Embed Size (px)
Citation preview

Personality Traits and the Classification of Mental Disorders:Toward a More Complete Integration in DSM–5 and an Empirical
Model of Psychopathology
Robert F. Krueger and Nicholas R. EatonWashington University in St. Louis
Personality trait dimensions are related to a wide variety of important life outcomes,such as mortality, physical and mental health, and interpersonal relationships. Never-theless, the diagnostic system with arguably the most influence in mental health settings(Diagnostic and Statistical Manual of Mental Disorders, 4th ed. [DSM–IV]) formallyincludes personality primarily in the form of 10 putatively categorical personalitydisorders. We advocate a more complete and extensive integration of personality infuture DSMs, via the explicit inclusion of an empirically based, dimensional personalitytrait model. To justify this position, we provide a broad review of the ways in whichpersonality traits have proven useful in the description and conceptualization ofpersonality disorders and other mental disorders, as well as in the prediction of keyclinical phenomena. We also discuss the importance of constructing a comprehensivequantitative model of psychopathology based on data, an endeavor that is motivatedand informed by the close conceptual and empirical parallels between personality andpsychopathology.
Keywords: nosology, dimensions, categories, personality disorders, psychometric modeling
There is no question that personality isclosely connected with many major mental dis-orders and other key clinical phenomena (e.g.,Hettema, Neale, Myers, Prescott, & Kendler,
2006; Krueger & Tackett, 2006; South, Eaton,& Krueger, in press). The current classificationsystem with arguably the most influence in clin-ical settings, the Diagnostic and StatisticalManual of Mental Disorders (4th ed.; DSM–IV;American Psychiatric Association, 1994), in-corporates personality into diagnostic conceptu-alization in several ways. First, DSM–IV in-cludes diagnostic criteria for 10 putatively cat-egorical forms of personality pathology labeled“personality disorders” (PDs). In addition tobeing conceptualized as qualitatively differ-ent from most other mental disorders (e.g.,with regard to course), the PDs were placedon a separate axis (Axis II) to ensure thatclinicians would consider their potential pres-ence, even when the symptoms of anothermajor mental disorder were prominent in theclinical picture. Second, the DSM–IV allowsmaladaptive personality traits that do notmeet the level of a PD to be included indiagnostic conceptualizations by allowing theclinician to record such traits on Axis II (al-beit DSM–IV does not provide a specificmodel for conceptualizing these traits, be-yond their appearance as features of the 10PDs). Finally, DSM–IV allows for personality
To see further discussion of the Target Conceptual Article,Commentaries, and Author Response, as well as to contrib-ute to the ongoing dialogue on this topic, please visit ourOnline Forum at http://pdtrtonline.apa.org.
Robert F. Krueger and Nicholas R. Eaton, Department ofPsychology, Washington University in St. Louis.
Robert F. Krueger and Nicholas R. Eaton are now withthe Department of Psychology, University of Minnesota.
We thank Thomas Oltmanns for allowing us access tothe data portrayed in Figure 1. We also thank BenjaminChapman, Andrew Skodol, and Erika Wolf for theirhelpful comments on drafts of the article. Finally, wethank the members of the DSM–5 Personality and Per-sonality Disorders Workgroup (Andrew Skodol, chair, andRenato Alarcon, Carl Bell, Donna Bender, Lee Anna Clark,W. John Livesley, Les Morey, John Oldham, Larry Siever,and Roel Verheul) for their intellectual camaraderie. Thisarticle is being co-published by Personality Disorders: The-ory, Research, and Treatment and the American PsychiatricAssociation.
Correspondence concerning this article should be ad-dressed to Robert F. Krueger, Department of Psychology,University of Minnesota, 75 E. River Rd., Minneapolis, MN55455. E-mail: [email protected]
Personality Disorders: Theory, Research, and Treatment © 2010 American Psychiatric Association2010, Vol. 1, No. 2, 97–118 1949-2715/10/$12.00 DOI: 10.1037/a0018990
97

change to be considered pathological when itis due to a general medical condition.
Through Axis II, DSM–IV provides some in-frastructure for connecting personality and psy-chopathology. However, the fifth edition of themanual (DSM–5) can—and should—incorpo-rate personality to a considerably greater de-gree. In particular, the extensive research liter-ature on dimensional personality traits— ontheir nature, structure, and impact on clinicaloutcomes—should influence the scope and formof DSM–5. More extensive integration of per-sonality traits into the DSM would yield myriadbenefits to conceptualization, diagnosis, andtreatment of mental disorder. In the current re-view, we justify and elaborate this position byreviewing the relevance of personality traits tothe conceptualization of mental disorders andtheir classification, as well as the utility of per-sonality traits in predicting and understandingother clinical phenomena (e.g., treatment-related variables). We also argue for the im-portance of constructing a comprehensive,empirically based quantitative model ofpsychopathology. Quantitative models of per-sonality trait variation have contributed un-equivocal conceptual clarity in personalityresearch, and would have similar utility ifapplied to psychopathology in a comprehen-sive manner that reflects the close links be-tween personality trait variation and risk forpsychopathology.
Personality Traits and theConceptualization of Mental Disorders
Our first goal is to highlight the relevance ofa personality trait model to the conceptualiza-tion of mental disorders. We first examineDSM–IV PDs and then turn to consider othermental disorders.
Personality Traits and DSM–IV PersonalityDisorders
Personality disorder categories versus di-mensions of pathological personality. Themost obvious way in which personality traitsconnect with DSM–IV mental disorders is intheir role as fundamental features of the PDs(for a recent introduction to modern theoreticalunderpinnings of personality trait psychology
and the ways in which traits encompass elicitingcircumstances, see Roberts & Mroczek, 2008;Tellegen, 1991). Although the relevance of per-sonality traits to PDs is essentially axiomatic,the specific PD classification system in DSM–IVhas been criticized on numerous grounds, asreviewed more extensively elsewhere (e.g.,Clark, 2007; Krueger, Skodol, Livesley, Shrout,& Huang, 2007; Trull & Durrett, 2005). First,the PDs are currently defined as 10 categoricalentities, but there is no evidence we are awareof that the latent structure of personality pathol-ogy is best characterized in terms of 10 dichot-omous variables (see Widiger, Simonsen,Krueger, Livesley, & Verheul, 2005). Second,PDs are conceptualized using arbitrary cut-points (e.g., at least five of nine diagnostic cri-teria present indicate the presence of borderlinePD, although there is little to no empirical jus-tification for that particular threshold; Kam-phuis & Noordhof, 2009). Third, PDs have highlevels of diagnostic overlap and comorbidity(e.g., Dolan-Sewell, Krueger, & Shea, 2001), asituation that greatly complicates both clinicalcase conceptualization and research design. Forexample, if the modal patient has “more thanone PD,” which should be the focus of inter-vention and why?
The limitations of the categorical DSM–IVsystem for classifying PDs have led many re-searchers to call for PDs to be reconceptualizedin terms of personality dimensions (e.g., Clark,2007; Frances, 1993; Livesley, Jang, & Vernon,1998; Trull & Durrett, 2005; Widiger, Livesley,& Clark, 2009; Widiger & Samuel, 2005).Widiger and Simonsen (2005) note that the “di-mensionalization” of PDs could be accom-plished in several ways, including simply re-taining the current PD diagnostic constructs buttreating them as ordinal dimensions (number ofdiagnostic criteria met; Oldham & Skodol,2000). Although this approach has the advan-tage of retaining familiar diagnostic conceptsthat have some traction in the literature (e.g.,borderline PD), it has the disadvantage of si-multaneously retaining diagnoses that have re-cruited little to no research or clinical attention(e.g., paranoid PD; Blashfield & Intoccia,2000).
As a result, the means of reconceptualizingPDs that have received the most attention in-volve replacing the existing PDs with an empir-ically derived model of dimensional personality
98 KRUEGER AND EATON

traits. Indeed, this was the focus of an officialAmerican Psychiatric Association–National In-stitute of Mental Health meeting on PDs, orga-nized in preparation for DSM–5 (Widiger et al.,2005). As discussed extensively at that meeting,four to five broad groups of traits have beenidentified by numerous research groups as theleading candidates for organizing the first tier ofthe domain-level structure of personality pa-thology (De Clercq, De Fruyt, Van Leeuwen, &Mervielde, 2006; Harkness & McNulty, 1994;Harkness, McNulty, & Ben-Porath, 1995;Livesley et al., 1998; Markon, Krueger, &Watson, 2005; Nestadt et al., 2006; Tackett,Silberschmidt, Krueger, & Sponheim, 2008;Watson, Clark, & Chmielewski, 2008; Widiger& Simonsen, 2005). Various investigators adoptvarious labels for these domains, but here wewill label the domains as (I) antagonism, (II)disinhibition, (III) negative emotionality, (IV)introversion, and (V) peculiarity. As a short-hand abbreviation, we will refer to this systemas the pathological five model (PFM).
The PFM and the five-factor model (FFM)of personality. The PFM designation is aptbecause these domains can be generally under-stood as maladaptive and extreme variants ofthe domains of the FFM of personality traits(agreeableness, conscientiousness, neuroticism,extraversion, and openness to experience; Costa& Widiger, 2001). With regard to the first fourtraits, antagonism is the opposite of agreeable-ness, disinhibition is the opposite of conscien-tiousness, negative emotionality encompassesextreme neuroticism, and introversion is the op-posite of extraversion.
We should note that, in distinguishing thePFM from the FFM, our intent is not to dimin-ish the importance of the FFM. The FFM is themost influential structural model of personalitytraits, and with good reason: It is supported byan extensive empirical literature (McCrae &Costa, 2008), and it forms the base of the higherorder structure of personality traits (Markon etal., 2005). Indeed, the similarities between theFFM and PFM far outweigh the differences.Nevertheless, our intent in articulating the PFMis to emphasize how the integration of normaland abnormal personality trait structure is anongoing enterprise. Specifically, although thePFM domains generally map well onto FFMdomains, the domain-level resemblance be-tween the two models is not isomorphic in every
respect. This is likely because the FFM was notcreated specifically to organize pathologicalpersonality dimensions (see, e.g., Nestadt et al.,2008). This notable yet imperfect mapping be-tween the PFM and FFM domains points toimportant topics for continued research.1
Peculiarity provides the clearest example ofthe partial isomorphism of the PFM and theFFM and the value of continued research in thisarea. Peculiarity is arguably the least well-understood domain in the PFM, and its relationsto the FFM are complex. A recent study byPiedmont, Sherman, Sherman, Dy-Liacco, andWilliams (2009) nicely illustrates this point.Piedmont et al. described the construction of theExperiential Permeability Inventory (EPI), aquestionnaire designed to assess maladaptive
1 An additional difference between the PFM and the FFMis that the FFM domains are typically conceptualized asbipolar (e.g., extraversion–introversion is conceptualized asa single bipolar trait domain), whereas our intention innaming the PFM domains as we have is to accentuatemaladaptive poles of these domains and to acknowledgethat the PFM domains may not be perfectly bipolar. Bycontrast, Widiger and Mullins-Sweatt (2009, e.g., Figure 2)conceptualize both the positive and negative poles of all fiveFFM domains as maladaptive (e.g., reckless sensation seek-ing is conceptualized as a maladaptive aspect of extremeextraversion). However, a number of the trait placementsthat stem from conceptualizing the structure of maladaptivepersonality as necessarily bipolar and isomorphic with theFFM may be factorially questionable. For example, recklesssensation seeking tends to align more closely with theantagonism and disinhibition (externalizing) domains thanwith the extraversion domain (Markon et al., 2005; Krueger,Markon, et al., 2007).
Another potentially important example is provided bycontemplating the location of compulsive personality traitsin factor space. Widiger and Mullins-Sweatt (2009) placethe traits of perfectionism and irresponsibility at the oppo-site poles of the conscientiousness domain. Yet, when thesetypes of facets are factor analyzed along with other mal-adaptive facets, compulsive qualities such as perfectionismtend to form their own broad domain, with irresponsibilityand similar traits falling in a separate domain encompassingdiverse antagonistic facets (Livesley et al., 1998; Nestadt etal., 2008). The general point is that the empirical structureof maladaptive personality facets is not necessarily isomor-phic with the structure of more normal-range personalitydomains as delineated in instruments designed to assessFFM facets in diverse settings (e.g., the NEO-PI–R; Costa& McCrae, 1992). Nor is the structure of maladaptivepersonality facets necessarily bipolar. As we describe moreextensively in this article using the peculiarity domain as anexample, there is still more to learn about the fine-grainedstructure of maladaptive personality facets and how thisstructure intersects with the structure of normal-range per-sonality facets (cf. Clark, 2007).
99PERSONALITY IN DSM–5

and extreme qualities theorized to lie at both thehigh and low poles of FFM openness. The EPIscales correlated with openness as measured bythe NEO Personality Inventory—Revised(NEO-PI–R; Costa & McCrae, 1992) in ex-pected and meaningful ways, but the EPI wasnot redundant with openness (e.g., the Odd andEccentric subscale of the EPI correlated .36with the NEO-PI–R openness domain score).
One could extend the pioneering research ofPiedmont and colleagues (2009) by workingtoward a comprehensive structural account ofelements of both openness and peculiarity. Thiskind of endeavor could benefit from consideringthe relative locations of specific traits alongbroader domain dimensions in addition to theircorrelational structure. For example, are open-ness and peculiarity part of a somewhat diffuseand hierarchically organized trait domain? Thisis a reasonable possibility inasmuch as the “corefeatures” of openness have been somewhatchallenging to identify unequivocally (John,Naumann, & Soto, 2008). Or are they betterunderstood as falling at different locations ordegrees of severity along one major axis ofvariation? Or are these constructs sufficientlydissimilar that openness and peculiarity shouldnot be regarded as delineating the same domain(see Watson et al., 2008)?
Facets of pathological personality. As theexample of openness and peculiarity illustrates,more narrow and specific (facet-level) dimen-sions can also be identified, and these constructsare subsumed within each of the broad domains.Facets provide an even more detailed account ofa patient’s personality profile. The challengewith facets is to achieve optimal fidelity ofpersonality description by including the “right”number of facets. A system with too manyfacets is potentially unwieldy (few cliniciansmay be enthusiastic about learning or workingwith, say, 40 specific personality dimensions2),yet a system with too few facets lacks the detailneeded for a psychologically rich conceptual-ization of a specific patient (cf. Widiger & Mul-lins-Sweatt, 2009). For example, it is arguablymore useful to understand the specific manifes-tations of negative emotional tendencies in aspecific patient and the circumstances that tendto elicit those reactions (the kind of informationconveyed by a detailed facet-level personalityassessment) versus simply knowing that the pa-tient has “elevated negative emotionality” (cf.
First & Westen, 2007; Westen, Gabbard, &Blagov, 2006).
Although personality trait models line upwell at the domain level (cf. Widiger & Simon-sen, 2005), they are less similar at the facetlevel. As a result, there are many potential fac-ets and lists of facets to choose among whencontemplating the inclusion of a specific set offacets in a diagnostic manual. To complicatematters somewhat further, the justification forincluding a specific set of facets would logicallyinclude both clinical judgment and psychomet-ric considerations. This is because many facetsin personality trait models were generated for abroad range of applications, as opposed to hav-ing been generated specifically because of theirrelevance in clinical settings. Clinical relevanceis partly a matter of judgment (although datacan of course assist in making such judgments,e.g., data on the relative predictive validity ofspecific facets with regard to key clinical out-come variables). The general point is that de-lineation of facet-level structure and articulationof the optimal facets for clinical applicationremain an important area for research, scholar-ship, and methodological innovation (Clark,2007). For example, factor analytic methods arewell suited to modeling the “big picture” ofpersonality variation (i.e., identifying trait do-mains), but are not necessarily optimal for de-lineating fine-grained details within thesebroader domains. This latter task benefits fromtaking other approaches, such as examining thedetailed hierarchical structure that can be de-rived from cluster analyses of correlationsamong specific elements of personality(Krueger, Markon, Patrick, Benning, & Kramer,2007).
Clinical applicability of a dimensionalmodel of pathological personality traits, com-pared with a system consisting of multipledichotomous PDs. Although there are over-whelming scientific reasons for replacing theDSM–IV PD system with a dimensional trait
2 This having been said, the DSM–IV is considerablymore unwieldy in terms of containing an extensive num-ber of diagnostic constructs and modifiers. The issuemight pertain less to the sheer number of facets in adimensional personality trait system than to clinical fa-miliarity with the DSM–III constructs that have carriedthrough, mostly unchanged in most fundamental respects,into DSM–IV.
100 KRUEGER AND EATON

scheme, it would be helpful if a change of thismagnitude were accompanied by considerationsof clinical applicability.3 Fortunately, the clin-ical benefits of this change accrue directlyfrom the conceptual advantages of dimen-sional over categorical models of human vari-ation. Consider, for example, a multidimen-sional personality trait model in the concep-tualization of a specific patient. Formalassessment of a patient on multiple dimen-sions in a system such as the FFM or PFMprovides a comprehensive understanding ofthat patient’s personality. By comparison, bi-nary diagnoses of one or more of the DSM–IVPDs signal only that the patient passed one ormore arbitrary thresholds, leaving additionalinformation about the patient’s personalityout of the clinical picture.
Consider the example of DSM–IV borderlinePD, which requires at least five of nine diag-nostic criteria to be present for a diagnosis to bemade. The “five or greater” threshold results in256 different combinations of criteria that jus-tify a diagnosis of borderline PD (Johansen,Karterud, Pedersen, Gude, & Falkum, 2004;Skodol et al., 2002). As a result of this diagnos-tic heterogeneity, a categorical diagnosis of bor-derline PD could indicate a great diversity ofspecific personality features in specific patients.Indeed, two patients diagnosed with borderlinePD could theoretically share only one diagnos-tic feature, and otherwise have entirely non-overlapping personality features.
Conceptual conundrums of this nature areobviated by the use of a multidimensionalmodel of pathological personality dimensions.Rather than describing a patient in terms of oneor more dichotomous variables (e.g., above orbelow the threshold for a borderline PD diag-nosis), the patient is assessed on multiple di-mensions. Graphical displays of patients’ traitprofiles provide an intuitive and appealing wayto communicate information about patients’personality features, as well as their similaritiesand dissimilarities (as discussed at greaterlength in Costa & Widiger, 2001).
To illustrate the within-category heterogene-ity problem, as well as the additional informa-tion contained in a multidimensional traitmodel, Figure 1 provides the NEO-PI–R (Costa& McCrae, 1992) domain-level trait profiles ofall six participants in the St. Louis Personalityand Aging Network study (SPAN; Thomas Olt-
manns, PI) who have participated to date andwho met criteria for a borderline PD diagnosis.SPAN is an National Institute of Health-fundedcommunity-based study of individuals ages 55to 64; the six participants we evaluated metDSM–IV borderline PD criteria after havingbeen interviewed on the Structured Interviewfor DSM–IV Personality (Pfohl, Blum, & Zim-merman, 1997). The SPAN study commenceddata collection only recently, so these datashould not be regarded as a complete account offindings or conclusions. However, the data dorepresent the trait personality profiles of sixspecific persons who were carefully interviewedand diagnosed and are illustrative in that regard.Specifically, although these six persons met cri-
3 Our use of the term clinical applicability is purposefuland should be distinguished from the term clinical utility,which has been a recent topic in discussions about consid-erations relevant in revising the DSM (e.g., First, 2005). Byclinical applicability, we mean that the translation fromscientifically valid concepts to ways of using those conceptsin the clinic has been made explicit. By contrast, recent“clinical utility” studies have tended to focus on assessingthe opinions of practitioners regarding their preferenceswhen asked to choose among a series of options regardingvarious models of psychopathology (e.g., Lowe & Widiger,2009). We do not believe that this kind of “practitionersurvey” research should carry much weight in constructinga nosology. Consider, for example, a hypothetical survey ofmedieval physicians regarding the clinical utility of trephi-nation as an intervention for mental illness or a similarsurvey regarding their ideas about the etiology of mentalillness. Few contemporary investigators would argue thatthe results of this kind of survey would have any meaningfulimplications for pursuing a model of psychopathology thatcould ultimately lead to both accurate understanding andeffective amelioration of symptoms.
In short, scientific hypotheses about psychopathologyobviously originate in clinical experiences, but they mustthen be formally tested, and the understanding that resultsfrom this scientific process must then feed back to clinicalapplication. Nevertheless, it is also critical to emphasize thata novel system with greater evidence of validity (e.g., adimensional model of personality pathology vs. the 10-category DSM–IV PD system) cannot simply be dumped inclinicians’ laps without any attempt to explain the scientificbasis for the change or how to use the new system effec-tively in the clinic. Should DSM–5 adopt novel dimensionalconceptualizations (something that has been proposed bythe DSM–5 task force chair and cochair as a cardinal goal ofthe revision effort; Regier, Narrow, Kuhl, & Kupfer, 2009;see also Helzer et al., 2008), a significant, well-organized,and compelling effort at educating front-line practitionersand researchers must be pursued. This is an essential step inensuring that the scientifically critical move to more dimen-sional conceptualizations of psychopathology resonates inboth clinical and research settings, and thereby ultimatelyserves to improve the lives of patients.
101PERSONALITY IN DSM–5
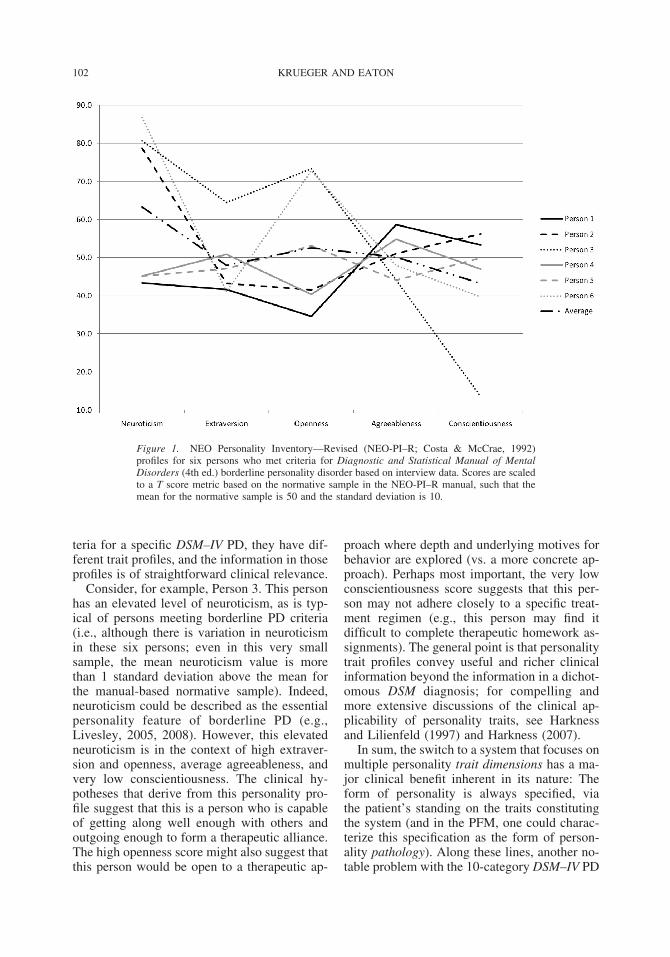
teria for a specific DSM–IV PD, they have dif-ferent trait profiles, and the information in thoseprofiles is of straightforward clinical relevance.
Consider, for example, Person 3. This personhas an elevated level of neuroticism, as is typ-ical of persons meeting borderline PD criteria(i.e., although there is variation in neuroticismin these six persons; even in this very smallsample, the mean neuroticism value is morethan 1 standard deviation above the mean forthe manual-based normative sample). Indeed,neuroticism could be described as the essentialpersonality feature of borderline PD (e.g.,Livesley, 2005, 2008). However, this elevatedneuroticism is in the context of high extraver-sion and openness, average agreeableness, andvery low conscientiousness. The clinical hy-potheses that derive from this personality pro-file suggest that this is a person who is capableof getting along well enough with others andoutgoing enough to form a therapeutic alliance.The high openness score might also suggest thatthis person would be open to a therapeutic ap-
proach where depth and underlying motives forbehavior are explored (vs. a more concrete ap-proach). Perhaps most important, the very lowconscientiousness score suggests that this per-son may not adhere closely to a specific treat-ment regimen (e.g., this person may find itdifficult to complete therapeutic homework as-signments). The general point is that personalitytrait profiles convey useful and richer clinicalinformation beyond the information in a dichot-omous DSM diagnosis; for compelling andmore extensive discussions of the clinical ap-plicability of personality traits, see Harknessand Lilienfeld (1997) and Harkness (2007).
In sum, the switch to a system that focuses onmultiple personality trait dimensions has a ma-jor clinical benefit inherent in its nature: Theform of personality is always specified, viathe patient’s standing on the traits constitutingthe system (and in the PFM, one could charac-terize this specification as the form of person-ality pathology). Along these lines, another no-table problem with the 10-category DSM–IV PD
Figure 1. NEO Personality Inventory—Revised (NEO-PI–R; Costa & McCrae, 1992)profiles for six persons who met criteria for Diagnostic and Statistical Manual of MentalDisorders (4th ed.) borderline personality disorder based on interview data. Scores are scaledto a T score metric based on the normative sample in the NEO-PI–R manual, such that themean for the normative sample is 50 and the standard deviation is 10.
102 KRUEGER AND EATON

system is the high prevalence of the PD–nototherwise specified (PD-NOS) diagnosis (Ver-heul & Widiger, 2004). This diagnosis conveyslittle clinically useful information (e.g., we arenot aware of programs of research focused onidentifying the optimal treatment for PD-NOS).By contrast, we know a great deal more aboutthe clinically relevant correlates of major do-mains of human personality variation. We re-view some of this research in the current articleas it pertains to clinical psychology and psychi-atry. But we first turn to consider two additionalissues inherent in moving from the DSM–IV10-category PD system to a dimensional per-sonality trait system for DSM–5, namely (a)how to render a PD diagnosis, given a dimen-sional system for personality trait description;and (b) what to do about the 10 PDs of DSM–IVif a dimensional personality trait system were tobe implemented in DSM–5.
Reconciling the clinical need to render PDdiagnoses with a dimensional personalitytrait model. In the DSM–IV PD system, thesymptoms of PDs and PD diagnoses are one inthe same construct. That is, crossing the symp-tom threshold for a specific PD justifies as-signing that PD diagnosis to a patient. If thePD categories of DSM–IV were replaced witha dimensional trait system in DSM–5, howwould the information in that system translateinto a diagnosis?
A simple answer to this question would in-volve setting cutoffs on the dimensions thatconstitute the DSM–5 trait model. The problemwith this approach is that it equates trait extrem-ity with disorder per se. Many would argue thatthe concept of disorder contains elements thatare distinct from trait extremity, and conceptualproblems with equating trait extremity and dis-order are easily envisioned. For example, isbeing highly introverted a “disorder” per se?Probably not, except to the extent that the per-son also shows hallmark features of disorderthat are connected to the introversion (e.g., in-ability to pursue meaningful employment be-cause of impairing shyness in spite of unequiv-ocal evidence that the person has the skillsneeded for meaningful employment).
The definitions of mental disorder and PD arechallenging topics that go beyond the scope ofthis article, but they are nevertheless importantconsiderations for DSM–5. These topics are dif-ficult because they cannot be adjudicated with
complete objectivity. The concept of disorderinvolves value judgments and is therefore in-herently a matter of societal and professionalopinion.
Moreover, recent papers on the concept ofpersonality disorder (as potentially distinct fromthe broader concept of mental disorder) tend toagree that personality disorder is a constructdistinguishable from personality traits (Parkeret al., 2004). For example, Widiger and Mul-lins-Sweatt (2009) argued that the judgment ofPD corresponds well with DSM–IV Axis V, theglobal assessment of functioning (GAF). Theysuggested that cutoffs could be placed on theGAF scale to establish clinically significantproblems in psychological, social, or occupa-tional functioning, thereby justifying the clini-cal judgment of disorder, with the personalityfeatures of the disorder described by traits. Al-though their approach is similar in many re-spects, Widiger and Mullins-Sweatt contrastedtheir views with those described by Krueger,Skodol, and colleagues (2007), who empha-sized three qualities to define PD: (a) interper-sonal functioning, (b) occupational functioning,and (c) having coherent and adaptive workingmodels of the self and others. As Widiger andMullins-Sweatt noted, the major difference be-tween their GAF conception and that of theKrueger, Skodol, et al. conception lies with theabsence of subjective distress in the Krueger,Skodol, et al. tripartite definition, this elementof the GAF having been replaced by self–otherrepresentation disturbance. Somewhat similar toKrueger, Skodol, et al., Livesley (2007) arguedthat the quintessence of PD is “adaptive failure”of the personality system. A coherently func-tioning personality system allows a person toadaptively construct working models of self andothers, to use those models to navigate closerelationships, and to pursue cooperative andmutually beneficial relationships at a broadergroup level. In PD, the functioning of this sys-tem is disrupted.
Some recent empirical work on the assess-ment of personality pathology, as distinguish-able from personality traits, may be helpful toconsider in this context. Verheul and colleagues(2008) constructed the Severity Indices of Per-sonality Problems (SIPP-118) as a self-reportassessment of personality problems, as opposedto personality traits or independent clinicaljudgments of disorder. The SIPP-118 scales en-
103PERSONALITY IN DSM–5

compass higher order domains of self-control,identity integration, relational capacity, socialconcordance, and responsibility. The authorspresent evidence that, although these scaleswere correlated with the scales of Livesley’sDimensional Assessment of Personality Pathol-ogy (DAPP; a self-report assessment of patho-logical personality traits per se; Livesley, 2007),the two instruments were not redundant, withmedian SIPP–DAPP correlations in the range of.23 to .37. This suggests that personality prob-lems can be distinguished from pathologicalpersonality traits per se, at least in the self-report domain.
The SIPP-118, the GAF, and operationaliza-tions of the clinical constructs delineated byKrueger, Skodol, and colleagues (2007) andLivesley (2007) provide good places to start inworking to use data to inform the conceptual-ization of PD in DSM–5. For example, onecould compare these conceptualizations as pre-dictors of unequivocal social costs, such as daysmissed of work owing to mental disorder symp-toms. The strength and nature of the relation-ship between personality pathology indices andsocial costs are important parameters that couldbe used to inform the definition of PD inDSM–5. Indeed, it is theoretically possible forlevel of personality pathology to have a nonlin-ear relationship with level of social cost, suchthat the likelihood of significant social costsaccelerates at some point along a dimension ofpersonality pathology. If this were the form ofthe relation between the two constructs, the“cusp” where social costs accelerate could beviewed as a reasonable location for the cutpointdelimiting disorder. However, a true nonlinearor other complex relationship of this sort maybe unlikely, given the robust predictive utility ofsimple linear models (Dawes, 1979). In anyevent, research comparing conceptions of PD(or mental disorder more generally) in terms oftheir links with “objective” social costs couldusefully inform thinking about the disorder con-struct, as well as thinking about the placementof cutpoints in DSM–5.
The vexing problem of popular diagnosticconstructs that do not map neatly onto con-structs from dimensional personality traitmodels. A critical issue in contemplating achange of the magnitude we are discussing here(replacing the 10 DSM–IV PDs with a dimen-sional trait model—something Widiger & Trull,
2007, equated with the shifting of continentalplates) concerns the fate of the 10 DSM–IV PDs.With apologies to Mr. Gore, the “inconvenienttruth” is that the 10 DSM–IV PD constructs donot map perfectly onto the broad domains ofdimensional personality trait models. Variousstances on this issue can be articulated.
A hard-line stance on this issue would focuson the idea that the continued use of constructsthat do not accurately represent the empiricalstructure of pathological personality is probablynot helping anyone in the long run. Clinicalpsychology and psychiatry continue to movetoward “evidence-based practice,” and in thiszeitgeist, the use of diagnostic constructs thatare incompatible with what is known about theempirical structure of pathological personalityis obviously problematic.
A somewhat softer stance might note that—although the resemblance is not perfect—thereare notable points of connection between thePFM domains and DSM–IV PD constructs, withtraction in both clinical and research settings.Relative to the other PDs, there seems to begreater interest and attention focused on border-line PD, antisocial PD, and schizotypal PD(Blashfield & Incotta, 2000). Borderline PD hasbeen conceptualized by some theorists as beingessentially the extreme end of negative emo-tionality or neuroticism (e.g., Livesley, 2005,2008). Similarly, antagonism (or “meanness”)is a core feature of psychopathy (which mightbe thought of as a more “personality-basedsyndrome” than the somewhat more sociole-gally defined antisocial PD; Patrick, Fowles,& Krueger, 2009). Finally, peculiarity is thequintessence of schizotypal PD, as defined inDSM–IV. As a result of these three points ofoverlap, a potential strategy would involveretaining borderline, antisocial (perhaps re-named psychopathic), and schizotypal PDs asDSM–5 diagnoses, but redefining them interms of the facets that define the broad traitdomains of negative emotionality, antago-nism, and peculiarity, respectively.
This idea has some appeal because (a) itresults in retention of the three DSM–IV PDs inwhich there is substantial interest, and (b) itgrounds those constructs in the domains of em-pirically based dimensional trait models. Nev-ertheless, other research speaks to some poten-tial empirical disjunctions that require furtherconsideration. An example that has attracted
104 KRUEGER AND EATON
recent empirical interest is the emotion dysregu-lation element of DSM–IV borderline PD. Anumber of recent studies suggest that emotiondysregulation is not simply the equivalent ofneuroticism or negative emotionality (Glenn &Klonsky, 2009; Kamen, Pryor, Gaughan, &Miller, in press; J. D. Miller & Pilkonis, 2006;Trull et al., 2008). For example, Trull et al.(2008) used ecological momentary assessment(EMA; sampling peoples experiences as theyunfold in their daily lives) to illustrate that per-sons with borderline PD showed more affectiveinstability in their natural environments whencompared with persons with current depressivedisorder (although both diagnoses are associ-ated with trait negative emotionality or neurot-icism; Bagby, Costa, Widiger, Ryder, & Mar-shall, 2005; Krueger, Caspi, Moffitt, Silva, &McGee, 1996). Similarly, DSM–IV borderlinePD also includes “transient, stress-related dis-sociation” as a symptom, and dissociation fallsmore in the peculiarity domain than in the neg-ative emotionality domain (Koffel & Watson,2009).
Recognizing the imperfect map, however,might give rise to interesting ideas for research.For example, the “transient and stress-related”part of the aforementioned dissociation criterionmight be critical; perhaps this variety of disso-ciation (e.g., traumatic intrusions) emerges atthe extremely high end of negative emotional-ity, whereas the general propensity to dissociate(with or without accompanying negative emo-tional experiences) is located in the peculiaritydomain (Koffel & Watson, 2009). In addition,in other recent EMA research (D. J. Miller,Vachon, & Lynam, 2009), neuroticism (traitnegative emotionality) predicted the typicallevel of negative affect people experienced, butantagonism (low agreeableness) was linked tounstable negative affect (i.e., the extent of ex-treme and frequent fluctuations in negative af-fect). This EMA work dovetails in an interest-ing way with structural work on borderline PD.Borderline PD shows relatively polymorphouscomorbidity (i.e., people who meet criteria forborderline PD also tend to meet criteria fornumerous other diagnoses; James & Taylor,2008). Part of the reason for this polymorphouscomorbidity might be that borderline PD, ascurrently defined, taps into multiple personalitydomains (e.g., negative emotionality, disinhibi-tion, antagonism, peculiarity; Skodol et al.,
2002; Tragesser & Robinson, 2009). Each ofthese domains predicts somewhat differentforms of psychopathology (e.g., peculiarity con-fers risk for psychotic experiences; negativeemotionality confers risk for internalizing dis-orders; Krueger et al., 1996; Kwapil, Miller,Zinser, Chapman, & Chapman, 1997). Whenthese domains combine in a specific person (i.e.,the prototypical borderline PD case), the com-bination gives rise to a diversity of problems.
In sum, the general issue and questions in thisarea can be framed as follows: Clinically salientPD constructs are somewhat, but not perfectly,aligned with the major domains of empiricallybased personality trait models. Are these dis-junctions structural (e.g., borderline PD as cur-rently defined is an interstitial, or “in between,”construct combining elements of numerouspathological personality domains)? Are the dis-junctions a matter of range (e.g., extremely highlevels of negative emotionality lead to dissoci-ation from that affect or to specific cognitivedisturbances accompanied by negative affect,such as traumatic intrusions)? Are they a matterof measurement domain (e.g., emotional dys-regulation is harder to measure with question-naire items, relative to trait negative emotional-ity, and emerges more clearly in the ecology ofdaily life)? Are they due to personality disorderhaving features (e.g., deficits in self-conceptand mental representations of other people) thatdo not overlap completely with personalitytraits (Krueger, Skodol, et al., 2007; Verheul etal., 2008)?
It seems unlikely that these questions wouldbe fully answered by the time the DSM–5 isslated to be published (2013). As a result, aneven softer stance might involve mapping someDSM–IV PDs—perhaps even all 10 DSM–IVPDs— onto the trait model adopted for theDSM–5 and providing these maps in the text ofthe DSM–5 as a means of cross-walking back toDSM–IV diagnoses. An extensive literatureshows how the 10 DSM–IV PDs can be repre-sented in terms of dimensional personality traitmodels, such as the FFM, as combinations oftraits (J. D. Miller, Bagby, Pilkonis, Reynolds,& Lynam, 2005; J. D. Miller et al., 2008; Sam-uel & Widiger, 2008). The obvious disadvan-tage of this approach is that it undermines thepoint of moving to an empirically based dimen-sional model of pathological personality in
105PERSONALITY IN DSM–5

DSM–5 and reifies the structurally invalidDSM–IV PD system.
Stepping back from the scientific details andviewing this area more from the perspective ofthe sociology of science, these are very chal-lenging issues because (a) they intersect withthe value placed on different kinds of evidence,and (b) they have serious implications for peo-ple’s lives (e.g., the careers of professionals andthe ways in which patients connect with clinicalservices). For example, what matters more inthinking about classification: the empirical fac-tor structure of personality traits, or the clinicalsalience and documented social costs of border-line PD as currently defined? What are we tomake of the extensive literature on borderlinePD if it ceases to be officially recognized byDSM–5, or of programs of research focused onelucidating and ameliorating borderline PD?What becomes of the sociostructural entitiesthat have arisen around DSM–IV PD constructs(e.g., patient advocacy groups and researchfoundations focused on borderline PD)?
Practically speaking, our view is that DSM–5must include some means of describing at leastsome DSM–IV PDs in personality trait terms,particularly those that have traction in currentclinical thinking and research (cf. J. D. Miller etal., 2008). With this in mind, we favor the lastoption described above: focusing effort on ar-ticulating a trait model as the foundation forconceptualizing personality and personality dis-orders in DSM–5, but also articulating all 10DSM–IV PDs in trait terms, probably in anappendix that describes these PDs as “legacyconstructs from DSM–IV.” These PDs can bewell captured as combinations of specific traits,along with requiring the patient to pass thethreshold for a PD diagnosis (see Krueger,Skodol, et al., 2007, for an example of how thisapproach might work focused on borderline PD;see also Widiger & Mullins-Sweatt, 2009, for asimilar proposal). A reasonable system forDSM–5 would consist of (a) an empiricallybased personality trait model; (b) a general def-inition of the PD diagnosis, rendered as athreshold on an ordinal dimension of overalldeficits in conceptualization of self and othersand accompanying problems pursuing meaning-ful occupational and interpersonal goals; and (c)articulation of person-centered PD prototypesfrom the DSM–IV as combinations of traits,
accompanied by passing the threshold for thePD diagnosis (Krueger, Skodol, et al., 2007).
On the Inevitable Role of StructuralValidity in Constructing an EmpiricallyBased and Useful System for ClassifyingMental Disorders
Although improving PD conceptualizationand classification is an important and timelytopic, the questions and issues the foregoingdiscussion raises have broader implications forthe classification of psychopathology. The pu-tative Axis I–Axis II distinction proposed byDSM–IV has little empirical basis (Clark, 2005;Krueger, 2005), and as a result, personality traitresearch has broad implications for the classifi-cation of all mental disorders.
Since the time of the neo-Kraepelinian revo-lution in psychiatry in the 1970s, the emphasisin classification has been on reliability (Blash-field, 1984). The narrative paragraphs ofDSM–II gave way to the explicit criterion listsof DSM–III, which led to increased reliabilityfor a number of key mental disorders (Spitzer,Forman, & Nee, 1979). However, a reasonableargument can be made that this focus on reli-ability in mental disorder classification was atthe expense of validity (Kendell & Jablensky,2003).
The validity of a system for classifying psy-chopathology is a challenging and multifacetedtopic (G. T. Smith & Combs, in press; Strauss &Smith, 2009). Nevertheless, there is one keyaspect of validity that we see as both critical andtractable at this point in the evolution of think-ing about the classification of mental disorders.Specifically, we believe that any diagnostic sys-tem that is a serious contender for being a usefulframework for pursuing research on the etiologyand treatment of psychopathology, and there-fore research of potential clinical relevance,must start from a position of structural validity(Loevinger, 1957).
By structural validity, we specifically meanthat a classification system for psychopathology(a) should be able to be explicated as a formalquantitative model of human variation and (b)should fit data suited to estimating the parame-ters of said formal quantitative model. Simplyput, it is extremely difficult to make sense of(and, often, even to pursue) research on psycho-pathology given a structurally invalid system. In
106 KRUEGER AND EATON

addition, we emphasize quantification in ourdefinition simply because models need to bestated in formal quantitative terms to seewhether they actually work (i.e., to see whetherthey fit relevant data) and to be vulnerable tofalsification (Popper, 1959). Without this step,classification science devolves into efforts thatgenerate more heat than light, that is, argumentsbased on training, background, or a priori con-ceptual preferences versus genuine insightsabout the nature of psychopathology. For exam-ple, one could hypothesize that borderline PD issomehow different in kind from dimensionalpersonality traits, and comprises a nonarbitraryclass of persons (a “taxon”), based on clinicalexperience (albeit this hypothesis has been eval-uated and rejected; Edens, Marcus, & Ruiz,2008). But there is no way to evaluate this kindof hypothesis (“borderline PD is a category innature”) if it cannot be stated in terms of itsimplications for what one would expect to ob-serve in relevant data, and data always come inthe form of numbers (Meehl, 2006). Moreover,it is helpful also to be able to state an alternativehypothesis in formal quantitative terms (e.g.,“borderline PD as currently conceptualized is aconfiguration of extreme standing on a series ofdimensions, e.g., pathological traits and overalldeficits in self and other conceptualization, thatvary continuously in nature”) because this fa-cilitates direct comparison of competing modelsof psychopathology in relevant data (cf.Krueger, Markon, et al., 2005; Markon &Krueger, 2005).
The DSM–IV system of 10 putatively dichot-omous PDs, plus a panoply of additional andputatively dichotomous mental disorders onAxis I, provides a particularly compelling ex-ample of the problems that emerge when tryingto work with a system that suffers from prob-lems related to structural validity. As an exam-ple, consider a current “hot topic”: moleculargenetic research on mental disorders (Psychiat-ric GWAS Steering Committee, 2009). Giventhe rather amazing recent advances in genotyp-ing technology, we could, for example, pursue agenomewide search for the single nucleotidepolymorphisms (SNPs) that are associated withDSM–IV-defined borderline PD using a designin which cases and controls are compared ontheir SNP profiles across the genome (agenomewide association study, or GWAS, fo-cused on borderline PD as the target pheno-
type). A key methodological consideration arisesimmediately in contemplating this study: Shouldour borderline PD cases be free of other mentaldisorders? Probably not, because the typical bor-derline PD case is a person with extensiveadditional psychopathology— both PDs perDSM–IV criteria as well as other DSM–IV-defined mental disorders (Skodol et al., 2002).So, perhaps we should simply work with bor-derline PD cases (regardless of any additionalpsychopathology they might have) and comparethem with persons who have never met border-line PD criteria (e.g., in themselves or in theirfirst-degree relatives). But then can we concludethat borderline PD is driving the findings of ourresearch? This conclusion seems unwarrantedbecause the rate of psychopathology, generallyspeaking, and across Axes I and II of theDSM–IV, will be significantly elevated in theborderline PD group. So, perhaps one optionhere might be to assess all the other psychopa-thology, and then include these variables ascovariates in models predicting case status fromSNPs. Unfortunately, this is also not a particu-larly compelling solution because it brings usback to our original dilemma. In the “covariatemodeling approach,” we are creating (using sta-tistical means rather than by initial screening)an artifactual “pure form” of borderline PD thatwe know does not exist in nature (cf. Meehl,1971)—or at the very least an artifactual “pureform” that does not resemble the modal border-line PD patient in clinical settings.
As this discussion illustrates, thinking aboutstructural validity leads to topics beyond thePDs and to a more fundamental consideration ofthe dilemmas of a diagnostic system such asDSM–IV, in which structurally awkward situa-tions involving comorbidity, within-categoryheterogeneity, and NOS diagnoses are the norm(Krueger & Markon, 2006). Might a structurallyvalid dimensional personality trait model haveimplications for understanding psychopathol-ogy that go beyond its ability to resolve prob-lems with the DSM–IV approach to classifyingPDs?
Beyond Personality Disorders and Towarda Structurally Valid Model ofPsychopathology Grounded in Personality
Perhaps the most serious problem with contem-porary psychodiagnosis is the lack of empirical
107PERSONALITY IN DSM–5

constraints on the form of psychodiagnostic sys-tems. Our current scientific understanding of psy-chopathology is modest at best, in spite of exten-sive efforts aimed at identifying the underlyingpathophysiology and etiology of psychopathologyand significant expenditures of taxpayer dollars.Nevertheless, the hope remains that, given reli-able markers of underlying pathophysiologyand etiology (e.g., specific genetic polymor-phisms or neurobehavioral indices) and knowl-edge of potent environmental elicitors, we couldcreate a valid diagnostic system to drive appro-priate intervention strategies.
The question is how to bootstrap a psychodi-agnostic system with this kind of validity fromour current understanding. As we began de-scribing in the foregoing section, our view isthat the only way we can accomplish this isthrough a first step aimed at using numericaltaxonomy to articulate a structurally validmodel of psychopathology. By numerical tax-onomy, we are referring to the formal quan-titative modeling that underlies the pursuit ofstructural validity. A discussion of quantitativemodeling per se would go well beyond thescope of this article, but the basic idea is thatdata on manifest psychopathological signs andsymptoms are quantified, and formal quantita-tive models are compared in terms of their fit tothose data. As just one example, one couldcompare and contrast models positing that psy-chopathology is more continuous (or dimen-sional) versus more discrete (or categorical; see,e.g., Krueger, Markon, Patrick, & Iacono, 2005;Waller & Meehl, 1998). Indeed, a key findingfrom this kind of research is that psychopathol-ogy tends to be more continuous than discrete(Krueger, Watson, & Barlow, 2005).
Pursuing structural validity via numericaltaxonomy involves conducting research de-signed to place nonarbitrary, empirically de-rived constraints on the form of a psychodi-agnostic system. It is important to note thatthese constraints may be misleading at someother level of analysis if their conceptualstrengths and limitations are not properly un-derstood. For example, there is extensivestructural evidence for the existence of a per-vasive neuroticism or negative emotionalitydimension in psychopathology data underly-ing essentially all forms of psychologicalmaladjustment (Lahey, 2009). Is this dimen-sion akin to fever in internal medicine—a
highly general indicator of distress (cf.Ormel, Rosmalen, & Farmer, 2004)? Andwhat should we conclude if this were indeedan apt analogy?
From the “fever analogy,” one could arguethat neuroticism is clinically useless because“all patients in mental health settings have ele-vated neuroticism.” But few physicians wouldargue that fever is a useless construct, particu-larly if one thinks about fever on a nonarbitrarycontinuous scale, as opposed to thinking interms of “high fever versus normal tempera-ture.” Rather, a modern understanding is thatdistinguishable underlying etiologies can giverise to final common clinical signs and symp-toms (e.g., high fever) that are important toassess, and a high fever is cause for greateralarm than a mild fever. Knowing someonesuddenly developed a high fever initiates a pro-cess of differential diagnosis in search of theetiology of the high fever and brings into playdiagnostic constructs that are less likely to beconsidered in the context of a mild elevation inbody temperature (e.g., meningitis). The pointis that structurally valid constructs do not nec-essarily have a 1:1 map with underlying etiolo-gies or pathophysiologies (e.g., the quantitativedimension of fever can result from a variety ofunderlying causes, some of which are discrete,and we may very well discover that neuroticismis similarly multidetermined; Zuckerman,2005). Nevertheless, the search for the biologi-cal and environmental factors that contribute topsychopathology is importantly constrained andassisted by knowing about the manifest empir-ical structure of psychopathology. The concep-tualization of psychopathology in DSM–IV—that mental disorders are discrete categorieswith well-defined boundaries—is untenable andincompatible with the data (Kendell & Jablen-sky, 2003; Krueger & Markon, 2006).
Consider the following specific neurobehav-ioral example. The monoamine neurotransmit-ter serotonin is involved in many diverse behav-ioral functions. As a result, “the functioningof the serotonin system” probably relates tomultiple “individual differences in behavioralpropensities.” For example, DeYoung (2006)argues that neuroticism, disagreeableness, andunconscientiousness are sufficiently correlatedto give rise to a higher order dimension of “(in)stability,” and that the confluence of these char-acteristics maps reasonably well onto seroton-
108 KRUEGER AND EATON

ergic functioning. In a somewhat different ac-count, Carver, Johnson, and Joormann (2009)argue that these diverse phenotypic individualdifferences are associated with serotonin be-cause low serotonin reduces the organism’s ca-pacity to bring deliberate effortful control tobear on behavior. As a result, whatever cues aresalient at a more basic motivational level (e.g.,signals for reward vs. punishment) are morelikely to drive behavior in the context of lowserotonin, and those cues could drive the organ-ism toward ruminative neuroticism (whichmight eventuate in a depressive episode) orimpulsive aggression (disagreeable unconscien-tious behavior), depending on the nature of theimmediate circumstances.
The point here is that this discussion aboutthe role of serotonin in human individual dif-ferences is framed and constrained by our un-derstanding of the structure of human personal-ity. The phenotypic constructs that constrainthis discussion are known to map the structureof individual differences in human personalitytraits (McCrae & Costa, 2008), thereby usefullyconstraining theory and research on the role ofserotonin in human individual differences.DeYoung (2006) and Carver et al. (2009) areoffering somewhat different theories, but theyare also talking about the same empirically de-rived phenotypic domains.
Contrast this with a theoretical propositionsuch as “the serotonin system is ‘disrupted’ inDSM–IV unipolar mood disorders.” Taken atface value, this proposition is not unreasonable(cf. Carver et al., 2009). However, it is veryhard to test this proposition as stated becausethe DSM–IV categories are not well constrainedby data on the empirical structure of psycho-pathological signs and symptoms. For example,Brown, Campbell, Lehman, Grisham, and Man-cill (2001) found that 95% of individuals whomet criteria for lifetime major depression ordysthymia in a clinical sample also met criteriafor a current or past anxiety disorder. As aresult, if we sought evidence of serotonergicabnormalities in depression, that evidencewould probably have to be derived from casesof depression with at least some history of anx-iety, and we would be unable to state with muchclarity that the abnormalities we observed couldbe attributed to a specific diagnostic construct asopposed to a host of other putatively distinct
DSM–IV diagnoses that flow naturally alongwith each other.
In sum, we advocate using numerical taxon-omy to articulate a structurally valid model ofdescriptive psychopathology as a key next stepin the evolution of research on the classificationof psychopathology. This is a tractable goalthat builds on the advances that began withDSM–III, that is, the ability to assess reliablythe presence versus absence of specific psycho-pathological signs and symptoms. We have thestatistical modeling technology needed to con-verge on a structurally valid model of psycho-pathology, given the right data (e.g., large-scalesymptom-level data derived from reliable as-sessment instruments, but unconstrained by ex-isting DSM conventions). A structurally validmodel of psychopathology is vital because itprovides a data-based framework for workingtoward an understanding of the underpinningsof psychopathology, and therefore, a frameworkwith enhanced clinical applicability. Because ofphenomena such as comorbidity, within-category heterogeneity, and NOS diagnoses, re-search framed by DSM–IV constructs is difficultto interpret at best. As a direct result, suchresearch has limited applicability in clinical set-tings. For example, if the modal patient meetingcriteria for a commonly encountered diagnosissuch as major depressive disorder also meetscriteria for other disorders, research on personswith “pure major depressive disorder” (a com-mon strategy) has questionable relevance to ev-eryday clinical practice. By contrast, researchframed by structurally valid constructs (such asconstructs from empirically derived models ofpersonality traits) is considerably more inter-pretable. Such research parses people as theyactually occur in nature, and is therefore morereadily translated to application in clinical set-tings. We turn now to discuss how personalitytrait research per se could be drawn on to helpframe DSM–5 in a broad sense and therebypropel a move to a structurally valid system ofpsychodiagnosis.
Linking Personality Traits With Axis IPsychopathology in DSM–5
It is probably unrealistic to think that a com-plete and structurally valid model of psychopa-thology derived from numerical taxonomic re-search could be prepared in time for DSM–5. A
109PERSONALITY IN DSM–5

major reason for this is that the field, and hencethe potentially relevant data, are constrained bythe constructs of DSM–IV. However, the poten-tial exists to frame DSM–5 by structural re-search on DSM–IV constructs, as a bridge to acomprehensive, structurally valid model of psy-chopathology. In addition, DSM–5 could be de-signed to help encourage the collection of datathat could be used to pursue numerical taxo-nomic research to inform DSM–6 (cf. Helzer,Kraemer, & Krueger, 2006; Watson & Clark,2006).
As a starting point for this discussion, con-sider data on relations between personality traitsand Axis I phenomena (keeping in mind that themultiaxial system of DSM–IV may also be dis-carded in DSM–5). In addition to their clearrelevance to improving conceptualization ofPDs, dimensional personality traits show ro-bust, sizable, and psychologically meaningfulconnections with Axis I disorders. For example,a recent meta-analysis examined 33 studieslinking the FFM personality domains with awide variety of mental disorders and foundcompelling links with all FFM domains exceptopenness (Malouff, Thorsteinsson, & Schutte,2005). Indeed, the effect size for the link be-tween neuroticism and clinical disorderswas 0.92, a “large effect” by Cohen’s (1988)standards.
The link between personality and Axis I dis-orders extends beyond bivariate correlations toparallels in the multivariate structure of bothdomains. Specifically, comorbidity patternslinking common Axis I mental disorders can beunderstood in terms of two superordinate, orga-nizing spectrum constructs: internalizing andexternalizing (for recent reviews, see Eaton,South, & Krueger, in press; Krueger & Markon,2006; Slade & Watson, 2006). The internalizingspectrum includes unipolar mood and anxietydisorders, and the externalizing spectrum in-cludes antisocial behavior disorders and sub-stance use disorders. These spectrum constructsreflect both the phenotypic structure of comor-bidity and the underlying genetic structure ofcomorbidity (Kendler, Prescott, Myers, &Neale, 2003; Krueger et al., 2002). Recentstructural modeling work by Markon (2010)focused on the symptom rather than the disorderlevel, and including both Axis I and II symp-toms has extended this phenotypic model byindicating the existence of thought disorder
and pathological introversion domains in ad-dition to internalizing and externalizing. Theparallels between Markon’s four psychopa-thology factors and the PFM are apparent(i.e., internalizing resembles negative emo-tionality, externalizing resembles disinhibi-tion and antagonism, thought disorder resem-bles peculiarity, and pathological introversionresembles introversion).
The parallels in the structure of common AxisI disorders and personality traits can also beexamined from a number of other vantagepoints. One way to address these connections isto see whether personality traits “fit” along withDSM constructs in the same spectra. Alongthese lines, trait neuroticism has been shown tofit into the internalizing spectrum when mod-eled simultaneously with mental disorders suchas major depression, generalized anxiety disor-der, panic disorder, agoraphobia, and socialphobia (Hettema et al., 2006; South & Krueger,2008). Similarly, disinhibitory personality traitsfit in the externalizing spectrum, along withantisocial personality disorder features per se(Krueger et al., 2002). From this vantage point,personality traits and mental disorders can beconceptualized as manifestations of the sameunderlying spectra of human variation, with en-vironmental circumstances having a key impacton the manifest form of behavior (e.g., the de-velopment of personality tendencies vs. diag-nosable psychopathology).
Another vantage point on personality trait–Axis I relations involves seeing how much co-morbidity can be attributed to personality traits.Khan, Jacobson, Gardner, Prescott, and Kendler(2005) investigated the proportion of comorbid-ity between disorders due to personality traits.Neuroticism was found to play a particularlysubstantial role in the comorbidity of commonmental disorders. With regard to any two of theinternalizing disorders assessed (i.e., major de-pression, generalized anxiety disorder, panicdisorder, and any phobia), neuroticism ac-counted for a substantial proportion of the co-morbidity between the disorders.
Drawing from this kind of evidence, we re-cently joined forces with colleagues to suggest apotential metastructure for DSM–5 and theInternational Classification of Diseases–11(Andrews et al., 2009). The idea in this workwas to take existing diagnostic constructs atface value, but to try to rearrange them in a way
110 KRUEGER AND EATON

that might be more parsimonious and betterreflect data on shared underlying connections.Five broad clusters of disorders emerged fromthis exercise: (1) neurocognitive disorders(e.g., the dementias), (2) neurodevelopmentaldisorders (e.g., autism), (3) psychoses (e.g.,schizophrenia), (4) emotional or internalizingdisorders (e.g., unipolar mood and anxietydisorders), and (5) externalizing disorders(e.g., antisocial behavior and substance usedisorders). Some of these classificatory ru-brics are not explicitly connected with thestructure of personality. However, the explicitbasis for clustering emotional (internalizing)and externalizing disorders was their sharedpersonality trait antecedents.
The model described by Andrews and col-leagues (2009) represents a reasonable start on aclassification better connected with data, but itis only a beginning because it is based on ex-isting diagnostic categories. Nevertheless, it of-fers a reasonable way to incorporate personalitytraits in DSM–5, with regard to Axis I condi-tions, should those constructs persist in theircurrent form. Specifically, if disorders were or-ganized into these sorts of clusters, the person-ality trait basis for the organization of the rele-vant clusters could be made explicit in the text.This would help in breaking down the relativelyartificial barrier between personality and psy-chopathology (cf. Clark, 2005; Krueger &Tackett, 2003). Nevertheless, ultimately, thesymptoms of Axis I disorders and the affective,cognitive, and behavioral phenomena that con-stitute personality traits need to be merged moreexplicitly in the pursuit of a structurally validmodel of personality and psychopathology (cf.Krueger, Markon, et al., 2007).
Personality Traits and Other Outcomes ofClinical Relevance
We have reviewed how personality traits arecentral to improving the classification of psy-chopathology. Yet, including an empiricallybased personality trait model in DSM–5 couldalso have benefits beyond clarifying the role ofpersonality in working toward a structurallyvalid nosology. Specifically, personality traitsare also relevant in predicting and understand-ing clinically important outcomes beyond psy-chopathology per se. We turn now to brieflydescribe two particularly compelling examples
of domains in which the broad relevance ofpersonality traits in clinical settings seems clear:physical health and interpersonal functioning.
Physical health. Perhaps no outcome ismore important to the health care professionsthan mortality. In longitudinal data, personalitytraits have been shown to predict mortality morestrongly than socioeconomic status (SES) andequivalently to IQ (Roberts, Kuncel, Shiner,Caspi, & Goldberg, 2007). Personality traits arealso relevant to overall physical health. Lahey’s(2009) compelling recent review of the publichealth implications of neuroticism notes that,even after controlling for other risk factors (e.g.,social support), neuroticism is related to a di-versity of physical health concerns. These prob-lems range broadly from cardiovascular diseaseto asthma to eczema. Furthermore, the coursesof at least some medical conditions can be pre-dicted by neuroticism, such as cardiac diseaseand renal deterioration in diabetes (Lahey,2009). Personality traits also appear to be rele-vant to resilience, for example, optimism con-veys resilience to physical disease (T. W.Smith, 2006).
Evidence is mounting that personality is as-sociated with and often prospectively predictsphysical health outcomes, but the precise natureof the mechanisms underlying these links is lessclear (Ozer & Benet-Martı́nez, 2006). Onelikely mechanism involves the impact of per-sonality on health-related decision making. Forexample, the link between neuroticism andphysical health and mortality has been hypoth-esized to result from more neurotic individualsengaging in behaviors that put their health atrisk (e.g., smoking). Mroczek, Spiro, and Turi-ano (2009) tested this hypothesis, and foundthat the link between neuroticism and mortalitywas reduced by 40% when the effect of smok-ing was removed. Personality may also be partof the explanation for well-replicated socioeco-nomic disparities in mortality. Chapman, Fis-cella, Kawachi, and Duberstein (in press) foundthat personality traits were able to explain 20%of the SES gradient in mortality.
Interpersonal functioning. Interpersonalfunctioning is clearly relevant in many clinicalsituations, and, similar to mortality, personalitytraits such as neuroticism, disagreeableness, andunconscientiousness predict divorce longitudi-nally (Roberts et al., 2007). Indeed, when com-pared with SES, personality traits are better
111PERSONALITY IN DSM–5

predictors of divorce. A recent review by Ozerand Benet-Martı́nez (2006) further supports thelink between interpersonal outcomes and per-sonality traits. Relations with peers in childhoodare predicted by agreeableness and extraver-sion; young adults’ neuroticism, conscientious-ness, and extraversion levels predict the qualityof relationships with their parents; and romanticrelationship outcomes, including abuse, con-flict, and dissatisfaction, are predicted by levelsof agreeableness and neuroticism.
Personality Traits and TreatmentConsiderations
A growing literature—including a recent spe-cial issue of the Journal of Personality Assess-ment (Hilsenroth, 2004)—indicates that person-ality is also an important consideration inframing interventions for both mental disordersand physical diseases. Personality predicts over-all treatment effectiveness, as well as specificcomponents of effectiveness, such as an indi-vidual’s adherence to a treatment regimen.
Depression has been a particular focus ofresearch in this area. In one study, for example,depressed patients received both medicationand psychotherapy, and treatment respondershad lower levels of neuroticism and higher lev-els of extraversion and openness than nonre-sponders (Quilty et al., 2008). Further analysesindicated that conscientiousness as well as Neu-roticism � Extraversion and Extraversion �Conscientiousness interactions were also pre-dictive of treatment response. In addition, per-sonality traits have been shown to predict dif-ferential treatment response of specific patientsto specific treatment modalities. For instance,Bagby and colleagues (2008) investigated thelink between personality traits and response toeither cognitive–behavioral therapy or pharma-cotherapy. The results of this study indicatedthat the higher a depressed patient’s level ofneuroticism, the more likely he or she was torespond to pharmacological treatment ratherthan to cognitive–behavioral treatment. Resultssuch as these underscore the ways in whichpersonality traits may influence overall treat-ment outcome as well as inform the choice oftreatment modality for particular patients giventheir personality profiles.
Part of the reason personality traits are rele-vant to intervention may lie in traits being in-
direct targets of intervention. Neuroticism isetiologically connected with internalizing disor-ders (Hettema et al., 2006), and interventionstargeting internalizing disorders may also betargeting neurobiological systems linking per-sonality and psychopathology (Costa, Bagby,Herbst, & McCrae, 2005). A recent empiricalexample was provided by Hellerstein, Kocsis,Chapman, Stewart, and Harrison (2000). Pa-tients with a primary diagnosis of dysthymiawere randomized into treatment with sertraline,imipramine, and placebo; these patients alsocompleted Cloninger’s Tridimenisonal Person-ality Questionnaire (TPQ; Cloninger, 1987) atboth pre- and posttreatment. Pretreatment TPQharm avoidance scores were 1.5 standard devi-ations higher than community norms, yet remis-sion of dysthymia was associated with reduc-tion in TPQ harm avoidance. Indeed, for thesertraline group, 36% showed a decrease of atleast 1 standard deviation from baseline harmavoidance. Psychosocial interventions origi-nally aimed at specific clinical problems mayalso have beneficial effects on personality.Blonigen, Timko, Moos, and Moos (2009)showed that a longer duration of involvementin Alcoholics Anonymous predicted a reduc-tion in impulsivity, which in turn predicted areduction in legal problems over a 16-yearfollow-up period.
Another means by which personality couldaffect treatment outcome is through adherence.One recent study examined cholesterol-lower-ing treatment adherence by objectively assess-ing the regularity with which patients took pre-scribed medication (Stilley, Sereika, Muldoon,Ryan, & Dunbar-Jacob, 2004). Among the FFMpersonality traits, only conscientiousnessshowed a significant association with medica-tion compliance. At 1 week into the study, con-scientiousness showed a small and nonsignifi-cant link to adherence (r � .06, ns). Over time,however, this association increased, and, byWeek 24, the link between conscientiousnessand adherence was notable (r � .24, p � .01).
In addition, specific treatments appear towork better than others for patients with differ-ent personalities. Personality trait assessmentcould be used by health care professionals toselect the interventions to which the client ismost likely to adhere (e.g., using long-lastingmedication injections every few weeks vs. re-quiring an unconscientious patient to take med-
112 KRUEGER AND EATON

ications daily, or allotting time in session for anunconscientious patient to complete homework;cf. Harkness & Lilienfeld, 1997; J. D. Miller,Pilkonis, & Mulvey, 2006). Personality assess-ment could also be used as a prescreening forvulnerability to future disorder and as a tool foridentifying individuals at high risk who maybenefit from preemptive intervention (e.g.,stress inoculation; Lahey, 2009).
Finally, personality traits are also worth con-sidering on the other side of the equation, thatis, the traits of the practitioners. Concernedabout burnout among primary care physicians,Krasner and colleagues (2009) evaluated theeffects of a continuing medical education coursefocused on mindfulness in clinical encounters.They found that their course resulted in signif-icantly increased conscientiousness and de-creased neuroticism among the physician par-ticipants (as well as other clinically relevantimprovements, such as reduced burnout) at theend of the course. The conclusion is that thetraits of practitioners can affect the care they areable to provide, and these dispositions are ame-nable to intervention that could enhance thenature of clinical care.
Toward DSM–5: An “Open Source”Perspective
Our aim in this review was to illustrate thediverse ways in which the inclusion of an em-pirically based personality trait model couldconstitute a critical innovation in the transitionfrom DSM–IV to DSM–5. Our initial focus wason personality disorder classification and con-ceptualization because this is the area in whichdimensional models of personality traits havebeen discussed most extensively. We alsobriefly touched on the role of personality inorganizing Axis I disorders and the relevance ofpersonality in predicting other clinically impor-tant phenomena, including treatment consider-ations. Our hope is that the reader joins us in ourenthusiasm regarding the critical role personal-ity traits can play in both research and in theclinic. Importantly, personality traits are farfrom “untreatable” and may, in fact, be the truetargets of psychopharmacologic interventionsoriginally intended for Axis I conditions (Knut-son et al., 1998; Tang et al., 2009). Moreover,personality traits are not static entities or per-manent and unchanging characteristics. Rather,
traits change over time in normative ways (Rob-erts & Mroczek, 2008). Erroneous conceptionsof personality traits as static, unchanging, anduntreatable have given way to a more nuancedunderstanding that traits can and do changegiven the right circumstances.
More broadly, our hope is that the readerjoins us in our enthusiasm for the constructionof a structurally valid model of psychopathol-ogy that draws on parallels in the structure ofpersonality. DSM–III and its offspring consti-tuted a critical innovation in the history of thefield because they offered concrete, observablecriteria for psychopathology, many of whichcould be reliably assessed. Nevertheless, wehave learned a lot since DSM–III was publishedin 1980, particularly regarding the limitations ofa categorical and polythetic conceptualizationof mental disorder. The time therefore has cometo evolve the conceptualization of mental dis-orders described in DSMs III to IV. Numericaltaxonomy has an important role to play in thisevolutionary period in the history of thinkingabout mental disorder classification. Formalquantitative models are indispensible tools inthe development of a structurally valid model ofpsychopathology, a model that could be veryhelpful in framing both clinical thinking andresearch.
Because it is slated to be published very soon(2013), creating a quantitative model of psycho-pathology is not a realistic goal for DSM–5.However, it is a tractable and desirable goal ingeneral. The key to pursuing this goal is toencourage—rather than constrain through fiat—creative and novel research on the classificationof psychopathology. DSM–5 will be a successstory to the extent that it becomes an “opensource” document, fostering novel and creativethinking about classification, as opposed to re-ifying necessarily provisional and imperfectdefinitions of mental disorders.
References
American Psychiatric Association. (1994). Diagnos-tic and statistical manual of mental disorders (4thed.). Washington, DC: Author.
Andrews, G., Goldberg, D. P., Krueger, R. F., Car-penter, W. T., Jr., Hyman, S. E., Sachdev, P., &Pine, D. S. (2009). Exploring the feasibility of ameta-structure for DSM–V and ICD–11: Could it
113PERSONALITY IN DSM–5
improve utility and validity? Psychological Medi-cine, 39, 1993–2000.
Bagby, R. M., Costa, P. T., Jr., Widiger, T. A., Ryder,A. G., & Marshall, M. (2005). DSM–IV personalitydisorders and the five-factor model of personality:A multi-method examination of domain- and facet-level predictions. European Journal of Personal-ity, 19, 307–324.
Bagby, R. M., Quilty, L. C., Segal, Z. V., McBride,C. C., Kennedy, S. H., & Costa, P. T., Jr. (2008).Personality and differential treatment response inmajor depression: A randomized controlled trialcomparing cognitive–behavioral therapy and phar-macotherapy. The Canadian Journal of Psychia-try, 53, 361–370.
Blashfield, R. K. (1984). Classification of psychopa-thology. New York: Plenum Press.
Blashfield, R. K., & Intoccia, V. (2000). Growth ofthe literature on the topic of personality disorders.The American Journal of Psychiatry, 157, 472–473.
Blonigen, D. M., Timko, C., Moos, B. S., & Moos,R. H. (2009). Treatment, Alcoholics Anonymous,and 16-year changes in impulsivity and legal prob-lems among men and women with alcohol usedisorders. Journal of Studies on Alcohol andDrugs, 70, 714–725.
Brown, T. A., Campbell, L. A., Lehman, C. L.,Grisham, J. R., & Mancill, R. B. (2001). Currentand lifetime comorbidity of the DSM–IV anxietyand mood disorders in a large clinical sample.Journal of Abnormal Psychology, 110, 585–599.
Carver, C. S., Johnson, S. L., & Joormann, J. (2009).Two-mode models of self-regulation as a tool forconceptualizing effects of the serotonin system innormal behavior and diverse disorders. CurrentDirections in Psychological Science, 18, 195–199.
Chapman, B. P., Fiscella, K., Kawachi, I., & Duber-stein, P. R. (in press). Personality, socioeconomicstatus, and all-cause mortality in the United States.American Journal of Epidemiology.
Clark, L. A. (2005). Temperament as a unifying basisfor personality and psychopathology. Journal ofAbnormal Psychology, 114, 505–521.
Clark, L. A. (2007). Assessment and diagnosis ofpersonality disorder: Perennial issues and anemerging reconceptualization. Annual Review ofPsychology, 58, 227–257.
Cloninger, C. R. (1987). A systematic method forclinical description and classification of personal-ity variants. Archives of General Psychiatry, 44,573–588.
Cohen, J. (1988). Statistical power analysis for thebehavioral sciences (2nd ed.). Mahwah, NJ:Erlbaum.
Costa, P. T., Jr., Bagby, R. M., Herbst, J. H., &McCrae, R. R. (2005). Personality self-reports areconcurrently reliable and valid during acute de-
pressive episodes. Journal of Affective Disor-ders, 89, 45–55.
Costa, P. T., Jr., & McCrae, R. R. (1992). RevisedNEO Personality Inventory (NEO-PI–R) and NEOFive-Factor Inventory (NEO-FFI) professionalmanual. Odessa, FL: Psychological AssessmentResources.
Costa, P. T., Jr., & Widiger, T. A. (2001). Personalitydisorders and the five-factor model of personality(2nd ed.). Washington, DC: American Psycholog-ical Association.
Dawes, R. M. (1979). The robust beauty of improperlinear models in decision making. American Psy-chologist, 34, 571–582.
De Clercq, B., De Fruyt, F., Van Leeuwen, K., &Mervielde, I. (2006). The structure of maladaptivepersonality traits in childhood: A step toward anintegrative developmental perspective for DSM–V.Journal of Abnormal Psychology, 115, 639–657.
DeYoung, C. G. (2006). Higher-order factors of thebig five in a multi-informant sample. Journal ofPersonality and Social Psychology, 91, 1138–1151.
Dolan-Sewell, R. T., Krueger, R. F., & Shea, M. T.(2001). Co-occurrence with syndrome disorders.In W. J. Livesley (Ed.), Handbook of personalitydisorders (pp. 84 –104). New York: GuilfordPress.
Eaton, N., South, S., & Krueger, R. F. (in press). Thestructure of comorbidity among mental disorders.In T. Millon, R. Krueger, & E. Simonsen (Eds.),Contemporary directions in psychopathology: Sci-entific foundations of the DSM–V and ICD–11.New York: Guilford Press.
Edens, J. D., Marcus, D. K., & Ruiz, M. A. (2008).Taxometric analyses of borderline personality fea-tures in a large-scale male and female offendersample. Journal of Abnormal Psychology, 117,705–711.
First, M. B. (2005). Clinical utility: A prerequisite forthe adoption of a dimensional approach in DSM.Journal of Abnormal Psychology, 114, 560–564.
First, M. B., & Westen, D. (2007). Classification forclinical practice: How to make ICD and DSMbetter able to serve clinicians. International Re-view of Psychiatry, 19, 473–448.
Frances, A. J. (1993). Dimensional diagnosis of per-sonality—Not whether, but when and which. Psy-chological Inquiry, 4, 110–111.
Glenn, C. R., & Klonsky, E. D. (2009). Emotiondysregulation as a core feature of borderline per-sonality disorder. Journal of Personality Disor-ders, 23, 20–28.
Harkness, A. R. (2007). Personality traits are essen-tial for a complete clinical science. In S. O. Lilien-feld & W. T. O’Donohue (Eds.), The great ideas ofclinical science (pp. 263–290). New York: Rout-ledge.
114 KRUEGER AND EATON
Harkness, A. R., & Lilienfeld, S. O. (1997). Individ-ual differences science for treatment planning: Per-sonality traits. Psychological Assessment, 9, 349–360.
Harkness, A. R., & McNulty, J. L. (1994). The Per-sonality Psychopathology Five (PSY-5): Issuesfrom the pages of a diagnostic manual instead of adictionary. In S. Strack & M. Lorr (Eds.), Differ-entiating normal and abnormal personality (pp.291–315). New York: Springer.
Harkness, A. R., McNulty, J. L., & Ben-Porath, Y. S.(1995). The Personality Psychopathology Five(PSY-5): Constructs and MMPI–2 scales. Psycho-logical Assessment, 7, 104–114.
Hellerstein, D. J., Kocsis, J. H., Chapman, D., Stew-art, J. W., & Harrison, W. (2000). Double-blindcomparison of sertraline, imipramine, and placeboin the treatment of dysthymia. Effects on person-ality. The American Journal of Psychiatry, 157,1436–1444.
Helzer, J. E., Kraemer, H. C., & Krueger, R. F.(2006). The feasibility and need for dimensionalpsychiatric diagnoses. Psychological Medi-cine, 36, 1671–1680.
Helzer, J. E., Kraemer, H. C., Krueger, R. F., Witt-chen, H.-U., Sirovatka, P. J., & Regier, D. A.(Eds.). (2008). Dimensional approaches in diag-nostic classification: Refining the research agendafor DSM–V. Washington, DC: American Psychi-atric Publishing.
Hettema, J. M., Neale, M. C., Myers, J. M., Prescott,C. A., & Kendler, K. S. (2006). A population-based twin study of the relationship between neu-roticism and internalizing disorders. The AmericanJournal of Psychiatry, 163, 857–864.
Hilsenroth, M. J. (2004). An introduction to the spe-cial issue on personality assessment and psycho-therapy. Journal of Personality Assessment, 83,187–189.
James, L., & Taylor, J. (2008). Revisiting the struc-ture of mental disorders: Borderline personalitydisorder and the internalizing/externalizing spec-tra. British Journal of Clinical Psychology, 47,361–380.
Johansen, M., Karterud, S., Pedersen, G., Gude, T., &Falkum, E. (2004). An investigation of the proto-type validity of the borderline DSM–IV construct.Acta Psychiatrica Scandinavica, 109, 289–298.
John, O. P., Naumann, L. P., & Soto, C. J. (2008).Paradigm shift to the integrative big-five trait tax-onomy: History, measurement, and conceptual is-sues. In O. P. John, R. W. Robins, & L. A. Pervin(Eds.), Handbook of personality: Theory and re-search (pp. 114–158). New York: Guilford Press.
Kamen, C., Pryor, L. R., Gaughan, E. T., & Miller,J. D. (in press). Affective lability: Separable fromneuroticism and the other big four? PsychiatryResearch.
Kamphuis, J. H., & Noordhof, A. (2009). On cate-gorical diagnoses in DSM–V: Cutting dimensionsat useful points? Psychological Assessment, 21,294–301.
Kendell, R., & Jablensky, A. (2003). Distinguishingbetween the validity and utility of psychiatric di-agnoses. The American Journal of Psychiatry, 160,4–12.
Kendler, K. S., Prescott, C. A., Myers, J., & Neale,M. C. (2003). The structure of genetic and envi-ronmental risk factors for common psychiatric andsubstance use disorders in men and women. Ar-chives of General Psychiatry, 60, 929–937.
Khan, A. A., Jacobson, K. C., Gardner, C. O., Pres-cott, C. A., & Kendler, K. S. (2005). Personalityand comorbidity of common psychiatric disorders.British Journal of Psychiatry, 186, 190–196.
Knutson, B., Wolkowitz, O. M., Cole, S. W., Chan,T., Moore, E. A., Johnson, R. C., . . . Reus, V. I.(1998). Selective alteration of personality and so-cial behavior by serotonergic intervention. TheAmerican Journal of Psychiatry, 155, 373–379.
Koffel, E., & Watson, D. (2009). Unusual sleep ex-periences, dissociation, and schizotypy: Evidencefor a common domain. Clinical Psychology Re-view, 29, 548–559.
Krasner, M. S., Epstein, R. M., Beckman, H.,Suchman, A. L., Chapman, B., Mooney, C. J., &Quill, T. E. (2009). Association of an educa-tional program in mindful communication withburnout, empathy, and attitudes among primarycare physicians. Journal of the American Medi-cal Association, 302, 1284 –1293.
Krueger, R. F. (2005). Continuity of Axes I and II:Toward a unified model of personality, personalitydisorders, and clinical disorders. Journal of Per-sonality Disorders, 19, 233–261.
Krueger, R. F., Caspi, A., Moffitt, T. E., Silva, P. A.,& McGee, R. (1996). Personality traits are differ-entially linked to mental disorders: A multitrait–multidiagnosis study of an adolescent birth cohort.Journal of Abnormal Psychology, 105, 299–312.
Krueger, R. F., Hicks, B. M., Patrick, C. J., Carlson,S. R., Iacono, W. G., & McGue, M. (2002). Etio-logic connections among substance dependence,antisocial behavior, and personality: Modeling theexternalizing spectrum. Journal of Abnormal Psy-chology, 111, 411–424.
Krueger, R. F., & Markon, K. E. (2006). Reinterpret-ing comorbidity: A model-based approach to un-derstanding and classifying psychopathology. An-nual Review of Clinical Psychology, 2, 111–133.
Krueger, R. F., Markon, K. E., Patrick, C. J., Ben-ning, S. D., & Kramer, M. (2007). Linking antiso-cial behavior, substance use, and personality: Anintegrative quantitative model of the adult exter-nalizing spectrum. Journal of Abnormal Psychol-ogy, 116, 645–666.
115PERSONALITY IN DSM–5
Krueger, R. F., Markon, K. E., Patrick, C. J., &Iacono, W. G. (2005). Externalizing psychopathol-ogy in adulthood: A dimensional-spectrum con-ceptualization and its implications for DSM–V.Journal of Abnormal Psychology, 114, 537–550.
Krueger, R. F., Skodol, A. E., Livesley, W. J., Shrout,P., & Huang, Y. (2007). Synthesizing dimensionaland categorical approaches to personality disor-ders: Refining the research agenda for DSM–VAxis II. International Journal of Methods in Psy-chiatric Research, 16(Suppl. 1), S65–S73.
Krueger, R. F., & Tackett, J. L. (2003). Personalityand psychopathology: Working toward the biggerpicture. Journal of Personality Disorders, 17,109–128.
Krueger, R. F., & Tackett, J. L. (Eds.). (2006). Per-sonality and psychopathology. New York: Guil-ford Press.
Krueger, R. F., Watson, D., & Barlow, D. (2005).Introduction to the special section: Toward a di-mensionally based taxonomy of psychopathology.Journal of Abnormal Psychology, 114, 491–493.
Kwapil, T. R., Miller, M. B., Zinser, M. C., Chap-man, J., & Chapman, L. J. (1997). Magical ide-ation and social anhedonia as predictors of psycho-sis proneness: A partial replication. Journal ofAbnormal Psychology, 106, 491–495.
Lahey, B. B. (2009). Public health significance ofneuroticism. American Psychologist, 64, 241–256.
Livesley, W. J. (2005). From shifting diagnoses toempirically-based diagnostic constructs. In M.Maj, H. S. Akiskal, J. E. Mezzich, & A. Okasha(Eds.), Personality disorders (pp. 232–234). WestSussex, England: Wiley.
Livesley, W. J. (2007). A framework for integratingdimensional and categorical classifications of per-sonality disorder. Journal of Personality Disor-ders, 21, 199–224.
Livesley, W. J. (2008). Toward a genetically in-formed model of borderline personality disorder.Journal of Personality Disorders, 22, 42–71.
Livesley, W. J., Jang, K. L., & Vernon, P. A. (1998).Phenotypic and genetic structure of traits delineat-ing personality disorder. Archives of General Psy-chiatry, 55, 941–948.
Loevinger, J. (1957). Objective tests as instrumentsof psychological theory. Psychological Reports, 3,635–694.
Lowe, J. R., & Widiger, T. A. (2009). Clinicians’judgments of clinical utility: A comparison of theDSM–IV with dimensional models of general per-sonality. Journal of Personality Disorders, 23,211–229.
Malouff, J. M., Thorsteinsson, E. B., & Schutte, N. S.(2005). The relationship between the five-factormodel of personality and symptoms of clinicaldisorders: A meta-analysis. Journal of Psychopa-thology and Behavioral Assessment, 27, 101–114.
Markon, K. E. (2010). Modeling psychopathologystructure: A symptom-level analysis of Axis I andII disorders. Psychological Medicine, 40, 273–288.
Markon, K. E., & Krueger, R. F. (2005). Categoricaland continuous models of liability to externalizingdisorders: A direct comparison in NESARC. Ar-chives of General Psychiatry, 62, 1352–1359.
Markon, K. E., Krueger, R. F., & Watson, D. (2005).Delineating the structure of normal and abnormalpersonality: An integrative hierarchical approach.Journal of Personality and Social Psychology, 88,139–157.
McCrae, R. R., & Costa, P. T., Jr. (2008). The five-factor theory of personality. In O. P. John, R. W.Robins, & L. A. Pervin (Eds.), Handbook of per-sonality: Theory and research (3rd ed., pp. 159–181). New York: Guilford Press.
Meehl, P. E. (1971). High school yearbooks: A replyto Schwarz. Journal of Abnormal Psychology, 77,143–148.
Meehl, P. E. (2006). The power of quantitative think-ing. In N. G. Waller, L. J. Yonce, W. M. Grove, D.Faust, & M. F. Lenzenweger (Eds.), A Paul Meehlreader: Essays on the practice of scientific psy-chology (pp. 433–444). Mahwah, NJ: Erlbaum.
Miller, D. J., Vachon, D. D., & Lynam, D. (2009).Neuroticism, negative affect, and negative affectinstability: Establishing convergent and discrimi-nant validity using ecological momentary assess-ment. Personality and Individual Differences, 47,873–877.
Miller, J. D., Bagby, R. M., Pilkonis, P. A., Reyn-olds, S. K., & Lynam, D. R. (2005). A simplifiedtechnique for scoring the DSM–IV personality dis-orders with the five-factor model. Assessment, 12,404–415.
Miller, J. D., Lynam, D. R., Rolland, J. P., De Fruyt,F., Reynolds, S. K., Pham-Scottez, A., . . . Bagby,R. M. (2008). Scoring the DSM–IV personalitydisorders using the five-factor model: Develop-ment and validation of normative scores for NorthAmerican, French and Dutch–Flemish samples.Journal of Personality Disorders, 22, 433–450.
Miller, J. D., & Pilkonis, P. A., (2006). Neuroticismand affective instability: The same or different?The American Journal of Psychiatry 163, 839–845.
Miller, J. D., Pilkonis, P. A., & Mulvey, E. P. (2006).Treatment utilization and satisfaction: Examiningthe contributions of Axis II psychopathology andthe five-factor model of personality. Journal ofPersonality Disorders, 20, 369–387.
Mroczek, D. K., Spiro, A., & Turiano, N. A. (2009).Do health behaviors explain the effect of neuroti-cism on mortality? Journal of Research in Person-ality, 43, 653–659.
Nestadt, G., Costa, P. T., Jr., Hsu, F.-C., Samuels, J.,Bienvenu, O. J., & Eaton, W. W. (2008). The
116 KRUEGER AND EATON
relationship between the five-factor model and la-tent Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition personality disorder di-mensions. Comprehensive Psychiatry, 49, 98–105.
Nestadt, G., Hsu, F.-C., Samuels, J., Eaton, W. W.,Bienvenu, O. J., & Costa, P. T. (2006). Latentstructure of the Diagnostic and Statistical Manualof Mental Disorders Fourth Edition personalitydisorder criteria. Comprehensive Psychiatry, 47,54–62.
Oldham, J. M., & Skodol, A. E. (2000). Charting thefuture of Axis II. Journal of Personality Disor-ders, 14, 17–29.
Ormel, J., Rosmalen, J., & Farmer, A. (2004). Neu-roticism: A non-informative marker of vulnerabil-ity to psychopathology. Social Psychiatry and Psy-chiatric Epidemiology, 39, 906–912.
Ozer, D. J., & Benet-Martı́nez, V. (2006). Personalityand the prediction of consequential outcomes. An-nual Review of Psychology, 57, 401–421.
Parker, G., Hadzi-Pavlovic, D., Both, L., Kumar, S.,Wilhelm, K., & Olley, A. (2004). Measuring dis-ordered personality functioning: To love and towork reprised. Acta Psychiatrica Scandanavica,110, 230–239.
Patrick, C., Fowles, D., & Krueger, R. (2009). Tri-archic conceptualization of psychopathy: Develop-mental origins of disinhibition, boldness, andmeanness. Development and Psychopathology, 21,913–938.
Pfohl, B., Blum, N., & Zimmerman, M. (1997).Structural Interview for DSM–IV Personality Dis-orders. Washington, DC: American PsychiatricAssociation.
Piedmont, R. L., Sherman, M. F., Sherman, N. C.,Dy-Liacco, G. S., & Williams, J. E. (2009). Usingthe five-factor model to identify a new personalitydisorder domain: The case for experiential perme-ability. Journal of Personality and Social Psychol-ogy, 96, 1245–1258.
Popper, K. R. (1959). The logic of scientific discov-ery. New York: Basic Books.
Psychiatric GWAS Steering Committee. (2009). Aframework for interpreting genome-wide associa-tion studies of psychiatric disorders. MolecularPsychiatry, 14, 10–17.
Quilty, L. C., De Fruyt, F., Rolland, J., Kennedy,S. H., Rouillon, F., & Bagby, R. M. (2008). Di-mensional personality traits and treatment outcomein patients with major depressive disorder. Journalof Affective Disorders, 108, 241–250.
Regier, D. A., Narrow, W. E., Kuhl, E. A., & Kupfer,D. J. (2009). The conceptual development ofDSM–V. The American Journal of Psychiatry, 166,645–650.
Roberts, B. W., Kuncel, N. R., Shiner, R., Caspi, A.,& Goldberg, L. R. (2007). The power of person-ality: The comparative validity of personality
traits, socioeconomic status, and cognitive abilityfor predicting important life outcomes. Perspec-tives on Psychological Science, 2, 313–345.
Roberts, B. W., & Mroczek, D. (2008). Personalitytrait change in adulthood. Current Directions inPsychological Science, 17, 31–35.
Samuel, D. B., & Widiger, T. A. (2008). A meta-analytic review of the relationships between thefive-factor model and DSM–IV–TR personality dis-orders: A facet level analysis. Clinical PsychologyReview, 28, 1326–1342.
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger,T. A., Livesley, W. J., & Siever, L. J. (2002). Theborderline diagnosis: I. Psychopathology, comor-bidity, and personality structure. Biological Psy-chiatry, 51, 936–950.
Slade, T., & Watson, D. (2006). The structure ofcommon DSM–IV and ICD–10 mental disorders inthe Australian general population. PsychologicalMedicine, 36, 1593–1600.
Smith, G. T., & Combs, J. (in press). Issues ofconstruct validity in psychological diagnoses. In T.Millon, R. F. Krueger, & E. Simonsen (Eds.),Contemporary directions in psychopathology: To-ward the DSM–V and ICD–11. New York: Guil-ford Press.
Smith, T. W. (2006). Personality as risk and reliancein physical health. Current Directions in Psycho-logical Science, 15, 227–231.
South, S., Eaton, N., & Krueger, R. (in press). Theconnections between personality and psychopa-thology. In T. Millon, R. F. Krueger, & E. Simon-sen (Eds.), Contemporary directions in psychopa-thology: Toward the DSM–V and ICD–11. NewYork: Guilford Press.
South, S., & Krueger, R. F. (2008). The moderatingeffect of marital quality on genetic and environ-mental contributions to internalizing psychopa-thology. Journal of Abnormal Psychology, 117,826–837.
Spitzer, R. L., Forman, J. B., & Nee, J. (1979).DSM–III field trials: I. Initial interrater diagnosticreliability. The American Journal of Psychiatry,136, 815–817.
Stilley, C. S., Sereika, S., Muldoon, M. F., Ryan,C. M., & Dunbar-Jacob, J. (2004). Psychologicaland cognitive function: Predictors of adherencewith cholesterol lowering treatment. Annals of Be-havioral Medicine, 27, 117–124.
Strauss, M. E., & Smith, G. T. (2009). Constructvalidity: Advances in theory and methodology.Annual Review of Clinical Psychology, 5, 1–25.
Tackett, J. L., Silberschmidt, A. L., Krueger, R. F., &Sponheim, S. R. (2008). A dimensional model ofpersonality disorder: Incorporating DSM Cluster Acharacteristics. Journal of Abnormal Psychology,117, 454–459.
117PERSONALITY IN DSM–5
Tang, T. Z., DeRubeis, R. J., Hollon, S. D., Am-sterdam, J., Shelton, R., & Schalet, B. (2009).Personality change during depression treatment:A placebo-controlled trial. Archives of GeneralPsychiatry, 66, 1332–1330.
Tellegen, A. (1991). Personality traits: Issues of def-inition, evidence, and assessment. In W. M. Grove& D. Cicchetti (Eds.), Thinking clearly about psy-chology (pp. 10–35). Minneapolis: University ofMinnesota Press.
Tragesser, S. L., & Robinson, R. J. (2009). The roleof affective instability and UPPS impulsivity inborderline personality disorder features. Journal ofPersonality Disorders, 23, 370–383.
Trull, T. J., & Durrett, C. A. (2005). Categorical anddimensional models of personality disorder. An-nual Review of Clinical Psychology, 1, 355–380.
Trull, T. J., Solhan, M. B., Tragesser, S. L., Jahng, S.,Wood, P. K., Piasecki, T. M., & Watson, D.(2008). Affective instability: Measuring a core fea-ture of borderline personality disorder with eco-logical momentary assessment. Journal of Abnor-mal Psychology, 117, 647–661.
Verheul, R., Andrea, H., Berghout, C. C., Dolan, C.,Busschbach, J. J., van der Kroft, P. J., . . . Fonagy, P.(2008). Severity Indices of Personality Problems (SIPP-118): Development, factor structure, reliability, and va-lidity. Psychological Assessment, 20, 23–34.
Verheul, R., & Widiger, T. A. (2004). A meta-analysisof the prevalence and usage of the personality disor-der not otherwise specified (PDNOS) diagnosis.Journal of Personality Disorders, 18, 309–319.
Waller, N. G., & Meehl, P. E. (1998). Multivariatetaxometric procedures: Distinguishing types fromcontinua. Thousand Oaks, CA: Sage.
Watson, D., & Clark, L. A. (2006). Clinical diagnosisat the crossroads. Clinical Psychology: Scienceand Practice, 13, 210–215.
Watson, D., Clark, L. A., & Chmielewski, M. (2008).Structures of personality and their relevance topsychopathology: II. Further articulation of a com-prehensive unified trait structure. Journal of Per-sonality, 76, 1545–1585.
Westen, D., Gabbard, G. O., & Blagov, P. (2006).Back to the future: Personality structure as a con-text for psychopathology. In R. F. Krueger & J.Tackett (Eds.), Personality and psychopathology(pp. 335–384). New York: Guilford Press.
Widiger, T. A., Livesley, W. J., & Clark, L. A.(2009). An integrative dimensional classificationof personality disorder. Psychological Assess-ment, 21, 243–255.
Widiger, T. A., & Mullins-Sweatt, S. N. (2009).Five-factor model of personality disorder: A pro-posal for DSM–V. Annual Review of Clinical Psy-chology, 5, 197–220.
Widiger, T. A., & Samuel, D. B. (2005). Diagnosticcategories or dimensions? A question for the Di-agnostic and Statistical Manual of Mental Disor-ders—Fifth Edition. Journal of Abnormal Psy-chology, 114, 494–504.
Widiger, T. A., & Simonsen, E. (2005). Alternativedimensional models of personality disorder: Find-ing a common ground. Journal of Personality Dis-orders, 19, 110–130.
Widiger, T. A., Simonsen, E., Krueger, R., Livesley,J. W., & Verheul, R. (2005). Personality disorderresearch agenda for the DSM–V. Journal of Per-sonality Disorders, 19, 315–338.
Widiger, T. A., & Trull, T. J. (2007). Plate tectonicsin the classification of personality disorder: Shift-ing to a dimensional model. American Psycholo-gist, 62, 71–83.
Zuckerman, M. (2005). Psychobiology of personal-ity. New York: Cambridge University Press.
118 KRUEGER AND EATON