within Tier 2) that are on the formulary.
Furthermore, the changes in the marketplace have ensured that they have a much greater breadth of choice. Numerous blockbusters are now coming off patent – and good drugs do not cease to be good drugs just because they are no longer patent-protected. The number of branded drugs on the market has multiplied as well, and some of those drugs have very similar medical properties. It is therefore becoming very much easier to buy cheaper substitutes that are reasonably interchangeable.
Figure 5 shows how both these trends are moving the goalposts and reducing the areas of unmet market need. Whereas once it was enough to make new drugs that were better than any generic alternatives, the industry must now make drugs that are measurably better than any generic alternatives and any rival branded prescription drugs on the market. Yet many Pharma companies are still making “me-too” medicines and failing to meet this rising threshold of innovation.
Figure 5. The managed care organizations are now defining, and raising, the threshold of innovation.
.
That’s not all. The decision as to whether a new drug is better than rival brands rests with the MCOs, which have a vested interest in putting as many new drugs as possible in Tier 3 (where patients pick up a big portion of the bill), unless such drugs are demon-strably better than their rivals. This is making it more diffi cult than ever for drug makers to achieve the prices and volumes required to produce a blockbuster – the very model on which they have become increasingly dependent.
The worldwide spread of cost controlsThe situation in the U.S. is getting tougher, then, but there are no easy alternatives anywhere else. The European Union (EU) has introduced various measures for reducing drug prices – including reference-pricing rules that mean prices can only go down – and individual member states have taken other steps to cut the bill. A similar drive to contain costs is taking place in Japan. Moreover, although some governments are willing to pay for products they regard as genuinely new, they are becoming much more vociferous in their demands for a quid pro quo in the form of lower prices for drugs that are already on the market.
Several countries have also adopted new prescribing criteria. They have set up “gatekeepers” for evaluating products and therapies in terms of their cost-effectiveness as well as their safety and effi cacy – the two conventional measures for assessing a drug. The UK’s National Institute of Clinical Excellence (NICE) and the Canadian Coordi-nating Offi ce for Health Technology Assessment are two such instances, as is the center for evidence-based medicine at Kyoto University in Japan. But during the last decade almost every country in the developed world has introduced stringent measures to contain soaring healthcare costs, and these measures are becoming increasingly sophis-ticated. So the industry needs to become much more proactive in pointing out that drugs constitute a relatively small percentage of overall healthcare costs.
As if this were not bad enough, the therapeutic competition is also becoming much fi ercer. Just one example illustrates the point. In 1999, Searle (now part of Pharmacia) launched Celebrex, the fi rst of the new class of Cox-2 inhibitors. Merck followed hard on its heels with Vioxx. Today, Pharmacia has another two Cox-2 inhibitors on the market: Bextra, which was approved by the FDA in November 2001; and Dynastat, which was approved by the European Medicines Evaluation Agency in March 2002. There are at least another nine similar products in late-stage development in other companies – and it is hard to see how all these medicines will be able to surmount the rising threshold of innovation.
Pharma 2010: The threshold of innovation IBM Business Consulting Services12

The slowdown in sales growthIn sum, the outlook is bleak. R&D productivity and shareholder value are falling, much as we predicted in “Pharma 2005: An Industrial Revolution,” the report we published in 1998.17 Revenues from existing products are highly exposed, with a very large number of top-selling products due to come off patent over the next few years. Opportunities to make conventional blockbusters are shrinking, as control over the defi nition of innovation moves from the laboratory to the marketplace, and it is becoming increasingly diffi cult to differen-tiate products that treat common chronic conditions on therapeutic grounds alone.
Our research suggests that all these problems will substantially reduce the pace at which sales of branded products grow. We have estimated probable revenues from drugs that are already on the market and from drugs that are likely to be launched over the next eight years. Our fi gures indicate that they will collectively deliver compound annual growth of just 5.3 percent between 2001 and 2010 (see Figure 6).
Figure 6. The growth in sales of branded pharmaceuticals is expected to be very much slower Figure 6. The growth in sales of branded pharmaceuticals is expected to be very much slower between 2002 and 2010. between 2002 and 2010.
This is signifi cantly lower than the 9 percent per annum at which the industry was growing just a few years ago, and massively below the double-digit growth it enjoyed in the early 1990s. A recent analysis of 26 leading pharmaceutical companies by Goldman Sachs confi rms this gloomy picture.18 So it is clearly time for a fundamental review of the way in which Pharma works.
Pharma 2010: The threshold of innovation IBM Business Consulting Services13
Pharma 2010: The threshold of innovation IBM Business Consulting Services14
Chapter 2: The old ways don’t workMost Pharma companies have made strenuous efforts to improve the effi ciency of their R&D, without much success; the odds of getting a molecule to market remain as slim as they did a decade ago. Most companies have also tried to close the fi nancial gap by resorting to three traditional strategies for improving their bottom line:
• They have acquired new products from biotechnology and genomics companies – but this is now becoming very expensive and increasingly difficult, as biotech companies come of age.
• They have maximized revenues from existing products by increasing their market penetration, extending their product lines and raising prices.
• And they have tried to cut costs, usually in the wake of a merger or acquisition.
But although these strategies can reduce the gap between what investors expect and what Pharma can deliver, there is little to suggest they can eliminate it.
A big bill for biotechBiotech and genomics companies currently perform nearly a fi fth of all pharmaceutical R&D, a fi gure that is set to double within the next 10 years.19 Indeed, William Haseltine, chairman and chief executive of Human Genome Sciences (HGS), predicted at a conference in February 2002 that over half of all the New Active Substances (NASs) developed in the next 10 to 15 years will result from research into antibodies.20 Recog-nizing the importance of this work, the industry leaders have been actively shopping around to fi ll the gaps in their pipelines.
But as the competition for drug candidates increases, so prices go up – and there is no guarantee that such money will be well spent, as BMS recently learned. BMS paid ImClone Systems more than US$2bn for the cancer drug Erbitux in a part-cash, part-equity deal, only to see the FDA fi nd fault with ImClone’s trial data in January 2002.
The choice is also becoming more restricted, as the biotech industry matures. A number of the biotech companies that began life by selling technology have evolved into producers in their own right because they are now big enough to go it alone and the capital markets value the direct sales of drugs more highly than royalties from a pharmaceutical partner. Millennium Pharmaceuticals and HGS have products in the clinic, and Genentech has bought back the licensing rights to some of its own drugs. Other companies have benefi ted from the collapse of the dotcom bubble, when investors moved heavily, albeit briefl y, into biotech stocks. In 2000, the biotech industry raised more
Pharma 2010: The threshold of innovation IBM Business Consulting Services15
capital than ever before – and some fi rms were able to raise enough funds to cover their cash requirements for the next four or fi ve years.21
When it comes to stocking the pipeline, then, biotech is in a much stronger position than it was a short while ago. The economic downturn may make some biotech companies more vulnerable, and it is likely that the biggest pharmaceutical companies will still be able to exert a considerable degree of market control. Even so, many companies may well end up paying more than they expected to get their hands on the most promising leads.
Marketing at the limitThe industry’s second line of attack – maximizing revenues from products that are already on the market – is also coming under huge strain. Take the expansion of the sales force to secure greater market penetration. Most Pharma executives would argue, with considerable justifi cation, that the pundits have repeatedly claimed increasing the size of the sales force no longer works – and the industry has repeatedly proved them wrong. But there are now a number of signs that this technique really is reaching the end of its life.
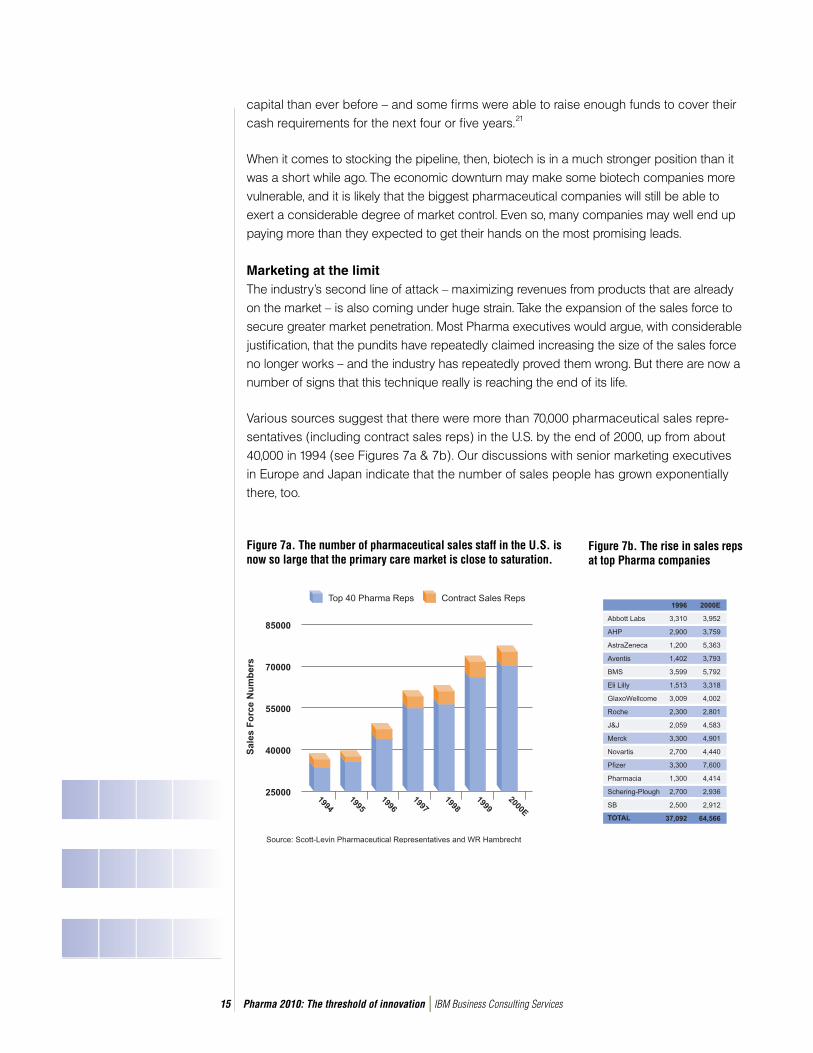
Various sources suggest that there were more than 70,000 pharmaceutical sales repre-sentatives (including contract sales reps) in the U.S. by the end of 2000, up from about 40,000 in 1994 (see Figures 7a & 7b). Our discussions with senior marketing executives in Europe and Japan indicate that the number of sales people has grown exponentially there, too.
Figure 7a. The number of pharmaceutical sales staff in the U.S. is now so large that the primary care market is close to saturation.
Figure 7b. The rise in sales reps at top Pharma companies

Pharma 2010: The threshold of innovation IBM Business Consulting Services16
But research by Lehman Brothers, the U.S. investment bank, shows that the primary care market in the U.S. at least is now close to saturation. There are only 400,000 practicing physicians in the whole country – and 250,000 of them write four-fi fths of all prescriptions. Moreover, most companies put most of their efforts into targeting the top 150,000 physi-cians, so each top physician would need to see a sales rep every two hours to justify such a large sales force.22 Further expansion of the sales force therefore seems likely to yield diminishing returns – and some companies may have recognized this already. It would certainly explain the growing level of interest in e-detailing, as a means of reaching doctors as effectively and economically as possible.
The situation is very different when it comes to DTC advertising; the more the industry spends, the more it sells. But the sheer enthusiasm with which consumers have responded has begun to elicit alarm. Expenditure on DTC advertising in the U.S. reached US$3.3bn in 2003.23 The EU is also testing the waters; it recently loosened the constraints on DTC advertising of products for HIV/AIDS, diabetes and asthma.
However, a survey conducted by the FDA in 1999 found that when patients asked their doctors for a specifi c product, 82 percent got a prescription – and 50 percent got the particular brand they requested.24 Similarly, Merck-Medco estimates that expenditure on the most heavily promoted drugs is rising three times more than it is on those drugs that are not advertised at all.25 There may thus be something of a backlash against DTC advertising, if it proves as powerful a weapon as some people suspect.
Many companies are also trying to extend the economic life span of drugs that are already on the market by spinning off new formulations or versions of them. Indeed, 65 percent of the new drug applications (NDAs) the FDA approved between 1989 and 2000 were for drugs containing existing active ingredients.26 This practice is certain to continue, although it carries several dangers. First, the attempt may backfi re, as it did for BMS when it failed to persuade U.S. Congress to extend the monopoly on Glucophage. Second, it may prove diffi cult to migrate patients to newer formulations that do not offer genuine medical advances. Several industry sources have, for example, expressed doubts that the discount Schering-Plough is offering on Clarinex, the follow-up drug to Claritin, will be enough to persuade patients to switch products, given that generic versions of Claritin will retail at half the price of the branded drug.
Aggressive promotion of new, more expensive versions of existing medicines has boosted revenue. Pharma has also lifted prices, in common with other industry sectors. But though each of these factors has contributed to the rise in prescription

Pharma 2010: The threshold of innovation IBM Business Consulting Services17
The splurge to merge
In November 1998, we predicted that financial constraints
would fuel a spate of M&As, leaving as few as 13 industry
giants by 2005.33 Since then, Hoechst and Rhône Poulenc
have amalgamated to create Aventis; Astra and Zeneca
have joined forces, as have Glaxo Wellcome and SmithKline
Beecham; Sanofi and Synthélabo have united; Pharmacia &
Upjohn has merged with Monsanto; and Pfizer has pulled
off the industry’s biggest hostile bid with the acquisition of
Warner-Lambert. It also plans to buy Pharmacia, creating a
combined group with annual revenues of more than US$48bn.
Serious money is involved. The merger of Glaxo Wellcome
and SmithKline Beecham was valued at US$76bn and the
purchase of Warner-Lambert at US$87bn. But these are just
the deals that have garnered the bulk of the headlines, partly
because of their size. In 2001, the industry completed 334
M&As – only seven less than it completed the year before.
The trend towards consolidation has been driven by several
factors – including the desire to secure economies of scale;
boost tired pipelines; get a stronger foothold in the most
important geographic and therapeutic markets; and strip out
surplus capacity. It has also concentrated market share. Data
from IMS Health shows that in 2000 the top 20 companies,
measured by pharmaceutical revenues, accounted for 64.6
percent of audited sales worldwide. The next 20 companies
accounted for just 11.3 percent.34
drug spending, increasing drug utilization accounts for a bigger share. Merck-Medco estimates that, between 1996 and 2000, the average U.S. drug spend per member per year nearly doubled. Greater use of drugs was responsible for almost half this additional sum; higher prices accounted for only 22 percent of the overall increase.27 Prices went up more in 2001. Nevertheless, it is clear that the main reason the drugs bill is climbing is because more people are taking more medicines for a wider array of conditions than ever before, not because Pharma has been especially successful in making and selling innovative new medicines.
Big but not always betterSo have mergers and acquisitions (M&As) proved any better a route? The rate of consoli-dation has certainly been frenetic. During the past four years alone there have been six “mega-mergers” and many hundreds of smaller transactions (see box on The splurge to merge). In July 2002, Pfi zer also announced plans to buy Pharmacia in a US$60bn, all-stock deal that will make it by far the world’s largest drug maker with 11 percent of the global market, and Roche is currently completing the friendly takeover of Chugai, Japan’s tenth biggest pharmaceutical company.
There is some evidence that size counts when it comes to licensing in good new medicines. However, critics say that there is little sign of greater productivity in the industry giants that have consolidated. In its latest assessment of pipeline valuations, for example, Goldman Sachs has measured the productivity of the industry leaders by comparing the net present value (NPV) of their late-stage pipelines with their capitalized R&D. Between 1997 and 1999, 29 top-selling drugs were in-licensed – and Pharma’s heavyweights secured the rights to four times as many of these drugs as the middleweights did.28 This shows that three of the fi ve companies with the highest pipeline NPVs, in absolute terms, score below the global sector average on productivity (as do half the top 10 companies).29
Moreover, M&As are notoriously diffi cult to manage, and many actually destroy shareholder value. In a study of 193 mergers conducted by Southern Methodist University in the U.S., 89 percent of the target companies had experienced a slowdown in revenue growth by the third quarter after the deal was announced. Additional research by McKinsey on more than 160 acquisitions suggests that only 12 percent of acquiring companies manage to accelerate their growth signifi cantly over the next three years, while 42 percent lose ground.30

Pharma 2010: The threshold of innovation IBM Business Consulting Services18
In short, the strategies to which Pharma has historically resorted are no longer suffi cient. They are reducing the gap between the fi nancial expectations of investors and the actual performance of the industry leaders, but they are certainly not eradicating it.
The global challengeTo make matters worse, the industry has also come under growing social and political pressure both at home and abroad. Economic, demographic and political changes are sweeping through the world (see box on The global picture). These changes will open up new markets, but they will simultaneously compound the diffi culties the leading drug makers face.
Pharma’s traditional expertise lies in making medicines for people who live in the developed world and selling them at premium prices. However, it has attracted increasing criticism in the media for failing to tackle the plight of the very poor. In fact, some companies have made much more active efforts in this respect than the press coverage might suggest, but their efforts have been individual rather than co-ordinated with those of other industry players and governments. The World Health Organization (WHO) Commission on Macroeco-nomics and Health concluded in a report published in December 2001: “The corporate principles that have spurred recent and highly laudable programs of drug donations and price discounts need to be generalized to support the scaling up of health interventions in the poor countries.”31
If the industry is to preserve its reputation and provide better healthcare for everyone, then, it must simultane-ously develop more innovative products and make a bigger effort to serve the needs of people in the less and least developed regions – although it certainly cannot, and should not be expected to, solve the health problems bedeviling these populations by itself.
The global picture
About 1.2bn people live in the developed countries.35 The population
is also becoming more diverse, as political and economic migration
redraw the global map. But the biggest change of all is the gray factor.
Thirteen percent of the people living in North America, 15 percent
of those living in Europe and 17 percent of those living in Japan are
now over 65 – compared with a global average of just 7 percent.36 In
all, the WHO estimates that there are some 355m elderly people in
the key Pharma markets today.37 Mass longevity and the increasing
expectations of aging “Baby Boomers” – spurred on by the information
they have gleaned from DTC advertising and the Internet – are
stimulating demand for more and better healthcare. But they are also
straining already over-stretched healthcare budgets to breaking point.
The less developed world is likewise struggling to curb soaring
healthcare bills. The problem is especially acute in Asia, where
AIDS may become an even bigger killer than it is in Africa.38 But the
population is growing very rapidly, too. About 4.2bn people live in Latin
America and the Caribbean, Asia Pacific and the Indian sub-continent;
and the UN predicts that the numbers will reach 6.3bn over the next 50
years. Many of these people do not have very much money, but most
less developed countries are effectively multiple markets, with different
financial and educational attributes, medical problems and expectations
for healthcare provision. China, for example, can be divided into two
distinct segments: the rural and urban. About 455m people – 35
percent of the country’s 1.3bn inhabitants – now live in cities, enjoy
increasing prosperity and rely to a growing extent on the branded
pharmaceuticals produced by the big Western drug makers rather than
local generics, so the urban market is starting to look very attractive.
Moreover, the population is aging; according to the national census in
2000, 88.1m people are 65 or older.39
The situation is different again in the least developed world. About
700m people live in sub-Saharan Africa and the population is also
growing very rapidly. However, AIDS has wreaked havoc on its health
and the vast majority of people cannot afford the drug prices that
prevail in the developed world. In fact inadequate infrastructure is an
even bigger barrier than poverty, and the shortage of medicines goes
much further than treatments for AIDS; many of the diseases from
which these populations suffer are not prevalent in developed countries
and so drugs have not been produced to treat them (although Pharma
has been successful in developing vaccines for some conditions). But
it is clear that the industry will never be able to make any money in the
very poorest parts of the world, and this is why it gives drugs away in
such areas.

Pharma 2010: The threshold of innovation IBM Business Consulting Services19
As PhRMA, the leading U.S. trade body, states: “The tremendous challenges facing developing countries demand continued and concerted efforts from both the private and public sectors – and we stand ready to participate in effective partnerships to help improve public health.”32
The road to the futureThe industry has traditionally produced “one-size-fi ts-all” drugs that share certain thera-peutic and economic features, but a new type of product is now beginning to emerge. A growing number of these products are also biological in nature, and most biologically based molecules are both safer than chemical entities and easier to develop (although they are more diffi cult to formulate). Meanwhile, the molecular sciences are providing the tools with which to acquire a much more accurate understanding of disease. Together, these trends will enable Pharma to develop highly profi table healthcare packages for patients suffering from specifi c disease states.
Chapter 3: The rise of the targeted treatment solutionMany of the most successful medicines Pharma has produced have a similar thera-peutic profi le. They are typically fi rst-line treatments; come in a single, one-size-fi ts-all form; are aimed at a mass population; are easy to take (often orally); treat a chronic condition; and ameliorate the symptoms of the disease rather than changing the way in which it progresses.
These medicines have similar economic features, too. They are typically very expensive to research and develop; the Tufts Center for the Study of Drug Development estimates that average costs per drug are now US$802m (including the cost of capital).40 They take about 10-12 years to progress from the laboratory to launch.41 They require an intensive marketing and sales push to promote them; rely on premium pricing; and are expected to cover their costs within a few years of being approved. However, the rising threshold of innovation will make it increasingly diffi cult for such drugs to attain blockbuster status in the future.
The development of high density productsA growing number of what we have called “high density” products are also coming onto the market. These have a different therapeutic profi le. They are typically second-line treatments; designed for a clinically defi ned population; and administered by specialists. But like conventional blockbusters, they come in a single, one-size-fi ts-all form and (with the exception of oncology drugs) generally treat a chronic condition – albeit that they sometimes modify the disease as distinct from just alleviating the symptoms.

Pharma 2010: The threshold of innovation IBM Business Consulting Services20
High density products share some of the economic characteristics of conventional block-busters. They are, for example, expensive and time-consuming to develop. That said, they usually face less intense competition and have lower sales costs because they are marketed to specialists rather than general practitioners and consumers. There is also some evidence to suggest that high density products that modify the progression of a disease now have the potential to generate greater revenues than traditional drugs.
Our analysis of the top 200 prescription medicines, measured by revenues in 2001, shows that 31 percent of them are high density products. They are predominantly oncology drugs but they also include Remicade and Enbrel, both pioneering treatments for rheumatoid arthritis; Neupogen, which maintains the white blood cell count in patients undergoing chemotherapy; Procrit, which boosts the production of red cells in patients suffering from anaemia; and Risperdal, the fi rst truly new anti-psychotic in 20 years.
The beauty of biologicsIf the number of high density products is increasing, so is the number of biologi-cally based drugs (biologics) – large molecules such as soluble proteins, monoclonal antibodies and antibody fragments, as well as smaller molecules such as antisense RNA. IMS Health reports that biotechnology products (predominantly biologics) accounted for more than 35 percent of the 37 NASs that were launched in 2001.42
This is no accident. The biological approach rests on a fundamental understanding of disease. In addition, biologics possess several advantages over chemical entities. They are increasingly derived from human proteins or antibodies (as opposed to those of mice, pigs or other animals) and are therefore less likely to trigger an immune response; it is generally much easier to predict how they will be distributed, metabolized and eliminated; and they typically have much faster development cycles. Indeed, research from CMR International shows that biologics have a four-fold greater chance than chemical entities of making it to market from the point at which they fi rst get tested in man.43
Further evidence of the growing importance of biologics comes from the fact that the FDA now plans to bring the review of such products under the auspices of its main drug division, the Center for Drug Evaluation and Research (CDER). The biologics division has attracted criticism for being slower than CDER. In September 2002, the agency responded to these complaints by announcing that it would consolidate oversight of chemical and biological drugs to improve the effi ciency and consistency of the process.44

Pharma 2010: The threshold of innovation IBM Business Consulting Services21
But though biologics offer considerable promise, that promise has so far been limited and the fault lies mainly within the industry itself. This is not to say that all diseases will be amenable to treatment with biologics. However, Pharma lacks experience in dealing with the problems of discovering, developing and manufacturing large molecules. It is also wary of making drugs that must generally be delivered by injection – believing they will generate lower revenues than medicines that can be taken orally – and has therefore tended to steer clear of such research opportunities. The new challenge is thus to formulate biologics so that they can be delivered in more acceptable forms.
The molecular mazeThe new molecular sciences will enable the industry to change its approach, but they will not do so in the way it originally hoped. The sequencing of the human genome has revealed about 25,000-50,000 new targets, although not all of them are suitable for treating with drugs. And, as scientists readily acknowledge, very little is known about these targets precisely because they are so new. The average number of academic citations per target fell from about 100 in 1990 to almost none in 2002, refl ecting the degree to which the industry has been moving into uncharted territory.
Moreover, the scale of the challenge has proved much greater than anyone initially envisaged, with the dawning realization that it is proteins and their interactions – rather than the mapping of our genes – which hold the key to understanding and treating disease. The human body may contain as many as 500,000 different proteins, so the number of points at which pharmaceutical intervention is possible could increase by a factor of 1,000.
Fortunately, a number of technologies are now emerging that should eventually enable Pharma both to come to grips with genomics and proteomics, and to understand biological systems as coherent entities. For example, the U.S. National Institutes of Health (NIH) has launched the Protein Structure Initiative, which aims to identify 10,000 protein structures over the next decade. And the supercomputer Blue Gene, which should be built by 2005, will be 30 times faster than the fastest machine available today. This enormous computing power will help biologists explore how proteins fold themselves up into their distinctive shapes, and drugs can be more easily directed at particular proteins when their characteristics are known. It will also be used to improve homology searching and pattern recognition, and in systems biology – the study of living systems, using biological models that simulate the behavior of organs and cell tissues.
Pharma 2010: The threshold of innovation IBM Business Consulting Services22
Two other major classes of molecule – carbohydrates (simple and complex sugars) and lipids (fats) – likewise play a big part in the way the body works. In fact, sugars perform multiple jobs: they modify many proteins and fats on cell surfaces; they also affect cell-to-cell communication, the operation of the immune system, the impact of certain infec-tious agents, and the progression of cancer. Recognition of the importance of sugars has spurred a growing number of academics and biotech companies to look into this area more closely.45
In short, exploration into fi elds such as genomics, proteomics and metabonomics will provide Pharma with plenty of new biological targets, but researchers will know very little about which targets are relevant or which diseases they are associated with. So, unless the industry makes radical changes in the way it conducts R&D, the direct benefi ts of the new molecular sciences are likely to be fairly restricted in the short to medium term. They will certainly not facilitate the development of a stream of new drugs.
A disease-centric approachNevertheless, they will effect two major changes. First, they will put an end to the current one-size-fi ts-all approach. It is widely recognized that most drugs only work for between 40 percent and 60 percent of the patients for whom they are prescribed, and that drugs which work well for some patients cause intolerable side effects in others. This is sometimes because drugs act in unexpected ways. But it is often because Pharma’s understanding of many common diseases is so limited that it can only defi ne them in very simplistic terms – and patients who do not respond, or do not respond well, to a particular drug actually suffer from a different disease.
However, thanks to genomics, researchers are gradually acquiring a much better grasp of the factors involved in a particular disease state, including its severity, how it progresses, and why particular individuals are susceptible in the fi rst place. They are also beginning to devise genetic tests that will predict which drugs would work best on which patients, and which would not. So, for example, GSK is working on a test for Ziagen – one of the components in Trizivir, its three-drug treatment for HIV, which some 20 percent of patients cannot take because they have an allergic reaction to Ziagen.
The ability to segment patients on the basis of their probable responses to a particular drug will inevitably fragment the market and end the monolithic approach that has characterized past blockbusters. But it could also give some products a new lease of life; drugs that cause serious side effects in a small percentage of the patient population could then be administered to the “right” patients without causing any harm (see box on One size doesn’t fi t all).

Pharma 2010: The threshold of innovation IBM Business Consulting Services23
One size doesn’t fi t all
Under the current “one-size-fi ts-all” approach, patients are treated in the same manner, even
though complex biomolecular and genetic variations in individuals, as well as the different environ-
mental infl uences to which they are exposed, mean that many drugs do not work for a signifi cant
percentage of the patient population. Beta-blockers, for example, do not work for between 15
percent and 35 percent of the patients for whom they are prescribed; tricyclic antidepressants
do not work for between 20 percent and 50 percent; and interferons do not work for between 30
percent and 70 percent.
Some drugs also cause serious side effects in some people (without necessarily doing them any
good). In fact, an article recently published in the Journal of the American Medical Association
suggests that more than half the 27 drugs frequently cited for causing adverse reactions are linked
to at least one enzyme with a variant allele (one of two or more forms of a gene that may occur
alternatively at a given site on a chromosome) that is known to cause poor metabolism.48 Moreover,
most medicines for adult patients (with the exception of oncology products) are prescribed without
regard for variations in body size, even though there is a roughly three-fold difference between the
biggest and smallest adults.
These differences in genetic make-up and body size cause numerous problems. Research
conducted at University College, London, shows that every year more than 800,000 patients using
the UK National Health Service (NHS) experience adverse drug reactions (ADRs). As a result, about
68,000 patients die and 50,000 are permanently disabled.49 Similarly, one U.S. study estimates
that in 1994 over two million patients were admitted to hospital because they had been prescribed
inappropriate drugs or had experienced adverse effects from drugs that had been correctly
prescribed. Over 100,000 died as a result – suggesting that ADRs are between the fourth and sixth
leading cause of death in the U.S.50
The human cost of such injuries is clearly considerable, but so is the economic cost. Three U.S.
studies, conducted between 1995 and 1997, put the bill for medication-related problems in nursing
homes, hospitals and the community at almost US$85bn.51 But the number of adverse events
is rising, as drugs get steadily more powerful and as aging Baby Boomers take more medicines
– especially drugs for long-term use on chronic conditions. Indeed, it is widely thought that for
every dollar the U.S. spends on drugs, it spends another correcting the problems caused by drugs.
Given that retail expenditure on prescription drugs reached US$154.5bn in 2001, this sum would
be enough to cover the cost of treating every patient with cardiovascular disease in the country.52
Pharma 2010: The threshold of innovation IBM Business Consulting Services24
Genomics and proteomics will not only enable the industry to develop tests that distin-guish between patients with different genetic features, though; they will enable Pharma to defi ne diseases much more accurately and make commercially viable drugs for smaller patient populations. Researchers will eventually be able to separate diseases that currently get lumped together as if they were the same disease, and treat them as different diseases within a particular disease family (or collection of related diseases).
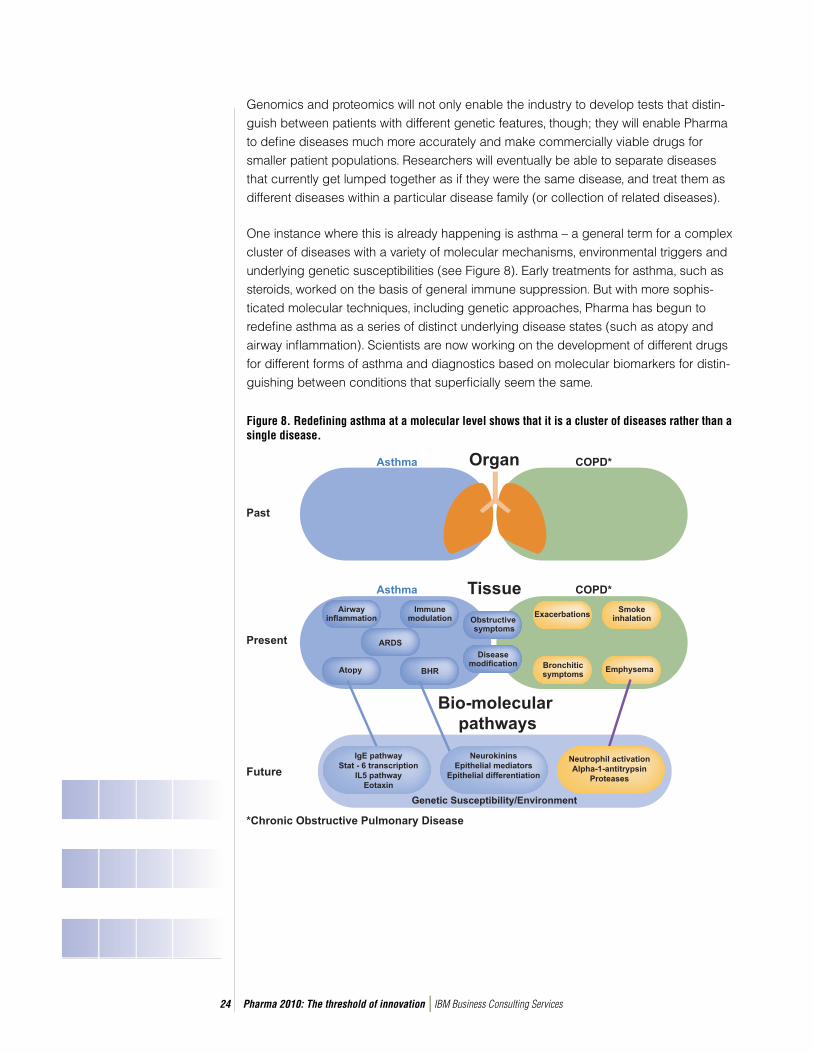
One instance where this is already happening is asthma – a general term for a complex cluster of diseases with a variety of molecular mechanisms, environmental triggers and underlying genetic susceptibilities (see Figure 8). Early treatments for asthma, such as steroids, worked on the basis of general immune suppression. But with more sophis-ticated molecular techniques, including genetic approaches, Pharma has begun to redefi ne asthma as a series of distinct underlying disease states (such as atopy and airway infl ammation). Scientists are now working on the development of different drugs for different forms of asthma and diagnostics based on molecular biomarkers for distin-guishing between conditions that superfi cially seem the same.
Figure 8. Redefining asthma at a molecular level shows that it is a cluster of diseases rather than a single disease.
Pharma 2010: The threshold of innovation IBM Business Consulting Services25
A similar trend is evident in the fi eld of cancer. The Winship Cancer Institute at Emory University has joined forces with NuTec Sciences and IBM to develop a system that will segment breast, prostate, lung and other forms of cancer into sub-types. The system will pinpoint the genes and gene combinations that cause cancer in individual patients, and enable doctors to treat such patients according to their specifi c genetic make-up. As Jonathan Peck, Vice President of the U.S. Institute for Alternative Futures, notes: “We will probably go from the roughly 200 forms of cancer that are known today to 2,000 recognized forms of the disease by 2010. Pathologists have historically defi ned cancers according to where they are located, but that scheme is already being challenged by the emerging molecular taxonomy.”46
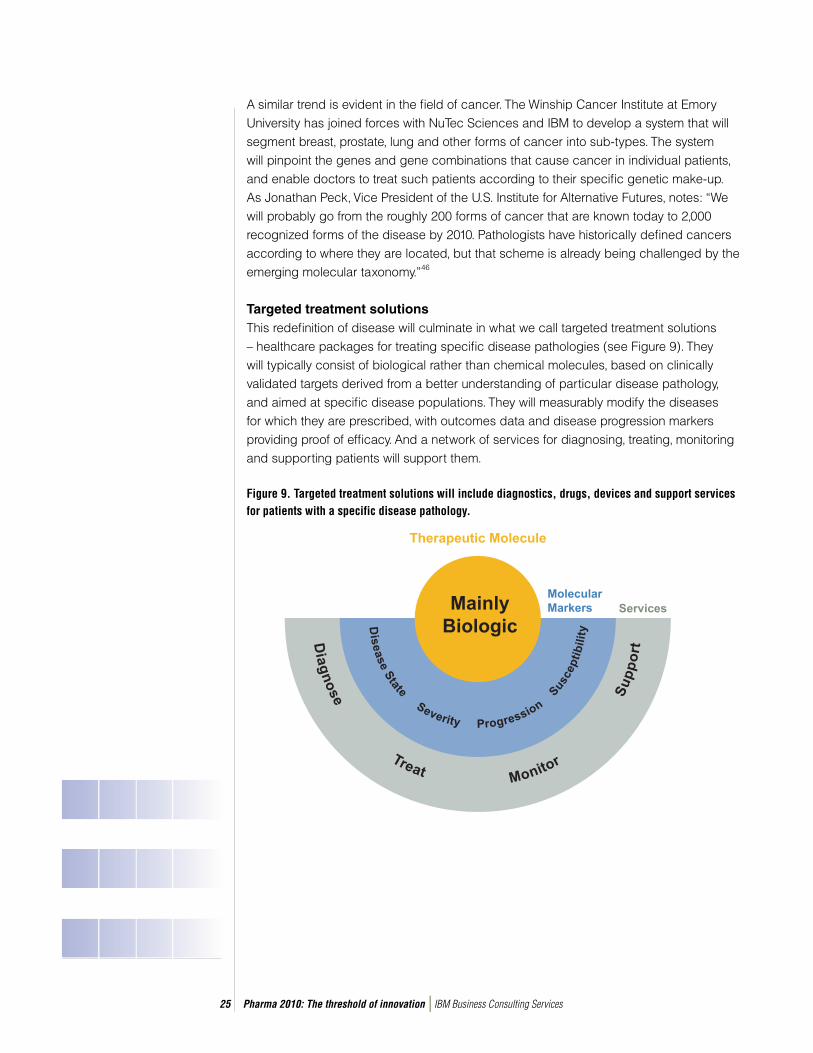
Targeted treatment solutions This redefi nition of disease will culminate in what we call targeted treatment solutions – healthcare packages for treating specifi c disease pathologies (see Figure 9). They will typically consist of biological rather than chemical molecules, based on clinically validated targets derived from a better understanding of particular disease pathology, and aimed at specifi c disease populations. They will measurably modify the diseases for which they are prescribed, with outcomes data and disease progression markers providing proof of effi cacy. And a network of services for diagnosing, treating, monitoring and supporting patients will support them.
Figure 9. Targeted treatment solutions will include diagnostics, drugs, devices and support services for patients with a specific disease pathology.
Pharma 2010: The threshold of innovation IBM Business Consulting Services26
Advances in web-based and mobile technologies will play a big part in facilitating the development of these wrap around services and enabling the industry to generate additional revenues. They will also allow individual pharmaceutical companies to generate more intellectual capital and get closer to patients, which will in turn help them to establish a dominant position in the treatment of particular disease pathologies.
Similarly, new forms of data management will help the industry to handle the vast quantities of outcomes data it will need to support the development of targeted treatment solutions. One such technique is “database federation” – where users can access data sources independently, in their original format, as well as searching all the opera-tional databases in the system. The UK Department of Health has just commissioned a massive distributed computing grid for the screening and diagnosis of breast cancer, which operates on this basis. eDiamond, as it is called, will be used to build a massive digital “photo album” of mammogram scans, which medical experts throughout the country will then be able to search, no matter where or how they were created.
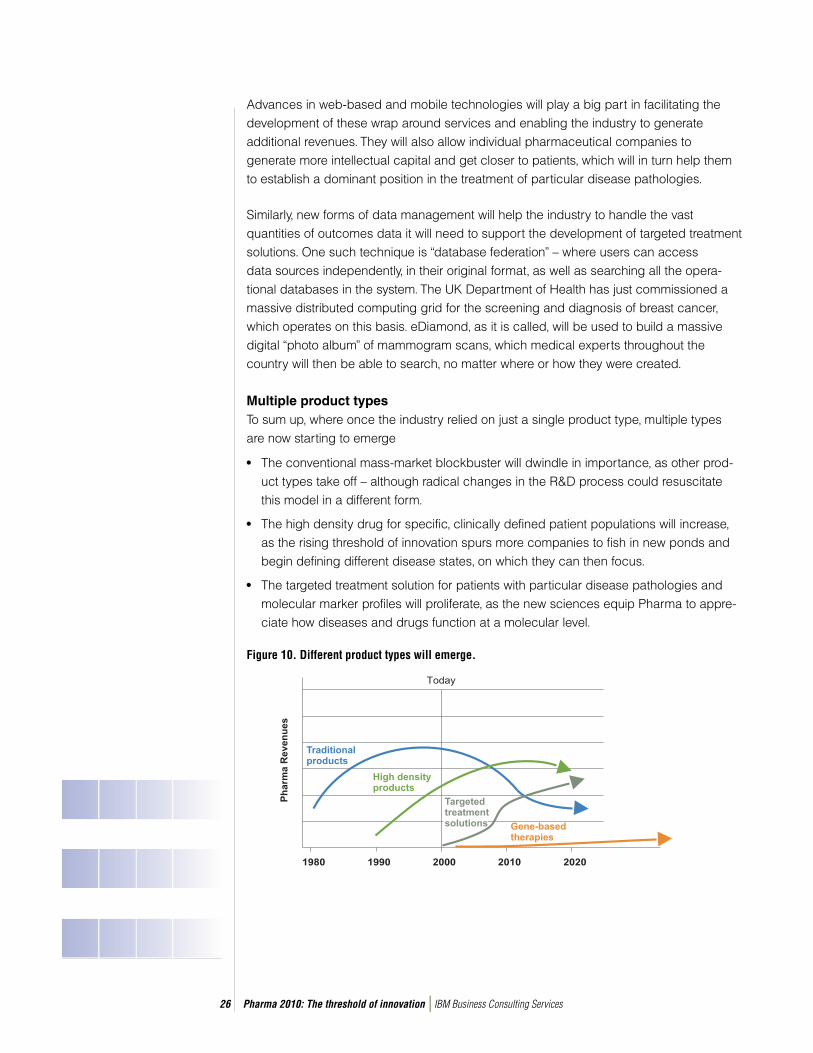
Multiple product typesTo sum up, where once the industry relied on just a single product type, multiple types are now starting to emerge
• The conventional mass-market blockbuster will dwindle in importance, as other prod-uct types take off – although radical changes in the R&D process could resuscitate this model in a different form.
• The high density drug for specific, clinically defined patient populations will increase, as the rising threshold of innovation spurs more companies to fish in new ponds and begin defining different disease states, on which they can then focus.
• The targeted treatment solution for patients with particular disease pathologies and molecular marker profiles will proliferate, as the new sciences equip Pharma to appre-ciate how diseases and drugs function at a molecular level.
Figure 10. Different product types will emerge.

Pharma 2010: The threshold of innovation IBM Business Consulting Services27
We believe it is this last product type that offers the industry the greatest opportunities to improve the quality of healthcare, generate new revenues for the long term and protect its intellectual capital (See Figure 10). It is already clear that concentrating on a few intensely competitive therapeutic areas for which there are already many good drugs on the market will produce diminishing returns. It is equally clear that making high density drugs for therapeutic areas which are clearly defi ned but poorly treated may well produce some additional growth. However, the development of targeted treatment solutions for specifi c disease states will create new market spaces. It will also benefi t patients, healthcare professionals and payers, and the industry alike.
It will ultimately give patients comprehensive therapies that work for them – diagnostics for evaluating their susceptibility to a particular disease; prophylactics for those at risk; molecular markers for defi ning the disease state from which they suffer, and for measuring its severity and progression; and monitoring mechanisms that help them to comply with their individual medical regimens. It will also give doctors the means with which to provide better medical care and healthcare payers better value for money – by enabling them to get the right drugs to the right patients and eliminating the cost of treating people with adverse drug reactions.
Similarly, it will enable Pharma to charge premium prices for treatments that demon-strably work for particular disease states, even though the target market may be smaller; to add value with the provision of diagnostics, biomarkers and monitoring devices; and to increase drug utilization with better compliance and persistence (see box on Persis-tence pays off). In addition, the industry will have numerous opportunities to exploit the same research, because it can build on its expertise in one disease state by moving onto other disease states in the same disease family, and developing entire treatment packages as distinct from single drugs.
It may also help Pharma to stave off a danger that is just beginning to emerge. In August 2002, a German bill on product liability reversed the burden of proof. Under the old rules, a patient had to prove that a drug had harmed him; under the new rules, the pharma-ceutical company must prove that its drug did not cause the injury.47 So any company that wants to defend itself from such allegations will need to be able to show that any treatment it has developed is appropriate for the particular disease state and patient for whom it has been prescribed, or that it was incorrectly used.

Pharma 2010: The threshold of innovation IBM Business Consulting Services28
Persistence pays off
Many patients do not stick to their treatment regimen, even when they risk becoming seriously ill. In a
study of Canadian patients with hypertension, 82 percent of those who had been diagnosed before the
program began were still taking their medicine 4.5 years afterwards. But only 46 percent of those who had
been newly diagnosed at the start of the program were still doing so.53 Persistence levels in another study
of patients with high cholesterol were even lower. Only 33 percent of patients were still using a statin at the
end of 12 months, and only 13 percent were still doing so at the end of five years.54
Predictably, persistence and compliance rates are lower for preventative medications than for drugs for acute
symptomatic illnesses. However, outcomes data on patients with adult hypertension are similar in all Western
countries, despite wide variations in the financing of medical care and the reimbursement of prescription
drugs. So the issue is not simply money. Fear of drugs, denial of illness, confusion, forgetfulness and the
belief that a disease has been cured when the symptoms fade are also contributing factors.55
Yet failure to persist with a medication or comply with the conditions under which it should be taken
increases the risk to individual patients and the overall cost to healthcare providers in terms of
hospitalization and surgery. A landmark study conducted in 1994 shows, for example, that simvastatin
(marketed under the brand name Zocor) can reduce the risk of a fatal heart attack by 40 percent, and the
risk of a non-fatal heart attack by 33 percent, over a period of six years.56
Furthermore, short-term withdrawal of some drugs produces a “rebound” phenomenon that actually leaves
patients more vulnerable. In one piece of research, patients with stable coronary heart disease experienced
a three-fold increase in thrombosis after treatment with simvastatin was stopped and replaced with lower
doses of fluvastatin.57 Another more recent study shows that giving people statins before a major cardiac
event can reduce the risk of a heart attack by as much as half, but withdrawing statin therapy after the onset
of symptoms completely abrogates the beneficial effects.58
Greater persistence in taking drugs that treat chronic conditions would improve the health of many patients,
then, but it also represents a huge opportunity for Pharma. Over 85 percent of patients enrolled in the
big, multi-year trials that have been used to test statins persisted with their treatment for the full five-year
duration. So, if persistence levels in everyday use of such drugs equated with those in clinical trials, and
prices and patient numbers remained the same, the revenues they earned would be roughly 2.7 times
higher. (If 90 percent of patients take a statin for five years, persistence is 2.7 times greater than it is with
a median persistence of 25 weeks, with only 33 percent patients persisting for 12 months, and only 13
percent persisting for five years.) To put it another way, sales of Zocor would be US$18bn a year instead of
US$6.7bn.
In fact, it is far more likely that there would be some sort of trade-off between volume and pricing, not
least because few (if any) countries could afford to pick up such a sudden surge in the drugs bill. But with
a two- or three-fold increase in demand for medicines that treat such conditions, Pharma would certainly
not suffer. As John Urquhart, Professor of Pharmacoepidemiology at Maastricht University and Professor
of Biopharmaceutical Sciences, at UCSF, San Francisco, points out: “Finding a cost-effective solution to the
persistence problem with drugs for chronic use has enormous economic potential. It is comparable with
tripling the pipeline for new drugs.”59

Pharma 2010: The threshold of innovation IBM Business Consulting Services29
RecommendationsAny pharmaceutical company that wants to capitalize on these advances in the under-standing of disease will need to alter its entire scientifi c and commercial model. It will have to start by acquiring an in-depth knowledge of particular diseases. It will also have to use modeling, simulation and the molecular sciences to a much greater extent in the early stages of research. It will have to call on the most sophisticated web-based technol-ogies and data management systems to support both discovery and development. It will have to collaborate much more closely with the regulators, healthcare payers, physicians and patients. And it will have to ensure that it has the requisite marketing, sales and manufacturing infrastructure to support multiple product types.
These are huge changes, but they have the potential to cut attrition rates, cycle times and costs dramatically. Indeed, they could collectively transform the economic founda-tions of drug discovery and development so greatly that they not only enable the industry to make very profi table targeted treatment solutions for affl uent patients in the developed world, but also to make mass-market blockbusters for dealing with some of the big infec-tious diseases that beset people in the less developed world.
Chapter 4: A disease-driven approach to drug discovery
Flipping the telescope around and looking at pharmaceutical R&D in terms of redefi ning diseases much more precisely not only provides opportunities for developing different treatments for different pathologies, it also provides opportunities for cracking medical problems that have previously proved intractable. One such instance is rheumatoid arthritis.
Reverse viewIn the mid-1970s, several scientists identifi ed a cytokine called tumor necrosis factor (TNF). After extensive additional research, they deduced that it must play a signifi cant role in the pathology of rheumatoid arthritis, since they could see that people suffering from the disease have higher than normal levels of TNF in their synovial fl uid. But no company could develop a chemical compound that would either reduce TNF levels or bind to the key receptor in order to block the action of TNF.
Concluding that TNF was “undruggable” – a target that is not amenable to intervention with a small molecule – various companies concentrated on developing products aimed at targets in different biomolecular pathways that would reduce the infl ammation caused by rheumatoid arthritis and relieve the pain. In 1999, these efforts culminated in the launch of the highly successful Cox-2 inhibitors Celebrex and Vioxx.

Pharma 2010: The threshold of innovation IBM Business Consulting Services30
In the early 1990s, however, scientists at Immunex decided to take a different approach. They focused on the receptor for TNF alpha, which is present on certain cell types in the synovial membrane, peripheral blood and synovial fl uid, and began thinking about how to “mop up” the excess TNF that is produced in patients with rheumatoid arthritis, using large molecules rather than small ones.
The result was Enbrel, a human recombinant soluble TNF receptor which supplements the soluble TNF receptors in the human body, capturing TNF molecules before they have a chance to attach to the immune cells and trigger infl ammation. By interrupting the infl ammation process, Enbrel simultaneously reduces the short-term symptoms of rheumatoid arthritis and inhibits the progressive long-term damage it wreaks on the joints. Whereas Celebrex and Vioxx merely alleviate the symptoms of rheumatoid arthritis, Enbrel impedes the course of the disease.
The moral is clear. Concentrating on the discovery and development of chemical entities restricts the way in which Pharma companies defi ne and treat disease. Reversing the historical emphasis and concentrating on the disease itself paves the way for new forms of treatment that are much more innovative, accurate and effi cacious – the very criteria for which people are willing to pay more (see box on Right on target).
The death knell for traditional drug discoveryIf Pharma is to alter its focus, though, it will have to transform the way in which it discovers drugs. The Human Genome Project has ensured that an unprec-edented number of potential molecular targets are now in the public domain. But the industry can no longer rely on academic research to glean additional information on those targets, because there are simply too many targets and there is little or no literature on the vast majority of them.
Right on target
Herceptin and Gleevec both work by targeting the genetic
abnormality that causes the cancers they are designed to treat,
rather than functioning as general chemotherapeutic agents. They
can thus fairly be called Pharma’s fi rst targeted treatments – and
the FDA approved both in record time.
Herceptin was developed for the 25-30 percent of women who
contract breast cancer as a result of over-expression in the
HER2 receptor: a diagnostic test to identify patients who show
an abnormally large amount of the HER2 protein was developed
alongside the drug itself. The treatment works so well in such
patients that it commands a much higher price than other
therapies. The average wholesale price for a 440mg vial of
Herceptin is US$2,447 – and the cost of treatment ranges from
US$26,000 to US$81,000 a year, depending on dosage. This
compares with US$1,050 a year for a traditional oral oncology
drug like tamoxifen and US$14,000 a year for surgery or other
invasive treatments. In 1999, its fi rst full year on the U.S. market,
Herceptin generated sales of US$188m. By 2001, sales had nearly
doubled to US$347m – more than the average annual revenue
from a drug that targets the entire population. And in 2003 sales
reached US$425m.60
Gleevec was developed for patients with chronic myeloid
leukemia (CML), which is caused by a genetic defect that arises
from the “translocation” of DNA between chromosomes 9 and
22. When these genes fuse, they produce an abnormal protein
that accelerates cell growth and division. Conventional treatments
for CML include interferon therapy and bone marrow transplants,
but many patients do not respond well; the fi ve-year survival rate
for CML is just 32 percent. Gleevec should improve the odds
for patients in the early stages of the disease quite signifi cantly.
Launched in May 2001, it is the fi rst of a new class of anti-
proliferative agents called signal transduction inhibitors, which
interfere with the pathways that signal the growth of tumor cells.
Gleevec, like Herceptin, commands a premium price. It costs
a hefty US$30,000 a year – nearly three times the cost of
Interferon-alpha, which was previously the standard therapy
for CML. Even so, it is very much cheaper than a bone marrow
transplant. Recognizing the burden this represents for many
patients, Novartis has also priced the drug in an unprecedented
manner, with a sliding scale of charges based on what individual
patients can afford to pay.
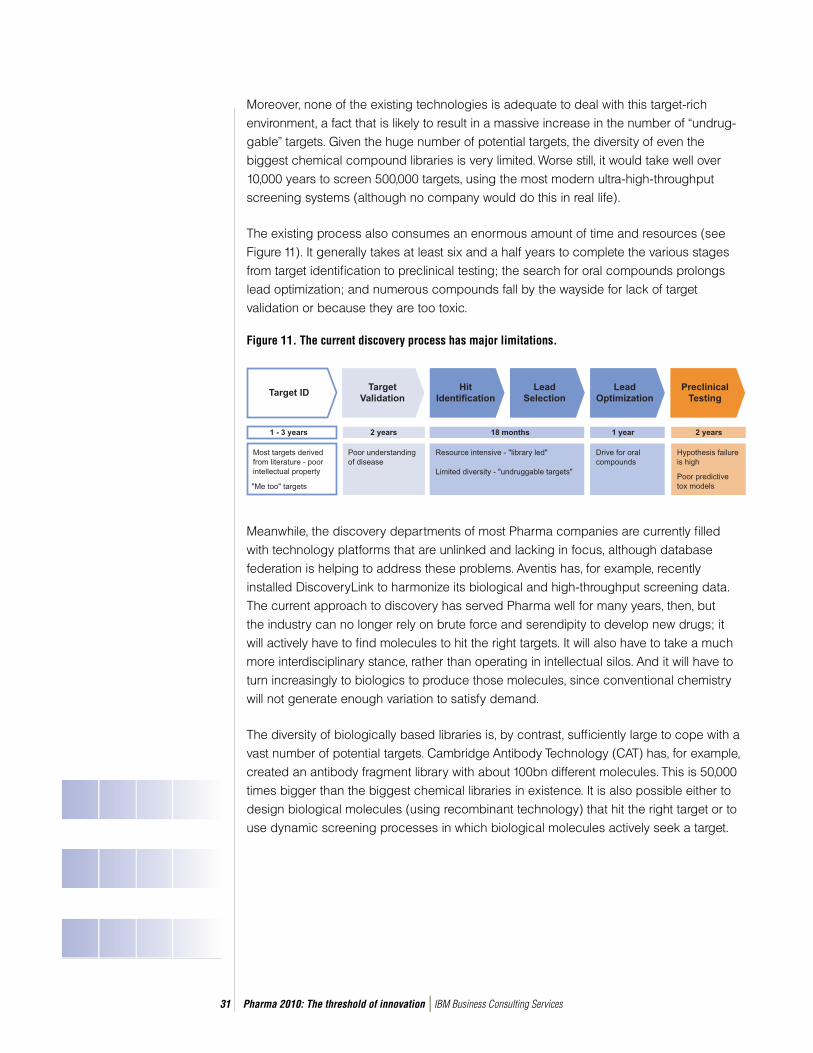
Pharma 2010: The threshold of innovation IBM Business Consulting Services31
Moreover, none of the existing technologies is adequate to deal with this target-rich environment, a fact that is likely to result in a massive increase in the number of “undrug-gable” targets. Given the huge number of potential targets, the diversity of even the biggest chemical compound libraries is very limited. Worse still, it would take well over 10,000 years to screen 500,000 targets, using the most modern ultra-high-throughput screening systems (although no company would do this in real life).
The existing process also consumes an enormous amount of time and resources (see Figure 11). It generally takes at least six and a half years to complete the various stages from target identifi cation to preclinical testing; the search for oral compounds prolongs lead optimization; and numerous compounds fall by the wayside for lack of target validation or because they are too toxic.
Figure 11. The current discovery process has major limitations.
Meanwhile, the discovery departments of most Pharma companies are currently fi lled with technology platforms that are unlinked and lacking in focus, although database federation is helping to address these problems. Aventis has, for example, recently installed DiscoveryLink to harmonize its biological and high-throughput screening data.The current approach to discovery has served Pharma well for many years, then, but the industry can no longer rely on brute force and serendipity to develop new drugs; it will actively have to fi nd molecules to hit the right targets. It will also have to take a much more interdisciplinary stance, rather than operating in intellectual silos. And it will have to turn increasingly to biologics to produce those molecules, since conventional chemistry will not generate enough variation to satisfy demand.
The diversity of biologically based libraries is, by contrast, suffi ciently large to cope with a vast number of potential targets. Cambridge Antibody Technology (CAT) has, for example, created an antibody fragment library with about 100bn different molecules. This is 50,000 times bigger than the biggest chemical libraries in existence. It is also possible either to design biological molecules (using recombinant technology) that hit the right target or to use dynamic screening processes in which biological molecules actively seek a target.
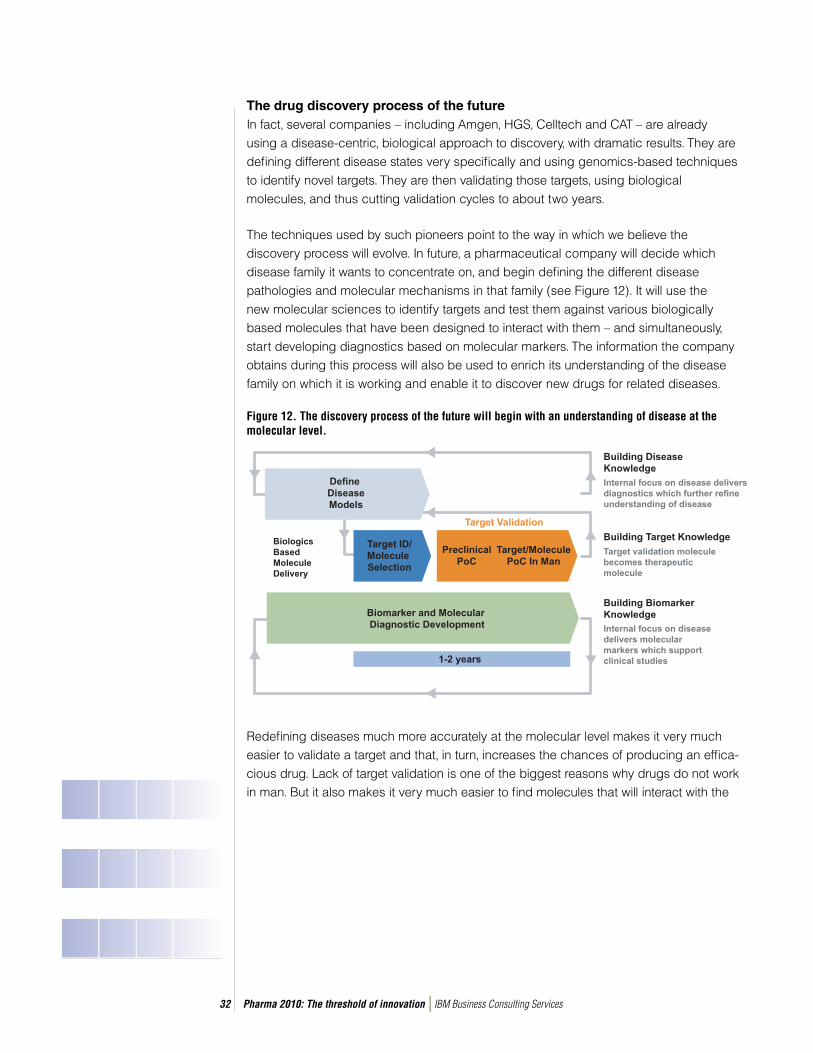
Pharma 2010: The threshold of innovation IBM Business Consulting Services32
The drug discovery process of the futureIn fact, several companies – including Amgen, HGS, Celltech and CAT – are already using a disease-centric, biological approach to discovery, with dramatic results. They are defi ning different disease states very specifi cally and using genomics-based techniques to identify novel targets. They are then validating those targets, using biological molecules, and thus cutting validation cycles to about two years.
The techniques used by such pioneers point to the way in which we believe the discovery process will evolve. In future, a pharmaceutical company will decide which disease family it wants to concentrate on, and begin defi ning the different disease pathologies and molecular mechanisms in that family (see Figure 12). It will use the new molecular sciences to identify targets and test them against various biologically based molecules that have been designed to interact with them – and simultaneously, start developing diagnostics based on molecular markers. The information the company obtains during this process will also be used to enrich its understanding of the disease family on which it is working and enable it to discover new drugs for related diseases.
Figure 12. The discovery process of the future will begin with an understanding of disease at the molecular level.
Redefi ning diseases much more accurately at the molecular level makes it very much easier to validate a target and that, in turn, increases the chances of producing an effi ca-cious drug. Lack of target validation is one of the biggest reasons why drugs do not work in man. But it also makes it very much easier to fi nd molecules that will interact with the
Pharma 2010: The threshold of innovation IBM Business Consulting Services33
target in the fi rst place. Moreover, since many of those molecules will be biological rather than chemical, many of them will have a very much lower toxic load and thus reduce the danger of producing a drug that fails because it produces undesirable side effects.
Of course the transition from the old to the new model will take some time and for the biggest companies there will probably be an intermediate stage in which they use biologically based molecules to conduct faster proof of concept (PoC) studies in man and thus accelerate target validation. Once a company has validated a target, it can feed that target into the traditional drug discovery process, safe in the knowledge that attrition due to lack of effi cacy will be much lower.
However, the ultimate step is to adopt a totally new approach, and that has two wider implications. First, the scientifi c community’s grasp of how specifi c diseases work originates mainly in academia; Pharma only comes on the scene when that information is already in the public domain. But when the disease itself is the focus of attention, a clear understanding of that disease is what positions a company to add value – not possession of the biggest compound library on the block.
Second, the industry will need to communicate with the regulators at a much earlier stage in the R&D process. At present, the fi rst formal contact with the regulator occurs when a company fi les an investigational new drug application before starting Phase I trials. But with earlier use of proof of concept studies in man for both target and molecule validation, it will be necessary to consult the regulators long before this point.
Chapter 5: The transformation of drug development
The current paradigm of clinical development, with its reliance on double-blinded, randomized control tests, was devised in the wake of the Thalidomide tragedy. But it has hardly altered since then – and, if Pharma is to make the transition from mass-market drugs to targeted treatment solutions, the development process will need to undergo every bit as big a transformation as discovery.
Big dollars, few drugsThe existing approach is very expensive and extremely ineffi cient (see Figure 13). Despite spending almost US$5bn a year on R&D, for example, Pfi zer expects to launch only two products per annum from in-house research. As John Niblack, former president of global R&D, said in a recent newspaper interview, only one of the 12 molecules that Pfi zer classifi es as its best bets – those drugs that have made it to the verge of
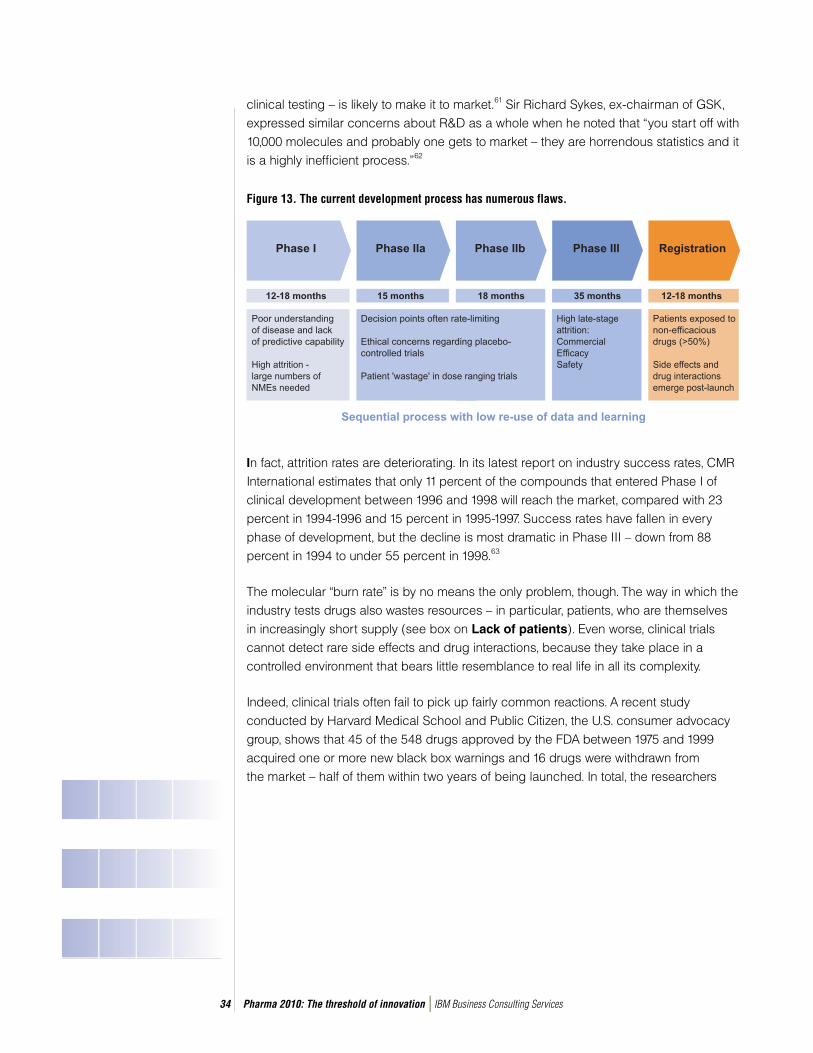
Pharma 2010: The threshold of innovation IBM Business Consulting Services34
clinical testing – is likely to make it to market.61 Sir Richard Sykes, ex-chairman of GSK, expressed similar concerns about R&D as a whole when he noted that “you start off with 10,000 molecules and probably one gets to market – they are horrendous statistics and it is a highly ineffi cient process.”62
Figure 13. The current development process has numerous flaws.
In fact, attrition rates are deteriorating. In its latest report on industry success rates, CMR International estimates that only 11 percent of the compounds that entered Phase I of clinical development between 1996 and 1998 will reach the market, compared with 23 percent in 1994-1996 and 15 percent in 1995-1997. Success rates have fallen in every phase of development, but the decline is most dramatic in Phase III – down from 88 percent in 1994 to under 55 percent in 1998.63
The molecular “burn rate” is by no means the only problem, though. The way in which the industry tests drugs also wastes resources – in particular, patients, who are themselves in increasingly short supply (see box on Lack of patients). Even worse, clinical trials cannot detect rare side effects and drug interactions, because they take place in a controlled environment that bears little resemblance to real life in all its complexity.
Indeed, clinical trials often fail to pick up fairly common reactions. A recent study conducted by Harvard Medical School and Public Citizen, the U.S. consumer advocacy group, shows that 45 of the 548 drugs approved by the FDA between 1975 and 1999 acquired one or more new black box warnings and 16 drugs were withdrawn from the market – half of them within two years of being launched. In total, the researchers

Pharma 2010: The threshold of innovation IBM Business Consulting Services35
estimated that 20 percent of all new drugs are eventually found to have serious side effects which are unknown or undisclosed at the time of their approval.64
Moreover, even though most of the industry leaders have experimented with electronic data capture, about 95 percent of clinical trials are still paper-based – and use multiple systems for inputting case reports, producing investigator visit reports and management reports, and managing trial supplies and investigator payments. This inevitably wastes time and money, and increases error rates.
The development process is ineffi cient and costly, then, but it also raises a number of ethical issues. One such concern is the use of placebos. A second is the effec-tiveness of the regulations for protecting people partici-pating in clinical trials. In May 2002, two members of the U.S. House of Representatives introduced a bill to improve patient protection.65 But in even the most scrupulously organized trials, more than 50 percent of patients are still exposed to drugs that do not work for them. And though compliance is much higher than it is in everyday life, clinical trials routinely ignore dose omissions, drug holidays (where a patient does not take a drug for three days or more), and other types of deviation from the treatment guidelines specifi ed by the clinical protocol.
In short, the existing clinical development process has served man well for some 35 years, but it has numerous fl aws and is now badly in need of reform. The redefi nition of disease states will exacerbate these problems, since it will then be necessary to test new drugs on patients who have the “right” disease and genotype – and that will increase both the bottlenecks in patient recruitment and the amounts of data the industry must store, share and manage.
Lack of patients
Promising new drugs are not all that is in short supply. So are the
doctors and patients whom the industry needs to conduct clinical
trials – and this is another big factor contributing to the rise in
development costs. The American Medical Association reports that
between 1984 and 1999 the number of trial investigators in the U.S.
dropped more than 37 percent from a peak of about 23,000 to less
than 15,000, and some industry experts predict that there will be a
15 percent shortfall by 2006.70
Matters are even worse when it comes to patients. Nearly 80
percent of all trials are delayed as a result of problems in enrolling
a suffi cient number of patients, and the average delay is about 90
days.71 Yet many potential candidates never even get approached.
One recent study shows that fewer than 5 percent of U.S. cancer
patients have ever participated in an oncology trial, although 74
percent say they would consider doing so. It also suggests that
a signifi cant gulf in the perceptions of doctors and patients helps
to account for the situation. More than half the doctors who were
surveyed thought that patients did not participate in trials for fear of
being given products that had not been fully tested or because they
did not want to be treated like “guinea pigs.” However, the biggest
obstacles patients cited were the need to travel further to receive
treatment (a problem that remote monitoring will address) and
concern about receiving a placebo.72
Some companies have now begun to use more imaginative recruiting
methods. They are looking outside the traditional geographic areas;
Merck, for instance, conducts 35 percent of its trials outside the
U.S.. They are also targeting potential trial patients directly via the
Internet, advertising and public relations initiatives. And they are
actively trying to reach patients who do not generally have access to
good healthcare, such as immigrants and people on low incomes.
Nevertheless, more than half of all clinical programs are still
conducted in the U.S. – the most expensive location – even though
the International Conference on Harmonization (ICH) has produced a
consistent set of standards for conducting development in the U.S.,
Europe and Japan. This means that Pharma companies can perform
clinical trials in areas like Eastern Europe and extend the patient pool.
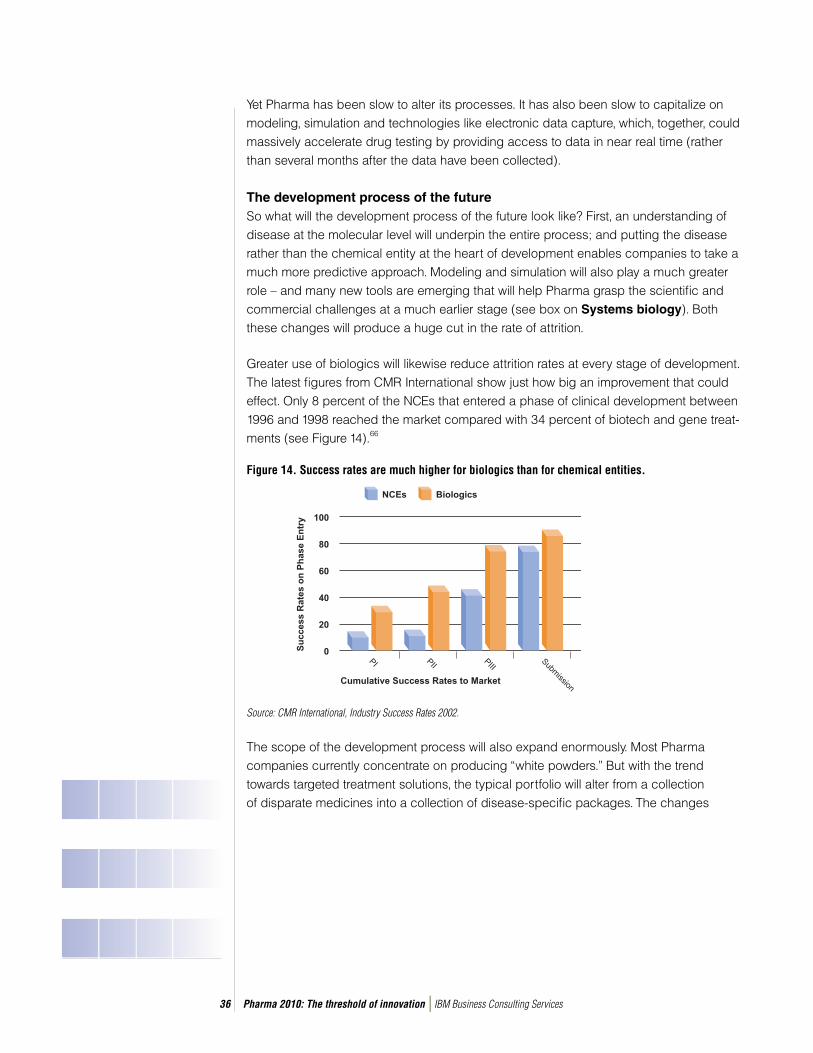
Pharma 2010: The threshold of innovation IBM Business Consulting Services36
Yet Pharma has been slow to alter its processes. It has also been slow to capitalize on modeling, simulation and technologies like electronic data capture, which, together, could massively accelerate drug testing by providing access to data in near real time (rather than several months after the data have been collected).
The development process of the future So what will the development process of the future look like? First, an understanding of disease at the molecular level will underpin the entire process; and putting the disease rather than the chemical entity at the heart of development enables companies to take a much more predictive approach. Modeling and simulation will also play a much greater role – and many new tools are emerging that will help Pharma grasp the scientifi c and commercial challenges at a much earlier stage (see box on Systems biology). Both these changes will produce a huge cut in the rate of attrition.
Greater use of biologics will likewise reduce attrition rates at every stage of development. The latest fi gures from CMR International show just how big an improvement that could effect. Only 8 percent of the NCEs that entered a phase of clinical development between 1996 and 1998 reached the market compared with 34 percent of biotech and gene treat-ments (see Figure 14).66
Figure 14. Success rates are much higher for biologics than for chemical entities.
The scope of the development process will also expand enormously. Most Pharma companies currently concentrate on producing “white powders.” But with the trend towards targeted treatment solutions, the typical portfolio will alter from a collection of disparate medicines into a collection of disease-specifi c packages. The changes
Source: CMR International, Industry Success Rates 2002.

Pharma 2010: The threshold of innovation IBM Business Consulting Services37
occurring in the marketplace will also ensure that healthcare payers, patients and the regulators play a much greater role in both shaping and deciding the value of these packages.
Moreover, the process itself will become much more iterative, as work on product A for one disease in a particular disease family gets fed into work on products B, C and so forth for other diseases in the same disease family. The labeling of each product will refl ect this progression, altering as new drugs for related diseases in the same family come on stream and a specifi c company builds a greater and greater understanding of the disease family on which it is working.
The electronic infrastructure that underpins the devel-opment process will also become very much stronger, with an integrated network of communication channels that ensures people from multiple locations and disciplines can share data. In fact, reducing the barriers to information fl ow, making the right information available to the right people when they need it, and creating what we call “closed-loop feedback,” offers enormous benefi ts in both discovery and development.
A robust electronic infrastructure makes it very much easier both to recruit trial investigators and patients, and to provide them with the support they require – as well as expanding the pool of potential candidates. It automates workfl ows and increases the number of trials any one clinical research associate can manage. And it reduces the duration of many clinical trials by providing almost immediate access to the data that are generated.
Systems biology
The new in silico technologies, which apply computer modeling
to biology and physiology, promise to deliver huge benefits. We
discussed some of these technologies in “Pharma 2005: Silicon
Rally,” but there has been considerable progress in the intervening
three years.73 One such instance is the virtual heart created by
Raimond L. Winslow, associate professor of biomedical engineering
at Johns Hopkins University, which simulates how the heart
functions both as a whole and at a sub-cellular level, using parallel
computing, imaging and interactive visual exploration.
The Physiome Project is even more ambitious in its scope; it was
launched four years ago, with the dual aim of cataloguing every
existing piece of physiological information in digital form, and
organizing the information into a hierarchy of quantitative models
that will integrate the activity of the various organs. Scientists
operating under Physiome’s auspices are working on a computer
model of the lungs and the microvasculature – the network of
blood vessels that runs throughout the human body. Meanwhile,
Dr. Masaru Tomita of Keio University in Japan has already created
a model of human red blood cells and the NIH is mapping the
complex network of signals which cells use to send messages to
each other.
Most pharmaceutical companies are still wary about the value of
whole organ models, but several industry leaders, including Novartis
and Aventis, are already testing cellular simulations to see how
useful they will prove in developing interesting drug candidates.74
More than half of the top 40 pharmaceutical companies are also
using other simulation and modeling technologies.
The value of simulation and modeling is two-fold. It can be
used both to reduce the number of clinical trials that have to be
performed on real human beings and to design better trials once
a drug is ready for testing in man. Most drug makers already have
a considerable amount of information about similar compounds
when they begin testing a particular drug candidate. They can use
that information to model suitable trials, and use what they learn
in the course of those trials to modify the design of subsequent
trials. But simulation and modeling will ultimately help to erode the
distinctions between the three traditional phases of development
and replace parts of the process altogether.
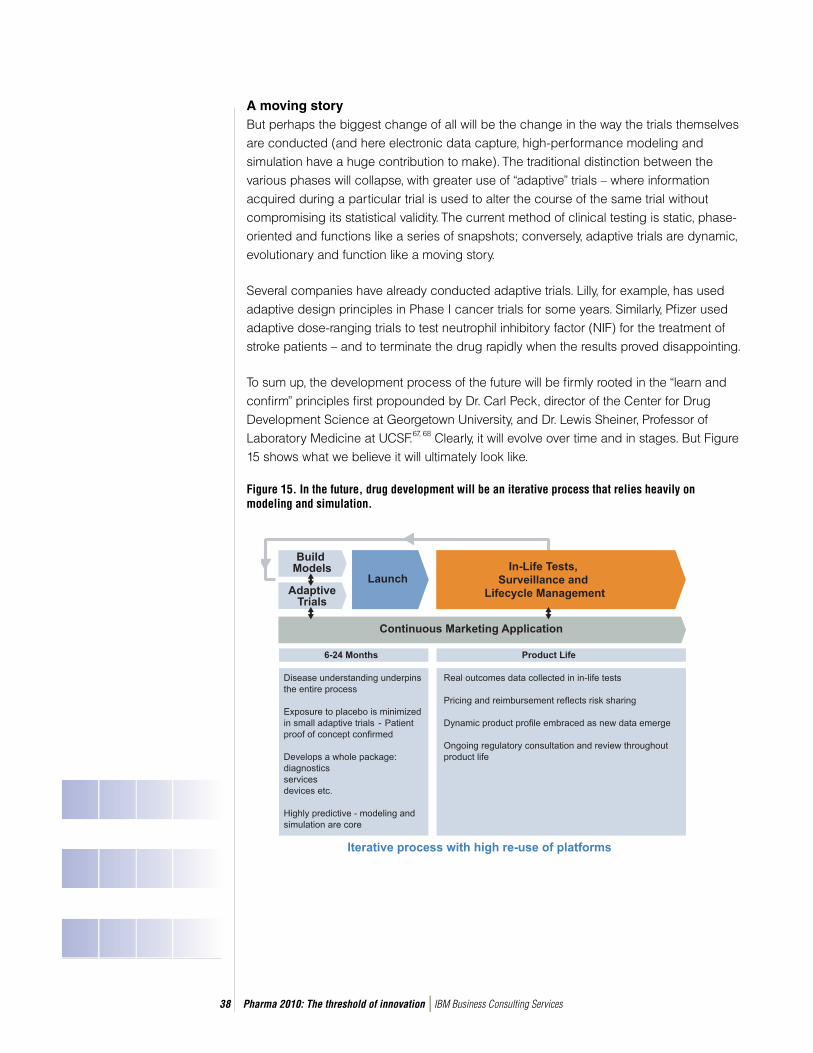
Pharma 2010: The threshold of innovation IBM Business Consulting Services38
A moving story But perhaps the biggest change of all will be the change in the way the trials themselves are conducted (and here electronic data capture, high-performance modeling and simulation have a huge contribution to make). The traditional distinction between the various phases will collapse, with greater use of “adaptive” trials – where information acquired during a particular trial is used to alter the course of the same trial without compromising its statistical validity. The current method of clinical testing is static, phase-oriented and functions like a series of snapshots; conversely, adaptive trials are dynamic, evolutionary and function like a moving story.
Several companies have already conducted adaptive trials. Lilly, for example, has used adaptive design principles in Phase I cancer trials for some years. Similarly, Pfi zer used adaptive dose-ranging trials to test neutrophil inhibitory factor (NIF) for the treatment of stroke patients – and to terminate the drug rapidly when the results proved disappointing.
To sum up, the development process of the future will be fi rmly rooted in the “learn and confi rm” principles fi rst propounded by Dr. Carl Peck, director of the Center for Drug Development Science at Georgetown University, and Dr. Lewis Sheiner, Professor of Laboratory Medicine at UCSF.67, 68 Clearly, it will evolve over time and in stages. But Figure 15 shows what we believe it will ultimately look like.
Figure 15. In the future, drug development will be an iterative process that relies heavily on modeling and simulation.
Pharma 2010: The threshold of innovation IBM Business Consulting Services39
Closer collaborationsEqually clearly, the success of this new model is contingent upon a number of changes – in particular, much greater co-operation between the various participants in the healthcare network. Companies will have to collaborate both with each other to establish common data standards and with the regulators to ensure that they are using robust simulations and monitoring outcomes data properly. They will also have to submit the data to the regulators on an ongoing basis, via rolling dossiers.
Forming such links is diffi cult and there are several practical problems, including the fact that most pharmaceutical companies use bespoke systems for compiling their drug dossiers. Few, if any, regulatory agencies could manage a constant fl ow of data in multiple formats and changing these systems would be prohibitively expensive. But one way of overcoming this dilemma is to use a trusted third party to store the data and “translate” it into a standard format, which the regulators could then access and process more easily.
Certainly, there are several advantages in forming a closer bond with the regulators. According to CMR International, a good fi fth of all NDAs fail to reach the market after fi rst submission to market.69 Rather than investing many years and a lot of money in a drug that ultimately fails to pass muster, it therefore makes sense for companies to submit data on an ongoing basis and terminate their weakest products at earlier stages of devel-opment. Moreover, the new molecular sciences will increase the complexity of the R&D process, so the industry will need more guidance from the authorities – especially when it comes to clinical development.
If Pharma is to ensure that its products really add value, it will also need to get much more feedback – both clinical and commercial – from healthcare payers, physicians and patients, and do so at a much earlier stage in the process. This may well stimulate the creation of risk-sharing arrangements such as the deal several drug makers producing beta interferons and glatiramer acetate for the treatment of multiple sclerosis struck with the UK Department of Health in February 2002.
But we believe the need for feedback from the marketplace will ultimately help to fuel a much bigger change – the use of “in-life” testing instead of Phase III trials. In-life testing will dispense with the need to expose numerous patients to placebos or dosing levels that are pharmacologically ineffective. They will also be better able to pick up rare side effects and drug interactions, thereby making the move from the rarefi ed atmosphere of the lab to real clinical practice much safer.

Pharma 2010: The threshold of innovation IBM Business Consulting Services40
Building strong relationships with healthcare payers, physicians and patients has another advantage; it may well be one of the best ways of persuading the regulatory agencies to participate in forming a new development model. Regulators tend to be quite conser-vative – for obvious, and often very good, reasons. But if there is clear support for such a model from the other parties in the healthcare network, they will listen.
It would certainly be impossible to change the development process without the co-operation of patients, physicians, payers and the regulators. However, if Pharma can collaborate with the rest of the healthcare network, everybody stands to gain. The industry will be in a better position to make safe new drugs that fulfi ll a genuine medical need at a price society can afford.
Pervasive computingPervasive computing will play a huge part in facilitating the new structure. In-life testing is currently too expensive and too risky to be practicable on a large scale, but greater bandwidth and the new network technologies that are now emerging will make it much easier and cheaper to transmit and collect biological data on a real-time basis. Mobile telecoms, radio frequency technologies and individual tracking devices will also make it much easier to collect the data outside a clinical setting.
These same technologies can be used to improve compliance and persistence rates in patients taking drugs for chronic treatments; to detect danger signs such as an irregular heart beat in patients with a history of cardiac problems, or a surge in blood sugar levels in patients with diabetes; and to individualize medical care (see Figure 16). Indeed, there is already at least one tracking mechanism so small that it can be inserted in a tablet, swallowed and used to track the course of the drug through the body.
Figure 16. Pervasive connectivity with patients will enable cost-effective in-life surveillance.
Source: Philips Medical Systems.

Pharma 2010: The threshold of innovation IBM Business Consulting Services41
Electronic medical records (EMRs) and online prescribing will also contribute to the transformation by ensuring that everyone in the healthcare provider network has a composite record for clinical and administrative purposes – and several countries are experimenting with both (see box on Dispensing with paper). Voice-recognition technologies will enable doctors to update the records quite easily, much as is already the case in some parts of the U.S., where paramedics working on accidents and emergencies can report on a patient’s condition while they are actually taking him to hospital. Together, these technologies will jointly help to ensure that patients get appropriate medical care, thereby reducing the number of people who suffer from avoidable side effects.
But EMRs will soon be vital in at least one other respect; they will make it very much easier to fi nd trial patients with a particular genetic profi le as well as a particular disease. The Mayo Clinic in the U.S. is currently participating in a pilot project to convert all its records, including genotypic data, from paper to electronic fi les. However, very few healthcare payers or providers have taken this step – and here Pharma could play an invaluable role in helping to create the necessary infrastructure and ensure the data are compiled in the most appropriate way.
Of course the use of medical records (and genotypic data, in particular) is a very sensitive subject because it increases the potential for abusing patient privacy. However, robust encryption technology that authenticates individuals through biometric characteristics such as a fi nger print or retinal scan already exist. The barriers are social and cultural rather than technological, and the advantages of creating an electronic health record system are so great that they will ultimately be overcome.
Dispensing with paper
A typical patient in a U.S. hospital has 11 medical charts
and takes 14 medicines, administered by three or more
physicians who may not even work in the same facility.
The U.S. Institute of Medicine (IoM) estimates that this
ineffi cient, paper-based system contributes enormously
to the number of medical errors that are made. The IoM
has outlined a comprehensive blueprint for creating an
electronic infrastructure to support healthcare delivery in its
much publicized report Crossing the Quality Chasm.76 This
should see IT spending in healthcare provision more than
double, to US$45bn, by 2005.
Meanwhile, the French Réseau Santé Sociale already
connects more than 30,000 doctors and 200 hospitals,
and processes more than 100m prescriptions a year.77
In Britain, the NHS is conducting trials on two interre-
lating types of electronic record and aims to implement a
nationwide EMR by 2005.78 The German health ministry
and the representative body of the Krankenkassen
(sickness funds) have also agreed to introduce e-health
cards and electronic prescriptions, and a pilot project on
the use of e-prescriptions will be launched on a voluntary
basis quite shortly.79
EMRs offer major advantages. The computer-based
patient record system jointly operated by Massachusetts
General Hospital and Harvard Medical School has cut the
frequency of serious medical errors by 55 percent; reduced
the number of overall medication errors by 81 percent;
and saved more than US$10m a year by reducing medical
errors, a 10-fold payback on annual operating costs.
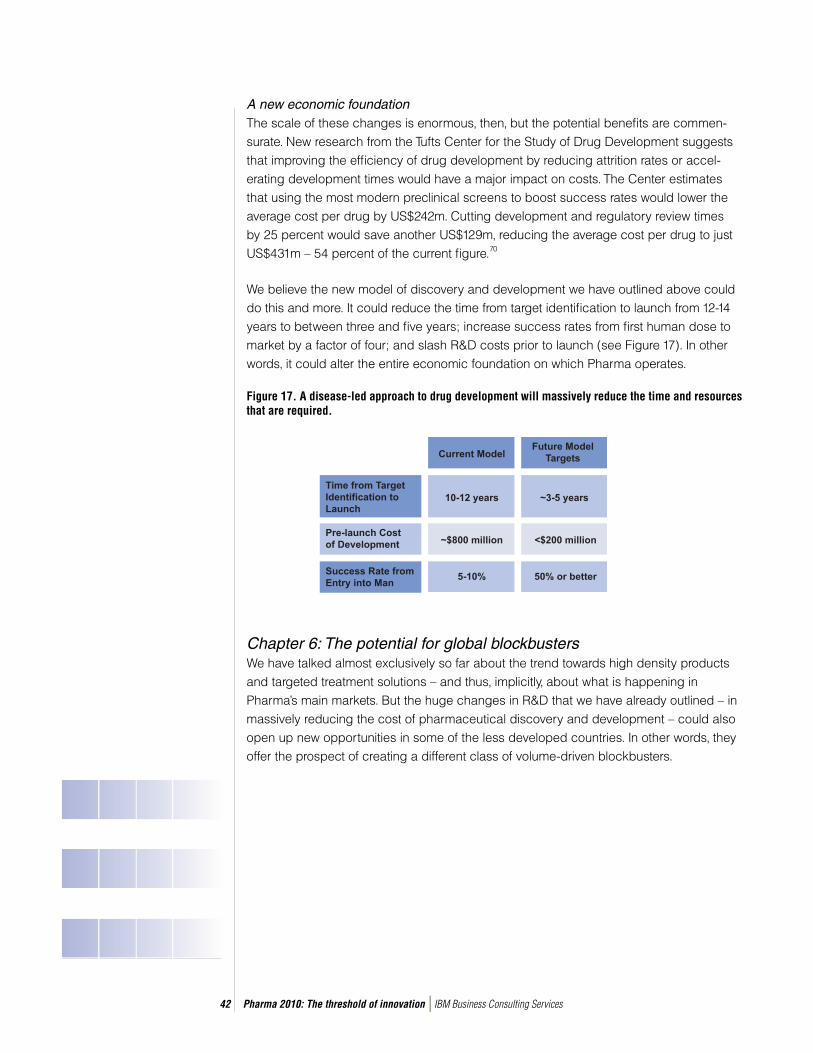
Pharma 2010: The threshold of innovation IBM Business Consulting Services42
A new economic foundationThe scale of these changes is enormous, then, but the potential benefi ts are commen-surate. New research from the Tufts Center for the Study of Drug Development suggests that improving the effi ciency of drug development by reducing attrition rates or accel-erating development times would have a major impact on costs. The Center estimates that using the most modern preclinical screens to boost success rates would lower the average cost per drug by US$242m. Cutting development and regulatory review times by 25 percent would save another US$129m, reducing the average cost per drug to just US$431m – 54 percent of the current fi gure.70
We believe the new model of discovery and development we have outlined above could do this and more. It could reduce the time from target identifi cation to launch from 12-14 years to between three and fi ve years; increase success rates from fi rst human dose to market by a factor of four; and slash R&D costs prior to launch (see Figure 17). In other words, it could alter the entire economic foundation on which Pharma operates.
Figure 17. A disease-led approach to drug development will massively reduce the time and resources that are required.
Chapter 6: The potential for global blockbustersWe have talked almost exclusively so far about the trend towards high density products and targeted treatment solutions – and thus, implicitly, about what is happening in Pharma’s main markets. But the huge changes in R&D that we have already outlined – in massively reducing the cost of pharmaceutical discovery and development – could also open up new opportunities in some of the less developed countries. In other words, they offer the prospect of creating a different class of volume-driven blockbusters.
Pharma 2010: The threshold of innovation IBM Business Consulting Services43
Some of the industry’s pioneers have already recognized this potential. IMS Health reports, for example, that 20 multinationals – including GSK, Merck, Johnson & Johnson and Bayer – have now established a presence in China, which is the world’s eighth largest market for prescription drugs.80
The poor and profitableNevertheless, many big companies are reluctant to trade in developing markets for fear of insuffi cient investment returns, inadequate infrastructure, political instability, infringe-ments of their intellectual property rights, corruption and the like – and here a seminal article by C.K. Prahalad and Allen Hammond in the Harvard Business Review is infor-mative, in arguing that it is quite possible to serve the poor profi tably.81 These fears are easy to understand, say the authors, but they are based on largely outdated assumptions about the developing world.
• The poor have no money. In fact, individual incomes are low, but the aggregate buying
power of poor communities is quite large.
• The poor cannot afford to spend what little they have on “luxuries.” The poor do buy
“luxury” items. They cannot afford to buy their own homes or get access to running water,
so they spend their income on the things they can get to improve the quality of their lives.
• The goods sold in developing markets are very cheap. Consumers at the bottom of the
economic pile often pay much higher prices than middle-class consumers.
• It is very expensive to market and deliver products and services to poor people. Many of
the poor live in densely populated cities, so companies that operate in such areas have
access to millions of potential new customers, who together have billions of dollars to
spend. Moreover, the latest information and communications technologies are opening up
new ways of reaching more people, whether they live in city slums or remote rural regions.
If these are the most common misperceptions about serving the less and the least developed countries, what about the commercial case? Because such markets are in their economic infancy, Prahalad and Hammond argue, the potential they present is considerable. First, they offer new and very rapidly growing sources of revenue. Second, they offer opportunities for cutting costs – not just by tapping into cheap labor pools but also by transferring operational effi ciencies and innovations developed to serve the poor into the rest of the business. Lastly, the new technologies are steadily reducing the impact of corruption, illiteracy, inadequate infrastructure and other such barriers to commerce.

Pharma 2010: The threshold of innovation IBM Business Consulting Services44
Drugs for everyone How does this apply to Pharma? Cutting the cost of pharmaceutical discovery and development will enable it to make drugs for markets that would once have been out of the question. It would be unrealistic to suggest that the products the industry makes for developing nations will be tailored to clinically defi ned populations, since it is the combination of much cheaper R&D and an enormous potential patient base that will make such drugs feasible in the fi rst place. It would be equally unrealistic to suggest that every country will be able to afford those drugs. In the very poorest nations, the annual per capita spend on healthcare is barely enough to buy a bottle of aspirin. Nevertheless, much wider access to mass-market medicines for the diseases from which people in such regions suffer would be an enormous improvement in itself.
The epidemiological changes wrought by greater mobility are also expanding the reach of some diseases and altering the fi nancial basis for treating them (see Figure 18 and box on The travel bug). Tuberculosis (TB) is one such instance. Almost eradicated from much of the world in the 1940s, TB has returned at alarming rates in new, more virulent forms.
Figure 18. Emerging and re-emerging infectious diseases have affected the entire world.
Source: U.S. Congress, January 2000.

Pharma 2010: The threshold of innovation IBM Business Consulting Services45
Industry estimates of the size of the TB market have generally put it at less than US$150m. However, recent research by Global Alliance for TB Drug Development, one of the public-private hybrids that have emerged in the past few years, suggests it is more like US$450m – rising to as much as US$670m by 2010. The Alliance is now backing a program to develop a drug that fi ghts multidrug-resistant strains of the disease and cuts the current six-month course of treatment to just two months. It estimates that with a cheaper, faster treatment resulting in better compliance rates, it could capture at least 50 percent of the total market – earning between US$316m and US$432m per year.82
Clearly, this is not conventional blockbuster economics, but it does imply that some of the diseases that have been neglected offer a viable market – and not just for smaller companies. In April 2000, Lehman Brothers analyzed the characteristics of 297 drugs that are already on the market. It found that 98 drugs made peak sales of less than US$200m a year, while 85 made peak sales of between US$200m and US$499m a year.83
Lehman Brothers also conducts regular reviews of products in the later stages of the R&D pipeline, based on a universe of 30 drug makers, and we have subjected the data in its last such review to further analysis.84 Our research shows that 116 of the 454 drugs in the pipeline are forecast to make peak sales of less than US$200m a year, and 120 are forecast to make peak sales of between US$200m and US$450m a year. To put it another way, half the drugs Pharma is currently developing will earn less than US$450m a year at the height of their popularity.
Thus a drug that commands annual revenues of between US$316m and US$432m – such as Global Alliance for TB Drug Development predicates – is actually one that falls well within industry norms. There is also a growing body of scientifi c
The travel bug
New diseases, and new versions of old diseases,
have created new market needs and opportunities.
According to the U.S. Centers for Disease Control, at
least 30 previously unknown infectious diseases have
been identifi ed in the last 30 years. HIV is the most
dramatic instance; it was transmitted around the globe
and infected every inhabited continent in the space
of a decade. Ebola, by contrast, was geographically
confi ned. But the risk of new infections is not restricted
to poor countries; witness the emergence of new variant
CJD (the human form of mad cow disease) in the UK
and its subsequent recognition throughout Europe.
Similarly, many old diseases – including TB, malaria,
and certain strains of streptococcus and staphylo-
coccus – are either re-emerging in the developed world
or spreading there, and some of them are becoming
increasingly resistant to antibiotics. Cholera resurfaced
in Latin America in the early 1990s, after a 100-year
absence; syphilis has resurfaced in Northern England;
and cases of West Nile Fever have been found in
southern Europe and New York City.
The spread in tropical killers and “superbugs” is partly
attributable to our growing hunger for foreign foods and
exotic holidays; and to greater international commerce.
An estimated two million people cross international
borders every day. It is also a source of serious
concern. Indeed, the UK Government is so worried that
in January 2002 it set up the National Infection Control
and Health Protection Agency to assess the threat and
oversee the development of vaccines.90
Pharma 2010: The threshold of innovation IBM Business Consulting Services46
knowledge about certain tropical diseases; in October 2002, for example, the gene sequence of the malarial parasite Plasmodium falciparum was published. Together with the changes in R&D that we have already discussed, and the fact that many people in the less developed world live in heavily populated urban areas, this should bring some of the big tropical killers within Pharma’s scope (see box on The big tropical infections).
Intellectual challenges Moreover, although that would be good news on humani-tarian grounds alone, there are several strategic reasons for making a more active effort to address the needs of the less and least developed countries. These regions have mainly refused to comply with the international rules on patent protection because they cannot get the drugs they need at prices they can pay.
In November 2001, the World Trade Organization (WTO) reached a compromise; the Doha Declaration states that the Trade-Related Intellectual Property (TRIPS) Accord “does not and should not prevent members from taking measures to protect public health.” It adds that HIV/AIDS, TB, malaria and other epidemics “can represent a national emergency or other circumstances of extreme urgency” suffi cient to justify the grant of compulsory licenses enabling generic manufacturers to make a drug that is still under patent.
The WTO also instructed the TRIPS Council to fi nd a solution to the problems countries with little or no pharmaceutical manufacturing capacity face in making effective use of compulsory licensing. And it agreed to a 10-year extension of the 2006 deadline for the least developed countries to implement the intellectual property provisions of the Accord.85 But providing people in these regions with affordable drugs for the illnesses from which they suffer would remove much of the incentive for ignoring the laws on intellectual property.
The big tropical infections
About 14m people die from infectious diseases every year.
The most dangerous diseases include:
• HIV/AIDS: An estimated 40m people are infected with
HIV, and about 3m die from it every year. Five million
people were infected in 2001 alone. Three-quarters of
those who have the disease live in Africa, where AIDS is
now the leading cause of death.
• Tuberculosis: About 8m people contract TB, and about
2m die from it, every year, but HIV is accelerating the
spread of the disease because it weakens the immune
system. The WHO estimates that between 2000 and
2020 nearly 1bn people will be newly infected, 200m will
get sick and 35m will die from TB, unless better controls
and medicines are introduced.
• Malaria: Malaria is transmitted through the bite of four
species of female mosquitoes, of which the Plasmodium
falciparum is the most lethal. Between 300m and 500m
new cases occur each year and more than 1m people
– mainly children under fi ve – die from it. Malaria is
prevalent in the least developed countries, especially
Africa, but over 12,000 cases were reported among
European travelers in 1999 and climactic changes could
increase its reach.
• Typhoid Fever: An estimated 16m people contract
typhoid fever, and about 600,000 people die from it,
every year.
• African sleeping sickness: African sleeping sickness is
a parasitic infection transmitted through the bite of the
tsetse fl y. Between 300,000 and 500,000 people contract
the disease each year and without treatment the disease
is fatal.
• Leishmaniasis: A parasitic disease caused by the bite of
the sand fl y, Leishmaniasis affl icts between 1.5m and 2m
people annually. It is prevalent in tropical and sub-tropical
regions but is now spreading to South Western Europe
– Spain, France and Portugal, in particular.
• Chagas Disease: Chagas Disease is transmitted by a
blood-sucking reduviid bug that deposits its feces on
the skin at the time of biting, or directly by transfusion of
infected blood. It is found in South and Central America.
Between 16m and 18m people are thought to be
infected.
Pharma 2010: The threshold of innovation IBM Business Consulting Services47
Local rivalsThis is not the only danger the big drug makers face. There is growing evidence that several less developed countries plan to establish their own Pharma “giants,” simulta-neously preventing the majors from breaking into new markets with signifi cant future potential and threatening margins at home.
The Chinese market is ripe for consolidation and the government favors the creation of large local concerns, although bureaucracy and provincial protectionism will probably impede this trend. The Indian market is even more overcrowded and at least two companies – Dr. Reddy’s Laboratories (DRL) and Ranbaxy Laboratories – have already set up their own R&D operations. DRL has also listed on the New York Stock Exchange and is fast becoming a multinational business.86 Meanwhile, the South Korean government is investing over US$45bn in research into biotechnology, bioengineering and nanotechnology, with the aim of establishing the country as a world leader by 2007.87 The Singapore government has also invested about US$5bn in the life sciences sector.88
The prospect of an emerging “New Pharma” raises some serious social concerns, not least the fact that most Pharma companies in less developed countries have little experience of discovering new drugs and running human trials. But this is certainly not an insurmountable obstacle. There is nothing to stop such companies learning from the West.
If Pharma does not serve the needs of people living outside its home ground more actively, then, it risks seeing the door to the markets of the less developed world closed as some countries promote their own local players. And it risks seeing its good name damaged still further, as the least developed countries agitate for access to the drugs they need at prices they can pay. The changes we have outlined provide a way of addressing these problems.
It is in all our interests that the industry should do so. Lethal diseases have played a signifi cant role in shaping human history. It is widely recognized, for example, that many more American Indians died from Eurasian germs than from European guns and swords. Similarly, analysis of archaeological remains in a cemetery in southern Italy, using the latest DNA techniques, has established the existence of a particularly virulent form of malaria in about 450 AD, lending weight to the hypothesis that a widespread outbreak of the disease contributed to the fall of the Roman Empire.89

Pharma 2010: The threshold of innovation IBM Business Consulting Services48
Chapter 7: Targeted marketing for targeted treatments
Making multiple product types for multiple markets is not just a matter of transforming the pharmaceutical discovery and development process. The industry will need to use completely different sales and marketing strategies. It will also need to forge much closer ties between its R&D and marketing operations, if it is to ensure that it creates products and services that are suffi ciently good to surmount the rising threshold of innovation.
The need for a new marketing approachThe current sales and marketing model was devised to promote one-size-fi ts-all drugs. It accordingly aims to change the prescribing behavior of general practitioners, either directly or by encouraging consumers to infl uence the decision. But this model is inade-quate for marketing and selling high density drugs and targeted treatment solutions.
• It focuses on maximizing success in the primary care market – whereas high density drugs cover secondary care and targeted treatment solutions will cover both, so the portfolios of most companies will become more specialist in emphasis.
• It aims to differentiate drugs, as distinct from classes of treatment or even entire thera-pies, whereas targeted treatment solutions will be designed for patients with specific disease states, so the disease state itself will be the main differentiating factor.
• It uses subjective arguments – i.e. what patients feel – as well as data from clinical trials, whereas targeted treatment solutions will be marketed using objective evidence, including outcomes data and even, perhaps, persistence and compliance algorithms.
• It promotes medicines that command a relatively low price per dose, whereas high density drugs command a high price per treatment and targeted treatment solutions will command prices that are based on the clinical results they deliver.
• It concentrates on stimulating demand for products, whereas the value of targeted treat-ment solutions will lie as much in the services that are wrapped around them – as new technologies and applications enable the industry to expand its offerings.
In short, Pharma will need to supplement its existing sales and marketing model with different models for different product types (see Figure 19). High density drugs will act as a stepping stone in this process, by extending the industry’s marketing and sales thrust in secondary care – although such drugs do not represent a transition from traditional products to targeted treatment solutions in any scientifi c sense.

Pharma 2010: The threshold of innovation IBM Business Consulting Services49
Figure 19. Different product types require different sales and marketing models.
Novel pricing schemesOne of the key issues is pricing. At present, drug makers usually price their products in line with competing products that are already available, and assume the cost will be reimbursed. But the move towards high density and targeted treatment solutions is predicated on achieving premium or “super” premium prices, and that will increase the diffi culties healthcare payers face in providing equitable access to such medicines without exceeding their budgets.
The need to reconcile these two factors has already resulted in the introduction of several novel pricing schemes. One such instance is the UK Department of Health’s deal for reimbursing manufacturers of beta interferons and glatiramer acetate on a sliding scale based on outcomes – although it is too early to say whether this plan is working, since practical diffi culties such as lack of specialist staff have impeded its implementation.91 A second is the arrangement into which Pfi zer and BMS entered with the state of Florida, whereby each company has guaranteed savings across its entire portfolio. And a third is the development of programs to help individual patients get reimbursed for their treatment, such as Pharmacia’s U.S. “Bridge Program” for patients taking the growth hormone therapy Genotropin.
Pharma 2010: The threshold of innovation IBM Business Consulting Services50
All these schemes have two important features in common; they depend on a much closer involvement between the company and the customer, and a much greater readiness to assume the risk. It is already clear that both these elements will become a more important component in the pricing process. Companies that make high density drugs and targeted treatment solutions will therefore need to interact with healthcare payers at a much earlier stage in the development process to ensure that a suitable funding structure is in place when their products come to market, rather than assuming that such products will simply be reimbursed.
Living dossiersThat’s not all. The very basis on which permission to market a drug is granted is also likely to change, so Pharma will need to work much more closely with the regulators, too. The traditional one-off endorsement will give way to a continuous process in which the right to market a drug is granted and re-confi rmed subject to regular reviews of its safety and effi cacy – reviews that are even more stringent than the annual checks that occur via the FDA’s adverse-event reporting process.
The European Community already plans to introduce marketing authorizations that would be valid for a year, “in particular cases when there is a specifi c and identifi ed patient need” and “suffi cient, but perhaps not defi nitive scientifi c data.”92 Together with the trend towards rolling submissions and in-life testing, this change in the way the right to market a drug is granted may herald the end of the conventional dossier, and the creation of a “living” document – a non-stop record that includes post-marketing studies, adverse event reports and more formal collection of feedback from patients – in its stead.
A more active dialogue with patientsGiven the economic differences between traditional drugs, high density drugs and targeted treatment solutions, the industry will also have to establish a much more active dialogue with patients. Pharmaceutical companies currently focus on generating prescriptions rather than keeping patients. But research from the fi nancial services sector shows that it costs between three and fi ve times more to acquire a new customer than to retain an old one. So companies that make high density drugs and targeted treatment solutions will have to improve their “customer retention” rates.
Pharma 2010: The threshold of innovation IBM Business Consulting Services51
At present, the main point of contact with patients is clinical trials. However, pharmaceu-tical companies can participate much more actively, and frequently, in the patient lifecycle by stimulating interest and awareness; promoting accurate diagnosis and treatment; getting actively involved with patients on a case-by-case basis; and helping them to comply with their treatment regimens. In this way, they can supplement and support the role of the doctor (though they would certainly not supplant it).
The big question is how best the industry should set about building such relationships. As we have already pointed out, DTC advertising works; the problem is that it works rather too well – and demand for the most actively promoted products is not always justifi ed on medical grounds. One recent study found, for example, that as many as two-thirds of the people taking Claritin and other heavily marketed allergy medicines do not even have allergies.93 If Pharma is to avoid a collision with healthcare payers and professionals, then, it will have to be much more responsible in the way it targets potential patients.
In fact, engaging with patients in a responsible, durable fashion has the potential to yield huge rewards for everyone. Although a relatively small number of people take drugs they do not need, a far greater number do not take the drugs they need, either because they have not been diagnosed or because they do not persist with their treatment.
Consider the management of high blood pressure in the UK. In 2001, about 17.1m people suffered from hypertension, but doctors participating in a survey recently conducted by Datamonitor estimated that only 51 percent of hypertensive patients are correctly diagnosed, mainly because the disease is often asymptomatic in the early stages.94 Persistence and compliance are even bigger issues, as we have already noted.
In effect, this means two things. First, there is a vast pool of undiagnosed and untreated consumers who genuinely need medication. Second, most blockbusters are only block-busters because the market is large enough to compensate for a huge patient fallout. But when the target market is much smaller, as it will be for high density drugs and targeted treatment solutions, such a “churn” rate is economically unfeasible.
Creating a constructive dialogue with patients – as distinct from bombarding them with mass-market messages – would reduce both these problems. It would help patients to identify when they should see a doctor and to understand the implications of the disease states from which they suffer, as well as why they should keep taking the medication. It would thus improve the quality of the healthcare they receive. This dialogue would also
Pharma 2010: The threshold of innovation IBM Business Consulting Services52
increase retention rates and generate more revenues for the industry itself. In other words, it would encourage the appropriate use of drugs – and that is a win for all. It is ultimately in the interests of patients, physicians, payers and Pharma that the right patients should get the right drugs at the right prices.
Evidence rather than infl uenceMany of the technologies that will be needed to underpin this more interactive approach to patients and the healthcare professionals who advise them are already emerging. The latest generation of multimedia call centers, such as the leading MCOs use, can literally deal with thousands of queries every hour on a 24-hour basis. Powerful web-enabled portals and video links can serve the same purpose. Similarly, radio frequency devices and new applications are facilitating the collection of biological data, as we have already mentioned. These new tools include home-based systems for monitoring patients, chips that can be attached to bottles or blister packs, and sensors that can be implanted in the human body (see box on Message on a bottle).
But they will also make it very much easier to collect outcomes data and determine which patients would benefi t from taking which products. And that will, in turn, shape the way in which the industry crafts its marketing and selling messages. When outcomes data are readily available, the “feel-good factor” will play a much less signifi cant role. Some of the other trends shaping the healthcare market – such as greater use of co-tiered payments in the U.S. – will reinforce this emphasis on evidence rather than infl uence. Patients who foot a large part of the bill for very expensive drugs (as they do with those that are in Tier 3) become much more aware of the cost of those drugs. They also expect much better and faster results.
A smaller, smarter sales forceIf the message has to change, so does the medium. The sales force will continue to play a vital role in the marketing and selling of pharmaceutical products, but promoting high density drugs and targeted treatment solutions requires a much smaller sales team with very different skills.
In fact, research by Novartis shows that there are grounds for changing the traditional model anyway, since productivity is falling rapidly. Although the U.S. sales force has doubled in size over the past fi ve years, there has only been a marginal rise in
Message on a bottle
The FDA has already approved a radio frequency device
developed by Applied Digital Solutions, which can be
implanted under the skin to make the human body into a
network node. VeriChip will initially be used to confi rm a
patient’s identity but has the potential to carry his or her
full medical history.
Companies like En-Vision America have devised systems
that work on similar principles; these can be attached
to a medicine bottle to remind elderly patients to take
their medicine. Several companies have also used radio
frequency technologies to create dispensing labels that
can be linked to a television and shown on screen or
read aloud, for use by people with poor vision.

Pharma 2010: The threshold of innovation IBM Business Consulting Services53
the number of contacts. Our own studies suggest that, in real terms, every dollar spent on the sales force now generates just US$10.3 in sales – a 22 percent drop since 1996 (see Figure 20).
Figure 20. U.S. Sales force productivity is in decline; so selling needs to get smarter.
Worse still, many pharmaceutical companies lack the resources to capitalize on all the leads they generate. We estimate that, in the U.S., the total number of follow-up actions required or requested as a result of sales visits, journal advertisements, the Internet, direct mail and promotional events is more than two million per year, simply to support a portfolio of average size. This translates into an average of 10,000 follow-up actions per working day – the equivalent of the direct marketing efforts of a medium-sized credit-card company.
There are also good reasons for believing that the regulators will take an increas-ingly tough stance and insist on compliant selling processes. Last year alone, the FDA issued 105 regulatory action letters for drug promotions that were determined to be false, misleading or lacking in fair balance, or promotions that publicized a product or indication before approval; and 190 letters regarding DTC advertisements which infringed the rules in some way.95
But the agencies may well extend their scrutiny to the sales force itself. The FDA has already hired more than 100 additional investigators to focus on violations of the Prescription Drug Marketing Act 1987, which governs the distribution of pharmaceutical
Source: Deutsche Bank, Global Pharmaceuticals Report, 2002 outlook; IBM Business Consulting Services estimates.
Pharma 2010: The threshold of innovation IBM Business Consulting Services54
samples – and, according to IMS Health, the industry distributed nearly US$8bn worth of samples in 2000. President Bush is also reported to have asked for an 8 percent increase in the agency’s 2003 budget for inspection-related activities.96
All these trends suggest that the sales force will undergo some considerable changes. So, of course, does the fact that the industry will be making very different sorts of products. Pharmaceutical companies that make high density drugs and targeted treatment solutions will need sales teams that can conduct in-depth discussions with specialists. And since there are far fewer specialists than there are general practitioners, they will need to employ fewer sales staff to promote secondary-care products. In short, they will have to create a smaller, smarter sales force capable of conversing with consul-tants – as Novartis has done with Gleevec.
However, some products will still fall within the domain of general practitioners – and here e-learning can also play a useful role in helping them to keep abreast of the latest developments. Online instruction has numerous advantages for often overworked general practitioners, in particular; it enables them to learn in their own time and at their own pace, and it provides a more dynamic learning environment that more closely mimics real experience than it is possible to create on paper.
Targeted messages The current method of marketing drugs to the entire patient population, using global brands and mass messages, cannot remain the only approach, then. In future, pharma-ceutical companies will have to build sales and marketing operations that can target customers much more accurately. They will also have to participate more actively and constructively in the patient lifecycle to encourage compliance and persistence.
The advent of high density drugs and targeted treatment solutions will dictate further adjustments, including the need for a sales force with a sound scientifi c grounding and the ability to provide much greater case management support. This will eventually culminate in a much more active relationship with healthcare providers and patients – not least because, as our understanding of disease becomes deeper, much of the expertise on particular disease states will reside in the companies that have focused on those diseases.

Pharma 2010: The threshold of innovation IBM Business Consulting Services55
New supply chainsThe changes in pharmaceutical research, development and marketing that we have described will obviously have an enormous knock-on effect on the supply chain as well. Over the next decade, the industry leaders will have to set up different supply chains for different product types and learn how to manage them all at the same time.
As if that were not hard enough, some of these product types will:
• Increase the complexity of the manufacturing process (see box on The biologic imperative)
• Cover a more complex range of products, with drugs, diagnostics, monitoring mechanisms, drug delivery systems and outcomes data; and
• Increase the fragility of the products that are made.
The scale of the products that are made will likewise vary much more widely, with small batches of targeted treatments and very big batches of volume-driven blockbusters. All these features will signifi cantly alter the industry’s manufacturing asset base and future investment strategy. They will also stretch its capacity to the full; Amgen is currently building a new plant specifi cally to manufac-ture Enbrel, for example, because it cannot make enough to meet demand.
However, many companies are already struggling with a wide range of manufacturing compliance problems, including the integration of legacy plant in the wake of a merger or acquisition and overall lack of investment in new technologies – a growing source of debate with the regulators. Janet Woodcock, head of the FDA’s CDER, recently complained that pharmaceutical companies treat drug manufac-turing as the “poor stepchild” to marketing and R&D.97
The industry argues in its defense that the FDA only provides manufacturing guidelines and, without a defi nitive set of manufac-turing procedures, it is diffi cult to know which technologies it should be investing in. But it is clear, both from the nature of the changes
Pharma is experiencing and the reaction of the regulators, that manufacturing must be moved much higher up the corporate agenda. It cannot remain a poor relation, in terms either of investment or of managerial focus.
The biologic imperative
Chemical compounds are quite stable and can be
manufactured relatively simply in some 20 steps.
Biologics are large molecules, typically between 10
and 100 times bigger than chemical entities, but it
is their instability rather than their size that makes
them so diffi cult to manufacture and distribute. The
shape of a biologic determines the way in which it
functions. So, for example, proteins have to fold in
certain ways; otherwise, they alter or decay. Biologics
are therefore vulnerable to anything that can affect
their shape, such as shifts in temperature, changes in
manufacturing scale, storage times and movement.
They are also more susceptible than chemical entities
to any impurities in the manufacturing process. But the
development of better technologies for manufacturing,
storage and distribution should overcome some of
these diffi culties.
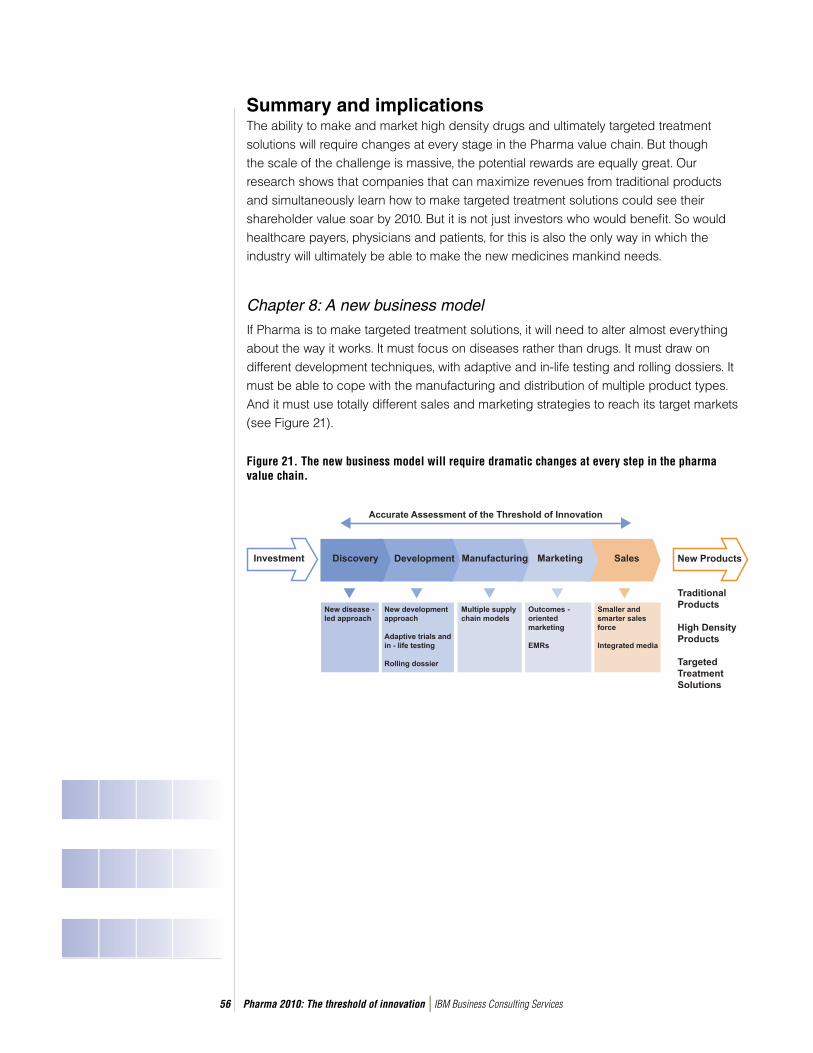
Pharma 2010: The threshold of innovation IBM Business Consulting Services56
Summary and implicationsThe ability to make and market high density drugs and ultimately targeted treatment solutions will require changes at every stage in the Pharma value chain. But though the scale of the challenge is massive, the potential rewards are equally great. Our research shows that companies that can maximize revenues from traditional products and simultaneously learn how to make targeted treatment solutions could see their shareholder value soar by 2010. But it is not just investors who would benefi t. So would healthcare payers, physicians and patients, for this is also the only way in which the industry will ultimately be able to make the new medicines mankind needs.
Chapter 8: A new business model
If Pharma is to make targeted treatment solutions, it will need to alter almost everything about the way it works. It must focus on diseases rather than drugs. It must draw on different development techniques, with adaptive and in-life testing and rolling dossiers. It must be able to cope with the manufacturing and distribution of multiple product types. And it must use totally different sales and marketing strategies to reach its target markets (see Figure 21).
Figure 21. The new business model will require dramatic changes at every step in the pharma value chain.

Pharma 2010: The threshold of innovation IBM Business Consulting Services57
In other words, the industry must be able to manage the complexity associated with working on multiple disease areas and multiple product types that use different research, development, manufacturing, marketing and sales techniques and serve different markets. Some pharmaceutical companies have already started focusing on particular disease pathologies and expanding their range with the acquisition of diagnostics operations. A few companies have also produced targeted treatments, but none has produced an entire package of targeted treatments and services for a specifi c disease area.
Hard numbersThis is not surprising, since the challenge is huge. But, as our calculations show, the potential rewards are equally large. We have used a full valuation model, such as investment banks use to value possible M&A targets.98 Our model covers the key components and process variables that infl uence total shareholder returns, including time, cost and success rates per phase per drug; in-licensed products; and sales curves by product category. It also examines various end-state scenarios, representing different degrees of transition from blockbusters to targeted treatment solutions.
Our analysis shows that the industry must change, if it does not want to grow at little more than 5 percent a year. It has a number of options for fi lling the value gap. It can use traditional tactics to prolong the life of traditional products, but this will deliver relatively little shareholder value. In addition, it can transform its entire value chain to create targeted treatment solutions.
Tactics for staying in the gameA company that takes the former course will need to review its entire R&D portfolio to assess the threshold of innovation each new product must overcome by the projected launch date and try to minimize the loss of value by optimizing prices; improving compliance and persistence; maximizing its market reach; streamlining its supply chain and support processes; acquiring new products; extending the life of those products; and making its R&D as effi cient as possible. But our research shows that even if it does everything it can to maximize revenues and the market remains broadly the same, its shareholder value will only grow by 122 percent over the next eight years. If rival drug makers start producing targeted treatment solutions and capture a signifi cant share of the market, its value could rise by as little as 20 percent by 2010.

Pharma 2010: The threshold of innovation IBM Business Consulting Services58
Strategies for winning the gameConversely, a company that decides to build a new business model will need to create a disease-centric approach to discovery and ensure that it owns the intellectual assets pertaining to the diseases on which it chooses to focus, rather than relying on academia to generate that knowledge. That, in turn, means it will have to employ many more biolo-gists, biochemists and bio-mathematicians. It will need to transform its development processes with the introduction of adaptive trials and in-life testing, and capitalize on the power of technology. It will also need to construct an outcomes-based marketing and sales model; create a fl exible supply chain that covers totally different sorts of products; forge closer relationships with the industry regulators, healthcare payers, physicians and patients; and promote the use of in-home diagnostic, monitoring and communications technologies that can deliver real-time access to patient data.
This is an enormous task. But our research shows that a company that develops the infrastructure and skills to make targeted treatment solutions, as well as using traditional tactics to maximize revenues from the products in its existing portfolio, could enhance its shareholder value very substantially. If the transition from blockbusters to high density drugs and targeted treatment solutions is relatively slow, it can expect to double its value by 2010. If the transition is very rapid and successful, it can expect to see that value increase by a factor of four to six (see Figure 22).
Figure 22. Companies that make targeted treatment solutions could enjoy even greater growth than they did in the last decade.
The bottom line is obvious. Companies that learn to make targeted treatment solutions could enjoy almost double the growth they enjoyed in the halcyon days of the early and mid-1990s, when investors were clamoring for Pharma stocks.
Source: BigCharts.com
Pharma 2010: The threshold of innovation IBM Business Consulting Services59
About the authorsSteve Arlington, PhD is a Partner with IBM Business Consulting Services. He can be reached at [email protected].
Sam Barnett, EdD is a Partner with IBM Business Consulting Services. He can be reached at [email protected].
Nick Davies, PhD is a Managing Consultant with IBM Business Consulting Services. He can be reached at [email protected].
Joe Palo is a Partner with IBM Business Consulting Services. He can be reached at
External sources of assistanceCMR International
Datamonitor
PricewaterhouseCoopers
John Urquhart, Professor of Pharmacoepidemiology, Maastricht University and Professor of Biopharmaceutical Sciences, UCSF, San Francisco
Editorial adviserHelen Kay, PhD
We should also like to express our gratitude to the many senior pharmaceutical execu-tives who have given us valuable input.
About IBM Business Consulting ServicesWith consultants and professional staff in more than 160 countries globally, IBM Business Consulting Services is the world’s largest consulting services organization. IBM Business Consulting Services provides clients with business process and industry expertise, a deep understanding of technology solutions that address specifi c industry issues, and the ability to design, build and run those solutions in a way that delivers bottom-line business value.

Pharma 2010: The threshold of innovation IBM Business Consulting Services60
References1 Paul Durman, “Giving up on Equities,” The Sunday Times Business Section (July 14,
2002): 5.2 Goldman Sachs, “Global Pharma Sector Update” (October 2002): 31. 3 “2001 – a year of drama and tragedy,” Scrip No. 2720 (February 13, 2002): 14.4 “GSK cuts Aids drug price,” The Times (September 6, 2002). Accessible at
www.timesonline.co.uk/printFriendly/0,,1-5-405457,00.html5 Our model includes the projected free cash fl ows out of which future dividends will be
paid, but rather than estimating those dividends and expressing the results in terms of annualised total shareholder returns it calculates the potential rise or fall in market capitalisation (excluding market movements) by 2010.
6 Jürgen Drews, “Drug Discovery: A Historical Perspective,” Science 287 (March 17, 2000): 1960-1964.
7 Goldman Sachs, “Global Research and Development Insight” (September 20, 2002): 4 , 11 & 14.
8 Med Ad News, July 2004. 9 IMS at website http://www.ims-global.com/insight/news_story/0403/news_story_
040323a.htm, visited 3rd Sept 2004, story entitled “Low NAS numbers highlight the need for new R&D tactics”.
10 Datamonitor “Global Generics Guide” (August 2002): 5.11 National Institute for Health Care Management Foundation, “Prescription Drug Expenditures
in 2001: Another Year of Escalating Costs” (May 2002): 8.12 Datamonitor, “The New Generation of Blockbusters” (May 2002): 6 & 26.13 IMS Health, “IMS Health Data Reveal Dramatic Growth in ‘Megabrands.’” Accessible at
www.imshealth.com/public/structure/dispcontent/1,2779,1203-1203-143992,00.... 14 IMS Health, “Global Pharmaceutical Sales by Region, 2001.” These data show that global
pharmaceutical sales in North America were US$181.8bn in 2001. We have stripped out the US$6.8bn worth of sales that occurred in Canada. Information accessible at www.imshealth.com/public/structure/dispcontent/1,2779,1343-1343-144153,00.html
15 PhRMA, “Industry Profi le” (2001), Chapter 5. Accessible at www.phrma.org/publications/publications/profi le01/
16 Goldman Sachs, “Healthcare: Managed Care” (December 18, 2001): 19.17 PricewaterhouseCoopers, “Pharma 2005: An Industrial Revolution in R&D” (November
1998).18 Goldman Sachs, “Tracking the ‘X Factor’ – Pipeline Valuations” (September 23, 2002).19 Morris Hosseini, Klaus Nagels et al., “Driving bio deals,” Scrip Magazine (December 2001):
22-25.20 William Haseltine, speech at The Economist 8th Annual Pharmaceutical Conference, London
(February 13-14, 2002). 21 Alison Taunton-Rigby, “Does biotech need pharma?” Drug Discovery Today, Vol. 6, No. 22
(November 2001): 1131-1133.22 Jo Walton, Lehman Brothers, “The Analysts’ Viewpoint? Pharma R&D Directions,”
presentation at the European Centre for Pharmaceutical Information Conference, Barcelona (June 27 2001).
23 Med Ad News, July 2004. 24 Center for Drug Evaluation and Research, Food and Drug Administration, “Attitudes and
Behaviors Associated with Direct-to-Consumer (DTC) Promotion of Prescription Drugs” (1999). Accessible at www.fda.gov/cder/ddmac/dtcindex.htm
Pharma 2010: The threshold of innovation IBM Business Consulting Services61
25 Merck-Medco, “The Merck-Medco Drug Trend Report 2001”: 7.26 National Institute for Health Care Management Foundation, “Changing Patterns of
Pharmaceutical Innovation” (May 2002): 3.27 Merck-Medco, “The Merck-Medco Drug Trend Report 2001”: 4.28 Sumit Agarwal, Sanjay Desai et al., “Unlocking the value in Big Pharma,” The McKinsey
Quarterly (2001) No. 2: 65-73.29 Goldman Sachs, “Tracking the ‘X Factor’ – Pipeline Valuations” (September 23, 2002): 12.30 Matthias M. Bekier, Anna J. Bogardus et al., “Why mergers fail,” The McKinsey Quarterly
(2001) No. 4. Accessible at www.mckinseyquarterly.com/article_page.asp?ar=1113&L2=5&L3=4
31 World Health Organisation, “Macroeconomics and Health: Investing in Health for Economic Development” (2001): 14.
32 PhRMA, “Health Care in the Developing World.” Accessible at world.phrma.org/partnerships.html
33 PricewaterhouseCoopers, “Pharma 2005: An Industrial Revolution in R&D” (November 1998): 5.
34 IMS Health, “World Review 2001: The Pharmaceutical Market” (2001): 32.35 Data provided by the United Nations Department of Economics and Social Affairs,
Population Division.36 Data provided by the U.S. Census Bureau, Population Division.37 World Health Organization, “Fact Sheet No. 135” (September 1998).38 “Asia’s AIDS epidemic set to overtake Africa,” Scrip No.2687 (October 12, 2001): 18. 39 Feng Cai, “Risks and Rewards for Pharma in Post-WTO China,” Pharmaceutical Executive
(April 2002): 68-74 & 118-120.40 Tufts CSDD, “Tufts Center Pegs Cost of a New Prescription Medicine at US$802 Million.”
Press release published on November 30, 2001. Accessible at www.tufts.edu/med/csdd/images/NewsRelease113001pm.pdf
41 CMR International, “Pharmaceutical R&D Compendium” (2000): 773, 776 & 777.42 IMS Health, “Growth in New Active Substances: How Biotechnology Drugs Are Making
Inroads.” Accessible at www.imshealth.com/public/structure/dispcontent/1,2779,1203-1203-144043,00....
43 CMR International, “Industry Success Rates 2002: Including Trends in Success Rates” (April 2002): 13. Copies of this report can be ordered at www.cmr.org/publications/bookstore1.html
44 Food and Drug Administration, “FDA to consolidate review responsibilities for new pharmaceutical products.” Press release (September 6, 2002). Accessible at www.fda.gov/bbs/topics/NEWS/2002/NEW00834.html
45 Thomas Maeder, “Sweet Medicines,” Scientifi c American (July 2002): 40-47.46 Conversation with Dr. Steve Arlington, IBM Business Consulting Services (November 2002).47 “Liability burden shifts in Germany,” Scrip No. 2761 (July 5, 2002): 3.48 Kathryn A. Phillips, David L. Veenstra et al., “Potential Role of Pharmacogenomics in
Reducing Adverse Drug Reactions,” JAMA, Vol. 286, No. 18 (November 14, 2001): 2270-2279.
49 Celia Hall, “Hospitals harmful to one in 10 patients,” The Daily Telegraph (March 2, 2001). Accessible at www.telegraph.co.uk/news/main.jhtml?xml=%2Fnews%2F2001%2F03%2F02%2Fnhosp02.xml
Pharma 2010: The threshold of innovation IBM Business Consulting Services62
50 Jason Lazarou, Bruce H. Pomeranz et al., “Incidence of adverse drug reactions in hospitalized patients. A meta-analysis of prospective studies,” JAMA, Vol. 279, No. 15 (April 15, 1998): 1200-1205.
51 Alliance for Aging Research, “When Medicine Hurts Instead of Helps: Preventing Medication Problems in Older Persons.” Accessible at www.agingresearch.org/brochures/medicinehurts/when medicine hurts.html
52 National Institute for Health Care Management Foundation, “Prescription Drug Expenditures in 2001” (May 2002): 2.
53 J. Jaime Caro, Maribel Salas et al., “Persistence with treatment for hypertension in actual practice,” Canadian Medical Association Journal, Vo1. 160 No. 1 (January 12,1999): 31-37.
54 V.S. Catalan & J. LeLorier, “Predictors of long-term persistence on statins in a subsidized clinical population,” Value in Health 3 (2000): 417-426.
55 John Urquhart, “Lessons learned from a decade of electronic monitoring of patient compliance with prescribed drug regimens: Labeling implications,” CASE lecture delivered at the Center for Drug Evaluation and Research, FDA, Rockeville, Maryland, February 27, 2001.
56 The Scandinavian Simvastatin Survival Study Group, “Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S),” The Lancet. Vol. 344 (1994): 1383–1389.
57 M. Thomas & J. Mann, “Increased thrombotic vascular events after change of statin.” Letter published in The Lancet, Vo1. 352 (1998): 1830-1831.
58 Christopher Heeschen, Christian W. Hamm et al., “Withdrawal of Statins Increases Event Rates in Patients with Acute Coronary Syndromes,” Circulation (March 26, 2002): 1446-1452.
59 E-mail correspondence with Dr. Steve Arlington, IBM Business Consulting Services (November 2002).
60 http://www.gene.com/gene/ir/fi nancials/historical/herceptin.jsp, visited 3rd September 2004.61 Adrian Michaels, “Quick-hit chemistry becomes elusive,” Financial Times (September 12,
2001). Accessible at www.ft.com 62 Rebecca N. Lawrence, “Sir Richard Sykes contemplates the future of the pharma industry,”
Drug Discovery Today, Vol.7, No. 12 (June 2002): 645-648.63 CMR International, “Industry Success Rates 2002: Including Trends in Success Rates” (April
2002): 5-6 & 12.64 Karen E. Lasser, Paul D. Allen et al., “Timing of New Black Box Warnings and Withdrawals
for Prescription Medications,” JAMA, Vol. 287, No. 17 (May 1, 2002): 2215-2220.65 “Patient safety in U.S. clinical trials under scrutiny,” Scrip No. 2760 (July 3, 2002): 15.66 CMR International, “Industry Success Rates 2002: Including Trends in Success Rates” (April
2002): 13. 67 For a fuller exposition of these principles, please see our earlier publication, “Pharma 2005:
Silicon Rally” (July 1999): 8-9.68 Dr. Lewis Sheiner passed away in the summer of 2004. One of the world’s foremost clinical
pharmacologists, his work had a great impact on the pharmaceutical industry and drug regulation.
69 CMR International, “Industry Success Rates 2002: Including Trends in Success Rates” (April 2002): 12.
70 Tufts CSDD, “Tufts Center for the Study of Drug Development Quantifi es Savings from Boosting New Drug R&D Effi ciency." Press release (September 9, 2002). Accessible at csdd.tufts.edu/NewsEvents/RecentNews.asp?newsid=20
71 “A Dying Breed,” R&D Directions (July/August 2001): 62.72 CenterWatch, An Industry in Evolution (Third edition, March 2001): 205.
Pharma 2010: The threshold of innovation IBM Business Consulting Services63
73 Coalition of National Cancer Cooperative Groups, Cancer Research Foundation of America, Cancer Leadership Council, Oncology Nursing Council & Harris Interactive, “A Quantitative Survey of Public Attitudes Towards Cancer Clinical Trials” (2000): 1-10.
74 PricewaterhouseCoopers, “Pharma 2005: Silicon Rally” (July 1999): 8.75 “The heart of the matter,” The Economist Technology Quarterly (December 8, 2001): 27-30.76 Institute of Medicine, Crossing the Quality Chasm: A New Health System for the 21st Century
(March 1, 2001): 111-144.77 PricewaterhouseCoopers, “HealthCast Tactics: A Blueprint for the Future” (May 2002): 5.78 NHS Information Authority, “NHS Medical Records,” NHS Week (July 1-8, 2002). Accessible
at www.nhsia.nhs.uk/text/pages/nhsweek2002/med_records.asp79 “German health services go electronic,” Scrip No. 2747 (May 17, 2002): 4.80 IMS Health, “Foreign Investment in China on the Increase.” Accessible at www.ims-
global.com/insight/news_story/0006/news_story_000630.htm81 C.K. Prahalad & Allen Hammond, “Serving the World’s Poor, Profi tably,” Harvard Business
Review (September 2002): 48-57.82 Global Alliance for TB Drug Development, “A Signifi cant Market for New Anti-TB Drugs.”
Accessible at www.tballiance.org/3_market.cfm?rm=economics&sub=market83 Lehman Brothers, “Pharma Pipelines” (April 2000).84 Lehman Brothers, “Pharma Pipelines” (December 2001). In our analysis, we have combined
the Introductory and Filed phases referred to by Lehman Brothers in one Regulatory Assessment phase, which is consistent with our overall approach for this study. We have also combined two product categories as defi ned by Lehman Brothers (US$200-US$349m and US$350-US$449m) in one.
85 Declaration on the TRIPS agreement and public health. Accessible at www.wto.org/english/thewto_e/minist_e/min01_e/mindecl_tripse.htm
86 “Dr. Reddy’s international business,” Scrip No. 2690 (October 26, 2001): 15.87 “Biotechnology in South Korea: An Industry in the Making,” Frost & Sullivan News Report
(January 17, 2002). Accessible at www.frost.com/prod/news.nsf/0/71337037CB422D5786256B44005549BB?Ope..
88 G. Heathers, “Biobusiness in Asia: Fiction or Fact?” Drug Discovery World (Fall 2002): 65.89 Andrew Thompson, “Malaria and the fall of Rome.” Accessible at www.bbc.co.uk/history/
ancient/romans/malaria_1.shtml90 Maxine Frith, “Exotic holidays spark rise in tropical diseases,” Evening Standard (January 10
2002): 7.91 “UK MS risk-sharing not working?” Scrip No. 2763 (July 12, 2002): 6.92 Erkki Liikanen, “Commission’s proposal to review EU pharmaceutical legislation.” Transcript
of speech /01/354, Brussels (July 18, 2001): 4. 93 John Carey & Amy Barrett, “Drug Prices What’s Fair? How Can We Encourage Research
and Still Keep Prices Within Reach for Cipro and Beyond?” Business Week (December 10, 2001): 49.
94 Datamonitor, “Treatment Algorithms: Hypertension Third Edition.” Findings reported in “Managing hypertension in the UK,” Pharmafocus (September 2002): 23.
95 CDER, “Report to the Nation: 2001.” Accessible at www.fda.gov/cder/reports/rtn/2001/rtn2001-3.htm
96 Patrick O’ Hara, “Policing CRM Sampling,” Pharmaceutical Executive (August 2002): 56-66.97 “FDA attacks: ‘Poor stepchild’ manufacturing blamed for product delays,” Pharmaceutical
Marketing (June 2002): 12.98 The valuation model we have used was constructed by PricewaterhouseCoopers.

© Copyright IBM Corporation 2004
IBM Global ServicesRoute 100Somers, NY 10589U.S.A.
Produced in the United States of America10-04All Rights Reserved
IBM and the IBM logo are registered trademarks of International Business Machines Corporation in the United States, other countries, or both.
Other company, product and service names may be trademarks or service marks of others.
References in this publication to IBM products and services do not imply that IBM intends to make them available in all countries in which IBM operates.
G510-3976-02









![THE PHARMA INNOVATION - JOURNAL · The Pharma Innovation - Journal Vol. 2 No. 3 2013 Page | 69 1.1 Advantages of Tablets[1,4,6] They are unit dosage form, and they offer the capabilities](https://img.pdfslide.us/doc/110x75/5ecb80f34dce2967c35acad8/the-pharma-innovation-the-pharma-innovation-journal-vol-2-no-3-2013-page-.jpg)



















