Embed Size (px)
Citation preview

___________________________________________________________________________ - 1 -
Offprint
Management of phantom pain with a textile, electromagnetically acting stump
liner
A randomized double-blind crossover study
Authors
U.Kern 1, B.Altkemper 2, M.Kohl 3
Institutions
1 Center of Pain Management and Palliative Care, Wiesbaden, Germany 2 Medi Ltd., Bayreuth, Germany, 3 Statistics & Mathematics Service (StaMatS), Bayreuth, Germany
Corresponding author:
Dr.Uwe Kern Center of Pain Management and Palliative Care
Blücherplatz 2 65195 Wiesbaden
phone: 0049 – 611 - 420665 or 0049 – 611 - 5808725 fax: 0049 – 611 – 8901894
---------
Original article Submitted Nov. 2005 for: Journal of Pain and Symptom Management
Acknowledgments
This study was supported by medi Bayreuth, Medicusstraße 1, D-95448 Bayreuth / Germany. Running title
Phantom pain treatment with stump liner
Key words Amputation stump, phantom pain, artificial limbs, silicon liner, electromagnetic

___________________________________________________________________________ - 2 -
ABSTRACT
Objectives: The treatment of phantom
pain is frequently dissatisfying. We
wanted to find out whether an
electromagnetically shielding stump
stocking interwoven with metal
(medipro®Liner RELAX) could have a
positive effect on phantom pain.
Methods: In a double-blind, randomized
and crossover trial, group 1 of a total of
30 leg amputees had the experimental
(=verum) silicon liner (VL) fitted to the
amputation stump after two weeks of
basic documentation, group 2 received a
dummy (=placebo) liner (PL). Treatment
was changed two weeks later. Daily
documentation focused on phantom
pain, quality of sleep and improvement
of well-being.
Results: 27 of 30 patients completed the
6 weeks’ study, 22 documentations
proved valid. The median of pain
intensity before treatment was rated
NRS 4, the median of maximum pain
NRS 6 on the numeric rating scale (NRS
1 -10). VL versus placebo reduced
permanent pain significantly more often
(p=0.008), the odds ratio being 5.95. The
degree of pain reduction in constant pain
was likewise highly significant (< 0.001).
Wilcoxon’s matched-pairs signed-rank
test for the medians of daily maximum
pain (attacks) showed a significant
reduction for both placebo (p < 0.001)
and verum (p <0.001) as compared to
baseline, with verum being highly
superior again (p< 0.001) versus
placebo. The experimental device also
led to significant amelioration of general
well-being (p = 0.037) at an odds ratio
of 3.85, and moreover to notable
improvement of the quality of sleep,
however not significantly versus placebo
(p = 0.223).
Discussion: The influence of a silicon
liner with electromagnetically protecting
properties on phantom pain is highly
significant. The precise mechanism
remains unclear, reduction of ectopic
neuroma activity is being discussed, as
well as shielding from possible
serotoninergic electromagnetic weather
impulses (sferics) or analgesic effects of
changes in the electromagnetic field as
described in animal experiment. PET or
fRMI examinations with or without
shielding silicon liner might help to
elucidate this observation further.

___________________________________________________________________________ - 3 -
INTRODUCTION
Pain in an amputated extremity as a
frequent phenomenon had already been
described by Ambroise Paré around
1550; the incidence of phantom pain
ranges between 50 and 90% (1,2).
Pathophysiology still remains unclear,
our present attempt at explanation
assumes a multicausative origin of these
phenomena including peripheral factors
(3), which cannot be held solely
responsible, though (4). Cortical
reorganization after amputations could
be proven by most recent research using
imaging techniques (5,6,7). Despite
many therapeutic approaches as
reported e.g. with anticonvulsive agents
(8), muscular relaxation techniques (9),
contralateral local anesthesia (10),
application of calcitonin (11), opiates
(12) and Botulinum toxin even (13,14),
the management of phantom pain has
altogether been dissatisfying in many
cases (15). It is not rare that the afflicted
patients resort to the coping strategy of
‘a quiet acceptance of pain’, which is
actually detrimental to their quality of life
(16).
Phantom pain could not only be
provoked by electrical stimulation at the
stump but also be treated. Phantom
pain patients are prone to feel under the
weather, and they employ self-help
measures such as „wrapping-up the
stump with aluminum foil“. We therefore
wanted to study the effect of a metal-
interwoven stump stocking (liner) made
of Umbrellan® and possessing
electromagnetically shielding properties.
MATERIAL AND METHODS
The study was conducted in a double-
blind, randomized crossover design
(fig.1).
After two weeks of basic documentation,
the patients had the silicon stocking
(liner) fitted to the amputation stump by a
likewise blinded orthopedic technician.
Half of the patients first received the
experimental liner with Umbrellan®, the
other half got a dummy liner. This
system was changed two weeks later,
and again in double-blind fashion.
Criteria for enrolment in the study
included phantom pain > VAS 3 at least
on 10 days per month and an age of >
18 years. Patients with pathologic stump
symptoms, stump pain alone,
inadequate command of language and
projected invasive interventions were
excluded. Prior to treatment, all stumps
were properly evaluated in order to

___________________________________________________________________________ - 4 -
detect obvious stump pathologies. In a
daily documentation using a numeric
rating scale (NRS, numeric rating scale
1-10), we recorded phantom pain as well
poor sleep and improvement of well-
being.
The so-called ‘liners’ we used are ‘silicon
stockings’ that are worn as a connection
between amputation stump and artificial
leg. The single components of the verum
liner were chosen accordingly to ensure
a connected conductive system with high
electromagnetic shield dampening. The
electrical direct current resistance varied
between 20 and 200 Ohm, with the
current flowing through the cover from
proximal to distal direction, being
conducted to the matrix then and inside
of it returning to the proximal margin.
Alternating electromagnetic fields are
largely kept away from the stump.
Dampening is about 40 db at the distal
end measured to a frequency of 7 GHz,
which is consistent with a residual
radiation performance of approximately
0.01 % from the baseline. Since silicon is
known to be an excellent isolator, a
normal liner can produce substantial
electrostatic charge when the patient is
walking, getting dressed etc., which
usually exposes the stump to high and
varying electrical field strength.
In the verum liner, however, the
elastomer is situated between two
equipotent surfaces since the skin
surface is connected to the cover of the
liner. This provides for a short-circuited
disk condenser. This way, the skin of the
liner-covered stump is also in a space
without electrostatic fields, even in the
presence of possibly motion-induced
static charge. Cover and matrix of the
placebo liner, however, along with the
synthetic element fused to the stump
consisted of nonconductive matter,
which prevented the above effect. There
was but one exception: the distal end of
the dummy (reaching barely above the
edge of the liner) is made of
UMBRELLAN® - in analogy to the
experimental liner, for the very reason
that the difference would have been too
obvious when using a substitute yarn.
Both the verum liner VL (medipro®Liner
RELAX) and the placebo liner PL without
interwoven Umbrellan® were
manufactured by the company medi
Bayreuth, Germany. Verum and placebo
stocking did not differ as to size,
thickness, weight or color (fig.2).

___________________________________________________________________________ - 5 -
RESULTS:
Thirty leg amputees were enrolled in the
study. Three patients dropped out early,
the remaining 27 amputees participated
throughout all three stages (old
treatment, placebo and verum periods).
Reasons for dropout were: 1)
participation in another study on new
drugs, 2) intolerance of the pressure
exerted by the liner, and 3) skin irritation
caused by the liner. Twenty-two of the
27 leg amputees (81.5%) furnished
complete and valid documentations.
Thirteen of these 22 amputees had
undergone below-knee amputation, 5
had an amputation through the thigh, 2
had below-knee and above-knee
amputations, and one was bilaterally
amputated below-knee. One participant
presented with knee exarticulation
(tab.1). Nine (40.9 %) of the 22
amputees had lost their left leg, in 10
(45.5 %) the right side was involved, and
three (13.6 %) had both legs amputated
(tab. 2).
Their age ranged between 33 and 92
years, mean age was 63.4 years; six of
the 22 participants were female (27.3%),
and 16 (72.7 %) male (tab. 2).
Time since amputation varied between
two and 734 months, with a median of
36.5 months. Median duration of
phantom pain was 35.0 months, mean
value 144.3 months with a standard
deviation of 251.5 months.

___________________________________________________________________________ - 6 -
The median above the medians of
baseline intensity of pain (obtained from
the 2 weeks’ baseline data) was NRS 4
on the numeric rating scale (NRS 1-10),
the median maximum intensity of pain
was NRS 6.
Twenty-one of the 22 patients used an
artificial leg part-time, prior to treatment
for approximately 11.0 hours a day
(median 11.5 h) with a standard
deviation of 3.4 hours. Eight (36.4 %) of
the amputees under previous
management did not have a liner so far.
On the grounds of the ordinal scale
(NRS 1-10) and the crossover design,
Wilcoxon’s matched-pairs signed-ranks
test was chosen to see whether there
was significant improvement. Decisions
were based on a significance level of
95% each.
Chronic pain
The diurnal median was chosen to
represent the chronic pain felt. The
results of Wilcoxon’s matched-pairs
signed-rank test are summarized in table
3. Assuming that, due to the physical
shielding, there would be no crossover
effects (meaning V-treatment does not
have a lasting effect and is thus without
influence on P-treatment and vice

___________________________________________________________________________ - 7 -
versa), a “wash-out” phase was refrained
from in the study design (fig. 1). Statistic
review by means of logistic regression
confirmed this assumption owing to the
absence of periodical (p=0.379) or
crossover effects (p=0.337). For this
reason, they were not reflected upon in
the following considerations.
In the model simplified accordingly, we
found a highly significant effect of the
verum device (p=0.008) in chronic pain
at an odds ratio of 5.95, i.e. chances to
encounter pain reduction was 5.95 times
greater with the experimental device
than with the placebo. 95% confidence
intervals for the prognosticated success
rates of verum (77.3%) and placebo
(36.4%), came to [ 59.8%-94.8%] for
verum and to [ 16.3%-56.5%] for placebo
(fig. 5).
We made use of the medians of diurnal
medians to analyze the extent of
reduced chronic pain in individual
amputees. An analysis aided by
Wilcoxon’s matched-pairs signed-rank
test revealed significant pain reduction
by both, placebo (p=0.035) and verum (p
< 0.001) as compared to baseline.
Verum in addition effected highly
significant reduction of pain (p < 0.001)
versus placebo. While pain reduction by
placebo versus baseline was significant
only >0 in NRS, pain reduction by verum
versus baseline was significant >= 1.5 in
NRS, and by verum versus placebo
significant >= 0.75 in NRS (fig. 3).
Relative pain reduction in individual
amputees is presented in tab. 4. Data
on these relative changes were
ascertained by relating the left margin of
the 95% confidence interval obtained by
Wilcoxon’s matched-pairs signed-rank
test to the median of diurnal medians
(baseline) for the old treatment.

___________________________________________________________________________ - 8 -
Maximum pain (pain attacks):
When using the verum liner, 18 of those
22 patients indicated a reduction in
maximum pain intensity, which was
effected in merely 11 patients using
placebo. The results of the Wilcoxon’s
matched-pairs signed-rank test are
summarized in tab. 3. Again neither
periodical (p = 0.670) nor crossover
effects (p = 0.794) proved significant and
were thus left unconsidered. A significant
effect of verum (p = 0.031) at an odds
ratio of 4.50 was noted by comparison
with placebo, implying that chances to
accomplish a reduction of maximum pain
by the experimental liner was 4.50
greater than by placebo. The 95%
confidence intervals for the
prognosticated success rates of verum
(81.8%) and placebo (50.9%) ranged
[67.7% - 97.9%] for the experimental
device and [29.1% - 70.9%] for the
placebo (fig. 5).
To analyze the extent of pain reduction,
we employed the median of the daily
maximum values of a given study period
and/or the maximum level over all days
of the study period, to serve as the
reference value of maximum pain (pain
attack)
of the individual amputees.
Median of daily maximum values:
Wilcoxon’s matched-pairs signed-rank
test showed significant pain reduction by
both placebo (p < 0.001) and verum (p <
0.001) versus baseline conditions, with
verum moreover effecting a highly
significant reduction of maximum pain (p
< 0.001) versus placebo (fig. 4).
Pain reduction by placebo was still
significant versus baseline >= 1 in NRS,
pain reduction by verum versus baseline
was significant >= 2.25 in NRS, and
finally pain reduction by verum versus
placebo was significant >= 0.75 in NRS.
___________________________________________________________________________ - 9 -
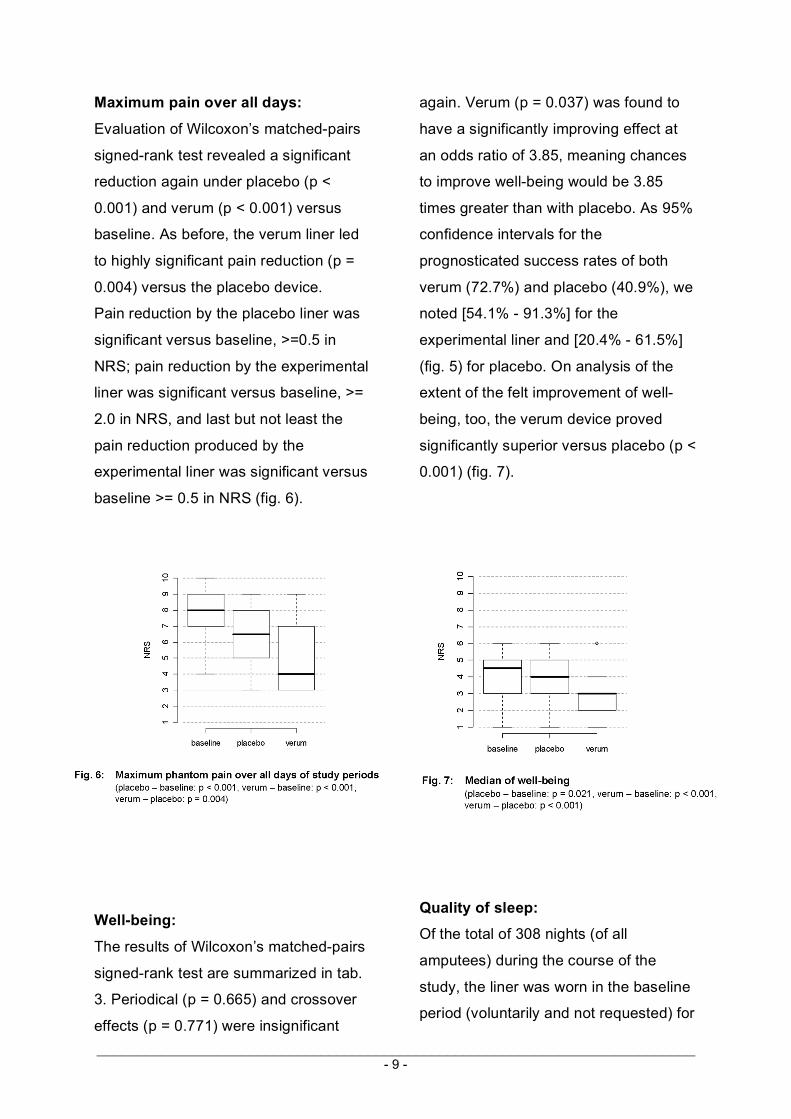
Maximum pain over all days:
Evaluation of Wilcoxon’s matched-pairs
signed-rank test revealed a significant
reduction again under placebo (p <
0.001) and verum (p < 0.001) versus
baseline. As before, the verum liner led
to highly significant pain reduction (p =
0.004) versus the placebo device.
Pain reduction by the placebo liner was
significant versus baseline, >=0.5 in
NRS; pain reduction by the experimental
liner was significant versus baseline, >=
2.0 in NRS, and last but not least the
pain reduction produced by the
experimental liner was significant versus
baseline >= 0.5 in NRS (fig. 6).
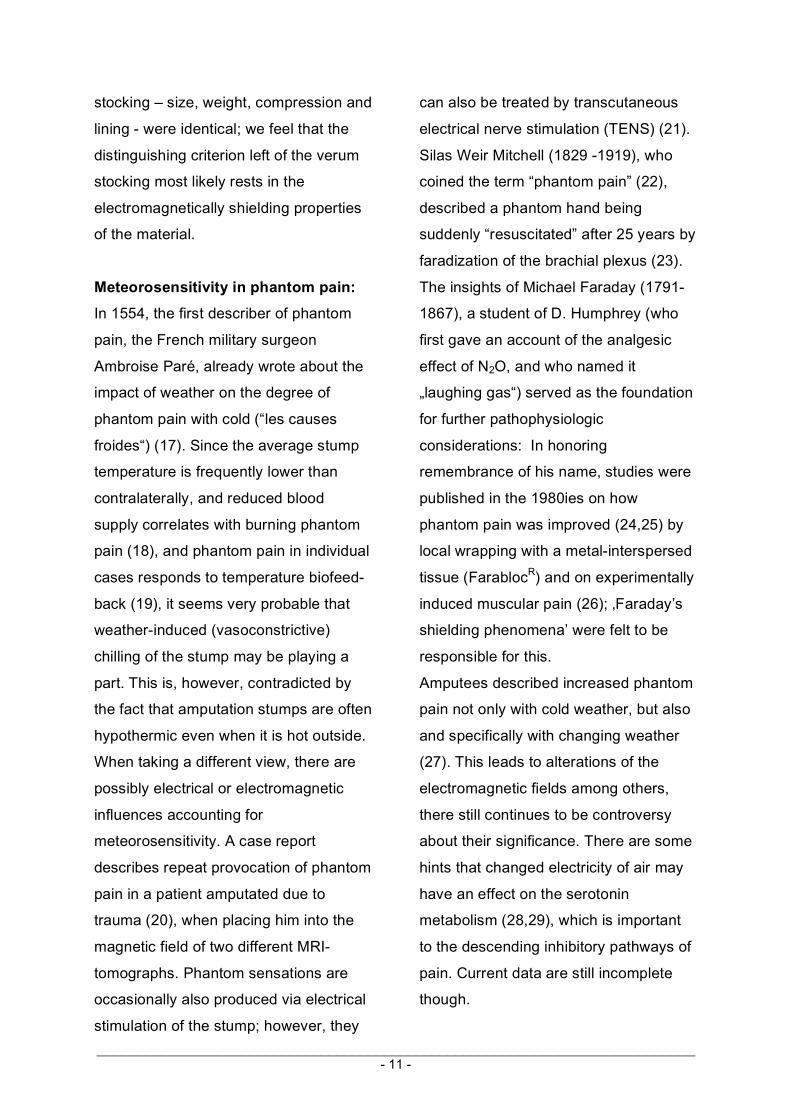
Well-being:
The results of Wilcoxon’s matched-pairs
signed-rank test are summarized in tab.
3. Periodical (p = 0.665) and crossover
effects (p = 0.771) were insignificant
again. Verum (p = 0.037) was found to
have a significantly improving effect at
an odds ratio of 3.85, meaning chances
to improve well-being would be 3.85
times greater than with placebo. As 95%
confidence intervals for the
prognosticated success rates of both
verum (72.7%) and placebo (40.9%), we
noted [54.1% - 91.3%] for the
experimental liner and [20.4% - 61.5%]
(fig. 5) for placebo. On analysis of the
extent of the felt improvement of well-
being, too, the verum device proved
significantly superior versus placebo (p <
0.001) (fig. 7).
Quality of sleep:
Of the total of 308 nights (of all
amputees) during the course of the
study, the liner was worn in the baseline
period (voluntarily and not requested) for

___________________________________________________________________________ - 10 -
2 nights only. This happened during the
placebo period for 64 nights, and during
the verum period for 121 nights.
Although this is indicative of a marked
effect under verum, which is also
suggested by the degree of improved
sleep, versus placebo (p = 0.223) we
saw no significant effect by verum at an
odds of 2.14, i.e. chances to improve
sleep were 2.14 times greater for verum
than for placebo. As 95% confidence
intervals for the prognosticated success
rates of verum (68.2%) and placebo
(50.0%), we note [48.7% - 87,6%] for
verum and [29.1% - 70.9%] for placebo
(fig. 5).
All of the results and significance
computations regarding the individual
patients are summarized in tab. 5.
DISCUSSION
Our examinations showed that the
duration of chronic phantom pain as well
as maximum phantom pain (pain
attacks) were in part highly significantly
reduced when patients were using the
metal-interwoven stump liner
(medipro®Liner RELAX) (as compared to
the placebo liner). Their general well-
being was likewise significantly
improved; the verum liner was
spontaneously and voluntarily worn for
twice as many nights than the placebo
stocking. Since the other qualities of the
___________________________________________________________________________ - 11 -
stocking – size, weight, compression and
lining - were identical; we feel that the
distinguishing criterion left of the verum
stocking most likely rests in the
electromagnetically shielding properties
of the material.
Meteorosensitivity in phantom pain:
In 1554, the first describer of phantom
pain, the French military surgeon
Ambroise Paré, already wrote about the
impact of weather on the degree of
phantom pain with cold (“les causes
froides“) (17). Since the average stump
temperature is frequently lower than
contralaterally, and reduced blood
supply correlates with burning phantom
pain (18), and phantom pain in individual
cases responds to temperature biofeed-
back (19), it seems very probable that
weather-induced (vasoconstrictive)
chilling of the stump may be playing a
part. This is, however, contradicted by
the fact that amputation stumps are often
hypothermic even when it is hot outside.
When taking a different view, there are
possibly electrical or electromagnetic
influences accounting for
meteorosensitivity. A case report
describes repeat provocation of phantom
pain in a patient amputated due to
trauma (20), when placing him into the
magnetic field of two different MRI-
tomographs. Phantom sensations are
occasionally also produced via electrical
stimulation of the stump; however, they
can also be treated by transcutaneous
electrical nerve stimulation (TENS) (21).
Silas Weir Mitchell (1829 -1919), who
coined the term “phantom pain” (22),
described a phantom hand being
suddenly “resuscitated” after 25 years by
faradization of the brachial plexus (23).
The insights of Michael Faraday (1791-
1867), a student of D. Humphrey (who
first gave an account of the analgesic
effect of N2O, and who named it
„laughing gas“) served as the foundation
for further pathophysiologic
considerations: In honoring
remembrance of his name, studies were
published in the 1980ies on how
phantom pain was improved (24,25) by
local wrapping with a metal-interspersed
tissue (FarablocR) and on experimentally
induced muscular pain (26); ‚Faraday’s
shielding phenomena’ were felt to be
responsible for this.
Amputees described increased phantom
pain not only with cold weather, but also
and specifically with changing weather
(27). This leads to alterations of the
electromagnetic fields among others,
there still continues to be controversy
about their significance. There are some
hints that changed electricity of air may
have an effect on the serotonin
metabolism (28,29), which is important
to the descending inhibitory pathways of
pain. Current data are still incomplete
though.

___________________________________________________________________________ - 12 -
The pain threshold could be altered (30)
by application of electromagnetic fields
in man. Chronic pelvic pain, whiplash
injuries and lumbar radiculopathies
responded favorably (31,32,33), pain in
CRPS I, however did not (34). Prato (35)
was able to prove reproducible
analgesia in CD-1-mice (consistent with
the potential of approximately 5mg/kg
morphine) by repeat placement in a
magnetically protected environment. He
related this to an opioid-mediated
mechanism, since the effect could be
antagonized by naloxone. An opiate-
mediated analgesia, however, was
attenuated with simple exposure.
Choleris (36) describes a reduction of
stress-induced analgesia in mice owing
to electromagnetic shielding, albeit only
when
this was incomplete. The effect was in
addition merely observed with shielding
prior to the onset of stress. This
illustrates the complexity of possible
connections; there is no final conclusion
regarding the electromagnetic influences
on pain phenomena yet.
Sferics: Sferics (derived from
“atmospherics“, atmospheric
disturbances) are electromagnetic waves
ranging from 1 to 100 kHz, and are also
referred to as very low frequency (VLF)-
sferics. These are consistent with
extremely low amplitude transitory
electromagnetic impulses, originating
during thunderstorms and friction of air
masses for instance, which can be
measured a long time before, in fact, the
weather is actually changing. Many
measuring stations collect these data to
make the weather forecasts. In
controversial discussion, they are
believed to be the cause of possible
meteorosensitivity in phantom pain and
other pain disorders. They are possibly
involved by intervening with the
serotonin metabolism in
meteorosensitive migraine (28), and they
were significantly correlated with
migraine in the winter time (37, 38).
Contrary to some animals (e.g. migrants
and sharks), man is incapable to
perceive electromagnetism; in
experiments, however, EEG changes
could be generated by sferics (39).
Attempts to correlate certain weather
conditions to headaches for instance,
have only yielded few results to date
(40). This may be due to the common
correlation of pain events to
synchronously measurable weather
data, whereas electromagnetic changes
are already occurring several days
earlier.
There are no insights as to the impact of
sferics on phantom pain; an influence on
severed nerve endings of the stump can
neither be confirmed nor excluded.
Electromagnetic shielding under this
assumption would be a therapeutic
approach unthought of before.

___________________________________________________________________________ - 13 -
Neuromic and ectopic activity:
Regenerative budding of the damaged
axon will set in after discission of
peripheral sensible nerve fibers.
Neuromas that might ensue in
consequence consist of thickened C-
fiber endings and demyelinated A-fibers
(41) with an increased spontaneous
discharge rate that is usually rhythmic
and high-frequency (42). Not only stump
pain but spastic phantom pain as well
may originate from neuromas (43). The
incidence of neuromas is nevertheless
said to be low (44), and phantom pain is
reported far to fast postoperatively to be
related to neuromic activity alone (18).
The longterm outcome of neuroma
surgery is, moreover, satisfying in rare
cases only.
Flor (3) maintains that defective stump
information is likely to generate ectopic
discharge from the posterior root
ganglion with the consecutive result of
phantom pain. The case report in an
fMRI study cites reorganization even by
stimulation not painful, with the
amputated leg producing an increased
cortical representation due to ‘abnormal
information’ (45).
Whether electrical of electromagnetic
influences from outside might be
involved in the form of ‘not painful faulty
information’ is not stated explicitly.
Neuromic excitation by external
electromagnetic influences is not yet
verified, on the other hand and
interestingly enough, application of local
anesthetics can terminate phantom pain
by blockade of the sodium channel
dampening the excitement of neuromas.
In sum, we may assume that ectopic
discharges from stump nerves contribute
to central sensitization with known
synchronously suppressed
(serotoninergic) pain-inhibiting systems,
thereby mediating phantom sensations.
Whether electromagnetic shielding of
neuromas can indeed reduce ectopic
discharge activity, will have to be left to
further research. For the time being it
may be accounting for the reduction of
phantom pain observed in our patients
by UmbrellanR shielding.
Silicon liner:
The silicon liner („stump stocking“)
together with a locking element
anchored to the artificial leg serves as
the secure connection between the
amputation stump and exoskeletal
artificial leg and significantly facilitates
handling of the prosthesis. Silicon liners
are rolled over the stump to precise
fitting, and have additional
decompressing effect besides
stimulating the blood flow. Steinbach
(46) describes lasting use of artificial leg
in 91% of the patients without phantom
pain, but only in 27% with phantom pain.
That phantom pain is reduced by
activation of the stump muscles (as
given e.g. with myoelectrical artificial

___________________________________________________________________________ - 14 -
legs) has been known (47,48),
decreased motor reorganization has also
been observed in the process (49).
Reduction of phantom pain could thus
be related alone to optimum use of the
stump via silicon liner or proprioceptively
mediated calming of pain, and – like in
our study - this effect should not differ
between verum and placebo liner. It
might, however, explain the likewise
obvious reduction of phantom pain in the
placebo group. There are no definite
data on antinociceptive properties of
silicon liners as opposed to other forms
of management.
Costs: Phantom pain is difficult to treat
(15) and results in extensive use of
medical resources. Costly longterm
management by opiates (12) and
anticonvulsive agents (8) is not rare, and
is substantially more expensive per year
than the prescription of a liner. Our
results suggest that costs for drugs and
other prescriptions can be effectively
reduced in individual responders,
thereby also diminishing the risk of
adverse drug effects with consecutive
medical contacts.
SUMMARY
Our study turned out to significantly
reduce both average and maximum
intensity of phantom pain and to
significantly increase well-being when a
stump silicon stocking with
electromagnetically shielding properties
was used versus a dummy. The precise
mechanism of action, e.g. possible
reduction of ectopic activity in cut nerve
endings, remains unclear. PET or fRMI
examinations with and without shielding
silicon liner in clinical responders as well
as trials to deliberately provoke phantom
pain by low-amplitude electromagnetic
impulses (sferics) might help to elucidate
this observation further.
___________________________________________________________________________ - 15 -
REFERENCES 1. Kooijman CM, Dijkstra PU, Geertzen JH, Elzinga A, van der Schans CP (2000). Phantom pain
and phantom sensations in upper limb amputees: an epidemiological study. Pain Jul;87(1):33-41.
2. Nikolajsen L, Lindvig M (2001). Phantom pain after amputation of extremities. Ugeskr Laeger Jun 11;163(24):3338-41.
3. Flor H, Bierbaumer N (2000). Phantom limb pain: cortical plasticity and novel therapeutic approaches. Current Opinion in Anaesthesiology 2000 13:561-564.
4. Flor H (2002). Phantom-limb pain: Characteristics, causes and treatment. The Lancet Neurology 2002 Vol 1, No 3:182-189.
5. Adler T (2001). Nachweis kortikaler Reorganisation bei Patienten mit Armamputationen und die Beziehung zu Phantomschmerzen – Eine fMRT-Studie. Z Orthop Ihre Grenzgeb Mar-Apr;139(2):M29-30.
6. Flor H, Elbert T, Knecht S (1995). Phantom-limb pain as a perceptual correlate of cortical reorganisation following arm amputation. Nature 375:482-484.
7. Huse E, Larbig W, Birbaumer N, Flor H (2001). Kortikale Reorganisation und Schmerz. Empirische Befunde und therapeutische Implikationen am Beispiel des Phantomschmerzes. Schmerz Apr;15(2):131-7.
8. Bone M, Critchley P, Buggy DJ (2002). Gabapentin in postamputation phantom limb pain: a randomized, double-blind, placebo-controlled, cross-over study. Reg Anesth Pain Med 2002 Sep-Oct;27(5):481-6.
9. Simanski C, Bathis H, Bouillon B, Koch-Epping G, Tiling T. Therapeutic concept for preventing chronic phantom pain after traumatic brachial plexus lesion.Unfallchirurg. 2001 Jul;104(7):659-64.
10. Gross D (1981). Contralateral local anesthesia in the treatment of stump and phantom pain. MMW Munch Med Wochenschr Sep 4;123(36):1332.
11. Jaeger H, Maier C (1992). Calcitonin in phantom limb pain: a double-blind study. Pain Jan;48(1):21-7.
12. Huse E, Larbig W, Flor H, Birbaumer N. (2001). The effect of opioids on phantom limb pain and cortical reorganization. Pain 2001 Feb 1;90(1-2):47-55
13. Kern U, Martin C, Scheicher S, Muller H. Long-term treatment of phantom- and stump pain with Botulinum toxin type A over 12 months. A first clinical observation. Nervenarzt. 2004 Apr;75(4):336-40.
14. Kern U, Martin C, Scheicher S, Müller H (2003). Treatment of phantom pain with botulinum-toxin A. A pilot study. Schmerz 2003 Apr;17(2):117-24.
15. Flor H, Bierbaumer N (2000). Phantom limb pain: cortical plasticity and novel therapeutic approaches. Current Opinion in Anaesthesiology 2000; 13:561-564 .
16. Machin P, de C Williams AC (1996). Stiff upper lip: coping strategies of World War II veterans with phantom limb pain. Clin J Pain 1998 Dec;14(4):290-4.
17. Keil G. So-called initial description of phantom pain by Ambroise Pare. "Chose digne d'admiration et quasi incredible": the "douleur es parties mortes et amputees". Fortschr Med 1990 Feb 10;108(4):62-6. German.
18. Hill A (1999). Phantom limb pain: a review of the literature on attributes and potential mechanisms. J Pain Symptom Manage 1999 Feb;17(2):125-42.
19. Belleggia G, Birbaumer N. Treatment of phantom limb pain with combined EMG and thermal biofeedback: a case report. Appl Psychophysiol Biofeedback 2001 Jun;26(2):141-6.
20. Yuh WT, Fisher DJ, Shields RK, Ehrhardt JC, Shellock FG. Phantom limb pain induced in amputee by strong magnetic fields. J Magn Reson Imaging 1992 Mar-Apr;2(2):221-3.
21. Gnezdilov AV, Syrovegin AV, Plaksin SE, Ovechkin AM, Ivanov AM, Sul'timov SA. Evaluation of the effectiveness of transcutaneous electroneuroanalgesia in phantom pain syndrome. Anesteziol Reanimatol. 1995 Mar-Apr;(2):97-102.
22. Mitchell SW. Phantom limbs. Lippincott's Mag Popular Literature & Science 1871;8:563-9. 23. Sacks O (2004). Der Tag, an dem mein Bein fortging.14. Aufl. 2004 Rowohlt ISBN 3-499-
18884-8, 99.
___________________________________________________________________________ - 16 -
24. Halbert J, Crotty M, Cameron ID. Evidence for the optimal management of acute and chronic phantom pain: a systematic review. Clin J Pain 2002 Mar-Apr;18(2):84-92.
25. Mertz DP. Neue therapeutische Versuche gegen Phantomschmerzen. Deutsches Ärzteblatt 83, 3548, 1986.
26. Zhang J, Clement D, Taunton J. The efficacy of Farabloc, an electromagnetic shield, in attenuating delayed-onset muscle soreness.Clin J Sport Med 2000 Jan;10(1):15-21. PMID: 10695845 [PubMed - indexed for MEDLINE.
27. Harlfinger O. Weather-induced effects on pain perception. Fortschr Med 1991 Nov 10;109(32):647-50.
28. Sulman FG. Migraine and headache due to weather and allied causes and its specific treatment. Ups J Med Sci Suppl 1980;31:41-4.
29. Sulman FG, Levy D, Lunkan L (1976). Wetterfühligkeit und ihre Beziehung zu Sferics, Ionen und Elektrofeldern. Z Physikal Med 6:229–238.
30. Ghione S, Seppia CD, Mezzasalma L, Bonfiglio L. Effects of 50 Hz electromagnetic fields on electroencephalographic alpha activity, dental pain threshold and cardiovascular parameters in humans. Neurosci Lett. 2005 Jul 1-8;382(1-2):112-7.
31. Thuile Ch, Walzl M. Evaluation of electromagnetic fields in the treatment of pain in patients with lumbar radiculopathy or the whiplash syndrome. NeuroRehabilitation 2002;17(1):63-7.
32. Rowe E, Smith C, Laverick L, Elkabir J, Witherow RO, Patel A. A prospective, randomized, placebo controlled, double-blind study of pelvic electromagnetic therapy for the treatment of chronic pelvic pain syndrome with 1 year of followup. J Urol 2005 Jun;173(6):2044-7.
33. Varcaccio-Garofalo G, Carriero C, Loizzo MR, Amoruso S, Loizzi P. Analgesic properties of electromagnetic field therapy in patients with chronic pelvic pain. Clin Exp Obstet Gynecol 1995;22(4):350-4.
34. Durmus A, Cakmak A, Disci R, Muslumanoglu L. The efficiency of electromagnetic field treatment in Complex Regional Pain Syndrome Type I. Disabil Rehabil 2004 May 6;26(9):537-45.
35. Prato FS, Robertson JA, Desjardins D, Hensel J, Thomas AW. Daily repeated magnetic field shielding induces analgesia in CD-1 mice. Bioelectromagnetics 2005 Feb;26(2):109-17.
36. Choleris E, Del Seppia C, Thomas AW, Luschi P, Ghione G, Moran GR, Prato FS. Shielding, but not zeroing of the ambient magnetic field reduces stress-induced analgesia in mice. Proc Biol Sci 2002 Jan 22;269(1487):193-201.
37. Vaitl D, Propson N, Stark R, Walter B, Schienle A. Headache and sferics.Headache 2001 Oct;41(9):845-53.
38. Walach H, Betz HD, Schweickhardt A. Sferics and headache: a prospective study.Cephalalgia 2001 Jul;21(6):685-90.
39. Schienle A, Stark R, Vaitl D. Sferics provoke changes in EEG power.Int J Neurosci 2001 Mar;107(1-2):87-102.
40. Walach H, Schweickhardt A, Bucher K. Does weather modify headaches? An empirical evaluation of bio-weather categorization. Schmerz 2002 Feb;16(1):1-8.
41. Fried K, Govrin-Lippmann R, Rosenthal F, Ellisman MH, Devor M. Ultrastructure of afferent axon endings in a neuroma.J Neurocyto 1991 Aug;20(8):682-701.
42. Blumberg H, Janig W. Discharge pattern of afferent fibers from a neuroma.Pain 1984 Dec;20(4):335-53.
43. Baron R, Janig W. Pain syndromes with causal participation of the sympathetic nervous system. Anaesthesist 1998 Jan;47(1):4-23.
44. Whipple RR, Unsell RS. Treatment of painful neuromas.Orthop Clin North Am 1988 Jan;19(1):175-85.
45. Condes-Lara M, Barrios FA, Romo JR, Rojas R, Salgado P, Sanchez-Cortazar J (2000). Brain somatic representation of phantom and intact limb: a fMRI study case report. Eur J Pain.2000;4(3):239-45.
46. Steinbach TV, Nadvorna H, Arazi D (1982). A five year follow-up study of phantom limb pain in post traumatic amputees. Scand J Rehabil Med 1982;14(4):203-7.
47. Flor H (1999). Helping patients with phantom pain. Prosthesis for the brain? Interview by Dipl.

___________________________________________________________________________ - 17 -
Biochem. Petra Eiden. MMW Fortschr Med 1999 Dec 16;141(51-52):16. 48. Weiss T, Miltner WH, Adler T, Bruckner L, Taub E (1999). Decrease in phantom limb pain
associated with prosthesis-induced increased use of an amputation stump in humans Neurosci Lett 1999 Sep 10;272(2):131-4.
49. Lotze M, Grodd W, Birbaumer N, Erb M, Huse E, Flor H (1999) Does use of a myoelectric prosthesis prevent cortical reorganization and phantom limb pain? Nat Neurosci 1999 Jun;2(6):501-2.
Double-blind study - Submitted Nov. 2005 for: Journal of Pain and Symptom Management





























