Embed Size (px)
Citation preview

SHORT REPORT
Persistent polyclonal B-cell lymphocytosis in identical twins
ROBERT CARR, KE ITH FIS HLOC K AND ESTE LLA MATUTE S* Department of Haematology, St Thomas’ Hospital,and *Department of Haematology, The Royal Marsden Hospital, London
Received 25 July 1996; accepted for publication 14 October 1996
Summary. This is the first report of the unusual syndrome ofpersistent polyclonal B-cell lymphocytosis occurring inmonozygotic twins. The syndrome is characterized by alymphocytosis, with circulating atypical, binucleated lym-phocytes, mild splenomegaly and raised serum IgM. It occurspredominantly in females, with serological evidence ofprevious EBV infection, and is associated with cigarette
smoking and HLA-DR7 phenotype. The association withDR7 suggests a genetic predisposition. Its occurrence inidentical twins, documented here, provides stronger supportfor a hereditary/genetic basis for the syndrome.
Keywords: polyclonal lymphocytosis, binucleated lympho-cytes, genetic predisposition, twins.
Over the past decade several reports have described cases ofasymptomatic patients with a characteristic polyclonal B-celllymphocytosis (PBL). The first description was in 1982(Gordon et al, 1982) and, more recently, a series of sixpatients whose lymphocytosis had remained stable for up to16 years of observation was reported (Troussard et al, 1994).
Patients with this syndrome have a mild lymphocytosis inthe range 5–15 × 109/l. The lymphocytes have a character-istic morphology, being medium sized with abundant clearcytoplasm and nuclei which range from being indented, orbilobed with a slender intranuclear bridge, to cells with twoapparently separate nuclei. All patients tested have had apolyclonal increase in serum IgM, with low to normal levelsof IgG and IgA. Approximately half have mild splenomegaly.Cell marker studies demonstrate the polyclonal B-cell natureof the lymphocyte population, which expresses both kappaand lambda light chains. In many cases the cells are positivewith FMC7, a marker expressed in most B-lymphoprolifera-tive diseases (Matutes et al, 1994). Most patients reportedhave been middle-aged females, heavy smokers, and withserological evidence of past EBV infection. In addition, themajority of cases have carried the HLA type DR7, which hasa normal frequency of only 26% in Caucasians (Gordon et al,1982; Carstairs et al, 1985; Casassus et al, 1987; Perreaultet al, 1989; Delannoy et al, 1993; Agrawal et al, 1994).The association of this syndrome with HLA-DR7 suggestsa genetic predisposition. Some further support for thiswas the finding by Troussard et al (1994) of occasional
similar binucleated lymphocytes in buffy coat preparationsfrom a non-smoking mother and a brother of two of theircases.
CASE REPORT
A 33-year-old Belgian lady was referred for treatment with apresumptive diagnosis of low-grade non-Hodgkin’s lym-phoma. She had no significant past history, but habituallysmoked 20 cigarettes per day. One year previously she hadhad a pre-pregnancy health screen when a mild ‘atypical’lymphocytosis had first been noted, associated with apalpable spleen. A bone marrow trephine showed normalhaemopoiesis, but with a single lymphoid nodule. 2 monthslater the lymphocytosis and splenomegaly had resolved. Shebecame pregnant, but miscarried at 3 months. Shortlyafterwards a raised lymphocyte count (6.7 × 109/l) wasagain recorded.
When first seen by us, 8 months after her miscarriage, shefelt and looked well. Her spleen was palpable 1 cm below thecostal margin and there was a single 0.5 cm supraclavicularlymph node. A thoracic and abdominal CT scan showedgeneralized but minor lymph node enlargement.
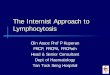
The peripheral blood count showed a lymphocytosis, withnormal haemoglobin and platelets. Most circulating lym-phocytes were medium sized with abundant cytoplasm andbilobed nuclei (Fig 1). There was a polyclonal increase in IgMand detectable anti-EBV IgG (Table I). Immunophenotypingof the blood mononuclear cells, with a panel of monoclonalantibodies, demonstrated the polyclonal B-cell nature of thelymphocytes (CD19+, kappa+, lambda+), which alsoexpressed FMC7 (Table I).
British Journal of Haematology, 1997, 96, 272–274
272 q 1997 Blackwell Science Ltd
Correspondence: Dr Robert Carr, Department of Haematology,St Thomas’ Hospital, United Medical and Dental Schools of Guy’sand St Thomas’s, Lambeth Palace Road, London SE1 7EH.

The patient had two siblings: an identical twin sister andanother sister who had died of ‘leukaemia’ during childhood.The twin sister was well, had two children aged 4 and 6years, and had a similar lifestyle, smoking 20 cigarettes daily.On examination her spleen was palpable, but only oninspiration. Laboratory investigation showed a moderatelymphocytosis (8.1 × 109/l) with peripheral blood morphol-ogy identical to her sister and characteristic of PBL (Fig 1).Additional investigations showed remarkable similarity tothose of the index case (Table I). Full tissue typing and bloodgenotyping confirmed them to be monozygotic twins, bothcarrying the HLA-DR7 haplotype.
DISCUSSION
The occurrence of the recently recognized syndrome ofpersistent polyclonal B-cell lymphocytosis in identical twinslends support to a genetic basis for the phenomenon andfurther supports the view that it is not a pre-malignantlymphoid proliferation.
That another sister died from an unspecified leukaemia inchildhood should be noted, but the significance is uncertain.One patient with PBL has developed a malignant pulmonaryblastoma 20 years after her PBL was diagnosed (Lawlor et al,1991). Two other patients have had an immunoglobulingene rearrangement identified using Southern DNA hybrid-ization (Troussard & Flandrin, 1996). But there is noconsistent pattern in these isolated cases to suggest a pre-malignant tendency.
The PBL syndrome itself has many features that suggestmalignancy to the unwary, with morphologically bizarreperipheral blood lymphocytes associated with splenomegaly,lymphoid aggregates in the bone marrow and FMC7expression. FMC7 is only expressed by a minor lymphocytepopulation in normal blood (Brooks et al, 1981), but isusually positive in most B-cell malignancies other than CLL
(Matutes et al, 1994). However, the polyclonal nature of thePBL proliferation is suggested by lack of light chainrestriction in the atypical lymphocytes and confirmed byimmunoglobin gene studies in 17 patients (Agrawal et al,1994; Troussard et al, 1994; Troussard & Flandrin, 1996).
Environmental factors that may trigger the full expressionof PBL in susceptible individuals have been discussed byothers. Evidence of past EBV infection is more common thanin the general population, and Chow et al (1992) demon-strated the presence of EBV DNA in the abnormallymphocytes of an affected patient. The association withcigarette smoking is equally strong, and in one reported casethe lymphocytosis resolved on stopping and returned onrestarting smoking (Carstairs et al, 1985).
Although further studies may elucidate the role ofenvironmental factors in the pathogenesis of PBL, thedocumentation of persistent polyclonal B-cell lymphocytosisin a pair of identical twins is strong supportive evidence for ahereditary/genetic basis for this rare syndrome.
REFERENCES
Agrawal, S., Matutes, E., Voke, J., Dyer, M.J.S., Khokhar, T. &
273Short Report
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 272–274
Fig 1. Characteristic peripheral blood lymphocytes from (left) theindex case and (right) her twin sister.
Table I. Laboratory data from the index case and her identical twinsister tested on the same date.
Index case Twin sister
Full blood countHb (g/dl) 13.8 13.4MCV (fl) 89 88WBC (×109/l) 15.0 13.9Neutrophils (×109/l) 5.1 4.4Lymphocytes (×109/l) 8.5 8.1Monocytes (×109/l) 1.2 1.1Platelets (×109/l) 245 287
Peripheral blood lymphocyte markers*CD3 (%) 22 24CD5 (%) 28 26CD19 (%) 74 64FMC7 (%) 72 64CD25 (%) 2 NTKappa (%) 35 38Lambda (%) 36 30
Serum immunoglobulinsIgM (g/l) (0.5–2.0) 7.2 6.4IgG (g/l) (5.4–16.1) 5.4 6.1IgA (g/l) (0.9–3.4) 0.3 0.3
Virus serologyEBV IgG þ þ
EBV IgM ¹ ¹
CMV IgG ¹ ¹
HLA - DR7 þ þ
The raised IgM in both patients was polyclonal; the normal rangefor immunoglobulins is shown in parentheses.
* The percentage of peripheral blood lymphocytes expressing themarker antigen.

Catovsky, D. (1994) Persistent polyclonal B-cell lymphocytosis.Leukemia Research, 18, 791–795.
Brooks, D.A., Beckman, I.G.R., Bradley, J., McNamara, P.J., Thomas,M.E. & Zola, H. (1981) Human lymphocyte markers defined byantibodies derived from somatic cell hybrids. IV. A monoclonalantibody reacting specifically with a subpopulation of human Blymphocytes. Journal of Immunology, 126, 1373–1377.
Carstairs, K.C., Francombe, W.H., Scott, J.G. & Gelfand, E.W. (1985)Persistent polyclonal lymphocytosis of B lymphocytes, induced bycigarette smoking. Lancet, i, 1094.
Casassus, P., Lortholary, P., Komarover, H., Lejeune, F. & Hors, J.(1987) Cigarette smoking-related persistent polyclonal B lympho-cytosis: a premalignant state. Archives of Pathological LaboratoryMedicine, 111, 1081.
Chow, K.C., Nacilla, J.Q., Witzig, T.E. & Li, C.Y. (1992) Is persistentpolyclonal B lymphocytosis caused by Epstein-Barr virus? A studywith polymerase chain reaction and in situ hybridization.American Journal of Hematology, 41, 270–275.
Delannoy, C., Dijan, D., Wallef, G., Deneys, V., Fally, P., Martiat, P. &Michaux, J.L. (1993) Cigarette smoking and chronic polyclonal B-cell lymphocytosis. Nouvelle Revue Francaise d’Hematologie, 35,141–144.
Gordon, D.S., Jones, B.M., Browning, S.W., Spira, T.J. & Lawrence,
D.N. (1982) Persistent polyclonal lymphocytosis of B lymphocytes.New England Journal of Medicine, 307, 232–236.
Lawlor, E., Murray, M., O’Brian, D., Blanay, C., Foroni, L., Sarsfield,P., Condell, D., Sullivan, F. & McCann, S.R. (1991) Persistentpolyclonal B lymphocytosis with Epstein Barr virus antibodies andsubsequent pulmonary blastoma. Journal of Clinical Pathology, 44,341–342.
Matutes, E., Owusu-Ankomah, K., Morilla, R., Marco, J.G., Houlian,A., Que, T.H. & Catovsky, D. (1994) The immunological profile ofB-cell disorders and proposal of a scoring system for the diagnosisof CLL. Leukemia, 8, 1640–1645.
Perreault, C., Boileau, J., Gyger, M., de Bellefeville, C., d’Angelo, G.,Belanger, R., Lacombe, M., Lavallee, R., Bonny, Y., Paquin, M. &Brochu, S. (1989) Chronic B-cell lymphocytosis. European Journalof Haematology, 42, 361–367.
Trousard, X. & Flandrin, G. (1996) Chronic B-cell lymphocytosiswith binucleated lymphocytes (LWBL): a review of 38 cases.Leukaemia and Lymphoma, 20, 275–279
Troussard, X., Valensi, F., Debert, C., Maynadie, M., Schillinger, F.,Bonnet, P., MacIntyre, E.A. & Flandrin, G. (1994) Persistentpolyclonal lymphocytosis with binucleated B lymphocytes: agenetic predisposition. British Journal of Haematology, 88, 275–280.
274 Short Report
q 1997 Blackwell Science Ltd, British Journal of Haematology 96: 272–274
![Characteristics of Bovine Lymphoma Caused by Bovine ...ajas.info/upload/pdf/18_115.pdf · polyclonal B-cell expansion in the peripheral blood (persistent lymphocytosis [PL]), and](https://img.pdfslide.us/doc/110x75/5e5ea9d6cd63f5193c20c604/characteristics-of-bovine-lymphoma-caused-by-bovine-ajasinfouploadpdf18115pdf.jpg)