Embed Size (px)
Citation preview


Personalized Medicine and Patient
Empowerment

Positive, 73%
Negative, 13%
Don't Know, 14%
Personalized Medicine Will Have Positive Impact
Personalized medicine refers to testing and treatment customized to an individual’s genetic makeup. Do you think that personalized medicine will have a positive or negative
impact on future health care?
SOURCE: THE PARADE/RESEARCH!AMERICAHEALTH POLLCHARLTON RESEARCH COMPANY, 2004

Don't Know, 4%
No, 34%
Yes, 62%
Americans Support Genetic Testing for Improved Medications
Would you want to be genetically tested to determine which medications might be most effective and safest for you?
SOURCE: THE PARADE/RESEARCH!AMERICAHEALTH POLLCHARLTON RESEARCH COMPANY, 2004

Americans Willing to Share Medical Information
Assuming that there is no way anyone will have access to your identity, would you be willing to
release your health information so that…
69
67
56
27
29
37
4
4
7
Doctors and hospitalscan try to improve
their services
Researchers can learnabout the quality ofhealth care, diseaseand prevention, and
related issues
Public health officialscan scan for
bioterrorist attacks
Yes No Don't KnowSOURCE: THE PARADE/RESEARCH!AMERICA HEALTH POLLCONDUCTED BY CHARLTON RESEARCH COMPANY, 2004

Public Trust in Sources of Research Information
As you are probably aware, there are many sources of information about medical and health research issues. For
each of these sources, I’d like you to tell me how trustworthy you think the information they provide is?
96%
95%
95%
93%
92%
89%
83%
56%
55%
53%
Nurses
Pharmacists
Your physician
Medical schools and teaching hospitals
Your dentist
Voluntary health agencies (such as theAmercian Heart Association)
Government agencies (such as NIH and CDC)
Internet
Media sources
Pharmaceutical companies
SOURCE: NATIONAL SURVEY, 2005CHARLTON RESEARCH COMPANY FOR RESEARCH!AMERICA

Clinical Research is ValuableHow do you perceive the value of clinical research? (In
clinical research, volunteers choose to participate to test the effectiveness of certain treatments, drugs or devices in improving the care of patients and understanding and
preventing disease.)
Don't Know, 3%
Not Much, No Value, 2%
Some Value, 27%
Great Value, 68%
SOURCE: THE PARADE/RESEARCH!AMERICAHEALTH POLLCHARLTON RESEARCH COMPANY, 2004

Don't Know, 4%
Would Not, 18%
Not Likely, 24%
Likely, 54%
Many Would Participate in a Clinical Research Study
How likely would you be to participate in a clinical research study?
SOURCE: THE PARADE/RESEARCH!AMERICAHEALTH POLLCHARLTON RESEARCH COMPANY, 2004

Don't Know, 9%
Less Likely, 9%
Somewhat more Likely,
36%
Much More Likely, 46%
Americans Associate Research and Training With Good Hospitals
If you knew that a hospital was doing research and training medical students and other health professionals, would that
make you more or less likely to think that it was a good hospital?
SOURCE: NATIONAL SURVEY, 2004CHARLTON RESEARCH COMPANY FORRESEARCH!AMERICA

Factors Affection Participation in Clinical Research
How much of a concern would the following factors be in your decision to participate as a volunteer in a clinical research study?
70%
58%
55%
46%
15%
Reputation ofinstitution
Improve health ofself/others
Privacy,confidentiality
Physician'srecommendation
Incentives toparticipate
SOURCE: THE PARADE/RESEARCH!AMERICA HEALTH POLLCHARLTON RESEARCH COMPANY, 2004

Targeting MM CellIGF-1 inhibitorsCD40 AbTelomestatin
Targeting BM Milieup38MAPK inhibitors
Targeting MM Cell &BM MilieuBortezomibThalidomide/Revlimid
Novel Therapies Targeting Multiple Myeloma
MultipleMyelomaCell
StromalCell
Bone Marrow
CellularCross-Talk
After Kenneth AndersonAfter Kenneth Anderson

Novel Therapies Novel Therapies Targeting Multiple Targeting Multiple MyelomaMyeloma
Multiple MyelomaCell Growth
Bone Marrow Stromal Cells
IL-6
Bone Marrow Vessels
ICAM-1VCAM-1
VEGFbFGF
TNFVEGF
Hideshima et al. Cancer Res 61: 3071, 2001Hideshima et al. Oncogene 20: 4519, 2001
Mitsiades et al. Blood 99: 4079, 2002Hideshima et al. J Biol Chem 277: 16639, 2002

Quality Improvement Model Adapted to Individualized Oncology
Waste
Empiric Therapy
Targeted Therapy
Waste due toExcessive Rx
Waste due toInsufficient Rx
OptimalIntervention
ExcessiveIntervention
InsufficientIntervention
Qua
lity

Preempt the Cancer Process
SusceptibilityPre-Cancerous
Changes
Malignant Transformation
Metastatic Progression
Life Span NaturalDeathBirth
Death due to CancerDeath due to Cancer
20052005
Prevent Detect Modulate Eliminate
20152015

Milken InstitutePersonalized Medicine and
Patient Empowerment
April 20, 2005

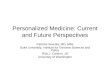
HIV Viral Load and Genotyping TestingAn Early Example of Personalized Medicine
u Death from AIDS in the U.S. climbed to over 50,000 per year until the introduction, in 1994, of protease inhibitors and combination therapy, monitored with viral load testing and followed by genotyping for drug resistance
u The combination became the standard of care and resulted in an immediate reduction in fatalities and improved quality of life for those affected
Source: U.S. Department of HHS HIV/AIDS Surveillance Report 12/01
0
10,000
20,000
30,000
40,000
50,000
60,000
1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
Dea
ths
Dur
ing
Inte
rval
1

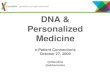
Patient Selection: Potentially Active Therapy Could be Missed
Easy to miss a potentially active new therapy as target prevalence decreases
SIMULATED MODEL
7000 182 months1.5 months (7.5%)All Patients
900 36 months6 months (30%)FISH (+)
Patients Only6 months
Required Sample Size and Study Duration
Actual Benefit(All Patients)
Enrolled Patients
Benefit in FISH (+) Patients
Example: First-line metastatic breast cancerHerceptin data: Median survival ~ 20 months
Source: Genentech2

u Improving current response rates:1
• Alzheimer’s Disease – 30%
• Cancer – 25%
• Osteoporosis – 48%
• HCV – 47%
• Rheumatoid arthritis – 50%
u Avoiding adverse drug reactions:2
• Of 2.8 billion annual prescriptions, 2 million resulted in adverse drug reactions (ADR’s) and >100,000 deaths
• ADR’s could be the 4th – 6th leading cause of death in the U.S., with annual cost of ~$1.3 billion
1 Spear, Heath-Chiozzi and Huff, Trends in Mol Med 7, 201 (2001).
2 Lazarou et al., JAMA, 279, 15 (1998).
Targeted MedicineRecent Technical Advances Make It Possible
3

Drug Development Costs Escalate
0
0.5
1
1.5
2
2.5
1995-2000 2000-2002
Preclinical
Phase I
Discovery
Phase II
Launch
Phase III/File
$1.1B
Discovery
PreclinicalPhase I
Phase II
Phase III/File
Launch
$1.7B
Investment required for one successfuldrug launch (discovery through launch)
CriticalPath
CriticalPath
Costs are becoming prohibitiveu FDA estimates the cost to develop one successful drug will increase to $1.7B –
up from $800MM – $1B just 4 years ago
Investment Escalation per Successful Compound
Source: Windhover’s In Vivo. The Business & Medicine Report. Bain drug economics model, 2003
($ in
Bill
ions
)
4

$803m
$20m$24m
$43m
$316m $403m
$400m
Phase I Phase II Phase III Clinical Failures
Successful NDA
Time Value ofmoney
Total costSuccessful NDA
Cost of Drug DevelopmentCumulative Cost per Step Including Failures to Get 1 NDA
Source: DiMasi et al, JHE 2003
Failures are the main cost component
~4xCost for Ph I-III
Failures
5

Why are NCEs terminated?
Source: Tufts Center for the Study of Drug Development, Hambrecht & Quist and Citigroup estimates
5 – 10%Other
30 – 35%Economics
20 – 25%Safety
35 – 40%Efficacy
6

u Aimed at modernizing preclinical/clinical medical product development
u Many evaluative tools (e.g. animal toxicology) have not changed much in over 50 years
u Need to invest in tools used to translate good ideas into actual products
u This approach will segment market but simplify and speed development process, while making it more informative
FDA’s Critical Path Initiative
Source: FDA7

u Targeted therapy to maximize benefit and minimize potential for harm
u New evaluative tools to assess toxicity and efficiency
u Linked diagnostics/pharmaceuticals (theranostics) to allow better drug selection
u Pharmacogenomic methods to individualize dose
FDA—New Science Provides a Way Forward
Source: FDA8

u Clarify process for adopting new biomarkers and surrogate markers for regulatory use
u Collaborate on development of important biomarkers (e.g., safety markers, imaging techniques)
u Assist in moving specific markers to surrogate status
FDA—Biomarkers and Surrogate Markers
Source: FDA9

u Voluntary submission can help FDA attain greater understanding • Prevents further delays if pharmacogenomics may be
utilized
u Pharmacogenomics is becoming an integral part of the FDA process
u FDA is flexible regarding integration
u FDA focus on utilizing a biomarker to establish scientific foundation• Physiologic, pharmacologic, toxicologic, and clinical
significance
FDA Recent Guidance
10

Pharmacogenomics' Key Applications, According to FDA
Area is ripe for investigation, but not currently done.Study of marketed drugs developed without PG information
Some clinical applications of this are emerging.Assess completeness of response to treatment
We don't really understand this phenomenon well. All AIDS patients are now genotyped for likelihood of developing drug resistance before going on therapy and before they become resistant.
Monitoring for development of drug resistance
Response to treatment. Widely done, particularly in life-threatening diseases such as AIDS and cancer, using traditional and some new markers. Genotyping is emerging as important here.
Therapeutic monitoring
This field is completely unexplored at present. Co-development may be very important to improve risk/benefit profiles of drugs.
Identify individual risk for side effects
This is a huge area of interest, with near-term applications. Currently can be done using metabolic markers, which generally provide insight but are not necessarily definitive as other proteins in the body also influence correct dosage. Will expand in future.
Individualize dose
This is an emerging application in cancer.Identify potential responders/ non-responders
Addresses important need to differentiate diseases better, but this doesn't necessarily dictate one treatment over another.
Diagnose disorders more precisely
Status/Impact on Drug UseApplication of PG
Source: Talk by Janet Woodcock & other FDA officials at FDA/Drug Industry Association meeting on July 29, 2004
11

u Shorter and smaller human clinical trials
• Faster clinical development and FDA turnaround
u More rapid uptake with managed care
u Lower marketing costs
u Easier reimbursement
u 12 years of effective patient life vs. 7 – 10 years
Why Personalized Medicine Should Be Embraced
12

Cancer Treatment DecisionsDisease Progression and Drug Response
DiagnosedPatients
Test for drugresponse
andprogression
Slow progressors/Non-responders
Slow progressors/Responders
Fast progressors/Responders
Fast progressors/Non-responders
Treat immediately
Consider delayingor changing
treatment
New therapies
Source: Celera13

uBlockbuster model being re-assessed
uEvery pharmaceutical and biotechnology company thinking about it• Difficult to do retrospective analysis
uBest if integrated early in drug development
uA fall-back strategy: can it save compounds?
Personalized Medicine Observations
14

u Is there a true benefit to checking all patients with an expensive test(s) to predict rare events
• May get a relative risk
• Primary care doctors not trained to handle these tests
u Is a marker or mutation a smoking gun for primary care?
• Will probably require multiple markers
u Could Tysabri have been avoided?
• Unlikely but patient stratification/monitoring may rescue it
Personalized Medicine Observations (continued)
15

u If Merck utilized markers to stratify patients according to potential cardiovascular complications, sales would have been much less
u Primary care—not the initial target of personalized medicine
u Many people respond differently to VIOXX (platelets, blood pressure, oxidative stress)
u Maybe look at simple blood or urine tests to find a signal or imaging to exclude patients?
u Most extensive pre-market clinical work until then marketed NSAIDS
• No signal of cardiac events in pre-market activities
Personalized Medicine and VIOXX
16

u Specialty fields
• Life threatening diseases
– Significant adverse affects
– Critical to avoid major toxicity and enhance response rates
– Beginning to understand the genetic patterns
u Primary care
• Not life threatening
• Lower disease severity/impact
• Multifactorial and complex mechanisms
• Genetic pathways not well understood
Near-term Benefits of Personalized Medicine
17

u Regulatory guidance for data in drug applications
• FDA approval of diagnostic tests/platforms
u Developing robust diagnostic tests and platforms and data analysis packages that can be used easily by physicians to tailor drug therapy and dosage
u Overcoming pharma/biotech companies’ fear that targeted medicine could limit blockbuster potential of future therapies
Challenges of Pharmacogenomics
Source: Baird Equity Research and Citigroup18

u Cost-benefit analysis by hospitals and clinics
• Reimbursement issues by payors such as gov’t and insurance companies
u Ethical issues of patient stratification
• Privacy issues of genetic data
• Potential repercussions of future insurability—discrimination
Challenges of Pharmacogenomics(continued)
Source: Baird Equity Research and Citigroup19

u Pre-Vioxx, discussion that statins and other categories were headed to OTC
• Zocor available “under the counter” in the UK
• Most Americans who need a statin don’t take one
• Many who do, discontinue
• FDA officials have been quoted that the benefit to risk ratio is strongly in favor of switching a statin to OTC
Consumer Empowerment
20

uGetting, filling, and re-filling a prescription is a major barrier
uWe may see anti-obesity, BPH, respiratory, and even hypertension drugs get switched from Rx to OTC
uOne big pharma is planning a low dose OTC and high dose Rx from scratch
• Advertise the OTC to the public to drive Rx sales, as DTC may get banned
Consumer Empowerment (continued)
21

©2004 Burrill & Company. Confidential & Proprietary.
37
G. Steven Burrill, CEO
Burrill & Company
Milken InstituteGlobal Conference
April 20, 2005
Comments on
Personalized Medicine

©2004 Burrill & Company. Confidential & Proprietary.
38
US, European, Canadian & Australian Biotech
$13.8 B
81
7,440
470
$0.6 B
$1.7 B
Canada
$5.0 B
58
6,393
226
$0.1 B
$1.0 B
Australia
$25.6 B$400.5 BMarket Capitalization
96356Number of Public Cos.
32,470146,100Number of Employees
1,8781,473Number of Companies
$4.2 B$16.8 BAnnual R&D
$7.5 B$59.5 BSales / Revenue
EuropeUSA
Source: Burrill & Company, Ernst & Young

©2004 Burrill & Company. Confidential & Proprietary.
39
A New Revolution is Taking Place . . . Systems Biology
§ Taking whole-genome biology to the next level
§ Integrated understanding of cellular components and how they function to create biological systems
§ Computational methods and capabilities to better understand (and predict) complex biological systems . . . and their behavior
§ Understanding of how microbial and human cells respond to environmental changes
§ . . . integrating “wet” biology the “digital” biology

©2004 Burrill & Company. Confidential & Proprietary.
40
Today’s medicine challenge: One size doesn’t fit all

©2004 Burrill & Company. Confidential & Proprietary.
41
Pharmacogenomics shapes the healthcarebusiness in 2000+

©2004 Burrill & Company. Confidential & Proprietary.
42
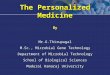
Paradigm Shift
Traditional Medical Evaluation and Record
• Chief Complaint• History of Illness• Past Medical History• Family History• Social History • Physical Exam• Diagnostic Tests• Assessment and Plan
Prospective Evaluation and Record
• Health Profile Summary• Current (immediate) Health
Status• Health Risk Analysis
– Genetic– Environmental– Lifestyle
• 1 year health plan• 5 year health plan
• Risk Assessments• Early Detection• Means for prevention/ early intervention• Individual health plan• Effective delivery system• Effective reimbursement
Requires:
© 2004, Ralph Snyderman

©2004 Burrill & Company. Confidential & Proprietary.
43
Stratifying into risk categoriesDiabetes type 1: What’s becoming possible?

©2004 Burrill & Company. Confidential & Proprietary.
44
What’s Personalized Medicine Really All About?
§ Genetic testing becomes routine
§ Diseases will be understood at a molecular level§ Proteins, pathways, mechanisms
§ Patient populations at risk for ADR will be identified
§ Targeted clinical trials patient selection
§ Healthcare moves to predictive, preventative care with pre-symptomatic Dx and Rx routine

©2004 Burrill & Company. Confidential & Proprietary.
45
What Will Drive Personalized Medicine?
§ Convergence in technology…scientific advances and new technology
§ Patient care and rising consumerism
§ Payors (of all types) have economic incentives§ Government health policy and global spending (e.g.: CMS)

©2004 Burrill & Company. Confidential & Proprietary.
46
Market Trends and Drivers: Revolutionary Technologiesand Evolutionary Practices

©2004 Burrill & Company. Confidential & Proprietary.
47
MDx is at the Center of the New Dx World

©2004 Burrill & Company. Confidential & Proprietary.
48
G. Steven Burrill, CEO
Burrill & Company
Milken InstituteGlobal Conference
April 20, 2005
Comments on
Personalized Medicine

Watch the discussion again or share it.Order this session–and many more–on DVD!
Please visit the DVD Center in the Executive Center to order copies for you and your associates.
Special discount for attendees only for the duration of the event.