-
8/11/2019 Personality DisordersTheory, Research, And
1/15
Personality Disorders: Theory, Research, andTreatment
Five-Factor Model Personality Disorder Prototypes in aCommunity
Sample: Self- and Informant-ReportsPredicting Interview-Based DSM
Diagnoses
Erin M. Lawton, Andrew J. Shields, and Thomas F. OltmannsOnline
First Publication, March 28, 2011. doi: 10.1037/a0022617
CITATION
Lawton, E. M., Shields, A. J., & Oltmanns, T. F. (2011,
March 28). Five-Factor Model
Personality Disorder Prototypes in a Community Sample: Self- and
Informant-Reports
Predicting Interview-Based DSM Diagnoses. Personality Disorders:
Theory, Research, and
Treatment. Advance online publication. doi: 10.1037/a0022617
-
8/11/2019 Personality DisordersTheory, Research, And
2/15
Five-Factor Model Personality Disorder Prototypes in a
CommunitySample: Self- and Informant-Reports Predicting
Interview-Based
DSM Diagnoses
Erin M. Lawton, Andrew J. Shields, and Thomas F.
OltmannsWashington University in St. Louis
The need for an empirically validated, dimensional system of
personality disorders isbecoming increasingly apparent. While a
number of systems have been investigated inthis regard, the
five-factor model of personality has demonstrated the ability
toadequately capture personality pathology. In particular, the
personality disorder proto-types developed by Lynam and Widiger
(2001) have been tested in a number ofsamples. The goal of the
present study is to extend this literature by validating
theprototypes in a large, representative community sample of later
middle-aged adultsusing both self and informant reports. We found
that the prototypes largely work well
in this age group. Schizoid, Borderline, Histrionic,
Narcissistic, and Avoidant person-ality disorders demonstrate good
convergent validity, with a particularly strong patternof
discriminant validity for the latter four. Informant-reported
prototypes show similarpatterns to self reports for all analyses.
This demonstrates that informants are notsuccumbing to halo
representations of the participants, but are rather
describingparticipants in nuanced ways. It is important that
informant reports add significantpredictive validity for Schizoid,
Antisocial, Borderline, Histrionic, and Narcissisticpersonality
disorders. Implications of our results and directions for future
research arediscussed.
Keywords: personality disorder, prototypes, five-factor model,
informant report, validity
Over the last few decades, dimensional mod-els of personality
disorders (PDs) have garnereda great deal of support and
enthusiasm. Of thediagnoses in the Diagnostic and Statistical
Manual(DSMIV; American Psychological As-sociation, 1994), PDs
are often considered themost problematic (e.g., in terms of
reliabilityand co-occurrence). However, there are a num-ber of
reasons to be hopeful that a dimensionalmodel may yield a dramatic
improvement indealing with these issues. First, evidence has
demonstrated that personality pathology is con-
tinuously distributed (Livesley, 1998; Widiger,1992). It appears
that, rather than askingwhether a PD is or is not present,
researchersand clinicians should be asking about thedegreeto which
features are present. Dimensionalmodels of PDs have also gained
support throughthe consistent finding that abnormal personalityis
highly related to normal personality function-ing, which has long
been conceptualized as con-tinuous (Costa & Widiger, 2002;
OConnor,2002). Finally, Skodol et al. (2005) found thatdimensional
models of four PDsSchizotypal,Borderline, Avoidant, and
Obsessive-Compul-sive PDsaccounted for more variance in func-tional
impairment (e.g., work or interpersonalfunctioning) than did
theDSMIVcategories orsimply measures of normal personality. Each
ofthese areas of research seems to suggest thatidentifying and
implementing a dimensionalmodel of PDs would provide a
much-neededempirical base for the diagnosis and study ofpersonality
pathology.
Of the various dimensional models that havebeen proposed, the
five-factor model (FFM) ofpersonality has received the most
attention, and
Erin M. Lawton, Andrew J. Shields, and Thomas F.Oltmanns,
Department of Psychology, Washington Univer-sity in St. Louis.
This research was supported by a grant from the
NationalInstitute of Mental Health (MH077840). We thank
MerlynRodrigues, Tami Curl, Rickey Louis, Christie Spence, Am-ber
Bolton, and Marci Gleason for their assistance with datacollection
and management.
Correspondence concerning this article should be ad-dressed to
Thomas F. Oltmanns, Department of Psychology,WA University, 1
Brookings Drive, Campus Box 1125, St.Louis, MO 63130. E-mail:
[email protected]
Personality Disorders: Theory, Research, and Treatment 2011
American Psychological Association2011, Vol. , No. , 000000
1949-2715/11/$12.00 DOI: 10.1037/a0022617
1
-
8/11/2019 Personality DisordersTheory, Research, And
3/15
research suggests that the FFM is largely able todepict the 10
DSMIVPDs (Costa & Widiger,2002; Saulsman & Page, 2004;
Schroeder,Wormworth, & Livesly, 1992). This model is
based on lexical analyses of trait descriptors andsuggests five
higher-order domains of personal-ity: neuroticism, extraversion,
openness to ex-perience, agreeableness, and conscientiousness.The
NEO Personality Inventory (NEO-PI-R;Costa & McCrae, 1992), the
most widely usedmeasure of the FFM, further separates each ofthese
five broad domains into six facets.
Using item response theory, Samuel, Simms,Clark, Livesley, and
Widiger (2010) examinedthe relationship between the NEO-PI-R and
twomeasures of personality pathology (the Sched-ule for Nonadaptive
& Adaptive Personality;Clark, 1993; and the Dimensional
Assessmentof Personality Pathology; Livesley & Jackson,2009).
Results from these analyses demonstratea shared dimensional
structure among measuresof normal and pathological personality,
withfour of the five domains emerging (opennesswas not consistently
found). Moreover, thisstudy found that, while the measures of
patho-logical personality typically provided more in-formation at
higher levels of the latent trait
dimensions, there was a large degree of overlapbetween
instrument coverage. This providesstrong evidence that features of
personality dis-orders can indeed be conceptualized as
extremevariants of general personality traits.
At the most basic level, high neuroticism andlow agreeableness
appear to be associated withmost of the PDs. The exception is
DependentPD, which is characterized by both high neurot-icism and
high agreeableness (Saulsman &Page, 2004). However, more
differentiating re-
lationships between the NEO-PI-R and PDs areachieved at the
facet level (Widiger, Trull, Clar-kin, Sanderson, & Costa,
1994). Lynam andWidiger (2001) proposed a more disorder-specific
approach using expert consensus to de-termine a distinct subset of
facets characteristicof each PD. This approach enjoys a number
ofbenefits, such as an aggregation of judgmentsand the
identification of facets not overtly iden-tified in
DSMIVcriteria.
Since their development, these prototypicalprofiles have been
validated in a number of
samples. Miller, Reynolds, and Pilkonis (2004)found generally
good agreement between theexpert consensus prototypes and
NEO-PI-R
profiles in a clinical sample, with the exceptionof
Obsessive-Compulsive PD and DependentPD. These authors also found
overall good con-vergent and discriminant validity with respect
to two measures of personality pathology. Thesame study reported
high temporal stability andadequate predictive validity with regard
to theseprototypes across 6- and 12-month periods in asecond
clinical sample. Again, Obsessive-Compulsive PD had the lowest
similarityscores. This and other studies have indicatedthat this
prototype does not seem to be workingas well as the others. More
generally, a numberof studies have reported that the FFM is not
ableto describe Obsessive-Compulsive PD consis-tently (Haigler
& Widiger, 2001; Miller, Bagby,& Pilkonis, 2005).
To avoid the time consuming and demandingmethod of prototype
matching, Miller, Bagby,Pilkonis, Reynolds, and Lynam (2005)
devel-oped a simplified scoring technique. This tech-nique (known
as the PD count method) createsa summed score of all relevant
NEO-PI-R facetsfor each PD. The PD count score techniqueyields
correlations comparable to those betweensimilarity scores and PD
symptom counts(Miller, Bagby, Pilkonis, et al., 2005). These
count scores can then be compared to the NorthAmerican, French,
or Dutch-Flemish normativescores established and validated by
Miller et al.(2008). The FFM PD count scores have alsobeen
validated when assessed via StructuredInterview for the Five-Factor
Model of Person-ality, as well as when rated by clinicians(Miller,
Bagby, & Pilkonis, 2005; Miller,Maples, et al., 2010).
One limitation of many of the aforemen-tioned studies is their
reliance on self-report.
Although some attempt has been made to ex-plore the utility of
other-report (Miller, Pilko-nis, & Clifton, 2005; Miller,
Pilkonis, & Morse,2004), the use of informants with respect to
thePD prototypes is largely absent despite beingacknowledged as an
important pursuit (e.g., Wi-diger & Samuel, 2005). It is
commonly recog-nized in the literature that individuals with
per-sonality pathology often lack insight due to theego-syntonic
nature of these disorders (Klon-sky, Oltmanns, & Turkheimer,
2002). Indeed,research using peer-report of PD features has
suggested that this source seems to be adding aunique
perspective; although informant reportappears to differ appreciably
from self report,
2 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
4/15
informants tend to agree with each other (Klon-sky et al., 2002;
Oltmanns & Turkheimer,2009). The fact that others agree
suggests thatmeaningful constructs are being captured.
This begs the question: are there systematicdifferences with
regard to the constructs that theself versus an informant can draw
upon whenreporting? Much of this literature has focusedon the
observability of traits. In terms of theFFM, neuroticism is
typically associated withlow observability, while extraversion is
linkedto high observability. Because it relies heavilyon knowledge
of internal thoughts and feelings,neuroticism should produce
somewhat lowerself-other agreement. Conversely extraversionis, by
definition, more observable and shouldtherefore result in higher
levels of self-otheragreement. Indeed a number of studies
havedemonstrated this pattern (e.g., Harkness, Tel-legen, &
Waller, 1995; Naumann, Vazire, Rent-frow, & Gosling, 2009),
though agreement ontraits of neuroticism appear to increase
some-what as level of acquaintance between the targetand the
observer increases (Vazire, 2010). Ingeneral then we see that the
observability oftraits plays an important role in the study
andinterpretation of other reports.
Beyond the realm of normal personality, dif-ferent sources
appear to provide varied infor-mation regarding PDs and
functioning. UsingFFM domain and facet scores, rather than
pro-totypes, Miller, Pilkonis, and Clifton (2005)found that other
report generally provided ad-ditional information with respect to a
targetspersonality pathology in a clinical sample, par-ticularly
for Paranoid PD and the Cluster Bdisorders (Antisocial, Borderline,
Histrionic,and Narcissistic). Miller, Pilkonis, and Morse
(2004) found a median correlation of .47 be-tween self- and
informant-reported PD proto-type scores in another sample of
psychiatricpatients. Informant-reported prototypes demon-strated
incremental validity in the prediction offunctional and
interpersonal impairment in thisstudy. This pattern was
particularly strong forParanoid, Antisocial, Borderline,
Histrionic,and Avoidant PDs. Additionally, their analysesindicated
that self-other agreement increased asthe observability of
maladaptive traits in-creased. This may provide an explanation
for
why informants are proving particularly usefulas a source of
information regarding Cluster Bdisorders, pathologies for which
criteria tend to
be more externalizing than the other PD diag-noses. Ultimately,
Miller, Pilkonis, and Morse(2004) suggest that while internal
distress isbetter predicted by self report, interpersonal
dysfunction is better predicted by informants.A suggested
advantage of a dimensional
model is the ability to account for and handlethe considerable
diagnostic co-occurrence seenwith PDs (Lynam & Widiger, 2001;
Trull &McCrae, 2002; Widiger & Frances, 2002). Re-search
studies consistently show that individu-als diagnosed with one PD
frequently meet cri-teria for at least one other (e.g., Oldham et
al.,1992; Widiger & Chaynes, 2003). However, asnoted by Lynam
and Widiger, a great deal ofPD comorbidity may be explained using
theFFM, as disorders are expected to co-occur tothe extent that
they assess common FFM do-mains and facets (p. 403). Because the
FFMallows a wide variety of personality profiles,latent PD
constructs may be more accuratelyrepresented. Before such a system
can be im-plemented, its relationship to the existing sys-tem must
be examined.
In addition to the benefits of any dimensionalmodel (e.g.,
consistent empirical support thatpersonality pathology is
continuous, their po-
tential to better handle diagnostic co-occur-rence), because
they are based on normalpersonality, the NEO prototypes may prove
par-ticularly useful when examining age. In herreview on stability
and variability in PDs, Clark(2009) noted an overall decrease in
personalitypathology over time. However, Balsis, Gleason,Woods, and
Oltmanns (2007) found that a num-ber of the DSMIVcriteria contain
age bias. Anolder adult in their sample was more likely toendorse
the Dependent PD criterion, feels un-
comfortable and helpless when alone because ofexaggerated fears
of being unable to care forhimself or herself than a younger adult
with thesame level of underlying latent variable. TheNEO-PI-R, on
the other hand, has been usedextensively in later middle-aged and
olderadults, and has demonstrated good temporal sta-bility (Costa
& McCrae, 1994; Widiger & Trull,2007). For these reasons,
the prototypes may bebetter indicators of levels of latent
pathology inolder adults than the DSMIVdiagnoses.
The present study addresses several issues.
First, we attempt to validate the PD prototypesin a later
middle-aged adult sample. Throughthe use of informants, we are able
to examine
3SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
5/15
self-other agreement among the prototypes, aswell as to identify
the areas in which otherreport may be particularly useful. Very
fewstudies look at informant-generated prototypes,
particularly in a community sample. Addition-ally, this study
expands upon earlier work byshedding light on the relation between
age andself-other congruence using the FFM and pro-totypes, as
opposed to pathological personalitymeasures. Finally, we examine
convergent anddiscriminant validity, looking both at the
rela-tionships among the prototypes as well as be-tween each
prototype and an interview-basedmeasure.
Method
Participants
Results in this manuscript are reported as partof an ongoing,
prospective study of the trajec-tory of personality pathology in
later middle-age (Oltmanns & Gleason, 2011). This commu-nity
sample was recruited using standardepidemiological methods and
consisted of 898adults between the ages of 55 and 64 yearsliving in
the St. Louis Metropolitan area (demo-
graphic characteristics are reported in Table 1).Though we do
not possess data regarding thespecific racial/ethnic break-down for
this age
group, census data for St. Louis city and countyindicate a 65%
white and 29% black population.Therefore, this sample is
representative of St.Louis racial/ethnic composition. Data from
males and females were analyzed together forthis paper, as it is
neither our purpose to exam-ine gender differences, nor are
findings consis-tent with respect to established gender
differ-ences in the prevalence of specific PDs (with theexception
of Antisocial PD; e.g., Grant et al.,2004; Lenzenweger, Lane,
Loranger, & Kes-sler, 2007; Torgersen, Kringlen, &
Cramer,2001). Analyses conducted separately by gen-der revealed
that correlations for each groupwere typically very close to those
reported forthe whole sample, and there did not appear to beany
systematic differences. When they differed,correlations for males
were frequently slightlysmaller than those for females. Similarly,
nosystematic differences emerged when analyseswere stratified by
participant race/ethnicity andthese too were very close to the
entire samplecorrelations. In general, the prototypes seemedto be
functioning approximately equivalently inboth groups, supporting
the analysis of the over-all sample.
We utilized a community sample for a num-
ber of reasons. Perhaps most important is thefact that most
middle-aged people who wouldmeet the diagnostic criteria for a
personalitydisorder are likely not in treatment. Studies thatfocus
on clinical samples have the advantage ofincluding people with more
pronounced person-ality pathology, but there is no way to
determinewhether those problems are representative ofthe nature or
extent of personality disorders inthe general population. While the
NEO PD pro-totypes have been used with informants in clin-
ical samples (e.g., Miller, Pilkonis, et al., 2005),the
relationship between self and other reportshas not yet been
examined in a communitysample.
Participants were recruited using a pool ofrandomly selected,
listed phone numbers forhouseholds with at least one inhabitant in
ourage range. Specific information regarding resi-dents was
provided by a sampling company thatcross-referenced households with
census data.Households were asked to identify all eligibleresidents
between the ages of 55 and 64 years. If
a household contained more than one eligibleresident, the Kish
method (Kish, 1949) wasused to randomly select a target. We did
not
Table 1Sample Demographic Characteristics
%
Sex
Female 55.4
Race/ethnicity
White 69.4African American 29.4
Other 1.2
Born in St. Louis 58.7
Education
High school 40.5
College 26.2
Advanced degree 32.1
Employment
Full-time 46.1
Part-time 19.4
Retired 32.4
Unemployed due to disability 9.7
Median household income $40,000$59,999
Note. Employment exceeds 100% due to those workingpart-time
since retirement.
4 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
6/15
recruit other eligible residents if the target re-fused to
participate (sampling without replace-ment). Participants were paid
$60 to complete a3-hr assessment.
Informants
Each participant was asked to identify some-one who would be
able to provide the bestdescription of the participants personality
char-acteristics. We preferred that the participantidentify a
spouse or romantic partner as theirinformant. If a romantic partner
was unavailableor refused to participate, the participant wasasked
to identify another person who knewthem well. For this sample, data
were collectedfrom 760 informants, comprised of 47.4% ro-mantic
partners, 24.8% family members, 23.0%close friends, and 4.8%
other.
Measures
Structured Interview for DSMIVPerson-ality (SIDP-IV). The
SIDP-IV (Pfohl, Blum,& Zimmerman, 1997) is a semistructured
inter-view designed to assess each criterion of the 10
DSMIVpersonality disorders. Questions on the
SIDP-IV are arranged by themes (e.g., emo-tions,
self-perception, stress and anger) ratherthan by disorder. Items
are written in nonpejo-rative lay language. The SIDP-IV utilizes
a5-year rule, meaning participants were asked todescribe
personality traits that predominatedover the most recent 5-year
period. PD criteriaare rated on a 0 to 3 scale, from not
presenttostrongly present. Diagnoses can be obtainedusing the
SIDP-IV by simply dichotomizing theitem scores (i.e., 0 and 1
indicate that the crite-
rion is not present, while a 2 or a 3 wouldindicate presence).
However, we maintained thedimensional nature of the scoring by
simplycreating a summed score of the total points foreach disorder
for the analyses in the currentstudy.
NEO Personality InventoryRevised(NEO-PI-R). The NEO-PI-R (Costa
&McCrae, 1992) is a 240-item questionnairemeasuring the FFM of
personality. It provides asystematic assessment of emotional,
interper-sonal, experiential, attitudinal, and motivational
styles. The NEO-PI-R is a concise measure ofthe five major
domains of personality (neuroti-cism, extraversion, openness,
agreeableness,
and conscientiousness), as well as six facetsassessing more
specific traits comprising eachdomain. Parallel forms of the
NEO-PI-R wereused for self- (form S) and informant-reports
(form R). Items are rated on a 5-point Likertscale, with
responses ranging fromstrongly dis-agreetostrongly agree. Taken
together, the fivedomains and 30 facet scales of the
NEO-PI-Rprovide a comprehensive and detailed assess-ment of adult
personality.
PD counts were computed by summingscores on FFM facets that were
deemed proto-typically high or low as reported by Lynam andWidiger
(2001). Prototypically low facet scoreswere reverse coded, and
summed with prototyp-ically high facet scores. For example,
theSchizotypal PD prototype was computed bysumming two facets of
neuroticism (anxiety andself-consciousness), one facet of
openness(ideas), three reverse-scored facets of extraver-sion
(warmth, gregariousness, and positiveemotions), and one
reverse-scored facet of con-scientiousness (order). Count scores
were cre-ated for each of the 10 PDs, and separate scoreswere
computed for self- and informant-ratings.We used the revised
scoring method for theDependent PD count (Miller & Lynam,
2008).1
Results
Nine percent of the participants in our samplequalify for a
diagnosis of at least one PD. Thisprevalence rate is comparable to
those reportedin other epidemiological studies, which consis-tently
find estimates of 913% (e.g., Ekselius,Tillfors, Furmark, &
Fredrikson, 2001; Samuelset al., 2002; Torgerson, 2005). An
addi-tional 8.6% of our participants (i.e., those whodid not
qualify for a PD) fell short of a diagnosisby only one
criterion.
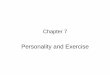
We began our analyses by considering self-other agreement on the
NEO-PI-R, both at thedomain and the facet level. As demonstrated
inTable 2, bivariate correlations were generallymoderate and all
were significant at the p .01level. Domain correlation coefficients
rangedfrom .35 (agreeableness) to .51 (both extraver-sion and
openness). Facet-level rs ranged from
1
Although a prototype exists for psychopathic personal-ity, the
discussion surrounding its relationship to AntisocialPD lies beyond
the scope of the current study. For thisreason, it is not included
in these analyses.
5SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
7/15
.23 (altruism, from the agreeableness domain)to .57 (aesthetics,
from the openness domain).Median rs within each domain were .37
(neu-roticism), .47 (extraversion), .46 (openness),
.32(agreeableness), and .38 (conscientiousness).
We then examined the relations among inter-view-based PD scores
pathology, self-reportedprototypes, and informant-reported
prototypesusing bivariate correlations (see diagonals inTable 6).
The self-reported prototypes correlate
significantly (p .01) with SIDP scores fornine of the 10 PDs,
the exception being Obses-sive-Compulsive PD. Of these nine
significant
findings, correlation coefficients ranged from.22 (Schizotypal
PD) to .50 (Avoidant PD), witha medianrof .34. We found the same
pattern ofcorrelations between informant-reported proto-
types and SIDP scores, again with the onlynonsignificant result
being Obsessive-Compul-sive PD. Significant correlations ranged
from.14 (Schizotypal PD) to .39 (Borderline PD),with a median r of
.24. The correlations be-tween self-reported prototypes and
informant-reported prototypes were as follows: Paranoid(.42),
Schizoid (.51), Schizotypal (.50), Antiso-cial (.45), Borderline
(.43), Histrionic (.47),Narcissistic (.43), Avoidant (.55),
Dependent(.44), ObsessiveCompulsive PD (.52). Allwere significant
at the p .01 level.
Next, we examined the connection betweenself-reported NEO
prototypes and the SIDP af-ter controlling for the variance
accounted for byneuroticism and agreeableness using partial
cor-relations. This analysis was conducted to ensurethat these
prototypes provided incremental va-lidity beyond the broad
personality domainsthat are most obviously associated with PDs.
Ascan be seen in Table 3, the prototypes continueto correlate
significantly (p .01) with SIDPpathology for all 10 PDs even after
partialing
these two related higher-order factors, demon-strating the
incremental validity of the proto-types. Partial correlation
coefficients range from.09 (Paranoid) to .36 (Schizoid) with a
medianpartial rof .16.
We also used partial correlations to explorethe association
between informant-reported pro-totypes and the SIDP while
controlling for self-
Table 3
Correlations Between SIDP Interview Scores andSelf Prototype
After Controlling for Levels ofNeuroticism and Agreeableness
pr p
Paranoid .09 .01
Schizoid .36 .001
Schizotypal .13 .001
Antisocial .16 .001
Borderline .16 .001
Histrionic .32 .001
Narcissistic .13 .001
Avoidant .31 .001
Dependent .16 .001Obsessive-compulsive .10 .01
Note. N 862.
Table 2Self-Other Agreement of NEO-PI-R Domains
and Facets
r
Anxiety .39
Angry hostility .36
Depression .46
Self-consciousness .32
Impulsiveness .37
Vulnerability .37
Neuroticism .46
Warmth .41
Gregariousness .49
Assertiveness .50
Activity .48
Excitement seeking .45
Positive emotions .44
Extraversion .51Fantasy .30
Aesthetics .57
Feelings .36
Actions .43
Ideas .48
Values .54
Openness .51
Trust .35
Straightforwardness .24
Altruism .23
Compliance .39
Modesty .30
Tendermindedness .34Agreeableness .35
Competence .35
Order .50
Dutifulness .30
Achievement striving .43
Self-discipline .40
Deliberation .27
Conscientiousness .42
Note. N varies from 491 to 502 across correlations due
tosporadic missing data. All correlations were significant at
p 0.01.
6 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
8/15
reported prototypes. As Table 4 shows, five ofthe 10 informant
prototypes maintain a signifi-cant relationship with the SIDP at p
.05. Wefound interesting that all four Cluster B PDs
were significant, with Schizoid PD yielding thefinal significant
result. Among the significantpartial correlations, coefficients
range from .08(Schizoid PD) to .24 (Borderline PD).
We subsequently examined the associationsamong the self-reported
prototypes as the firststep in evaluating their convergent and
discrim-inant validity. As can be seen in Table 5, cor-relations
are mostly moderate with a few in thehigh range. Significant
correlations among self-reported prototypes range from .07
(betweenAntisocial and Schizotypal PD, p .05) to .86(between
Antisocial and Narcissistic PD). Themedianrwas .43. The analysis
was repeated forthe informant-reported prototypes, and the re-sults
show a similar pattern. Significant corre-lations among informant
prototypes range from.08 (Borderline with Schizoid, p .05) to
.90(Antisocial with Narcissistic, p .01). Themedianrwas .40.
Additionally, Cronbachs al-phas were largely good to very good. The
low-est alpha was obtained for Schizotypal PD (.54and .53 for self-
and informant- report, respec-
tively) and the highest was obtained with De-pendent PD (.87 for
self-report and .86 for in-formants). The median alpha for
self-reportedprototypes was .67 and for
informant-reportedprototypes was .76.
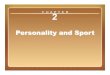
We concluded our analyses by extending theexamination of the
validity of the self- andinformant-reported prototypes using SIDP
rat-ings as the criteria. The heterotrait-hetero-
method matrix (as defined by Campbell &Fiske, 1959) for
self-report in Table 6 showsthat each of the values in the validity
diagonalare significant, with the exception of Obsessive-
Compulsive PD. Five of the 10 PDs demon-strate good convergent
validity. The Schizoid,Borderline, Histrionic, Narcissistic,
andAvoidant prototypes each show their highestcorrelation with
their corresponding SIDP PDratings. Of the five prototypes showing
conver-gent validity, four demonstrate a particularlystrong pattern
of discriminant validity (Border-line, Histrionic, Narcissistic,
and Avoidant).Median discriminant r across all PDs was .13(p .01).
Furthermore, expected relationshipsamong the PDs emerged across
measurementtype. It is interesting that the presence of nu-merous
negative correlations suggests that asimple halo effect, or
tendency to endorse, isunlikely.
The heterotrait-heteromethod matrix for in-formant-report shows
generally lower correla-tions, but largely the same pattern as that
of theself. Nine of the 10 coefficients in the validitydiagonal
(all but Obsessive-Compulsive PD)are significant. Similarly, the
Schizoid, Border-line, Histrionic, Narcissistic, and Avoidant
PD
prototypes demonstrate good convergent valid-ity. The latter
four again showed the strongestpattern of discriminant validity.
Median dis-criminantramong informant prototypes acrossall disorders
was .10 (p .01). We find ex-pected relationships among the PDs
within in-formant report, as well.
Discussion
The transition to a dimensional model of PDs
would afford many empirically supported ben-efits. This
conceptualization provides more in-formation, offers a way to
describe diagnosticco-occurrence and within-disorder
heterogene-ity, and avoids the dichotomization of aconsistently
demonstrated continuous variable(Livesley, 1998; Widiger &
Chaynes, 2003).Additionally, research has shown the
distinctionbetween normal and abnormal personality to belargely
arbitrary (OConnor, 2002). For in-stance, the DSMIVPDs are largely
able to bedescribed within the framework of the FFM
(Schroeder et al., 1992; Widiger & Trull, 2007)and IRT
analyses indicate a great deal of over-lap among the NEO and
measures of personality
Table 4Correlations Between Informant Prototype and
SIDP Rating After Partialing Self Prototype
pr p
Paranoid .07 .06
Schizoid .08 .04
Schizotypal .04 .33
Antisocial .15 .001
Borderline .24 .001
Histrionic .09 .02
Narcissistic .15 .001
Avoidant .07 .08
Dependent .06 .10Obsessive-compulsive .00 .92
Note. N 729.
7SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
9/15
Table5
BivariateCorrelationsAmongSelf-ReportedPrototypesandAmongInforma
nt-ReportedPrototypes
Self-reportedNEO
prototypes
Paranoi
d
Schizoid
Schizotypal
Antis
ocial
Borderline
Histrionic
N
arcissistic
Avoidant
Dependent
Obsessive-
compulsive
Paranoid
(.79)
Schizoid
.62
(.79)
Schizotypal
.61
.68
(.54)
Antisocial
.48
.2
2
.07
(.6
0)
Borderlin
e
.41
.05
.52
.4
5
(.74)
Histrionic
.5
0
.8
3
.4
4
.4
0
.24
(.63)
Narcissis
tic
.68
.05
.21
.8
6
.28
.01
(.60)
Avoidant
.49
.84
.74
.3
8
.30
.7
1
.2
0
(.70)
Dependent
.48
.44
.70
.1
2
.79
.1
7
.07
.68
(.87)
Obsessiv
e-compulsive
.06
.20
.2
0
.5
1
.4
9
.5
7
.1
5
.21
.3
3
(.55)
Informant-reportedNEO
prototyp
es
Paranoid
(.85)
Schizoid
.60
(.80)
Schizotypal
.61
.68
(.53)
Antisocial
.65
.0
3
.19
(.7
4)
Borderlin
e
.48
.08
.54
.5
4
(.78)
Histrionic
.4
0
.7
5
.4
0
.3
4
.27
(.63)
Narcissis
tic
.80
.17
.28
.9
0
.40
.01
(.74)
Avoidant
.39
.79
.73
.2
8
.30
.6
1
.1
5
(.67)
Dependent
.45
.38
.69
.2
7
.83
.0
2
.18
.61
(.86)
Obsessiv
e-compulsive
.0
4
.18
.1
5
.5
1
.4
3
.5
2
.2
2
.28
.3
9
(.65)
Note.
S
elf-reportedNEO
prototypeN
875,
andinformant-reportedN
760.
Valuesonthediagonalsindicateinternalconsistencycoefficients.
p
.05.
p
0.0
1.
8 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
10/15
pathology (Samuel et al., 2010). Lynam andWidiger (2001)
proposed expert-generatedNEO prototypes that, along with Miller,
Bagby,Pilkonis et al.s (2005) count score method,have largely
demonstrated good convergent anddiscriminant validity. These
prototypes have
also shown satisfactory predictive validity andstrong temporal
stability.While previous studies have demonstrated
the utility of the prototypes, most have done soin clinical
samples. Our representative sampleof community residents not only
taps a typicallyoverlooked population in PD research (the5564 age
group), but also utilizes informantreport. While informant report
is likely to beuseful for the assessment of many disorders andtheir
associated functioning, we believe that it isparticularly important
for PDs due to their ego-
syntonic nature. To our knowledge, this is thefirst study
examining the informant-reportedprototypes in an adult, community
sample. The
present study therefore takes advantage of anovel sample to
broaden the scope of the pro-totypes use.
In the current study, we first wanted to deter-mine whether the
prototypes were useful in oursample of later middle-aged adults. We
found
that, with the exception of Obsessive-Compul-sive PD, the PD
prototypes as reported by bothself and informant were significantly
correlatedwith ratings based on the SIDP interview. TheSIDP was
used as the validity criterion, becausesemistructured diagnostic
interviews are oftenconsidered the gold standard in personality
dis-order assessment. It is not our intention, how-ever, to suggest
that the DSMIVor its relatedmeasures are without fault. Instead our
goal wasto compare two alternative approaches to themeasurement of
latent constructs associated
with conventionally accepted definitions of per-sonality
pathology. Ultimately, the questionwill be which measure proves
more value with
Table 6Bivariate Correlations Among Self- and Informant-Reported
NEO PD Prototypes and SIDP Ratings
SIDP ratings
Self-reported NEO PD prototypes
PRD SZD SZTL ASPD BDL HSTR NARC AVD DEP OCPD
PND .33 .12 .22 .17 .24 .14 .22 .16 .23 .02
SZD .34 .39 .34 .02 .08 .33 .11 .32 .16 .07
SZTL .26 .17 .22 .09 .13 .16 .17 .14 .15 .03
ASPD .20 .00 .07 .26 .20 .06 .22 .01 .15 .15
BDL .29 .08 .25 .25 .47 .02 .19 .17 .39 .18
HSTR .01 .29 .11 .26 .22 .29 .12 .22 .07 .20
NARC .17 .14 .04 .34 .13 .14 .34 .18 .02 .07
AVD .27 .38 .45 .16 .31 .29 .11 .50 .49 .02
DEP .13 .15 .21 .05 .27 .05 .09 .28 .38 .09
OCPD .22 .11 .22 .05 .19 .09 .06 .18 .21 .02
Informant-reported NEO PD prototypes
PRD SZD SZTL ASPD BDL HSTR NARC AVD DEP OCPD
PND .20 .08 .13 .15 .18 .04 .16 .07 .17 .06
SZD .23 .25 .25 .05 .10 .20 .11 .20 .15 .01
SZTL .18 .09 .14 .14 .13 .06 .15 .07 .15 .08
ASPD .22 .05 .10 .24 .19 .04 .22 .02 .16 .15
BDL .25 .10 .23 .24 .39 .05 .18 .13 .36 .20
HSTR .03 .17 .05 .19 .18 .21 .12 .13 .09 .16
NARC .18 .04 .08 .29 .12 .08 .29 .13 .02 .09
AVD .15 .24 .25 .06 .18 .18 .03 .33 .27 .03
DEP .03 .05 .11 .02 .19 .02 .06 .16 .23 .06
OCPD .14 .14 .18 .04 .07 .11 .06 .14 .11 .00
Note. Self,N 898; Informant,N 743. PND Paranoid; SZD Schizoid;
SZTL Schizotypal; ASPD Antisocial
Personality; BDL Borderline; HSTR Histrionic; NARC Narcissistic;
AVD Avoidant; DEP Dependent;OCPD Obsessive-compulsive Personality
Disorder. p 0.01. p .05.
9SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
11/15
regard to identifying current and future prob-lems in social
adjustment, health, and subjectivewell-being. In a far more
stringent test of utility,we computed partial correlations while
control-
ling for neuroticism and agreeableness. As ex-pected, the
strength of the associations de-creased, but all 10 relationships
remained sig-nificant at the p .01 level or below,
withObsessive-Compulsive PD actually becomingsignificant. Because
neuroticism and agreeable-ness are the global personality domains
mostconsistently associated with PDs (OConnor,2002), these results
are a robust testament to thevalue of the prototypes, and
demonstrate theirutility in a middle-aged sample.
We also found levels of self-other agreementamong the prototypes
very similar to those re-ported by Miller, Pilkonis et al. (2004).
Theseauthors reported a median correlation of .47,while we found a
median correlation of .46. Ofnote, the self-other agreement between
the pro-totypes (as reported here and in the Miller,Pilkonis, et
al., 2004 study) is generally largerthan that found using other
measures of patho-logical personality (Klonsky et al.,
2002).Perhaps informants are more familiar with con-sidering others
normal range traits and be-
haviors than those of a pathological nature. Thefact that
correlations between the prototypesand the SIDP are lower than
those between self-and informant-reported prototypes is not
sur-prising given the method variance of both in-terview versus
questionnaire and normal versusabnormal personality
functioning.
We next examined the contribution of infor-mant report with
respect to the prototypes. Theinformant report correlated
moderately with selfreport for all 10 PDs. An even more
compelling
argument for the use of informants in additionto self report is
that, for five of the 10 PDs,informants account for unique variance
in theinterviewers ratings after controlling for theself. Other
report adds significant predictiveutility for Schizoid, Antisocial,
Borderline, His-trionic, and Narcissistic PDs. The fact that
allfour Cluster B disorders emerge as significant isconsistent with
findings that the observability ofthe features may play a key role
in the extent ofself-other agreement (Miller, Pilkonis, et
al.,2004). However, our results further suggest that
observability may also play an important role inthe ability of
others to contribute additionalinformation. It is therefore
remarkable that in-
formants account for unique variance in osten-sibly more
internalizing disorders, such asSchizoid (p .04) and Avoidant (p
.08)PDs. Because these prototypes contain a num-
ber of facets of extraversion, we might haveexpected higher
self-other agreement for theseprototypes. However, we did not
necessarilyexpect informants to provide more informationthan the
self. In this way, the performance ofinformant-reported prototypes
somewhat ex-ceeded our expectations. The replication of thisfinding
and its interpretation within the self-other knowledge asymmetry
model (Vazire,2010) will be an interesting direction for
futureresearch.
The interrelationships among the prototypesfor both self and
informant were also encourag-ing. Associations between disorders
that wewould expect to see (e.g., Schizoid andAvoidant, or
Antisocial and Narcissistic) didemerge. Although within-cluster
correlationsare not specifically high, which might be ex-pected,
the associations between disorders areoften intuitive. For example,
the strong relationbetween Borderline and Dependent is likelydriven
by the intense fear of being left alone thatis characteristic of
both PDs. Conversely the
insignificant relation between Histrionic andNarcissistic PD is
also easily interpretable, asHistrionic PD is characterized by
feelings ofcloseness toward many people while Narcis-sistic is
characterized by feelings of superior-ity over others. It is
important that theserelationships were mirrored in the
informant-reported prototypes. This suggests that thereis not
simply a tendency to generalize positiveor negative feelings toward
a target, but ratherinformants are painting nuanced pictures of
the participants.We also find evidence of good
convergentvalidity for the Schizoid, Borderline,
Histrionic,Narcissistic, and Avoidant prototypes, and aparticularly
strong pattern of discriminant va-lidity for the latter four
disorders. Because anumber of the PDs as we currently know themare
facing potential elimination (includingSchizoid, Histrionic, and
Narcissistic), countscores such as these may be the method bywhich
the constructs in question need to beassessed. The demonstration of
convergent and
discriminant validity in these PDs are thereforeparticularly
encouraging. Among the five re-maining prototypes that did not
demonstrate
10 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
12/15
convergent validity, four shared their largestcorrelation with
an intuitive alternative, or wereconsistent with co-occurrence
literature (e.g.,Lenzenweger et al., 2007; Oldham et al.,
1992).
Namely, the Paranoid prototype was slightlymore strongly related
to Schizoid SIDP ratings,Schizotypal was most strongly related
toAvoidant, Antisocial most highly correlatedwith Narcissistic PD
ratings, and Dependentslargest association was with Borderline PD.
Un-like pathological personality measures thatlargely do not have
items that contribute tomultiple disorders, the PD prototypes
necessar-ily contain overlap, as they are driven by theitems.
Of particular interest is the relationship be-tween Antisocial
and Narcissistic PDs. Thesetwo disorders are consistently shown to
behighly correlated (Gunderson & Ronningstam,2001; Oldham et
al., 1992), and the presentstudy finds the Antisocial prototype
morehighly related to SIDP ratings of Narcissismthan to those of
Antisocial. One potential inter-pretation of this result is that,
as Antisocialindividuals age, they find themselves unable toengage
in the reckless or aggressive behaviorsindicative of this disorder.
Instead, they may
turn to more subtle actions, such as manipula-tion. The concept
of heterotypic continuity sug-gests that there may be a number of
ways inwhich a latent trait can manifest, and this man-ifestation
may be dependent upon context (e.g.,across cultures or age). Thus,
it is possible thatantisocial behaviors shift toward a more
narcis-sistic presentation as the person approacheslater life. We
mention this simply because theexamination of potential heterotypic
continuitywill be an important direction for further re-
search in the study of PDs in older adults.Although expected
relations emerge as stron-ger, a large number of the correlations
amongprototypes are significant. These, as well as thesomewhat low
discriminant validity of a few ofthe disorders, attest to the
considerable overlapamong the constructs (Lenzenweger et al.,2007;
Widiger & Chaynes, 2003). Because PDsare highly co-occurring
syndromes, we wouldexpect toand dofind the same to be true forthe
prototypes.
One noticeable aspect of our results is the
relatively weak evidence for the validity of theSchizotypal
prototype. It has the lowest corre-lation with the SIDP for both
self- and infor-
mant-report. Furthermore, the prototype corre-lates highly with
Avoidant and Dependent PDs(.74 and .70, respectively for self
report, and .73and .69 for informants). Similarly when com-
pared with the SIDP, the Schizotypal prototypeshows poor
convergent and discriminant valid-ity. The strong relation with
Avoidant PD par-ticularly suggests that this prototype may bedoing
an adequate job of tapping interpersonaldiscomfort. However,
because the NEO-PI-Rwas developed to assess general
personality,aspects of Schizotypal PD such as odd percep-tual
experiences are not covered well. Kruegerand Eaton (2010) instead
argue that an alterna-tive personality dimension, which they term
pe-culiarity, is needed to obtain sufficient coverageof this
disorder. Inquiries such as these arebecoming increasingly
important as DSM-5discussions continue.
A potential limitation of the current study isthat the strength
of the associations dependsupon the amount of variability in the
sample.Because ours is a representative communitysample of later
middle-aged adults, we havelimited variation with respect to the
features ofsome disorders. As compared with the others,we found
relatively poor convergent and dis-
criminant validity for Schizotypal, Antisocial,and Dependent
PDs. These disorders are lesswell represented in our sample, which
may sim-ply indicate that with greater heterogeneity,stronger
patterns of validity may emerge.
In addition, some aspects of the FFM havebeen criticized for
their inability to describepathological personality traits. Some
research-ers have questioned whether these prototypesare subject to
a ceiling effect. For instance, onewould expect a relationship
between conscien-
tiousness and Obsessive-Compulsive PD. How-ever, this
relationship is consistently reported asweak or absent (Miller,
Bagby, Pilkonis, et al.,2005; Trull, 1992). Haigler and Widiger
(2001)suggest that the NEO-PI-R uses considerablymore adaptive
behaviors to define the high endof conscientiousness,
agreeableness, and open-ness in comparison to items that define the
lowends of these dimensions. In an attempt to cap-ture the more
maladaptive extremes of the do-mains, Haigler and Widigers study
rewordeditems from the NEO-PI-R (e.g., by adding the
word excessively). These authors found thatcorrelations between
Obsessive-CompulsivePD and conscientiousness increased
markedly.
11SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
13/15
In a similar vein, the Pathological Five Model(Krueger &
Eaton, 2010) has been proposed forincorporation into the DSM-5 as a
means ofassessing the maladaptive extremes of neuroti-
cism, extraversion, agreeableness, and consci-entiousness. Their
proposed domains thereforeconsist of negative emotionality,
introversion,antagonism, and disinhibition. As noted above,they
label their fifth domain peculiarity. Therelationship between
peculiarity and opennessis still relatively unexplored, but appears
to benonredundant. Investigating the relationship be-tween the PD
prototypes and models that spe-cifically attempt to include
pathological featureswill be an interesting and important avenue
forfuture research.
Conversely, one could argue that the use ofDSMIVPD
conceptualizations as the validitycriterion provides drawbacks of
its own. In theirexamination of clinician-rated NEO PD proto-types,
Miller et al. (2010) found that these pro-totypes accounted for
unique variance (i.e., be-yond that ofDSMIVcategories) in
occupation,social, and overall impairment, as well as dis-tress
caused to others. This research indicatesthat, while the
predominant model, the currentDSM is limited in its function as the
point of
comparison. It also highlights the importance ofvaried
validation criteria.
Though the 10 PDs as they are currentlydefined may not be
retained in DSM-5, severalprinciples appear to emerge from the
presentanalyses. Indeed, these are precisely the issuesraised by
Krueger, Skodol, Livesley, Shrout,and Huang (2007) in their
discussion of direc-tions for DSM-5. Their review speaks
specifi-cally to the use of facet-level traits to
compriseprototypes to which individuals can be matched.
Research investigating the relative validity ofsuch models is of
critical importance as thedevelopment ofDSM-5 proceeds.
As the field approaches a dimensional con-ceptualization,
researchers will be charged withthe task of defining a model, and
thus far allevidence seems to suggest that the FFM is doinga
reasonably good job of capturing pathology.More specifically, Lynam
and Widigers (2001)PD prototypes have been useful in a variety
ofsample types and age ranges. These prototypeshave also now
demonstrated similarly good
convergent and discriminant validity for infor-mant report. And
by using informants as well asself-report, we are able to explain
significant
additional variance in five of the 10 PDs. Ofcourse, the next
question is concerned with con-struct validity. By establishing the
prototypes asan empirically supported system of PDs, in
which the benefits of a dimensional model canbe coupled with
meaningful informant report,we can begin to examine its relation to
real lifeproblems and functioning.
References
American Psychiatric Association. (1994). Diagnos-tic and
statistical manual of mental disorders (4thed.). Washington, DC:
Author.
Balsis, S., Gleason, M. E., Woods, C. M., & Olt-
manns, T. F. (2007). An item response theoryanalysis of DSMIV
personality disorder criteriaacross younger and older age groups.
Psychologyand Aging, 22, 171185.
Campbell, D. T., & Fiske, D. W. (1959). Convergentand
discriminant validation by the multitrait-multimethod matrix.
Psychological Bulletin, 56,81105.
Clark, L. A. (1993). Manual for the Schedule forNonadaptive and
Adaptive Personality. Minneap-olis, MN: University of Minnesota
Press.
Clark, L. A. (2009). Stability and change in person-
ality disorder.Current Directions in Psychological
Science, 18, 2731.Costa, P. T., Jr., & McCrae, R. R. (1992).
Revised
NEO Personality Inventory (NEOPIR) and NEO
FiveFactor Inventory (NEOFFI) professionalmanual. Odessa, FL:
Psychological AssessmentResources.
Costa, P. T., Jr., & McCrae, R. R. (1994). Stabilityand
change in personality from adolescencethrough adulthood. In C. F.
Halverson, G. A.Kohnstamm, & R. P. Martin (Eds.), The
develop-ing structure of temperament and personality from
infancy to adulthood. Hilldale, NJ: Erlbaum, Inc.
Costa, P. T., Jr., & Widiger, T. A. (Eds.).
(2002).Personality disorders and the five-factor model of
personality (2nd ed.). Washington, DC: AmericanPsychological
Association.
Ekselius, L., Tillfors, M., Furmark, T., & Fredrikson,M.
(2001). Personality disorders in the generalpopulation: DSMIV and
ICD-19 defined preva-lence as related to sociodemographic profile.
Per-sonality and Individual Differences, 30, 311320.
Grant, B. F., Hasin, D. S., Stinson, F. S., Dawson,D. A., Chou,
S. P., Ruan, W. J., & Pickering, R. P.(2004). Prevalence,
correlates, and disability ofpersonality disorders in the United
States: Resultsfrom the National Epidemiologic Survey on Alco-hol
and Related Concerns.Journal of Clinical Psy-chiatry, 65,
948958.
12 LAWTON, SHIELDS, AND OLTMANNS
-
8/11/2019 Personality DisordersTheory, Research, And
14/15
Gunderson, J. G., & Ronningstam, E. (2001). Differ-entiating
narcissistic and antisocial personality dis-orders.Journal of
Personality Disorders, 15, 103109.
Haigler, E. D., & Widiger, T. A. (2001). Experimen-tal
manipulation of NEO-PI-R items. Journal ofPersonality Assessment,
77, 339358.
Harkness, A. R., Tellegen, A., & Waller, N.
(1995).Differential convergence of self-report and infor-mant data
for Multidimensional Personality Ques-tionnaire traits:
Implications for the construct ofnegative emotionality. Journal of
Personality As-sessment, 64, 185204.
Kish, L. (1949). A procedure for objective respon-dent selection
within the household.Journal of theAmerican Statistical
Association, 44, 380387.
Klonsky, E. D., Oltmanns, T. F., & Turkheimer, E.
(2002). Informant-reports of personality disorder:Relation to
self-reports and future research direc-tions. Clinical Psychology:
Science and Prac-tice, 9, 300311.
Krueger, R. F., & Eaton, N. R. (2010). Personalitytraits and
the classification of mental disorders:Toward a more complete
integration in DSM-5andan empirical model of psychopathology.
Person-ality Disorders: Theory, Research, and Treat-
ment, 1, 97118.Krueger, R. F., Skodol, A. E., Livesley, W. J.,
Shrout,
P. E., & Huang, Y. (2007). Synthesizing dimen-
sional and categorical approaches to personalitydisorders:
Refining the research agenda for DSM-5Axis II. International
Journal of Methods in Psy-chiatric Research, 16, 6573.
Lenzenweger, M. F., Lane, M. C., Loranger, A. W.,& Kessler,
R. C. (2007). DSMIVpersonality dis-orders in the national
comorbidity survey replica-tion.Biological Psychiatry, 62,
553564.
Livesley, W. J. (1998). Suggestions for a frameworkfor an
empirically based classification of person-ality disorder.Canadian
Journal of Psychiatry Re-vue Canadienne De Psychiatrie, 43,
137147.
Livesley, W. J., & Jackson, D. (2009).Manual for
theDimensional Assessment of Personality Patholo-gy-Basic
Questionnaire. Port Huron, MI: SigmaPress.
Lynam, D. R., & Widiger, T. A. (2001). Using thefive-factor
model to represent theDSMIVperson-ality disorders: An expert
consensus approach.Journal of Abnormal Psychology, 110, 401412.
Miller, J. D., Bagby, R. M., & Pilkonis, P. A. (2005).A
comparison of the validity of the five-factormodel (FFM)
personality disorder prototypes us-ing FFM self-report and
interview measures. Psy-chological Assessment, 17, 497500.
Miller, J. D., Bagby, R. M., Pilkonis, P. A., Reyn-olds, S. K.,
& Lynam, D. R. (2005). A simplifiedtechnique for scoring DSMIV
personality disor-
ders with the five-factor model. Assessment, 12,404415.
Miller, J. D., & Lynam, D. R. (2008). Dependentpersonality
disorder: Comparing an expert gener-ated and empirically derived
five-factor model per-sonality disorder count. Assessment, 15,
415.
Miller, J. D., Lynam, D. R., Rolland, J. P., De Fruyt,F.,
Reynolds, S. K., Pham-Scottez, A., . . . Bagby,R. M. (2008).
Scoring the DSMIV personalitydisorders using the five-factor model:
Develop-ment and validation of normative scores for NorthAmerican,
French, and Dutch-Flemish samples.Journal of Personality Disorders,
22, 433450.
Miller, J. D., Maples, J., Few, L. R., Morse, J. Q.,Yaggi, K.
E., & Pilkonis, P. A. (2010). Usingclinician-rated five-factor
model data to score theDSMIVpersonality disorders.Journal of
Person-
ality Assessment, 92, 296305.Miller, J. D., Pilkonis, P. A.,
& Clifton, A. (2005).
Self- and other-reports of traits from the five-factormodel:
Relations to personality disorder. Journalof Personality Disorders,
19, 400419.
Miller, J. D., Pilkonis, P. A., & Morse, J. Q.
(2004).Five-factor model prototypes for personality dis-orders: The
utility of self-reports and observerratings. Assessment, 11,
127138.
Miller, J. D., Reynolds, S. K., & Pilkonis, P. A.(2004). The
validity of the five-factor model pro-totypes for personality
disorders in two clinicalsamples. Psychological Assessment, 16,
310322.
Naumann, L. P., Vazire, S., Rentfrow, P. J., & Gos-ling, S.
D. (2009). Personality judgments based onphysical appearance.
Personality and Social Psy-chology Bulletin, 35, 16611671.
OConnor, B. P. (2002). The search for dimensionalstructure
differences between normality and abnor-mality: A statistical
review of published data onpersonality and psychopathology. Journal
of Per-sonality and Social Psychology, 83, 962982.
Oldham, J. M., Skodol, A. E., Kellman, H. D., Hyler,S. E.,
Rosnick, L., & Davies, M. (1992). DiagnosisofDSMIIIR
personality disorders by two struc-
tured interviews: Patterns of comorbidity. TheAmerican Journal
of Psychiatry, 149, 213220.
Oltmanns, T. F., & Gleason, M. E. J. (2011). Person-ality,
health, and social adjustment in later life. InL. B. Cottler (Ed.),
Mental health in public health:The next 100 years. New York: Oxford
UniversityPress.
Oltmanns, T. F., & Turkheimer, E. (2009). Personperception
and personality pathology. Current Di-rections in Psychological
Science, 18, 3236.
Pfohl, B., Blum, N., & Zimmerman, M. (1997). Struc-tured
interview for DSMIV personality. Washing-ton, DC: American
Psychiatric Association.
Samuel, D. B., Simms, L. J., Clark, L. A., Livesley,W. J., &
Widiger, T. A. (2010). An item responsetheory integration of normal
and abnormal person-
13SELF AND INFORMANT PD PROTOTYPES
-
8/11/2019 Personality DisordersTheory, Research, And
15/15
ality scales. Personality Disorders: Theory, Re-search, and
Treatment, 1, 521.
Samuels, J., Eaton, W. W., Bienvenu, O. J., III,Brown, C. H.,
Costa, P. T., Jr., & Nestadt, G.(2002). Prevalence and
correlates of personalitydisorders in a community sample. British
Journalof Psychiatry, 180, 536542.
Saulsman, L., & Page, A. C. (2004). The five-factormodel and
personality disorder empirical litera-ture: A meta-analytic review.
Clinical PsychologyReview, 23, 10551085.
Schroeder, M. L., Wormworth, J. A., & Livesley,W. J. (1992).
Dimensions of personality disorderand their relationships to the
big five dimensions ofpersonality. Psychological Assessment, 4,
4753.
Skodol, A. E., Oldham, J. M., Bender, D. S., Dyck,I. R., Stout,
R. L., Morey, L. C., . . . Gunderson,
J. G. (2005). Dimensional representations ofDSMIV personality
disorders: Relationships tofunctional impairment. The American
Journal ofPsychiatry, 162, 19191925.
Torgersen, S. (2005). Epidemiology. In J. M. Old-ham, A. E.
Skodol, & D. S. Bender (Eds.), Text-book of personality
disorders (pp. 129141). Ar-lington, VA: American Psychiatric
Publishing,Inc.
Torgersen, S., Kringlen, E., & Cramer, V. (2001).The
prevalence of personality disorders in a com-munity sample.
Archives of General Psychia-try, 58, 590596.
Trull, T. J. (1992). DSMIIIR personality disordersand the
five-factor model of personality: An em-pirical comparison.Journal
of Abnormal Psychol-ogy, 101, 553560.
Trull, T. J., & McCrae, R. R. (2002). A
five-factorperspective on personality disorder research. In
P. T. Costa, Jr. & T. A. Widiger (Eds.),
Personalitydisorders and the five-factor model of personality
(2nd ed., pp. 4557). Washington, DC: AmericanPsychological
Association.
Vazire, S. (2010). Who knows what about a person?The self-other
knowledge asymmetry (SOKA)model. Journal of Personality and Social
Psychol-ogy, 98, 281300.
Widiger, T. A. (1992). Categorical versus dimen-sional
classification: Implications from and for re-search.Journal of
Personality Disorders, 6, 287300.
Widiger, T. A., & Chaynes, K. (2003). Current issuesin the
assessment of personality disorders. CurrentPsychiatry Reports, 5,
2835.
Widiger, T. A., & Frances, A. J. (2002). Toward adimensional
model for the personality disorders. In
P. T. Costa, Jr. & T. A. Widiger (Eds.),
Personalitydisorders and the five-factor model of personality
(2nd ed., pp. 2344). Washington, DC: AmericanPsychological
Association.
Widiger, T. A., & Samuel, D. B. (2005). Evidence-based
assessment of personality disorders.Psycho-logical Assessment, 17,
278287.
Widiger, T. A., & Trull, T. J. (2007). Plate tectonicsin the
classification of personality disorder: Shift-ing to a dimensional
model. American Psycholo-gist, 62, 7183.
Widiger, T. A., Trull, T. J., Clarkin, J. F., Sanderson,C.,
& Costa, P. T., Jr. (1994). A description of theDSMIIIR and
DSMIV personality disorderswith the five-factor model of
personality. In P. T.Costa Jr. & T. A. Widiger (Eds.),
Personalitydisorders and the five-factor model of personality
(pp. 4156). Washington, DC: American Psycho-logical
Association.
14 LAWTON, SHIELDS, AND OLTMANNS