-
Pes Cavus and Pes Planus Analyses and Treatment ABBY HERZOG
FRANCO
The arch of the foot serves as an adaptable, supportive base for
the entire body. This article discusses how the arch of the foot
affects the normal biomechanics of the lower limb. An anatomical
overview of the three components of the arch of the foot is
presented, identifying the medial longitudinal arch as the arch
mainly responsible for related structural problems throughout the
lower limb. Deviations in the normal structure of the medial
longitudinal arch produce unbalanced, functionally unstable
conditions of the foot such as pes cavus or pes planus. Specific
evaluation criteria for both pes cavus and pes planus are
discussed, in addition to the adverse effects these two disorders
have on weight bearing, force dissipation, and normal gait.
Compensatory pronation associated with pes planus is one of the
most common lower extremity disorders seen currently by physical
therapists working in sports medicine, and its causes and related
lower limb disorders are discussed. Most of these structural
deformities can be corrected through the use of various orthotic
devices. Specific guidelines are presented for using both soft and
permanent orthoses, which offer the foot increased shock absorption
and proper structural alignment.
Key Words: Foot, Orthotic devices, Physical therapy.
A functional relationship exists be-tween the structure of the
arch of the foot and the biomechanics of the lower limb. The arch
of the foot provides an elastic, springy connection between the
forefoot and the hindfoot. This relation-ship ensures that most of
the forces in-curred during weight bearing can be dis-sipated
before reaching the long bones of the leg and thigh.
The arch of the foot demonstrates two extremes of anatomical
structural posi-tionthe high arch characteristic of pes cavus and
the flat arch characteristic of pes planus. Although three distinct
arches function to support the foot, the medial longitudinal arch
(MLA) has been found to be the arch of clinical significance in
both of these disorders. Problems and malalignments originat-ing
specifically with the MLA ultimately affect the functioning of the
muscles and joints of the ankle, knee, hip, and low back, all of
which depend on the base of support provided by the MLA.
A strong need exists for physical ther-apists to understand
applied anatomy and biomechanics of the arch of the foot
as it relates to common lower limb dis-orders. Muscular
imbalances, structural malalignments of joints, compensatory
pronation of the foot, and gait abnor-malities often are caused by
pes cavus or pes planus. After a comprehensive evaluation, the
physical therapist can use various orthotic devices to balance the
foot and restore normal function of the lower limb.
ANATOMICAL OVERVIEW The intricate alignment of the bony
structure of the foot, produced by the tarsal and metatarsal
bones and their corresponding ligaments, results in the
interdependent formation of one trans-verse and two longitudinal
arches. These supporting arches are designed to absorb and
distribute body weight and to im-prove locomotion by increasing
speed and agility during gait. The plantar arches provide both
stability and flexi-bility, meeting the different, complex
requirements of the foot at different phases of the gait cycle.1-5
The arches must act as a rigid lever for proper mo-bility, but they
also must be resilient and flexible for adaptation to different
surfaces.
The design of the arches can be under-stood by picturing the
foot as a twisted osteoligamentous plate.2 The anterior edge of the
plate (formed by the meta-tarsal heads), is horizontal and in full
contact with the ground. The posterior edge of the plate (the
posterior calca-
neus), is vertical. The resulting twist forms the longitudinal
and transverse arches. During weight bearing, the plate will
untwist, flattening the arches slightly. As the foot is unloaded of
weight, the resilient arches return to their original shape. The
actual mecha-nism of twisting and untwisting is ac-complished
through motion at the talo-calcaneonavicular, transverse tarsal,
and tarsometatarsal joints that link the bones of the plantar
arches.2
The transverse arch of the forefoot is located immediately
behind the meta-tarsal heads and can be visualized span-ning across
the tarsometatarsal joints, its integrity being maintained by the
wedge-shaped cuneiforms. The middle cuneiform serves as the
keystone of the transverse arch.6 At the level of the metatarsal
heads, the curvature of the arch is reduced greatly because the
metatarsal heads are in alignment, par-allel to the weight-bearing
surface. Also assisting in holding the base of the arch together
are the tendons of the peroneus longus muscle, the oblique head of
the adductor hallucis muscle, and the flexor hallucis brevis
muscle.7
The longitudinal arches, both medial and lateral, are supported
by the plantar ligament arising from the calcaneus and extending
forward to attach to the meta-tarsals near the heads.8 The
longitudinal arch also is supported by the plantar aponeurosis,
which is the dense fascia that spans from the calcaneus to the
Ms. Franco is a student in the physical therapy program, Florida
International University, Tam-iami Trail, Miami, FL 33199. She was
Head Ath-letic Trainer, Barnard College of Columbia Univer-sity,
606 W 120 St, New York, NY 10027, when this study was conducted.
Address correspondence to 8181 Boca Rio Dr, Boca Raton, FL 33433
(USA).
This article was submitted March 27, 1986; was with the author
for revision three weeks; and was accepted July 23, 1986. Potential
Conflict of Inter-est; 4.
688 PHYSICAL THERAPY
-
PRACTICE
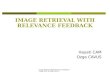
Fig. 1. Supporting structures of the medial longitudinal arch:
1) The tibialis anterior, 2) the tibialis posterior, 3) the spring
ligament, 4) the plantar aponeurosis.
proximal phalanx of each toe.4,9 The lateral longitudinal arch
is formed by the bony structural relationship between the
calcaneus, cuboid, and metatarsals, with the cuboid serving as the
keystone of the arch.10 Both the long and short plantar ligaments
restrict motion at the calcaneocuboid aspect of the transverse
tarsal joint by maintaining the normal twist between the forefoot
and hindfoot.
The integrity of the MLA is preserved by the bony structure of
the foot, strong ligaments, and active muscles (Fig. 1). The MLA is
composed of five bones, with the navicular serving as the key-stone
of the arch.6 The spring ligament, or the plantar calcaneonavicular
liga-ment, is the main support of the MLA.1 As the spring ligament
crosses the trans-verse tarsal joint (the calcaneocuboid and
talonavicular joints), it restricts joint motion that contributes
to the flat-tening of the arch. During weight bear-ing, the spring
ligament offers some elasticity and springiness to the arch.2
Normally, the dorsum of the foot is domed because of the MLA. The
arch is more prominent in the nonweight-bearing position than in
the weight-bearing position. The MLA is reinforced further by the
tibialis anterior and tibi-alis posterior muscles, whose tendons
pull the medial border of the foot up-ward.6 The long flexor
muscles, whose
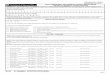
Fig. 2. Normal foot. Weight bearing is dis-tributed evenly on
all five metatarsal heads.
tendons are attached to the foot behind the medial malleolus and
under the MLA, also offer support and act like a sling.7 Evidence
exists, however, that the muscles related to the arch are inactive
during standing and that the ligaments
alone maintain the arched form of the foot.11 The MLA, which is
the arch of clinical significance in both pes cavus and pes planus,
will be the arch referred to in the remainder of this article.
NORMAL WEIGHT BEARING AND FORCE DISSIPATION
In normal weight bearing, forces are transmitted through the
talus to the me-dial aspect of the foot, specifically to the
talonavicular part of the transverse tar-sal joint, causing
pronation of the fore-foot. The weight of the body drives the head
of the talus downward between the calcaneus and the navicular, and
this force is resisted by the spring ligament.7 This downward
motion is accompanied by eversion of the calcaneus at the sub-talar
joint and slight depression of the navicular.4 In the normal foot,
the lat-eral portion of the MLA rests on the ground. This contact,
in addition to the absorption of forces at all five metatarsal
heads, offers additional support to the foot (Fig. 2).
In the properly aligned foot, the cal-caneus is in a vertical
position, perpen-dicular to the horizontal metatarsal heads.
Because the metatarsals must re-main flat on the floor for weight
bearing, their positional relationship with the cal-caneus and thus
the shape of the MLA are controlled by the plantar aponeu-rosis.
Hicks found that the plantar apo-neurosis absorbed about 60% of the
stress of weight bearing.12,13 As the toes are extended during the
push-off phase of gait, the increased tension in the plan-tar
aponeurosis raises the MLA by facil-itating supination (Fig. 3).
This mecha-
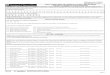
Fig. 3. Windlass effect. Tightening of the plantar aponeurosis
on push-off increases the medial longitudinal arch. This increase
stabilizes the foot during ambulation as weight is shifted onto the
ball of the foot.
Volume 67 / Number 5, May 1987 689
-
nism is known as the windlass effect.13 The pronation that
occurs immediately on weight bearing slightly flattens the MLA,
which aids in the absorption of shock.
PES CAVUS In the extremely high-arched foot
characteristic of pes cavus, weight bear-ing is distributed
unevenly along the metatarsal heads and along the lateral border of
the foot (Fig. 4). This type of disorder causes the foot to be
prone to metatarsal head and calcaneal contu-sions resulting from
the excessive pres-sure of weight bearing. The foot also is prone
to osteophyte formation at the junction of the metatarsal bases and
the cuneiforms. This area is quite promi-nent under the skin and
quite suscepti-ble to damage.8
To identify pes cavus, the patient should sit at the edge of a
tabletop with his foot dangling in a nonweight-bearing position. If
the forefoot is lower than the heel and the arch is high but
depresses on weight bearing, the patient's condi-tion may be
diagnosed as "flexible" pes cavus. If the arch remains high when
the patient is in a full weight-bearing posi-tion, the condition is
"rigid" pes cavus.14
The foot with flexible pes cavus usu-ally displays a callus
under the second metatarsal head. This condition is caused by the
arch's inability to dissipate forces and lack of shock absorption.
The foot with flexible pes cavus responds well to orthotic devices,
which support the MLA, balance the foot, and provide shock
absorption.
The foot with rigid pes cavus poses additional problems. Besides
callus for-mation under the first, second, and fifth metatarsal
heads, these feet have tight, cordlike plantar fascia resulting
from the stresses created by the high arch. The abnormal stresses
produced by the struc-tural problems of a rigid, high-arched foot
also tighten the Achilles tendon and produce claw toes.9
Because of poor shock absorption and a very small weight-bearing
area, feet with either flexible or rigid pes cavus are prone to
heel pain and stress fractures, in addition to various
shock-related pathological conditions that are trans-mitted up the
leg to the knees and hips 8,10,14,15 Both types of pes cavus usu_
ally are accompanied by excessive in-version at the subtalar joint
and supi-nation of the forefoot at the transverse tarsal joint
(Fig. 5).4 Calluses develop under the metatarsal heads when
abnor-mal weight bearing must be accommo-
dated. The forces of weight bearing com-monly are shifted to the
dropped head of the second metatarsal, causing plan-tar callus
formation.16
Treatment for this condition should be directed at providing
arch support, structural alignment, and shock absorp-tion through
the use of orthotic devices and should include stretching of tight
musculature throughout the lower limb. The orthotic device for a
high-arched foot usually is made of soft, flexible materials to
increase foot shock absorp-tion. These softer, flexible materials
often compromise joint control, how-ever, making treatment for this
condi-tion more difficult. The physical thera-pist can further help
the patient with pes cavus by evaluating the lower limb for
muscular imbalances. Tight ankle in-verter and plantar flexor
muscles and weak ankle everter muscles often ac-company pes cavus.
Stretching the tibialis posterior and the gastrocnemius-soleus
complex and strengthening the peroneal muscles will help to balance
the foot's supporting structures in an effort to restore the foot
to its proper alignment.
PES PLANUS
In pes planus, the head of the talus is displaced medially and
plantarward from the navicular. This displacement stretches the
spring ligament and the tendon of the tibialis posterior
muscle,
Fig. 4. Foot with pes cavus. Weight bearing is on the lateral
border of the foot and first, second, and fifth metatarsal
heads.
Fig. 5. Supinated foot with pes cavus. Note the inversion at the
subtalar joint.
resulting in the loss of the MLA.16 Be-cause of this medial
displacement of the talar head, a callus may develop where the
prominent talar head presses against the medial counter of the
shoe. When viewed from the posterior aspect of the foot, the
calcaneus will be everted. The person whose calcaneus is in valgus
will have a relatively flat-arched foot because of the untwisting
of the interconnecting ligaments of the forefoot and the hind-foot.
If the MLA is absent in both seated and standing positions, the
patient has "rigid" flatfoot. If the MLA is present while the
patient is sitting or is standing up on the toes, but disappears
during foot-flat stance, he has "supple" flatfoot, which is
correctable with arch sup-ports.16
The flattening of the MLA disrupts the normal process of weight
bearing and causes functional changes in the foot. Many people with
pes planus dem-onstrate a flat-footed gait with no toe-off,10 often
associated with a large plan-tar weight-bearing surface (Fig. 6).
Symptoms include a pronated foot, a shortening of the everter
muscles of the foot (ie, the peroneal muscles), tender-ness of the
plantar fascia, and laxity of the supporting structures of the
medial side of the foot (ie, the medial ligaments or deltoid group)
and the tibialis poste-rior tendon.17 Over time, this
functional
690 PHYSICAL THERAPY
-
PRACTICE
Fig. 6. Foot with pes planus. Note large weight-bearing surface
with main force ab-sorption on first and second metatarsal
heads.
deformity will develop into a chronic structural deformity, and
abnormal stresses will be transferred to more prox-imal areas,
affecting the knees, hips, and low back.
Pes planus is not necessarily sympto-matic. Many cases of fallen
arches are painless because the foot adapts by changing the shape
of bones and by the stretching of ligaments. The structural changes
that accompany a flat-arched foot, however, affect the normal
bio-mechanics of the lower extremity. Pro-nation, which is a normal
component of gait, becomes exaggerated in the foot with pes planus.
The lack of an arch maintains the foot in a flexible, unstable
position, hindering normal gait and cre-ating a wide variety of
compensatory pronation disorders. An understanding of the
components of pronation and its role during gait is necessary
before the compensatory pronated foot can be dis-cussed.
PRONATION AND GAIT Pronation is an integral component
of the stance phase of gait. Normal pro-nation is 4 to 8
degrees.15,18 Pronation for a foot with pes planus is between 10
and 12 degrees.15 Pronation of the fore-foot, which causes
flattening of the MLA, also flattens the transverse arch by
splaying or spreading the metatarsals. The movements of pronation
and supi-nation are produced when the foot ro-tates around its long
axis, the second
ray. Pronation is a component of a more complex motion,
eversion. Eversion of the forefoot is a combination of move-ments
in all three planes (ie, pronation, dorsiflexion, and
abduction).1,4,5
In the initial phase of gait, the foot contacts the ground in
supination. This inversion of the calcaneus at the subtalar joint
locks the forefoot and provides the rigid lever to absorb the force
of heel-strike. Immediately after heel-strike, the hindfoot
pronates to unlock the trans-verse tarsal joint and create a
loose-packed position in the forefoot. As the posterior aspect of
the calcaneus rolls laterally, the sustentaculum tali of the talus
rolls medially, producing the pro-nation.1119 The direct effect of
this pro-nation is to create a shortening of the lower limb
immediately after heel-strike, while providing a small degree of
shock absorption.3 This change allows the foot greater flexibility
of movement to adapt to changing ground surfaces. When the foot
overpronates during this phase, the tibia also rotates medially,
causing the knee to flex earlier than
normal. This flexion puts abnormal stresses on the quadriceps
femoris mus-cles, which are contracting eccentrically to control
knee flexion.4
In the late stance phase of gait, the foot again must function
more as a rigid lever. This action requires an elevated arch and a
locked forefoot. The foot inverter muscles, in addition to the
sec-ondary actions of the triceps surae and tibialis anterior
muscles, cause the cal-caneus to invert at the subtalar joint. This
inversion produces supination at the transverse tarsal joint and
lateral rotation of the tibia.11 The act of supi-nation causes the
osteoligamentous plate of the MLA to twist and tighten, which
elevates the arch and locks the foot, providing the rigid lever
needed for push-off.
A flat-footed person requires more muscle action than a
nonflat-footed per-son to support and propel the weight of his
body.2 In pes planus, the hindfoot is in valgus (Fig. 7). This
eversion at the subtalar joint creates an untwisted foot with
little or no ligamentous support. If, at heel-strike, this foot
makes impact in the valgus position, the foot is mobile already and
is unprepared to act as a rigid lever to absorb these ground
forces. The foot, therefore, must rely on acces-sory muscles for
stabilization. This ac-tivity fatigues not only the extrinsic
muscles but also the intrinsic muscles of the foot, which are
functioning maxi-mally to compensate for the lack of ligamentous
support.
COMPENSATORY PRONATION The most common pathomechanical
problem associated with pes planus is compensatory pronation.
Overprona-tion and pes planus are key factors in preventing the
subtalar joint from lock-ing during the complex biomechanical
functioning of the lower extremity. This failure of the subtalar
joint to lock cre-ates a hypermobile foot, setting the stage for
structural deformities and problems throughout the lower quarter.
The phys-ical therapist can use three static obser-vations to
detect abnormal pronation: 1) Helbing's sign, the medial bowing of
the Achilles tendon secondary to calca-neal valgus; 2) Feiss's
line, indicating the position of the navicular in relation to a
line drawn between the first meta-tarsophalangeal joint and the
medial malleolus; and 3) the amount and place-ment of callus
formation, usually thicker under the first and second meta-tarsal
heads and the medial, plantar sur-face of the calcaneus.15
Fig, 7. Pronated foot with pes planus. Note the eversion at the
subtalar joint and the medial displacement of the talus and
navic-ular.
Volume 67 / Number 5, May 1987 691
-
A common cause of overpronation is a limitation of muscular
flexibility any-where along the lower limb. A tight triceps surae
causes an early heel-off, which does not allow adequate time for
resupination.15 Tight hamstring, hip flexor, iliotibial band, and
hip medial rotator muscles all produce a toe-out gait. Toeing out
prevents the foot from resupinating before toe-off, leaving a
flexible, unstable foot.
Compensatory pronation is associ-ated often with other lower
extremity disorders. In the patient with a leg-length discrepancy,
excessive pronation of the foot generally is a telltale sign of a
longer limb.15 This pronation is ac-companied usually by early knee
flexion and longer stance time on the longer limb. In runners who
train on paved roads, a functionally longer limb is cre-ated
unconsciously by the "crowning" of the road. The sloped surface of
the road will cause pain on the "downside" leg, the functionally
longer limb. On a small track with sharp-banked curves, medial knee
pain usually will occur on the "inside" leg. Forces are transmitted
up the leg as the downside foot over-pronates in an attempt to make
a func-tionally longer limb shorter.
Another common cause of overpron-ation is forefoot varus (Fig.
8). This disorder can be detected by sitting the patient on a
treatment table with his foot hanging over the edge of the
table-top. With the subtalar joint in a neutral position, the
forefoot will hang in an inverted position at rest. This congenital
deformity originates as a supinated foot, but gravity pulls the
medial aspect of the foot down when making contact with the ground
during weight bearing. The foot thus becomes excessively pron-ated
because of the overcompensation of bringing the foot to the ground.
In addition to the common problems of tight peroneal muscles and
stresses up the lower extremity, which can lead to such problems as
shin splints, Hughes found that soldiers with a greater than normal
forefoot varus are 8.3 times more likely to develop a stress
fracture than soldiers with normal forefoot va-rus.20 A valgus
deformity causes the first metatarsal to contact the ground before
the fifth metatarsal, which forces all loads to the medial aspect
of the foot. The first metatarsal head is twice the size and can
absorb 2.6 times the force of the second metatarsal head.20 The
head and shaft of the second metatarsal of the overpronating foot
with pes planus, therefore, commonly develop
callosities and stress fractures, respec-tively.
Overpronation of the forefoot can lead to subsequent
malalignments of the entire lower limb. In response to
over-pronation, the tibia will rotate medially. In these patients,
the hip adductor mus-cles will be tight, and the external rotator
muscles will be weak. The knee tends to assume a valgus position
when the foot pronates. The distractive forces on the medial side
of the knee lead to medial knee pain. The increased valgus also
affects the proper tracking mechanism of the patella, predisposing
the knee to chondromalacia and other patella track-ing
dysfunctions.1017 Unilateral prona-tion, if allowed to progress to
more ce-phalic joints, will lead to a scoliosis. Bilateral
pronation will increase the lor-dosis of the lumbar spine.21
Decreasing pronation appears to increase the stabil-ity of the
extensor mechanism of the knee and decrease runners' knee
symp-toms.22
Treatment for the overpronated foot with pes planus should
revolve around reducing the stresses that caused the problem.
Long-distance runners with foot, knee, or hip pain secondary to pes
planus should reduce their mileage, or perhaps even temporarily
stop running, to allow the tissues to heal. A muscle strengthening
program to strengthen the anterior and posterior tibialis and
intrin-sic foot muscles might increase the mus-cular support of the
arch, forcing mus-cles to absorb most of the load. Other
treatments include arch taping or sup-ports, ultrasound to heal
damaged tis-sues, stretching of tight muscle groups, and orthotic
devices. An understanding of the principles behind the use of
or-thotic devices will enable the physical therapist to correct
both pes cavus- and pes planus-related problems by realign-ing the
weight-bearing surfaces of the foot.
ORTHOTIC DEVICES After a comprehensive lower extrem-
ity evaluation applying their back-ground knowledge of the
anatomy and kinesiology of normal foot function, physical
therapists should be able to construct foot orthoses to balance the
body's base of support. By following several simple principles and
using read-ily available, inexpensive materials, nor-mal foot
function can be restored in minutes.
An orthosis is a soft, semiflexible or rigid, device whose
purpose is to balance the foot in the neutral position during the
gait cycle. Soft, temporary supports can be made by adding felt and
other soft materials to the insoles of the shoes. These materials,
which will adapt to the contours of the foot, help correct
prob-lems such as abnormal pronation and supination, offer
metatarsal and arch support, and provide better shock ab-sorption.
The main function of an or-thotic device is to provide a
combina-tion of neuromuscular reeducation and a change in body
mechanics in an at-
Fig. 8. A. Normal relationship between the hindfoot and
forefoot. Note that the calcaneus and metatarsal heads are
perpendicular. B. Forefoot varus. The forefoot rests in an inverted
position relative to the subtalar joint, which is in a neutral
position. (Adapted from Wallace.15)
692 PHYSICAL THERAPY
-
PRACTICE
Fig. 9. Structural tripod of the foot: the calcaneus and the
first and fifth metatarsal heads.
tempt to readjust the foot into a more ideal weight-bearing
position. Arch sup-ports support the arch of the foot; how-ever,
they do not balance or offer me-chanical control to the foot.
When making orthotic devices for a patient, several principles
should be kept in mind. Most important, undercorrec-tion is the
preferred treatment protocol. Maximal foot control is unnecessary,
and a balancing effect of the foot is best. Visualize the foot as a
structural tripod, with the heel and the first and fifth
metatarsals as the bases of support (Fig. 9). The purpose of the
orthotic device is to fill in the space between the balanced foot
and the ground. Imagine bringing the ground up to the foot. When
cor-recting an overpronating foot, remem-ber that the foot has a
natural tendency to pronate to some degree, usually 4 to 8
degrees.15,18 An orthotic device should not block all pronation. In
addition, an entire lower quarter examination must be performed
involving an assessment of muscle strength and flexibility and
proper joint function.
An orthotic device consists of two basic parts: 1) the base, the
material you start with, and 2) the post, or the extra material
that is added to the base to
"bring the ground up to the foot." In forefoot varus, the medial
aspect of the foot is posted. Most compensatory pro-nation problems
can be corrected by balancing in this manner.23 In the pa-tient
with anteromedial knee pain caused by excessive pronation, orthotic
devices balance the heel at contact, sup-port the arch at
mid-stance, and allow eversion at the subtalar joint just before
push-off.24 For pes cavus, a 0.25-in* felt heel lift and a lateral
0.12-in forefoot extension between the lateral half of the hindfoot
and the fourth and fifth meta-tarsal heads have been found to be
help-ful.22
Soft, temporary supports wear down quickly, and readjustments
must be made as needed. A wide variety of tem-porary orthotic
devices can be made on the spot with minimal supplies and
time.15,25,26 When making temporary or-thotic devices for a
patient, the physical therapist might want to use athletic tape
either to tape the posting materials into the shoes or to bind the
patient's feet into the desired position. When the cor-rect
temporary support is given and foot function has improved
substantially, a
permanent orthotic device should be custom made.
Permanent orthotic devices are made from a positive model cast
of the foot. The two methods most often used are the foam box
impression and a plaster-of-Paris slipper cast impression, both
taken with the subtalar joint held in a neutral position. The
neutral position of the foot is maintained when the long axis of
the lower limb and the vertical axis of the calcaneus are parallel.
Ther-moplastic, or heat pliable, orthotic ma-terials are molded
onto the positive models to form the base. Postings and more
durable materials then are added to complete the correction.
In unidirectional sports, such as run-ning, an orthosis can help
the foot attain a neutral position at the middle of mid-stance.
Rigid orthotic devices, made from a hard plastic material, are
pre-ferred by runners and by patients for use during walking and
normal daily activ-ities. In sports in which pivoting is in-volved
or multidirectional forces are placed on the foot, the orthosis
must provide arch control while allowing eversion at the subtalar
joint to offer more forefoot flexibility.22 Semiflexible orthotics,
made of leather and more pli-able materials, are preferred by these
athletes.
SUMMARY
The arches of the foot play an integral role in determining the
proper mechan-ics of the entire lower limb. Both pes cavus and pes
planus demonstrate typi-cal patterns of structural deformity.
Through an understanding of lower limb biomechanics, the physical
thera-pist can evaluate and recognize struc-tural imbalances and
other disorders that originate with the arch of the foot. When
detected, various related, symp-tomatic pathological conditions may
be treated and relieved by balancing the foot through the use of
orthotic devices. * 1 in = 2.54 cm.
Volume 67 / Number 5, May 1987 693