Embed Size (px)
Citation preview
Running Head: PLAN OF CARE AUTOMATION
Plan of Care Automation for Care Management Organization.
Paul Godfrey, MBA, BSN, RN, MSN Candidate
Rutgers University, Newark NJ
School of Nursing
NINF5305: Nursing Informatics Practicum
Faculty Advisor: Rose P. Estrada, DNP, RN, BC, CPN
Preceptor: Deidra Brown, RN, MSN, NP
Facility/Address: Montefiore Care Management, 200 Corporate Blvd, Yonkers, NY 10701
December 3, 2014
PLAN OF CARE AUTOMATION 1
Abstract
When a patient comes to the hospital or any of the health care institutions, the
interdisciplinary team (IDT), which is made up of nurses, physicians, pharmacists, social
workers, etc., will in most cases assess the patient physically before any plan of care is initiated.
The nurse will follow the nursing process of assessment, diagnoses, planning, intervention, and
evaluation. The plan of care is documented electronically or manually in some cases and the
nurse charts periodic activities showing patient progress and interventions provided. Discharge
planning begins the day of admission as is the case in traditional health care institutions. The
complexities of performing these functions is multiplied if not quadrupled while performing care
plans for patients you can neither see or touch. While using communication sources such as a
telephone, electronic email, manual mail, and other communication mechanisms, efforts are
made to apply the nursing process for the ultimate health of the patient.
The nurse being the patient advocate and leader of the IDT chairs the task of coordinating
the activities of the IDT. This is enormous and daunting task. The complexity is exemplified
with the fact that some of the nurses may have hundreds of patients/members to manage.
“President Obama is pushing to establish EHR for all Americans prior to 2015 by making $17
billion available to e-health projects and programs. Database companies will be investing
significant effort in developing health and medical database systems that are accessible on the
Internet” (Stair & Reynolds, 2012, p138). The automation of plan for members/patients of care
coordination entities will help to provide all needed interventions effectively and also foster the
efficient and detailed documentation of all triggered problems which should be made part of the
Electronic Health Record (EHR) for members.
PLAN OF CARE AUTOMATION 2
Project Scope
Within the scope of this project, issues relating to the possible economic impact of care
coordination and resource allocation will be addressed. This project will also highlight possible
information technology issues affecting care coordination outside traditional health care
institutions and offer possible solutions. The application of nursing science to care coordination
outside of traditional health care institutions will be highlighted to show how different it is from
the traditional health care institutions. Montefiore Care Management Organization (CMO) will
be used as an example, to show some of the efforts that have been made in the area of
automation of Plan of Care with regards to care management outside traditional health care
institutions. Lastly, this project will highlight leveraging information technology in educating the
clinicians to become effective in performing their attributed task toward achieving positive
health outcomes.
Project Goal/Purpose
The goal of this project is to show how automating the process of care planning for
managing patients outside a traditional health care institution will help to drive the enormous
inherent tasks of patient care management. This function will add decision support to the care
management application system. Some of the domains of care for care management and care
coordination outside of the traditional health care institutions includes the following: Palliative,
Hospice, Behavioral Health, Benefits/Entitlements, Care Access, Care-Giving, Functions,
Housing, Legal, Life Planning, Preventative, and Psychosocial. A patient presenting with many
problems originating from many of the aforementioned domains of care, presents a challenge as
to which problem should take precedent before the other. Automating a plan of care will help to
drive the problem, goals and intervention into an automated task system. Tasks can be collected
PLAN OF CARE AUTOMATION 3
within a workbasket shared by a group of clinicians responsible for providing care to the
patient/member. The tasks in the workbasket can now be automated to be divided among the
team using round-robin logic to drive the tasks into worklist. These tasks are to be called
interventions which may lead to interactions between patient/member and the clinician. “The
promise of fully realized EHRs is having a single record that includes all of a patient's health
information: a record that is up to date, complete, and accurate. This puts providers in a better
position to work with their patients to make good decisions.” (www.healthit.gov). Some of the
benefits of EHR are listed by www.healthit.gov as the following: improving the quality and
convenience of patient care, increasing patient participation in their care, improving accuracy of
diagnoses and health outcomes, improving care coordination, and increasing practice efficiencies
and cost savings.
Project Objectives
The objective of this project with regards to the related health care industry is to highlight
the difficult task of care management outside traditional health care institutions. Acknowledging
the involved daunting task will lead to solutions related to automation of the process of care
planning for members/patient enrolled in care management outside traditional health care
institutions. The solution will center on task driven logic that will help the clinicians to manage
multiple tasks for members/patients of care management. To effectively accomplish the ultimate
goal of positively affecting patient/member health outcome, educating the IDT on the usefulness
and benefits of utilizing information technology will be invaluable. Identifying the competency
of the IDT in utilizing the provided technology and suggested ways of providing needed
education will be discussed as one of the objectives.
PLAN OF CARE AUTOMATION 4
With respect to accomplishing the course objectives through this project, the role of
information technology in care management is addressed. The concomitant relationship between
positive patient care outcome and utilization of information technology is paramount in this
project. After the completion of this project, I would have demonstrated how to initiate a project;
manage the triple constraints of a project which are time, resources, and scope; and finally,
demonstrated how to maintain the quality of a product as the ultimate end goal of the project.
Project Stakeholders/Organizational culture
The umbrella project for an application that will be capable of encapsulating care
planning automation will be a replacement of CMO legacy care management system called
CCMS. Several stakeholders will include outside vendor, Montefiore Information Technology
Team (Montefiore IT), CMO Data Reporting Team (DAR), CMO Care Management Process
Engineering Team (CMPE), CMO Center for Innovation and Learning Team (CIL), CMO
Management Information Systems Team (MIS), and CMO Clinical Subject Matter Experts. The
CIL is responsible for assessing computer competency of CMO clinicians and providing
educational strategy and training to address the identified deficiencies. The component of a
Decision Support System, which is a primary focus of this project, is the Plan of Care
Automation.
Project Schedule/timeline
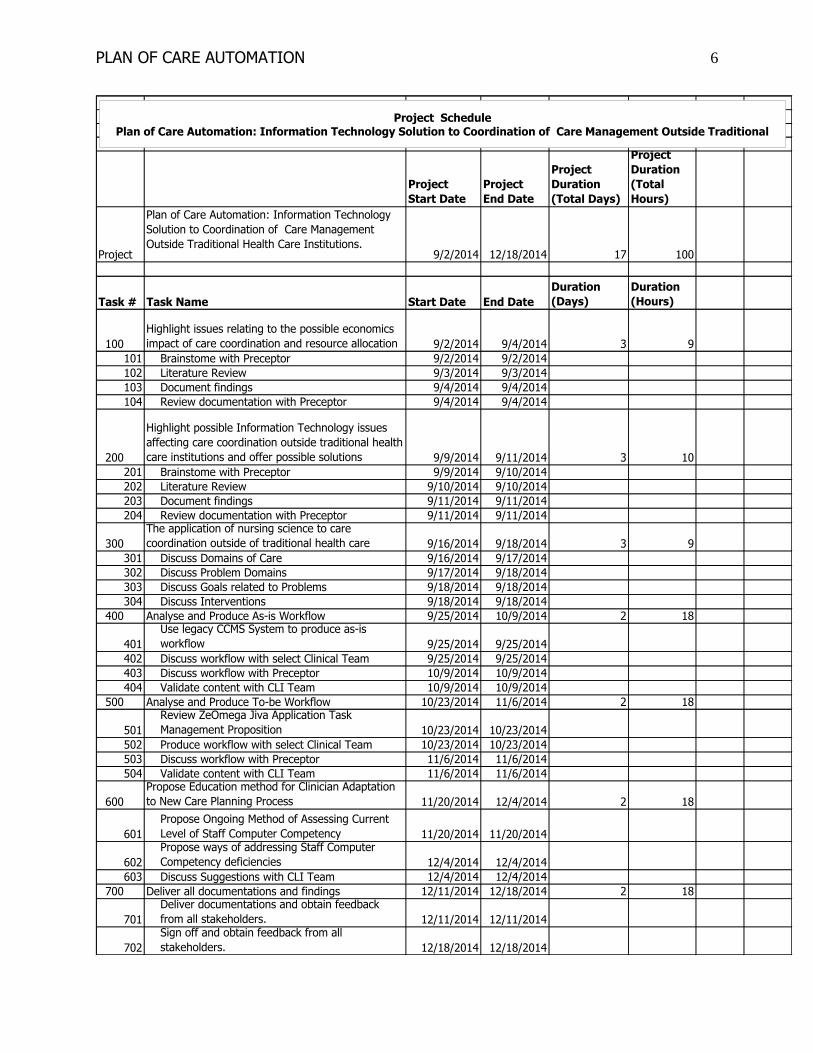
Work Breakdown Structure (WBS) is a technique used for organizing and subdividing all
the tasks and deliverables attributed to a project into more manageable components (Gido and
Clements, 2012, p107). Deliverables in this project is derived from the scope of the project in
alliance with triple constraints of a project. The following will be the deliverables within this
project: discuss enormous economic impact of care coordination without automation of care
PLAN OF CARE AUTOMATION 5
planning, discuss information technology issues affecting care coordination outside traditional
health care institutions, discuss and relate the application of Nursing Science to the possible
domains of care, and finally using Montefiore Hospital as an example without divulging
proprietary information, I will explain and show the efforts that have been made in the area of
automation of Plan of Care with regards to care management outside traditional health care
institutions.
Project Cost Analysis (Tangible and Intangible Benefits)
Montefiore is planning to implement an application for CMO entity to be used for Care
Management and also planning to implement Epic Application for the Hospital Inpatient and
CMO Utilization Management. The cost of implementing plan of care automation is expected to
be assumed within Care Management project. The automation of Plan of Care has enormous
intangible and tangible benefits. When intervention tasks are automated, clinicians can reach out
to members more effectively and better manage their work load; these will inevitably have a
positive effect on care outcome. More members can be reached within a reasonable time period
when scheduling tasks are automated. The turnaround time is greatly improved between
assigning a member to a care manager and being able to reach out to the member.
Project Monitoring and quality management
Negotiation is ongoing for vendor selection. Staff education will be ongoing and
subsequent meeting with clinical subject matter experts are also ongoing to foster buy-in and
assurance that the system will meet the goals of the clinicians. The ultimate test of quality will
also be established when the clinicians are able to manage their work load more effectively
through the effective deployment of the automated care planning process.
PLAN OF CARE AUTOMATION 6
Project
Start Date
Project
End Date
Project
Duration
(Total Days)
Project
Duration
(Total
Hours)
Project
Plan of Care Automation: Information Technology
Solution to Coordination of Care Management
Outside Traditional Health Care Institutions.9/2/2014 12/18/2014 17 100
Task # Task Name Start Date End Date
Duration
(Days)
Duration
(Hours)
100
Highlight issues relating to the possible economics
impact of care coordination and resource allocation 9/2/2014 9/4/2014 3 9
101 Brainstome with Preceptor 9/2/2014 9/2/2014
102 Literature Review 9/3/2014 9/3/2014
103 Document findings 9/4/2014 9/4/2014
104 Review documentation with Preceptor 9/4/2014 9/4/2014
200
Highlight possible Information Technology issues
affecting care coordination outside traditional health
care institutions and offer possible solutions 9/9/2014 9/11/2014 3 10
201 Brainstome with Preceptor 9/9/2014 9/10/2014
202 Literature Review 9/10/2014 9/10/2014
203 Document findings 9/11/2014 9/11/2014
204 Review documentation with Preceptor 9/11/2014 9/11/2014
300
The application of nursing science to care
coordination outside of traditional health care 9/16/2014 9/18/2014 3 9
301 Discuss Domains of Care 9/16/2014 9/17/2014
302 Discuss Problem Domains 9/17/2014 9/18/2014
303 Discuss Goals related to Problems 9/18/2014 9/18/2014
304 Discuss Interventions 9/18/2014 9/18/2014
400 Analyse and Produce As-is Workflow 9/25/2014 10/9/2014 2 18
401
Use legacy CCMS System to produce as-is
workflow 9/25/2014 9/25/2014
402 Discuss workflow with select Clinical Team 9/25/2014 9/25/2014
403 Discuss workflow with Preceptor 10/9/2014 10/9/2014
404 Validate content with CLI Team 10/9/2014 10/9/2014
500 Analyse and Produce To-be Workflow 10/23/2014 11/6/2014 2 18
501
Review ZeOmega Jiva Application Task
Management Proposition 10/23/2014 10/23/2014
502 Produce workflow with select Clinical Team 10/23/2014 10/23/2014
503 Discuss workflow with Preceptor 11/6/2014 11/6/2014
504 Validate content with CLI Team 11/6/2014 11/6/2014
600
Propose Education method for Clinician Adaptation
to New Care Planning Process 11/20/2014 12/4/2014 2 18
601
Propose Ongoing Method of Assessing Current
Level of Staff Computer Competency 11/20/2014 11/20/2014
602
Propose ways of addressing Staff Computer
Competency deficiencies 12/4/2014 12/4/2014
603 Discuss Suggestions with CLI Team 12/4/2014 12/4/2014
700 Deliver all documentations and findings 12/11/2014 12/18/2014 2 18
701
Deliver documentations and obtain feedback
from all stakeholders. 12/11/2014 12/11/2014
702
Sign off and obtain feedback from all
stakeholders. 12/18/2014 12/18/2014
Project SchedulePlan of Care Automation: Information Technology Solution to Coordination of Care Management Outside Traditional
PLAN OF CARE AUTOMATION 7
PLAN OF CARE AUTOMATION 8
PLAN OF CARE AUTOMATION 9
Project Executing Process
Consultation with CMO clinicians and the vendor will be ongoing in the process of
executing this project. Following the system development life cycle, there will be a period when
super users will be trained on the new process of care planning. The super users will in turn train
the general staff. There will be a process in place to train the incumbent staff on the new
workflow for care planning using the new system when fully implemented. There is a need also
to leverage hands-on self-paced training for reinforcing knowledge of the staff. There will also
be a process in place to train new staff and establish their level of computer proficiency. Plan
will also be in place on how to address deficiency because proper utilization of the automated
tasks and care planning will be dependent upon staff ability to use the system effectively.
Project Communication/Reporting
Communication during the project development is mostly through meetings and emails.
Remote meeting is regularly scheduled to review the status of the project between the vendors,
and other stakeholders.
Ethical and legal considerations
The project is mostly centered on the content of Electronic Medical Record and does not
present information to be shared with outside entity without the consent of the member. Member
is consented to be enrolled in the program managed by CMO. The automation of the Plan of
Care simply provides a better way of performing the necessary task to help provide the best care
for the member. The legal department of Montefiore takes care of all legal issues but the
clinician upon communicating with the member seeks consent for the service to be provided. All
HIPAA and other related regulations are adhered to accordingly.
PLAN OF CARE AUTOMATION 10
Conclusions/Analysis of Project Outcome and Success
Much of the analysis of the outcome of the project will be centered on the delivery of the
product with the automated care plan process. The success of the project will be attributed to a
task driven intervention process where all clinicians can have a portion of their task in their
work-list and also the system can transfer work from one work-list to another using an algorithm
to decide who has the most/least task, absenteeism, and other business level decision factors. The
system will also successfully offer a set of goals and interventions when a problem is identified
for a member. The clinicians will also have proper training on how to use the system and also
show proficiency in utilizing the functions of the system to provide the best care for the
members. Vendor selection is still ongoing for this project. Most project do not succeed because
of ineffective vendor performance. Montefiore is still performing vendor selection. In the United
States, about $275 billion is spent annually on software projects and it is estimated that about
50% of these project encountered more cost than originally estimated and about 23% of these
project fail outright (Chiang & Mookerjee, 2004, p3). This is the reason Montefiore is
reconsidering the original vendor selected, to increase the chances of completing this important
project.
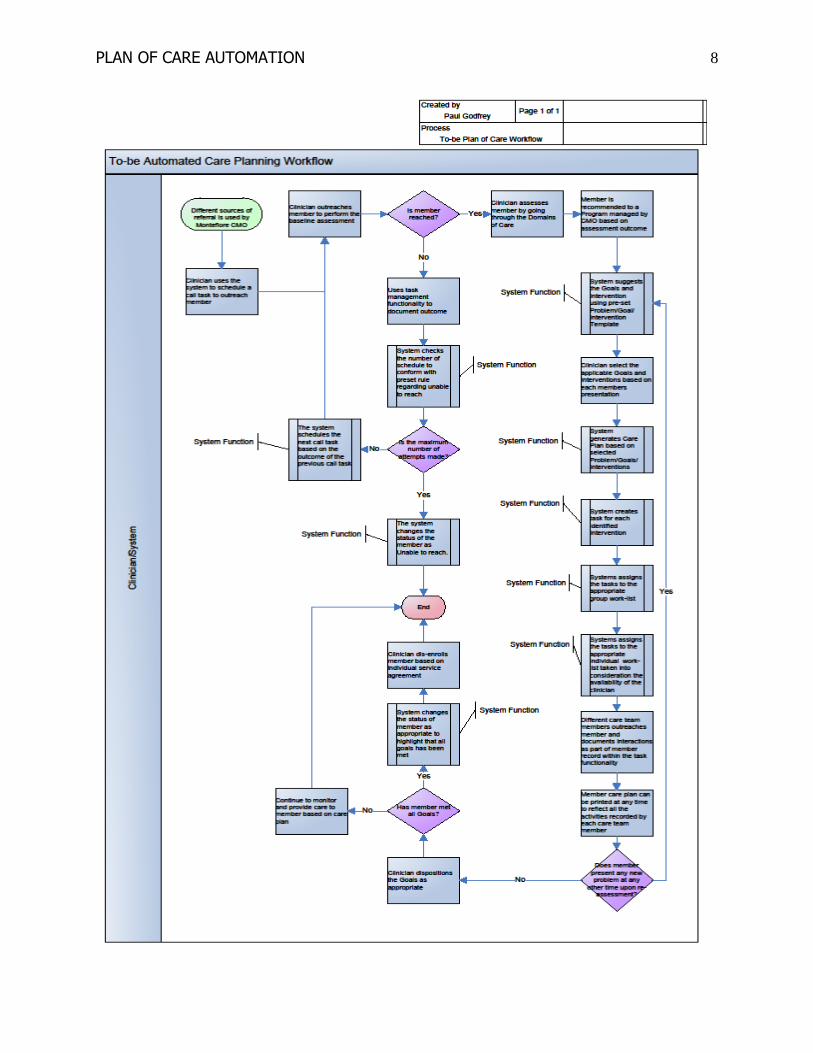
Care Planning
Montefiore anticipated that the automation of care plan will give the clinicians the ability
to update the status of intervention against each goal it is linked with. It is expected that there has
to exist a strong rule not to allow clinicians to close problems without first closing the
intervention linked with the problems. The most daunting task is gathering all the domain of care
and identifying all possible problems, associated goals, and interventions. It is anticipated that a
member can present with many problems from different domains of care (heart failure, diabetes,
PLAN OF CARE AUTOMATION 11
behavioral, access to care, financial assistance, etc.). Each problem can have many goals
associated with it and also many interventions. Interventions are geared towards reaching goals
associated with the problem.
Goals are preconfigured with priority which will help to drive the priority of associated
interventions. The interventions will become tasks which will be assigned to a workbasket. It is
anticipated that the system will not allow a member to be assigned the same problem from the
same domain at the same time. Preventing duplication of item to be placed in the member’s care
plan is an invaluable expected function. “The dynamics of communicating resident needs and the
associated interventions of the written resident care plan to direct caregivers confound the
effectiveness of care planning and delivery” (Adams-Wendling et al, 2008, p54).
Intervention Task Management
Montefiore is anticipating that this system should provide some functionality which will
automate the process of care management after care planning has been established. Montefiore
anticipated that the system should provide the ability to allow configuration of possible outcomes
which will be displayed to the end users upon selecting task. The anticipated system must have
the ability to automatically close certain type of member tasks, for example, intervention, goals,
and problems, when there is a change of status for the member with the outcome of the task
showing the new status. “One of the other benefits of using electronic systems is the potential for
automating activities and processes as well as streamlining clinical workflow.” (Hosker, 2007,
p393)
The system should allow users to filter their assigned tasks and show the status of the task
as either outstanding or completed. The system must have dynamic window popup which should
take the user to a required window or screen to complete a task and toggle back to the original
PLAN OF CARE AUTOMATION 12
screen as needed. The system must also use auto assignment to stratify which workbasket should
contain what type of task, for example, tasks for physicians should be auto assigned to the
physician’s workbasket and tasks for the registered nurse should be auto assigned to the
registered nurse workbasket. “Electronic care planning, assessments and referrals are other areas
which offer opportunities for automation. For example, if a patient has a care plan for a central
venous access device created in the system this can trigger an automatic referral to the
appropriate specialist nurse which reduces the potential for human error or confusion.” (Hosker,
2007, p394) Montefiore anticipates that the system will provide a logic which will move
intervention task from one work queue to another based on set rules. When a clinician is not
available for a reasonable time, the changing of a status for clinician availability will trigger the
system to automatically move intervention task to the other group members in that queue.
Plan of Care Automation as an attribute of a Decision Support System (DSS)
Stair and Ralph (2012) explained that DSS “is an organized collection of people,
procedures, software, databases, and devices used to help make decisions that solve problems”
(p288). Problem solving support is the hallmark of DSS. Manipulation of repository of
information is utilized to offer opinions or possible solutions to a problem. In patient care, most
diseases have established signs and symptoms using evidenced based practice, and when these
signs and symptoms are stored in a system, suggestion could be offered to the user when similar
signs and symptom are manifested and presented. The plan of care automation will follow
similar concept. Information will be linked with logics and suggestions will be disseminated to
the clinicians when similar problems are presented. In that manner, the goals and interventions
options will be presented to the clinicians as well. The ultimate decision is left for the clinician to
make using a DSS.
PLAN OF CARE AUTOMATION 13
Sookyung et al. (2013) presented a research that involved the School of Nursing at
Columbia University, which was conducted in 2002. In this research, it was stated that Advanced
Practice Nurse (APN) students will keep a clinical log which will contain patient encounter data
documentation, patient diagnoses information relating to nursing and medical diagnosis, and then
documentation of nursing interventions using mHealth platform. It was concluded that by
incorporating evidence based practice into the workflow within mHealth DSS, it can invariably
assist nurses in managing a smoking cessation plan of care and potentially expand the nurses’
roles in making referrals and providing helpful information to smokers with the ultimate goal of
encouraging smoking cessation (Sookyung et al., 2013).
Addressing the Clinician’s Resistance to Plan of Care Automation
Nursing process includes assessment, nursing diagnoses, planning, implementation, and
evaluation. Evidenced based practice is the pivot upon which the wheels of nursing process
rotate. A DSS cannot implement the nursing care plan but will offer a suggestion based on
repository of information which supports the decision. Weber (2007) estimated that the first
computer based DSS was developed in the 1980’s. In different practices of nursing, there are
established workflows when certain actions related to a care plan are carried out. These
established workflows can be automated and presented as a DSS to help the nurse in making
decisions relating to patient care effectively. Wills et al. (2010) explained that “a variety of
systems and technologies support knowledge creation in the clinical environment, including
neural networks, data mining techniques, Bayesian methods, and many others. These
technologies make it possible for knowledge to be created from disparate data sources and used
to support the clinical processes of diagnosis, treatment, monitoring and prognosis” (p569).
PLAN OF CARE AUTOMATION 14
User initial involvement in the development process is critical towards creating an
environment where migration to the new system could be with minimal resistance. User
confidence level is increased with proper migration plan. Change is never a seamless process but
detailed training plan and supportive user manual increases the user confidence level and the
ability to be productive with minimal resistance. “Every executive is responsible for ensuring
the highest quality of care provided in the most efficient manner, therefore, planning for any
restructuring must seriously consider plans for concurrent efforts to develop and maintain staff
competencies” (Miller & Arquiza, 1999, p49). The quality of care has a direct relationship with
the efficiency of the process. The process is improved with automation which helps to streamline
the workflow and remove redundancies and unnecessary process bottlenecks, which contributes
to waste. Limited resources demand that scale of preference and opportunity cost analysis must
be done in order to maximize resource output. Cost containment can be achieved when DSS is
properly utilized and the users can see the need for improved process.
The CLI department in CMO is tasked with assessing the competencies of the nursing
staff and providing proper training to bridge the identified gaps and foster productivity. Explain-
show-hands-on approach is highly utilized in a classroom setting for ongoing nursing staff
training. With respect to implementing a new system, super users are selected from different
departments within CMO under the guidance and leadership of CLI. “According to MacBride &
Nagle (1996), it is of essence that positive attitudes towards computers be promoted among
nurses if they are to use computers at optimal levels in both educational and practical setting
(Kivuti & Chepchirchir, 2011, p2). Negative attitude towards change is detrimental to successful
implementation of a new system. The automation of a care plan will rely on the clinician’s
ability to use the system options as intended.
PLAN OF CARE AUTOMATION 15
References
Adams-Wendling, L., Piamjariyakul, U., Bott, M., & Taunton, R. (2008). Strategies for
translating the resident care plan into daily practice. Journal Of Gerontological
Nursing, 34(8), 50-56. doi:10.3928/00989134-20080801-11
Chiang, I. R., & Mookerjee, V. S. (2004). A Fault Threshold Policy to Manage Software
Development Projects. Information Systems Research, 15(1), 3-21.
doi:10.1287/isre.1040.0012
Gido, J., and Clements, J. P. (2012). Successful project management, Fifth Edition,
South-Wester Cengage Learning, Mason, Ohio.
Hosker, N. (2007). Exploiting the potential of informatics in health care... last article of
the series. Nurse Prescribing, 5(9), 391-394.
http://www.healthit.gov/providers-professionals/benefits-electronic-health-records-ehrs,
Retrieved 10/7/2014
Kivuti, L. W., & Chepchirchir, A. (2011). Computerization readiness. Online Journal Of Nursing
Informatics, 15(1),
Miller, E., & Arquiza, E. (1999). Improving computer skills to support hospital
restructing. Journal Of Nursing Care Quality, 13(5), 44-56.
Sookyung, H., Hodorowski, J. K., Nirenberg, A., Perocchia, R. S., Staats, J. A., Velez, O., &
Bakken, S. (2013). Mobile Health-Based Approaches for Smoking Cessation
Resources. Oncology Nursing Forum, 40E312-E319. doi:10.1188/13.ONF.E312-E319
Stair, R. & Reynolds, G. (2012). Fundamentals of Information Systems. (6th
Edition).
Boston, MA: Course Technology
Weber, S. (2007). Critical care nurse practitioners and clinical nurse specialists interface patterns
PLAN OF CARE AUTOMATION 16
with computer-based decision support systems. Journal Of The American Academy Of
Nurse Practitioners, 19(11), 580-590. doi:10.1111/j.1745-7599.2007.00262.x
Wills, M. J., Sarnikar, S., El-Gayar, O. F., & Deokar, A. V. (2010). Information Systems and
Healthcare XXXIV: Clinical Knowledge Management Systems--Literature Review and
Research Issues for Information Systems. Communications Of The Association For
Information Systems, 26(26), 565-597.





























