Embed Size (px)
Citation preview
11/12/2014
1
Pediatrics
Pertussis:
Trends, Prevention
and Challenges
Flor M. Munoz, MD
Associate Professor
Pediatric Infectious Diseases
Page 1
xxx00.#####.ppt 11/12/2014 2:57:40 PM Pediatrics
Disclosure
I do not have any relevant conflicts of
interest to disclose.
Page 2
xxx00.#####.ppt 11/12/2014 2:57:40 PM Pediatrics
Objectives
1. Epidemiology of Pertussis in US and Texas
2. Current Pertussis Prevention Strategies and
Vaccine Coverage
3. Update on Disease Prevention Strategies:
Maternal Immunization
4. Challenges and Future Direction of Pertussis
Prevention in the US
Page 3
xxx00.#####.ppt 11/12/2014 2:57:40 PM Pediatrics
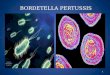
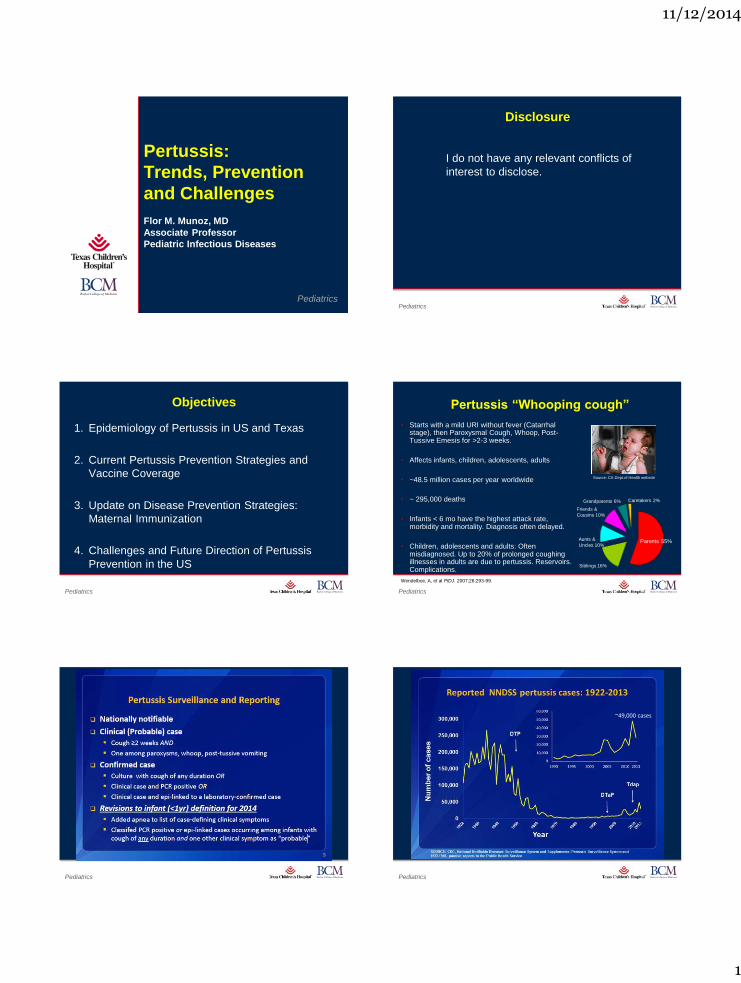
Pertussis “Whooping cough”
• Starts with a mild URI without fever (Catarrhal stage), then Paroxysmal Cough, Whoop, Post-Tussive Emesis for >2-3 weeks.
• Affects infants, children, adolescents, adults
• ~48.5 million cases per year worldwide
• ~ 295,000 deaths
• Infants < 6 mo have the highest attack rate, morbidity and mortality. Diagnosis often delayed.
• Children, adolescents and adults: Often misdiagnosed. Up to 20% of prolonged coughing illnesses in adults are due to pertussis. Reservoirs. Complications.
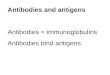
Source: CA Dept.of Health website
Parents 55%
Siblings 16%
Aunts &
Uncles 10%
Friends &
Cousins 10%
Grandparents 6% Caretakers 2%
Wendelboe, A, et al PIDJ. 2007;26:293-99.
Page 4
xxx00.#####.ppt 11/12/2014 2:57:40 PM Pediatrics
Page 5
xxx00.#####.ppt 11/12/2014 2:57:40 PM Pediatrics
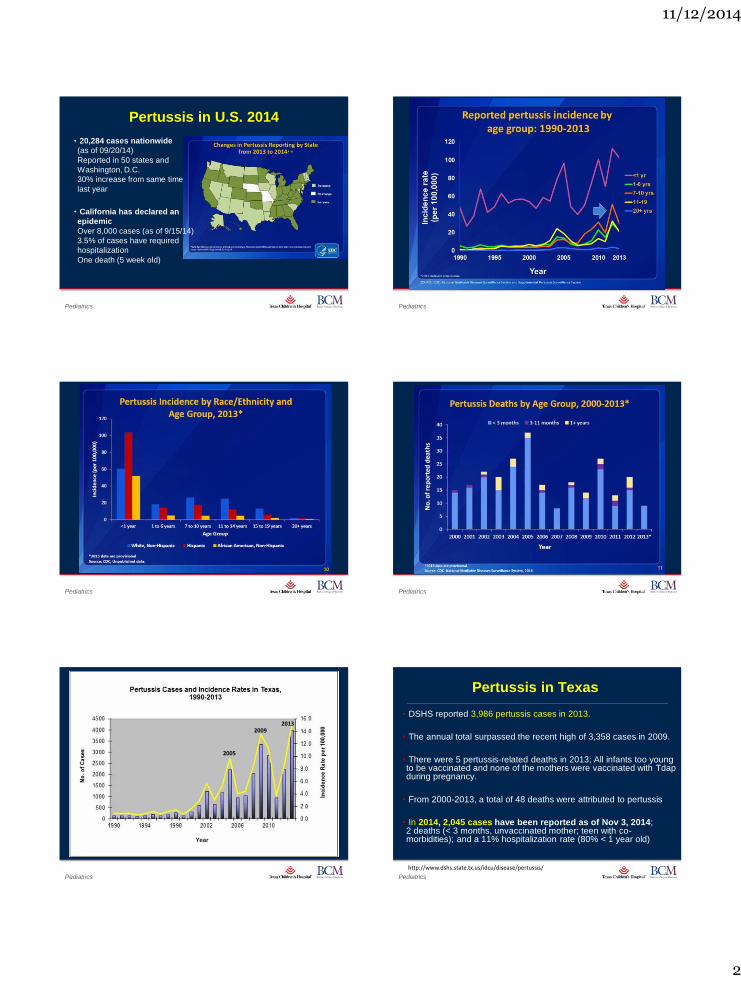
~49,000 cases
11/12/2014
2
Page 6
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
Pertussis in U.S. 2014
• 20,284 cases nationwide
(as of 09/20/14)
Reported in 50 states and
Washington, D.C.
30% increase from same time
last year
• California has declared an
epidemic
Over 8,000 cases (as of 9/15/14)
3.5% of cases have required
hospitalization
One death (5 week old)
Page 7
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
Page 8
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
Page 9
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
Source: CDC.gov
Page 11
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
2009 2009
2005
2013
Page 12
xxx00.#####.ppt 11/12/2014 2:57:42 PM Pediatrics
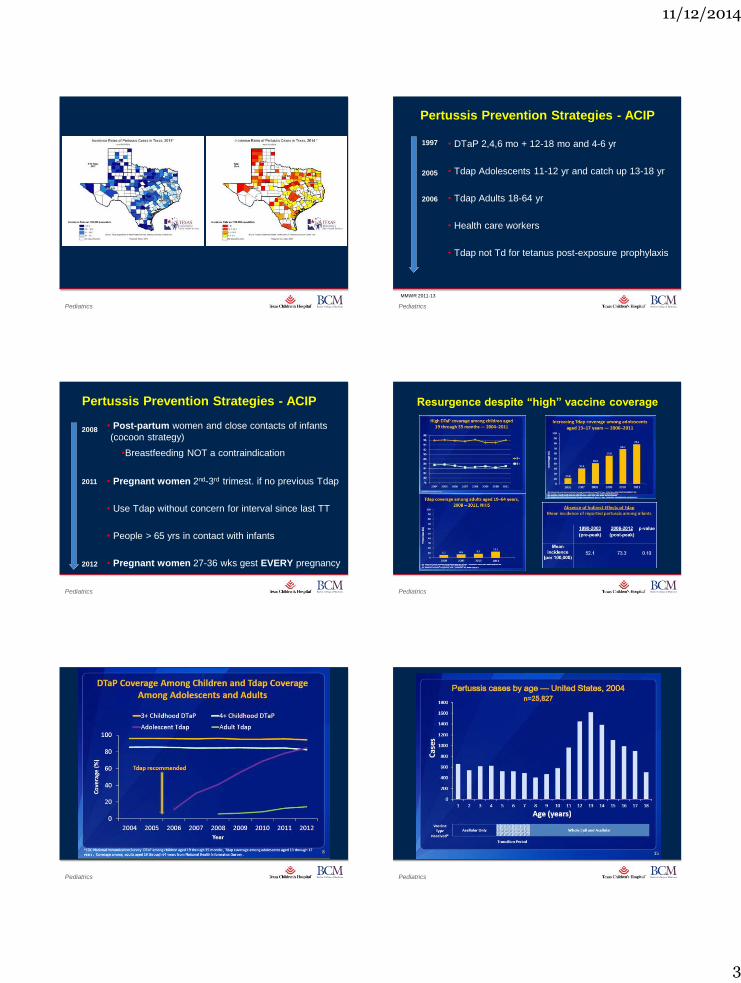
Pertussis in Texas
• DSHS reported 3,986 pertussis cases in 2013.
• The annual total surpassed the recent high of 3,358 cases in 2009.
• There were 5 pertussis-related deaths in 2013; All infants too young to be vaccinated and none of the mothers were vaccinated with Tdap during pregnancy.
• From 2000-2013, a total of 48 deaths were attributed to pertussis
• In 2014, 2,045 cases have been reported as of Nov 3, 2014; 2 deaths (< 3 months, unvaccinated mother; teen with co-morbidities); and a 11% hospitalization rate (80% < 1 year old)
http://www.dshs.state.tx.us/idcu/disease/pertussis/
11/12/2014
3
Page 13
xxx00.#####.ppt 11/12/2014 2:57:43 PM Pediatrics
Page 14
xxx00.#####.ppt 11/12/2014 2:57:43 PM Pediatrics
Pertussis Prevention Strategies - ACIP
• DTaP 2,4,6 mo + 12-18 mo and 4-6 yr
• Tdap Adolescents 11-12 yr and catch up 13-18 yr
• Tdap Adults 18-64 yr
• Health care workers
• Tdap not Td for tetanus post-exposure prophylaxis
MMWR 2011-13
1997
2005
2006
Page 15
xxx00.#####.ppt 11/12/2014 2:57:44 PM Pediatrics
MMWR 2011-13
Pertussis Prevention Strategies - ACIP
• Post-partum women and close contacts of infants
(cocoon strategy)
•Breastfeeding NOT a contraindication
• Pregnant women 2nd-3rd trimest. if no previous Tdap
• Use Tdap without concern for interval since last TT
• People > 65 yrs in contact with infants
• Pregnant women 27-36 wks gest EVERY pregnancy
2008
2011
2012
Page 16
xxx00.#####.ppt 11/12/2014 2:57:44 PM Pediatrics
Resurgence despite “high” vaccine coverage
Page 17
xxx00.#####.ppt 11/12/2014 2:57:44 PM Pediatrics
Page 18
xxx00.#####.ppt 11/12/2014 2:57:44 PM Pediatrics
11/12/2014
4
Page 19
xxx00.#####.ppt 11/12/2014 2:57:44 PM Pediatrics
Page 20
xxx00.#####.ppt 11/12/2014 2:57:45 PM Pediatrics
Page 21
xxx00.#####.ppt 11/12/2014 2:57:45 PM Pediatrics
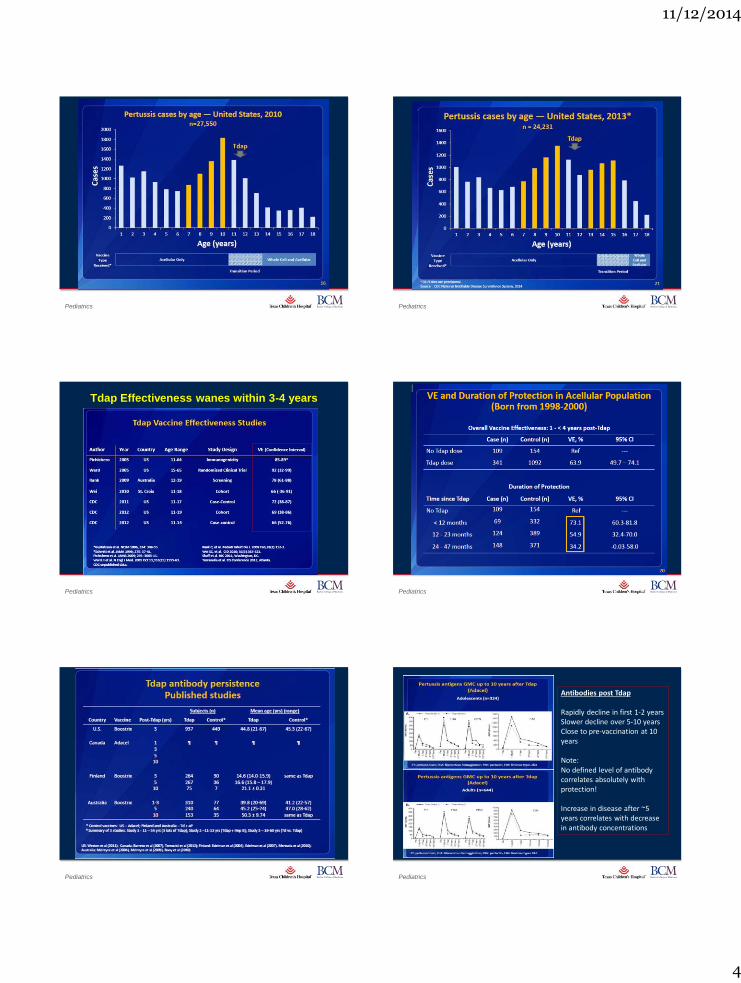
Tdap Effectiveness wanes within 3-4 years
Page 22
xxx00.#####.ppt 11/12/2014 2:57:45 PM Pediatrics
Page 23
xxx00.#####.ppt 11/12/2014 2:57:45 PM Pediatrics
Page 24
xxx00.#####.ppt 11/12/2014 2:57:45 PM Pediatrics
Antibodies post Tdap Rapidly decline in first 1-2 years Slower decline over 5-10 years Close to pre-vaccination at 10 years Note: No defined level of antibody correlates absolutely with protection! Increase in disease after ~5 years correlates with decrease in antibody concentrations
11/12/2014
5
Page 25
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
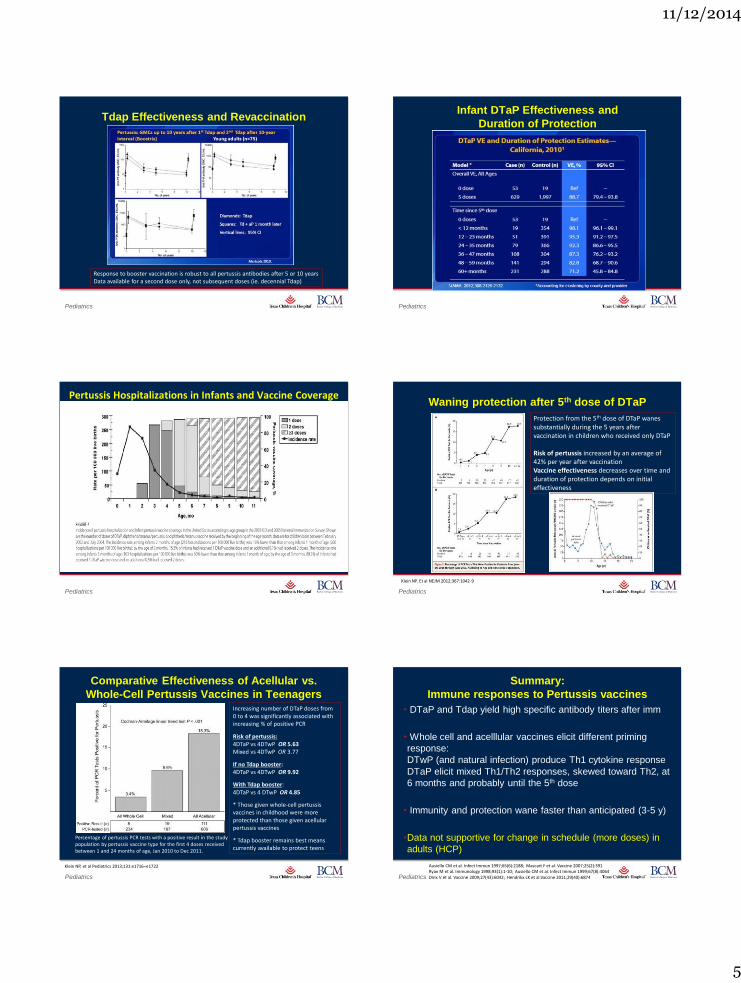
Response to booster vaccination is robust to all pertussis antibodies after 5 or 10 years Data available for a second dose only, not subsequent doses (ie. decennial Tdap)
Tdap Effectiveness and Revaccination
Page 26
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
Infant DTaP Effectiveness and
Duration of Protection
Page 27
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
Pertussis Hospitalizations in Infants and Vaccine Coverage
Page 28
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
Waning protection after 5th dose of DTaP
Protection from the 5th dose of DTaP wanes substantially during the 5 years after vaccination in children who received only DTaP Risk of pertussis increased by an average of 42% per year after vaccination Vaccine effectiveness decreases over time and duration of protection depends on initial effectiveness
Klein NP. Et al NEJM 2012;367:1042-9
Page 29
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
Comparative Effectiveness of Acellular vs.
Whole-Cell Pertussis Vaccines in Teenagers
Klein NP, et al Pediatrics 2013;131:e1716–e1722
Increasing number of DTaP doses from 0 to 4 was significantly associated with increasing % of positive PCR
Risk of pertussis: 4DTaP vs 4DTwP OR 5.63 Mixed vs 4DTwP OR 3.77
If no Tdap booster: 4DTaP vs 4DTwP OR 9.92
With Tdap booster: 4DTaP vs 4 DTwP OR 4.85
* Those given whole-cell pertussis vaccines in childhood were more protected than those given acellular pertussis vaccines
* Tdap booster remains best means currently available to protect teens
Percentage of pertussis PCR tests with a positive result in the study population by pertussis vaccine type for the first 4 doses received between 1 and 24 months of age, Jan 2010 to Dec 2011.
Page 30
xxx00.#####.ppt 11/12/2014 2:57:46 PM Pediatrics
Summary:
Immune responses to Pertussis vaccines
• DTaP and Tdap yield high specific antibody titers after imm
• Whole cell and acelllular vaccines elicit different priming
response:
DTwP (and natural infection) produce Th1 cytokine response
DTaP elicit mixed Th1/Th2 responses, skewed toward Th2, at
6 months and probably until the 5th dose
• Immunity and protection wane faster than anticipated (3-5 y)
•Data not supportive for change in schedule (more doses) in
adults (HCP)
Ausiello CM et al. Infect Immun 1997;65(6):2188; Mascart F et al. Vaccine 2007;25(2):391 Ryan M et al. Immunology 1998;93(1):1-10; Ausiello CM et al. Infect Immun 1999;67(8):4064 Dirix V et al. Vaccine 2009;27(43):6042; Hendrikx LK et al.Vaccine 2011;29(40):6874
11/12/2014
6
Page 31
xxx00.#####.ppt 11/12/2014 2:57:47 PM Pediatrics
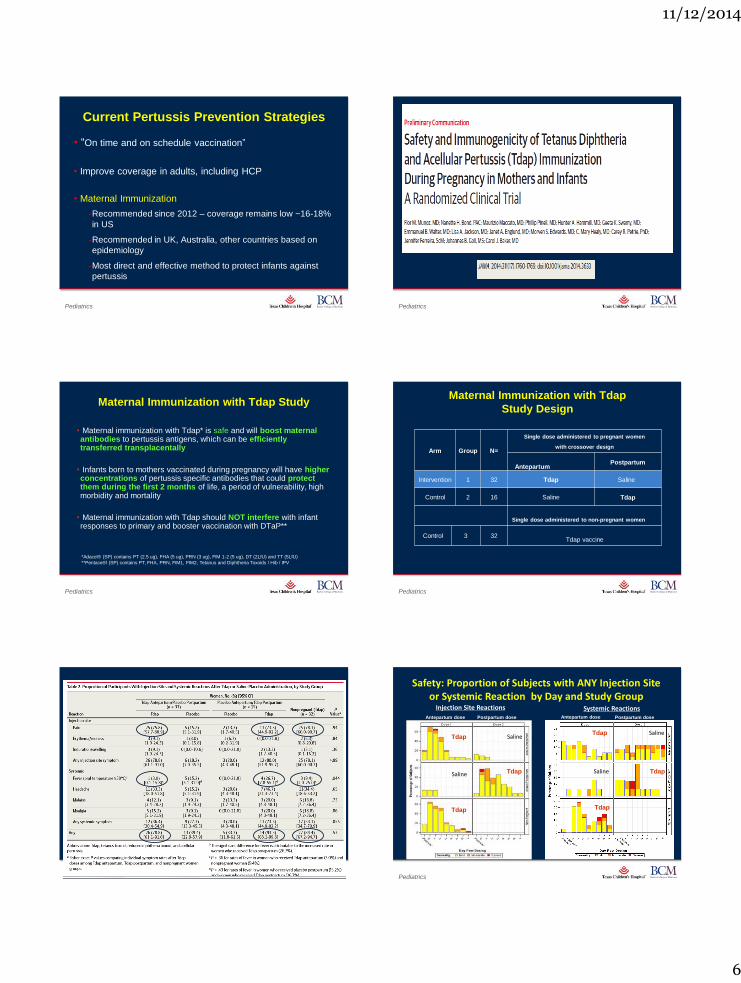
Current Pertussis Prevention Strategies
• “On time and on schedule vaccination”
• Improve coverage in adults, including HCP
• Maternal Immunization
‐Recommended since 2012 – coverage remains low ~16-18%
in US
‐Recommended in UK, Australia, other countries based on
epidemiology
‐Most direct and effective method to protect infants against
pertussis
Page 32
xxx00.#####.ppt 11/12/2014 2:57:47 PM Pediatrics
Page 33
xxx00.#####.ppt 11/12/2014 2:57:47 PM Pediatrics
Maternal Immunization with Tdap Study
• Maternal immunization with Tdap* is safe and will boost maternal antibodies to pertussis antigens, which can be efficiently transferred transplacentally
• Infants born to mothers vaccinated during pregnancy will have higher concentrations of pertussis specific antibodies that could protect them during the first 2 months of life, a period of vulnerability, high morbidity and mortality
• Maternal immunization with Tdap should NOT interfere with infant responses to primary and booster vaccination with DTaP**
*Adacel® (SP) contains PT (2.5 ug), FHA (5 ug), PRN (3 ug), FIM 1-2 (5 ug), DT (2LfU) and TT (5LfU)
**Pentace®l (SP) contains PT, FHA, PRN, FIM1, FIM2, Tetanus and Diphtheria Toxoids / Hib / IPV
Page 34
xxx00.#####.ppt 11/12/2014 2:57:48 PM Pediatrics
Maternal Immunization with Tdap
Study Design
Arm Group N=
Single dose administered to pregnant women
with crossover design
Antepartum Postpartum
Intervention 1 32 Tdap Saline
Control 2 16 Saline A
Single dose administered to non-pregnant women
Control 3 32
Tdap vaccine
Tdap
Page 35
xxx00.#####.ppt 11/12/2014 2:57:48 PM Pediatrics
Munoz FM et al. JAMA May 7, 2014 Page 36
xxx00.#####.ppt 11/12/2014 2:57:48 PM Pediatrics
Safety: Proportion of Subjects with ANY Injection Site or Systemic Reaction by Day and Study Group
Saline
Saline
Injection Site Reactions Systemic Reactions
Saline
Saline
Antepartum dose Antepartum dose Postpartum dose Postpartum dose
Tdap
Tdap
Tdap
Tdap
Tdap
Tdap
11/12/2014
7
Page 37
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
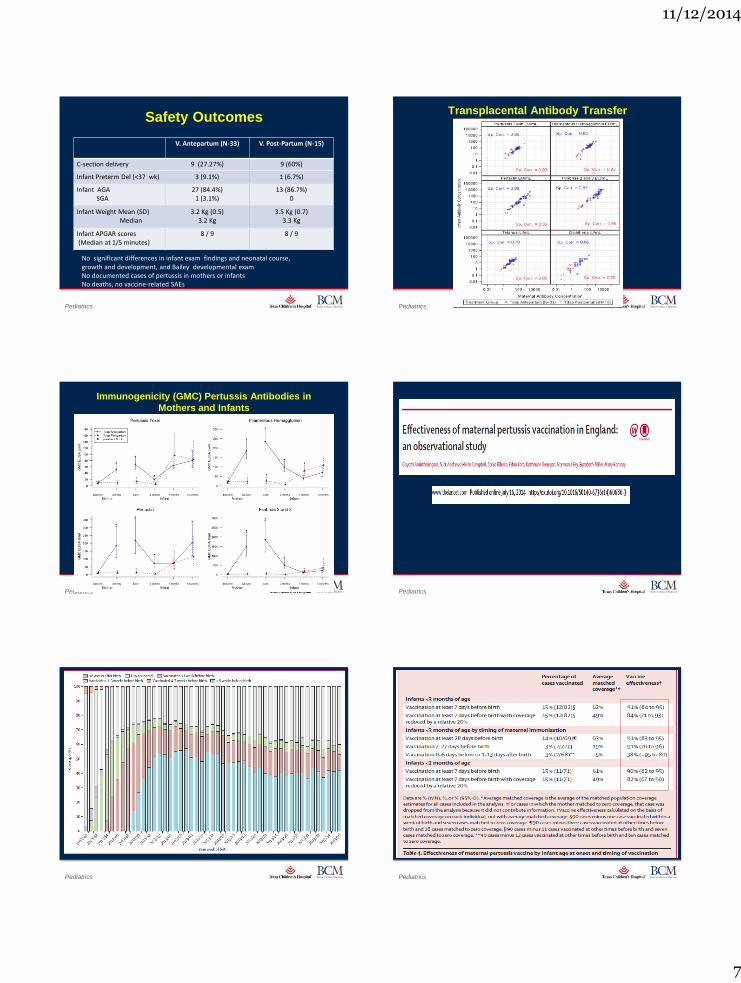
Safety Outcomes
V. Antepartum (N-33) V. Post-Partum (N-15)
C-section delivery 9 (27.27%) 9 (60%)
Infant Preterm Del (<37 wk) 3 (9.1%) 1 (6.7%)
Infant AGA SGA
27 (84.4%) 1 (3.1%)
13 (86.7%) 0
Infant Weight Mean (SD) Median
3.2 Kg (0.5) 3.2 Kg
3.5 Kg (0.7) 3.3 Kg
Infant APGAR scores (Median at 1/5 minutes)
8 / 9 8 / 9
No significant differences in infant exam findings and neonatal course, growth and development, and Bailey developmental exam No documented cases of pertussis in mothers or infants No deaths, no vaccine-related SAEs
Page 38
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
Transplacental Antibody Transfer
Page 39
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
Immunogenicity (GMC) Pertussis Antibodies in
Mothers and Infants
Page 40
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
Page 41
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
Page 42
xxx00.#####.ppt 11/12/2014 2:57:49 PM Pediatrics
11/12/2014
8
Page 43
xxx00.#####.ppt 11/12/2014 2:57:50 PM Pediatrics
Page 44
xxx00.#####.ppt 11/12/2014 2:57:50 PM Pediatrics
Page 45
xxx00.#####.ppt 11/12/2014 2:57:50 PM Pediatrics
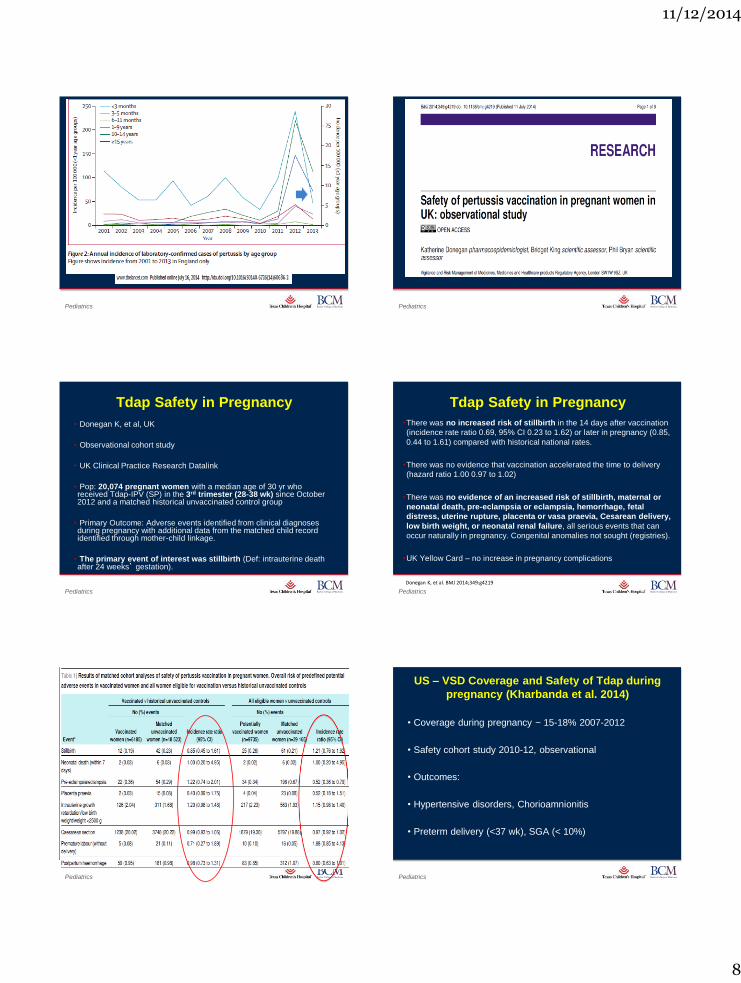
Tdap Safety in Pregnancy
• Donegan K, et al, UK
• Observational cohort study
• UK Clinical Practice Research Datalink
• Pop: 20,074 pregnant women with a median age of 30 yr who received Tdap-IPV (SP) in the 3rd trimester (28-38 wk) since October 2012 and a matched historical unvaccinated control group
• Primary Outcome: Adverse events identified from clinical diagnoses during pregnancy with additional data from the matched child record identified through mother-child linkage.
• The primary event of interest was stillbirth (Def: intrauterine death after 24 weeks’ gestation).
Donegan K, et al. BMJ 2014;349:g4219 Page 46
xxx00.#####.ppt 11/12/2014 2:57:51 PM Pediatrics
Tdap Safety in Pregnancy
•There was no increased risk of stillbirth in the 14 days after vaccination
(incidence rate ratio 0.69, 95% CI 0.23 to 1.62) or later in pregnancy (0.85,
0.44 to 1.61) compared with historical national rates.
•There was no evidence that vaccination accelerated the time to delivery
(hazard ratio 1.00 0.97 to 1.02)
•There was no evidence of an increased risk of stillbirth, maternal or
neonatal death, pre-eclampsia or eclampsia, hemorrhage, fetal
distress, uterine rupture, placenta or vasa praevia, Cesarean delivery,
low birth weight, or neonatal renal failure, all serious events that can
occur naturally in pregnancy. Congenital anomalies not sought (registries).
•UK Yellow Card – no increase in pregnancy complications
Donegan K, et al. BMJ 2014;349:g4219
Page 47
xxx00.#####.ppt 11/12/2014 2:57:51 PM Pediatrics
Page 48
xxx00.#####.ppt 11/12/2014 2:57:51 PM Pediatrics
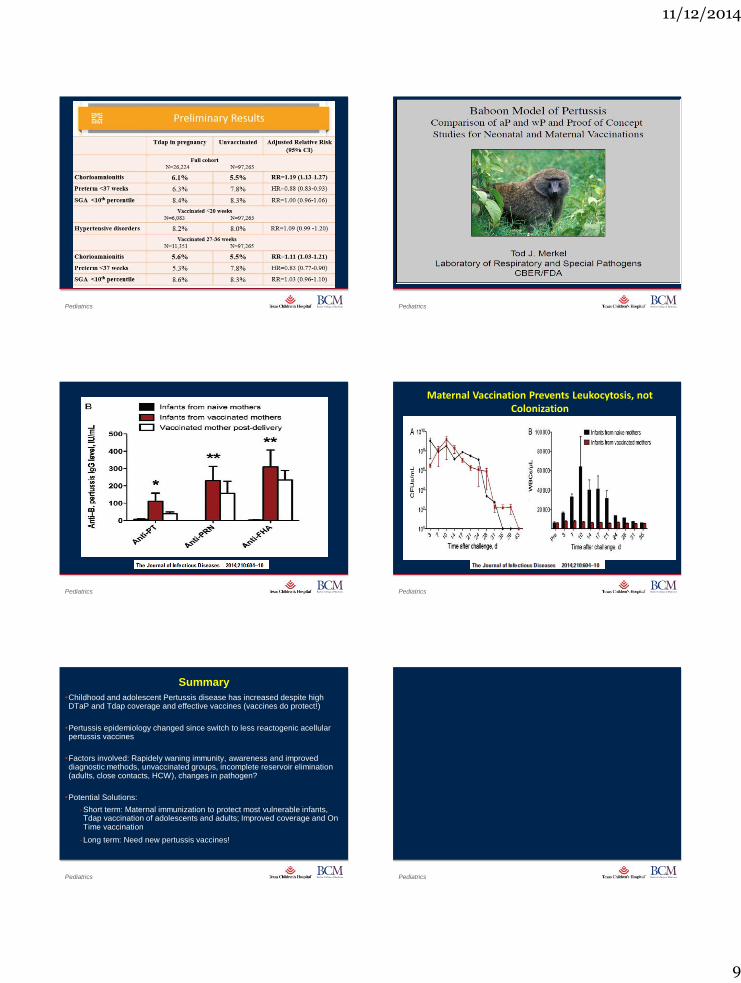
US – VSD Coverage and Safety of Tdap during
pregnancy (Kharbanda et al. 2014)
• Coverage during pregnancy ~ 15-18% 2007-2012
• Safety cohort study 2010-12, observational
• Outcomes:
• Hypertensive disorders, Chorioamnionitis
• Preterm delivery (<37 wk), SGA (< 10%)
11/12/2014
9
Page 49
xxx00.#####.ppt 11/12/2014 2:57:52 PM Pediatrics
Page 50
xxx00.#####.ppt 11/12/2014 2:57:52 PM Pediatrics
Page 51
xxx00.#####.ppt 11/12/2014 2:57:52 PM Pediatrics
Page 52
xxx00.#####.ppt 11/12/2014 2:57:52 PM Pediatrics
Maternal Vaccination Prevents Leukocytosis, not Colonization
Page 53
xxx00.#####.ppt 11/12/2014 2:57:53 PM Pediatrics
Summary
•Childhood and adolescent Pertussis disease has increased despite high DTaP and Tdap coverage and effective vaccines (vaccines do protect!)
•Pertussis epidemiology changed since switch to less reactogenic acellular pertussis vaccines
•Factors involved: Rapidely waning immunity, awareness and improved diagnostic methods, unvaccinated groups, incomplete reservoir elimination (adults, close contacts, HCW), changes in pathogen?
•Potential Solutions:
‐Short term: Maternal immunization to protect most vulnerable infants, Tdap vaccination of adolescents and adults; Improved coverage and On Time vaccination
‐Long term: Need new pertussis vaccines!
Page 54
xxx00.#####.ppt 11/12/2014 2:57:53 PM Pediatrics