Embed Size (px)
Citation preview

ikhs\. Rex & Th, rat.1 1976. \ol. II. pp. 97 101. Pqamon Pr,.s* P+nrd in Great Bntain
PERSUADING PEOPLE TO STOP SMOKING
MARTIK RAW
Addiction Research Unit. Institute of Psychiatry. 101 Denmark Hill. London SE5 SAF England
Summary--Forty smokers attending a chest clmic were given a quebtionnaire designed to mea- sure motivation to stop smoking. The effects of three variables on their smoking level were investigated: (II advice from the chest physician to stop smoking: (2) subjection to a further ‘motivating’ Interview by a psychologist: (3) the wearing of a white coat by the psychologist during his mterview. The questionnaire proved a useful predictor of smoking reduction over a 3-month follow-up period. Advice from the chest physician had a sigificant effect in getting people to reduce smoking over 3 months but the extra ‘motivating’ interview was ineffective. Patients responded to the white coat by reducing their smoking level sygificantl~. irrespective of whether the psychologist wearing the, white coat was advismg them to reduce smoking or not. These results suggest that the advice-giving role of the doctor could be used more effective11 than it currently is in preventive medicine. and that the psychologist has an important role to play in measuring the successful parameters of such advice and hence improving its quality.
The Royal College of Physicians’ report on Smoking and Health (1971) estimated that about 50 million working days are lost each year through the effects of smoking. This is about seven times as many days as were lost in Britain in 1973 through industrial action. The Department of Health estimated that in 1968 there were seven times as many deaths caused by smoking as deaths caused by road accidents. In the same study they noted the value to be gained from cutting down smoking. Reduction of smoking level does reduce health risk (Department of Health and Social Security. 1972). In 1968 about 69”,, of men and 439/, of women in the United Kingdom smoked (Todd. 1969) but the above-mentioned facts have apparently not gone unnoticed. About 509,; of smokers wish to stop smoking (McKennell and Thomas. 1967). This estimate means that there are about 10 million cigarette smokers with some desire to give up smoking.
Much has been attempted to help these unwilling smokers. little achieved. A review of the literature on the modification of smoking behaviour reveals that attempts to help people stop smoking have been largely unsuccessful (Raw. 1974). The only foolproof way to abolish smoking was discovered by the 17th-century Chinese who decapitated people caught smoking (Tooley and Pratt, 1967). Treatments have emerged which can help people achieve abstinence in the short term (Von Dedenroth. 1964a: Russell. 1970; Schmahl. Lichtenstein and Harris. 1973) but long term abstinence is far more difficult to achieve. It depends not only on specific treatment effects but also on complex psycho- logical and social factors. Few of the successful treatment studies show clearly what mechanisms account for their success and there is considerable evidence that ‘nonspecific’ variables (therapist attention, self-monitoring. structured treatment. motivation) play an important role in response to treatment and in final outcome (McFall and Hammen, 1971).
The purpose of the research described in this paper is two-fold. Firstly. a questionnaire measure of motivation (to give up smoking) was given to a sample of chest clinic patients and its predictive usefulness over three months was observed. Secondly. the effect of two aspects of advice-giving upon smoking behaviour was determined. It was hypothe- sized that (a) a motivation measure would predict ability to reduce smoking (b) advice to stop smoking would significantly affect smoking behaviour in the advised direction.
METHOD
Slhjccts
Patients were seen in a chest clinic attached to a general hospital with a catchment area of about 350.000. All patients attending the clinic to see the chest physicians who
97

98 MAKTIN RA%
smoked cigarettes were included in the study. provided they were willing to participate. There were no other criteria of acceptance into the study and only two people refused to co-operate. There were 23 males and 17 females. with an average age of 47 yr. They had been smoking on average for 29 yr and had begun smoking at the age of 18 yr. The average smoking level was 19 cigarettes per day when I first saw them. and 14 cigarettes per day 3 months later; an average reduction of 280, (range -75’1, to + 100%).
Proced we
As patients arrived at the clinic. they were asked if they were smokers and if they were, to co-operate in a study of peoples’ smoking habits. They were then asked to fill in the Eysenck Personality Questionnaire and the Smoking (motivation) Question- naire while waiting for their chest consultation. This part of the procedure was adminis- tered routinely by the nurses at the clinic. Immediately after they had seen the doctor the patients saw me. I asked them all to fill in the Smoking Questionnaire once more, and whether or not the doctor had advised them to stop smoking. Half of them were then given information about (a) the risks involved in smoking and (b) the benefits of giving up smoking in an interview intended to increase their motivation to stop smoking (‘motivated’ condition). The other half were given a placebo interview in which smoking was discussed in neutral terms, At the end of this interview I asked all patients to fill in the Smoking Questionnaire once more. Superimposed on the ‘moti- vated’ condition was a ‘white coat’ condition. For half of the patients I was wearing a white coat (chest clinic standard issue) and for the other half I was not.
The Smoking Questionnaire had a space on it for patients to record their current smoking level. I also asked them in more detail in my interview how much they were smoking at the time. At the end of the interview I asked them to monitor their smoking level for one week on a specially prepared card which was stamped and addressed for return to me. They were told they would be followed up in 3 months. and the 3-month follow-up was conducted by posting them self-monitoring cards. Those who did not reply were followed up by phone or a visit. The dependent variable was percent- age reduction in smoking level-measured in cigarettes per day-at the end of the 3-month follow-up period.
The ‘Personality Questionnaire’ is the latest form of the E.P.I. The latest manual for the questionnaire. by Eysenck and Eysenck is currently in press.
The Smoking Questionnaire was developed to measure motivation to stop smoking. Evidence that a factor of motivation can predict smoking behaviour change was pro- vided by McFall and Hammen (1971) but they gave few details of their instrument. The present instrument is modelled on a questionnaire by Hartrnann (1972). A 20-item version was given to a sample of 90 people, and on the basis of a factor analysis ten items were selected for the instrument, representing two factors. Each item is a statement with which the subject has to indicate agreement/disagreement, scored on a five point scale from STRONGLY DISAGREE to STRONGLY AGREE, yielding a potential range of scores from 0 to 40. The final form of this questionnaire can be found in Raw (1974).
RESULTS
Product-moment correlation coefficients were computed between the Smoking Ques- tionnaire scores and percentage reduction in smoking at 3 months follow-up. For the Questionnaire given to the patients on their arrival Y was 0.43 (p -=c 0.01). For the Ques- tionnaire given at the beginning of my interview I’ was 0.58 (p < 0.01) and at the end of this interview, 0.59 (p < 0.01). All these correlations are significant (see Maxwell, 1970 for a t-test for the significance of a correlation).

Persuading people to stop smoking 99
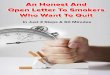
Fig. 1. Differences in per cent reduction in smoking for three conditions (significance levels given below bottom axis). (Note: for the ‘white coat’ group, I wore a white coat while seeing
them; for the ‘no white coat’ group, I did not wear a white coat.
The effects of the experimental conditions on smoking reduction are shown in Fig. 1. Patients advised by the chest physician to reduce or stop their smoking reduced by 39% on average compared with 17% in those not so advised (p = 0.05). The ‘motiva- ting’ interview was not effective. The ‘motivated’ group reduced smoking level by an average of 20% compared with 36% in the ‘non-motivated group @ < 0.05).
The group for which I wore a white coat reduced their smoking by an average of 467; compared with 9% in the non-white coat group (p < 0.01). Four of the five who actually stopped smoking altogether were in the white coat group. Unfortunately the white coat condition was contaminated by two variables, age and sex. There were more males in the white coat group and this group was also older (54 yr compared with 42 yr). Age and sex were intercorrelated, the males being older. Both age (1. = 0.48) and sex (1. = 0.40) were correlated with smoking reduction, therefore an analysis of covariance was performed to look at the effect of the white coat condition on smoking reduction with age and sex taken into account. Table 1 shows that the white coat manipulation was still effective when age and sex were accounted for (p < 0.035).
DISCUSSION
Accuracy/honesty of the patients’ report of their smoking level was assumed in this study. However, they might reasonably have been expected to underestimate their smok- ing level in this situation. In addition, self-monitoring of behaviour has some reactive properties dependent on the instructions given (McFall. 1970; McFall and Hammen, 1971). The only attempt made to cope with this problem was the use of the Personality Questionnaire Lie scale. Since the correlation between Lie score and low smoking level was fairly similar at baseline and at follow-up I am arguing that any underestimation of smoking level was constant. There are, of course, weak assumptions in that argument and it is offered as a suggestive comment rather than an infallible proof.
Table 1. The analysis of covariance for the white coat effect with age and sex as covariates. The dependent variable is per cent reduction in smoking
Variables eliminated F d.f P
None 9.09 1.36 < 0.002 Age 5.52 1.35 <O.OlO Sex 3.53 1.35 < 0.034 Age and sex 3.45 1.34 < 0.035
The Lie scale of the Personality Questionnaire was correlated with smoking level at baseline (-0.34, p < 0.05) and at follow-up (-0.26. p > 0.05).

loo MARTIV RAW
It was noted in the introduction that there is a very large number of cigarette smokers who wish to stop smoking. but for whom little help has been forthcoming. This is partly because there are so few resources available to help them. Smoking withdrawal treatment is offered by a few research psychologists, a few private practitioners and a few clinics run by enthusiastic doctors usually in conjunction with local Authorities. For this reason. the positive correlation between the Smoking Questionnaire scores and smoking reduction is considered to be useful. If reasonably large clinics could be set up (preferably community based; in Health Centres for example) the Question- naire could be used routinely as a screening measure. Only the most motivated 5 or IO”. would receive help (or whatever percentage could be coped with). thereb!, saving wasted resources on treating ambiguously motivated people who would relapse anyway. We could also concentrate effort to motivate the unmotivated.
A second major consequence follows from the observation above about lack of resources. Because we cannot treat all the smokers who need help we must do whatever we can to help them without actually offering treatment. The help envisaged is the giving of advice. The results of the experimental manipulations on smoking reduction confirm Williams’ (1969) report that routine advice given b! a doctor can achieve a great deal. All patients of chest clinics will have seen their General Practitioners long before they had to see a specialist. The GP is in a strategic position. and this result shows that simple advice can achieve results.
The white coat result shows one of the characteristics of the advisor which can be manipulated to increase the effectiveness of the advice. I interpret this result as showing that the white coat confers an aura of authority and credibility on the advisor (in this study all the chest physicians wore white coats all the time). It throws a little light upon the predilection of medics for white coats. perhaps. The strength of the result was a little surprising to me. As far as I know such an effect has never before been demonstrated in the therapeutic setting, although social psychologists have shown the relevance of dress and appearance in gaining co-operation (Raymond and Unger, 197 1: Schiavo. Sherlock and Wicklund, 1974). Appearance of the therapist can now be included as another known and potent ‘non-specific’ variable in treatment.
The uselessness of the ‘motivating’ interview was disappointing. It may be that after seeing the doctor the patients’ minds were on other things. What is more likely though is that irrespective of what was said in the interview they perceived it. and the whole chest clinic environment as an anti-smoking one and perceived me as an ‘expert’ on smoking and ~/KVY@C against smoking. Some evidence for this interpretation comes from the observation that (in the analysis of covariance) there was no interaction between the white coat effect and the motivating interview effect. In other words. the white coat was effective in reducing smoking irrespective of whether the interview was ‘motiva- ting’ or placebo.
To sum up. it has been shown that simple routine anti-smoking advice given by chest physicians can significantly affect peoples’ smoking behaviour. The way the person perceives the advisor, for instance whether or not he is wearing a white coat, affects that person’s response considerably. These points imply that further use might be made of the potential advice-giving role of the General Practitioner. since he can reach the maximum number of people for the minimum cost. in the community.
-1~~~,to1~/r,~/~/[,,11~,1rr.~~ Sincere th;unks arc extended to Dr. R. Fanthorpe. Dr. S. Rachm;m. Dr. M. A. H. Russell. Prof. E. Lichtcnstcm. Dr. P. Nicholls, Miss T. Banford. Mrs. A. Glenny. Mrs. P. Enge and the nurses of the chest clinic for their help in this research.
REFERENCES
DHSS f 1Y721 .Sulo!iiry trrrtl Hctrlth. DHSS. London. HAKTMAYY PAI I. (1Y72) A study of attitudes in industrial rehabilitation. Occupcrriorurl P.sr~cho/. 46. X7--97. MASW LL A. t. f I Y70) Brr.vc~ Sllrri.\rrc.\ iu Bc/~rrriourd Kc.wLII.~~/I. Penguin. Harmondsworth. MC’FALL R. M. (1970) Effects of self-monitoring on normal smoking behaviour. J. mdt. dirr. Psycho/.
35. I?5 142.

Persuading people to stop smoking 101
MCFALL R. M. and HAMME~Y C. L. (1971) Motivation. structure and self-momtoring: role of nonspecitic factors in smoking reduction. J. corlsulr. c/i!]. Ps~chol. 39. X&86.
MCKENNELL A. C. and THOMAS R. K. (1967) Adults’ md Adolrscem’ Stnokirlg Habits md Attitudes (Govt. Social Survey). H.M.S.O., London.
RAW MARTIN (1974) Motivation in smoking withdrawal. Unpublished dissertation. University of London. RAYMOND B. .I. and UNGER R. K. (1971) Effects of deviant and conventional attire on co-operation. Proc.
Am. Psychol. Ass. 6. 357-358. ROYAL COLLEGE OF PHYSICIANS (1971) Smoking arld Health Now. Pitman. London. RUSSELL M. A. H. (1970) Effect of electric aversion on cigarette smoking. Br. med. J. 1. 82X6. SCHIAVO R. S.. SHERLOCK B. and WI~KLUND G. (1974) Effect of attire on obtaining directions. Psn-ho/. Rep.
34. 245-246. SCHMAHL D. P.. LICHTENSTEIN E. and HARRIS P. E. (1972) Successful treatment of habitual smokers with
warm smoky air and rapid smoking. J. co~~sult. cli~r. Pspchol. 36. 105-I I I. TODD G. F. (Ed.) (1969) Statistics OJ Sntokiny in the L’rlitrd Kirlydorn. 5th edn. Tobacco Research Council.
London. TWLEY .I. T. and PRATT S. (1967) An experimental procedure for the extinction of smoking behaviour. Ps~~chol.
Rec. 17. 209-218. VON DEDENROTH T. E. A. (1964a) The use of hypnosis with tobaccomaniacs. Am. J. clirr. Hypr~osis. 6. 32633 I
(a). WILLIAMS H. 0. (1969) Routine advice against smoking. A chest clinic pilot study. Pructitionrr 202. 671-676.